
Abstract
Background
Out-of-hospital cardiac arrest (OHCA) is associated with high morbidity and mortality, often requiring complex decision-making in the intensive care unit (ICU). Palliative care may facilitate goal-aligned care but remains underutilized in this population.
Objective
To evaluate the impact of palliative care consultation on end-of-life decision-making and clinical outcomes in ICU patients following OHCA.
Methods
We conducted a mixed retrospective–prospective cohort study of 61 retrospective and 40 prospective adult patients admitted to the ICU after OHCA at a tertiary academic center. Patients were grouped by palliative care consultation. Primary outcomes were in-hospital mortality and ICU and hospital length of stay. Secondary outcomes included the proportion of patients with code status change, the timing of code status changes and withdrawal of life-sustaining treatment from ICU admission in both groups, and withdrawal of life-sustaining treatment. Illness severity was assessed using the Sequential Organ Failure Assessment (SOFA) score at ICU admission and at 72 hours.
Results
Among 101 patients admitted after OHCA, 34 (33.7%) received a palliative care consultation. In-hospital mortality was higher among patients who received palliative care consultation than among those who did not (79.4% vs 41.8%; P = 0.0003). SOFA scores at ICU admission and at 72 hours were similar between patients seen by palliative care and those not seen by palliative care (P = 0.72 and P = 0.27, respectively). All patients who received a palliative care consultation (100%) had a change in code status during hospitalization, compared to 32.8% of those who did not (P < 0.0001). The time from ICU admission to withdrawal of life-sustaining treatment was significantly longer in the palliative care group (6.0 vs 3.0 days, P = 0.016), while the time to code status change was similar between groups (P = 0.415). There were no significant differences in ICU or hospital length of stay, or use of vasopressors, mechanical ventilation, or continuous renal replacement therapy. Among patients who received palliative care consultation, the most common interventions included goals-of-care clarification (85.3%), symptom management, and spiritual or emotional support.
Conclusion
In ICU patients following OHCA, palliative care consultation was associated with higher in-hospital mortality despite similar baseline characteristics, illness severity by SOFA score, and treatment intensity, likely reflecting preferential consultation in patients with greater clinical complexity rather than a causal relationship. Palliative care consultation was strongly associated with goals-of-care redirection and a more deliberate process of end-of-life decision-making.
Introduction
Out-of-hospital cardiac arrest (OHCA) is a significant public health issue marked by high rates of morbidity and mortality, creating complex decision-making scenarios within the intensive care unit (ICU). 1 Despite advancements in medical care, survival rates are often low, and patients who do survive may face substantial long-term consequences. This situation frequently necessitates difficult conversations about the continuation or withdrawal of life-sustaining treatments. 2
Palliative care is a specialized medical approach that focuses on improving the quality of life for patients and their families facing serious illnesses by providing relief from symptoms and stress. 3 In the ICU setting, palliative care can facilitate goal-aligned care; however, it remains underutilized for the OHCA population. 4 While existing knowledge suggests benefits in other critically ill patient groups, there is limited data on how palliative care consultation specifically affects decision-making and outcomes among patients admitted after an OHCA.5
To address this knowledge gap, we conducted a mixed retrospective-prospective cohort study to evaluate the impact of palliative care consultation on end-of-life decision-making and clinical outcomes in ICU patients following OHCA. We examined primary outcomes, such as in-hospital mortality and length of stay, and secondary outcomes, including the timing of code status changes and the withdrawal of life-sustaining treatments. We hypothesized that palliative care consultation in patients with out-of-hospital cardiac arrest would be associated with differences in end-of-life care patterns, reflecting a shift in the focus of care, without significant changes in length of stay or treatment intensity.
Methods
Study Design
This was a mixed retrospective and prospective observational study conducted at Memorial Hermann–Texas Medical Center, a tertiary academic hospital affiliated with the University of Texas Health Science Center at Houston (UTHealth). The study was carried out over a two-year period, beginning in October, 2023 and ending in March, 2025. The institutional review board approved the study, and a waiver of informed consent was granted, given the minimal risk, observational design, and the use of de-identified data.
Patients
Adult patients (aged ≥18 years) admitted to the intensive care unit (ICU) with a diagnosis of out-of-hospital cardiac arrest were eligible for inclusion. For the retrospective cohort, patients were identified through ICU and hospital admission databases. The prospective cohort enrolled patients in real-time during the ICU stay. Inclusion criteria required that patients had the return of spontaneous circulation (ROSC) and were admitted to the ICU for post-cardiac arrest care. Patients were excluded if they were admitted for in-hospital cardiac arrest, died in the emergency department before ICU admission, or lacked sufficient documentation for outcome assessment. Patients were then categorized into two groups based on whether they received a palliative care consultation at any point during hospitalization. All patients with complete clinical and outcome data were included in the final analysis.
Palliative Care Consultation
A multidisciplinary team of palliative care physicians, physician assistants, nurse practitioners, social workers, chaplains, and case managers provide palliative care consultation at Memorial Hermann- Texas Medical Center. Consultations are initiated at the discretion of the primary ICU team and are available seven days a week. The focus of the palliative care team includes clarification of goals of care, assistance with complex decision-making, management of symptoms (including pain and non-pain-related distress), support for surrogate decision-makers, and provision of spiritual and psychosocial support. For this study, a palliative care consultation was defined as any formal evaluation documented by the palliative care service during the ICU or hospital stay. The timing, frequency, modality (in-person, telephone, or teleconference), and type of interventions provided during each consultation were recorded for patients in the palliative care group.
Data collection
Data was collected using the hospital’s electronic medical record system (Epic Systems, Verona, WI), a combination of retrospective chart review and prospective data entry. For patients in the retrospective cohort, trained study team members abstracted relevant clinical and demographic information using a standardized data collection tool. For prospective cases, data were recorded in real-time during the patient’s ICU stay.
Collected variables included demographics (age, sex), past medical history (hypertension, diabetes, coronary artery disease, heart failure, chronic kidney disease, malignancy), and cardiac arrest-related information (cause of arrest and initial code status). Clinical course data included ICU length of stay, total hospital length of stay, use of vasopressors or inotropes, mechanical ventilation, continuous renal replacement therapy (CRRT), and mechanical circulatory support.
For patients who received palliative care consultation, additional information was collected regarding the number of encounters, provider type, mode of communication (in-person, telephone, teleconference), and nature of the interventions provided (eg, goals of care clarification, pain management, spiritual support). For all patients, the time from ICU admission to code status change and the time from withdrawal of life-sustaining treatment were recorded. The timing of palliative consultation relative to ICU admission was also documented.
Outcomes Measures
The primary measures included in-hospital mortality, ICU length of stay, and hospital length of stay.ICU and hospital length of stay were calculated for all patients regardless of discharge status, including those who died during hospitalization. Secondary outcomes included the time from ICU admission to code status change and to withdrawal of life-sustaining treatment in both groups, as well as the proportion of patients in each group who experienced a change in code status during hospitalization. Illness severity was assessed using the Sequential Organ Failure Assessment (SOFA) score, collected at ICU admission and at 72 hours, and compared between groupsFor patients who received a palliative care consultation, additional secondary measures included the timing of the consultation relative to ICU admission, the number and type of palliative care encounters, and the nature of palliative interventions provided. These interventions were categorized into domains such as goals-of-care clarification, pain and symptom management, psychosocial support, spiritual support, and assistance with surrogate decision-making. All outcome measures were compared between patients who received palliative care consultation and those who did not.
Statistical Method
Descriptive statistics were used to summarize patient baseline characteristics and clinical outcomes. Continuous variables were reported as means with standard deviations (SD) and medians with interquartile ranges (IQR). Categorical variables were summarized using frequencies and percentages. As the continuous variables in this study were not normally distributed, they were analyzed using the Wilcoxon rank-sum test. Categorical variables were compared using chi-square tests or Fisher’s exact tests, as appropriately based on cell counts. A two-sided P-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using SAS 9.4 software (SAS Institute Inc., Cary, NC, USA).
Results
Demographic and Clinical Characteristics
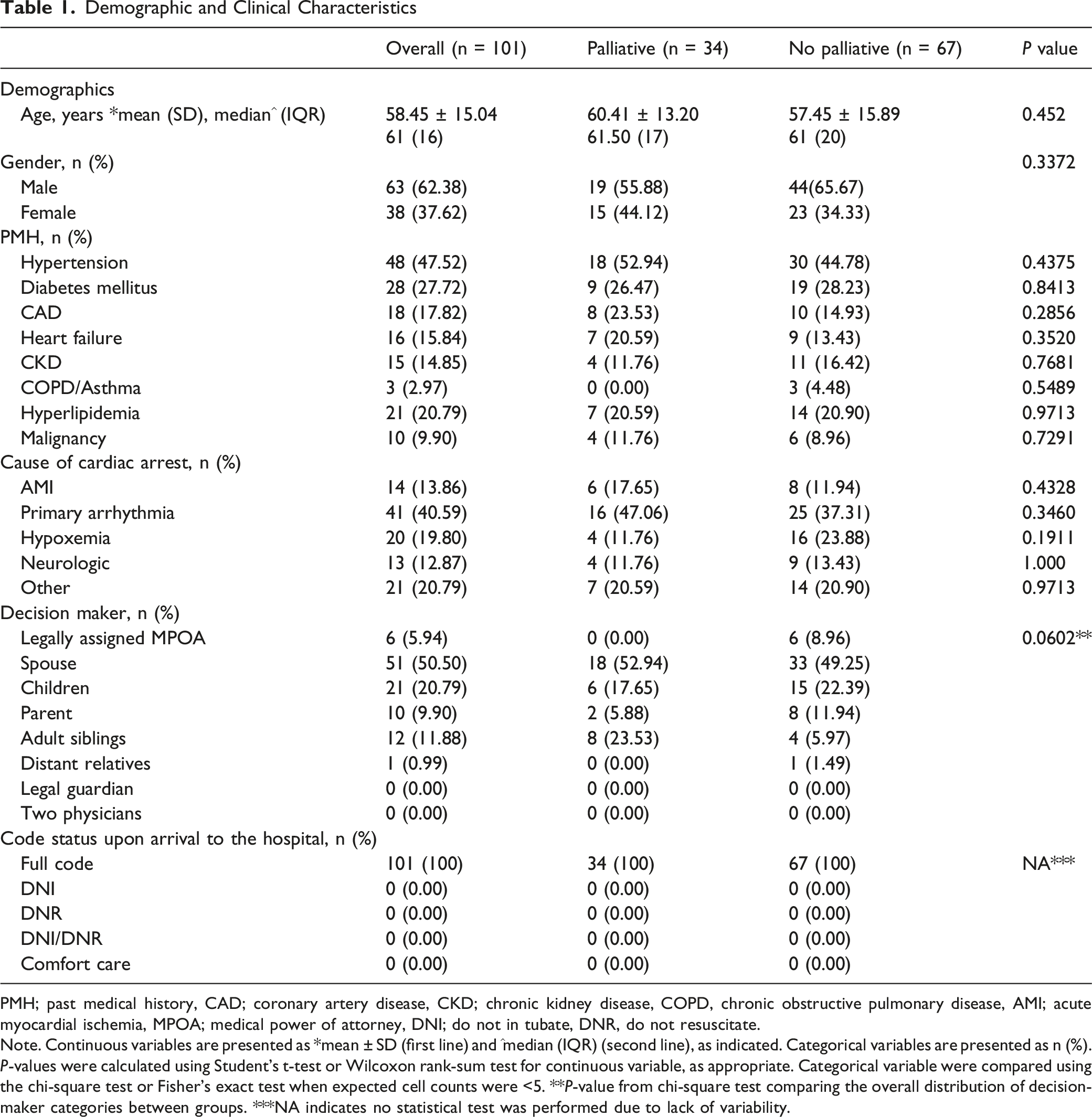
PMH; past medical history, CAD; coronary artery disease, CKD; chronic kidney disease, COPD, chronic obstructive pulmonary disease, AMI; acute myocardial ischemia, MPOA; medical power of attorney, DNI; do not in tubate, DNR, do not resuscitate.
Note. Continuous variables are presented as *mean ± SD (first line) and ^median (IQR) (second line), as indicated. Categorical variables are presented as n (%). P-values were calculated using Student’s t-test or Wilcoxon rank-sum test for continuous variable, as appropriate. Categorical variable were compared using the chi-square test or Fisher’s exact test when expected cell counts were <5. **P-value from chi-square test comparing the overall distribution of decision-maker categories between groups. ***NA indicates no statistical test was performed due to lack of variability.
ICU Course, Mortality, and Life-Sustaining Treatment
The median ICU length of stay was longer in patients seen by palliative care (6.0 days, IQR 5.5) compared to those not seen (4.0 days, IQR 5.0), though this difference was not statistically significant (P = 0.0999). Median hospital length of stay was 6.0 days (IQR 5.5) in the palliative group and 5.0 days (IQR 7.0) in the non-palliative group (P = 0.28). In-hospital mortality was significantly higher in the palliative care group (79.4%) compared to the non-palliative group (41.8%) (P = 0.0003). SOFA scores at ICU admission and at 72 hours were similar between patients seen by palliative care and those not seen by palliative care [8.0 (IQR 7.0-11.0) vs 9.0 (IQR 5.0-11.0), P = 0.72; and 9.0 (IQR 6.0-11.8) vs 7.5 (IQR 3.0-11.0), P = 0.27, respectively].
Comparison of Critical Care Measures and Life-Sustaining Treatments Between Patients With and W/Out Palliative Care Consultation

Code Status Changes and Timing by Group

Characteristics of Palliative Care Encounters
Characteristics of the Group Evaluated by Palliative
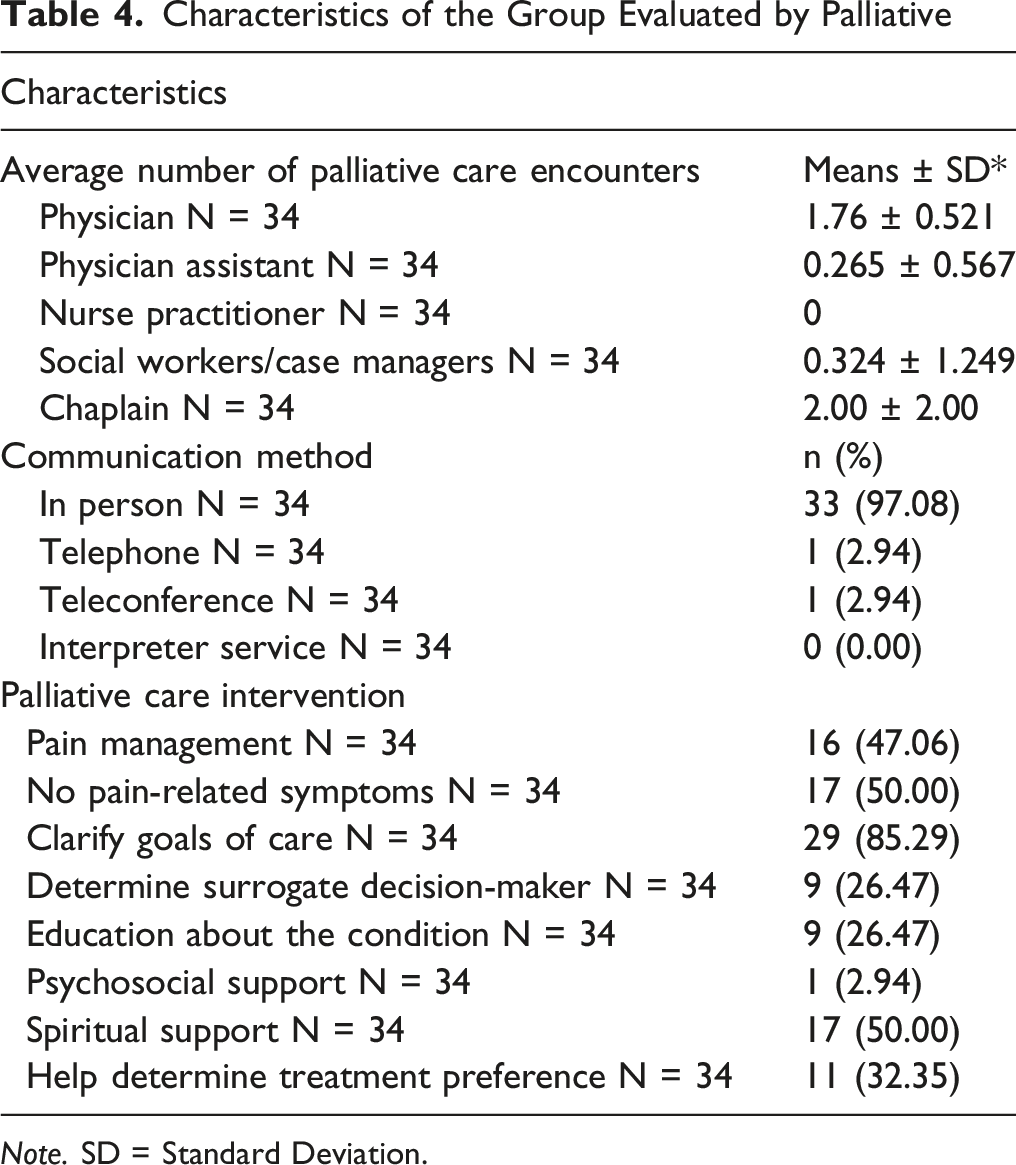
Note. SD = Standard Deviation.
Discussion
This mixed retrospective-prospective cohort study evaluated the impact of palliative care consultation on end-of-life decision-making and clinical outcomes among 101 patients admitted to the ICU after out-of-hospital cardiac arrest (OHCA) at a large tertiary academic center. Several important findings emerged.
First, patients who received a palliative care consultation (33.7% of the cohort) experienced substantially higher in-hospital mortality (79.4% vs 41.8%) despite having similar baseline demographic characteristics, comorbidities, and use of life-sustaining therapies. This association likely reflects differences in clinical context, prognostic uncertainty, and evolving goals of care at the time of consultation. Second, all patients who received a palliative care consultation (100%) had a change in code status during hospitalization, compared to only 32.8% of those who did not (P < 0.0001), suggesting that palliative care consultation was strongly associated with goals-of-care discussions that led to a redirection of care. Furthermore, the time from ICU admission to withdrawal of life-sustaining treatment was significantly longer in the palliative care group (6.0 vs 3.0 days, P = 0.016), while the time to code status change was similar between groups (P = 0.415). Third, the utilization of life-sustaining therapies (including vasopressors, mechanical ventilation, and continuous renal replacement therapy) was similar between groups, indicating that palliative care engagement did not lead to early withdrawal of aggressive interventions. Palliative care teams primarily focused on clarifying goals of care (85.3%), symptom management, and spiritual support. Finally, palliative care consultation occurred in approximately one-third of patients in this cohort, highlighting variability in referral patterns within this high-risk population. Palliative care involvement was not associated with differences in ICU or hospital length of stay.
The high in-hospital mortality among patients receiving palliative care consultation in our cohort (79.4% vs 41.8%) aligns with prior critical care observational studies, including those by Curtis et al 6 and the SUPPORT trial. 7 This association has been described in prior observational studies and, in some contexts, has been attributed to confounding by indication, whereby palliative care consultation is initiated in the setting of perceived poor prognosis, particularly after catastrophic events like OHCA, as discussed by Lilly et al 8 and Elmer et al 9 Notably, SOFA scores at ICU admission and at 72 hours were similar between patients seen by palliative care and those not seen by palliative care (P = 0.72 and P = 0.27, respectively), suggesting that the decision to consult palliative care was likely driven by clinical factors beyond objective severity scores, such as perceived neurological prognosis, illness trajectory, or the treating team’s overall assessment of prognosis. In the OHCA population specifically, neurological prognosis following anoxic brain injury is a critical determinant of outcomes that is not captured by the SOFA score, and may have influenced the decision to consult palliative care independent of measured illness severity. The higher mortality in the palliative care group should therefore be interpreted as a reflection of the clinical context in which consultation was requested, rather than as evidence that palliative care adversely influenced outcomes.
Although baseline demographic characteristics and treatment intensity were similar between groups, palliative care consultation may have been influenced by the broader clinical context and evolving goals of care rather than measurable differences in baseline illness severity. Prior work has demonstrated that proactive palliative care consultation can shorten the time to establish comfort-focused goals, particularly when consultation occurs early and systematically. Structured communication models (Campbell & Guzman 10 ) and family engagement interventions (Azoulay et al 11 ) further highlight the role of palliative care teams in supporting timely, value-concordant decision-making. However, in our cohort, the timing of end-of-life decision-making remained variable and did not demonstrate a consistent temporal pattern following palliative care consultation. Our findings are consistent with prior systematic reviews describing the role of proactive palliative care consultation in supporting goals-of-care discussions in critically ill patients. 12 Comparable use of life-sustaining therapies between groups challenges the misconception that palliative care automatically leads to treatment withdrawal. However, the significantly longer time from ICU admission to withdrawal of life-sustaining treatment in the palliative care group (6.0 vs 3.0 days, P = 0.016) suggests that palliative care facilitated a more deliberate and structured process of goals-of-care decision-making rather than an abrupt withdrawal of care. Of note, interventions such as mechanical ventilation and vasopressors are typically initiated following ROSC before palliative care is consulted, and the absence of duration data for these treatments is a limitation that precludes definitive conclusions about their trajectory in each group. Aslakson et al 13 emphasize that palliative care in the ICU supports patient- and family-centered, goal-directed decision-making, which may include the continuation of intensive interventions. This echoes findings from ethics consultations (Schneiderman et al 14 ), demonstrating that palliative care promotes goal-directed care rather than premature therapy limitation. Our finding of no significant difference in length of stay is consistent with some literature (Norton et al 15 ) but not all (Kyeremanteng et al, 16 Morrison et al 17 ), likely due to variations in study design, patient populations, and “early” consultation definitions (Turnbull et al 18 ). The absence of differences in several outcomes may also reflect limited statistical power to detect modest effects in this relatively small cohort.
Underutilization of palliative care consultation in our OHCA cohort (33.7%) reflects a persistent gap (Nelson et al, 19 Wunsch et al 20 ). Barriers include prognostic uncertainty, lack of clear triggers, 21 time constraints, limited primary palliative skills, and misconceptions. 22 Nevertheless, the core functions provided by palliative are teams in our study (goals-of-care clarification, symptom management, and spiritual support) align with established quality indicators 23 and professional guidelines. 24
The higher mortality observed among patients receiving palliative care consultation should be interpreted within the context of evolving goals of care following OHCA. In this setting, palliative care consultation may be best understood as part of a broader decision-making framework that emphasizes communication, clarification of goals of care, and support for patients and families. Although the timing of end-of-life decision-making varied in our cohort, prior studies highlight the role of palliative care in supporting structured communication and aligning care with patient goals. 10 Larger studies may be needed to further clarify whether the timing of consultation influences decision-making patterns in this population.
Palliative care consultation was not associated with differences in life-sustaining therapies or ICU and hospital length of stay. These findings suggest that consultation was integrated alongside ongoing critical care rather than serving solely as a marker of treatment withdrawal. Further study is needed to better characterize referral patterns and to define the optimal integration of palliative care principles in this high-risk population.
Future research should address several key areas. Standardized screening tools or trigger criteria for palliative care consultation may help mitigate selection bias and ensure timely involvement. Incorporating patient- and family-reported outcome measures will be important to better characterize the impact of palliative care interventions. Further work is warranted to define the optimal timing and model of palliative care delivery after OHCA.
Conclusion
In this study of ICU patients following out-of-hospital cardiac arrest, palliative care consultation was associated with higher in-hospital mortality, while baseline characteristics, illness severity treatment intensity, and length of stay were similar between groups. Palliative care consultation was strongly associated with goals-of-care redirection and a more deliberate end-of-life decision-making process. Palliative care services primarily focused on goals-of-care clarification and supportive interventions and were utilized in only a minority of this high-risk population. These findings provide insight into current referral patterns and reinforce the importance of integrating palliative care as a complementary tool to support patient and family-centered decision-making after OHCA, rather than interpreting its consultation as a marker of poor prognosis.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.