
Abstract
Introduction
Effective communication is key to quality end-of-life care. This study assessed sex, racial/ethnic, and temporal differences in perceived experience and communication among elderly U.S. Medicare patients with cancer in the last year of life.
Methods
The Surveillance, Epidemiology, and End Results (SEER)-Consumer Assessment of Healthcare Providers and Systems (CAHPS) data resource from 2000-2019 was used. Multivariable, survey-weighted linear regression models assessed sex, racial/ethnic, and temporal differences in patient experience and communication at the end of life.
Results
A total of 10,108 patients were included. Women had higher “rate care” scores compared with men. No significant differences in ratings were found between non-Hispanic Black and non-Hispanic White patients nor between Hispanic and non-Hispanic White patients
Conclusion
Overall, there were small differences in end-of-life patient experience and communication by sex or race/ethnicity among older adults with cancer. Improvements in reported communication over time may reflect changes in care delivery and information access, while lower ratings for “getting needed care” suggest persistent challenges in care access during the last year of life, highlighting opportunities to improve patient-centered end-of-life care.
Introduction
Effective communication is key to optimal cancer management and patient-centered outcomes during the last year of life. Patient-centered communication ensures that individuals’ care choices align with their end-of-life priorities and preferences. 1 Known sex and racial/ethnic differences exist across the cancer care continuum, including in end-of-life care. 2 Women tend to have lower health care utilization and higher hospice enrollment than men, 3 patterns influenced by lived experiences, older age at death, and other factors.4,5 Non-Hispanic Black and Hispanic patients have higher health care utilization, and lower hospice use compared with non-Hispanic White patients. 3
There are also differences in each unique patient’s interactions and communication with the health care system, affected by individual factors such as culture, language, and religion. 6 Prior studies examining sex differences in patient experience and communication have shown that women report higher satisfaction or communication ratings than men in some domains, 7 but greater difficulty in getting referrals, equipment or assistance. 8 Similarly, studies have found that non-Hispanic Black patients report experience and communication ratings similar to those of non-Hispanic White patients, while Hispanic patients often rate communication more favorably but report greater difficulty in “getting needed care.”7,9 These inconsistencies suggest that patient-reported experience may not directly mirror observed disparities in utilization or outcomes.
In general, women and racial minorities are more likely to experience lower socioeconomic status and higher levels of disability and comorbidity, 10 requiring more complex medical management and communication. Communication is especially relevant and important at the end of life and in cancer management, when medical complexity, caregiving, pain, and other symptoms can peak. In a scoping review, marginalized populations, including race and ethnic minorities and females, were noted to have differences in provider-patient communication practices and quality. 9
Most of the prior literature examines data through 2011. In the past decade, however, the healthcare experience as well as cancer treatment and survivorship have changed dramatically; health care systems begun adopting digital technologies and telemedicine, potentially changing the delivery of care experience 11 ; value-based systems and metrics promoted by the Center for Medicare and Medicaid Services have incentivized hospitals to provide better care at a reduced cost. 12 Finally, cancer care progressed in the last decade with the approval of new immunotherapy treatments for several cancers, targeted therapies becoming the standard of care, and advances in the delivery of radiotherapy.13,14 It is possible that the experiences of patients shift through time and therefore it is important to continue to evaluate sex differences in measures that may differentially affect males and females, including physician communication.
The purpose of this study is to assess sex, racial/ethnic, and temporal differences in patient experience and communication among elderly U.S. Medicare beneficiaries with cancer in the last year of life using the SEER-CAHPS national dataset from 2000-2019.
Materials & Methods
Data Source
We used data from the SEER-CAHPS data resource, a resource for quality of cancer care research based on a linkage between the National Cancer Institute’s (NCI) Surveillance, Epidemiology and End Results (SEER) cancer registry data and the Centers for Medicare & Medicaid Services’ (CMS) Medicare Consumer Assessment of Healthcare Providers and Systems (CAHPS®) patient surveys.15,16
Study Cohort
Inclusion criteria included: (a) completion of the CAHPS survey between 2000 and 2019, (b) age ≥66 years at the time of survey completion, (c) survey completion within the last year of life (LYOL), and (d) diagnosis of breast, prostate, lung, colorectal, uterine, skin, kidney, bladder, pancreatic, and/or ovarian cancer prior to survey administration. Cancer sites were limited to the ten most common cancer types to ensure stable estimates and comply with SEER-CAHPS guidelines. The age restriction (≥66 years) ensured Medicare eligibility during the entire LYOL and at the time of CAHPS survey completion. Patients who were not Hispanic, non-Hispanic White (NHW) or non-Hispanic Black (NHB) were excluded due to small sample size (Appendix Table 1).
Variables
Patient characteristic collected included age at the time of survey completion, sex, race/ethnicity, Medicare/Medicaid dual eligibility, plan type, proxy use, survey language, marital status, cancer type and time from diagnosis to survey completion and general and mental health self-reported scores. We also included the period of survey completion (2000-2011 or 2012-2019) to account for healthcare changes over time.
Outcomes
Primary outcome variables included CAHPS patient experience and communication ratings and composite measures. Patient experience measures included the individual items “rate MD” and “rate care,” where patients are asked to rate their doctor and healthcare using any number from 0 (worst) to 10 (best) during the past 6 months, respectively. For each composite measure, patients were asked a series of questions regarding their experiences in the last 6 months, and a composite score was created. For “getting care quickly,” participants were asked about whether they received necessary care without delay, were able to schedule appointments in a timely manner, and saw a provider within 15 minutes of their scheduled appointment time. For “getting needed prescription drugs,” patients were asked about ease of getting prescriptions and filling prescriptions at the pharmacy and by mail. For “getting needed care,” patients were asked about ease of getting specialist appointments, tests and treatments, a personal doctor or nurse and delays in healthcare due to waiting for Medicare approval. 15
Communication measures included the “doctor communication” composite. Patients were asked how often doctors clearly explain things, listen carefully, show respect and spent enough time with the patient. 15
For outcome measures, linear mean scoring was used to transform patient responses to survey items to a 0-100 scale, where 0 and 100 represent the lowest and highest possible mean score, respectively. 16
Statistical Analysis
Descriptive patient characteristics and outcomes are reported by sex and race/ethnicity as weighted mean (standard error [SE]) or weighted percentage (95% confidence intervals [CIs]), as appropriate. Chi-square tests or analysis of variance (ANOVA) were used to assess statistically significant differences between groups.
We used multivariable, survey-weighted linear regression models to evaluate sex and racial/ethnic differences in patient ratings and to assess whether ratings differed between 2000-2011 and 2012-2019, adjusting for age, race/ethnicity, sex, education, general and mental health, proxy use, dual eligibility, marital status, language, cancer type, survey period, and time from cancer diagnosis to survey completion. We also used multivariable, survey-weighted linear regression models to evaluate sex and racial/ethnic interactions in patient ratings. All analyses accounted for survey weights and were conducted using survey procedures from SAS version 9.4 (SAS Institute Inc).
Results
Patient Characteristics
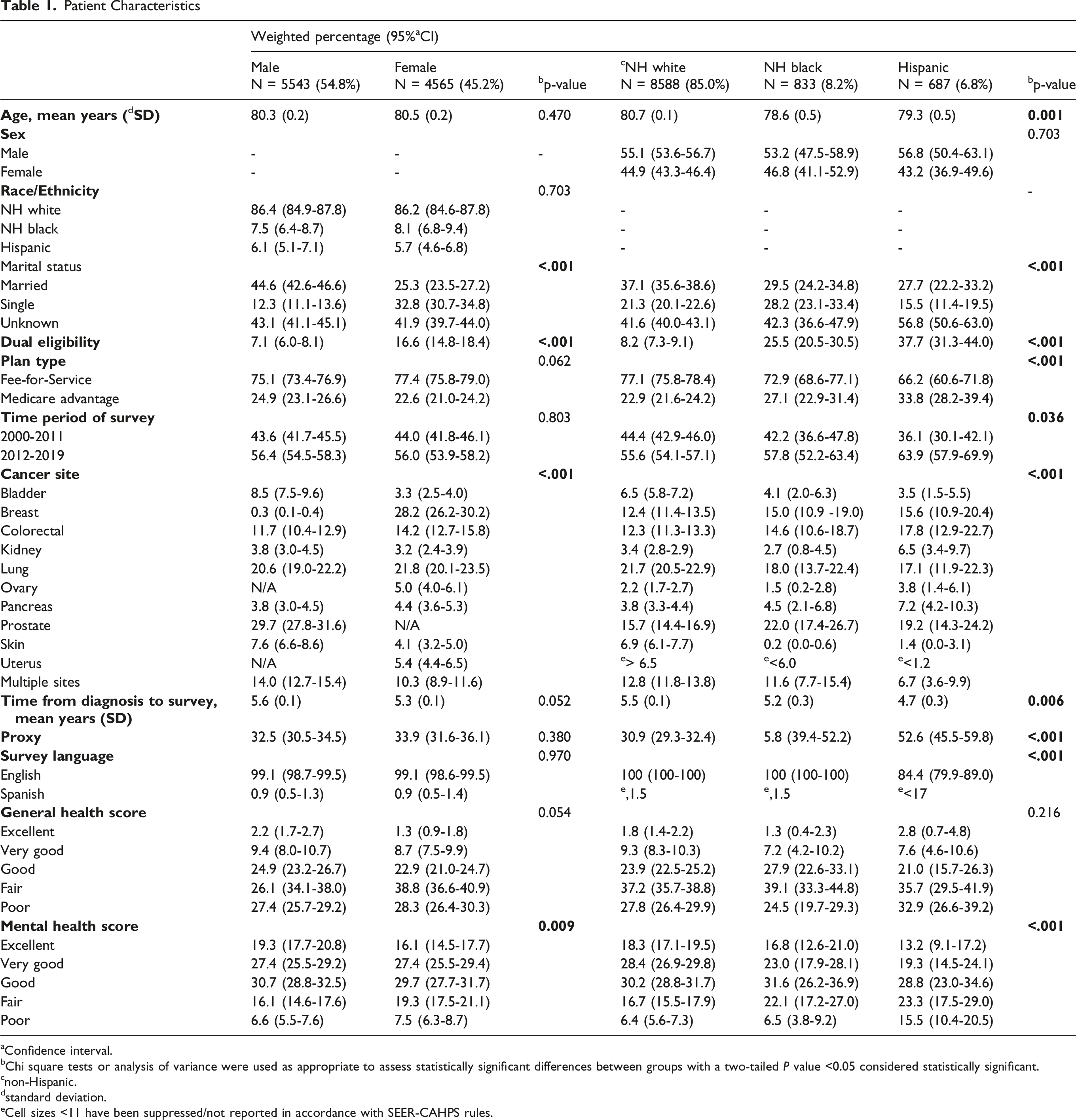
aConfidence interval.
bChi square tests or analysis of variance were used as appropriate to assess statistically significant differences between groups with a two-tailed P value <0.05 considered statistically significant.
cnon-Hispanic.
dstandard deviation.
eCell sizes <11 have been suppressed/not reported in accordance with SEER-CAHPS rules.
In Appendix Table 2, weighted mean (SE) ratings are reported. In unadjusted analyses, women reported significantly higher ratings for “rate care” compared with men (mean: 86.0 [SE 0.4] vs 84.7 [SE 0.4], P = .019). Non-Hispanic Black patients reported significantly lower ratings for “rate care” compared with non-Hispanic White patients (mean: 82.6 [SE 1.3] vs 85.6 [SE 0.3], P = .027). Hispanic patients reported significantly lower ratings for “getting needed care” (mean: 82.0 [SE 1.7] vs 87.2 [SE 0.3], P = .001) and “getting needed drug” (mean: 86.2 [SE 1.7] vs 91.3 [SE 0.4], P = .001) compared with non-Hispanic White patients.
Multivariable, Survey-Weighted Linear Regression Models
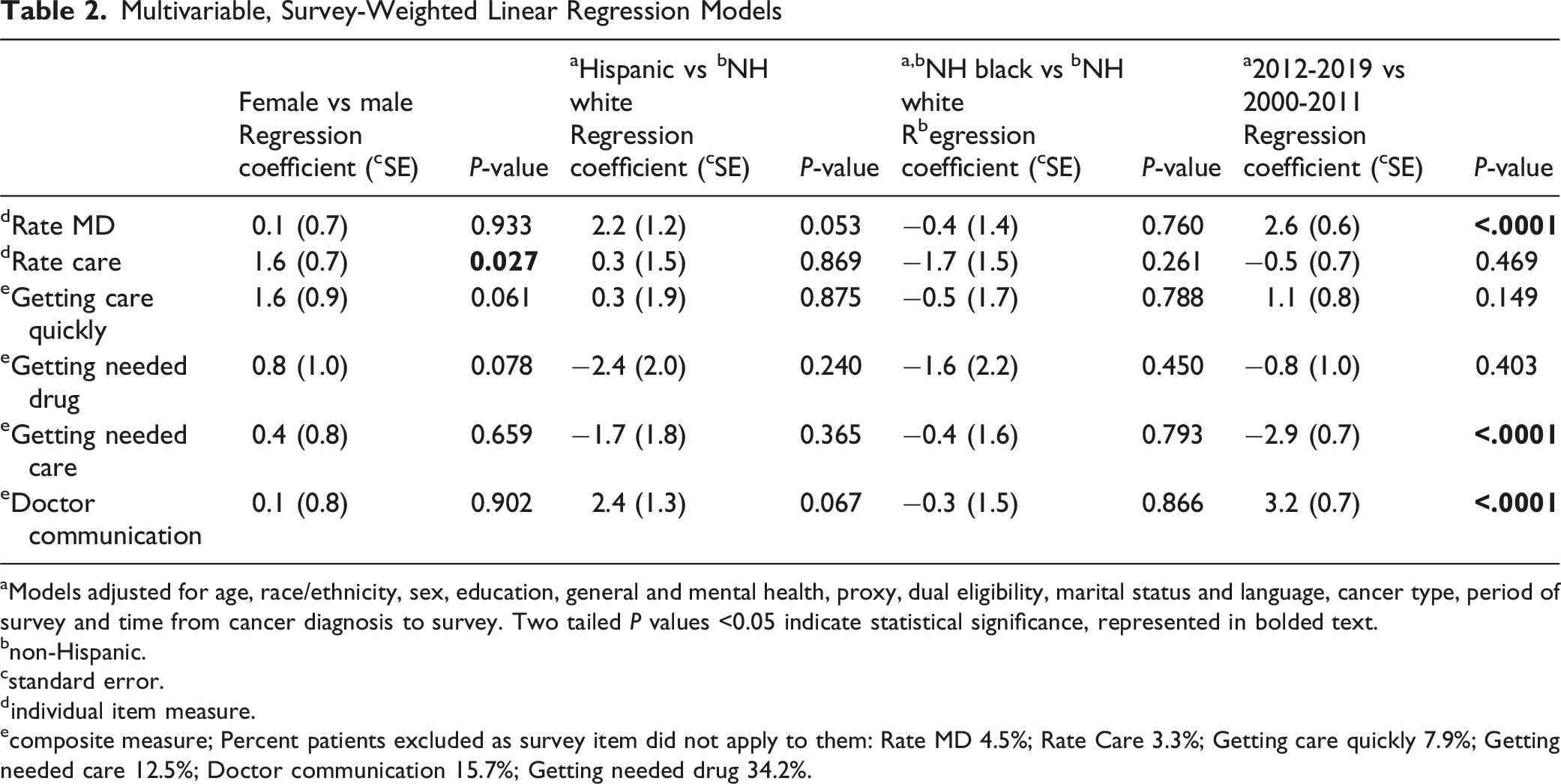
aModels adjusted for age, race/ethnicity, sex, education, general and mental health, proxy, dual eligibility, marital status and language, cancer type, period of survey and time from cancer diagnosis to survey. Two tailed P values <0.05 indicate statistical significance, represented in bolded text.
bnon-Hispanic.
cstandard error.
dindividual item measure.
ecomposite measure; Percent patients excluded as survey item did not apply to them: Rate MD 4.5%; Rate Care 3.3%; Getting care quickly 7.9%; Getting needed care 12.5%; Doctor communication 15.7%; Getting needed drug 34.2%.
Discussion
Women reported significantly higher ratings for “rate care” compared with men. No significant differences in ratings were observed between non-Hispanic Black and non-Hispanic White patients nor between Hispanic and non-Hispanic White patients, despite known differences in cancer survival and other outcomes for minoritized patients. Patient ratings for “rate MD” and “doctor communication” were significantly higher for surveys completed during 2012-2019 compared with 2000-2011. These findings may reflect shifting trends in technology use, such as increased patient access to medical records and the ability to message providers. Increasing advance care planning may also play a role. However, ratings for “getting needed care” were significantly lower, possibly due to improved survival with greater care needs at the end of life.
Women reporting better “rate care” scores compared with men aligns with prior literature, 7 including qualitative research showing that women generally have a stronger belief that health care systems empower and benefit patients, whereas men may feel disempowered and fear harm from the health care system. 17 Women also have lower health care utilization and more advance care planning at the end of life. 3 It is possible that women have higher expectations for detailed communication and greater ability to request information, 18 which may lead to better communication at the end of life and subsequently higher “rate care” scores. However, these findings do not necessarily correlate with proxy perception of excellent quality of care prior to death provided to female decedents compared with male decedents. 19
Non-Hispanic Black, Hispanic and non-Hispanic White patients had similar survey responses, despite known disparities in cancer screening and throughout the cancer care continuum, 20 including lower quality of end-of-life care such as increased pain, lower rates of palliative care consultations, and reduced hospice use among minoritized patients. 21 There were no significant findings for sex and racial/ethnic interaction terms despite known differences in experience for individuals with intersecting identities such as non-Hispanic Black women. 22
Ratings for the individual item “rate MD” and the composite measure “doctor communication” for surveys completed between 2012-2019 were significantly higher compared to ratings from 2000-2011. It is possible that increased access to medical information, 23 the expansion of telemedicine, and communication through more diverse means, including secure messaging, 24 contributed to this finding. In addition, advance care planning has evolved from a focus on code status and advance directives to an emphasis on aligning medical management with patient preferences and priorities.2,25 However, ratings for “getting needed care” were significantly lower, possibly due to improved survival with greater care needs at the end of life.
Our study adds to prior SEER-CAHPS studies by examining both patient-reported care experiences and access to end-of-life (EOL) care over nearly two decades (2000-2019). Although patient ratings of provider communication and overall care improved over time, access to needed care and services declined from the 2000-2011 period to the 2012-2019 period. These findings have important implications for hospice and palliative care practice. Delays in accessing appointments, tests, treatments, and medications are particularly concerning among patients with advanced cancer during the last year of life, when symptom burden and supportive care needs are often substantial. Timely access to supportive oncology, palliative care, medications, and care coordination services is critical for management of physical and psychological symptoms and may influence quality of life near the end of life. Potential approaches to improve timely access to EOL care include greater integration of patient navigation programs, earlier involvement of palliative care services, expanded telehealth-based supportive care models, and communication training initiatives for oncology and palliative care clinicians. 26
Limitations of this study include restricted generalizability due to the SEER-CAHPS linkage, which includes only Medicare beneficiaries; therefore, the analytic cohort was limited to individuals aged ≥ 66 years, which may not reflect the experiences of younger patients with cancer who differ in insurance coverage, care settings, and end-of-life care trajectories. Additionally, the sample included relatively limited representation of minoritized patients, with the exclusion of those who were not Hispanic or non-Hispanic Black due to low sample size. Additionally, not all questions applied to all patients. For example, there were no responses for 12.5% of “getting needed care,” 15.7% “doctor communication,” and 34.2% of “getting needed drug” for this reason. A greater proportion of Hispanic patients had a proxy complete the survey, and it is unclear whether patients would have responded similarly had they been able to complete the survey themselves. In addition, prior literature shows that different groups have different response styles which may not be representative of actual experience.27,28 Hispanics, for example, have a tendency towards extreme responding. 27
Conclusion
In conclusion, females had higher “rate care” scores compared with males. There were no differences in responses between non-Hispanic Black and non-Hispanic White patients nor between Hispanic and non-Hispanic White patients, despite known differences in cancer screening and across the cancer care continuum.20,21 Surveys completed during 2012-2019 had higher “rate MD” and “doctor communication” ratings but lower ratings for “getting needed care” compared with those completed between 2000-2011. These findings suggest that while aspects of patient-doctor communication may be improving, challenges in care access and coordination still persist at the end of life. Efforts to strengthen hospice and palliative care and improve timely access to services remain important priorities for end-of-life care.
Footnotes
Acknowledgments
This study used the linked SEER-CAHPS data resource. The interpretation and reporting of these data are the sole responsibility of the authors. The authors acknowledge the efforts of the National Cancer Institute; the Centers for Medicare & Medicaid Services; Information Management Services (IMS), Inc; and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER-CAHPS data resource. The collection of cancer incidence data used in this study was supported by the California Department of Public Health pursuant to California Health and Safety Code Section 103885; Centers for Disease Control and Prevention’s (CDC) National Program of Cancer Registries, under cooperative agreement 1NU58DP007156; the National Cancer Institute’s Surveillance, Epidemiology and End Results Program under contract HHSN261201800032I awarded to the University of California, San Francisco, contract HHSN261201800015I awarded to the University of Southern California, and contract HHSN261201800009I awarded to the Public Health Institute. The ideas and opinions expressed herein are those of the author(s) and do not necessarily reflect the opinions of the State of California, Department of Public Health, the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractor.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data Management and Analysis Core for Comparative Effectiveness Research on Cancer in Texas (RP 210130).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Précis
Data from the Surveillance, Epidemiology, and End Results (SEER) cancer registry linked with Consumer Assessment of Healthcare Providers and Systems (CAHPS) patient survey were used to assess sex, racial/ethnic, and temporal differences in patient experience and communication at the end of life. Females had higher “rate care” scores compared with males, and surveys completed during 2012-2019 had higher communication ratings but lower ratings for “getting needed care” compared with those completed between 2000-2011.
Appendix
Cohort selection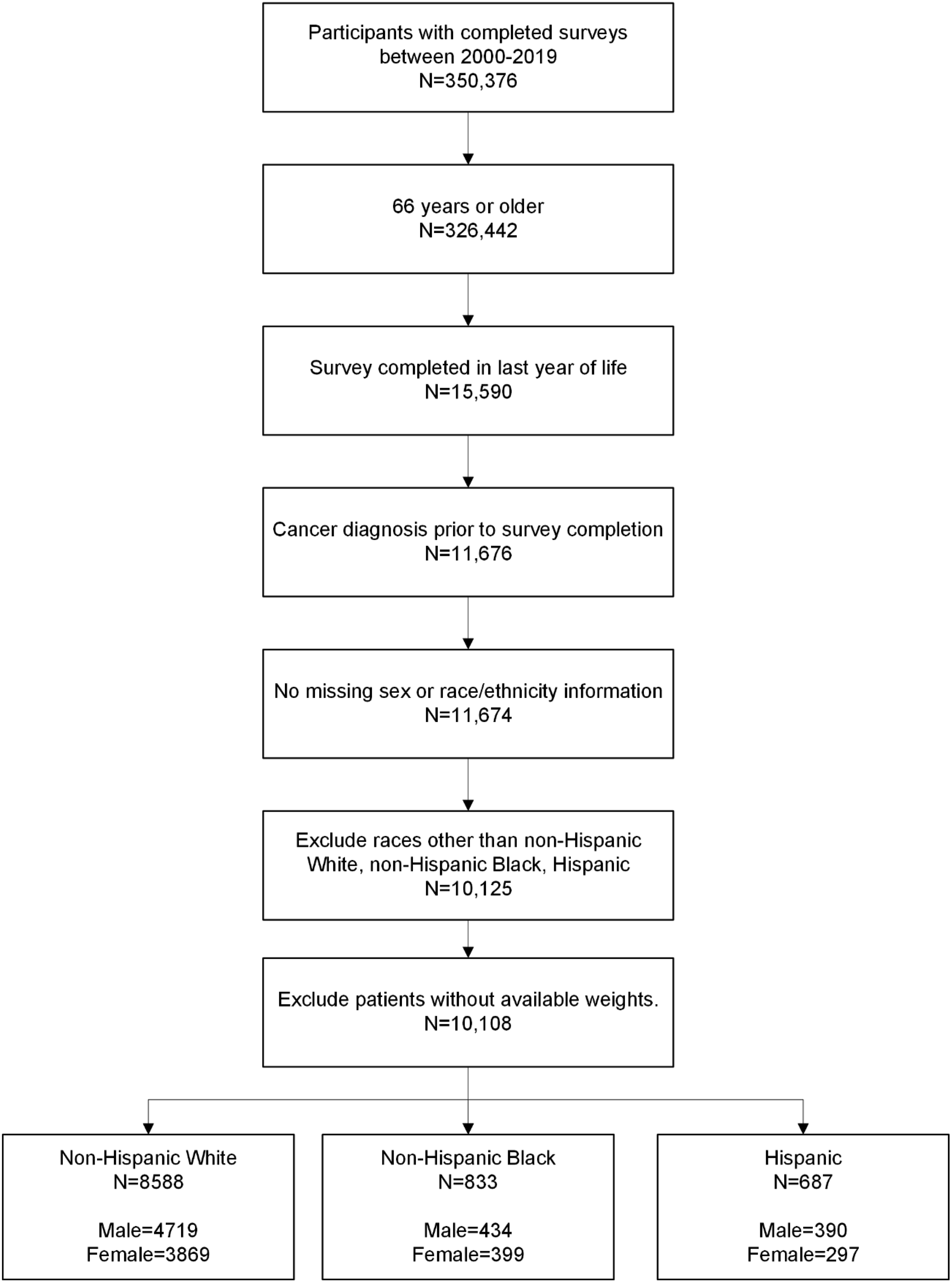
Breakdown of Race Prior to Excluding Races With Low Frequency/Unknown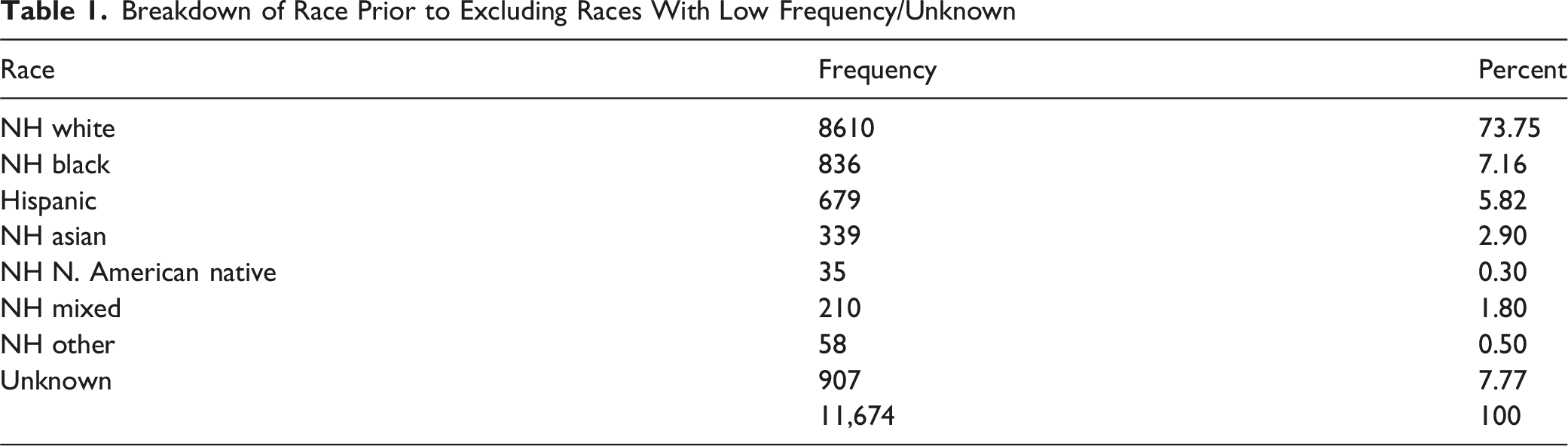
Race
Frequency
Percent
NH white
8610
73.75
NH black
836
7.16
Hispanic
679
5.82
NH asian
339
2.90
NH N. American native
35
0.30
NH mixed
210
1.80
NH other
58
0.50
Unknown
907
7.77
11,674
100
Weighted Mean (SE) Ratings for Single Items and Composite Measures aANOVA was used to assess statistically significant differences between groups with a two-tailed P value <0.05 considered statistically significant. Bold text signifies statistical significance; Percent patients excluded as survey item did not apply to them: Rate MD 4.5%; Rate Care 3.3%; Getting care quickly 7.9%; Getting needed care 12.5%; Doctor communication 15.7%; Getting needed drug 34.2%.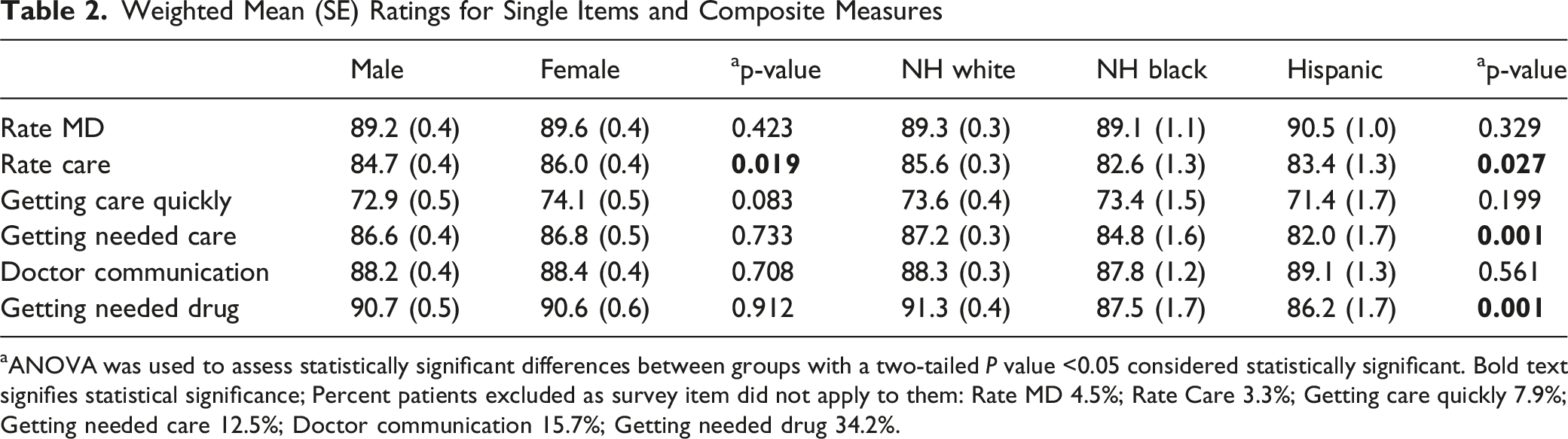
Male
Female
a
p-value
NH white
NH black
Hispanic
a
p-value
Rate MD
89.2 (0.4)
89.6 (0.4)
0.423
89.3 (0.3)
89.1 (1.1)
90.5 (1.0)
0.329
Rate care
84.7 (0.4)
86.0 (0.4)
85.6 (0.3)
82.6 (1.3)
83.4 (1.3)
Getting care quickly
72.9 (0.5)
74.1 (0.5)
0.083
73.6 (0.4)
73.4 (1.5)
71.4 (1.7)
0.199
Getting needed care
86.6 (0.4)
86.8 (0.5)
0.733
87.2 (0.3)
84.8 (1.6)
82.0 (1.7)
Doctor communication
88.2 (0.4)
88.4 (0.4)
0.708
88.3 (0.3)
87.8 (1.2)
89.1 (1.3)
0.561
Getting needed drug
90.7 (0.5)
90.6 (0.6)
0.912
91.3 (0.4)
87.5 (1.7)
86.2 (1.7)