
Abstract
Background:
Differentiated thyroid cancer (DTC) is the most prevalent cancer of thyroid and is among the most frequently diagnosed cancers in the United States. The practice guidelines of the American Thyroid Association (ATA) for DTC management in adult patients (previously combined with thyroid nodules) were published initially in 1996, with subsequent revisions based on advances in the field. The goal of this update is to provide clinicians, patients, researchers, and those involved in health policy with rigorous, comprehensive, and contemporary guidelines to assist in the management of adult patients with DTC, emphasizing the patient journey beginning with a thyroid cancer diagnosis.
Methods:
The questions addressed were based, in part, on prior versions of the guidelines, with input from a larger, more diverse complement of stakeholders. The panel included members from multiple specialties involved in thyroid cancer care, including a patient advocate and an expert in systematic reviews/meta-analyses/guidelines who educated and supported task force members. The panel conducted systematic literature reviews to inform the recommendations and commissioned two additional systematic reviews. Published English-language articles were eligible for inclusion, with a final search date of July 1, 2024. A modified Grading of Recommendations Assessment, Development and Evaluation system was used for critical appraisal of evidence and determining the quality of data. The guidelines panel had editorial independence from the ATA. Competing interests of task force members were pre-vetted, regularly updated, communicated with task force members, and assessed and managed by ATA leadership and the Clinical Practice Guidelines and Statements Committee.
Results:
These revised guidelines begin with the initial cancer diagnosis and continue with recommendations for staging and risk assessment, initial treatment decisions, assessment of treatment responses, monitoring approaches, diagnostic testing, and subsequent therapies based on the strength of evidence for response and consideration of side effects and outcomes. Patient-reported outcomes and identified areas of need for additional high-quality research are highlighted.
Conclusions:
These revised evidence-based recommendations inform clinical decision-making in the management of DTC that reflect the changing science and optimize the evidence-based clinical care of patients throughout their journey with DTC. Critical areas of need for additional research are highlighted.
Keywords
Table of Contents 2025 ATA Guidelines for DTC
F, Figure; R, recommendation; T, Table.
Introduction
Differentiated thyroid cancer (DTC) includes papillary, follicular, and oncocytic carcinomas, comprising the vast majority (>90%) of all thyroid cancers.
1
In the United States, it is estimated that there were 44,020 new cases of thyroid cancer in 2024,2,3 compared with 37,200 in 2015 when the last American Thyroid Association (ATA) guidelines were published. The yearly incidence tripled from 4.9 per 100,000 in 1975 to 14.3 per 100,000 in 2015.
4
Approximately 25% of the new thyroid cancers diagnosed in 1988–1989 were <1 cm, compared with 39% of the new thyroid cancer diagnoses in 2008–2009.
4
This shift to earlier detection/diagnosis correlates with the increasing use of neck ultrasonography and other imaging along with the advent of ultrasound-guided fine needle aspiration (FNA).
5
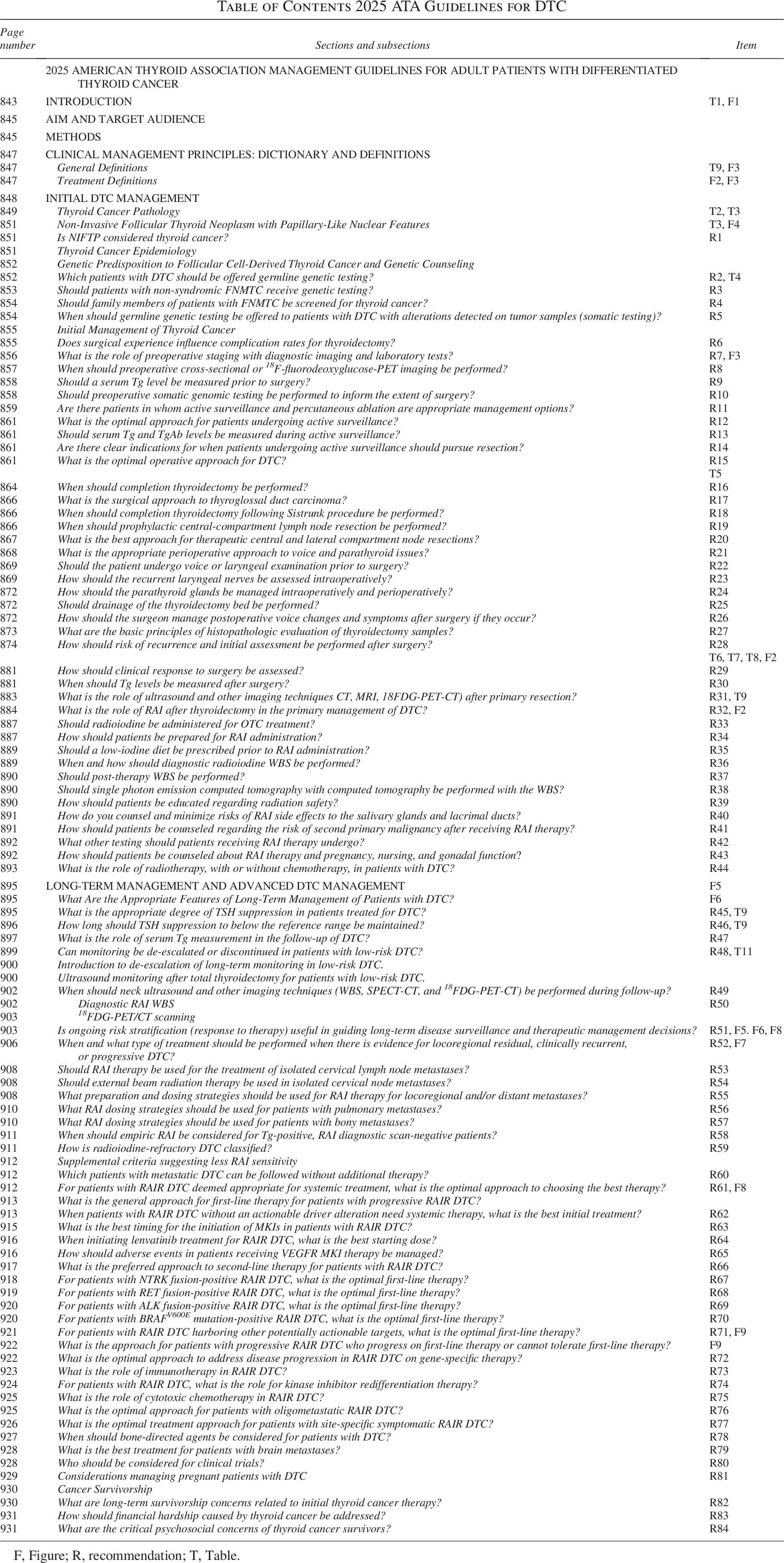
The incidence of thyroid cancer, and particularly small thyroid cancers, has reduced in the United States since 2014.2,6 This change in incidence trajectory is likely a reflection of the adoption of guidelines’ recommendations from the ATA and other organizations discouraging FNA of small nodules <1 cm in the absence of abnormal lymph nodes or local invasion, due to the overall outstanding prognosis associated with these tumors and weighed against the potential risks of unnecessary treatment. In addition to changes in the management of early-stage thyroid cancer, prior guidelines introduced criteria to enhance initial decision-making and a response framework following interventions to facilitate further management decisions. These have been validated since the prior guidelines, enabling adoption in clinical practice. There have been major advances in understanding the molecular causes of thyroid cancer development and progression that have created newly approved treatment options for subsets of patients. Published data in these and other areas require serial updates of existing guidelines to facilitate clinical care. In the current guidelines, an approach to clinical decision-making is introduced based upon the individual patient and clinician journey with thyroid cancer, which we term DATA:
Overall DATA framework for clinical management.
In 1996, the ATA published treatment guidelines for patients with thyroid nodules and DTC. 7 Over the last 25–30 years, there have been remarkable advances in knowledge affecting the diagnosis and treatment of DTC, but clinical controversy continues to exist in many areas. In the end, the goal is to provide individualized therapy for each patient based on the best application of clinical data to their unique case. For example, a less aggressive approach would be recommended for individuals with early-stage DTC who have an excellent prognosis or for individuals at higher risk of side effects, while a more aggressive approach would be recommended for those patients with higher risk disease or those with inadequate response to initial therapy. Overall, there are too few high-quality clinical trials in thyroid cancer, contributing to uncertainty and controversy surrounding several important areas of clinical management. As a group, specific areas where future research is felt to be essential to support data-informed clinical care are noted in the text.
Finally, as clinical decisions in the office are made jointly by patients and clinicians (i.e., shared decision-making), we provide specific sections regarding survivorship concerns from patient advocates and point to areas where patient-reported outcomes research is needed. In situations where clinicians from multiple disciplines are managing patients, a transdisciplinary approach is recommended to optimize collaborative clinical care and communication with the patient and between physicians. Examples may include multidisciplinary tumor boards, co-located clinics, and direct communication between clinicians.
Aim and Target Audience
The objective in these guidelines is to inform clinicians, patients, researchers, and health policy makers about the best available evidence (and its limitations) relating to the diagnosis and treatment of adult patients (over 18 years of age) with DTC. ATA guidelines for pediatric thyroid cancer have been published and/or are under development. 8 Compared with prior guidelines, this document applies only to patients with DTC, including individuals diagnosed with noninvasive follicular tumors with papillary-like nuclear features (NIFTP) and follicular tumors with uncertain malignant potential (FUMP), extremely low-risk lesions with diagnosis possible only after surgical excision.
This document is intended to inform clinical decision-making using the DATA framework for patients as they proceed through their individual journey with thyroid cancer, minimizing potential harm from overtreatment in patients at low risk for disease-specific mortality and morbidity while more intensively monitoring and treating patients at higher risk, including those with aggressive forms of DTC. These guidelines should not be interpreted as a replacement for clinical judgment and should be used to complement informed, shared patient–clinician consideration of complex issues. It should also be recognized that specific recommendations apply most to those patients reflected by participants in the studies referenced and therefore may or may not be applicable to individuals with unique demographic, clinical, and pathological characteristics. National clinical practice guidelines may not necessarily constitute a legal standard of care in all jurisdictions. 9 If important differences in practice settings present barriers to meaningful implementation of the recommendations of these guidelines, interested physicians or groups (in or outside of the United States) may consider adapting the guidelines using established methods10,11 (ADAPTE Collaboration, 2009, http://www.g-i-n.net). ADAPTE Collaboration is an international group of researchers, guideline developers, and guideline implementors who aim to promote the development and use of clinical practice guidelines through the adaptation of existing guidelines. As our primary focus was reviewing the quality of evidence related to health outcomes and diagnostic testing, we have decided a priori not to focus on economic resources and financial implications within specific recommendations. However, with attention to survivorship and with participation of a patient advocate, we include a section on this important topic (i.e., “financial toxicity”) as an emerging area of research and attention.
It is recognized that other groups have developed clinical practice guidelines for DTC in the United States and worldwide. While there are many similarities in approaches and recommendations across guidelines, there also are many controversies, differences in critical appraisal approaches and in clinical practice patterns across geographic regions and clinician specialties, as well as inconsistency in available testing and treatment approvals in different countries. In the end, it is not surprising that organizational guidelines will not completely agree for all issues. These differences highlight the importance of clarifying evidential uncertainties with additional research.
Methods
The first ATA Thyroid Nodules and Differentiated Thyroid Cancer guidelines were published in 1996 7 and revised in 2006, 12 2009, 13 and 2015. 14 Due to the expansion of knowledge concerning the management of thyroid nodules and DTC, a decision was made to separate the topics into two sets of updated guidelines. Task force chairs were appointed by the ATA President with approval of the Board of Directors (BOD). A committee of specialists with complementary expertise was appointed representing Endocrinology, Surgery (endocrine surgery and otolaryngology—head and neck surgery), Nuclear Medicine, Pathology, Medical Oncology, Cancer Genetics, and Medical Informatics/Clinical Epidemiology. For the first time, a patient advocate was included. Conforming to ATA policy to ensure broad specialty and geographic representation with fresh perspectives, at least one-third of the task force was made up of new members who did not help to create prior ATA guidelines.
Management of potential competing interests
Task force chairs were proposed and vetted by the ATA Guidelines and Statements Committee (GSC) and then confirmed by the ATA BOD. Potential conflicts of interest (COI) also were assessed by the ATA GSC and BOD. Task force chairs were selected for their expertise, and 11 proposed task force members were evaluated for COI prior to invitations to serve on the committee. Any potential financial competing interests were declared (see COI section), and, where appropriate, individuals were not involved in the final approval of recommendations for which a potential or perceived conflict was identified. Competing interests were re-evaluated annually by the task force chairs and members. The opinions expressed herein are those of the authors, and the task force had complete editorial independence from the ATA. Except for the methodology consultant (R.C.), who received payments from the ATA, no individual task force members received funding from the ATA or from industry for work on these guidelines.
Systematic review methods
A series of systematic reviews were conducted to inform these guidelines. The key questions used to guide the systematic reviews were developed by the guidelines task force using the PICO (Population, Interventions, Comparisons, and Outcomes) framework. The population was people with DTC, as described above. Outcomes were prioritized through discussion and consensus of the group. Survival or mortality outcomes (all-cause and/or cancer-specific) were prioritized most highly, followed by other oncologic (e.g., metastasis, progression, recurrence) and clinical ones (e.g., quality of life [QoL], function, adverse events). Intermediate (e.g., radiological or laboratory) outcomes were assigned lower priority.
For key questions addressing active surveillance versus immediate surgery and diagnostic accuracy of serum thyroglobulin (Tg) management following partial thyroidectomy or total/near-total thyroidectomy without radioactive iodine (RAI), the guidelines task force commissioned systematic reviews from the Pacific Northwest Evidence-based Practice Center at Oregon Health & Science University.15,16 For these systematic reviews, searches were conducted by an information specialist on Ovid MEDLINE, Embase, and Cochrane Central for relevant studies using search terms based on the corresponding prespecified inclusion criteria (PICOs). Searches were supplemented by reference list review for additional studies. Inclusion was restricted to English-language studies, and studies published only as conference abstracts were excluded. Two investigators independently reviewed titles, abstracts, and full-text articles for eligibility for inclusion. Data on study characteristics, patient and tumor characteristics, and results were extracted by one investigator and verified by a second. The quality (risk of bias) of each study was assessed using study-design specific criteria adapted from the U.S. Preventive Services Task Force Procedure Manual. The overall quality of evidence was assessed using methods adapted from the Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group, based on risk of bias, consistency, directness, precision, and reporting bias. Evidence was graded as “high,” “moderate,” “low”, or “very low” certainty, indicating the confidence in the findings; in accordance with the adapted approach to GRADE developed by the Clinical Guidelines Committee of the American College of Physicians, 17 evidence too limited to permit reliable conclusions was graded as “insufficient.”
For the other Key Questions, task force members also conducted searches of electronic databases (Medline using PubMed or OVID) with assistance from an information specialist, selected articles using prespecified eligibility criteria, and assessed the quality of evidence using methods adapted from GRADE and the American College of Physicians.
Guideline development methods
Each recommendation was developed by a subgroup of members based on the findings of the systematic reviews. Draft recommendations were reviewed by the full committee and revised based on full committee input prior to final voting. Approval of recommendations was by group discussion and an informal consensus process in meetings led by the co-chairs17–19 ; final recommendations required majority approval from all nonconflicted task force members. Task force members used criteria adapted from methods developed by the U.S. Preventive Services Task Force and the Cochrane Collaboration to assess the quality of included papers.20,21
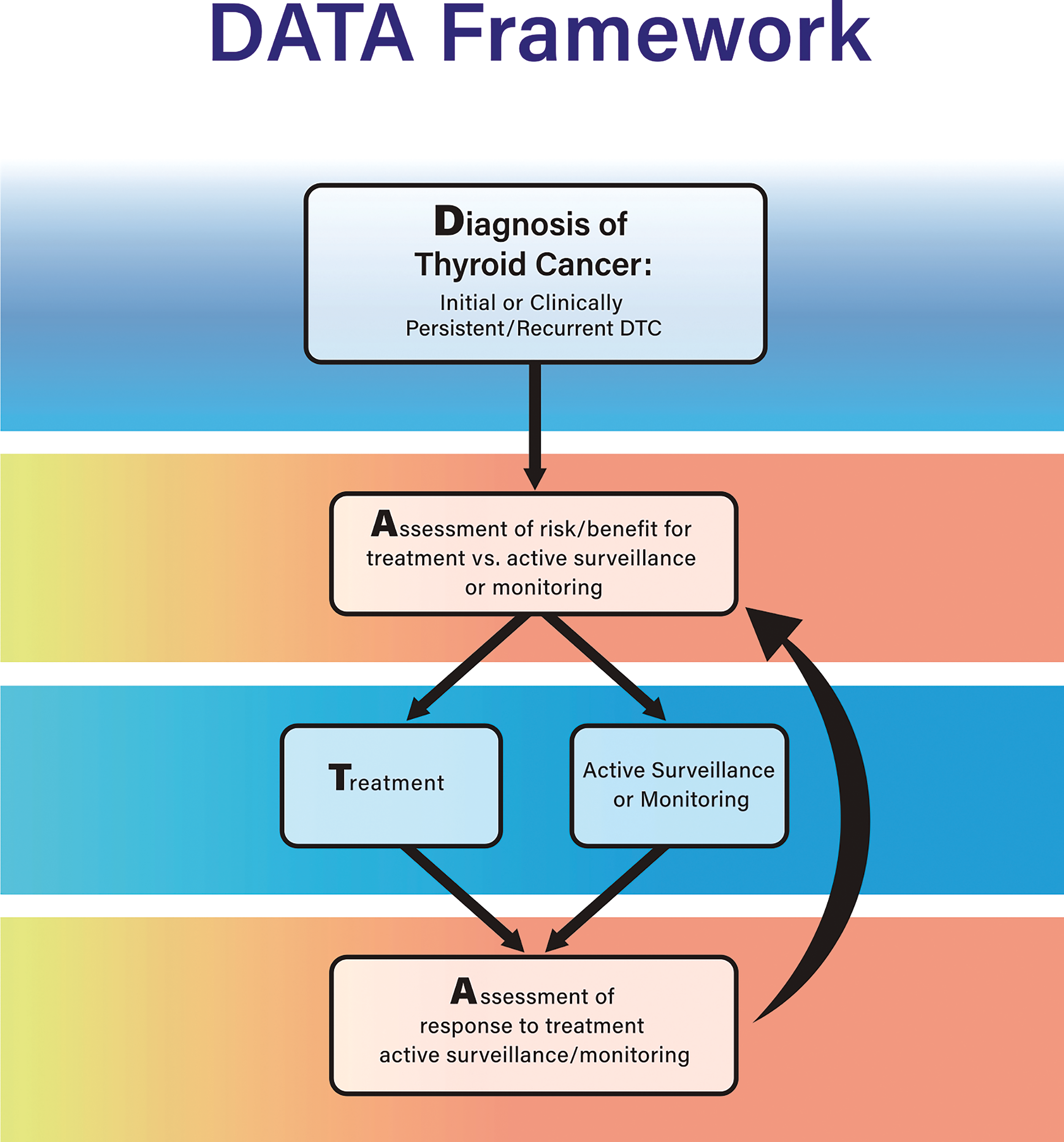
Each recommendation was graded as strong or conditional (Table 1). 22 Strong recommendations are applicable to all or nearly all persons or situations and are indicated when benefits clearly outweigh harms with at least moderate certainty. Other factors supporting strong recommendations are non-sensitivity to values/preferences regarding outcomes, high feasibility and acceptability, low or efficient costs or use of resources, and anticipated positive impacts on equity. When certainty is low, strong recommendations require a strong rationale for benefit despite uncertainty in the evidence and strong supporting considerations (e.g., low cost, high feasibility, high acceptability, and/or likely positive impacts on equity). Conditional recommendations are applicable to most people or situations, though other courses of action might be appropriate in certain circumstances or under certain conditions. Conditional recommendations are indicated when the balance of benefits to harm is relatively close, when there is lower certainty about benefits and/or harms, when decisions are preference-sensitive, or when there are important concerns about feasibility, acceptability, resource use, or equity impact.
GRADE Recommendation Grid
Strong recommendations are only indicated when certainty is low or very low in limited circumstances.
When the quality of evidence was low or insufficient, a Good Practice Statement (GPS) served as an alternative to a graded recommendation in selected situations. 23 A GPS is not GRADE-d but is like a strong recommendation, in that it is applicable to all or nearly all persons or situations; not following a GPS would be considered outside of usual clinical practice. To be a GPS, the benefits of the recommended intervention must be obvious and actual certainty of benefits must be high despite the lack of direct evidence demonstrating benefits. In many cases, collecting direct evidence showing benefits may not be feasible. Rather, inferred benefits are based on a compelling chain of indirect evidence that must be clearly described. In general, to qualify as a GPS, there must be consensus from the guidelines group. A unanimous consensus was required for all GPS included in these guidelines.
After completion of approved recommendations, a final literature review was performed by each group, including manuscripts published and available electronically or in print through July 1, 2024. A single exception was made to include the recently published updated World Health Organization’s (WHO) classification of tumors or endocrine organs in 2025. 24 Once the article was drafted, all recommendations were re-reviewed by all panel members until no further suggestions for revisions were requested by any panel members. Thus, consensus on acceptability of recommendations and article text was reached for all recommendations. This approach adheres to best practices in guideline consensus statements. Patient representative input was requested for all recommendations; the patient representative was a full member of the committee and included in all consensus discussions.
The guidelines article was reviewed and approved by the ATA Clinical Practice Guidelines and Statements Committee and the ATA BOD and then made available to the entire ATA membership for review and comments in the Fall of 2024. Feedback and suggestions were discussed by the task force, and revisions were made to the article prior to journal submission. The organization of management guideline recommendations is shown in the table of contents.
Clinical Management Principles: Dictionary and Definitions
Several terms are utilized throughout the guidelines in different sections and recommendations. Important definitions used by the committee are included below:
General definitions
Active surveillance
The ongoing observation or active monitoring of a known or suspected primary, intrathyroidal, low-risk DTC with serial imaging as an alternative to upfront surgical intervention. This is a type of expectant management and is only appropriate for a subset of low-risk DTCs (see
Disease monitoring
Monitoring for biochemical (elevated level of serum Tg) and/or structural persistence or recurrence of disease (as confirmed by imaging and/or biopsy) following the diagnosis and initial treatment (surgery ± RAI) of thyroid cancer. It is deployed to evaluate patients for disease progression and inform the type and timing of interventions deemed appropriate.
Response to therapy
Response assessment is performed after intervention, either for initial or clinically persistent/recurrent disease14,16,25 (see
Excellent response
No biochemical or structural evidence of persistent thyroid cancer (i.e., remission).
Indeterminate response
The presence of nonspecific findings on imaging; mildly elevated serum Tg levels; or positive, but stable or declining, anti-Tg antibody (TgAb) levels in persons who have undergone total thyroidectomy with or without RAI. Most patients in this category prove to have a “good” clinical response to therapy, especially if they have a low risk of clinical recurrence, and findings are nonspecific. However, those at intermediate or high risk of clinical recurrence based on histopathologic and staging characteristics in this category may have higher rates of recurrence.
Biochemically incomplete response
Elevated serum Tg concentrations or rising TgAb levels without radiological evidence of structural recurrence in persons who have undergone total thyroidectomy with or without RAI.
Structurally incomplete response
Structural evidence of disease recurrence (by imaging or biopsy), usually in conjunction with elevated Tg and/or TgAb levels.
Persistent or recurrent disease
Clinically persistent disease
Biochemical or structural evidence of disease within 90 days of initial therapy (or intervention for persistent disease).
Clinically recurrent disease
Biochemical or structural disease subsequently identified in patients previously deemed to have an excellent response following therapy. Clinically recurrent disease likely represents progression of residual disease that is below the lower limits of detection.
Risk of recurrence
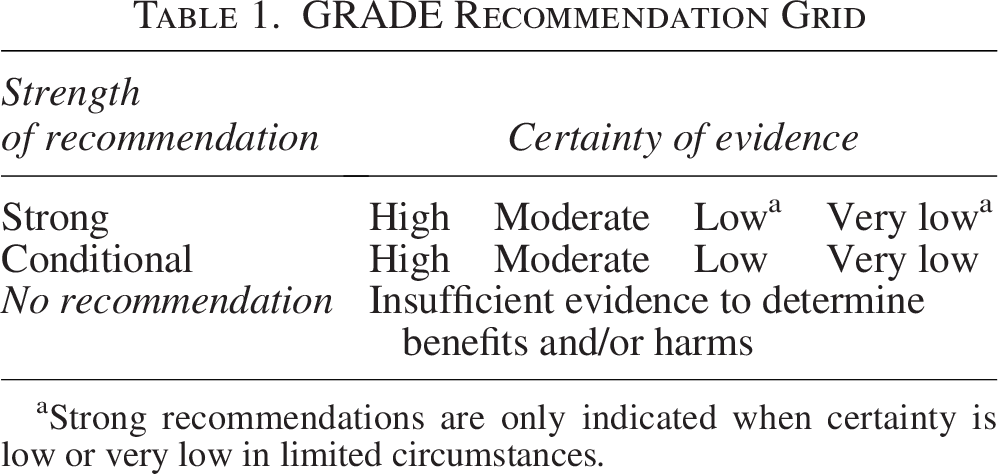
We use the term “recurrence” to mean clinical recurrence, recognizing that most recurrences reflect growth of residual disease to clinically detectable levels (Fig. 2). An overall assessment of risk of biochemical or structural recurrence determined by incorporating a combination of factors: histopathologic characteristics of the resected tumor, American Joint Committee on Cancer (AJCC) staging, imaging, molecular analysis of tumor, and response to therapy at subsequent evaluation. 27 For the purpose of these guidelines, categories are designated as low (<10%), low-intermediate (10–15%), intermediate-high (≥16–30%), and high (>30%) risk of recurrence.
Treatment definitions
Extent of surgery definitions (ATA website definitions)
Extent of lymphadenectomy definitions
Central neck dissection
Central neck lymph nodes include Levels VI and VII (Fig. 3).29–33 Central neck dissection is a comprehensive removal of pretracheal and prelaryngeal lymph nodes, along with at least one paratracheal nodal basin. It can be unilateral or bilateral; the laterality and extent of dissection should be documented at the time of operation in addition to surgical intent (therapeutic vs. prophylactic).
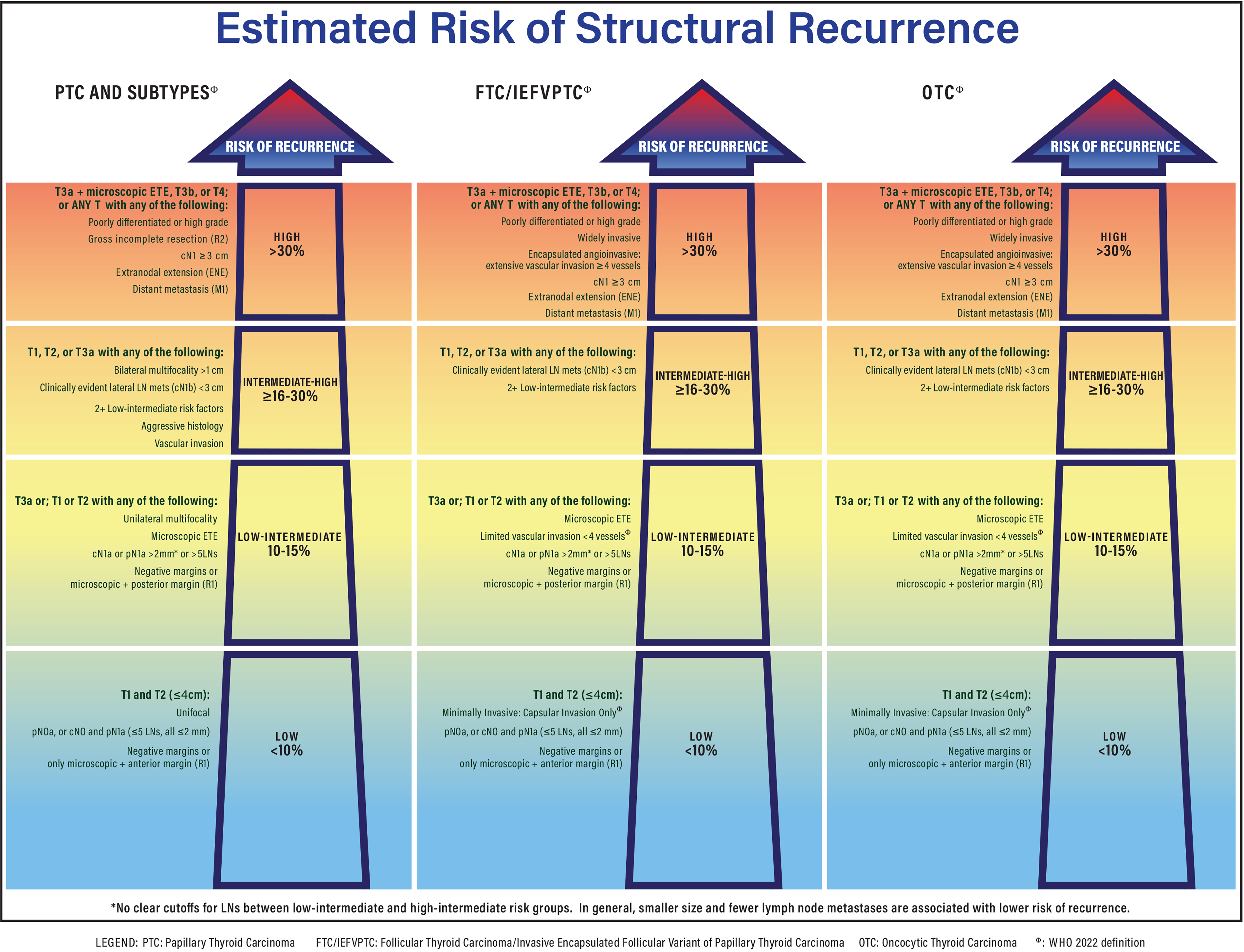
ATA 2025 Risk of Recurrence for PTC, FTC, and OTC. *Lymph metastases are uncommon in OTC and FTC/IEFVPTC. FTC, follicular thyroid carcinoma; IEFVPTC, invasive encapsulated follicular variant of papillary thyroid carcinoma; OTC, oncocytic thyroid carcinoma; PTC, papillary thyroid carcinoma.
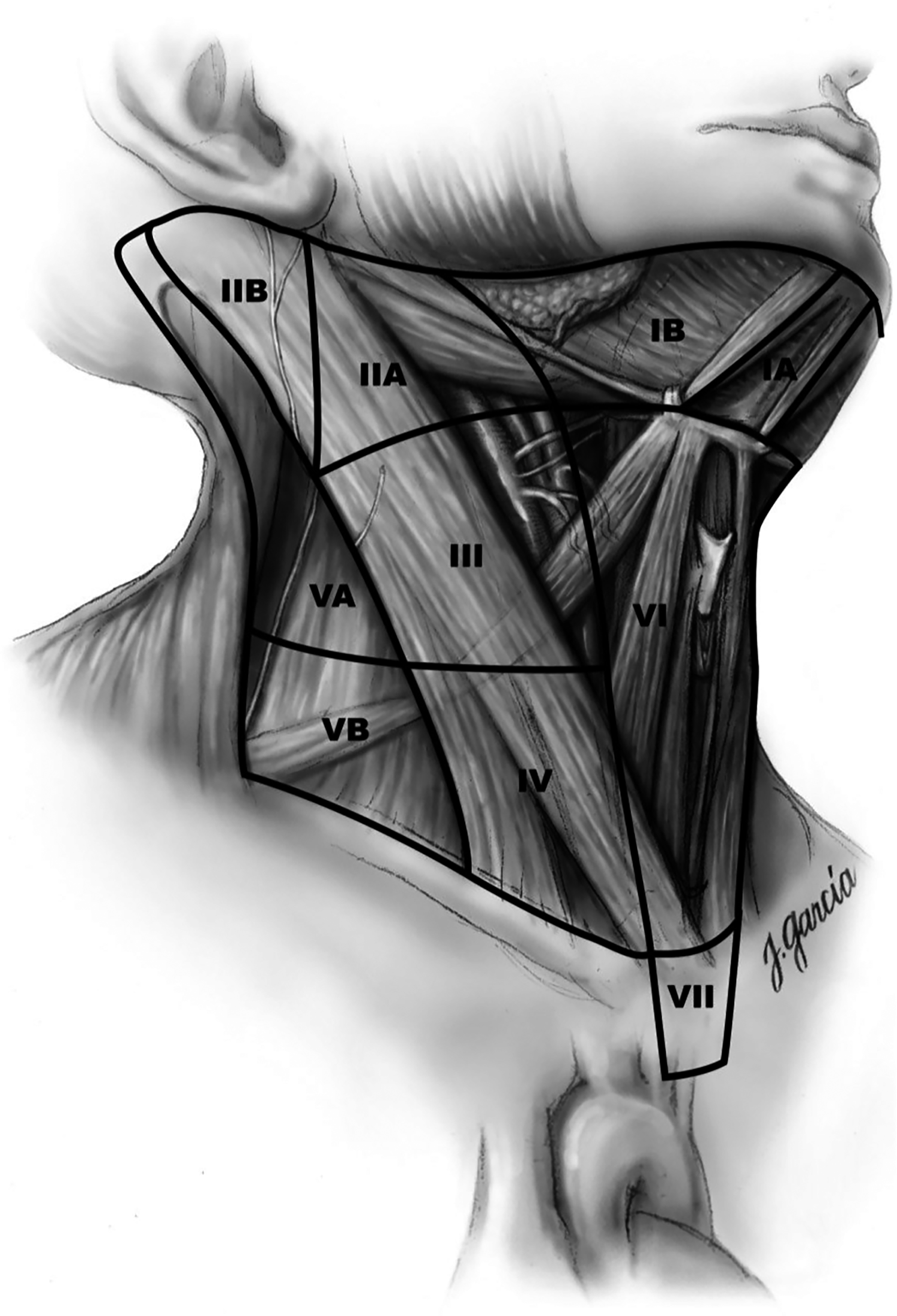
Nodal levels with corresponding anatomical landmarks (used with permission from R. Udelsman, MD).
Therapeutic
It implies that metastatic nodal disease is apparent clinically preoperatively or intraoperatively by examination and/or imaging, cN1a.
Prophylactic
It implies that no metastatic nodes are detected by examination or imaging preoperatively or intraoperatively, cN0.
Lateral neck dissection
Full compartment dissection of the lateral cervical neck lymph nodes in Levels IIA, III, IV, and VB ipsilateral to the tumor and performed for clinical evidence of metastatic involvement. Dissection of Levels I, IIB, and VA are not regularly performed but can be considered based on findings suggestive of metastatic disease in these compartments (Fig. 3).
Completeness of surgical resection
The goal of surgery is to remove safely as much thyroid cancer as possible. To define the completeness of resection, the AJCC created definitions that are used in these guidelines to facilitate communications. An R0 resection means that the surgical margin is microscopically negative for residual tumor. An R1 resection means that there is no residual macroscopic tumor but that microscopically positive margins still demonstrate the presence of tumor. R2 resection means that gross (macroscopic) disease remains post-surgery.
131I, RAI administration
Remnant ablation
RAI administration to destroy benign remnant thyroid tissue following total or near-total thyroidectomy. 26
Adjuvant therapy
RAI administration to destroy suspected (but not identified) remaining thyroid cancer following total or near-total thyroidectomy.
Therapeutic treatment
RAI administration to treat known residual or recurrent thyroid cancer, either initially or with subsequent progression of thyroid cancer after total or near-total thyroidectomy.
Thyrotropin suppression therapy
Use of thyroid hormone to suppress serum thyrotropin (TSH) concentrations below the normal range based on the risk of recurrence and/or response to therapy.
Initial DTC Management
The DTC guidelines begin with a certain or near-certain diagnosis of thyroid cancer on preoperative FNA testing (Bethesda VI cytology and/or molecular results with high certainty of malignancy) as reviewed in the thyroid nodule guidelines, or after initial surgery based on surgical histopathology analysis. We also include a discussion of the NIFTP and FUMP due to their malignant potential. Recent updates were made to the histological criteria, subtypes of thyroid cancer, and staging. They are summarized in the following section.
Thyroid cancer pathology
Throughout this document, the 5th edition of the WHO Classification of Thyroid Tumors has been utilized for descriptions of the types of non-anaplastic follicular cell-derived thyroid carcinomas and NIFTP (Tables 2 and 3). 24 Approximately 90% of thyroid cancer cases are well differentiated and are classified based on the predominant histomorphology; however, they now also can be categorized based on their molecular profiles. Four main types of DTC include follicular thyroid carcinoma (FTC), invasive encapsulated follicular variant of papillary thyroid carcinoma (IEFVPTC), papillary thyroid carcinoma (PTC), and oncocytic thyroid carcinoma (OTC).24,34–36
Pathological Diagnostic Criteria of NIFTP

Tumors are well demarcated from the surrounding thyroid parenchyma and can be thinly or partially encapsulated.
Features requiring histopathologic examination of the entire tumor capsule and tumor.
NIFTP, noninvasive follicular tumors with papillary-like nuclear features.
WHO Pathological Classification of Differentiated Thyroid Carcinoma (WHO, 5th Edition) 24
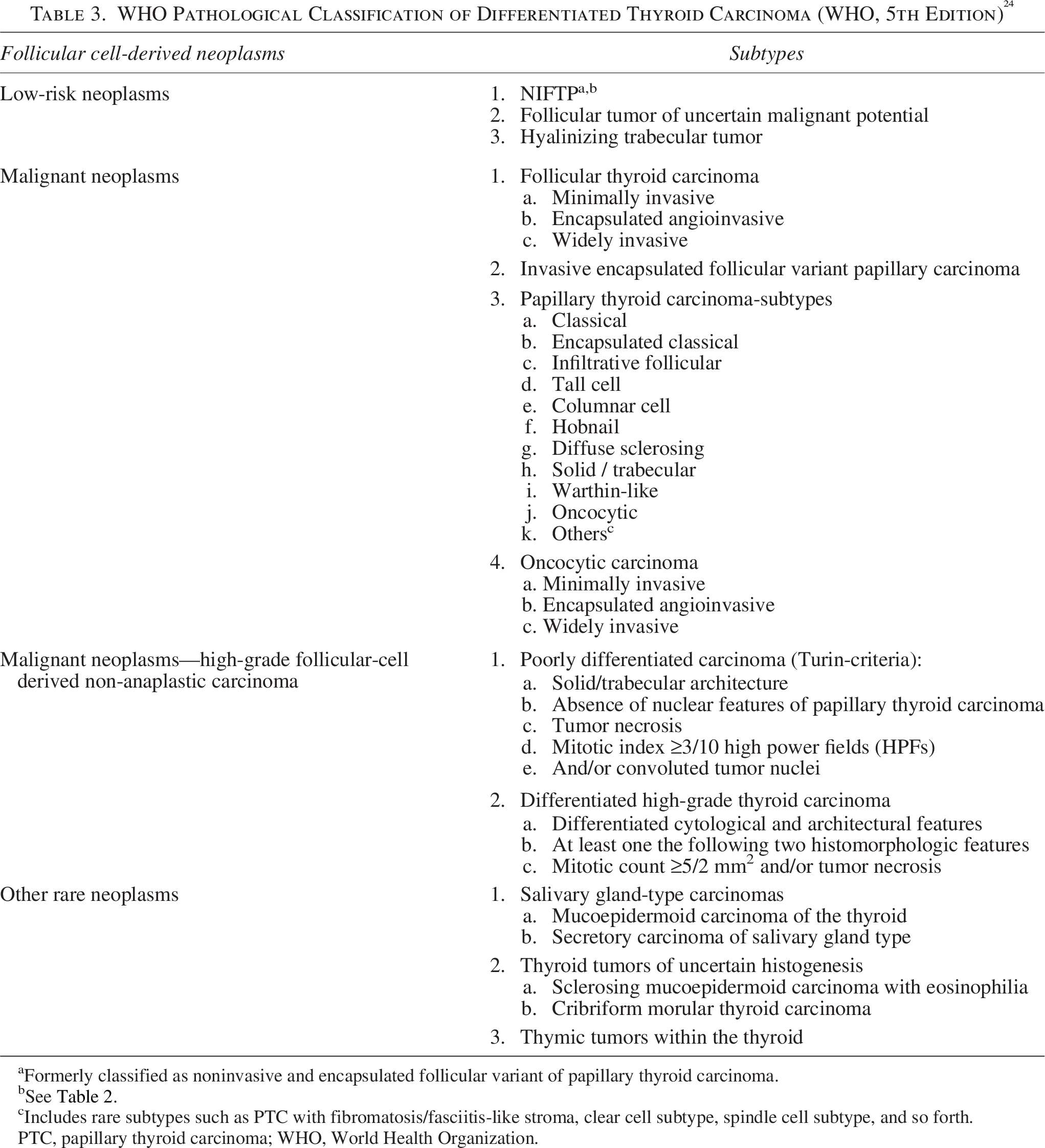
Formerly classified as noninvasive and encapsulated follicular variant of papillary thyroid carcinoma.
See Table 2.
Includes rare subtypes such as PTC with fibromatosis/fasciitis-like stroma, clear cell subtype, spindle cell subtype, and so forth.
PTC, papillary thyroid carcinoma; WHO, World Health Organization.
PTC is the most common type of DTC. PTC is typically indolent and associated with excellent long-term survival: 96% at 5 years, 93% at 10 years, and >90% at 20 years. Overall, mortality rates for PTC are 1–6.5%, with an overall recurrence rate of 15–35%; tumor recurrence typically occurs in the tumor bed, cervical lymph nodes, or (rarely) distant sites.14,37 PTCs have characteristic nuclear features and can present as infiltrative and encapsulated tumors. Molecular studies have shown that most PTCs (90%) develop by the activation of a Mitogen-activated protein kinase (MAPK) pathway-event.38,39 This activation occurs via mutually exclusive mutations in BRAF or RAS oncogenes. A subset of PTCs is acquired by gene fusions involving rearranged during transfection (RET) or (less commonly) other receptor tyrosine kinases. Oncogenic mutations at BRAFV600E are the most common in PTC; a minority can show non-V600E mutations, such as BRAFK601E or BRAF fusions. The IEFVPTC is an encapsulated and invasive follicular-patterned tumor. Based on its tendency for vascular invasion, distant metastasis, and molecular profile, it can behave similarly to FTC.26–32
Histologically, FTCs are encapsulated follicular patterned tumors without the nuclear features of PTC; they are characterized by the presence of vascular (limited or extensive) and or capsular invasion (vascular invasion involving vessels within the tumor capsule) and widely invasive (extensive invasion of the thyroid parenchyma beyond the tumor capsule). 24 These tumors are mostly driven by activating mutations in RAS oncogenes (NRAS>HRAS>KRAS), PAX8::PPARγ fusions, EIF1AX mutations, PIK3CA mutations, or loss of PTEN expression. BRAFV600E and RET fusions typically are not seen in FTC. Expression of PAX8::PPARγ fusions oncoprotein occur in 25% of FTC, in which the thyroid transcription factor PAX8 drives the expression of PPARγ,38,40 a receptor involved in adipocyte biology. Mutations in DICER1, which encodes a ribonuclease in the processing of microRNA precursors, occur in RAS-like thyroid neoplasms and are prevalent in FTC. DICER1 mutations can also be seen in subsets of PTC, differentiated high-grade thyroid carcinoma (DHGTC), poorly differentiated thyroid carcinoma (PDTC), and anaplastic thyroid carcinoma (ATC).
With greater recognition of the unique genomic features of OTC (previously known as Hürthle cell carcinoma) and different clinical behavior from classical forms of FTC, these tumors are now considered a third form of DTC rather than a subtype of FTC in the current WHO classification; they account for ∼3% of all DTC.24,41,42 An “oncocyte” is an enlarged polygonal cell with an abundant granular eosinophilic cytoplasm, round nuclei with even chromatin pattern, and prominent nucleoli. As defined by WHO, oncocytic neoplasms are usually encapsulated and composed of ≥75% oncocytic cells.24,36,43 Oncocytic features can be identified in some PTC or FTC cells at lower frequencies. Most of these tumors are larger in size; however, smaller tumors can be identified. Like FTC, the presence of invasive characteristics (i.e., tumor capsule and/or vascular invasion in an encapsulated oncocytic neoplasm) is diagnostic of OTC, and OTCs can be classified as minimally invasive, encapsulated angio-invasive, and widely invasive.
Genomically, OTCs are characterized typically by a near-haploid genome, mitochondrial DNA mutations commonly involving genes encoding Complex 1 of the mitochondrial respiratory chain, and mutations in DAXX and ATRX involved in telomere length. OTCs can also have mutations that activate mammalian target of rapamycin (mTOR) and MAPK signaling, and like PTC and FTC, more aggressive OTCs can have mutations in the TERT promoter or TP53.44,45 Clinically, some studies have shown that OTCs have a greater tendency toward lymph node metastases while retaining a predilection for distant metastases, and unlike FTC, OTCs often are not radioiodine-avid despite retaining other differentiated features, such as Tg secretion and TSH receptor expression.46–55
The 5th edition of the WHO Classification of Thyroid Tumors also introduces a new category of high-grade follicular cell derived, non-anaplastic carcinoma that includes PDTC and DHGTC. 24 By molecular analysis, poorly differentiated thyroid cancer and DHGTC harbor driver mutations in BRAF (BRAFV600E) and RAS genes, and some cases may show gene fusions (often RET and NTRK3). Additional mutations in the TERT promoter, PIK3CA, and TP53 are commonly identified.36,43,56–59
DHGTC has been defined by certain authors as a “thyroid malignancy” that is recognized as DTC but in which certain histological and cytopathologic features are present that justify the lesion being classified as “high-grade.”37,60–67 The DHGTCs are invasive, high-grade carcinomas that show one of the following two histological features: mitotic count ≥5 per 2 mm2 and tumor necrosis.36,43,56,58,68–70 By contrast, thyroid carcinomas classified as PDTC are follicular cell-derived tumors that show a minor component of DTC (papillary, follicular, oncocytic), show solid and/or insular growth pattern with presence of either necrosis or ≥3 per 2 mm2, and lack the usual histological characteristics and aggressiveness of ATC. In both cases, clinical behavior is considered intermediate between DTC and ATC.24,36,65,71–75
Non-invasive follicular thyroid neoplasm with papillary-like nuclear features
NIFTP is the pathological definition of a type of noninvasive follicular cell-derived thyroid neoplasm that was first described in 2016. 76 This topic post-dated the 2015 ATA thyroid nodule and DTC guidelines, but a subsequent ATA task force statement in 2017 supported adoption of the NIFTP nomenclature for this entity. 77 In 2017, NIFTP were classified as a distinct category in the revised WHO Classification of Tumors of Endocrine Organs, corresponding to a neoplasm with very low malignant potential. 24
NIFTP comprise approximately 2.1–9.6% of follicular cell-derived thyroid neoplasms, with relatively lower incidence in Asia than in North America and Europe.78–82 NIFTP are characterized by validated histological inclusion and exclusion features (Table 3). The original NIFTP validation study excluded tumors measuring ≤1 cm and those with oncocytic features. 76 However, as subsequent literature has shown that tumors measuring ≤1 cm (micro-NIFTPs) or with oncocytic features (oncocytic-NIFTPs) demonstrate similar clinical behavior to those of original NIFTP,62,76,83–85 these features also are included in the tumor’s current pathological definition. The initial definition of NIFTP had required the presence of <1% papillae, 76 but subsequent experience83,86,87 has shown this feature can be associated with lymph node metastases; therefore, the diagnostic criteria have been revised to require that papillae are absent. 83 It is recommended to carefully examine the entire tumor capsule interface and tumor to exclude the possibility of invasive features and presence of papillae. 76 NIFTPs often coexist with one or more NIFTPs or other thyroid malignancies in the ipsilateral or contralateral lobes.
Studies assessing the molecular profile of NIFTPs have shown them to be clonal neoplasms.88–91 Molecular alterations are present in approximately 78% of cases, with approximately 30–54% of NIFTP tumors harboring a RAS mutation (NRAS mutations most common, followed by HRAS and rarely KRAS mutations).89,92 However, the NRAS mutations seen in NIFTPs may also be identified in FTCs and IEFVPTC; therefore, they are nonspecific. A small subset of NIFTP cases have been shown to harbor PAX8::PPARγ fusions, THADA fusions, and BRAFK601E mutations.89,93 Some studies also have explored miRNA expression in NIFTP cases, demonstrating that two mi-RNAs (miR-10a05p and miR-320e) can effectively discriminate between NIFTP and the infiltrative follicular variant of PTC. 94 Further studies are required to validate these findings.
While NIFTPs are characterized by a follicular growth pattern and nuclear features of PTC (Fig. 4), they are associated with extremely low malignant potential.76,95,96 Several multi-institutional series (largest sample, n = 363), including several that reclassified DTCs as NIFTP upon retrospective analyses, have mostly reported zero risk of disease persistence/recurrence over a mean or median follow-up of up to 11.8 years. 97 Lymph node metastases have been seen in <5% of the total cohort and in only a few series.80,87,98,99 Only one retrospective analysis of 102 cases showed the presence of distant metastases (to the lungs) in one case, although this study was limited by incomplete follow-up (80%) and a high proportion of patients who received more aggressive care (total thyroidectomy and radioiodine ablation). 80 At present, there are no available data comparing the clinical benefits and harms of various short- and long-term monitoring strategies in patients with NIFTP tumors.
Is NIFTP considered thyroid cancer?
▪
NIFTP and other tumors of uncertain malignant potential (Follicular Tumor of Uncertain Malignant Potential and Hyalinizing Trabecular Tumor) are diagnosed pathologically and have a very low malignant potential (lower than the lowest-risk DTC). Further treatment with completion thyroidectomy/lymphadenectomy and/or RAI is not advised routinely. The optimal approach to postoperative monitoring of these tumors is uncertain.
Thyroid cancer epidemiology
After rising for three decades, thyroid cancer incidence peaked in 2015 at 14.9 per 100,000. Then, between 2015 and 2017, a decline was observed for the first time in 30 years. 100 The initial increase in incidence was thought to be related to a true increase in the incidence of PTC as well as widespread use of diagnostic imaging and FNA of thyroid nodules leading to potential “overdiagnosis.”101–104 “Overdiagnosis” is defined as the diagnosis of cancers that would not, if left in place, result in symptoms or death. 105 The decline in incidence may be due to a heightened awareness of the potential harms of overdiagnosis. 106 The observed decrease has correlated temporally with clinical management recommendations from the 2009 and 2015 ATA guidelines, which suggested a larger nodule size threshold and higher ultrasound suspicion for biopsy of thyroid nodules and use of molecular markers for small, indeterminate nodules.13,14 Similar recommendations were published by the American College of Radiology with its thyroid imaging reporting and data system. 107 In 2017, the U.S. Preventative Services Task Force (USPSTF) recommended against thyroid cancer screening in asymptomatic adults. This also might have contributed to decreasing thyroid cancer incidence.108,109 The 2016 reclassification of NIFTP also is reported to have contributed to the observed decline. 104 Notably, the increase in thyroid cancer incidence observed from 1974 to 2013 occurred for all stages of disease, and the mortality rate from that same period increased annually by 1.1% in advanced disease.109,110
Accepted risk factors for thyroid cancer include a history of childhood head and neck radiation, total body radiation for bone marrow transplantation, 111 and exposure to ionizing radiation from fallout in childhood or adolescence. 112 Adult occupational radiation exposure in the low-to-moderate dose range (<0.5 Gy) has not been associated with a significantly increased risk of thyroid cancer.113,114
Additional potential risk factors have been identified, and further study is necessary to determine their causative relationship with thyroid malignancy. As outlined in
DTC can occur in families, which is termed familial non-medullary thyroid cancer (FNMTC). FNMTC is further classified as “syndromic” when it is one of a constellation of tumors (e.g., PTEN [phosphatase and tensin homolog] hamartoma tumor syndrome [Cowden disease], familial adenomatous polyposis [FAP], Carney complex, Werner syndrome/progeria) or “non-syndromic,” when DTC is the single or prevailing inherited malignancy. Specific approaches and recommendations for both syndromic and non-syndromic forms of DTC are discussed below.
It has been shown that Ki-67/MIB-1 as a marker for cell proliferation can be used to assess clinical behavior in numerous malignancies. Ki67 is expressed in all cell proliferation stages except G0 and can be easily evaluated immunohistochemically in tissue samples. High Ki-67 proliferation index correlates with poor prognosis in thyroid carcinomas; however, additional studies are needed to make this an essential step in the pathological assessment of well-differentiated thyroid carcinomas.121–123
Genetic predisposition to follicular cell-derived thyroid cancer and genetic counseling
Principles of germline genetic testing
The genetic testing process involves pre-test counseling, identification of the most appropriate testing options, and post-test result disclosure. Ideally, this is conducted by a certified genetic counselor and/or other provider (endocrinologist, oncologist, geneticist, etc.) with expertise and experience in cancer genetics and thyroid cancer. Clinicians without direct referral access to the appropriate expertise should be aware of the telehealth genetic counseling options available. In the United States, both in-person and telehealth resources can be found through the National Society of Genetic Counselors “Find a Genetic Counselor” tool (www.nsgc.org).
Pre-test counseling components should include the following: (i) a carefully performed three- to four-generation pedigree of the patient’s family; (ii) assessment of the patient’s risk to carry a heritable cancer susceptibility gene variant, as well as the patient’s absolute risks to develop various types of cancer, given the patient’s family history; (iii) psychosocial assessment and counseling of the patient; (iv) education of the patient regarding the suspected hereditary cancer syndrome (e.g., inheritance, penetrance); (v) implications of having genetic testing from the personal, family, and insurance perspectives; and (vi) informed consent prior to obtaining a sample for genetic testing.
Due to overlapping phenotypes of hereditary predisposition conditions, genetic testing often utilizes multigene panel testing. Once test results are back, the post-test genetic counseling visit should include not only disclosure of the results in verbal and written form but also verbal and written information regarding the significance of the test results about cancer risk and the medical management options based on the estimated cancer risk to the patient. It also should include verbal and written discussions of the implications of the test results for family members, identification of resources for psychosocial support and future decision-making related to medical management, and results should be communicated to the treating physicians, particularly if counseling is performed by a genetic counselor rather than the treating physician.
Which patients with DTC should be offered germline genetic testing?
▪
Germline genetic testing may be offered in the following scenarios (Table 4):
Syndromes Associated with DTC

OTC was previously included as a subtype of FTC and is likely also associated with these hereditary predispositions.
CHRPE, congenital hypertrophy of the retinal pigment epithelium; CI, confidence interval; CMTC, cribriform-morular thyroid carcinoma; DM, diabetes mellitus; DTC, differentiated thyroid cancer; FTC, follicular thyroid carcinoma; NCCN, National Comprehensive Cancer Network; OR, odds ratio; OTC, oncocytic thyroid carcinoma; PDTC, poorly differentiated thyroid carcinoma; PHTS, PTEN hamartoma tumor syndrome.
Clinical suspicion for Cowden/PTEN hamartoma tumor syndrome (PHTS) due to a combination of DTC and non-thyroid malignancy/tumors/features
In patients who were diagnosed with FNMTC as children, clinical and family history should be evaluated for features of DICER1 tumor predisposition. Consideration may be given to germline DICER1 testing in patients from families with pediatric patients with DTC.
Pathologic diagnosis of cribriform morular thyroid carcinoma (APC gene)
Other combinations of tumors and/or cancers in a patient and/or their family members may raise concern for a hereditary predisposition condition, including rare conditions such as Carney complex or Werner syndrome. In these patients, genetic counseling and testing may be offered.
The National Comprehensive Cancer Network (NCCN) regularly updates testing guidelines for Cowden syndrome/PHTS. These criteria require a combination of major and minor criteria, with FTC (and presumably OTC) serving as a major criterion and PTC (including FVPTC) and structural thyroid lesions serving as minor criteria. 127 As a result, numerous clinical presentations can fulfill PTEN testing criteria. The spectrum of conditions resulting from pathogenic variants in PTEN is referred to as PHTS. Cowden syndrome is a part of this spectrum and characterized by an increased risk for thyroid, breast, endometrial, and (to a lesser degree) colon and renal cancers. Benign thyroid and breast tumors, other tumors such as trichilemmomas, papillomatous papules, lipomas, gastrointestinal hamartomas, or ganglioneuromas, and macrocephaly, intellectual disabilities, or autism spectrum disorders are common manifestations. 128 In PTEN-related disorders, there is an enrichment of FTC, but PTC remains the most common histology. PTC (including IEFVPTC) represents 56–60%, while FTC accounts for 25–45% of reported PTEN-related thyroid cancers.129,130
DICER1 tumor predisposition is characterized by an increased risk for pleuropulmonary blastoma, pulmonary cysts, thyroid neoplasia, ovarian tumors, and cystic nephroma. Germline pathogenic DICER1 variants were seen in 1 of 6 pediatric patients with PDTC, 131 4 of 15 pediatric patients with FTC, 132 and 0 of 20 pediatric patients with PTC. 133 However, other reports do suggest a relationship between germline DICER1 variants and pediatric PTC.134,135 The recommendations put forth by the International DICER1 Symposium suggest that germline DICER1 testing be considered based on the presence of multinodular goiter or thyroid cancer in two or more first-degree relatives. 124 However, given the commonality of this presentation in adults and the relative rarity of germline pathogenic variants in DICER1, the yield in this scenario may be low. Further research is required to determine the best screening strategy.
Cribriform-morular thyroid carcinoma (CMTC) is a rare malignancy that is frequently identified in patients with FAP due to a germline pathogenic variant in APC.136–138 It is characterized by a prominent cribriform architecture and formation of whorls or morules composed of spindle cells. The presence of aberrant beta-catenin immunoreactivity provides strong evidence for this cancer type.139–141 The cancer cells typically stain for NKX2-1 (TTF1) but are negative for Tg, raising the hypothesis that the tumor morules seen in this cancer are of thymic/ultimobranchial pouch origin. 142 Approximately 40% of patients with CMTC are found to have FAP. Although no microscopic tumor features can distinguish between familial and sporadic disease, tumor multifocality is more common in the setting of familial disease.139,143 Since many patients with CMTC have FAP, and thyroid cancer can precede clinically detectable colonic abnormalities in up to 40% of patients, 143 this diagnosis should raise the possibility of a hereditary predisposition and prompt consideration for genetic testing/counseling. Established syndromes associated with DTC are summarized in Table 4.
Recently, it has been reported that individuals with long telomeres due to variants in genes encoding components of the shelterin complex have a clinically identifiable multicancer predisposition that may include PTC. 144 Component cancers of the syndrome include melanoma, leukemia, and sarcoma, and the syndrome has been termed long telomere syndrome.144–147 PTC also was identified as being one of the 12 cancers associated with genetically determined long telomere length in a systematic review. 148 Interestingly, short telomeres also have been reported to predispose to thyroid cancer, and a U-shape relationship has been reported. 149 Further research in this area is needed to inform genetic screening recommendations.
Should patients with non-syndromic FNMTC receive genetic testing?
▪
There is a lack of evidence to suggest the utility of clinical germline genetic testing in non-syndromic FNMTC. In non-syndromic FNMTC, the non-thyroid malignancies in the family may drive decision-making regarding genetic testing.
Several studies have been performed in multigenerational kindreds with DTC (mostly PTC); in some families candidate genes have been identified through a combination of linkage analyses and sequencing.150–152 To date, variants in these candidate genes, while important for individual families, are nonrecurring and appear to be “private” to those families. Therefore, data do not support their inclusion in clinical panel testing. Because of the autosomal dominant inheritance pattern in most families, there may be a role for thyroid cancer screening in selected non-syndromic FNMTC in which there appears to be high penetrance, early age onset thyroid cancer, or aggressive disease (see below).
Some families with FNMTC may have enrichment of non-thyroid malignancies, which may be an indication for germline genetic testing. Therefore, some patients with sporadic DTC can also have a documented pathogenic variant in a cancer predisposition gene for other tumor types. Whether or not the DTC in those patients is related to their cancer predisposition is not always certain. For example, pathogenic variants (PV) in CHEK2 are a relatively common finding on clinical multigene panel testing and are associated with an increased risk for a variety of cancers. 153 Most notably, CHEK2 PVs are associated with a moderate increase in the risk for breast cancer. While associations with DTC have been suggested, 154 the magnitude of risk is modest, with an approximately two-fold risk for PTC associated with common CHEK2 variants. 155
Should family members of patients with FNMTC be screened for thyroid cancer?
▪
Individuals with a family history of FNMTC should have a careful history and directed neck examination as a part of regular health maintenance. Ultrasound screening may be considered in first-degree family members of individuals who meet criteria for a clinical diagnosis of FNMTC due to the presence of three or more (first or second degree) related individuals with diagnoses of NMTC. Ultrasound screening may also be considered in families with only two affected individuals showing other concerning features (such as particularly young ages of diagnosis) or with limited family structure. The age for initiation of such screening requires further study and should be carefully weighed against the risk of overtreatment.
Family members of patients with FNMTC may be considered at risk for disease based on epidemiological evidence showing that 5–10% of NMTC have a familial occurrence. However, in most of these families, only two members are affected. There is controversy about whether two family members are sufficient to define familial disease rather than a coincidental or screening-related association. Estimates suggest that when only two first-degree family members are affected, the probability that the disease is sporadic is 62%, with the probability decreasing to ≤6% when the number of affected family members is three or more. 156 However, while controversial, stratification of families with two first-degree family members based on age of diagnosis (both ≤45 years vs. one or both >45 years) has been reported to predict subsets of individuals with more frequent multifocal/bilateral cancers, more extrathyroidal extension, and compromised outcomes when compared to matched sporadic NMTC, and no significant differences when comparing families with one or more members with older ages at diagnosis. 157
A prospective interventional screening program investigated the impact of yearly screening in a cohort of 109 individuals from 25 kindreds (12 with two members affected and 13 with ≥3 members affected). Screening started as early as 7 years of age and included neck ultrasound and FNA of thyroid nodule(s) >0.5 cm. This led to the detection of thyroid cancer in 4.6% (2/43) of at-risk individuals from families with two members affected and in 22.7% (15/66) of at-risk members from families with ≥3 patients affected (p = 0.01). The youngest age of thyroid nodule detection was 7 years, and the youngest age of thyroid cancer diagnosis was 18 years. 158 Based on these data, Capezzone et al. suggest consideration of screening with yearly ultrasound in kindreds with ≥3 affected family members, starting from the age of 20 years, or 10 years before the earliest age of diagnosis in the family. 159 Further studies are needed to determine the optimal approach to family screening that address costs and the potential risks of overtreatment.
The USPSTF discourages screening for thyroid cancer in asymptomatic adults. 108 However, this recommendation was aimed at population-based screening. Screening programs in the setting of FNMTC should be initiated with caution, as there are no data regarding the impact of screening on outcomes in FNMTC, and the frequency of ultrasound is inconsistently applied. Several studies have suggested that FNMTC is associated with earlier age-of-onset and more aggressive behavior,143,160–163 although others have not demonstrated this relationship.164,165
When should germline genetic testing be offered to patients with DTC with alterations detected on tumor samples (somatic testing)?
▪
When genomic testing is performed on tumor samples for clinical purposes, both somatic and germline genetic alterations can be detected. If a potentially clinically relevant germline cancer-predisposing variant is detected, evaluate patients and their family histories for clinical correlation, and consider referral for genetic counseling for possible germline testing.
Sequencing of thyroid cancer specimens can occur at initial diagnosis as part of thyroid nodule evaluation, or later in the course of the disease to assist in determining treatment options. In both cases, pathogenic variants identified through sequence analysis of a tumor sample are either acquired somatic events or may be of germline origin. These tests are optimized for somatic variant detection. While paired tumor and analysis of normal tissue can help distinguish variant origin, such analysis is not a reliable method to detect germline variants, and studies have shown that up to 8.1% of pathogenic germline variants are missed on standard tumor sequencing assays. 166 Therefore, tumor analysis is not a replacement for germline testing, and confirmatory germline testing in the context of genetic counseling should be performed prior to further evaluation of a family. The potential to identify germline variants ideally should be considered when consenting patients for tumor sequencing.
Guidelines for the optimal approach to identify germline pathogenic variants based on somatic tissue analysis have been developed outside the specific context of thyroid cancer. For example, the NCCN Genetic/Familial High-Risk Assessment: Breast, Ovarian and Pancreatic Guideline states that a likely pathogenic variant or known pathogenic variant in PTEN detected by tumor profiling of any tumor type should prompt careful evaluation of personal and family history of the individual to determine the yield of germline sequencing. 127 If personal or family history consistent with PHTS is present, genetic counseling/testing should be offered. Furthermore, the European Society for Medical Oncology Precision Medicine Workgroup recommends focused germline testing for up to 40 genes if somatic mutations are identified in any tumor type, especially for seven genes deemed “most actionable,” which include BRCA1, BRCA2, MLH1, MSH2, MSH6, PALB2, and RET. This recommendation is based on a >5–10% tumor-to-germline conversion rate for variants with variant allele fractions >30% in a cohort of 49,264 cancer samples with paired sequencing data. Thyroid cancers constituted approximately 2% of this cohort. 167
Initial management of DTC
Shared decision-making between patients and their treating clinicians is paramount in determining the goals of initial therapy for patients with DTC. The preference of the patient must be considered when recommending the following, as appropriate:
In patients selected for thyroid surgery, the initial goal is to resect the primary tumor, any disease that has extended beyond the thyroid, and clinically significant lymph node metastases. Completeness of surgical resection is an important determinant of outcome, as lymph nodes represent the most common site (74%) of neck disease persistence/recurrence, followed by the thyroid remnant (20%) and the trachea and adjacent muscle (6%).
168
Consider which of the available multimodal treatment options is appropriate, to (a) decrease the risk of disease persistence/recurrence and metastatic spread and (b) minimize treatment-related morbidity. In addition to initial surgery, postoperative RAI administration, serum TSH suppression, and other management strategies may be appropriate in selected patients. However, it is important to balance the benefits and risks of the treatment(s), which may outweigh the burden imposed by the disease itself. Determine staging and risk stratification to estimate prognosis. Cancer staging is useful to estimate risks of disease-specific mortality, while initial risk stratification can be used to estimate short- and long-term risks of disease persistence/recurrence.
Does surgical experience influence complication rates for thyroidectomy?
▪
Due to lower complication rates and improved outcomes on average associated with high volume thyroid surgeons (>25–50 thyroidectomies/year), patients with thyroid cancer should be offered referral to a high-volume surgeon, particularly for tumors requiring more extensive surgery.
Physician experience and expertise have long been revered in patient care, but quantifying the benefits can be challenging, particularly at an individual provider level. There are many aspects of care where physician expertise is important in the diagnosis, staging, and management of patients with thyroid cancer, including sonography, pathology, surgery, endocrinology, nuclear medicine, oncology, and radiation therapy. Ultrasound of the neck is a prime example, due to its well-documented dependence on the skill and experience of the sonographer coupled with its importance for preoperative diagnosis, staging, and surveillance.169–173 The experience of the cytopathologist also has been demonstrated to improve the accuracy of ultrasound-guided FNA biopsy diagnosis 174 The evidence supporting improved outcomes at the hands of experienced surgeons is most compelling.
The relationship between thyroid surgery case volume and patient outcomes has been studied extensively during the past 20 years. In one of the first studies examining the relationship between surgeon volume and thyroidectomy outcomes, Sosa et al. 175 found a strong association between higher surgeon volume and favorable patient outcomes, especially with respect to recurrent laryngeal nerve injury and wound complications. This was most pronounced for patients undergoing total thyroidectomy for thyroid cancer. Others have made similar observations on a larger scale.176–179 In a study of the Health Care Utilization Project Nationwide Inpatient Sample (HCUP-NIS), 180 over 80% of thyroidectomies were performed by low- and intermediate-volume surgeons (≤29 thyroidectomies/year). On average, high-volume surgeons (≥30 thyroidectomies/year) had the lowest complication rates for patients who underwent total thyroidectomy for cancer (high 7.5% vs. intermediate 13.4% vs. low 18.9%; p < 0.001). A recent meta-analysis including 22 studies found unanimity in the association of lower complication rates with higher thyroid surgery volume. 181
When hospital volume and surgeon volume are both considered, on average, high-volume surgeons are associated with lower complication rates, lower hospital mortality, and lower cost, whereas high-volume centers are associated primarily with lower cost and shorter lengths of stay.181–183 Estimates of the annual thyroid surgical volume necessary to achieve lower complication rates range from 25 to 50,181,184–187 with one series suggesting >50 cases for more advanced thyroid cancer. 188 A study specifically designed to address this number concluded that annual total thyroidectomy case volume >25/year was associated with improved outcomes. Patients have an 87% increase in the odds of having a complication if the surgeon performed just 1 case/year, 68% for 2–5 cases/year, 42% for 6–10 cases/year, 22% for 11–15 cases/year, 10% for 16–20 cases/year, and 3% for 21–25 cases/year. 189 Patients undergoing total thyroidectomy for cancer at the hands of high-volume surgeons also are reported to have significantly less thyroid remnant tissue after resection, resulting in a reduced radioiodine dose requirement for remnant ablation (if indicated).188,190 Finally, patients having thyroid cancer surgery at low-volume centers were significantly more likely to have an involved tumor margin compared to those treated at high-volume centers. 191 An overwhelming body of evidence demonstrates improved outcomes for patients undergoing thyroid cancer surgery with higher-volume surgeons.
Referral of patients to high-volume thyroid surgeons is associated with, on average, superior outcomes. However, referral is not always possible, in view of the relative scarcity of high-volume surgeons and their geographic concentration in larger urban areas. Conclusions at an overall population level cannot always be applied to individual surgeons and patient circumstances. It seems reasonable to encourage referral of patients with grossly invasive and/or extensive disease to a high-volume surgeon experienced in the management of advanced thyroid cancer, and perhaps even to refer those patients undergoing total thyroidectomy for low- to intermediate-risk cancers.
It is important to recognize that even high-volume surgeons have a higher overall postoperative complication rate when performing total thyroidectomy (when compared with lobectomy). 192 In the HCUP-NIS study, high-volume thyroid surgeons had a complication rate of 7.6% following thyroid lobectomy compared with a rate of 14.5% following total thyroidectomy. For low-volume surgeons, the complication rates were 11.8% and 24.1%, respectively. 192 Older patients with thyroid cancer generally have a worse prognosis and higher rates of complications than younger patients; therefore, they may benefit from referral. Decision-making regarding extent of surgery, role of radioiodine therapy, and referral to high-volume surgeons or centers for thyroid cancer has many facets, and patient preference is an important component.193–198
What is the role of preoperative staging with diagnostic imaging and laboratory tests?
▪
Preoperative neck ultrasound to evaluate cervical lymph nodes in the central and lateral neck compartments as well as for gross extrathyroidal extension is recommended for all patients undergoing surgery for malignant cytologic or molecular findings. ( Ultrasound-guided FNA of sonographically suspicious lymph nodes greater than 8–10 mm in the smallest diameter should be performed to confirm malignancy if this would change management. ( The addition of FNA-Tg washout in the evaluation of suspicious cervical lymph nodes may be performed in select preoperative patients, but interpretation may be difficult in patients with an intact thyroid gland.
DTC (and particularly PTC) involves cervical lymph nodes in 20–50% of patients in most series using standard pathological techniques,199–203 and these metastases may be present even when the primary tumor is small and intrathyroidal. 204 The frequency of micrometastases (less than 2 mm) may approach 90%, depending on the sensitivity of the detection method.205,206 However, the clinical implications of micrometastases are likely less significant compared with macrometastases, and they do not appear to affect survival 207 ; when they are in the central neck, they also do not appear to increase recurrence. 208 Preoperative ultrasound identifies suspicious cervical adenopathy in 20–31% of cases, potentially altering the surgical approach209,210 in as many as 20% of patients.211–213 It has significantly less clinical utility in identifying central neck lymph nodes due to the presence of the overlying thyroid gland. 214
Sonographic features suggestive of abnormal metastatic lymph nodes include enlargement, loss of the fatty hilum (odds ratio [OR] 1.9), a rounded rather than oval shape (long axis/short axis ≤2; OR 1.6), hyper-echogenicity (OR 5.4), cystic change (OR 71.8), calcifications (OR 6.2), and peripheral vascularity or abnormal blood flow (OR 3.8). 215 No single sonographic feature has adequate sensitivity for detecting lymph nodes with metastatic thyroid cancer; however, cystic change has the highest odds of malignancy. 215 Absence of a fatty hilum, cystic changes, microcalcifications, abnormal vascularity, and cortical hyper-echogenicity are all independent features of metastatic lymph nodes with a high specificity of 87–99.6%. Absence of a fatty hilum has the highest sensitivity but low specificity at 66.4%. 216
The location of the lymph nodes also may be useful for decision-making. Figure 3 illustrates the delineation of Levels I through VI cervical lymph nodes. Metastatic lymph nodes are much more likely to occur in Levels III, IV, and VI than in Level II,214,217 although this may not be true for PTC tumors arising in the upper pole of the thyroid, which have a higher propensity to produce skip metastases to Levels II and III.
218
Confirmation of malignancy in lymph nodes with a suspicious sonographic appearance is achieved by ultrasound-guided FNA aspiration for cytology and/or measurement of Tg in the needle washout (FNA-Tg). Tg washout is a helpful adjunct to FNA, particularly in cases where the lymph nodes are cystic, cytological evaluation of the lymph node is inadequate, or the cytological and sonographic evaluations disagree (e.g., normal cytological biopsy of a large lymph node with microcalcifications).
219
False positive Tg washout may occur, particularly in lymph nodes in the central compartment when the thyroid gland is still present,220,221 but it remains valid in the presence of positive serum TgAb.
Data are limited to support a definitive FNA-Tg threshold for diagnosis of a metastatic lymph node. A systematic review and meta-analysis showed that FNA cytology with FNA-Tg washout has a negative predictive value (NPV) of 99.4% and accuracy of 86.8% in the evaluation of pathological-appearing lymph nodes. 222 If the FNA-Tg level is 1.0 ng/mL or lower, then the NPV approximates 100%. However, non-metastatic lymph nodes can have concentrations as high as 32 ng/mL Accuracy, specificity, positive predictive value (PPV), and NPV are significantly higher if the FNA-Tg threshold is 28.5 ng/mL. 222 Another systematic review analyzed 22 studies with 2,670 suspicious lymph nodes during thyroid nodule workup or PTC follow-up and found that the highest sensitivity was observed with a FNA-Tg cut-off of 1 ng/mL and the highest specificity was observed with a cutoff of 40 ng/mL. In this study, other factors that influenced the accuracy of FNA-Tg included TSH suppression, presence of serum Tg, and methodologic differences in Tg measurement. 223 Another study found the presence of serum TgAb interferes with circulating serum Tg measurement but does not appear to interfere with FNA-Tg measurements.224–226 Further studies are needed to determine an optimal FNA-Tg threshold to diagnose metastatic lymph nodes. 222
In addition to assessing for pathological lymph nodes, ultrasound evaluation of the thyroid gland to gauge gross extrathyroidal extension is important for surgical planning, as this typically demonstrates indication for RAI and therefore total thyroidectomy. 227 If there is evidence of more advanced locoregional disease, additional imaging with computed tomography (CT) may be useful. While ultrasound is more specific for nodal disease, CT is more sensitive, and the combination of both may increase diagnostic accuracy.228,229 In view of the higher cost of CT compared with ultrasound, the associated radiation exposure, and potential risks of intravenous contrast administration in specific populations, it is important to determine the imaging needs on an individual patient basis.
Accurate staging is important for determining the prognosis and tailoring treatment for patients with DTC. However, unlike many tumor types, the presence of metastatic disease does not obviate the need for thyroidectomy. 230 Because distant metastatic disease may respond to RAI therapy, removal of the thyroid as well as the primary tumor and accessible loco-regional disease is an important component of initial treatment for most patients with distant metastatic disease.
When should preoperative cross-sectional or 18F-fluorodeoxyglucose-PET imaging be performed?
▪
Preoperative use of cross-sectional imaging studies (CT, magnetic resonance imaging [MRI]) of the neck and mediastinum with intravenous contrast is recommended as an adjunct to physical examination and ultrasound for patients with clinical suspicion for advanced or invasive disease, including primary tumors with gross extrathyroidal extension, extensive (e.g. bulky or invasive) adenopathy, or disease concerning for aerodigestive tract and/or thoracic involvement Performing preoperative cross-sectional imaging of the chest, abdomen, and pelvis in search for distant metastases is recommended in situations when results will influence extent of surgery. Routine preoperative 18F-fluorodeoxyglucose (FDG)-PET/CT is not recommended prior to surgery. (
Since ultrasound evaluation is operator-dependent and cannot always adequately image deep anatomical structures or those acoustically shadowed by bone or air, alternative imaging procedures may be preferable or useful adjuncts in some clinical settings. Patients displaying bulky or widely distributed nodal disease on initial ultrasound may have nodal regions involved beyond typical cervical stations (some of which may be difficult to evaluate by ultrasound, including the mediastinum, infra-clavicular, retropharyngeal, and parapharyngeal regions).
In a systematic review and meta-analysis of 6378 patients with thyroid cancer assessing the diagnostic performance of CT in the detection of metastatic cervical lymph nodes, the pooled sensitivity was 55%, and the pooled specificity was 87%; however, there was considerable variation based on different CT protocols. 231 A meta-analysis of ultrasound and CT diagnosis with 5656 patients with thyroid cancer showed that CT had a higher sensitivity than ultrasound for assessment of cervical lymph nodes in the central and lateral compartments but that ultrasound has a higher specificity. Neither modality performed well in the central compartment (sensitivity of CT 40% vs. 28% for ultrasound). 228 While ultrasound had a higher specificity, the addition of CT reduces the rate of missed disease and improves surgical planning. 228
MRI does not entail exposure to ionizing radiation, and its contrast agents are less nephrotoxic than those employed in CT scanning. However, MRI is more subject to motion artifacts during the scan, though there have been recent advances in rapid acquisition of MRI images. In a meta-analysis of 504 patients with thyroid cancers, the pooled sensitivity of MRI for the diagnosis of metastatic cervical nodes was 80% and the specificity was 85%, but there was considerable heterogeneity, here reflecting fat-suppressed imaging and analytic techniques. 232 CT and MRI with intravenous (IV) contrast probably perform comparably in the detection of cervical nodal disease.
When cross-sectional imaging is performed, use of IV contrast is important, as it helps to delineate the anatomical relationship between the primary tumor or metastatic disease and other structures. If a retroesophageal innominate artery is identified, a right nonrecurrent laryngeal nerve should be suspected. Iodine is cleared within 4–6 weeks in most patients, so concern about iodine burden from IV contrast causing a clinically significant delay in subsequent whole body scans or RAI treatment after preoperative imaging is unfounded for most patients.233–235 The benefit gained from improved anatomical imaging almost invariably outweighs any potential risk of deferring RAI imaging or therapy. When there is a clearance concern, a spot urinary iodine level can be measured.
18Fluorodeoxyglucose positron emission tomography (18FDG-PET) has been employed preoperatively for lymph node staging. However, a meta-analysis of 759 patients with thyroid cancer showed a pooled sensitivity of only 30% despite a high specificity of 94%. 236 The findings are reinforced by a network meta-analysis of 3571 patients from 19 direct comparison studies using two or more different imaging modalities (ultrasound, CT,18FDG-PET, or 18FDG-PET/CT). 237 This showed that the imaging studies afford comparable detection of lymph node metastases. For all lymph node levels, ultrasound is superior in terms of PPV, NPV, and accuracy. Sensitivity and specificity of the three modalities vary when considering the lateral neck nodes, central compartment, and all lymph node levels, but none is significantly superior to ultrasound. Therefore, 18FDG-PET or 18FDG-PET/CT should not regularly be undertaken prior to initial treatment.
Locally invasive DTC has been reported to occur in 10–15% of patients at the time of diagnosis.238,239 For this group of patients, if suspected preoperatively, cross-sectional imaging can be useful for surgical planning to delineate the extent of laryngeal, tracheal, esophageal, or vascular involvement.240,241 Prior to resection, tracheoscopy and/or esophagoscopy, with/out ultrasonography, looking for evidence of intraluminal extension also may be helpful in cases of suspected aerodigestive tract invasion.
Locally invasive primary cancers may be associated with characteristic signs and symptoms, including rapid tumor enlargement, vocal cord paralysis, tumor fixation to the airway or neck structures, progressive dysphagia, respiratory compromise, hemoptysis, and significant voice change. Sonographic features of the primary tumor, including extrathyroidal extension (especially with posterior capsular penetration and disease reaching the mediastinum), also may prompt axial imaging. Chest CT can be useful in defining the inferior border of disease (and determining the extent to which mediastinal structures are involved) in cases with significant caudal spread. CT findings may influence management by suggesting the uncommon need for sternotomy and/or tracheal or laryngeal resection/reconstruction, which often would require assembling additional resources and personnel in preparation for the operation. Neck CT or MRI with contrast may define the extent of laryngeal, tracheal, and/or esophageal involvement in tumors displaying aggressive local invasion, as well as delineating bulky lymphadenopathy with clinical extranodal extension that involves adjacent structures. Preoperative appreciation of these features of the primary tumor or metastases has the potential to influence the surgical plan. 241
Should a serum Tg level be measured prior to surgery?
▪
Routine preoperative measurement of serum Tg or TgAb levels is not recommended.
Data from a systematic review and meta-analysis suggested that high preoperative concentrations of serum Tg may predict a higher sensitivity for postoperative surveillance with serum Tg. 242 In a prospective, observational study of patients undergoing total thyroidectomy, preoperative serum Tg was not a significant predictor of malignancy 243 Similarly, in a retrospective review of 131 patients who underwent surgery for benign multinodular goiter or indeterminate thyroid nodules, Tg levels did not significantly differ between those proving to have benign and malignant histologies 244 In contrast, Scheffler and co-workers reported that the addition of preoperative serum Tg to the McGill Thyroid Nodule Score for Well-Differentiated Thyroid Cancer improved its sensitivity in predicting malignancy in thyroid nodules. 245
A related issue is whether preoperative Tg levels can predict the extent of disease in patients with a preoperative diagnosis of thyroid cancer. Kim et al. performed a retrospective review of 4029 DTC cases between 1994 and 2006. 246 They report a linear association between preoperative Tg level and size of primary tumor and number of lymph node metastasis, with a threshold of 13.15 ng/mL as a predictor of ipsilateral lateral lymph node metastasis, 30.05 ng/mL for contralateral lateral lymph node metastasis, and 62.9 for distant metastasis. However, in a retrospective review of 422 patients with thyroid cancer who had preoperative Tg levels, Patell and co-workers found that while preoperative Tg was significantly correlated with size of the gland and T category, it did not correlate with presence of metastasis and was of low utility in the preoperative evaluation of thyroid cancer. 247
While the presence of TgAbs preoperatively do not appear to be an independent preoperative predictor of stage in patients with DTC, evidence is limited. In a cross-sectional analysis of 1770 patients with perioperative TgAb level data in the National Thyroid Cancer Treatment Cooperative Study (NTCTC, a thyroid cancer registry that included 11 North American centers and enrolled patients between 1987 and 2011), serum TgAb status was not significantly associated with the stage of disease on multivariable analysis, nor was it associated with disease-free or overall survival on univariate or multivariable analyses. 248
Should preoperative somatic genomic testing be performed to inform the extent of surgery?
▪
Genomic evaluation of confirmed DTC prior to surgery is not recommended routinely. However, if the genomic profile is known or performed, the presence or absence of specific combinations of abnormalities may be considered in the context of clinical, radiographical, and cytopathologic data to inform extent of surgery.
Several groups have studied whether incorporation of molecular results using different preoperative tests might have a role in guiding surgical planning for preoperatively defined thyroid cancers. The basis for these studies is summarized in
Several molecular tests have been developed to improve diagnostic accuracy of thyroid nodule FNA cytology. These approaches have been studied to determine if they can predict tumor behavior to guide preoperative surgical planning.257,266–269 Categories (low-, intermediate-, and high-risk) have been developed based on clinical outcomes on retrospective analyses.267–269 In these studies, patients with high-risk molecular profiles had more extensive initial surgery, larger cancers, a higher frequency of nodal metastasis, and vascular invasion as well as shorter recurrence-free survival than those with low-risk molecular profiles. Features included in the low-risk categories included RAS and RAS-like mutations (i.e., BRAFK601E, PAX8/PPARγ fusions), intermediate risk categories including BRAF-like alterations (i.e., BRAFV600E, NTRK3 fusions, and RET fusions), and high-risk categories including TERT promoter, TP53, AKT1, and PIK3CA mutations.
One study 269 retrospectively reviewed patients who underwent total thyroidectomy for DTCs between 1 and 4 cm without nodal disease and reviewed available molecular testing results grouped into low-risk (RAS and RAS-like alterations and gene expressions) or intermediate risk (BRAF-like alterations and gene expressions and copy number alterations). T3a tumors were excluded, while T3b and T4 <4 cm were included. Molecular results in the high-risk category were excluded, as the assay used to assess high-risk genomic features was not available at the time that many in the cohort were tested. In multivariable analysis, both intermediate-risk and low-risk molecular categories predicted recurrence, as did pN1a disease. Because preoperative ultrasound was not included in the analysis, and molecular testing was not performed in consecutive patients, but rather in those selected by their treating clinicians, it is not possible to directly correlate preoperative clinical findings with molecular markers. Few patients in the cohort underwent lobectomy, none of whom recurred, making it impossible to compare outcomes from total thyroidectomy versus lobectomy by molecular assessment. In this same cohort, the association between molecular classification and recurrence was compared with the 2015 postoperative ATA risk stratification system. In this analysis, the preoperative molecular associations were like those of the 2015 postoperative ATA Risk of Recurrence. 270 Another study approach has been to categorize tumors by their BRAF and RAS-like expression profiles. 266 When retrospectively analyzed, the BRAF-like tumors were more associated with extrathyroidal extension, lymph node metastases, and multifocality.
In addition to identifying patients who might benefit from total thyroidectomy based on high-risk molecular testing, it also has been suggested that patients with low-risk molecular results might be selected for lobectomy. One group reported on 685 consecutive patients who underwent surgery for PTC of which 78.5% had a BRAFV600E mutation and 19.4% had a TERT promoter mutation. 252 Patients with TERT promoter mutations had worse outcomes than those who did not. Isolated BRAFV600E mutations did not impact outcome. In those who were TERT promoter mutation-negative, there was no difference in 10-year disease-free or cancer-specific survival among patients with intrathyroidal tumors 1–4 cm. In another retrospective study tumors were categorized by molecular risk profiles on testing performed preoperatively in clinically selected patients. 269 DTCs in the intermediate molecular risk category were more likely to recur than those in the low-risk category (7.2% vs. 0.7%, retrospectively). Recurrence rates for the intermediate-risk group were influenced by tumor size. Patients with tumors >2 and <4 cm recurred more frequently than those with tumors between 1 and 2 cm. Recurrence was low at 3.8% for the entire cohort. Because most patients underwent total thyroidectomy (85.6%), it is not possible to know if extent of surgery would have impacted outcomes.
Several retrospective studies assessing a possible role for molecular testing among patients being considered for active surveillance (T1a PTC) have conflicting results.253,271 Thus, there are insufficient data to support use of molecular testing to stratify the approach for patients with T1a PTC.
The potential application of molecular testing for preoperatively defined DTC to individualize initial therapy may be particularly relevant for select patients with cT2N0 DTC for whom extent of surgery is not clear after consideration of clinical and radiographical features, and patient preferences (see
Are there patients in whom active surveillance and percutaneous ablation are appropriate management options?
▪
Active surveillance may be offered as an appropriate management option for some patients with cT1aN0M0 PTCs. Shared clinical decision-making between the patient and clinical team regarding risks and benefits of this approach is essential. Ultrasound-guided percutaneous ablation may be considered as an alternative to active surveillance or resection for cT1aN0M0 PTC in selected patients. Shared clinical decision-making between the patient and clinical team regarding risks and benefits of this approach is essential.
Active surveillance
FNA is not routinely recommended for thyroid nodules ≤1 cm with low-risk features. However, if thyroid cancer is diagnosed in a tumor ≤1 cm by FNA, active surveillance is an acceptable management option in selected patients. A systematic review published by a subgroup of this guidelines task force reviewed the published literature regarding active surveillance versus immediate resection and found low-certainty evidence that in adults with small, low-risk DTC, active surveillance and immediate resection are associated with similar, low risk of all-cause or cancer-specific mortality, distant metastasis, and recurrence after thyroidectomy.15,202,272–290 In patients managed with active surveillance, rates of tumor growth were low. Data on harms were limited, but temporary vocal fold paralysis and hypoparathyroidism were complications from thyroid surgery.
15
Rates of later surgery varied and were driven more by patient choice than signs of progression. Evidence regarding QoL or functional outcomes also was limited but indicated small or no differences. Cohort studies found that surgery was associated with improved all-cause or thyroid cancer mortality, but findings were potentially influenced by patient age, tumor risk category, and eligibility for, and actual receipt of, active surveillance.291–294
TSH goals in the setting of active surveillance are discussed in
There are limited data on the role of active surveillance in cancers >1 cm, as most of the existing studies have focused on enrollment for tumor sizes ≤1 cm.202,272–298 One study evaluated 77 patients with tumor size ≤1.2 cm who underwent active surveillance and 18 who underwent immediate operation. Of the patients undergoing active surveillance, only one had progression of disease requiring surgery after 30 months of follow up; in that case, tumor growth was associated with suspicion of extrathyroidal invasion. 279 A study that included 392 patients with tumors ≤2 cm (T1bN0M0) found that only 61 (16%) of the patients with tumors ≤2 cm selected active surveillance as management over immediate surgery, whereas 360 (89%) of those with tumor size ≤1 cm chose active surveillance. During a mean follow-up of 7.4 years (range 0.5–25 years), no significant difference was seen in the tumor progression of patients with tumor sizes ≤1 cm versus ≤2 cm; however, the cohort was small, and there was a risk of selection bias. 280 More recently, a prospective, nonrandomized controlled trial of 222 patients with Bethesda V and VI nodules that were ≤2 cm over a mean follow-up of 37.1 months found equivalent disease-specific and overall survival. 299 Of the 112 patients who underwent active surveillance, 90% continued, 41% experienced tumor shrinkage, and none developed regional/distant metastases. Size growth of >5 mm was observed in 4% of those undergoing active surveillance, and volumetric growth of >100% was seen in 7%.
Determining which patients are candidates for active surveillance involves shared decision-making among the patient, endocrinologist, surgeon, and other clinicians involved in the patient’s care. Some patients may not want active surveillance, whereas for others the benefit of avoiding surgical complications, which may be higher in some settings versus others, is a priority.300,301 In addition to patient preferences regarding surgery versus active surveillance, consideration should be given to the tumor and patient characteristics and the medical team’s ability to provide long-term observation. For patients considering an active surveillance approach, it is important that clinicians provide a description of the “unknown.” For example, the risk of tumors growing or de-differentiating over time could narrow the window of earlier effective treatment if they are not properly monitored. Practitioners should stress the critical need for long-term follow-up and how non-compliance with such follow-up invalidates claims for safety of this approach. 302 In this context, some patients may choose earlier treatment rather than active surveillance. Patients who have evidence of aggressive histology on review of cytopathology; patients with cancers that on imaging studies appear to invade the recurrent laryngeal nerve, trachea, or esophagus, or exhibit visible extrathyroidal extension; or regional or distant metastases are not candidates for active surveillance. Due to concern for tumor growth near critical local structures, active surveillance for cancers that abut the posterior capsule/trachea have been excluded from studies. Although this exclusion limits our ability to draw conclusions from existing data, it is reasonable to infer that active surveillance of posteriorly located tumors may be inappropriate due to the risk of invasion into vital structures.15,303 A cohort study from Japan (N = 1235, mean follow-up 75 months) suggested that older patients (i.e., patient age >60 years) with T1a PTCs may be better candidates for active surveillance because they are significantly less likely to experience tumor size increase of ≥3 mm, new lymph node metastases, or new clinical disease compared to young adults (age <40 years). 273
Percutaneous ablation
Thermal ablation using radiofrequency (RFA), microwave (MWA), and laser (LA) and ethanol ablation have been studied as primary treatment of low-risk PTC in carefully selected patients. Selection criteria are similar to those employed for active surveillance. Patients who are uncomfortable with active surveillance or with surgery may prefer a percutaneous ultrasound-guided ablative treatment for their cancer. Compared with lobectomy, ablation has a lower likelihood of resultant hypothyroidism, but it affords less certainty of complete tumor eradication, and it does not permit histopathologic evaluation.304–306 A meta-analysis on the subject included 11 studies involving 715 patients from Asia, with significant heterogeneity between the studies. 307 The pooled rate of complete tumor disappearance was 57.6% [confidence interval (CI) 35–80%] with a pooled recurrence rate of 0.4% [CI 0.0–1.1%]. Complication rates were 3.2% overall and 0.7% for major events, the latter of which consisted mostly of temporary voice changes. Subset analysis comparing modalities revealed no significant difference in rates of complete tumor disappearance (p = 0.35) or complications; however, there was a significant difference in volume reduction rates (RFA 99%, MWA 95%, and LA 89%, p < 0.001). 299
Another more recent meta-analysis of thermal ablation for cT1N0M0 included 36 studies with a pooled complete tumor disappearance rate of 91% [CI 83–97%] for cT1a and 60% [CI 50–70%] for cT1b carcinomas using RFA. 308 The local recurrence rates were 2–3% with nodal metastasis rates of 1–2%, across three thermal ablation techniques (RFA, LA, and MWA). Minor complication rates varied from 3% to 13%, and major complications were not reported. Comparisons of effectiveness between techniques were difficult to perform due to potential different tumor sizes. 308
A single-institution, prospective study of RFA for low-risk cT1a PTC included 98 tumors in 92 patients with complete tumor disappearance in 42% at 6 months and 96% at 1 year. At 18 months, no recurrences or nodal metastases were identified. 309 Another single-institution, retrospective study with at least 5 years of follow-up from RFA for cT1a PTC, including 84 nodules in 74 patients, found 99% and 100% complete tumor disappearance rates at 2 and 5 years.310–312 Fifteen percent of nodules required repeat RFA. 310 Four additional cancers developed in three patients; they were successfully ablated, and no patients developed metastases. The major complication rate was 1.4%.
A larger retrospective study of 414 patients with low-risk, unifocal cT1a PTC treated with RFA found a complete tumor disappearance rate of 88%, with 3% of patients requiring additional ablation. 313 The overall rate of local tumor progression was 4%. Local recurrence occurred in 2.4% of patients, and 1% developed nodal metastasis with an average follow-up of 3.5 years (range 2–5 years). No life-threatening complications were observed.
A single-institution, retrospective cohort study of 1613 individuals with PTC ≤2 cm treated with RFA had a median follow-up of 58.5 months. 314 During this follow-up, local tumor progression was observed in 69 of 1613 (4.3%) patients, tumor recurrence occurred in 42 (2.6%) patients, and persistence occurred in 27 (1.7%) patients. Mean time after RFA to development of local tumor progression was 21.5 months. The disease-free survival rate differed based on tumor size (T1a vs. T1b), number of tumors (unifocal vs. multifocal), and subcapsular tumor location distance from the capsule or trachea (≤2 mm or >2 mm).
Yan et al. retrospectively evaluated RFA for patients with unifocal (n = 432) versus multifocal (n = 55) cT1a PTC and found no significant differences in outcomes between the two groups with a mean follow-up of 4 years. Complete disappearance rates were reported as 89% versus 96% (p = 0.2). There were no significant differences between the two groups in rates of local progression, nodal metastasis rates, local recurrence, disease persistence, and recurrence-free survival. 315 However, another study demonstrated better outcomes for unifocal versus multifocal PTC with RFA (hazard ratio [HR] 0.5, p < 0.001), as well as for T1a versus T1b PTC (HR 0.4, p < 0.001). 314
Yang et al. reported retrospective results evaluating RFA for cT1a PTC in 91 patients with tumors adjacent to the tracheoesophageal groove and anticipated location of recurrent laryngeal nerve (“danger triangle”) and found no significant difference in complete tumor disappearance rates between those located near or away from that region (74% vs. 78%, p = 0.5) with no difference in disease progression (2% vs. 2%, p = 0.99) and no significant difference in complications (3.3% vs. 1.7%, p = 0.65) but may have been underpowered to show a difference. 316
A retrospective study of MWA for multifocal, cT1a PTC in 66 patients with 158 tumors and 5 years of follow-up found complete tumor resolution in all lesions with tumor progression in 3%, nodal metastases in one patient, and development of a new cancer in another. Repeat MWA was successful, and the complication rate was 3%. 317
Retrospective results using ultrasound-guided percutaneous ethanol ablation for cT1aN0M0 papillary thyroid cancer were reported from a single center involving 15 patients with 17 tumors utilizing injections on two successive days. Forty-seven percent of cancers completely resolved with median tumor volume reduction of 80–90%. No new cancers developed, and no nodal metastasis occurred with a median 5-year follow-up. 318
A retrospective study comparing individuals who underwent RFA versus surgery for unilateral multifocal papillary microcarcinoma with over a 5-year follow up period showed no statistically significant differences in disease progression (4.5% vs. 3.8%; p > 0.99), lymph node metastasis (2.3% vs. 3.8%; p > 0.99), persistent lesions (2.3% vs. 0%; p = 0.27) and RFS rates (97.7% vs. 96.2%; p = 0.67). 312 The data suggest that percutaneous ablation may represent an alternative to active surveillance or resection in selected patients. Additional studies are needed to assess widespread applicability, 304 particularly given that many of the referenced studies are subgroup analyses from a single group.309,312–315
What is the optimal approach for patients undergoing active surveillance?
▪
For patients undergoing active surveillance, neck ultrasound should be used to monitor disease progression. (
It is important that members of the medical team offering active surveillance have experience and confidence in their use of neck ultrasound. 171 Neck ultrasound, assessing the thyroid gland and all cervical lymph node compartments, is key to monitoring for cancer progression. Based on prior studies addressing active surveillance, neck ultrasound should be performed every 6 months for 1–2 years and then annually.202,273,274,290 The length of necessary follow-up remains unknown. None of the prior studies on active surveillance used neck CT for routine follow-up.
Should serum Tg and TgAb levels be measured during active surveillance?
▪
For patients undergoing active surveillance, routine measurement of serum Tg and/or TgAb levels is not recommended.
Data are lacking on the role of serum Tg levels when the entire thyroid is intact, as is the case during active surveillance. Since there is no clear role for measuring serum Tg levels preoperatively or postoperatively after lobectomy for thyroid cancer monitoring
Are there clear indications for when patients undergoing active surveillance should pursue resection?
▪
In patients undergoing active surveillance, surgical resection is indicated if there is evidence of new biopsy-proven lymph node metastases, growth of the primary tumor by ≥3 mm, distant metastases, evidence of extrathyroidal extension, posterior growth, when there is patient anxiety, inability to follow-up, and/or expressed preference for surgery. (
Since patients with regional or distant metastases would not routinely be candidates for active surveillance, initial or follow-up surgical consultation is indicated when patients who are undergoing active surveillance develop new (not previously observed), biopsy-proven lymph node metastases, ultrasound evidence of extrathyroidal extension, or distant metastases. Since surgical timing is relevant, discussion with their surgeon would be appropriate for patients considering active surveillance, particularly those with tumor adjacent to, but not invading, the recurrent laryngeal nerve, trachea, or esophagus. Invasion into the recurrent laryngeal nerve, trachea, or esophagus should prompt the patient to visit their surgeon, as patients with cancers with these features would not be appropriate for active surveillance.
Based on prior studies, prompt initial or follow-up consultation with the involved thyroid surgeon is indicated if there is clinically significant increase in tumor size described as cancer growth by ≥3 mm in any dimension.274,280,290 Patient preference for pursuing surgery after a period of active surveillance, as well as the patient’s inability to follow-up regularly for monitoring (risk of non-compliance), also are appropriate indications for another consultation with their surgeon.
What is the optimal operative approach for DTC?
▪
When resection is performed for patients with thyroid cancer ≤2 cm without gross extra-thyroidal extension (cT1) and without metastases (cN0M0), the initial surgical procedure should be a thyroid lobectomy unless there are bilateral cancers or other indications to remove the contralateral lobe. ( For patients with low risk, unilateral thyroid cancer >2 and ≤4 cm (cT2N0M0), thyroid lobectomy may be the preferred initial surgical treatment due to significantly lower risk and side effects. However, the patient and treatment team may adopt total thyroidectomy to enable RAI administration and/or enhance follow-up based on disease features, suspicious contralateral nodularity, and/or patient preferences. When thyroid lobectomy is offered as initial treatment, counsel the patient about the possibility of conversion to total thyroidectomy or need for subsequent completion thyroidectomy if higher-risk factors emerge intraoperatively or postoperatively. ( For patients with thyroid cancer >4 cm (cT3a), cancer of any size with gross extra-thyroidal extension (cT3b or cT4), or clinically apparent metastatic disease to lymph nodes (cN1) or distant sites (cM1), the initial surgical procedure should include a total thyroidectomy with gross removal of all primary tumor and node dissection unless there are contraindications to this procedure. (
A preoperative FNA biopsy diagnostic for DTC is almost always interpreted as conventional PTC based upon cytology (Bethesda VI), whereas IEFVPTC, FTC, and OTC more often fall into one of the indeterminate categories (Bethesda III, IV, or V). The identification of a BRAFV600E mutation or RET fusion on molecular testing of a thyroid nodule FNA sample, if performed, is diagnostic of PTC. Thus, in the absence of clinical features confirming malignancy with indeterminate cytology, the preoperative diagnosis of DTC typically involves classical PTC. Surgery for thyroid cancer is an important element of an often straightforward but potentially complex treatment approach, best coordinated preoperatively with a multidisciplinary team and reflecting patient desires. The operation should be compatible with the overall treatment strategy and follow-up plan recommended by the managing team, understood by the patient and respecting their personal preference(s). 319
Earlier ATA guidelines12,13 endorsed total thyroidectomy as the primary initial surgical treatment option for nearly all DTCs >1 cm with or without evidence of loco-regional or distant metastases, with lobectomy sufficient for unilateral T1a carcinomas (T1a PTC) without metastasis. The recommendation was based on data suggesting that for cancers >1 cm, a bilateral surgical procedure was associated with improved survival,
320
decreased recurrence rates,321–323
allowed routine use of RAI remnant,168,324 and facilitated detection of recurrent/persistent disease during follow-up. However, the 2015 ATA guidelines
14
suggested lobectomy as an alternative to total thyroidectomy for cT1b-T2N0M0, low risk, unilateral PTCs (particularly follicular variant) and FTCs. This change was based on data demonstrating that for properly selected patients, clinical outcomes are very similar following unilateral or bilateral thyroid surgery.325–330
There has been a trend away from routine use of RAI for remnant ablation (which requires total thyroidectomy), and there are higher rates of complications following total thyroidectomy versus thyroid lobectomy (see
Near total or total thyroidectomy is necessary if the overall strategy is to include RAI therapy post-operatively. Therefore, near-total or total thyroidectomy was recommended in prior ATA guidelines in situations where postoperative RAI therapy was recommended: that is, for primary DTCs >4 cm (cT3a), with gross extrathyroidal extension (cT3b or T4), and/or regional (cN1) or distant metastases (cM1). For tumors between 1 and 4 cm and without evidence of metastasis (cT1b-2, N0, M0), prior ATA guidelines suggested that patient age >45 years, contralateral thyroid nodules, a personal history of radiation therapy to the head and neck, or FNMTC might prompt recommendations for total thyroidectomy because of plans for RAI therapy, to facilitate follow-up strategies, or to address greater suspicion of bilateral disease.325,329,333,334 Ultrasound-guided FNA of significant/suspicious contralateral nodule(s) helped inform a recommendation for total thyroidectomy.
Since publication of the 2015 guidelines suggesting that thyroid lobectomy/hemi-thyroidectomy may be sufficient for low risk (cT1-2N0M0) DTC, numerous studies have been published evaluating this recommendation. Several systematic reviews and meta-analyses have been performed, with approximately half showing no difference in recurrence or survival but with higher complication rates for total thyroidectomy.335–337 The other approximate half demonstrate statistically significant, lower recurrence rates with total thyroidectomy compared with lobectomy alone.338–340 Only one meta-analysis found improved overall survival with total thyroidectomy over lobectomy, but the benefit was confined to T2 primary tumors. 340 This result is influenced by a National Cancer Database (NCDB) study analyzing PTC (1–4 cm, T1b-2) demonstrating significantly better survival with total thyroidectomy for classical PTC but not FVPTC; however, in subset analysis, this seemed to be true only for T2 (not T1b) classical variant PTC. 341 A recent narrative review of these studies and published guidelines concluded that lobectomy was sufficient for low-risk T1 tumors and that either lobectomy or total thyroidectomy would be reasonable treatment alternatives for low-risk T2 tumors. They recommended that patients with cT2N0M0 tumors should be informed that lobectomy has a significantly lower risk of complications and side effects but carries a slightly higher risk of locoregional recurrence and possibly reduced overall survival. 342 This conclusion was supported by another recent systematic, qualitative narrative review. 343 Most recurrences following lobectomy alone appear to occur in the contralateral lobe and are successfully salvaged with completion thyroidectomy.339,340 A Surveillance, Epidemiology and End Results (SEER) database study involving only FTC without extrathyroidal extension or metastasis (cT1a-T3aN0M0) found no difference in 15-year disease-specific survival between lobectomy and total thyroidectomy (98% vs. 97%, respectively), but it did not evaluate recurrence. 344 A large, single-institution study of minimally invasive FTC found patient age >55 years and tumor size >4 cm were both independently associated with higher 10-year risk of recurrence on multivariable analysis. 345 Results of single-institution studies of primarily PTC are mixed.346–353
A few studies have addressed the issue of multifocality with lobectomy versus total thyroidectomy for PTC <1cm (T1a). One found a significantly higher recurrence rate with lobectomy versus total thyroidectomy (26% vs. 5%, respectively), with lower disease-free survival at 5 and 10 years, particularly in male patients with a sum of all tumors >1 cm. 354 Another study found a higher recurrence rate for lobectomy in patients with PTC T1a tumors, with a higher rate of recurrence beyond the contralateral lobe in the presence of multifocality. 355 Additional studies looked specifically at pathologically node positive disease discovered in the central compartment at the time of lobectomy (cN0 but pN1a); one demonstrated no significant difference in recurrence-free survival at 15 years between total thyroidectomy and less than total thyroidectomy, 356 but the other showed a significantly lower recurrence rate but higher complication rate with total thyroidectomy compared with lobectomy, with no difference in recurrence if pN0. 357 A study examining the impact of minimal extra-thyroidal extension in T1N0 PTC tumors found no difference in recurrence rates between lobectomy and total thyroidectomy (3% vs. 2%, respectively). 358 A recent SEER database study of patients with unilateral T1a PTCs found no difference in overall or disease-specific survival between lobectomy and total thyroidectomy after propensity matching; a subset analysis revealed lower disease-specific survival for younger patients (<55 years) and those with multifocality and/or extrathyroidal extension treated with lobectomy alone. 359 Another database study involving a Chinese cohort suggested younger patients (<35 years) benefit from total thyroidectomy over lobectomy, and particularly for T3 (>4 cm) cancers. 360
Recent studies of intermediate-risk (see
Several retrospective studies have examined the estimated proportion of patients who might require completion thyroidectomy after initial lobectomy for clinically low-risk, unilateral, intrathyroidal, node-negative DTCs; estimates ranged greatly, from 5% to 43%366–369 of patients, which is similar to a meta-analysis estimate of 11–34%. 339 Two additional studies found a 21% rate of conversion to total thyroidectomy from lobectomy based on high risk findings identified intraoperatively and a 27–30% rate of completion thyroidectomy based on pathologically higher-risk findings.370,371 More important, one study that compared actual rates of initial total thyroidectomy versus lobectomy and rates of completion thyroidectomy after initial lobectomy (before and after publication and implementation of the 2015 ATA guidelines) found a reduction in the utilization of total thyroidectomy (from 61% to 31% of all initial operations) and also completion thyroidectomy (from 74% to 20%), suggesting that doing more lobectomies for lower-risk cancers does not result in a higher rate of completion thyroidectomy. 372 Several additional studies373–375 document increased use of lobectomy for cancer after publication of the 2015 ATA guidelines, as well as lower rates of completion thyroidectomy (from 50% to 25%).374,376 However, total thyroidectomy remains the more commonly performed initial operation (70–88%), even for cT1-2N0M0 cancers, despite significantly higher postoperative morbidity.373–375,377 Increasing primary tumor size from T1a-T1b to T2 was associated with increased utilization of initial total thyroidectomy 375 and completion thyroidectomy. 377 The one prospective study of lobectomy for T1a PTC found only a 3% conversion rate to total thyroidectomy due to higher risk intraoperative findings and a 20% salvage surgery rate, with resultant 99% disease-free survival (similar to a retrospective cohort treated with initial total thyroidectomy and central neck dissection). 378 Accurate preoperative ultrasound227,379 and targeted use of frozen section380–382 can help identify patients best treated with total thyroidectomy, reducing the need for subsequent completion thyroidectomy. Cost-effectiveness assessment found greater utility with lobectomy over total thyroidectomy for PTCs that are 1–4 cm (T1b-2N0M0).343,367
The risks of total thyroidectomy are significantly greater than those for thyroid lobectomy, with a meta-analysis suggesting a relative risk (RR) significantly greater for all complications, including recurrent laryngeal nerve injury (transient RR = 1.7, permanent RR = 1.9), hypocalcemia (transient RR = 10.7, permanent RR = 3.2), and hemorrhage/hematoma (RR = 2.6). 383 Total thyroidectomy is associated with the rare risk of bilateral recurrent laryngeal nerve injury necessitating tracheostomy. Surgeon experience likely influences the risks of thyroidectomy, with higher-volume surgeons having lower complication rates.175,176,178,384,385 However, as noted above, even high-volume surgeons still have a higher complication rate when performing total thyroidectomy versus lobectomy (14.5% vs. 7.6%, respectively), which is higher on average than the complication rate for lobectomy undertaken by low-volume surgeons (11.8%). Highest risk is associated with total thyroidectomy at the hands of a low-volume surgeon (24.1%). 192 Therefore, patients should carefully weigh the relative benefits and risks of total thyroidectomy versus thyroid lobectomy, even when the operation is performed by high-volume surgeons. Total thyroidectomy necessitates thyroid hormone replacement, while lobectomy is associated with postoperative biochemical hypothyroidism estimated on average to be 22%, with clinical or overt hypothyroidism estimated at 4%. 386
A significantly increased risk of hypothyroidism following lobectomy has been reported in the presence of autoimmune thyroid disease (e.g., as reflected by the presence of thyroid antibodies) or high normal/elevated preoperative TSH.383,386 Hypothyroidism is not an indication for thyroidectomy, and its use as justification for total thyroidectomy over lobectomy should be weighed against the other higher risks associated with total thyroidectomy. In contrast, coexistent hyperthyroidism may be an indication for total thyroidectomy, depending upon the etiology. Patients with high-normal TSH levels following lobectomy for cancer may still need thyroid hormone supplementation to reduce TSH levels into their target range (see TSH target section).387–395 Regardless, two recent studies confirm significantly better quality-of-life measures in patients undergoing lobectomy compared with total thyroidectomy for cancer.396,397 A third found this was only true for the first few months postoperatively, with no significant differences at 6–12 months. 398 A separate report found a decreased rate of chronic asthenia (generalized weakness) with lobectomy. 399
Preoperative somatic molecular testing and neoadjuvant therapy
Preoperative molecular testing obtained from FNA has been proposed to help determine extent of initial thyroid surgery in selected patients with cT1-cT2 cN0 DTC (see
In contrast, another study of 1–4 cm DTCs in which cT4, cN1, or cM1 disease were excluded (but included cT3b tumors) found no difference between lobectomy and total thyroidectomy in 10-year cause-specific survival for BRAF and/or TERT promoter-mutated tumors. 252 No patients died of their disease. Disease-free survival was not significantly better in patients with TERT promoter-mutated tumors (predominately also BRAF-mutated) treated with total thyroidectomy versus lobectomy (100% vs. 65%, p = 0.09). There was no difference in disease-free survival for patients whose tumors were TERT promoter-negative and predominantly BRAF mutation-positive treated with total thyroidectomy versus lobectomy (97% vs. 97%, p = NS). 252
Another retrospective study of 105 patients with PTC and Bethesda V or VI cytologies (85% Bethesda VI) found high-risk mutations in 6%, all of whom underwent total thyroidectomy and had T3b-4 and/or N1 and/or M1 disease. 400 An increased recurrence rate was observed for patients with high-risk molecular tumors versus low- and intermediate-genomic risk groups, although the number of patients in the high-risk group was small (n = 6). 400 Of the 19% of patients who underwent initial lobectomy, 21% underwent completion thyroidectomy based upon postoperative risk of recurrence assessment. None had a high-risk mutation, and no comparison between low- or intermediate-risk mutations was performed. 400
In summary, high-risk mutations appear to be uncommon in patients with cT1b-2N0M0 DTC. BRAFV600E and BRAFV600E-like mutations are common in these tumors, as most patients with Bethesda VI cytology have classical PTC. Because low-risk mutations (RAS-like) occur primarily in cytologically indeterminant (Bethesda III–V) nodules, data for these nodules may not be as applicable for patients with Bethesda VI cytology on preoperative FNA. Thus, routine use of molecular testing is not recommended for patients with these smaller intrathyroidal DTCs as prospective studies that included cost analyses have not yet been performed (see
For patients with large, locally invasive DTC in whom high-risk mutations are more common and a R0 or R1 resection is unlikely without high morbidity, use of systemic multi-kinase or targeted therapy with or without immunotherapy in the neoadjuvant setting has been reported. These reports thus far show variable results depending on the type and side effects of therapy.401,402 Results from larger prospective clinical trials are needed to determine for whom such a strategy may be appropriate to consider.
In view of the significantly lower risk of complications and better QoL with lobectomy in comparison to total thyroidectomy, and limited oncologic benefit of total thyroidectomy, it appears that lobectomy for low-risk DTC is the preferred initial operation when the primary tumor is clinically small, unilateral, intra-thyroidal, and without evidence of regional or distant metastasis. However, patients must be aware of a ≥20% possibility of conversion to total thyroidectomy intraoperatively, or subsequent completion thyroidectomy. Multifocality with clinically significant contralateral nodularity may make total thyroidectomy the preferred initial operation for some patients to reduce the risk of recurrence and need for additional surgery. Most recurrences in the setting of multifocality/contralateral nodularity can be successfully salvaged with completion thyroidectomy if the patient is compliant with sonographic surveillance. With appropriate follow-up, deferral of completion thyroidectomy has little to no impact on survival. Patients with larger cT2N0M0 classical PTC are also good candidates for lobectomy but may prefer to undergo total thyroidectomy and RAI postoperatively to possibly reduce their risk of recurrence and improve survival.340–343 Patients with clinically more advanced primary tumors (cT3-4), nodal involvement (cN1), and/or distant metastasis (cM1) are generally best treated with total thyroidectomy to facilitate RAI and biomarker surveillance (Table 5). Decisions regarding the extent of initial thyroidectomy should be part of a patient-centered, multidisciplinary treatment plan; patient preference serves as a very important component. Clinical risk factors such as age, male sex, family history of thyroid cancer, and/or history of radiation exposure may further influence decision-making regarding total thyroidectomy.
Extent of Initial Thyroid Surgery for DTC

Clinical stage based upon AJCC 8th edition.
If surgery chosen for initial therapy.
AJCC, American Joint Committee on Cancer.
When should completion thyroidectomy be performed?
▪
Completion thyroidectomy for cancer following initial lobectomy may be considered to address persistent primary malignancy, facilitate RAI administration, and/or enhance follow-up based upon higher estimated risk of recurrence identified postoperatively, accounting for recurrent laryngeal nerve function. Completion thyroidectomy for OTC may be considered based on indications like other histological types of DTC.
Completion thyroidectomy after initial lobectomy may be indicated when the diagnosis of DTC was not known preoperatively or recognized intraoperatively. However, most cytologically indeterminate cases that prove to be malignant on final histology are low-risk cancers adequately treated with lobectomy alone. When final histology reveals heightened risk factors for recurrence (see Pathology section and
Minimal/microscopic extrathyroidal extension no longer promotes tumors to T3 in the AJCC 8th edition staging system 418 and may not require completion thyroidectomy, particularly for T1 and small T2 unifocal tumors, 358 unless there is clinical concern for involvement of the nerve, trachea, or esophagus with involved posterior margins. 419 In contrast, gross extrathyroidal extension is associated with higher risk of recurrence354,397,420 and warrants conversion of lobectomy to total thyroidectomy, with complete tumor resection to grossly free margin. With uncertainty about whether there is extrathyroidal tumor extension into overlying strap musculature versus scarring from needle biopsy, leaving a cuff of sternothyroid muscle at the area of concern and deferring to final histology may be a more prudent approach than pursuing total thyroidectomy because minimal/microscopic extrathyroidal extension into strap musculature with a clearly negative margin does not mandate completion thyroidectomy. The microscopic histological finding of tumor transgressing the thyroid capsule and/or a microscopically positive margin (in the absence of clinical concern for extrathyroidal extension) does not mandate completion thyroidectomy, particularly if the finding is noted anteriorly.366,419,421,422
Microscopic, pathologically involved central compartment lymph nodes (cN0 but pN1a) identified incidentally after lobectomy or as part of ipsilateral central neck dissection may prompt completion thyroidectomy, but the procedure is not necessary for all patients.356,357,423 A larger number of nodes (more than three to five nodes),424–426 higher lymph node ratio (LNR, >0.3),426–428 or presence of extranodal extension429–431 suggests possible higher risk of recurrence and therefore potential benefit from completion thyroidectomy. Clinically evident nodal metastasis (cN1a) noted during lobectomy warrants conversion to total thyroidectomy with central lymph node dissection. Targeted frozen section of clinically suspicious nodes may aid intraoperative decision-making.380–382
Vascular invasion, particularly when extensive vascular invasion is identified in FTC or OTC, is associated with increased risk of distant metastasis432,433 and may warrant completion thyroidectomy. Vascular invasion in PTC is also associated with increased risk of distant metastasis and may warrant completion thyroidectomy.432,434
Some histological tumor variants also influence risk (see Pathology and Risk of Recurrence sections): minimally invasive FTC, OTC, and minimally invasive IEFVPTC generally have the lowest risk and would not typically warrant completion thyroidectomy in the absence of high-risk findings. In contrast, higher-risk variants of PTC (e.g., tall cell, hobnail, and solid variant and diffuse sclerosing) and widely invasive FTC, OTC, and PDTC (or a poorly differentiated component) are associated with higher risk of recurrence and may warrant completion thyroidectomy.
341
Noninvasive, encapsulated follicular variant of PTC, now known as NIFTP, is considered very low risk from a clinical perspective, and while it requires surgery for definitive diagnosis, it does not typically warrant completion thyroidectomy, although further data are needed, particularly for larger tumors (see
Clinical risk factors such as patient age, male sex, family history of thyroid cancer, and/or history of radiation exposure may influence decision-making regarding completion thyroidectomy. Patient preference is critical, and decisions always should be made by a patient-centered multidisciplinary clinical team informed by knowledge of recurrent laryngeal nerve function.
What is the surgical approach to thyroglossal duct carcinoma?
▪
Initial surgical therapy for thyroid carcinoma arising within a thyroglossal duct (TGDCa) should include complete tumor/cyst excision along with the central portion of the hyoid bone (Sistrunk procedure). A Sistrunk procedure and thyroidectomy may be considered for TGDCa with significant/suspicious thyroid nodularity to ensure complete resection of possible multicentric disease and/or for larger tumors, particularly in older patients, to facilitate RAI and/or enhance follow-up. A Sistrunk procedure and total thyroidectomy should be performed for TGDCa with evidence of more advanced disease (e.g., gross extension of tumor into surrounding tissues, nodal or distant metastasis).
When should completion thyroidectomy following Sistrunk procedure be performed?
▪
Completion (total) thyroidectomy may be considered following resection of TGDCa with higher-risk factors (similar to completion thyroidectomy after lobectomy) or that proves to be a metastasis to the Delphian/prelaryngeal lymph node(s). ( Completion thyroidectomy may be considered following resection of lower-risk TGDCa associated with significant/suspicious thyroid nodularity to ensure complete resection of possible multicentric disease, or for larger tumors, particularly in older patients, to facilitate RAI and/or enhance follow-up. (
The diagnosis of TGDCa arising in association within a TGD cyst should only be rendered upon presence of a TGD cyst remnant, which shows squamous/columnar epithelium lining cysts and ectopic thyroid tissue in the cyst wall. The cyst wall can be of variable thickness, and the carcinomatous component is usually solid and/or nodular. 435 Almost 50% of all thyroid glands exhibit a pyramidal lobe (a remnant of the inferior portion of a TGD), which extends superiorly from the isthmus 436 and can be connected to the hyoid bone with fibrous tissue. A carcinoma arising in the pyramidal lobe should be staged as usual. 435 The Delphian or prelaryngeal lymph node(s) is/are located anterior to the cricothyroid membrane and superior to the isthmus. This is a common site for nodal metastasis from PTCs arising in the isthmus. In some cases, the Delphian node(s) can be completely replaced by metastatic PTC with cystic degeneration, which may pose difficulties in distinguishing it from PTC arising in a TGD cyst.
Rather than devising a separate definition and/or staging system for this rare carcinoma, it seems reasonable to apply the current TNM staging system in view of studies demonstrating increased rates of recurrence with larger tumors, “extrathyroidal” extension of the primary tumor, nodal metastasis, and/or older patient age. For TGDCas diagnosed preoperatively and without sonographic evidence of tumor extension beyond the cyst, suspicious thyroid nodules, or suspicious lymph nodes, the Sistrunk437–439 procedure alone is a reasonable initial treatment option, especially for younger patients. Patients should understand the potential need for conversion to total thyroidectomy or subsequent completion thyroidectomy if high-risk factors are appreciated intra- or postoperatively.418–420,422,425,426 A Sistrunk procedure in concert with total thyroidectomy may be reasonable initial therapy when suspicious/significant thyroid nodularity is present or for older patients with larger tumors.420,421,427 When there is nodal involvement, a compartment-oriented central lymph node dissection should accompany a Sistrunk procedure and total thyroidectomy.440,441 Completion thyroidectomy following an initial Sistrunk procedure may be warranted when the diagnosis of TGDCa was not assigned preoperatively and significant/suspicious thyroid nodularity is present, to facilitate RAI administration and/or enhance follow-up in the presence of gross tumor extension into surrounding tissues, or other higher-risk features.
When should prophylactic central-compartment lymph node resection be performed?
▪
Prophylactic central-compartment lymph node dissection should not be performed for most small, noninvasive, clinically node-negative PTC (cT1-T2, cN0) and for most FTCs. Prophylactic central-compartment neck dissection may be considered in patients with PTC and clinically uninvolved lymph nodes (cN0) who have advanced primary tumors (T3 or T4) or for whom the information will be used to plan further steps in therapy, but this approach should be weighed against the risks as they evolve during thyroidectomy.
The value of prophylactic central lymph neck dissection (pCLND) for clinically N0 (cN0) DTC remains unproven. Chen and co-workers 442 performed a meta-analysis on this topic that included 23 retrospective and prospective cohort studies with a total of 18,376 patients. Locoregional recurrence occurred in 280 (2.52% of 11,098) patients in the pCLND group and 254 (4.59% of 5583) patients in the non-pCLND group. Patients who underwent pCLND had a significantly lower locoregional recurrence rate (OR 0.65 [CI 0.48–0.88]) but significantly higher rates of transient recurrent laryngeal nerve injury (OR 2.03 [CI 1.32–3.13]), transient (OR 2.23 [CI 1.84–2.70]), and permanent hypocalcemia (OR 2.22 [CI 1.58–3.13]) versus the non-pCLND group. In contrast, Lee and co-workers 428 in a study assessing rates of occult lymph node metastasis and risk of regional recurrence in PTC after bilateral CLND saw no association between occult lymph node metastasis and regional recurrence. They concluded that the LNR, which is the ratio of the number of malignant lymph nodes excised to the total number of excised lymph nodes that exceeds 0.26, was an independent predictor of regional lymph node recurrence, especially in the lateral neck. Wang and co-workers 443 performed a meta-analysis and reported an overall recurrence rate of 3.8% for patients undergoing total thyroidectomy plus pCLND [CI 2.3–5.8]. In the six comparative studies that included 1740 patients, 995 patients undergoing total thyroidectomy and 745 patients undergoing total thyroidectomy with pCLND, the overall recurrence rate was 7.6%: 7.9% in the total thyroidectomy group and 4.7% in the total thyroidectomy plus pCLND group. The RR of recurrence was 0.59 [CI 0.33–1.07], favoring a lower recurrence rate in the total thyroidectomy plus pCLND arm. They concluded that it would be necessary to treat 31 patients with pCLND to prevent a single recurrence. Hence, the benefits of pCLND should be weighed against the risks, especially when a surgeon’s experience is limited.
Overall, expectant management of the central compartment when a patient is deemed cN0 seems prudent. Hughes et al. 444 examined 14 studies and evaluated the effect of pCLND on locoregional recurrence. They found that it was 6.75% for total thyroidectomy alone versus 4.55% for total thyroidectomy and pCLND 445 and found that the 5-year recurrence-free survival and central neck recurrence-free survival rates were 96.6% and 99.1%, respectively. The authors concluded that observation of the central neck is safe and should be recommended for all patients with PTC thought before and during surgery to be free of central compartment metastasis. Zhao et al. 446 performed a meta-analysis that included 17 studies comprising 4437 patients. Although the total thyroidectomy with pCLND group had a significantly reduced risk of loco-regional recurrence (risk ratio = 0.66 [CI 0.49–0.90]; p = 0.008) when compared with total thyroidectomy alone, they received higher RAI doses (74.6% vs. 59.9%); experienced more temporary hypocalcemia (OR = 2.37 [CI 1.89–2.96]; p < 0.00001), permanent hypocalcemia (OR = 1.93 [CI 1.05–3.57]; p = 0.03), and increased overall morbidity (OR = 2.56 [CI 1.75–3.74]; p < 0.00001). All these studies suggest equipoise when considering a pCLND, especially with T3 and T4 tumors.
The role of pCLND for patients treated with lobectomy alone has not been extensively studied. Choi et al. reviewed their outcomes for thyroid lobectomy with prophylactic ipsilateral CLND for low-risk PTC. Nine hundred and six patients were reviewed, with 52 experiencing recurrences (5.7%) during 10 years of follow-up. Thirty-two (61.5%) patients experienced recurrence in the remaining thyroid lobe, 11 (21.2%) in a lymph node only, and 9 (17.3%) in both. The recurrence-free survival rates at 5 and 10 years were 97.1% and 81%, respectively. There was no comparison group, and future studies are needed to evaluate the utility of pCLND in this scenario.
What is the best approach for therapeutic central and lateral compartment node resections?
▪
Therapeutic central-compartment (Level VI and upper Level VII) neck dissection for patients with clinically involved central nodes (cN1a) should accompany thyroidectomy to clear disease from the central neck. Therapeutic CLND with dissection of the ipsilateral central compartment lymph nodes is recommended to accompany lateral-compartment neck dissection and thyroidectomy for patients with clinically involved lateral neck lymph nodes (cN1b). Therapeutic lateral neck compartmental lymph node dissection, typically including Levels IIa, III, IV and Vb, should be performed as part of initial surgical therapy for patients with biopsy-proven or clinically obvious metastatic lateral compartment cervical lymphadenopathy.
It is generally accepted that compartmental dissection of lymph nodes known or suspected to be involved with DTC provides a recurrence-free advantage. 14 In the central neck, a compartmental dissection of at least the prelaryngeal, pretracheal, and involved paratracheal lymph node areas should be performed. 32 Recognizing the limitations of imaging (and especially ultrasound in detecting lymph node metastases with the thyroid present) and the increased risks associated with central compartment dissection especially when the surgery is bilateral, the question of whether to dissect a cN0 contralateral paratracheal compartment is pertinent. Yeh et al. 241 highlighted that in the absence of bilateral primary tumors >1 cm, contralateral Level VI is less commonly affected (prevalence 5–25%). Qu et al. 447 performed a systematic review and meta-analysis of the clinical risk factors for central compartment lymph node metastasis in PTC. Three studies assessed the association between lateral versus the central compartment lymph node metastasis.448–450 Central compartment lymph node metastases were significantly more frequent among patients with lateral compartment disease (88.7% vs. 31.1%) overall, with an OR obtained through analysis of these three studies of 14.33 ([CI 5.34–38.50]; p < 0.001). Likhterov et al. 451 reported that of patients with lateral neck nodal metastases, only 5% had “skip” metastases, leading the authors to advocate for ipsilateral central compartment neck dissection when lateral neck nodes are involved. Decision-making reflecting the circumstances that evolve during an operation should be an underlying guiding principle when performing a central compartment neck dissection. For example, if the initial side of the thyroidectomy for the primary tumor and involved paratracheal lymph nodes results in an injured recurrent laryngeal nerve and/or compromised parathyroid glands, it would be prudent to avoid the contralateral paratracheal compartmental dissection when it is cN0 to minimize the risk of possible bilateral vocal fold paralysis and hypoparathyroidism.
Miller et al. 452 demonstrated that half of residual lymph node metastases are due to failure to recognize the extent of nodal involvement preoperatively, while the other half result from incomplete nodal dissection. Improvements in nodal imaging protocols and standardization of nodal dissection technique with adherence to formal compartmental nodal dissections should reduce the risk of persistent disease and the need for further treatment. Consideration of removing lymph nodes along the transverse cervical artery and vein, the superior thyroid artery and vein, and behind the head of the clavicle when performing a lateral neck dissection will help reduce the risk of recurrence in these regions.
The concept of lymph node yield (LNY), the total number of excised lymph nodes (whether benign or malignant) examined, to determine adequacy of the nodal dissection and how it relates to prognosis may further support formal compartmental nodal dissections. LNY is relevant to risk of recurrence in many other malignancies. Robinson et al. 453 reviewed the NCDB (1998–2012) to characterize the distribution of involved lymph nodes among adult patients diagnosed with localized ≥1 cm PTC who underwent thyroidectomy with one or more lymph nodes examined. To rule out occult nodal disease with 90% confidence, 6, 9, and 18 lymph nodes would need to be examined for patients with T1b, T2, and T3 diseases, respectively. Sensitivity analyses limited to patients likely undergoing prophylactic central compartmental neck dissection resulted in need to assess three, four, and eight nodes to provide comparable adequacy of lymph node evaluation for T1b, T2, and T3 diseases, respectively. Heaton et al. 454 evaluated 125 patients who underwent CLND, of whom 20 had a nodal recurrence. The LNY of patients subsequently developing central neck recurrence was significantly less than that of those who experienced no recurrence (2.5 vs. 10.3, respectively; p < 0.0001). Of 71 patients who underwent lateral neck dissection, 23 had ipsilateral lateral neck disease recurrence. The LNY of patients with lateral neck recurrence had been significantly less than those who did not recur (10.5 vs. 24.6, respectively; p < 0.0001). Higher rates of recurrence were associated with smaller lymph node yield in both groups. LNY remains predictive of recurrence on multivariable analysis controlling for pT categories, pN categories, AJCC stage, and RAI treatment.
Amit et al. 455 studied 2542 patients (1801 [71%] males; median age, 48 years [range, 18–97 years]) with a median follow-up of 55 months (range, 4–192 months). The 10-year disease-specific survival rate was 98% for patients with an LNR 450 of ≤0.19, compared with 90% for those with an LNR >0.19 (effect size, 8% [CI 4–15%]). The 10-year overall survival was 87% for patients with an LNR of ≤0.19, compared with 79% for patients with LNR >0.19 (effect size, 8% [CI 3–15%]). Multivariable analysis revealed that LNR >0.19 was independently associated with an adverse disease-specific survival (HR 4.11 [CI 2.11–8.97]) and overall survival (HR 1.96 [CI 1.24–4.11]). Subgroup analysis of patients with ≥18 lymph nodes analyzed revealed that LNR >0.19 remained a significant marker for disease-specific survival (HR 2.94 [CI 1.36–9.81]) and overall survival (HR 2.26 [CI 1.12–5.34]). Lee et al. found that an LNR >0.42 had an HR of 3.35 for locoregional recurrence. 456 Multivariable analysis of 1082 PTC patients who underwent total thyroidectomy and prophylactic central compartment lymph node dissection (pCCLND) had an LNR of >0.5 and an HR of 1.794 (p < 0.001) for recurrence. 457 Multivariable analysis of 390 patients with PTC who underwent total thyroidectomy, CLND, and ipsilateral or bilateral modified radical neck dissection demonstrated that a central neck LNR of 0.44 had an HR for recurrence of 2.35, while a lateral neck LNR >0.29 had an HR for recurrence of 1.58. 427 A multivariable analysis of 437 patients with N1b reported that an LNR >0.25 in the lateral neck had an HR for recurrence of 2.09.428,458 Lee et al. evaluated 211 patients who underwent total thyroidectomy and bilateral pCCLND and reported an LNR >0.26 associated with an HR for recurrence of 11.49.428,459 In a retrospective multivariable analysis, Kim reported an LNR >0.5 as a risk factor for recurrence in T1a PTC. 426 Lee et al. proposed the LNR of 0.17857 should be used in combination with the ATA Risk of Recurrence category to determine overall risk of recurrence. 460
Griffin et al. 461 conducted a retrospective review of cases in which five lymph nodes or more were removed during thyroidectomy and five or fewer lymph nodes were found to be involved with PTC. Step-sectioning was performed on original tumor blocks, and all slides were re-reviewed by a senior pathologist. Step-sectioning significantly increased LNY compared with standard sectioning. In total, they found 12 new involved lymph nodes; 7 (58%) were in totally new lymph nodes, while 5 (42%) were in lymph nodes previously believed to be uninvolved. All were classified as micrometastases (≤2 mm). These data support using consistent standards of assiduous pathology specimen handling and sectioning related to lymph node assessment in DTC. This is relevant because future studies evaluating the number of lymph nodes resected and LNR as parameters for prognosis should include a description of the techniques used to harvest and analyze lymph nodes as well as the size of the focus of DTC in the lymph node(s).
What is the appropriate perioperative approach to voice and parathyroid issues?
▪
Prior to surgery, the surgeon should review surgical risks with the patient, including potential for nerve and parathyroid injury, through the informed consent process and communicate with associated physicians, including anesthesia colleagues, important findings elicited during the preoperative evaluation.
The preoperative consent process should include explicit discussion of the potential for temporary or permanent nerve injury (and its clinical sequelae, including voice change, swallowing disability, risk of aspiration, and tracheostomy) as well as hypoparathyroidism, discomfort, risks of anesthesia, bleeding, scarring, disease recurrence, reoperation, need for additional postoperative treatment, need for thyroid hormone supplementation/replacement, and surveillance thyroid function tests. The conversation should be informed by the operating surgeon’s own rates of complications. Results of the preoperative evaluation regarding extent of disease, risk stratification, and integrity of the airway should include findings from imaging, cytology, and physical examination.462–466
Should the patient undergo voice or laryngeal examination prior to surgery?
▪
All patients undergoing thyroid surgery should undergo voice assessment as part of their preoperative physical examination. This should include the patient’s description of vocal changes and the physician’s assessment of voice. Preoperative laryngeal exam should be performed in all patients with: Preoperative dysphonia History of cervical or upper chest surgery, which places the recurrent laryngeal nerve or vagus nerve at risk Known thyroid cancer with posterior extrathyroidal extension or extensive central compartment or jugular chain nodal metastases
Voice alteration is an important potential complication of thyroid surgery affecting patients’ QoL (with regard to voice, swallowing, and airway domains), and it has medico-legal and cost implications.467–475
Preoperative assessment provides a necessary baseline reference from which to establish subsequent expectations. 476 Also, preoperative voice assessment may lead to identification of vocal cord paralysis or paresis, which provides presumptive evidence of invasive thyroid malignancy and is important in planning extent of surgery and perioperative airway management.477–479 Contralateral surgical nerve injury in such patients could cause bilateral cord paralysis with airway implications.
Preoperative voice assessment should include the patient’s subjective response to questions regarding voice abnormalities or changes, as well as the physician’s objective assessment of voice, and should be documented in the medical record. 480 Voice and laryngeal function may be further assessed through laryngoscopy and the application of validated QoL and auditory perceptual assessment voice instruments. 476 Transcutaneous laryngeal ultrasound to evaluate laryngeal function gained popularity during the COVID-19 pandemic, but evaluation can be limited in some patients, particularly older males with calcified thyroid cartilage. It is important to appreciate that vocal cord paralysis, especially when chronic, may not be associated with significant voice symptoms due to a variety of mechanisms, including contralateral vocal cord compensation. Voice assessment alone may not identify such individuals. 476
Incidence rates for preoperative vocal cord paresis or paralysis for patients with benign thyroid disease at preoperative laryngoscopy range from 0% to 3.5% and up to 8% in patients with thyroid cancer.481–485 Finding vocal cord paralysis on preoperative examination strongly suggests the presence of locally invasive disease. Approximately 10–15% of thyroid cancers present with extrathyroidal extension, with the most common structures involved including strap muscle (53%), the recurrent laryngeal nerve (47%), trachea (30%), esophagus (21%), and larynx (12%).479,486–488 Undiagnosed preoperative laryngeal nerve dysfunction conveys greater risks of bilateral nerve paralysis during total thyroidectomy, respiratory distress, and need for tracheostomy. 489 Preoperative identification of vocal cord paralysis is important because surgical approaches to the management of the invaded nerve incorporate functional status. 490
A laryngeal exam should be performed if the voice is abnormal during preoperative voice evaluation. Any patient with a history of neck surgery which placed either the recurrent laryngeal nerve (such as past thyroid or parathyroid surgery) or the vagus nerve (such as carotid endarterectomy, cervical esophagectomy, and anterior approach to the cervical spine) at risk or with a history of prior external beam radiation to the neck should have laryngeal exam even if the voice is normal. Correlation between vocal symptoms and actual vocal cord function is poor due to the potential for (i) variation in paralytic cord position, (ii) degree of partial nerve function, and (iii) contralateral cord function/compensation. Therefore, voice symptoms may be absent in patients with vocal cord paralysis. Vocal cord paralysis may be present in 1.5–30% of such postsurgical patients; it can be asymptomatic in up to one third of the patients.477,491–497
A laryngeal exam is recommended in patients with the preoperative diagnosis of thyroid cancer if there is evidence for gross extrathyroidal extension of cancer, which extends posteriorly or if there is extensive nodal involvement, even with normal voice. The laryngeal exam should be performed in the above noted high-risk settings but may be performed on other patients based on the surgeon’s judgment.
How should the recurrent laryngeal nerves be assessed intraoperatively?
▪
Visual identification of the recurrent laryngeal nerve(s) (RLN) should be performed during thyroidectomy and/or para-tracheal node dissection, to preserve nerve integrity and function. Intraoperative neurophysiological monitoring of the RLN may be performed during thyroidectomy for malignancy in an effort to reduce the risk of RLN injury, particularly during total or re-operative thyroidectomy. Intraoperative identification and neurophysiological monitoring of the external branch of the superior laryngeal nerve (EBSLN) may be performed during thyroidectomy for malignancy in an effort to improve accurate nerve identification and improve voice outcomes. Intraoperative vagal nerve or proximal RLN stimulation (with monitoring or laryngeal palpation) should be performed after initial lobectomy to assess RLN integrity and function prior to removing the contralateral lobe in an effort to avoid possible bilateral nerve injury.
RLN injury rates are lower when the nerve is regularly seen in comparison to operations in which the nerve is simply avoided,480,495,498 and prior ATA guidelines have strongly recommended visual identification. No formal recommendation was made for nerve integrity monitoring (NIM) to prevent RLN injury, as the evidence confirming a benefit at the time was equivocal for routine use,492,499–501 but its use appeared beneficial for complex and re-operative thyroid surgery.479,502–506 Nerve stimulation (with or without monitoring) was recommended to confirm accurate identification and nerve function. 14
Subsequently, several meta-analyses have considered the subject. A Cochrane meta-analysis restricted to five randomized controlled trials (n = 5) found NIM and visual nerve identification alone are associated with similar rates of permanent RLN paralysis (0.7% vs. 0.9%, RR 0.77 [CI 0.33–1.77]); however, NIM was associated with a trend toward decreased RR of transient RLN injury that was not statistically significant (2.1% vs. 3.6%; RR 0.62 [CI 0.35–1.08]; p = 0.09). 507 In the Cochrane meta-analysis, there was also no statistically significant difference in risk of the composite outcome of permanent or temporary RLN paralysis (2.7% vs. 4.4%; RR 0.70 [CI 0.38–1.30]; p = 0.21). However, the absolute risk difference (2%) was statistically significant, with the number of nerves needed to treat/monitor (NNT) estimated to be about 50 to prevent one event (risk difference −2.0% [CI −3.0 to 0.0%]; p = 0.03). Our panel identified a small (n = 72) randomized trial 498 not included in the Cochrane review, which showed a nonsignificant difference in transient RLN injury of 2.7% in the NIM group versus 8.3% in the control group. Another meta-analysis including 24 randomized and nonrandomized trials found a significant reduction in overall (3.2% vs. 4.4%, p = 0.04) and transient (1.8% vs. 2.6%, p = 0.01) RLN injury rates with a possible reduction in permanent (0.7% vs. 1.1%, p = 0.15) RLN injury and a risk difference of 1.2% for overall rates, which suggests an NNT of about 80. 499 In the subset of four studies limited to patients with thyroid cancer, a significant reduction with NIM was noted for overall (3.9% vs. 6.6%, p < 0.05) and transient (3.0% vs. 5.0%, p < 0.05) but not permanent RLN injury (0.9% vs. 1.6%, p > 0.05), which translates into a NNT of approximately 30 patients. Another meta-analysis including 34 studies found significant reductions in overall (3.0% vs. 3.9%, p = 0.0002), transient (2.3% vs. 2.8%, p = 0.002), and permanent (0.7% vs. 1.0%, p = 0.003) nerve injury rates with NIM. This was significant in the subgroups undergoing total thyroidectomy (1.5% vs. 3.0%, p < 0.05; 1.1% vs. 2.1%, p < 0.05; 0.5% vs. 0.8%, p < 0.05) or thyroid surgery for cancer (2.6% vs. 4.4%, p = 0.02; 2.0% vs. 3.4%, p = 0.04; 1.2% vs. 1.1%, p = 0.73), for overall, transient, and permanent nerve injury rates, respectively. The authors recommended NIM for bilateral thyroidectomy (NNT approximately 70) and/or cancer (NNT approximately 60). A meta-analysis limited to high-risk thyroid surgery that included 10 studies found significant reduction in overall (2.5% vs. 4.5%, p = 0.003), transient (2.4% vs. 3.9%, p = 0.02), and permanent (0.1% vs. 0.6%, p = 0.10) RLN injury rates, with subgroup analysis demonstrating significantly lower overall RLN injury rates for cancer (2.1% vs. 3.5%, p = 0.03) and reoperation (4.5% vs. 7.6%, p = 0.02). The authors recommended NIM, particularly in these two situations, with estimates of NNT of approximately 70 and 30, respectively. 501 Results of subsequent individual studies vary, but the majority demonstrate a significant benefit of nerve monitoring to prevent RLN injury.508–521
These reports are supported by several recent large database studies demonstrating significant reduction in RLN injury rates with NIM. A National Surgical Quality Improvement Program (NSQIP) study involving nearly 10,000 patients found a significant reduction in RLN injury with NIM use, particularly for thyroid cancer (OR 0.76, p = 0.01). 522 This is confirmed by an even larger NSQIP study of nearly 18,000 patients showing significant reduction in RLN injury with NIM use (5.7% vs. 6.8%, OR 0.67, p = 0.00001) 523 and verified by a third NSQIP study. 524 These results were recapitulated in a large endocrine and thyroid registry from the United Kingdom, with a significant reduction in both transient and permanent RLN injury with NIM use (OR 0.63 and OR 0.47, respectively, both p < 0.0001). 525
Studies comparing automatic persistent (often termed “continuous”) vagal nerve stimulation with monitoring versus conventional laryngeal NIM with intermittent stimulation have been conflicting.523,526–529 Further study may be warranted to determine whether the potential advantage of continuous vagal nerve stimulation with monitoring is worth the potential added risk of device placement compared with traditional NIM.
Evaluation of NIM cost-effectiveness suggested a benefit in two520,530 but not a third publication. 531 Results of the later publication would change if the RR reduction were ≥50% (as shown in the meta-analyses above). Studies517,532 including a randomized controlled trial 533 have shown a reduction in time to find the nerve with NIM use, but the differences may not be clinically meaningful (<5 minutes). A recent survey of North American surgeons revealed increasing utilization of NIM, with 70% using NIM always, 15% sometimes, and 13% never. 534 One percent reported it was not available at their institution. Of those using it sometimes, indications included reoperation (94%), preoperative RLN paralysis or dysphonia (84%), patient preference (46%), and cancer (34%). Commercially available NIM endotracheal tubes were used most (89%), regular endotracheal tubes with electromyography adhesive (8%), or palpation of laryngeal twitch alone (2.5%). Only 0.4% employ persistent stimulation for vagus nerve monitoring. 534
The ATA 2015 guidelines suggested deploying RLN stimulation at the completion of lobectomy to determine the safety of contralateral resection to avert bilateral vocal cord paralysis and resultant airway compromise.14,504,535–537 Subsequently, the International Nerve Monitoring Study Group (INMSG) recommended deferring completion thyroidectomy in cases with loss of nerve function on the first side, thus preventing bilateral RLN paralysis; most RLN injuries are temporary and will usually resolve within a few months. 538 This approach is supported by recently published surgical thyroidectomy guidelines of the American Head and Neck Society (AHNS) 539 and the American Association of Endocrine Surgeons (AAES). 540 Several studies have evaluated the results of such an approach. Reported NPV, confirming intact RLN function postoperatively when nerve stimulation shows appropriate NIM signal and/or palpable laryngeal twitch of the arytenoid, are remarkably high at 99–99.9%, with specificity of 99%.508,541,542 The PPV confirming RLN paralysis postoperatively is somewhat lower but has been considered acceptably high at 77–78%, with sensitivity of 90–94%.508,541–544 In practice, this has resulted in a two-stage procedure in 4–5% of planned total thyroidectomies following lobectomy accompanied by loss of stimulation NIM signal or laryngeal twitch. Approximately 80% of those cases demonstrate early postoperative RLN palsy with subsequent recovery in 90% of those cases.541,544,545 Another team eliminated bilateral RLN paralysis completely (0% vs. 2.7%, p = 0.03) after adoption of the approach. 546 A recent analysis evaluating NIM to prevent bilateral RLN paralysis demonstrated cost-effectiveness of this approach. 547 A protocol evaluating the potential for intraoperative return of signal within 20 minutes of its loss, either spontaneously or following treatment with 4 mg dexamethasone found a significantly greater rate of intraoperative return of signal (18% vs. 88%, p < 0.001) with significantly lower rates of transient (82% vs. 6%, p < 0.001) and permanent (50% vs. 0%, p < 0.001) postoperative RLN paralysis in the dexamethasone-treated group. 548
Management of invasive thyroid cancer involving the RLN is challenging, and the topic of several recently published statements/guidelines from the AHNS,488,539 AAES, 540 and INMSG. 549 Knowing the preoperative functional status of the nerve is critical to intraoperative management. When the nerve is functioning preoperatively, removal of all gross tumor with the nerve dissected intact is preferable. When the nerve is encased in tumor and/or paralyzed preoperatively, then nerve sacrifice to ensure complete tumor removal should be undertaken. In cases of nerve sacrifice, primary anastomosis is ideal if feasible. Otherwise ansa cervicalis nerve anastomosis to the distal segment may be performed. Primary or delayed vocal fold medialization is another option.488,539,540,549
The EBSLN is small. It innervates the cricothyroid muscle and facilitates tensing the vocal folds to raise voice pitch, which is particularly important to singers and other professional voice users. The EBSLN is vulnerable to injury during thyroid surgery, and traditional surgical strategies to avoid injury include visual identification and/or ligation of the superior pole vasculature as close to the superior pole capsule as possible (as recommended in the prior ATA guidelines). Cernea, who developed the first classification system for EBSLN anatomy in relation to the thyroid gland, 550 was also the first to report a lower rate of EBSLN injury with stimulation of the nerve compared to the traditional approach. 551 A recent study of post-thyroidectomy patients revealed that 15–20% of patients had a change in their speaking fundamental frequency because of EBSLN injury, highlighting the importance of this problem. 552 A recent monograph documented a significant association between decreased EBSLN stimulation response after superior pole dissection and worse voice outcomes. 553
The INMSG has published guidelines suggesting EBSLN stimulation/monitoring to reduce the risk of injury. 506 A recent meta-analysis revealed a significantly greater rate of EBSLN identification with nerve stimulation compared to visual identification alone (96% [CI 94–97] vs. 77% [CI 69–83]). 554 A randomized controlled trial of NIM-based stimulation versus conventional technique aided by a widely available battery-powered nerve stimulator demonstrated a greater rate of nerve identification and preservation with NIM than with the battery-powered device (89% vs. 18%, p < 0.001). Fewer female patients experienced postoperative voice impairment in the NIM group (3% vs. 11%, p = 0.02). 555 Another randomized controlled trial comparing the use of NIM-supported stimulation to traditional ligation of the superior pole vessels close to the capsule revealed a lower EBSLN injury rate (9% vs. 1%, p = 0.01) and lower voice impairment scores 1 and (p = 0.02) 3 (p = 0.03) months postoperatively in the NIM-supported stimulation group.556,557 This is supported by another randomized controlled trial of NIM versus traditional ligation of the superior pole vessels with lower rates of EBSLN injury (9% vs. 1%, p = 0.01) and lower voice impairment scores 1 (p = 0.012), 3 (p = 0.015), and 6 months postoperatively (p = 0.02) in the NIM group. 558 These results are similar to an earlier randomized controlled trial of NIM versus visualization alone with higher rates of EBSLN identification in the NIM group (84% vs. 34%, p < 0.001); lower rates of EBSLN injury (1.5% vs. 6%, p = 0.02) 559 ; and lower early postoperative rates of diminished mean phonation time (2% vs. 10%, p = 0.018), voice level (2% vs. 13%, p = 0.003), and fundamental frequency (1% vs. 9%, p = 0.03). 559 Several recent studies have confirmed higher rates of nerve identification with the use of NIM-supported stimulation (94–98%) compared with visual identification (28–82%).556,560–566 In one study with a relatively high rate (79%) of visual identification of the EBSLN, nerve stimulation showed the impression to be erroneous in 21%. 565
In sum, visual identification of the RLN during operations for thyroid cancer remains the gold standard for prevention of injury. Laryngeal NIM appears to reduce risk of RLN injury during thyroid surgery, particularly for total thyroidectomy, cancer, or reoperation for recurrent disease with estimated NNT/monitor ranging from 30 to 70 to prevent one injury. Visual identification of the EBSLN is challenging due to the size of the nerve so that accurate identification and preservation are significantly improved with NIM-supported stimulation, resulting in better voice outcomes. In fact, the evidence supporting NIM use appears even stronger for EBSLN than RLN. Commercially available NIM systems seem available in approximately 99% of institutions performing thyroid surgery in North America. Some 70% of surgeons always use them, and another 15% employ NIM systems selectively. Common indications for selective use include reoperation, preoperative dysphonia/paralysis, patient preference, and thyroid cancer. The predictive value of a response to vagal and/or proximal RLN stimulation confirming a functioning RLN after completion of dissection is on the order of 99% and proceeding to the contralateral side in planned total thyroidectomy under this circumstance is exceedingly unlikely to result in bilateral cord paralysis with attendant airway compromise. The predictive value of loss of response to stimulation suggesting RLN injury is also high at 75–80%. Deferring resection of the contralateral side (when oncologically sound) to allow a likely transient RLN injury to resolve seems to prevent bilateral injury with need for tracheostomy. Initiating resection on the side of the cancer during planned total thyroidectomy for unilateral disease is imperative when employing this strategy. Palpation of arytenoid/laryngeal twitch with vagal/RLN stimulation is a long-standing and acceptable alternative to the use of NIM endotracheal tubes to confirm RLN function at the completion of dissection.
How should the parathyroid glands be managed intraoperatively and perioperatively?
▪
The parathyroid glands and their blood supply should be preserved during thyroid surgery to reduce the risk of hypoparathyroidism. Parathyroid glands, if devascularized or removed, should be auto-transplanted into nearby muscle after frozen section (of a portion) confirms benign parathyroid tissue. After total thyroidectomy and/or central lymph node dissection, or after unilateral operations that follow prior contralateral thyroid resections, parathyroid hormone-directed calcium and vitamin D supplementation (regular or selective) should be provided to reduce rates of hypocalcemia and shorten hospital stays compared with observation with serial calcium measurement alone.
Typically, parathyroid gland preservation is enhanced by gland identification benefiting from meticulous dissection.535,567 If the parathyroid(s) cannot be located, the surgeon should attempt to dissect on the thyroid capsule and ligate the inferior thyroid artery very close to the thyroid, since most parathyroid glands receive their blood supply from this vessel. Superior glands may receive blood supply from the superior thyroid artery. If the parathyroid glands are discovered to have been inadvertently or unavoidably removed during thyroidectomy or central lymph node dissection, or if devascularized, then frozen section confirmation (of a portion) of the suspected parathyroid gland should be performed to confirm parathyroid tissue without evidence of cancer. Then, the remainder of the parathyroid can be auto-transplanted into strap or sternocleidomastoid muscles. It is important to inspect the thyroidectomy and/or central lymphadenectomy specimen after resection and before passing it off the sterile field to find parathyroid glands that can be salvaged for auto-transplantation. This is particularly important if the parathyroid glands were not identified during dissection. Regular sacrifice of a parathyroid gland for auto-transplantation may increase transient hypoparathyroidism without improving long-term outcomes, 568 but there is no firm consensus in the literature,569,570 and interpretation is obscured by need to reimplant ischemic and excised glands. Intraoperative adjuncts designed to aid in parathyroid gland identification remain investigational in the United States. Optical technologies, such as near-infrared autofluorescence and near-infrared fluorescence imaging with indocyanine green, seem promising and potentially superior to employing the naked eye for parathyroid identification,571–576 as do carbon nanoparticles, which are not widely available.577–579
Hypocalcemia resulting from hypoparathyroidism is a risk primarily following total or completion thyroidectomy, as well as central compartment lymph node dissection involving both paratracheal basins and unilateral central lymphadenectomy after contralateral operations. Symptoms of hypocalcemia can progress to tetany if left untreated. Strategies to prevent development of hypocalcemia, rather than awaiting the onset of symptoms, include selective supplementation based upon early rapid postoperative parathyroid hormone testing regular use of postoperative calcium and vitamin D supplementation or selective supplementation based upon early rapid postoperative parathyroid hormone testing and are supported by ATA and surgical society guidance, and in more recent prospective randomized study addressing universal versus symptomatic-driven treatment.540,580,581
Should drainage of the thyroidectomy bed be performed?
▪
Under most circumstances, drainage of the thyroidectomy bed is not recommended; it is associated with increased length of stay, may increase infections, and does not reduce the incidence of hematoma.
Drainage of the surgical bed after thyroidectomy was once common. Proponents expressed concerns surrounding ready detection of postoperative hemorrhage and prevention of fluid collections. Opponents have cited drains as a potential source of infection. Meta-analyses and randomized trials have been undertaken. In a meta-analysis of more than 1900 patients, drainage of the thyroid bed was associated with increased length of stay, increased infection rate, and increased incidence of hematoma. 582 Selective use may be reasonable with very large (chiefly retrosternal) glands, excessive intraoperative bleeding, and/or bleeding disorders. In contrast, due to lymphatic disruption following comprehensive lateral neck dissection for nodal disease, drain placement is typically employed to reduce seroma formation and to aid adherence of elevated flaps.
How should the surgeon manage postoperative voice changes and symptoms after surgery if they occur?
▪
Patients should have their voice assessed in the postoperative period. Formal laryngeal exam should be performed if the voice is abnormal. Important intraoperative findings and details of postoperative care should be communicated by the surgeon to the patient and other physicians who are important in the patient’s post-operative care. If there is known recurrent laryngeal nerve injury from surgery, timely referral to a speech language pathologist and physician specializing in voice is recommended.
Voice assessment should occur after surgery and should be based on the patient’s subjective report and physician’s objective assessment of voice in the office. 14 Typically, this assessment can be performed at 2 weeks to 2 months after surgery. Early detection of vocal fold motion abnormalities after thyroidectomy is important for facilitating prompt intervention (typically through early injection and/or vocal fold medialization), which is associated with better long-term outcome, including a lower rate of formal open thyroplasty repair. 583 There are many options for the management of RLN paralysis, including voice therapy, vocal fold injection techniques, and open vocal fold medialization. Rates of vocal fold paralysis after thyroid surgery can only be assessed by laryngeal exam postoperatively. 583
Effective thyroid cancer management requires a highly collaborative, interdisciplinary effort centered around the patient, starting with issues surgeons face related to the wound and postoperative neck. The cervical scar that results after thyroid surgery is a result of multiple factors that are both surgical technique and patient related. Many studies have reported that the appearance of the cervical scar after thyroid surgery has a significant quality of life (QoL) impact on patients, especially within the first few years after surgery.584,585 Management of the scar and lessening its impact should be a focus for the thyroid surgeon. Some patients experience a “tight neck” after thyroid surgery that is most noticeable in the first 3 months but may persist even longer. This tightness may result in a globus sensation or dysphagia. 586 Massage and neck range of motion exercises in the immediate post-op period may help to minimize this effect for the short and long term. 587
Surgeon communication with the clinical teams
Carty et al. 588 defined a multidisciplinary data set of essential perioperative information requiring documentation and communication in this process. Since their publication, the increasingly nuanced management recommendations should be carefully considered and discussed among all stakeholders involved in treatment decision-making. The discussion of risks, benefits, and alternatives to active surveillance for T1a PTC is one such feature (see Active Surveillance section). Another is the decision whether to perform a thyroid lobectomy only for T1 and T2 DTC that meets appropriate criteria. This requires shared decision-making. It is important for the team that will be performing surveillance after thyroid surgery to concur with the selected surgical option. Consensus for management that includes the patient’s view should be achieved and documented through this interdisciplinary communication.
The AHNS Endocrine Section 589 developed a consensus-based, unified, preoperative, perioperative, and postoperative workflow for North American use. The AAES guidelines for thyroidectomy list key findings that should be communicated in an operative note. These should include information about indication(s), informed consent, surgical findings (e.g., extrathyroidal extension, lymph node status, aberrant anatomy), parathyroid gland status, recurrent laryngeal nerve identification and preservation, attending surgeon presence during procedural steps, hemostasis, closure methods, and patient disposition. 540 Electronic health records allow for computerized and/or synoptic operative reporting, which has the potential to improve documentation and efficiency.590,591 The surgeon should also relay information regarding the completeness of resection and should help to reconcile pathology findings, especially as they relate to involved margins and whether the resection was R0 versus R1 versus R2. This may inform the need for more intense adjuvant treatments and monitoring.
Dos Reis et al. 592 examined the Memorial Sloan Kettering Thyroid Surgery e-Form, the Alberta WebSMR, and the Thyroid Cancer Care Collaborative (TCCC) electronic health records. Each met all the general recommendations for effective reporting of the domains that are specified in the management of thyroid cancer, as recommended by the ATA. However, the TCCC format was the most comprehensive. The TCCC is a web-based disease-specific database designed to enhance communication of patient information between clinicians in a Health Insurance Portability and Accountability Act–compliant manner. There should be consideration of coordinated care linkages between electronic medical record portals for the guidelines-based management of patients with thyroid cancer. The before and after results of adoption of guidelines-based thyroid cancer care should be studied. Better adherence to guidelines should reduce variation in care and improve value for all stakeholders. One starting point in these efforts would be creating an intra-institutional multidisciplinary thyroid conference (MDTC). Moore et al. 593 compared the postoperative RAI regimens for patients with thyroid cancer before and after instituting an MDTC. In the intermediate and high-risk patient groups, there was a significant decrease in the number of patients who received high-dose RAI after implementation of a MDTC compared with before initiation of an MDTC (p = 0.04 and p < 0.01) without an associated increase in tumor recurrence (11 vs. 7%, p = 0.74). On multivariable analysis, presentation of a patient at MDTC was a negative predictor for receiving high-dose RAI noncompliant with guidelines (p = 0.002).
What are the basic principles of histopathologic evaluation of thyroidectomy samples?
▪
In addition to the essential histopathologic features of the tumor required for the latest AJCC thyroid cancer staging (including status of resection margins), pathology reports should include additional information helpful for risk assessment, including the presence of vascular invasion and the number of invaded vessels, number of lymph nodes examined and involved with tumor, size of the largest metastatic focus to the lymph nodes, and presence or absence of extranodal extension of the metastatic tumor. Histopathologic subtypes of DTC associated with unfavorable (e.g., tall cell, columnar cell, and hobnail subtypes of PTC; widely invasive FTC and OTC; high-grade follicular cell-derived non-ATC) or favorable (e.g., IEFVPTC with minimal invasion, minimally invasive FTC) outcomes should be identified during histopathologic examination and reported. Histopathologic subtypes associated with familial syndromes (cribriform-morular carcinoma can be associated with familial adenomatous polyposis, PHTS associated FTC or PTC) should be identified during histopathologic examination and reported.
The accurate reporting of the important findings from the histopathologic assessment of thyroidectomy specimens is critical to guide therapy and surveillance. A regularly updated synoptic pathology report template containing the essential elements to evaluate may be found at www.cap.org/protocols-and-guidelines/cancer-reporting-tools/cancer-protocol-templates. 594
How should risk of recurrence and initial assessment be performed after surgery?
▪
The 2025 ATA Risk Stratification System, which evaluates the histopathologic features of the tumor and number of cervical lymph nodes in combination with the AJCC staging system, postoperative imaging, and serum Tg and TgAb testing (if appropriate), is recommended to determine the risk of structural disease persistence/recurrence (locoregionally and/or distantly) and/or survival in patients with DTC. Molecular profiling of histologic specimens postoperatively is not recommended routinely. However, if such data have been obtained, they can be used to further estimate risks of recurrence derived from the 2025 ATA Risk Stratification System.
The 2025 ATA Risk Stratification System predicts clinical outcomes for patients with DTC (PTC, FTC/IEFVPTC, OTC) after initial diagnosis and surgery, in general within ∼3 months of surgery (Fig. 2). It is intended to be used in conjunction with the 8th edition AJCC staging system (Tables 6 and 7), postoperative imaging, and serum Tg and TgAb levels (if appropriate based on the extent of surgery). Previous ATA guidelines (2009 and 2015 versions) for the management of thyroid nodules and DTC recommended a three-tiered categorical system stratifying patients as low, intermediate, or high risk of structural disease persistence/recurrence. The current system identifies specific features of DTC that should be considered when determining the overall risk of future structural persistence/recurrence for an individual patient. The higher risk of recurrence is frequently dependent on co-existing factors rather than a single factor.
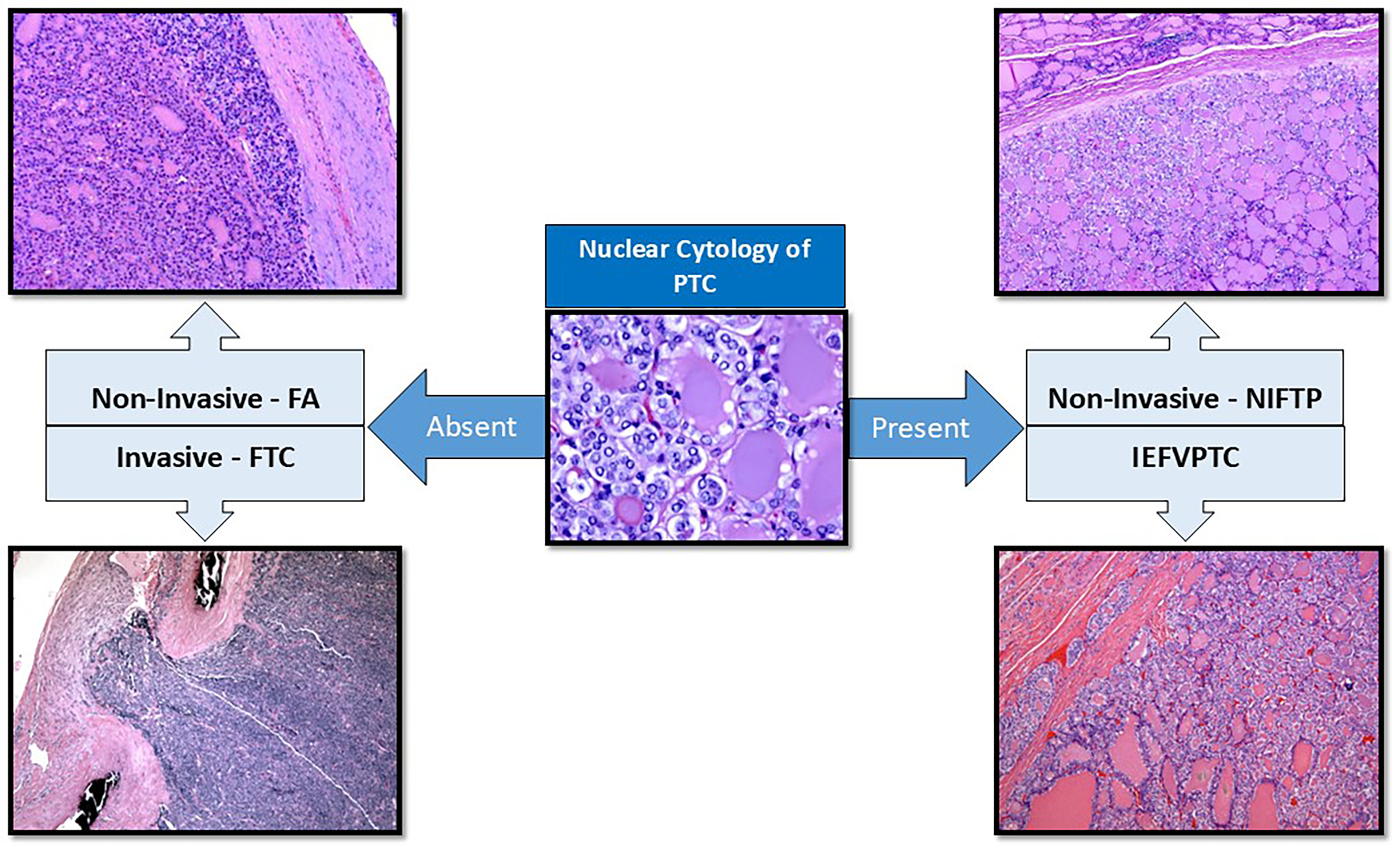
Major histological subtypes of differentiated thyroid carcinomas. FA, follicular adenoma; FTC, follicular thyroid carcinoma; PTC, papillary thyroid carcinoma; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; IEFVPTC, invasive encapsulated follicular variant of papillary thyroid carcinoma.
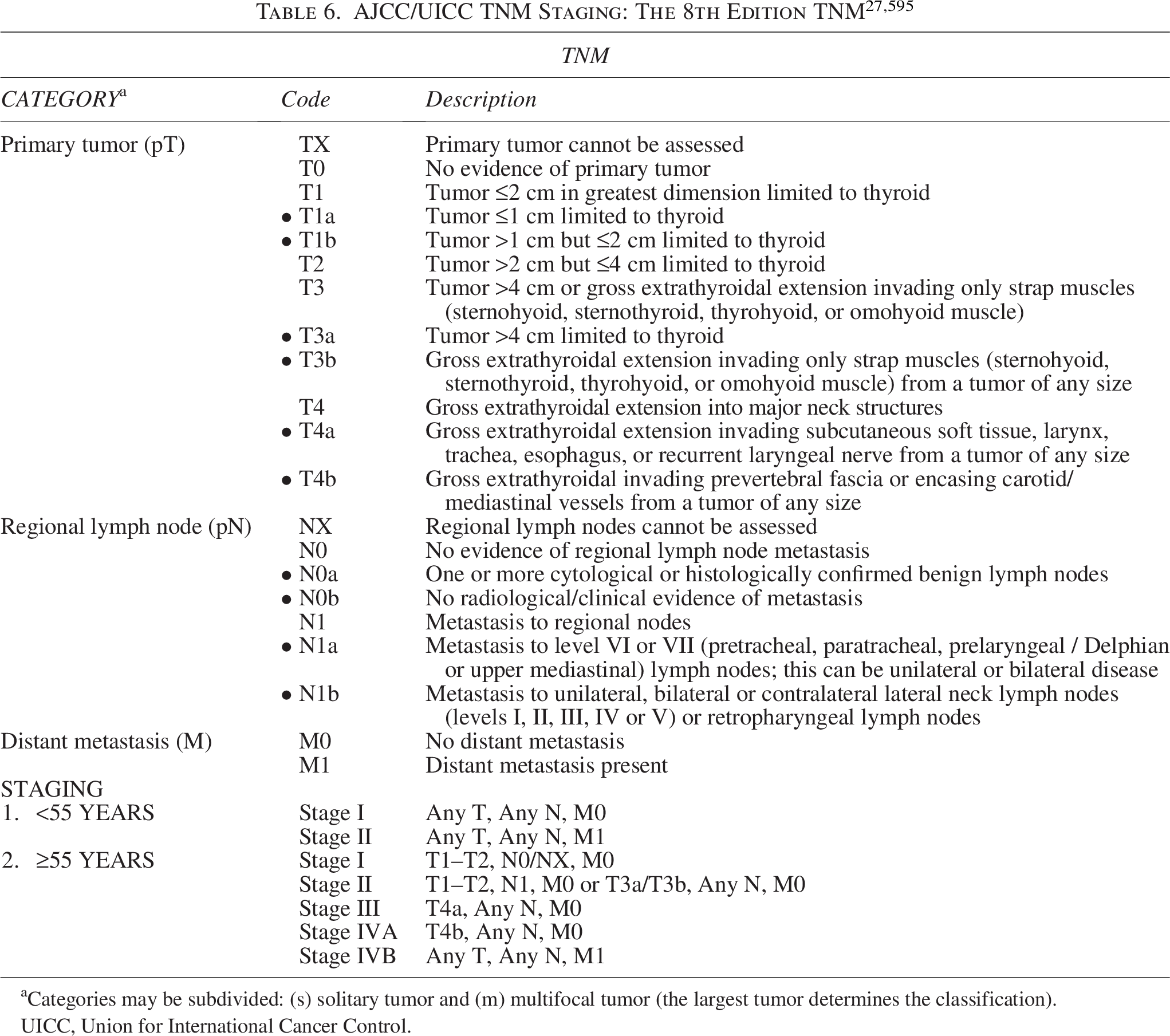
Categories may be subdivided: (s) solitary tumor and (m) multifocal tumor (the largest tumor determines the classification).
UICC, Union for International Cancer Control.

Since the 8th edition AJCC/Union for International Cancer Control (UICC) guidelines were published, multiple studies have compared staging using both the 7th and 8th edition AJCC/UICC staging systems. Overall, when using the 8th edition, 20–30% of patients are downstaged as compared with the 7th edition.595,597,598 The 7th edition did not clearly differentiate risk of recurrence-free survival between the lower TNM (I, I, III) stages, and only Stage IV predicted worse survival. The 8th edition stratification more appropriately predicts disease-free survival.595,596,598 Manzardo et al. evaluated the reasons for downstaging when using the 8th edition as compared with the 7th edition and reported 48.5% were downstaged due to the change in patient age cutoff, and 50.1% were downstaged because of changes in tumor characteristics, such as microscopic extrathyroidal extension. The risk of recurrence was higher in those who were downstaged to the 8th edition Stages I and II when compared with those who were considered Stages I and II in both the 7th and 8th editions. Those that were downstaged due to tumor characteristics had a higher risk of recurrence than those who were downstaged because of patient age. 597 Chereau et al. evaluated risk of recurrence in the 7th edition T3 DTC tumors specifically and so included T3 cancers that were >4 cm as well as those that were T3 due to microscopic extrathyroidal extension. They reported a risk of recurrence in cancers ≤1 cm with microscopic extrathyroidal extension that was 6%, cancers 1–4 cm with microscopic extrathyroidal extension had an 18% risk of recurrence, cancers >4 cm without extrathyroidal extension had a 12% risk of recurrence, and cancers >4 cm with microscopic extrathyroidal extension had a 48% risk of recurrence. 599 AJCC/UICC staging is designed to predict disease-specific survival and thus does not predict overall risk of structural persistence/recurrence.
The 2015 ATA Risk of Recurrence stratification system has been reported to be a better predictor of structural persistence/recurrence than AJCC/UICC TNM staging, which predicts disease-specific survival (Fig. 2). 597 Multivariable analysis of the 2015 ATA Risk of Recurrence categories in patients with PTC showed 1.5% recurrence in low-risk, 5.4% in intermediate-risk, and 25% in high-risk patients. 600 Similar rates of recurrence were seen when evaluating T1a PTC: 1.6% in low-risk, 7.4% in intermediate-risk, and 22.7% in high-risk disease. 601 Van Velsen et al. specifically addressed the 2015 ATA Risk of Recurrence stratification system in patients with high-risk PTC and FTC. They evaluated 236 patients with high-risk DTC (32% FTC) and found all the 2015 ATA high-risk criteria were associated with recurrence except pathological lymph nodes >3 cm. Twenty-nine percent had an excellent response, and 51% had structural persistence/recurrence; 4% had a biochemically incomplete response, and 16% had an indeterminate (16%) response. Of those that attained an excellent response, 14% developed structural recurrence. 602 Lee et al. evaluated ATA 2015 risk of recurrence, AJCC/UICC 8th edition staging, and LNR and found that using a combination of all three assessments most accurately predicted risk of recurrence. 460 Since the 2015 ATA DTC guidelines, additional features have been reported to influence overall risk of structural persistence/recurrence, and others have been refined. These features have been incorporated into the 2025 ATA Risk of Recurrence categories for PTC, FTC/IEFVPTC, and OTC.
Tumor focality
In the 2015 guidelines, unifocal T1a PTC and multifocal T1a PTC were both categorized as having a low risk of structural persistence/recurrence. However, multifocal T1a PTC with microscopic extrathyroidal extension is categorized as having intermediate risk of recurrence, and multifocality in T1a PTC is reported to have a higher risk of structural recurrence (4–6%) than unifocal disease (1–2%). 14 The data guiding the role of tumor focality are mixed. Multivariable analysis of 496 patients with PTCs >1 cm revealed structural recurrence in 21.4% of those with bilateral multifocality (HR = 4), 12.8% recurrence in those with unilateral multifocality, and 6.6% recurrence in those with unifocal disease. 603 However, additional retrospective multivariable analyses have not supported this association. Some studies report multifocality is not an independent predictor of structural recurrence but often is associated with other higher risk predictors of structural recurrence, such as extrathyroidal extension, lymph node metastases, and higher TNM stage.411,413 Wang et al. performed a multicenter study of 2638 persons with PTC and reported recurrence in 21.2% of classical PTC with multifocality, as compared with 14.1% of unifocal classical PTC. However, when evaluating only T1a PTC, recurrence was lower at 13.7% in the multifocal and 5.1% in the unifocal groups. When evaluating FVPTC, those with multifocality had 13.7% recurrence, and patients with unifocal disease had 8.2% recurrence. Wang also evaluated patients with intrathyroidal tumors without any risk factors (such as extrathyroidal extension, lymph node metastases, or distant metastasis) and found that there was no difference in recurrence between multifocality (4.4%) and unifocality (4.2%), and overall rates of recurrence were much lower than those with multifocality in the presence of other risk factors. 413 In contrast, Genpeng et al. found multifocality was significantly associated with tumor capsular invasion (HR 1.5), T category (HR 1.87), and N category (HR 1.8) in a multivariable analysis of 570 patients with PTC. 604 Woo et al. evaluated 1249 patients who had undergone total thyroidectomy for PTC and also found multifocality to be an independent predictor of structural recurrence (HR 1.986) using multivariable Cox regression analysis, but 10-year disease-free survival was also lower in those with multifocal tumors (93.3%) compared with 97.6% for unifocal tumors. 605 Four systematic reviews and meta-analyses support the association between multifocality and overall increased risk of recurrence in patients with PTC.606–609 Zhang et al. performed a meta-analysis of 15 studies with a total of 9,665 patients and reported structural recurrence/persistence in 13% of unilateral multifocal cancers after total thyroidectomy versus 5.7% of unifocal cancers. 607 Kim et al. evaluated 26 studies with a total of 33,976 patients and reported that ≥3 foci of tumor was associated with a higher risk of recurrence (pooled HR 1.95). 606 Cui et al. also performed a systematic review and meta-analysis of 23 studies with 41,616 patients and reported increased risk of extrathyroidal extension (RR 1.38), central compartment lymph node metastases (RR 1.21), lateral compartment lymph node metastases (RR 1.86), distant metastasis (RR 1.35), and postoperative recurrence (HR 1.76) with multifocality when compared with unifocality. 608 Overall, most studies show that multifocality is an independent predictor of a higher risk of persistence/recurrence as compared with unifocal tumors >1 cm. The data are not as strong for multifocality as a predictor of structural persistence/recurrence in T1a PTCs.
Vascular invasion
Vascular invasion is defined as tumor cells invading through a vessel wall and the presence of a fibrin thrombus adherent to intravascular tumor. 610 On pathology reports, it is often referred to as “lymphovascular invasion” rather than identifying lymphatic or vascular (angioinvasion) invasion separately. Distinguishing between lymphovascular invasion and differentiating lymphatic from angioinvasion still remains controversial among pathologists. The main reason is that with routine hematoxylin and eosin staining, it is difficult to differentiate between small lymphatics, veins, and arteries. However, it is understood generally that psammoma bodies and viable tumor emboli seen within the thyroid parenchyma are within lymphatics. This has been shown by performing lymphatic-vessel-specific immunostains, such as D2-40.
The term “angioinvasion” is more applicable and diagnostically reproducible when there are sizable veins and arteries showing defined muscle structure and endothelial lining. These can be highlighted or confirmed by doing immunostains for ETS-related gene, factor VIII, and/or CD31. Angioinvasion detected in sizable (medium to large sized) vessels, seen in the tumor capsule, at the periphery of the thyroid gland or in the pseudo-capsule is significant and reproducible among pathologists. However, the criteria for diagnosing angioinvasion in thyroid carcinoma remain inconsistent. It has been shown that rigid criteria for angioinvasion (tumor cells invading through a vessel wall and covered with endothelium and tumor thrombus attached to the vessel wall) are associated with distant metastases. 610
Based on these challenges, some authors recommend using the term “lymphovascular invasion.” However, for tumor staging, it is critical for synoptic reporting to differentiate between angioinvasion and lymphatic invasion (as intra-lymphatic psammoma bodies or viable tumor emboli or both). Wagner et al. performed a single-institution retrospective analysis of 610 patients from 1987 to 2016 that included multivariable regression analysis. In this study, lymphovascular invasion was not an independent predictor of recurrence; however, it was associated with other adverse prognostic factors. 611 Since both lymphatic and vascular invasion were classified as the same entity, it is possible this explains the lack of association. When evaluating specifically for vascular invasion, studies have shown a significant association with risk of recurrence in all types of DTC (PTC, FTC, and OTC).434,610,612–618
Papillary thyroid carcinoma
In the 2015 ATA DTC guidelines, vascular invasion in PTC was associated with an intermediate risk of recurrence of 15–30%. 14 In retrospective multivariable analyses of 698 patients with DTC, Wreesman et al. found that vascular invasion was not an independent predictor of local recurrence but was associated with poor prognostic factors, including tumor size >4 cm, gross extrathyroidal extension, and distant metastasis. 434 Systematic review and meta-analysis of 26 studies with a total of 11,961 patients with all types of DTC (including PTC, FTC, minimally invasive FTC, and OTC) showed significant associations between vascular invasion and tumor persistence (OR 2.75), locoregional recurrence (OR 4.44), and distant recurrence (OR 5.08). 619 Pooled recurrence rates for those with vascular invasion was 21%, and for those without, it was 4%. 619 Subgroup analysis of just PTC showed vascular invasion significantly increased the risk of locoregional recurrence and distant recurrence. Newer literature suggests that vascular invasion is associated in general with an intermediate risk of structural recurrence but more commonly predicts distant metastasis rather than locoregional recurrence.434,610,612–619
Follicular thyroid carcinoma
The 2015 ATA guidelines classify FTC with extensive vascular invasion (≥4 vessels) as high-risk with a 30–55% risk of recurrence and minimally invasive (<4 vessels) as low risk and a 2–3% risk of recurrence. 14 Recent studies have suggested that any vascular invasion may be associated with more aggressive behavior. 620 Extensive vascular invasion in FTC has been reported to be associated with a higher risk of distant metastasis than of locoregional recurrence. 621 Lee et al. evaluated 166 patients with FTC, and multivariable analysis showed the presence of any vascular invasion was associated with an HR of 29.06 for recurrence. However, when divided between <4 and ≥4 vessels, ≥4 vessels had an HR of 40.57 as compared with <4 vessels. 433 Xu et al. evaluated 276 patients with low grade encapsulated DTC and found overall higher rates of extensive vascular invasion in FTC and OTC compared with PTC. Those with focal (<4 vessels) vascular invasion had a 1% recurrence rate, but 26% of those with extensive vascular invasion developed recurrence. 66 Ito et al. evaluated 523 patients with FTC and compared those with no vascular invasion to those with <4 vessels and those ≥4 vessels and found a progressive increase in risk of distant metastatic disease with increasing vascular involvement, with an HR of 2.5 in those with <4 vessels (p = 0.021) and HR of 8.03 in those with ≥4 vessels (p = 0.001). 622 This also was confirmed by systematic review and meta-analysis, specifically separating FTC from all patients with DTC. In the FTC subgroup analysis, vascular invasion was significantly associated with tumor persistence, locoregional recurrence, distant recurrence, and overall recurrence/persistence. Additional subgroup analysis looking at focal (<4 foci) versus extensive (≥4 foci) vascular invasion demonstrated that extensive vascular invasion increased the risk of distant recurrence, with an OR of 26.38. 619
Oncocytic thyroid carcinoma
OTC was previously considered a subset of FTC but more recently has been recognized as a distinct clinicopathologic and genomic entity. The Mayo Clinic retrospectively analyzed 173 OTC cases and through multivariable analysis found those with minimally invasive OTC had no clinical recurrences or death. In contrast, widely invasive OTC (≥4 vessels or ≥4 foci of capsular invasion with minimal extrathyroidal extension), male sex, and higher TNM stage (III–IV) were significantly associated with clinical recurrence and death from OTC. 623 This is consistent with other studies reporting increased recurrence with widely invasive tumors.624–626 In a retrospective multivariable analysis comparing 252 patients with FTC with 126 patients with OTC, Wenter et al. showed that recurrence was significantly more common in OTC at 17% versus FTC at 8%. OTC was an independent adverse prognostic factor for disease-free survival. 627 Bishop et al. also observed that locoregional recurrence associated with OTC more commonly presents as soft tissue implants because of spread within venous channels rather than true lymph node metastases. 628
Lymph node metastasis
Metastatic lymph node size and number are important features when considering risk of structural recurrence. 629 In the 2015 ATA DTC guidelines, those with ≤5 micrometastases (defined as <2 mm) had a low risk of recurrence, and high risk included those with cN1 >3 cm. 14 Since the 2015 guidelines, multiple retrospective analyses have evaluated these parameters. Multivariable analysis of 252 patients with multifocal T1a PTCCGR who had undergone total thyroidectomy and lateral compartment lymph node dissection reported cN1 or lymph node metastases >5 mm were associated with a 25.9% risk of recurrence and pN1 > 3 cm had an HR of 4.2 and a 50% risk of recurrence. 630 Multivariable analysis of 398 patients with N1a PTC reported size >3.5 mm, and ≥4 lymph node metastases had an HR of 3.76 for recurrence. 424 Bardet et al. studied 305 patients with micro- and macroscopic tumors (latter defined as cN1/pN1, i.e., when evident on clinical examination or ultrasound before surgery and/or clearly suspected by the surgeon) and found that tumor size >2 cm had a RR of recurrence of 2.4; macroscopic tumors had a RR of 4.5, and microscopic tumors had a RR of 2.5 for recurrence. 631 Lee et al. also challenged this size cutoff of 3 cm as a predictor of higher risk of recurrence. Multivariable analysis of 324 N1b tumors found that lymph node metastases >2 cm have an HR of 1.15 for recurrence. 456
Further evaluating the number of lymph node metastases, Furtado et al. retrospectively evaluated 86 patients and reported ≤5 clinically evident lymph nodes in the central neck (cN1) predicted a lower risk of persistent disease. Three or fewer clinically metastatic lymph nodes were associated with a 4.6% rate of recurrence, and 9% of those with four or five metastatic lymph nodes experienced recurrence (p = NS). 425 Park et al. evaluated 1040 patients with PTC and reported the sensitivity and specificity of >3 lymph node metastases for predicting recurrence were 63.6% and 77%, respectively. 632 The association between lymph node metastases and survival is controversial. Adam et al. evaluated the association between number of lymph node metastases and survival using both the SEER (21,855 patients) and the NCDB (47,902 patients) and found that an increasing number of metastatic nodes up to six was associated with decreased survival (HR 1.12, p = 0.03), but >6 did not add additional mortality risk (p = 0.75). 633 Conversely, Ruel et al. also evaluated 39,301 patients with PTC ≥1 cm, cN0 or pN1a in the NCDB, and found increased use of RAI but no difference in overall survival if there were no clinically evident lymph nodes involved. 423
LNR has emerged as a potential predictor of recurrence (see
LNY (see
Extranodal extension
According to the 2015 ATA DTC guidelines, pN1 tumors with extranodal extension and >3 metastatic lymph nodes have a risk of recurrence at 40% and suggest a high-risk category. 14 This has been confirmed in multiple studies since those guidelines were published. Roh et al. evaluated 2071 patients who had undergone thyroidectomy, and multivariable analysis showed that both micro- and macro-extranodal extension, the number of positive nodes (>5), LNR of >0.3, and ATA risk group all were independent variables associated with an increased risk of recurrence. 431 Chereau et al. evaluated 2518 patients who underwent surgery for PTC between 1978 and 2014 and reported that extranodal extension and LNR in the lateral neck compartment were independent predictors of recurrence. 636 The association between extranodal extension and recurrence has been reported in many other studies.430,456,637 Macroscopic extranodal extension also is associated with decreased survival. 431 Meta-analysis of 23 studies evaluating extranodal extension and recurrence found patients with extranodal extension had significantly higher rates of all-cause and cancer-specific mortality and recurrence. 429 Hence, extranodal extension appears to predict a high risk of both locoregional recurrence and distant metastasis. Reporting of extranodal extension is currently part of the pathology synoptic report (www.cap.org/protocols-and-guidelines/cancer-reporting-tools/cancer-protocol-templates).
Extrathyroidal extension
In the 2015 ATA DTC guidelines and 7th edition AJCC/UICC staging, 638 microscopic extrathyroidal extension was sufficient for a tumor to be categorized as T3. AJCC 8th edition 27 guidelines no longer incorporate microscopic extrathyroidal extension into TNM staging. This change was made to avoid upstaging of small tumors without other risk factors for aggressive disease. The overall agreement among pathologists regarding identification and reporting minimal extrathyroidal extension is poor (kappa = 0.14). 639
Microscopic (also referred to as minor or minimal) extrathyroidal extension is categorized as low-risk and is associated with a 3–9% risk of recurrence, but extrathyroidal extension into subcutaneous soft tissues, larynx, trachea, esophagus, or the recurrent laryngeal nerve PTC (gross extrathyroidal extension) has a 23–40% risk of recurrence according to the 2015 ATA guidelines. 14 Since the last guidelines, the role of minimal extrathyroidal extension and the risk of recurrence also has been debated. Retrospective analysis of 252 patients with T1a PTC who underwent total thyroidectomy and CLND showed a recurrence rate of 3.8% in those with capsular extrathyroidal extension, 6.6% in those with soft tissue extrathyroidal extension, and 13.3% among those with extrathyroidal extension and strap muscle involvement. 630 In a prospective analysis, Danilovic and colleagues analyzed 596 patients with PTC according to their degree of extrathyroidal extension. They found recurrence in 3% of ATA low-risk patients without extrathyroidal extension, 14% recurrence in ATA intermediate-risk patients without extrathyroidal extension, 14% recurrence in patients with minimal extrathyroidal extension, and 25% recurrence in those with gross extrathyroidal extension. 420 Li et al. retrospectively evaluated 4045 patients and reported recurrence in 22.5% of patients with extrathyroidal extension into strap muscles, and strap muscle invasion was significantly associated with multifocality, lymph node involvement, and distant metastasis; however, it was not independently associated with recurrence. 640 Retrospective review and multivariable analysis of 721 patients with T1a PTC by Seifert et al. reported a 13.1% lymph node recurrence rate in those with minimal extrathyroidal extension compared with those without minimal extrathyroidal extension (1.25%) and a 7.8% distant metastatic disease rate in those with minimal extrathyroidal extension when compared to those without (1.1%). 641 Systematic review and meta-analysis evaluating the impact of strap muscle invasion versus gross extension into surrounding structures concluded that tumors exhibiting strap muscle invasion had a higher risk of recurrence compared with those without any extrathyroidal extension but lower risk than gross invasion. This analysis included six retrospective studies with 13,639 patients. They reported the local recurrence rate of those with strap muscle invasion to be 5–25.9%. The variability was attributed to the extent and location of invasion. There was significant heterogeneity, but even in subgroup analysis, the higher risk of recurrence persisted for strap muscle involvement. Further studies are needed to confirm these findings. 239 In contrast, Diker-Cohen et al. performed a meta-analysis that included 13 studies and concluded that minimal extrathyroidal extension is associated with a minimally increased risk of recurrence; the risk of recurrence was 7% with minimal extrathyroidal extension in tumors >1 cm, which is in the low risk of recurrence category. 642
Microscopically positive margin
Incomplete tumor resection and residual gross disease (R2) are categorized as ATA high-risk. 14 However, the presence of microscopically positive margins (R1) was not a component of the 2015 ATA DTC risk stratification system. Multiple studies have retrospectively evaluated this question, and the majority have found no association between microscopically positive margins and local persistence/clinical recurrence.419,422,643 Sanabria et al. performed a meta-analysis, evaluating six studies that included 7696 patients and found no association between microscopically positive margins and increased risk of locally persistent/recurrent disease. 421 Location of the positive margin (anterior vs. posterior) was not delineated in most of the reported studies, although Lang et al. retrospectively evaluated 638 patients with DTC, 100 of whom had microscopically positive margins. When they differentiated between the two margins, they found a 3.6% rate of recurrence in those patients with a positive anterior margin and 11.6% risk of recurrence in those patients with a positive posterior margin. This led the authors to conclude that a positive posterior margin is an independent risk factor for persistent/recurrent disease (HR = 22.95, p < 0.0001). 419 Retrospective review of >14,000 patients in the NCDB showed that microscopically positive margins are associated with an increased risk of death in both T1a PTC 644 and PTCs 1–4 cm. 645 Mercado et al. reported that recurrence-free survival is lower among patients with positive margins at 71% versus 90% among those with negative margins, regardless of other favorable risk factors. 646 More studies need to be done in this area, with special attention to the difference between anterior and posterior microscopically positive margins to determine the true risk of structural recurrence.
Subtypes of PTC
Since the last ATA DTC guidelines, a new classification of encapsulated follicular variant of PTC has been created, termed NIFTP. Previously, NIFTPs were included as encapsulated variants in the FVPTC category, which could have affected overall risk estimates for recurrence. Henke et al. performed a single-institution, retrospective multivariable analysis evaluating 1293 patients treated for thyroid cancer between 1943 and 2009 comparing classical PTC versus FVPTC (specifically excluding NIFTP from the analysis). The authors found that thyroid capsule invasion was associated with classical PTC and larger size, and tumors confined to the thyroid were associated with FVPTC. Overall, classical PTC was associated with a higher risk of recurrence compared with FVPTC. 647 Tunca et al. evaluated 258 patients with classical PTC and 153 patients with FVPTC and reported similar findings, with higher rates of capsular invasion, microscopic extrathyroidal extension, and lymph node metastases in classical PTC compared with FVPTC. 648 FVPTC had higher rates of multifocality and involvement of both lobes. Recurrence rates were higher in the classical PTC group ≥45 years, but there was no difference among those <45 years when compared with FVPTC. 648 Shi et al. compared classical PTC, FVPTC, and tall cell variant of PTC and found that recurrence was highest in the tall cell variant of PTC at 27.3%, 16.1% in classical PTC, and 9.1% in FVPTC. 109 It should be noted that in WHO 2022 FVPTC is now considered a separate category of DTC and is now termed IEFVPTC (see Pathology section).
Age
Patient age is included in the AJCC staging system and is believed to be a predictor of mortality. However, it has not been included among the ATA Risk of Recurrence predictors. Data are conflicting concerning the role of patient age at diagnosis and risk of recurrence and response to therapy. Several groups have reported older age (generally >45–55 years) in addition to the ATA Risk of Recurrence as predictors of recurrence for the high-risk categories.649–652 Alzahrani and Mukhtar reviewed 287 patients with intermediate- or high-risk DTC and found that patient age ≥55 years was significantly associated with risk of having biochemically or structurally incomplete response to therapy. 653 In a prospective cohort study using the Italian Thyroid Cancer Observatory database, Grani et al. also reported patient age as a variable that, when combined with the ATA Risk of Recurrence stratification system, can more accurately predict rates of persistence and recurrence. 654 However, Pitoia et al. performed a retrospective analysis of 268 patients with DTC and reported age at diagnosis was not associated with structurally incomplete response to therapy. 655 Additionally, Banerjee and colleagues evaluated 9273 patients with thyroid cancer in the SEER-Medicare database to determine factors associated with treatment-free survival and did not see an association with age. 656 Additional studies are needed to determine the overall impact of patient age at diagnosis as an independent predictor of long term outcomes.
Somatic genomic testing
Since the 2015 ATA Guidelines, many investigators have evaluated the role of molecular testing in predicting tumor aggressiveness, response to therapy, and recurrence. Multiple studies and meta-analyses have shown that co-existent BRAFV600E and TERT promoter mutations are associated with more aggressive clinical behavior and a higher risk of recurrence.657–659 A recent meta-analysis demonstrated the association of PTCs with a combination of BRAFV600E and TERT promoter mutations and more aggressive disease, including reduced disease-specific survival (RR 15.09 [CI 7.75–29.37]). 657 This association was more pronounced than for patients with a BRAFV600E mutation alone (RR 5.34 [CI 4.20–6.78]). Recently, the trio of TERT promoter mutation, BRAFV600E, and a BRAF genotype TT of rs2853669 was reported to have an even higher risk of recurrence (76.5%) when compared with tumors with no mutations (8.4%). 660 RAS mutations, in combination with TERT promoter mutations, also have been shown to be a significant predictor of aggressiveness and higher risk of recurrence.254,661,662 One study evaluated 388 patients with PTC from 19 centers within the Thyroid Cancer Genome Atlas (TCGA) thyroid cancer database and measured the outcomes association with BRAFV600E, RAS, and TERT promoter mutations. They reported an adjusted HR for recurrence of 106 [CI 15.3–744.49] for concurrent RAS and TERT promoter mutations and an HR of 6.59 [CI 1.55–27.94] for concurrent BRAFV600E and TERT promoter mutations. 662
RAS mutations in conjunction with EIF1AX mutations also have been associated with PDTC and ATC.261,663–666 In a multicenter retrospective review of 764 patients who underwent total or subtotal thyroidectomy and had molecular testing results, 42 patients (5.5%) were found to have an EIF1AX mutation, but an EIF1AX mutation alone was not predictive of malignancy (38% benign, 14% NIFTP, and 47% malignant). Thirty percent of the cancers had aggressive features; 83% of these were poorly differentiated. All the aggressive malignancies had an EIF1AX A113_splice site mutation (EIF1AX c.338-2A>T, exon 6), and 50% had at least one additional mutation. The authors concluded the co-occurrence of RAS and EIF1AX was associated with more aggressive behavior.
666
Other combinations of mutations, including RAS and BRAFV600E in conjunction with TP53, PIK3CA, and AKT1, also are associated with more aggressive behavior.
258
Some groups have categorized specific mutations, fusions, and copy number alterations into molecular risk of recurrence categories, like the ATA Risk of Recurrence categories based on histology. As discussed in
Another study applied an algorithm to the RNA-Seq expression dataset from the TCGA and assessed progression-free survival in more than 7,500,000 combinations of genes. 257 In total, they identified 82 genes associated with prognosis and divided them into three groups. The group with the highest risk of recurrence had >50% with BRAFV600E mutations; all of those with TERT promoter mutations were in this category. This group also had the lowest tumor differentiation scores, high levels of immune cell infiltrate, and the highest expression of immunoregulatory molecules. Another study reported a gene expression-based score (Molecular Aggression and Prediction [MAP]) composed of markers for cell cycle, differentiation, extracellular matrix, and immune cell infiltrate. 667 A positive MAP score was associated with more aggressive disease. The authors proposed that a positive MAP score in combination with genomic alterations may better predict recurrence and aggressiveness. These reports highlight a fraction of the emerging evidence that the tumor microenvironment also plays an important role in DTC recurrence. More studies are needed to evaluate the predictive role of tumor microenvironment alterations (with or without genomic alterations) as a DTC biomarker.
Overall, these publications shed light on the behavior of tumors with specific molecular alterations and tumor microenvironment findings (Table 8).36,53,54,133,261,269,665,668–703 The molecular risk of recurrence, if it was obtained, should be considered in conjunction with the ATA Risk of Recurrence categories, postoperative Tg levels, and imaging. Additional studies are needed to determine if routine postoperative genomic analysis of histological specimens improves the accuracy of the 2025 ATA Risk of Recurrence categories. Currently, the combination of 2025 ATA Risk of Recurrence category, AJCC staging, imaging, and laboratory results should be the primary approach to determine risk of recurrence. Use of somatic genomic testing to guide treatment for patients with progressive RAI resistant (RAIR) DTC is discussed in
Genomic Changes and Combinations of Events Associated with DTC
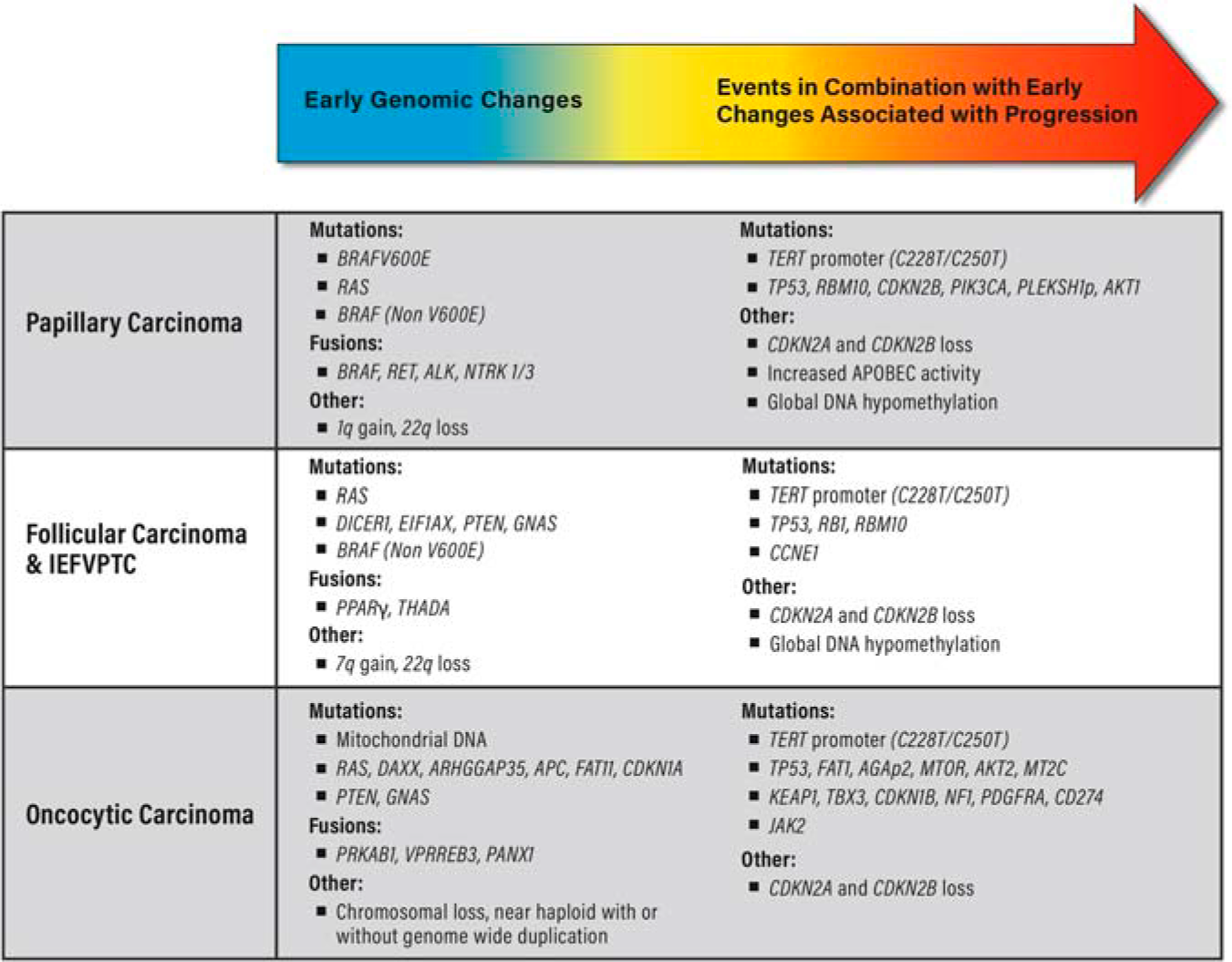
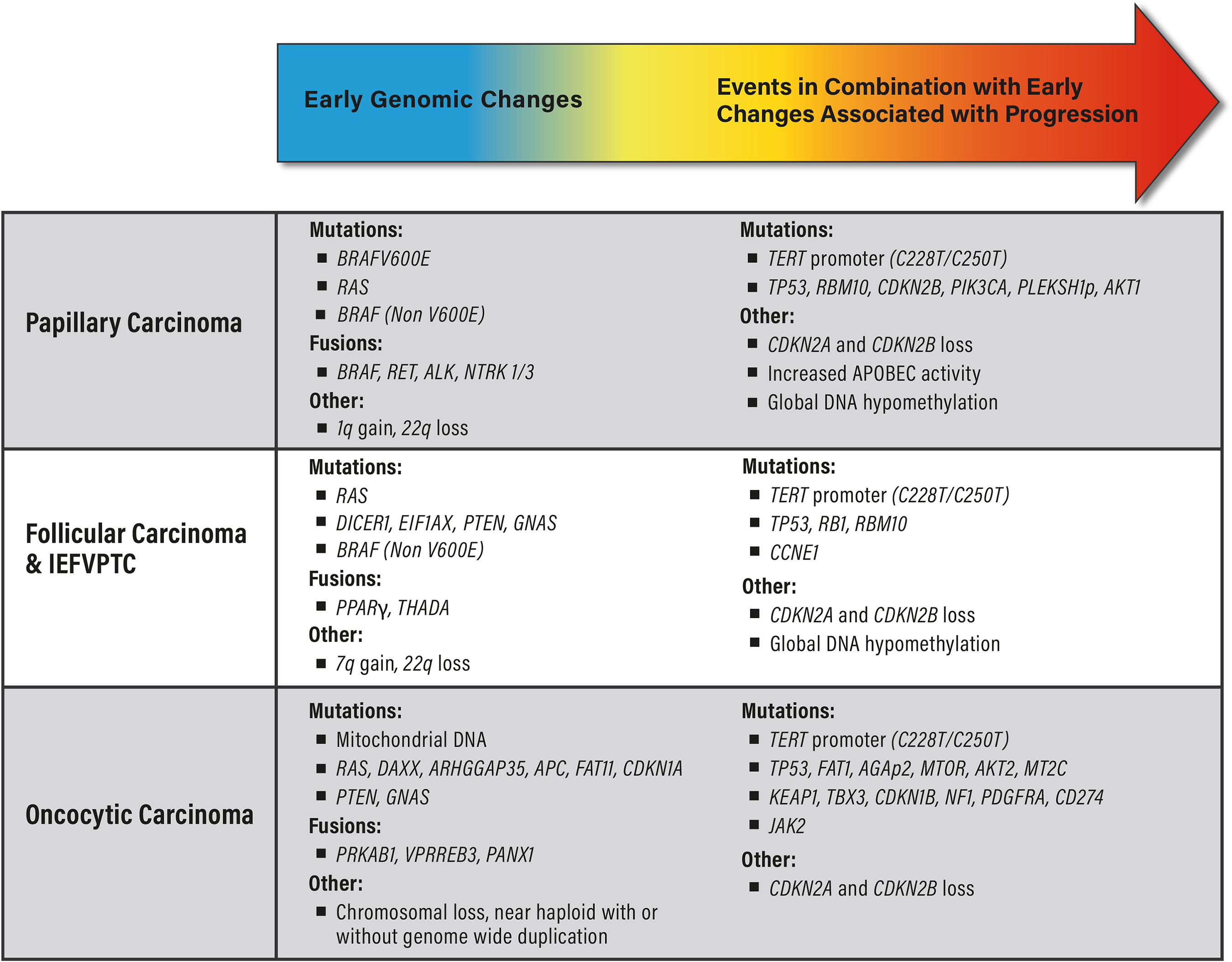
Sex
Male sex has been associated with higher prevalence of advanced stage DTC. 704 Hence, there are questions regarding the role of sex in risk of recurrence. Multivariable analysis reported that sex was not an independent prognostic factor for disease-specific survival. 704 Park et al. evaluated 5566 patients with DTC between 2009 and 2015 in Seoul, Korea, and reported a significantly higher recurrence rate in males compared with females. 705 However, after matching and multivariable analysis, male sex was not an independent prognostic factor for DTC recurrence. In view of the lack of an independent association, sex is not one of the considerations in the ATA Risk of Recurrence prediction modeling.
Body mass index
Overweight, obesity, and elevated body mass index (BMI) have emerged as risk factors for DTC. Two systematic reviews and meta-analyses evaluating the role of BMI and clinicopathologic features of PTC found obesity to be associated with larger tumor size, increased rates of multifocality, extrathyroidal extension, and lymph node metastasis, and these associations increased with higher BMI.706–708 In a prospective cohort study of 4713 patients with thyroid cancer using the Italian Thyroid Cancer Observatory database that includes patients from 40 centers, Grani et al. reported that body composition was predictive of response to therapy but had different impacts depending on the cluster or cohort of patients: it appeared to be protective in some and a risk factor for compromised outcome in others. 654 Greater waist circumference and adulthood weight gain also have been shown to be associated with thyroid cancers at higher risk for recurrence. 709 While not currently part of the ATA Risk of Recurrence predictors, overweight and obesity may play a role in future algorithms.
How should clinical response to surgery be assessed?
▪
The ATA Response Criteria should be used to categorize response to surgery prior to determining intensity of additional therapy or monitoring in combination with the ATA Risk of Recurrence Estimates.
While the ATA Risk of Recurrence and tumor staging estimates provide important insights into a patient’s risk of clinical recurrence and disease-specific mortality, they are not designed for individualization of therapy based on response to treatment. In the 2015 guidelines, the ATA proposed a risk stratification system that incorporates individual response to therapy into a real-time, dynamic risk stratification scheme in order to provide an individualized approach to ongoing management.710,711 While initially proposed for use during long-term follow-up, studies have shown now that many patients initially considered at intermediate- or high-risk of recurrence using the initial stratification systems can be re-classified subsequently to low risk of recurrence based on their excellent response to initial therapy.712–728
With the reduced use of RAI for patients with low risk of recurrence and an increase in the use of thyroid lobectomy, we propose that the first assessment following initial therapy should occur within 3 months after resection. In this way, it can be used to inform patient and physician decision-making for use of RAI and/or to individualize the administered dose. For example, a patient with multiple lymph nodes at high risk of recurrence may be treated with a lower dose if the serum Tg is not detectable on a highly sensitive assay (e.g., lower limit of detection 0.1 ng/mL) in the absence of TgAb during levothyroxine (LT4) administration, and neck ultrasound does not reveal residual disease after operation. Conversely, for the same patient, an elevated Tg level might prompt chest imaging to identify metastases, thereby changing the goals of treatment. More prospective outcome studies are required to support this as an initial approach; retrospective data using the ATA dynamic risk stratification schema support this paradigm during follow-up. Proportion of variance explained values associated with risk stratification systems that incorporate response to therapy variables into revised risk estimates are significantly higher (62 − 84%) than those seen with initial classification systems.712,729 These data indicate that long-term outcomes can be more reliably predictive using systems that respond to new data over time.710,712
The concept and initial validation of the four response categories presented here were described by Tuttle et al.
712
and modified by Vaisman et al.
730
As originally conceived, these clinical outcomes described the best response to initial therapy during the first 2 years of follow-up,710,712 but they are now being used to describe the clinical status at any point during follow-up. Application of these definitions to the postoperative time frame is summarized in Table 9. As described in the Definitions section above, response following tumor resection is categorized as the following:
Response Criteria After Initial Therapy Based on Type of Intervention
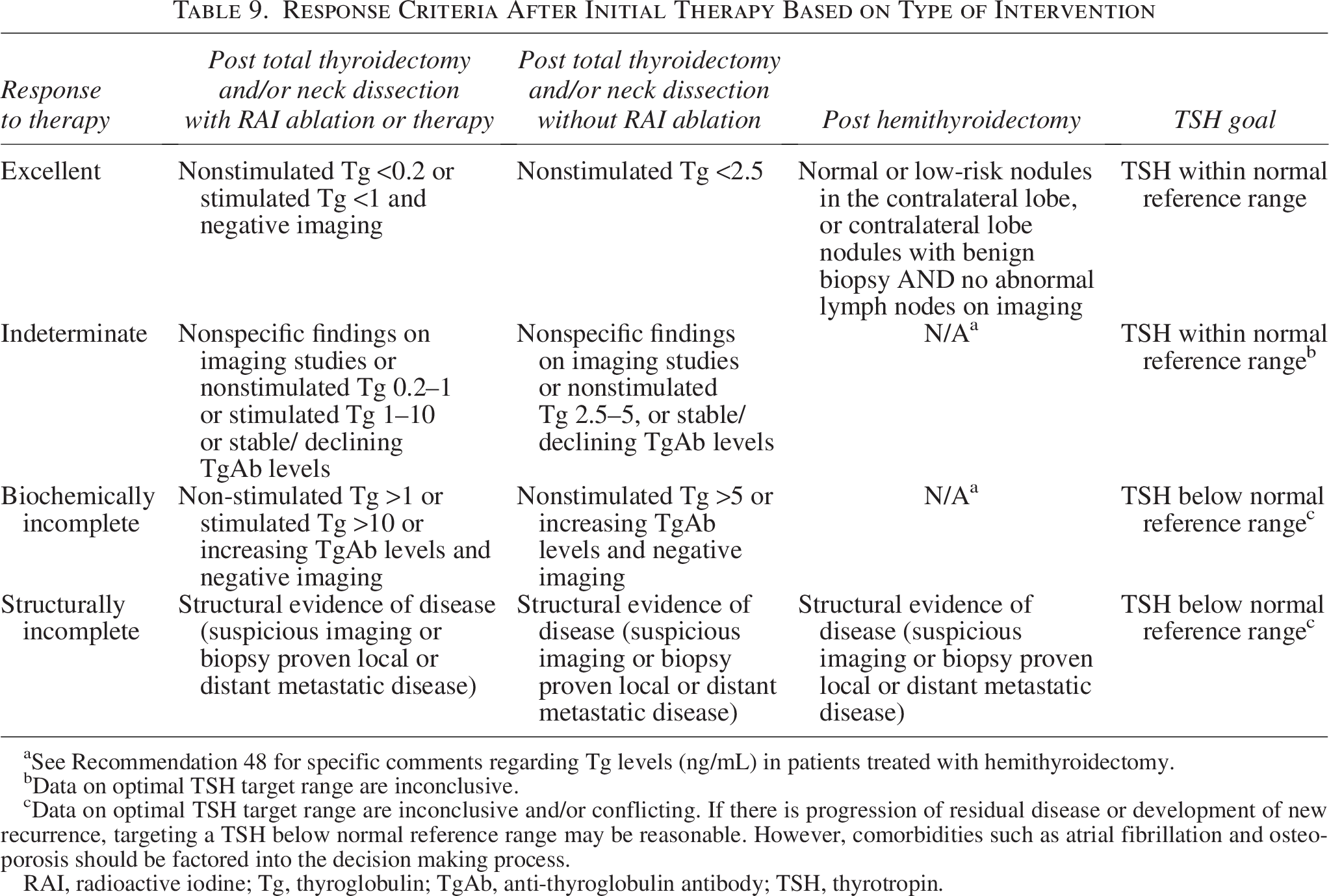
See Recommendation 48 for specific comments regarding Tg levels (ng/mL) in patients treated with hemithyroidectomy.
Data on optimal TSH target range are inconclusive.
Data on optimal TSH target range are inconclusive and/or conflicting. If there is progression of residual disease or development of new recurrence, targeting a TSH below normal reference range may be reasonable. However, comorbidities such as atrial fibrillation and osteoporosis should be factored into the decision making process.
RAI, radioactive iodine; Tg, thyroglobulin; TgAb, anti-thyroglobulin antibody; TSH, thyrotropin.
When should Tg levels be measured after surgery?
▪
Measuring a postoperative serum Tg level 6–12 weeks after total thyroidectomy while on thyroid hormone therapy or after TSH stimulation is recommended. Such measurements may guide additional decision-making regarding clinical management. Measurement of serum Tg on one occasion 6–12 weeks after thyroid lobectomy with a normal TSH may be helpful to ensure that it is not unexpectedly elevated; however, a specific cutoff value is uncertain.
Measurement of serum Tg is a fundamental tool for evaluating thyroid cancer tumor burden, assessing response to treatment, and monitoring for cancer recurrence. Details about assays and antibody interference are included in
A serum Tg level is recommended in the postoperative period to inform treatment decisions. The timing of the initial postoperative serum Tg measurement is guided by a study that performed preoperative and sequential postoperative serum Tg level measurements at multiple time points up to 1 year after surgery. 243 Preoperative serum Tg levels did not distinguish between patients with benign and malignant conditions. The median time to reach the nadir serum Tg after thyroidectomy in patients with both benign and malignant disease was 12 weeks, later than was previously thought.
Measurement of serum Tg after DTC treatment has the potential to provide highly sensitive detection of residual tumor. Serum Tg can be measured when the patient is euthyroid, either with an adequately functioning residual lobe after a thyroid lobectomy on LT4 replacement or while being treated with TSH suppressive doses of LT4. The other circumstances to measure serum Tg is a “TSH-stimulated” measurement, either achieved by stopping LT4 replacement (with or without temporary LT3) in an athyreotic patient and allowing the endogenous TSH to increase (usually >30 mIU/mL) or administering exogenous recombinant human TSH (rhTSH). TSH is a stimulus to Tg production; an individual patient may have a Tg that is in the reference range at baseline but that increases in response to rising TSH.
Both a stimulated Tg level and a basal Tg level have been used postoperatively to identify persistent and to predict recurrent disease, but a benefit of stimulated over basal Tg has not been consistently shown. A retrospective observational study evaluated 1093 patients with DTC with pre-RAI ablation, TSH-stimulated serum Tg and post-RAI, TSH-stimulated serum Tg. 731 The endogenous pre-ablation, TSH-stimulated Tg and recombinant TSH, post-ablation, stimulated Tg levels, as well as an index of serum Tg reduction, were predictors of disease progression and recurrence. Use of unstimulated serum Tg to follow patients not treated with RAI was addressed in a retrospective series of 570 patients with DTC, 187 of whom underwent lobectomy and 320 of whom had total thyroidectomy but did not receive RAI. 732 At a mean follow-up of 8 years, patients who had total thyroidectomy and a serum Tg of <0.2 ng/mL and patients who had lobectomy and a serum Tg <30 ng/mL had an excellent response with no evidence of recurrent structural disease. In a study of 100 patients with DTC who were given additional RAI if they had an elevated serum Tg, 62% of patients had a complete response at one year. Patients were then followed for an average of 96 months. The authors concluded that additional RAI for a persistently elevated serum Tg was associated with improved long-term outcomes. In another small study, 63 patients with DTC had an endogenous TSH-stimulated serum Tg measurement after thyroidectomy but before RAI; a TSH-stimulated serum Tg below 4.4 ng/mL predicted successful response to RAI ablative therapy.
Few studies have examined the association between postoperative serum Tg and DTC survival. An observational study of 1093 patients with DTC who underwent total thyroidectomy and RAI ablation examined the relationship between pre-RAI ablation thyroid hormone withdrawal stimulated serum Tg and ATA risk stratification on 10-year survival. 733 Initial ATA high-risk classification, patient age >55 years, and pre-ablation Tg ≥30 ng/mL were the primary factors associated with reduced 10-year survival. Patients with a stimulated Tg ≥30 ng/mL had a 10-year survival of 78%, compared with 95% for those with a stimulated Tg <30 ng/mL.
Serum Tg has not been shown to predict recurrence in patients with DTC after thyroid lobectomy. A cohort study of 208 patients with low-risk PTC followed serum Tg in patients who underwent lobectomy and did not require LT4 therapy. 734 Postoperative serum Tg, Tg/TSH ratio, and neck ultrasound were followed regularly for a median follow-up period of 6.9 years. The mean serum Tg and Tg/TSH ratio increased gradually, but there was no difference in serum Tg or Tg/TSH ratio in the 19 patients with tumor recurrence. Of those who had recurrence, all but one had a Tg <30 ng/ml, similar to those who did not have a recurrence. The authors concluded that serum Tg level was not predictive of disease recurrence in patients with PTC after thyroid lobectomy. In a retrospective study, 167 patients with PTC who underwent lobectomy were followed with serum Tg and TgAb measurements. 735 At 2 years of follow-up, serum Tg declined in 42% of patients, was stable in 22%, and rose in 36%. After 6 and half years of follow-up, 18 patients required completion thyroidectomy for PTC in the contralateral lobe or had metastatic disease, and serum Tg rose in only 3 of the 18 patients. The authors concluded that serum Tg level was not useful for detecting recurrence in patients with PTC who initially underwent lobectomy.
In view of the importance of understanding the diagnostic accuracy of serum Tg following thyroid lobectomy and total/near-total thyroidectomy without RAI treatment, a subset of the guidelines task force members initiated a systematic review to address this question. 16 A total of 37 studies met the inclusion criteria assessing the diagnostic accuracy of serum Tg in a variety of postoperative settings. Serum Tg measurement following partial thyroidectomy was not accurate for diagnosing DTC recurrence or metastasis. After total/near total thyroidectomy without RAI, there were few studies and very low rates of recurrence or metastasis, but serum Tg levels were usually stable and low. Since most patients who do not receive RAI are in lower risk groups for recurrence, it is difficult to compare the value of serum Tg in this group to the measurements in patients that receive RAI. The systematic review concluded that there was significant variability among the studies with respect to treatment protocols and approaches, but for patients who have undergone total or near-total thyroidectomy without RAI, serum Tg levels up to 1–2.5 ng/mL while on LT4 therapy generally identify patients at low risk for persistent or metastatic disease.
Finally, while it is acknowledged that the data do not support a firm cut-point for Tg monitoring after lobectomy, the task force unanimously felt that measuring a single Tg value ∼12 weeks after surgery with a normal TSH would be prudent to ensure it is not unexpectedly markedly elevated, whereupon further imaging would be appropriate. Additional studies are needed to clarify the optimal approach for monitoring patients after lobectomy.
What is the role of ultrasound and other imaging techniques (CT, MRI, 18FDG-PET-CT) after primary resection?
▪
Ultrasound to evaluate the thyroid bed and central and lateral cervical lymph node compartments is the preferred method of imaging surveillance for most DTC. If the serum Tg level after surgery is above the excellent response range (see Table 9), and/or there are Tg Ab, cervical ultrasound and/or cross-sectional imaging should be performed prior to administering RAI. Six to 12 months following completion of initial therapy, cervical ultrasound to evaluate the thyroid bed and central and lateral cervical lymph node compartments should be performed. Timing and frequency thereafter are informed by the patient’s risk for residual or recurrent disease and response to therapy. Suspicious lymph nodes or lesions <8–10 mm in shortest dimension may be followed without FNA unless they grow or threaten vital structures (such as the recurrent laryngeal nerve, trachea, esophagus, or great vessels). If cytological diagnosis of recurrent or metastatic DTC would influence treatment decisions or change management, ultrasonographically suspicious lymph nodes or lesions ≥8–10 mm in the shortest dimension should be assessed with FNA for cytology and measurement of Tg in the needle washout fluid. When Tg (or TgAb) levels rise following total thyroidectomy for DTC, and cervical ultrasound demonstrates no structural disease or only minimal tumor burden, additional cross-sectional imaging to evaluate common metastatic sites (e.g. lungs and bone) should be performed. When Tg (or TgAb) levels rise following total thyroidectomy for OTC and PDTC, and cervical ultrasound demonstrates no structural disease or shows only minimal tumor burden, 18FDG-PET/CT may be considered.
Cervical ultrasound is performed with a high-frequency probe (10 MHz) and is highly sensitive in the detection of cervical metastases in patients with DTC.736–738 These studies primarily evaluated patients with PTC, and the utility of neck ultrasound for monitoring patients with low-risk FTC is not well established. Neck ultrasound should interrogate all lymph node compartments and the thyroid bed. Limitations of ultrasound in the central compartment with the thyroid in place 738 should not limit detection of central neck recurrences after thyroidectomy, but ultrasound may not distinguish thyroid bed recurrence or nodal progression from benign gland remnants.739,740 Masses in the thyroid bed that are <6 mm in shortest dimension are seldom malignant; punctate echogenicity is worrisome. 741 During the first year after resection in patients with low serum Tg levels on thyroid hormone therapy (and without any other suspicious findings), if an ultrasound abnormality is found, then follow-up should be performed. Efficacy of ultrasound is operator-dependent; it is not uncommon for some team members involved to lack confidence in their ability to perform ultrasound.171,742 Whether ultrasound is best undertaken by radiologists, endocrinologists, cytopathologists, or surgeons is likely to vary from one center to another. In patients with PTC found to be at low risk for recurrence after total thyroidectomy (based on serum Tg measures and first follow-up neck ultrasound), there is a high incidence of false positive findings that may engender additional fruitless testing. 743 While the utility of follow-up in young patients without biochemical or ultrasound evidence of recurrence at 12 months has been questioned in view of the low frequency of structural recurrence, 744 on 10-year follow-up of 253 patients with PTC, 5 of 11 recurrences developed between 20 and 60 months after total thyroidectomy. 736 Correlation between ultrasound findings and surgical pathology 745 has shown that for lymph nodes ≥8–10 mm in shortest diameter, a cystic appearance or hyperechoic foci in patients with a history of DTC should be considered malignant. In addition, peripheral vascularity is worrisome, with a high sensitivity/specificity for malignancy. With such findings, FNA biopsy is justified. A hyperechoic hilum and central vascularity are reassuring. A round shape, hypoechoic appearance, or the loss of the hyperechoic hilum does not, as isolated findings, justify FNA biopsy.
Interpretation of neck ultrasound should reflect additional clinical and biological information. The risk of recurrence is closely related to the initial lymph node status. Most lymph node recurrences occur in already involved compartments; the risk increases with increasing number of involved lymph nodes and a greater number of lymph nodes with extranodal extension, 746 with macroscopic rather than microscopic lymph node metastases,629,747 and with higher metastatic LNRs.748,749
In low- and intermediate-risk patients after total thyroidectomy, the risk of lymph node recurrence is low (<2%) if there is an undetectable serum Tg level; it is much higher in those patients with detectable/elevated serum Tg levels.750,751 One gram of DTC should increase the serum Tg by ∼1 ng/mL during thyroid hormone treatment and by ∼2–10 ng/mL following TSH stimulation. 750 Neck ultrasound can detect involved nodes as small as 2–3 mm in diameter (among patients where the serum Tg level may be low or undetectable) but benefit from early discovery (when the smallest diameter is ≤8–10 mm) has not been demonstrated.
If diagnosing recurrent cancer will influence clinical decisions, then FNA biopsy for cytology and Tg measurement in the aspirated fluid generally should be performed for suspicious lymph nodes ≥8–10 mm in their shortest dimension. Ultrasound guidance improves the results of FNA biopsy for small lymph nodes and those located deep in the neck. However, FNA cytology alone misses thyroid cancer in up to 20% of patients.752,753 The combination of cytology and serum Tg determination in the aspirated fluid (which remains valid even if there in an environment of serum TgAb) increases sensitivity as described in
Tg measurement in the aspirated fluid should be compared with serum Tg measurement (secured on the same day, prior to the FNA) in most patients. FNA for Tg determination is technically demanding and has not been standardized. Variations in needle gauge, diluent volume, processing time, and number of punctures all have the potential to limit accuracy and reproducibility.757,758 Nodes without suspicious morphology and small, worrisome nodes (<8–10 mm in shortest dimension) can be managed expectantly.
Most patients with recurrent DTC will only have disease in the lymph nodes. The most common sites of extra-cervical metastases are the lung and bone, comprising more than 80%; pulmonary metastases represent the majority. 759 While well recognized, intra-abdominal and retroperitoneal disease is uncommon. Cutaneous metastases are detectable by examination. Hence, initial cross-sectional imaging should not be directed to sites other than lung and bone when screening for distant disease in the absence of ultrasound-detected cancer in cervical lymph nodes or the thyroid bed.
What is the role of RAI after thyroidectomy in the primary management of DTC?
▪
Remnant ablation is not recommended routinely after total thyroidectomy for patients with ATA low-risk DTC. RAI adjuvant therapy may be considered after total thyroidectomy in patients with ATA low-intermediate and intermediate-high risk of recurrent DTC. RAI adjuvant therapy is recommended routinely after total thyroidectomy for patients with ATA high-risk DTC. In patients with an initial diagnosis of DTC with distant metastases, RAI therapy is recommended routinely after total thyroidectomy.
Our recommendations regarding utilization of RAI and goals of therapy are adapted from the Martinique guidelines 760 and are summarized in Table 10. Important definitions include the following:
Summary of Recommendations for Initial RAI Following Thyroidectomy a
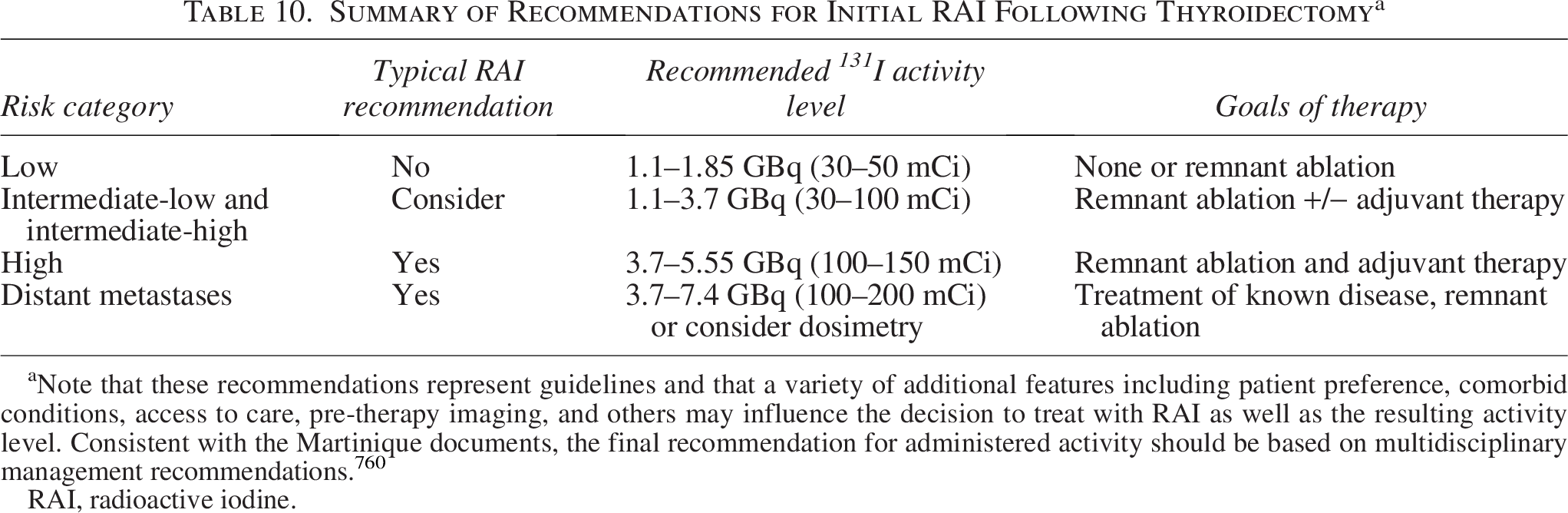
Note that these recommendations represent guidelines and that a variety of additional features including patient preference, comorbid conditions, access to care, pre-therapy imaging, and others may influence the decision to treat with RAI as well as the resulting activity level. Consistent with the Martinique documents, the final recommendation for administered activity should be based on multidisciplinary management recommendations. 760
RAI, radioactive iodine.
Remnant ablation
Eliminate residual benign thyroid tissue in the thyroid bed to facilitate treatment monitoring.
Adjuvant therapy
Additional RAI administered to reduce the risk of recurrence.
Treatment of known disease
Treatment of known areas of residual/metastatic disease.
Postoperative RAI administration can be used to accomplish remnant ablation, adjuvant therapy, or treatment for known residual disease. When deciding if RAI is appropriate, a variety of patient- and tumor-specific features should be considered. These include the histopathology of the thyroid cancer, concurrent comorbidities, serological biomarkers and metabolic function panel, logistic feasibility for post-treatment isolation recommendations and follow-up evaluation, and patient concerns and preferences.
Imaging and molecular genetic profiles features have been associated with favorable response or treatment resistance. Notably, favorable response to RAI therapy has been observed in tumors harboring RAS mutations and RET fusions, while resistance is more frequently observed in DTCs harboring BRAFV600E, TERT promoter, and/or TP53 mutations.761–763
The presence of concomitant BRAFV600E and TERT promoter or TP53 mutations is associated with loss of 131I avidity and poor clinical outcomes.764,765 These findings have motivated the development of strategies beyond administration of higher doses of 131I to overcome resistance to RAI, such as redifferentiation therapy (see
ATA low-risk
There is increasing evidence suggesting lack of a clinical benefit of RAI in ATA low-risk thyroid cancer, particularly for patients categorized as having an excellent response after surgery. A multi-institutional, retrospective study followed 1298 patients with ATA low-risk DTC for a median of 10.3 years and determined that there was no benefit of RAI therapy with respect to overall or disease-free survival. 767 The National Thyroid Cancer Treatment Cooperative Study Group (NTCTCSG) also found that RAI treatment for patients with Stage I and II DTC does not influence disease-specific and disease-free survival.768,769 However, it is important to note that studies are limited in truly determining RAI-associated outcomes due to the low incidence of disease-related mortality and morbidity in this cohort. As a result of these studies, the 2015 ATA guidelines determined that RAI should not be administered routinely for Stage I and II DTC. Since then, several prospective studies have been published regarding RAI administration in patients with low-risk DTC. A randomized Phase III trial (ESTIMABL2) evaluated 776 patients with low-risk DTC treated with total thyroidectomy with or without prophylactic lymph node dissection (pT1a N0 with a sum of the diameters of tumor lesions ≥10mm, pT1b N0). 770 Two to 5 months after surgery, in the absence of suspicious lateral neck lymph nodes demonstrated on ultrasound, patients were randomized either to the follow-up group (no RAI) or to the ablation group (1.1 GBq following rhTSH stimulation). Of the 730 patients, the percentage of patients without an event was 95.6% in the non-RAI group compared with 95.9% in the RAI group, which met noninferiority criteria. This Phase III clinical trial demonstrated noninferiority of a follow-up strategy when compared with systematic adjuvant postoperative administration of RAI in patients with low-risk DTC. 770 One potential limitation of these studies is the relatively limited duration of follow-up.
In the select cases where RAI is employed in low-risk patients based on postoperative risk assessment, a low dose of 1.1–1.85 Gbq (30–50 mCi) of 131I should be administered to reduce the potential for side effects. This conclusion is supported by another open label, randomized controlled factorial trial (HiLo). In this study, 438 patients were split evenly into two groups who received either low-activity RAI (1.1 GBq) or high-activity RAI (3.7 GBq, 100 mCi); they were followed for a median of 6.5 years. The authors found that the cumulative recurrence rates were similar between the low and high activity groups (3 years, 1.5% vs. 2.1%, respectively; 5 years, 2.1% vs. 2.7%; and 7 years, 5.9% vs. 7.3%; HR 1.10 [CI 0.47–2.59]; p = 0·83). 771 This suggested that use of low-dose RAI for patients with low-risk DTC is noninferior to use of a higher RAI dose as measured by risk of recurrence. 763 Similar findings were observed at 5 years of follow-up in the ESTIMABL1 trial. 764
ATA intermediate-risk (low-intermediate and high-intermediate)
Despite limited risk-group specific data examining RAI efficacy, RAI adjuvant therapy should be considered in patients with ATA intermediate-risk DTC. Data summarized in the 2015 ATA guidelines suggested that the greatest potential benefit of RAI in this patient cohort may be observed in those with adverse thyroid cancer histopathologies, extensive nodal disease including metastatic nodal disease outside the central neck, postoperative Tg level, and in older patients.
772
In the 2025 guidelines, we have divided this category into low-intermediate and high-intermediate, as not all criteria within the intermediate category predict the same risk of recurrence (Fig. 2 and
Recent studies support the guideline recommendations to administer RAI in this risk group. In a recent analysis of the NCDB, a total of 21,870 patients with intermediate-risk DTC who underwent total thyroidectomy with or without RAI administration were included and followed for an average of 6 years post-RAI. A total of 15,418 (70.5%) received RAI, and 6452 (29.5%) did not. In a multivariable logistic regression model, which adjusted for demographic and clinical factors, RAI treatment was associated with a 29% reduction in the risk of death, with a hazard risk of 0.71 [CI 0.62–0.82; p < 0.001]. For those less than 45 years of age, RAI usage was associated with a 36% reduction in risk of death, with a hazard ratio of 0.64 [CI 0.45–0.92; p = 0.016). In contrast with the findings from prior literature, this study demonstrated improved overall survival in patients with intermediate-risk DTC treated with RAI in both younger (<45 years) and older (>65 years) patients. 775 Similarly, Verburg et al. evaluated 11 retrospective cohort studies in a systematic review, where some demonstrated a benefit of RAI treatment even in T1a PTCs, while others showed no benefit. The authors concluded that unless further randomized prospective studies are conducted which generate other findings, 131I administration should be considered in all patients with intermediate-risk DTC with a primary tumor diameter exceeding 1 cm. 777
One additional benchmark comes from the prospective randomized Adjuvant Selumetinib for differentiated Thyroid cancer, Remission After RAI (ASTRA) trial designed to study use of redifferentiation therapy with selumetinib for first-line RAI treatment. In this study, 62% of patients treated without redifferentiation had persistent or recurrent structural disease after 18 months, raising concern about efficacy of such therapy. 778 However, this study was not designed to evaluate the efficacy of RAI alone. Finally, Tian et al. performed a retrospective analysis of 1349 patients who were treated with RAI versus 138 who were not; they found that not receiving RAI was an independent risk factor for structural and biochemical recurrence and that the non-RAI group had less favorable recurrence-free survival. 779 There are few studies that have evaluated RAI in a cohort of patients who are uniquely at intermediate risk or that can be classified as low-intermediate or intermediate-high risk of recurrence, limiting strong recommendations. Further studies are needed in this group of patients, including those that incorporate somatic genomic testing. RAI adjuvant treatment should be considered for intermediate-risk patients with an administered activity generally ranging from 1.1–3.7 Gbq (30–100 mCi) of 131I, considering the potential survival and disease-free benefits and limited adverse effects.
ATA high-risk
Several prior studies have demonstrated the overall benefit and need for administration of RAI in high-risk patients, as was recommended in the 2015 ATA guidelines. Data from SEER suggest that postsurgical RAI therapy is associated with improved overall survival in patients with PTC and distant metastases (when distant metastases are combined with an age >45 years, tumor size >2 cm, and metastatic lymph nodes at primary diagnosis). 780 SEER data showed that patients with FTC with distant metastases who were treated with postsurgical RAI had double the overall survival when compared with their counterparts who did not receive RAI. 773 The recommendation therefore remains that postsurgical RAI should be administered to patients with ATA high-risk DTC. The suggested activity of 131I for this group of patients when dosimetry is not available should be 3.7–5.55 GBq (100–150 mCi). For higher doses, especially doses greater than 7.4 GBq (200 mCi), dosimetry is recommended to reduce risk of adverse effects. When RAI is intended for initial adjuvant therapy to treat suspected microscopic residual disease, administered activities up to 5.55 GBq (150 mCi) are generally recommended (in the absence of known distant metastases).
Patients with known distant metastases
In patients with initial diagnosis of DTC and distant metastases, RAI therapy is routinely recommended after total thyroidectomy. In this cohort, 131I activity of at least 3.7 GBq (100 mCi and often greater) is recommended to achieve tumor control. There are two main approaches to choosing the 131I dose in patients with metastatic DTC: empirical and dosimetry-based treatment. In the first one, most delivered activities are 3.7GBq (100 mCi), 5.6 GBq (150 mCi), or 7.4 GBq (200 mCi), and the dose is selected based on patient parameters, the nuclear medicine physician experience, and patient preferences. An alternative strategy is the use of dosimetry employing either maximum tolerated activity (MTA) or lesional dosimetry methods. 781 The goal of MTA dosimetry is to identify the maximum dose that can be administered without exceeding empirically determined thresholds associated with higher risk of toxicity (a dose to the blood of 2 Gy or more, or whole body retained activity of 4.5 GBq or 3.0 GBq in the case of patients with diffuse lung metastases). The routine application of administered activities greater than 5.55–7.4 GBq (150–200 mCi) may exceed the MTA. Tuttle et al. 782 retrospectively analyzed 535 dosimetry studies performed as part of routine clinical care in 328 patients with hypothyroid with apparently normal renal function. They found that administration of 9.25 GBq (250 mCi) would exceed the MTA in 22% of patients <70 years and 50% of patients ≥70 years. Factors associated with a lowering of MTA to less than 9.25 GBq (250 mCi) were age at dosimetry >45 years, female sex, subtotal thyroidectomy, and 131I-avid diffuse bilateral pulmonary metastases. In conclusion, they suggest that dosimetry-guided RAI therapy may be preferable to fixed-dose RAI treatment strategies in older patients with thyroid cancer and in patients with 131I-avid diffuse bilateral pulmonary metastases (even when renal function is normal). 782 These results are further supported by Kulkarni et al. 783
Klubo-Gwiezdzinska et al. compared the treatment efficacy and side effects of dosimetry versus empirically guided therapy. 784 In this retrospective study, the authors found a lower rate of progression and a higher rate of remission in the dosimetry-guided group. Deandreis et al. retrospectively analyzed 352 patients with 131I-avid metastatic DTC treated with RAI by an empirical fixed activity of 3.7 GBq (GR, n = 231) or by personalized activity (2.7–18.6 GBq) based on whole-body/blood clearance dosimetry at a single center (n = 121). 778 No difference was identified in 5-year overall survival, and they concluded that routine use of whole-body dosimetry without lesional dosimetry provided no overall survival advantage when compared with empirical, fixed RAI activity in the management of patients with DTC with 131I-avid distant metastases. 778 There is a need for prospective clinical trials to evaluate the ideal RAI dose for metastatic DTC. Until further studies are completed, the suggested administered activity is 3.7–7.4 GBq (100–200 mCi), and dosimetry should be considered for appropriate cases, particularly for patients of advanced age and/or diffuse lung metastases or renal failure.
Should radioiodine be administered for OTC treatment?
▪
Outcome data are limited in OTC; thus, specific recommendations regarding use of RAI are not certain. If RAI is not administered empirically, evaluation of iodine avidity with a diagnostic whole-body scan (WBS) may be considered.
Several small retrospective studies have evaluated the impact of RAI treatment for patients with OTC with inconsistent results. One review of 32 patients with OTC and distant metastasis reported that 53% of the 30 patients (94%) who received RAI demonstrated iodine-avidity; over the 8.3 years reviewed in the study, the median number of RAI treatments was 4 (1–10 doses), with a median cumulative administered activity of 34.1 GBq (922 mCi) (range, 8.5–56.4 GBq, 230–1523 mCi). 785 Two larger studies, one with 239 patients 786 and the other with 2799 patients, 787 showed conflicting results when comparing the impact of RAI on survival in patients with OTC. Oluic et al. reported no impact on overall survival or disease-specific survival with RAI; they suggested an impact on disease-free survival on univariable analysis but not multivariable analysis. 786 Yang et al. reported that RAI was associated with improved overall survival but not disease-specific survival. 787 NCDB review of 1909 patients with OTC reported that 60.9% received RAI therapy, with improved 5-year and 10-year overall survival. 788
In contrast, three retrospective studies described below showed no benefit of RAI in patients with OTC. A single-institution review with 50 years of follow-up data reported 41% of the 48 patients with OTC after total thyroidectomy received RAI therapy, but this did not impact disease-free survival. 625 A SEER database review of 172 patients with OTC reported that RAI appeared to have no impact on survival for the 33% of patients who received RAI therapy. 789 A third study of 89 patients with OTC reported that RAI treatment had no impact on survival for the 16% of patients who received it. In this same report, all patients who had distant metastasis underwent initial iodine WBS, with only 3 of 33 patients (9%) with bone metastasis showing avidity and 2 of 27 patients (7%) with lung metastasis showing avidity. 790 Improved ability to employ Tg levels to facilitate monitoring in patients with low- and high-intermediate or high-risk OTC may serve as a potential rationale for RAI administration for individual patients. In sum, current data preclude a definitive recommendation with respect to RAI; further research is needed.
How should patients be prepared for RAI administration?
▪
In patients with DTC in whom RAI remnant ablation or adjuvant therapy is planned, preparation with rhTSH stimulation is preferred over thyroid hormone withdrawal. In patients with DTC of any risk level with significant comorbidity that may preclude thyroid hormone withdrawal prior to RAI administration, rhTSH preparation should be considered. If thyroid hormone withdrawal is planned prior to RAI therapy or diagnostic testing, LT4 should be withdrawn for 3–4 weeks. If LT4 is withdrawn for ≥4 weeks, substitution of LT4 with liothyronine (LT3) in the initial weeks should be considered. In such circumstances LT3 should be withdrawn for at least 2 weeks. Serum TSH should be measured prior to radioisotope administration to evaluate the degree of TSH elevation. A goal of TSH >30 mIU/L should be employed in preparation for RAI therapy or diagnostic testing. In patients with known distant metastases, either LT4 withdrawal or rhTSH can be used for preparation.
Early observational research established that TSH stimulation is required before RAI ablation/therapy or scanning. It is recommended that a TSH level >30 mIU/L be established in preparation for successful RAI absorption. TSH stimulation can be achieved by either thyroid hormone withdrawal or rhTSH stimulation. Lee et al. reported on an open-label, single-center study with 291 patients with DTC randomized to (a) withdrawal of LT4 for 4 weeks (n = 89), or (b) withdrawal of LT4 for 4 weeks with substitution of LT3 for the first 2 weeks (n = 133), or (c) recombinant human TSH (with withdrawal of LT4 for a few days from the time of the first rhTSH injection to radioisotope administration) (n = 69). 791 All patients received RAI with 1.1 GBq (30 mCi) for remnant ablation and were prescribed a low-iodine diet pre-ablation for 2 weeks. The baseline characteristics (including pre-ablation urinary iodine measurements) were well balanced among groups. The pre-ablation TSH was >30 in all patients in this trial, with no significant difference in mean pre-ablation TSH levels. The primary outcome, which was the rate of successful remnant ablation at 12 months, did not differ between groups (range, 91.0–91.7%). Administration of questionnaires in a double-blinded fashion found no significant difference in QoL during preparation for RAI ablation between the LT4 withdrawal group and the LT4 withdrawal with LT3 substitution group; however, QoL in both withdrawal groups before ablation was significantly worse than after rhTSH preparation. 791 Therefore, direct LT4 withdrawal or LT4 withdrawal with substitution of LT3 in initial weeks seem to be associated with similar short-term QoL and hypothyroidism symptoms; remnant ablation success rates appear to be comparable between all preparation methods.
There has been some uncertainty about the optimal TSH level following thyroid hormone withdrawal and before RAI administration when long-term outcome effects are considered. There is conflicting observational evidence surrounding whether any specific TSH level pre-RAI administration is associated with greater success at remnant ablation.792,793 Fallahi et al. reported that a pre-RAI TSH level of >25 mIU/L following LT4 and LT3 thyroid hormone withdrawal was associated with a significantly increased likelihood of successful remnant ablation (OR 2.36 [CI 1.28–4.35]; p = 0.006) after adjustment for RAI activity, baseline serum Tg, on-LT4 TSH level, patient sex, age, histology, baseline RAI uptake, and extent of surgery. 792 According to a more recent retrospective study, 689 patients were categorized into three groups (TSH levels of <30, 30–70, and ≥70 mIU/L), and the response to RAI was evaluated after a follow-up of 6–8 months. They found that a pre-RAI TSH level of 30–70 mIU/L has a higher rate of complete response compared with a TSH level of <30 mIU/L. 794 However, in another recent retrospective study that included 1873 patients without distant metastases referred for postoperative adjuvant RAI, Vrachimis et al. reported that TSH levels at the time of RAI are not related to ablation success rates, recurrence-free survival, or DTC-related mortality. 795 Most patients enrolled in the previously mentioned study (around 80%) were low-risk, so findings should not be extended to other risk groups.
rhTSH is currently approved by the U.S. Food and Drug Administration (FDA) and Health Canada for use in preparation for RAI remnant ablation in patients who have undergone a near-total or total thyroidectomy for DTC and who do not have evidence of distant metastases. Data from a compassionate use, observational study suggest that rhTSH raises serum TSH measurements in patients who are unable to mount an endogenous TSH increase and reduces the risk of hypothyroid-related complications in patients with significant medical or psychiatric comorbidities. 796 rhTSH therefore is the preferred approach for patients with significant medical (central nervous system or respiratory compromise, congestive heart failure, coronary artery disease) or psychiatric diseases in whom a hypothyroid state can produce serious complications. 796
Preparation with rhTSH for RAI for adjuvant therapy also is the preferred method of preparation for such patients who do not have evidence of distant metastases based on data demonstrating similar efficacy and fewer side effects versus thyroid hormone withdrawal. Several randomized controlled trials in patients with low- and intermediate-risk DTC have measured remnant ablation outcomes using rhTSH compared with thyroid hormone withdrawal, concluding that there are no differences between the two methods. 797 Data from 1535 patients across seven clinical trials were described in a meta-analysis that suggested that the rates of remnant ablation success did not differ significantly using rhTSH compared with thyroid hormone withdrawal (risk ratio 0.97 [CI 0.94–1.01]). 797 A pooled analysis suggested that QoL was superior on the day of remnant ablation in the rhTSH group, with no significant difference between the groups 3 months later. 797 Another meta-analysis including six of the previously mentioned randomized controlled trials also suggested that the success of remnant ablation did not differ between patients prepared with rhTSH or thyroid hormone withdrawal. 798 Patients who underwent thyroid hormone withdrawal had a worse health-related QoL outcome, attributed to hypothyroid symptoms.798–800
Prospective data comparing rhTSH with thyroid hormone withdrawal are lacking for patients with DTC with distant metastases. However, in a retrospective analysis of 175 patients with iodine-avid metastatic disease to lungs and/or bone, the authors observed no significant difference in overall survival after a mean follow-up period of 5.5 years between patients prepared with rhTSH alone for all RAI treatments, thyroid hormone withdrawal for all RAI treatments, or thyroid hormone withdrawal for initial treatment followed by rhTSH for subsequent treatment(s). 801 In this study, whole-body and blood dosimetry studies were performed in all patients; therefore, the results should not be extrapolated to RAI fixed dosing. Some important differences between groups in this study that could have affected the findings included differences in cumulative RAI activities received and longer follow-up in groups who had thyroid hormone withdrawal. 801 Although the authors performed a multivariable analysis examining predictors of overall survival (finding that the method of thyrotropin stimulation was not significant), their model did not adjust for all variables. In a two-center retrospective analysis comparing responses with treatment using RECIST 1.1 criteria in 56 patients with distant metastatic disease prepared with either rhTSH or thyroid hormone withdrawal prior to RAI administration, there were also no differences in outcomes between groups after a mean follow-up of about 6 years. 802 There were important baseline differences between groups, such as rates of use of dosimetry and mean cumulative RAI activity. Rates of xerostomia, leukopenia, or thrombocytopenia did not differ significantly between treatment groups. The overall mortality rate was 20% in the rhTSH group (3/15) and 7.3% in the thyroid hormone withdrawal group (3/41, p = 0.188), 802 although the study was probably not large enough to assess differences in this important outcome. The findings of the study cannot be readily extrapolated to fixed dosing RAI treatment regimens, because 80% of the individuals in the rhTSH group and 46% in the thyroid hormone withdrawal group received dosimetry-based RAI treatment. Randomized controlled trials comparing rhTSH with thyroid hormone withdrawal preparation pre-RAI treatment are needed to guide clinical care in patients with high-risk DTC.
Another scenario in which rhTSH is the preferred method of preparation is for patients with limited pituitary gland function due to previous head trauma/surgery/radiation and patients with obesity. In these settings, the patient would often have a suboptimal TSH elevation despite thyroid hormone withdrawal. It is important to consider that secretory metastatic DTC and large thyroid remnants may also cause suboptimal TSH response to hormone withdrawal; therefore, this uncommon possibility should be excluded.
Should a low-iodine diet be prescribed prior to RAI administration?
▪
A low-iodine diet for approximately 1–2 weeks should be used for patients undergoing RAI remnant ablation or treatment.
There are currently no randomized controlled trials that assess the impact of a low-iodine diet on the efficacy of RAI for any of its uses, limiting the strength of this recommendation. A low-iodine diet is generally defined as a restriction in iodine consumption to <50 mcg/day. Consultation prior to the administration of RAI should include a series of questions to confirm adherence to a low-iodine diet and exclude other known high-dose iodine sources (e.g., intravenous contrast within 3 months or amiodarone use) to prepare for the optimal timing of RAI imaging/therapy. Although urinary iodine should not be used to determine an individual’s long-term iodine status, it can be employed as a measure of iodine intake over the prior several days to confirm patients’ compliance with a low-iodine diet or to ensure clearance of amiodarone or IV contrast.
However, there are unresolved questions regarding the actual impact of a low-iodine diet on the outcome of remnant ablation, 803 with the best available evidence largely restricted to retrospective analyses using historical controls.804,805 In a study including 120 patients, the use of a 4-day low-iodine diet (with seafood restriction for 1 week) was associated with a higher rate of remnant ablation success (defined by absent neck activity and stimulated Tg <2 ng/mL) compared with normal diet. 804 In a study of 94 patients comparing a more stringent low-iodine diet with a less stringent diet of restricted salt/vitamins/seafood, each for 10–14 days, there was no significant difference in the rate of successful remnant ablation, using a visually negative WBS to define outcome. 805 The optimal stringency and duration of a low-iodine diet (if any) prior to therapeutic RAI administration are not known. In a randomized controlled trial including 46 patients, the increase in uptake and reduction in urinary iodine excretion did not significantly differ between patients who followed a low-iodine diet for 2 weeks compared with 3 weeks prior to RAI scanning, 806 suggesting that there may be little reason to extend the low-iodine diet beyond 2 weeks. A lack of association between urinary iodine excretion and the rate of successful thyroid ablation has been reported in patients not specifically prescribed a low-iodine diet 807 ; absence of a specific low-iodine diet comparison group in this study may limit the generalizability of the findings to situations where a specific low-iodine diet is prescribed. Notably, high urinary iodine and excessive iodine uptake have been linked to failure of remnant ablation. 808 More recent studies support 1–2 weeks as the optimal duration for a low-iodine diet.809–811
Although low-iodine diets may be cumbersome or unpalatable, serious side effects are relatively infrequent, 803 with case reports of potentially life-threatening hyponatremia occurring most often in patients who (i) are elderly and subject to thyroid hormone withdrawal, (ii) have metastatic disease, (iii) are concurrently treated with thiazide diuretics, and (iv) are on a low-iodine diet for longer than a week. 812 It is important to avoid restriction of non-iodized salt during the low-iodine diet, since this may be associated with hyponatremia, especially in patients undergoing thyroid hormone withdrawal.
When and how should diagnostic radioiodine WBS be performed?
▪
Postoperative diagnostic 123I or low-dose 131I WBS may be considered for patients undergoing RAI treatment prior to their therapeutic (ablative, adjuvant, or treatment) administration to help guide treatment planning.
RAI is a theranostic agent, as it provides both imaging and therapy in patients with DTC. Imaging with RAI is performed using either 123I or low-dose 131I WBS. Other methods including 124I positron emission tomography (PET) are employed in investigational settings. A variety of methods for WBS with 123I have been proposed and implemented. In many cases, 123I may be preferred for scanning due to the lower radiation dose and less concern for “stunning,” 813 where diagnostic activity of RAI is thought to reduce subsequent uptake of the therapeutic dose. However, this concept is controversial and possibly related to destruction of thyroid tissue by the diagnostic dose of 131I.814,815 In some cases, 131I may be preferred due to lower cost. In practice, both options are considered reasonable, 816 although 123I may be preferable if it is available. 817 When performed, diagnostic WBS should follow patient preparation similar to RAI therapy. 818 Technical parameters for acquisition of these scans have been summarized in practice guidelines from the Society of Nuclear Medicine and Molecular Imaging (SNMMI). 809 Diagnostic WBS may be performed either as surveillance or as a part of RAI treatment protocols.
One of the common indications for WBS is to help guide subsequent treatment with RAI. In general, the WBS includes whole body images as well as a measurement of uptake in the thyroid bed. These scans can provide useful information about (i) the retained activity in the thyroid bed and (ii) the presence of regional or distant metastatic disease. This information, in turn, can be used to inform the subsequent treatment dose along with standard clinical and laboratory assessment parameters as detailed in other sections. The value of pre-therapy diagnostic WBS has been documented in several prior studies that show diagnostic WBS may lead to changes in management at the time of RAI therapy.819–822 For example, Van Nostrand et al. found that in a cohort of 355 patients, 29% had findings on diagnostic WBS that would alter management prior to treatment. 823 In a single-center study, Chen et al. found that a pre-therapy 123I scan provided critical information in 31/122 (25%) patients. 824 More recently, in a retrospective review, Song et al. found that pre-therapy scanning altered the selected administered activity for RAI therapy in 49% of cases. 825 Use of pre-therapy imaging is particularly important when higher administered activities are considered. This is because higher activities, such as 7.4 GBq (200 mCi), will exceed safe MTA thresholds in some patients (e.g., the elderly and those with renal dysfunction,). 782 For these higher doses, pre-therapy imaging is strongly recommended, combined with blood-based dosimetry, for better determination of a safe MTA.
Overall, representative changes in management that can be obtained with use of pre-therapy WBS include (i) detection of very large thyroid remnants with greater than 15% uptake, which may be an indication for additional surgery; (ii) detection of an insignificant thyroid remnant, which, when combined with a Tg level of <1 ng/mL, may obviate the need for RAI therapy or lead to a dose reduction; and (iii) the detection of clinically unsuspected nodal or distant metastatic disease. These findings may alter the decision to pursue RAI treatment and could result in the modification of the selected activity.
Should post-therapy WBS be performed?
▪
Post-RAI therapy scans should be performed after RAI treatment.
When therapeutic 131I is administered, a post-therapy WBS generally should be obtained, since it provides critical prognostic information about the iodine sensitivity of tissues as well as the presence or absence of residual or metastatic disease. This scan utilizes the RAI dose administered as part of therapy, so no additional radiopharmaceuticals are administered. Post-therapy imaging (generally 2–10 days after treatment dose administration) may identify sites of disease even among patients with negative Tg measurements. 826 For example, Park et al. found that in a cohort of 824 postoperative patients, 52 (6.3%) demonstrated functioning metastases on post-therapy scans despite negative serum Tg measurements. 827 Since larger activities of 131I are administered at the time of therapy compared with the pre-treatment diagnostic scan, additional sites of disease may be identified on post-therapy scanning. Fatourechi et al. found that 13% of 117 post-treatment scans had abnormal uptake not identified on pre-therapy scan, and 9% experienced changes in management based on the differential biodistribution observed. 828 Therefore, a post-therapy scan after RAI treatment should be performed.
Should single photon emission computed tomography with computed tomography be performed with the WBS?
▪
Single photon emission computed tomography with computed tomography (SPECT/CT) may be performed when available with diagnostic or post-treatment WBS.
SPECT/CT enables more precise localization of areas of radionuclide uptake. This is because the tomographic map of the distribution of the radioactivity may be precisely overlaid upon the CT map, allowing more accurate localization than is possible with planar imaging alone. In many cases, the more accurate imaging provided with SPECT/CT enables discrimination between benign and malignant foci of RAI uptake. For example, Tharp et al. found that SPECT/CT imaging had an incremental diagnostic value over planar imaging alone in 41/71 (57%) patients by characterizing localization of regional or distant metastatic disease or identifying benign variants.829–831 Similar findings have been replicated across a variety of studies, including systematic reviews.819,832–836 While SPECT/CT is more accurate in providing diagnostic information, it may not be available at all centers, and it slightly increases the imaging time and cost. However, when available, it should be considered based on the additional information it provides.
How should patients be educated regarding radiation safety?
▪
Patients should be provided oral and written instructions before preparation for RAI begins to minimize exposure to their families and members of the public, consistent with guidelines in the country where therapy is performed (e.g., in the United States, those of the Nuclear Regulatory Commission).
Administration of RAI generally is performed as an outpatient procedure. In this context, it is imperative to provide proper information to patients to minimize radiation exposure to their families and members of the public. For example, in the United States, release after RAI treatment is subject to regulatory control by the U.S. Nuclear Regulatory Commission, as stated in Code of Federal Regulations Title 10, Part 35, Section 35.75. All patients receiving RAI for DTC are subject to these regulations. Beyond these requirements, the principles of radiation safety are guided by ALARA (“as low as reasonably achievable”). This topic is reviewed extensively by the ATA,
837
the Nuclear Regulatory Commission,
838
the SNMMI,
839
the National Council on Radiation Protection and Measurements,
840
and the International Commission on Radiological Protection.
841
Since 131I emits both gamma and beta radiation, there is potential for radiation exposure and contamination through bodily fluids. Models can be used to calculate the time during which a patient should follow precautions to protect others. Some controversy exists concerning which model most accurately predicts radiation exposure.
842
Broadly speaking, key parameters include biological half-life (determined by extent of disease, avidity for 131I), time of exposure, distance from source, and shielding. A key assumption often used is an “occupancy factor” (i.e., time spent <1 m from the patient) of <0.25. Recent data indicate that more traditional models overestimate radiation exposure contamination (i.e., produced by body fluids or waste).
843
Length of time precautions should be determined by calculations using an appropriate model. Breastfeeding and lactation must cease prior to treatment (see
How do you counsel and minimize risks of RAI side effects to the salivary glands and lacrimal ducts?
▪
Patients should be counseled that RAI treatment may be associated with (acute and chronic) salivary gland morbidity, lacrimal duct stenosis, and potential risk of secondary malignancies. For prevention of salivary gland side effects after RAI, general measures including hydration are recommended.
844
Patients with xerostomia are at increased risk of dental caries and should discuss preventive strategies with their dental health professional. Surgical correction should be considered for nasolacrimal outflow obstruction, which often presents with excessive tearing (epiphora) but also predisposes to infection.
Salivary gland epithelium expresses the Na, I symporter (NIS). Therefore, it is not surprising that salivary gland side effects are common after RAI treatment, with both acute and chronic toxicity noted. For this reason, it is important to counsel patients before treatment that significant morbidity can occur in the weeks following RAI administration in the form of salivary gland swelling, salivary pain, and dryness of the mouth. Rarely, sequelae can become chronic and severe, associated with dry mouth and increase in dental caries and interference with taste.
Grewal et al. reported that in the first year after RAI ablation, acute salivary gland side effects occurred in 39% of a cohort of 262 patients (66% women, 93% PTC; single oral administration, median 5.21 GBq [141 mCi]). 844 There was recovery from these adverse effects in most patients; persistent side effects after a median of 7 years were observed in less than 5% of the cohort. A dose–response relationship was seen among this group. A statistically significant dose–response effect was seen between administered activity of RAI and development of salivary gland swelling (p = 0.001, logistic dose–response curve) but not with dry mouth (p = 0.63), altered taste (p = 0.27), or salivary gland pain (p = 0.152). Salivary gland side effects developed in 14% of patients receiving administered activities of 1.1 GBq (30 mCi); administered activities of ≥2.8 GBq (75 mCi) were associated with symptoms in 40% of patients (p = 0.046). Patients prepared with thyroid hormone withdrawal received higher 131I activity than those prepared with rhTSH, yet thyroid hormone withdrawal was associated with a lower rate of salivary gland swelling (10% vs. 20%, p = 0.017). There were no differences in the development of dry mouth, altered taste, or salivary gland pain based on type of preparation for RAI. 838
Some centers suggest use of sour lozenges to promote salivary secretion after RAI therapy, but other groups consider it harmful, 845 and there is no evidence of reduction in salivary gland radiation-absorbed dose with vitamin C tablets. 846 Hence, the role of sour candies to increase salivary secretion after RAI is uncertain. A recent study reported promising reduction in acute symptoms of xerostomia and sialadenitis with bethanechol, a parasympathomimetic, after thyroid ablation. 847 This drug also has shown promise in prevention of xerostomia and sialadenitis caused by external beam radiation of the head and neck. 848 For salivary gland pain and swelling (radiation-induced sialadenitis), most patients respond well to nonsteroidal anti-inflammatory drugs, but occasionally a short course of steroids is required for severe symptoms.
There is the possibility of cumulative dose-related early- and late-onset complications such as salivary gland damage, dental caries, 849 nasolacrimal duct obstruction, 850 secondary malignancies,851–855 and (rarely) long-term dysphagia. 856 As a result, it is important to ensure that the benefits of RAI therapy (and its repeated use) outweigh the potential risks. There is probably no administered activity of RAI that is completely safe, nor is there any maximum cumulative administered dose that could not be used in selected situations. In general, with higher (single and aggregate) administered activities, there are increased risks of side effects.
For acute transient loss of taste or change in taste and sialadenitis, recommended measures to prevent damage to the salivary glands have included hydration, sour candies, amifostine, and cholinergic agents, 857 but evidence is insufficient to recommend for or against these modalities. One study suggested sour candy may increase salivary gland damage when given within one hour of RAI therapy, as compared to starting its use 24 hours post-therapy. 845 Another study showed that the use of lemon slices within 20 minutes of 123I administration resulted in increased radiation absorbed dose to the salivary glands. 858 Other studies have suggested that early use and multiple administered doses of lemon juice transiently decreased radiation exposure to the parotid glands,859,860 so the exact role and details of use of sialagogues to prevent salivary gland damage remain uncertain. Patients with painful sialadenitis may receive pain relief from local application of ice. For chronic salivary gland complications such as dry mouth and dental caries, cholinergic agents may increase salivary flow. 857 Interventional sialendoscopy has been shown in several small studies to be an effective treatment in patients with radioiodine-induced sialadenitis that is unresponsive to medical therapy.861–863
How should patients be counseled regarding the risk of second primary malignancy after receiving RAI therapy?
▪
Patients should be counseled about the risks of second primary malignancy (SPM) after RAI treatment for DTC. The absolute increase in risk attributable to RAI appears to be small and does not warrant additional screening for SPM.
Long-term follow-up studies report a low risk of SPM (e.g., breast, colorectal, kidney, salivary cancers, and leukemia) in long-term survivors of DTC following treatment with RAI.851,852,864–866 The incremental additional risk of SPM following RAI appears to be low 864 and does not justify enhanced cancer screening. One meta-analysis demonstrated a RR of 0.98 comparing RAI-treated with nontreated patients with DTC; an increased incidence of acute myeloid leukemia, a decreased incidence of multiple myeloma, and no change in the risk of solid tumors were reported. 867 A meta-analysis of two large multicenter studies showed that the risk of SPM was significantly increased with a RR of 1.19 ([CI 1.04–1.36]; p < 0.010) relative to patients with DTC not treated with RAI, although the absolute increase in risk attributable to RAI was small. 853 The risk of leukemia was increased in patients with DTC treated with RAI, with a RR of 2.5 ([CI 1.13–5.53]; p < 0.024). 853 A study from the SEER registry demonstrated a small but statistically significant increase in the risk of chronic and acute myeloid leukemia in patients treated with RAI. 868 The excess risk of leukemia was greater in patients aged <45 years (standardized incidence rate [SIR] 5.32 [CI 2.75–9.30] for those aged <45 years vs. an SIR of 2.26 [CI 1.43–3.39] in older individuals). 869 A population-based study of adults <30 years and children demonstrated an increased incidence of solid tumors following RAI treatment of 3.7 Gbq (100 mCi) or more. 870 The risk of SPM appears to be related to the administered activity of 131I, 852 with an excess absolute risk of 14.4 for solid cancers and 0.8 for leukemias per GBq (1 GBq = 27 mCi) at 10,000 person-years of follow-up. Pasqual et al. suggested that RAI treatment for DTC diagnosed in childhood or young adulthood was associated with an increased risk of both leukemia and several solid tumors. 866 Studies by Teng et al. and Seo et al. also reported increased leukemia risk at doses above 5.5 GBq (150 mCi). 871 There also appears to be an increased risk of breast cancer in women with DTC; however, it is uncertain if this is due to RAI or other factors.851,855,872,873 Reinecke et al. performed a systematic review and reported ranges of risk for SPM of 1.14–1.84 for patients with DTC treated with RAI versus those who did not receive RAI, but that quality of evidence was considered “very low.” 864 The risk of second hematological malignancies was higher (ranged from 1.30 to 2.50), and the quality of evidence was considered “low.” 864 Taken together, the evidence from studies with large number of patients suggests a small dose-related increase in SPM following RAI. Further studies to identify subgroups of patients at greatest versus lowest risk for SPM are needed to better individualize risk assessment for patients. The use of laxatives may decrease radiation exposure for the bowel, particularly in patients treated after prolonged thyroid hormone withdrawal; vigorous oral hydration reduces exposure of the bladder and gonads.809,839,874
What other testing should patients receiving RAI therapy undergo?
▪
Patients receiving therapeutic administration of RAI should have a baseline complete blood count and assessment of renal function.
Published data indicate that when administered activities remain below 200 cGy to the bone marrow, minimal transient effects are noted in white blood cell and platelet counts.
875
Transient abnormalities in blood counts may be seen after RAI,
870
but they generally return to baseline. Persistent mild reductions in white blood cell counts and/or platelets have been seen in some patients who have received multiple RAI therapies. Radiation to the bone marrow is impacted by several factors, including renal function. The kidneys are a major means of iodine excretion from the body, and physiological radioisotope study research in non-thyroidectomized individuals has shown that renal impairment significantly reduces RAI excretion.
871
In patients with significant renal failure, dosimetry-guided therapy should be considered. Females of reproductive age should have a negative pregnancy test prior to receiving RAI (see
How should patients be counseled about RAI therapy and pregnancy, nursing, and gonadal function?
▪
Female patients of reproductive age receiving RAI therapy should have a negative screening evaluation for pregnancy prior to RAI administration and avoid pregnancy for at least 6 months after receiving RAI. RAI should not be given to nursing female patients. Depending on the clinical situation, RAI therapy should be deferred until lactating women have stopped breast-feeding or pumping for at least 3 months. A diagnostic 123I scan may be performed in recently lactating women to detect breast uptake that may warrant deferral of therapy. Male patients receiving cumulative radioiodine activities >14.8 GBq (400 mCi) should be counseled regarding potential risks of infertility. Female patients receiving RAI should be counseled that such therapy has not been shown to impact future fertility.
Female patients should undergo pregnancy testing prior to RAI treatment. Treatment with 131I is contraindicated during pregnancy due to direct radiation to the developing embryo and fetus, as well as concentration and potential destruction of the developing fetal thyroid gland after about 12 weeks gestation. NIS is expressed in the placenta, and iodine is transported from the mother to the developing fetus; in addition to the direct effects of RAI in pregnancy from circulating 131I on kidneys, bladder and bone marrow, there are recognized effects of radiation on the ovaries.876–878 Temporary amenorrhea/oligomenorrhea occurs in 8–27% of menstruating women within the first year after RAI for DTC. 879 Although the numbers of patients studied are small, long-term rates of infertility, miscarriage, and fetal malformation do not appear to be elevated in women after RAI.879–881 One recent large retrospective cohort study demonstrated that RAI treatment was associated with delayed childbearing and lower birth rates in later years, although it is unclear whether this is due to reproductive choice or reproductive health. 882 Another large retrospective study suggested that pregnancy should be postponed for 1 year after RAI administration because of an increased miscarriage rate, 883 although this was not confirmed in a subsequent study. 884
A long-standing recommendation after RAI therapy for hyperthyroidism or thyroid cancer has been to wait at least 6 months after therapy before pregnancy. Several observational studies provide a basis for recommendations around the timing of pregnancy after 131I therapy. A large retrospective population-based cohort study from Korea utilizing the Health Insurance Review and Assessment database identified 10,842 women (out of 111,459 women of childbearing age) with thyroid cancer who then became pregnant. They assessed the impact of surgery or surgery and RAI on obstetrical complications and pregnancy outcomes. Overall, there were no differences in the assessed outcomes if pregnancy occurred more than 6 months after RAI was administered. When pregnancy occurred less than 6 months after RAI, there was a small but significant increase in congenital malformations in the offspring (OR 1.74 [CI 1.01–2.97]). 885
RAI is also concentrated in lactating breast tissue. Therefore, RAI should not be given to females who are nursing.837,886–890 In order to reduce radiation dose to the maternal breasts, cessation of breast feeding for 3 months prior to RAI therapy is recommended. A diagnostic 123I scan may be employed in recently lactating female patients to detect breast uptake that may warrant deferral of therapy, especially if more urgent treatment is desired. 823 Dopaminergic agents might be useful in decreasing breast exposure in recently lactating female patients, although caution should be exercised given the risk of serious, albeit rare, side effects, including cardiovascular, neurological, and psychiatric disorders associated with their routine use to suppress postpartum lactation. 891
In males, RAI therapy may be associated with a temporary reduction in sperm counts and elevated serum follicle-stimulating hormone (FSH) levels.892,893 A small study of thyroidectomized male patients receiving an ablative administration of 131I that averaged 1.256 GBq (33.9 mCi) measured total (beta and gamma) doses to the testes; these ranged from 30 to 43 uGy/MBq. 894 RAI therapy does not affect serum testosterone concentrations in males, but it is associated with a temporary elevation in serum FSH and a reduction in inhibin B levels.895–897 In general, serum FSH and inhibin B levels normalize within 18 months from the last administration of RAI. Reduced normokinetic sperm counts after 131I therapy also have been reported, but they returned to normal when evaluated at 12 months. 895 A longitudinal prospective multicenter study observed no DNA fragmentation in sperm, but a statistically significant increase in chromosomal abnormalities 3 months after a single 131I ablative dose with activity of 3.7 GBq. 896 The slight increase in chromosomal abnormalities persisted 13 months after therapy. 896 Although data are limited, it has been recommended that males who receive 131I wait at least 120 days (the lifespan of sperm) after 131I therapy before attempting conception or providing a sperm sample for assisted reproduction. 898
Higher cumulative activities (18.5–29.6 GBq, 500–800 mCi) in male patients are associated with an increased risk of persistent elevation of serum FSH levels, but fertility and risks of miscarriage or congenital abnormalities in subsequent pregnancies are not changed with moderate RAI activities (∼7.4 GBq, 200 mCi). 899 Permanent male infertility is unlikely with a single ablative dose of RAI, but theoretically, there could be cumulative damage with multiple treatments. It has been suggested that sperm banking be considered in males who receive cumulative RAI activities ≥14.8 GBq (400 mCi). 893 Gonadal radiation exposure is reduced with good hydration, frequent micturition to empty the bladder, and avoidance of constipation. 900
A retrospective study among 64 women with a history of thyroid cancer treatment who underwent in vitro fertilization/intracytoplasmic sperm injection, compared with 320 matched control women, found no difference in fertility treatment success or pregnancy outcomes in women treated for thyroid cancer. 901 RAI therapy has been recognized as influencing long-term ovarian function, resulting in significant decreases in ovarian reserve.902–904 A systematic review and meta-analysis examined 36 studies that compared pregnancy rates and ovarian function in menopause in thyroid cancer patients with and without RAI treatment to controls. There were no differences in pregnancy rates after RAI, but a slight reduction in anti-Müllerian hormone levels 1 year after RAI and a slightly earlier menopause, averaging 49.5 years old compared with 51 years old in controls. 879
What is the role of radiotherapy, with or without chemotherapy, in patients with DTC?
▪
Adjuvant external beam radiotherapy (EBRT) for patients with DTC with high-risk features for locoregional disease progression (such as aggressive histologic subtype, gross extrathyroidal extension, positive margins, and visceral or soft tissue invasion) may be considered in select cases, especially if the expected disease progression would not be amenable to salvage surgery. The potential benefit of improving locoregional relapse-free survival must be weighed against the absence of data demonstrating improvement in overall survival and the known risks of clinically meaningful toxicity. EBRT with or without concurrent chemotherapy in patients with DTC with gross residual disease in the postoperative setting or with locally advanced unresectable disease may be considered in select patients who may benefit from improved locoregional control. EBRT with or without concurrent chemotherapy may increase locoregional control but also causes acute- and long-term treatment-related toxicity.
Surgery is the mainstay of treatment for DTC, in part to achieve locoregional disease control and reduce the risk of recurrence, particularly involving critical anatomical structures, such as the larynx, trachea, esophagus, and recurrent laryngeal nerves. Surgery, with or without RAI administration, will achieve locoregional control in many patients with DTC. Risk factors for progression include older patient age, unfavorable histology, the presence of macroscopically positive margins or gross residual disease, tumor dissection off the recurrent laryngeal nerve, trachea or larynx, and gross extrathyroidal extension.905–907 Locoregional recurrence can contribute significantly to morbidity and even mortality in patients with DTC. For patients with distant metastases, the impact of locoregional disease progression must be considered in the context of the overall prognosis.
The role of EBRT to reduce the risk of locoregional recurrence or progression is debated, primarily because of the morbidity resulting from EBRT to the neck and lack of solid data demonstrating improvement in outcomes. Prospective data from clinical trials evaluating the benefits of EBRT weighed against its toxicities are limited. Only one multicenter randomized trial has been launched comparing RAI plus EBRT following thyroidectomy to RAI alone post-thyroidectomy in locally invasive DTC. 908 This study closed in 2003 due to slow accrual after only 45 patients were enrolled. Several single-institution retrospective reviews have examined the role of EBRT, primarily without concurrent chemotherapy, in heterogenous groups of patients with DTC with varying risk factors for locoregional progression.909–919 High-risk factors in DTC cases leading to EBRT have generally included aggressive histological subtype, gross extrathyroidal extension, positive margins, visceral or soft tissue invasion, and lymph node involvement. The range of radiation dose administered is primarily 6000–6600 cGy. Since the widespread adoption of intensity-modulated radiation therapy (IMRT) as a more precise technology for the delivery of radiation, it has replaced 3D conformal radiation as the standard approach. 920 The main advantage with IMRT is in reducing the radiation dose to normal structures, but acute and late radiation-related adverse events are still encountered. While grade 2 or less acute mucositis, esophagitis, xerostomia, dysphagia, dermatitis, and fatigue are quite common, grade 3 or higher acute and long-term toxicities, including dysphagia, gastrostomy tube-dependance, and tracheostomy, are rare.910,912–914,918 In single-institution reviews, locoregional relapse-free, disease-specific, and overall survival rates were reported at varying time periods spanning 4–10 years and ranged from 79% to 95%, 71% to 76%, and 65% to 93%, respectively.
Of the single-institution retrospective reviews that compared EBRT-treated patients with matched historical controls, locoregional relapse-free survival was improved with treatment. However, no differences in overall survival were seen, likely due to similar rates of distant metastasis.910,912,914,918 One single-institution phase II study of IMRT following surgery and RAI treatment in 65 patients with locoregionally advanced (pT4 or N1b) disease was performed. 911 No grade 3 or higher acute or long-term radiation-related adverse events were reported. The outcomes of the patients treated on study were compared to a propensity score-matched control group from the same period. Locoregional relapse-free survival at 4 years was 100% and 84.6% (p = 0.002) in the IMRT-treated patients and controls, respectively, and 4-year overall survival was 100% in both. In view of the lack of randomized controlled trials investigating adjuvant EBRT in high-risk DTC, a comparative effectiveness analysis of observational data from 870 locally advanced T4 PTC cases from SEER from 1988 to 2013 was conducted. 921 Of note, EBRT was associated with worse overall survival (HR 1.60 [CI 1.18–2.16]) and disease-specific survival (HR 1.58 [CI 1.09–2.30]). Systematic reviews and NCDB reviews also have been published.920,922,923 Despite data suggesting that locoregional relapse-free survival may be improved with adjuvant EBRT in high-risk DTC, disease-specific and overall survival were not improved. Adjuvant EBRT may be appropriate in select cases, such as in patients considered at high risk for an aggressive locoregional recurrence that could not be approached with surgical salvage, but results available to date do not support the adoption of adjuvant EBRT as a standard of care in patients with high-risk locally advanced DTC, particularly in light of the risks of acute and long-term treatment-related adverse effects that may impact patient QoL and make future revision neck surgery for recurrent disease still more challenging.
In patients with DTC with postoperative gross residual disease or presenting with unresectable locoregional disease, several retrospective reviews suggest that EBRT with or without concurrent chemotherapy may decrease the risk of locoregional progression.917,919,924,925 In treating gross disease, IMRT administered to 7000 cGy was most common, with evidence indicating that locoregional control is improved with doses higher than 5000 cGy.917,919,924 Concurrent chemotherapy schedules, variously including doxorubicin, cisplatin, cisplatin/etoposide, and taxanes, have been employed917,924; treatment-related acute and long-term toxicities were acceptable with chemoradiotherapy compared with radiation alone, but rates of hoarseness, dermatitis, and gastrostomy-tube placement may be higher with chemoradiotherapy.905,912 In these reports, locoregional control appeared to be improved with chemoradiotherapy compared with that seen with radiation alone, ranging from 86% to 90% at 3–4 years with chemoradiotherapy, versus 69–73% with radiation alone.
Data on differences in overall survival are conflicting. One multicenter retrospective review analyzed outcomes of patients initially presenting with unresectable DTC. 925 Patients were treated with EBRT, locoregional therapy of distant metastases, cytotoxic chemotherapy, and/or multi-kinase inhibitors (MKIs) such as sorafenib, pazopanib, or lenvatinib. Thirteen patients were treated initially with EBRT, resulting in disease stabilization in six patients. First-line MKI therapy was initiated in seven patients, yielding an overall RR of 29%. No responses to cytotoxic chemotherapy were reported. No difference in overall or disease-specific survival was found in comparing MKI-treated and non-MKI treated patients, or in EBRT-treated and non-EBRT treated patients. The authors concluded that initial MKI therapy may represent a promising treatment option for patients presenting with unresectable DTC, but more definitive data are needed. One single-institution phase II trial of IMRT with or without chemotherapy has been reported in the modern era. 926 Twenty-seven patients with gross residual or unresectable DTC were enrolled. The first eight patients were treated with IMRT (7000 cGy) alone before the protocol was amended to add concurrent weekly doxorubicin for the remaining 19 patients. Acute grade 3 or higher treatment-related adverse events were seen in one-third of patients. Chemoradiotherapy compared with IMRT alone was associated with higher rates of grade 2 or greater acute dermatitis (89.5% vs. 50.0%; p = 0.04), mucositis (73.7% vs. 25.0%; p = 0.03), and dysphagia (63.2% vs. 12.5%; p = 0.03). No difference in long-term adverse events was observed, although two chemoradiotherapy patients required tracheostomy for laryngeal edema, two chemoradiotherapy patients required gastrostomy placement, and two IMRT-only patients required tracheostomy after experiencing locoregional recurrence. Locoregional control at 2 years was 100% with chemoradiotherapy and 50% with IMRT alone (p = 0.001). In patients who were free of distant metastasis at enrollment, 23.5% developed distant metastasis by 2 years, and no difference was seen in the risk of distant metastases between chemoradiotherapy and IMRT alone. Two-year overall survival was 77.3% in all 27 patients, with no difference in overall survival between the two groups. The authors deemed chemoradiotherapy promising due to the superior locoregional control achieved; however, with increased toxicity and no difference in overall survival observed in this small single-institution phase II trial, chemoradiotherapy cannot be recommended for all patients with gross residual or unresectable DTC. Randomized clinical trials investigating the clinical benefits of IMRT with or without concurrent chemotherapy in patients presenting with unresectable locoregional disease or with gross residual disease post-thyroidectomy are needed.
Long-Term Management and Advanced DTC Management
What are the appropriate features of long-term management of patients with DTC?
Using the DATA framework, monitoring for possible clinical recurrence in patients thought to be free of disease and identifying progression in patients with suspected or diagnosed residual thyroid cancer are the primary goals (Fig. 5). Tests with high specificity allow for the identification of patients unlikely to experience disease recurrence so that less aggressive management strategies that are safer and more cost-effective can be pursued. De-escalation of monitoring based on low rates of clinical recurrence is possible for low-risk patients many years after initial therapy when they have a persistent excellent response. Those patients with a higher risk of recurrence should be monitored more closely, since early detection of recurrent disease offers the best opportunity to achieve an excellent response. A shared decision-making model should be pursued in consultation with the patient and consideration of side effects as well as financial implications.
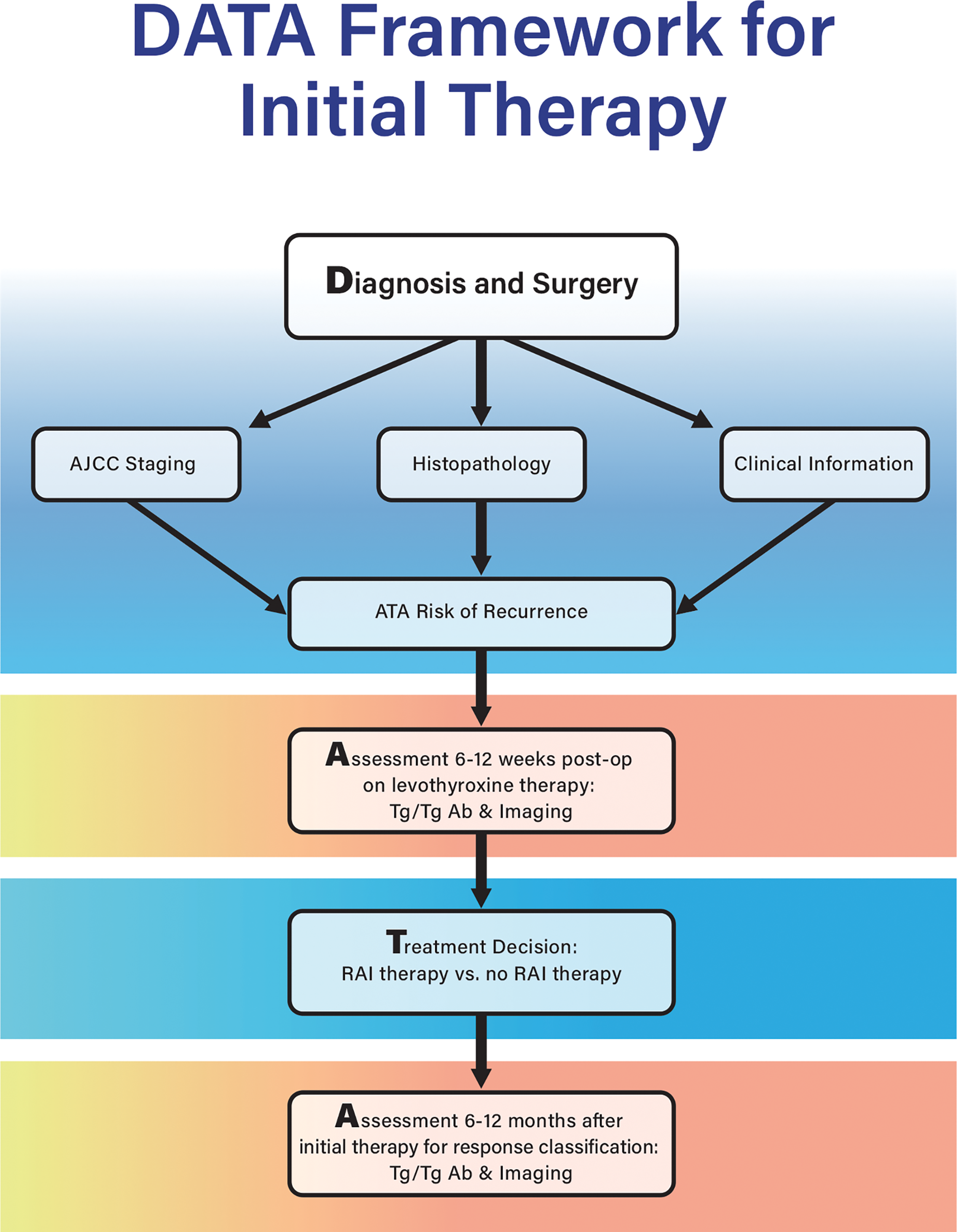
DATA framework applied to the first 12 months after DTC diagnosis. Imaging timing and type depend on risk of recurrence, Tg levels, and pathology/clinical factors. DTC, differentiated thyroid cancer; Tg, thyroglobulin.
What is the appropriate degree of TSH suppression in patients treated for DTC?
▪
Individualization of decisions to initiate TSH suppression to below the reference range is recommended based on potential benefits and risks; recognizing that patients with high-risk disease may be more likely to benefit from a TSH in the subnormal range than those with low-risk disease (see Table 9).
How long should TSH suppression to below the reference range be maintained?
▪
Long-term TSH suppression is not suggested for patients with low- or intermediate-risk disease who have no evidence of biochemical or structural recurrence. Risks versus benefits of TSH suppression and TSH goals should be re-evaluated over time.
DTC cells express the TSH receptor on their membranes and respond to TSH stimulation by increasing the expression of several thyroid-specific proteins (e.g., Tg, NIS) and by increasing the rates of cell growth. 927 Suppression of TSH using supra-physiological doses of LT4 historically was used to treat patients with DTC to decrease the risk of recurrence or reduce the rate of disease progression.768,928–931 Although there is a physiological rationale for why TSH suppression may be beneficial in some scenarios, there are mixed findings regarding which patients should or should not receive TSH suppression and the optimal degree of TSH suppression (see Table 9). The existing studies evaluating the role of TSH suppression in DTC management have many limitations, including small sample size for some studies and low event rates for many. Comparing and evaluating existing studies are complex due to variable length of follow-up, different disease severity in study cohorts, and approaches to categorizing TSH.
There have been several publications on TSH levels and DTC outcomes performed by the NTCTCSG.365,768,769,929 The most recent NTCTCSG study was published in 2015. Mean TSH categories were created with specified ranges reportedly correlating with degree of thyroid hormone suppression: aggressive suppression (undetectable to subnormal TSH), moderate suppression (subnormal to normal TSH), and non-suppression (normal to elevated TSH). This study had a median of 6 years of follow-up and found that among 3238 patients with DTC, there was improved overall survival and disease-free survival across all stages for mean TSH scores in the moderate suppression range (i.e., subnormal to normal TSH) and no further improvement for any stage with TSH levels averaging in the undetectable subnormal range. 365
Although there are conflicting data, evidence to support TSH suppression came from a meta-analysis from 2002 that described 4174 patients with thyroid cancer, of whom 2880 were on TSH suppression (defined as TSH below the lower limit of normal range, i.e., below 0.4–0.5 mIU/L). This study demonstrated an association between TSH suppression therapy and a reduced incidence of major adverse clinical events (defined as progression, recurrence, or death; RR = 0.73 [CI 0.60–0.88]; p < 0.05). 928 In a more recent retrospective single-center observational study of 366 consecutive patients with DTC who had a median follow-up of 8.85 years, there was a positive association between serum TSH levels and risk of recurrent disease and cancer-related mortality, with a threshold of 2 mIU/L differentiating between disease-free survival and recurrence or death. 932 In a retrospective study of 141 patients with a mean of 95 months of follow-up, a constantly suppressed TSH (i.e., TSH ≤0.05 mIU/L) was found to be associated with a longer recurrence-free survival than when serum TSH levels were always ≥1 mIU/L, and degree of TSH suppression was an independent predictor of recurrence in multivariable analysis. 933 A retrospective patient chart study of 157 patients with distant metastases from DTC found improved thyroid cancer-specific survival if the median TSH level was ≤0.1 mIU/L as opposed to non-suppressed, but no further improvement in outcome was seen with TSH suppression to <0.03 mIU/L compared with ≤0.1 mIU/L. 930
There also have been studies contesting the benefits of TSH suppression A cohort study of 867 intermediate and high-risk patients with DTC treated with total thyroidectomy and RAI found that TSH suppression showed no association with progression-free survival at 5 years. 934 A similar retrospective series of 166 intermediate- and high-risk patients with pre-ablation Tg <1 ng/mL found that disease recurrence risk did not differ based on TSH <0.1 mIU/L, 0.1–0.5 mIU/L, 0.5–2.0 mIU/L, or >2.0 mIU/L, and only four patients experienced recurrences during a median follow-up of 5.8 years. 935
There are also conflicting data surrounding TSH targets and the use of thyroid hormone in low-risk patients who have undergone lobectomy as described below. A small randomized controlled trial compared outcomes in 218 patients with PTC who were administered LT4 to keep their TSH levels suppressed versus 215 patients who had their TSH levels maintained in the normal range. 936 Most of the patients in this study did not undergo total thyroidectomy or RAI, and Tg levels were not monitored or reported. 936 This study showed that disease-free survival did not differ significantly between the cohort with normal TSH levels (TSH 0.4–5 mIU/L) compared with the cohort with suppressed TSH levels (TSH <0.01 mIU/L). Patients with T1a PTC, distant metastases, age ≥80 years, Graves’ disease, ischemic heart disease/arrhythmia, or severe osteoporosis were not eligible for the trial. Another study retrospectively reviewed 1528 patients who underwent thyroid lobectomy for low-risk disease and found that during 5.6 years of follow-up, only 1.4% experienced recurrence. 937 There was no difference in recurrences among patients with TSH levels ranging across <0.5, 0.5–1.9, 2.0–4.4, or >4.5 mIU/L. A separate retrospective study with 2297 low-, intermediate-, and high-risk patients who underwent lobectomy for DTC found that with a median follow-up of 70 months, mean TSH levels did not impact risk of recurrence. 392 In contrast, a retrospective study of 1047 patients who underwent thyroid lobectomy for low- or intermediate-risk PTC reported that a TSH level at 1 year was an independent risk factor for recurrence, with recurrence more frequently seen with a TSH >1.85 mIU/L. 938 A 2024 systematic review and meta-analysis evaluating the role of TSH suppression in patients with intermediate- and high-risk DTC found that progression-free survival, disease-free survival, and relapse-free survival were not significantly different between TSH suppression and non-suppression groups. 939
Since the desire to avoid thyroid hormone replacement is a reason that some patients with low-risk disease choose lobectomy over total thyroidectomy, optimal TSH goal is relevant to treatment decision-making. The TSH goal for those patients with low or intermediate risk for recurrence of thyroid cancer (after a total thyroidectomy or after a thyroid lobectomy) is in the normal reference range (Table 9). Prior studies suggest that if the TSH goal is within the normal range, about 70–80% of patients who undergo lobectomy can avoid thyroid hormone supplementation.940,941 In contrast, if the goal TSH level is 0.5–2.0 mIU/L, only 20–30% of patients who undergo lobectomy can avoid thyroid hormone supplementation.388,942 If TSH is above the normal reference range (after total thyroidectomy or after thyroid lobectomy), then thyroid hormone therapy should be initiated. Thyroid hormone replacement therapy is most frequently started in the first 2 years after thyroid lobectomy, but for up to a quarter of patients, it is started later. 943
There have been recent studies exploring the role of TSH suppression during active surveillance, also resulting in conflicting findings.944,945 In a study of 322 patients who had T1a PTC and who elected to pursue active surveillance, there was no significant association between mean TSH level and tumor growth. 944 However, a multicenter retrospective study of 234 patients with T1a PTC undergoing active surveillance used time-weighted average levels of TSH and found that for patients <50 years, a time-weighted average TSH >1.74 mIU/L was associated with disease progression (defined as tumor volume increase ≥50%, size increase ≥3 mm, or new lymph node metastases). 945 In addition, a prospective study from three referral hospitals in Korea included 699 participants who underwent active surveillance and found that serum TSH of 7 mU/mL or higher predicted tumor progression. 946 A study of 2509 patients with low-risk papillary thyroid microcarcinoma who underwent active surveillance, with only a subset receiving LT4, found that LT4 treatment may be associated with decreased tumor growth. 947 However, further research is needed.
When treating a patient with thyroid hormone replacement, it is critical to consider practical issues such as the ability to consistently maintain the goal TSH level without over- or under-replacing the patient, as well as clinically relevant issues such as balancing the benefits and risks of TSH suppression. It should be recognized that targeting and maintaining specific TSH goals can be difficult in real-world settings.948–950 For example, with use of target TSH levels per the 2015 ATA guidelines, of 1125 patients with DTC who were treated at 21 medical centers, only 29% had TSH levels at target normal reference range despite 82.8% having good or moderate adherence to therapy. Approximately 50% of the patients were overtreated, and 20% were undertreated. 950
The potential benefit of a suppressed TSH is greater in patients at high-risk for recurrence or death. When considering benefits and risks, there may be more benefits in patients with disease progression. In contrast, for patients at low-risk for recurrence, the risks of TSH suppression may exceed any potential benefit (Table 9). Some of the recognized adverse effects of TSH suppression are derived from studies of endogenous subclinical hyperthyroidism or from studies of exogenous subclinical hyperthyroidism that exclude patients with thyroid cancer. Based on these prior studies, recognized adverse outcomes of a low TSH include exacerbation of angina in patients with ischemic heart disease, increased risk for atrial fibrillation and stroke (especially in older patients), increased risk for cardiovascular mortality, and increased risk of osteoporosis and possibly fracture in postmenopausal women.951–955
Similar risks, particularly surrounding bone health in older women, have been found in studies evaluating TSH suppression for thyroid cancer.956–961 The importance of balancing benefits and risks is illustrated in a study of 771 patients with low- to intermediate-risk for recurrence who underwent total thyroidectomy. 962 Of this cohort, 5.6% had thyroid cancer recurrence, 3.9% were diagnosed with osteoporosis, and 2.3% were diagnosed with atrial fibrillation. Despite having similar risk of recurrence, patients with a TSH ≤0.4 mIU/L were at increased risk of atrial fibrillation and osteoporosis. 962 An observational study demonstrated increased risk of all-cause and cardiovascular mortality among patients with DTC compared with a control population. 963 The authors also showed that survival in the patients was lower when the serum TSH was <0.02 mIU/L. Therefore, optimal TSH goals for individual patients balance the potential benefit of TSH suppression with the possible harm from subclinical thyrotoxicosis, especially in patients with medical conditions that can potentially be exacerbated by aggressive TSH suppression.
What is the role of serum Tg measurement in the follow-up of DTC?
▪
Serum Tg should be measured by an assay that is calibrated against the BCR457 standard. Tg antibodies should be quantitatively assessed with every measurement of serum Tg. Measure serum Tg (on thyroid hormone therapy) after total thyroidectomy, with or without RAI, to monitor for response to therapy and to determine recurrence (although the predictive value is greater after RAI). ( Measurement of serum Tg during initial follow-up while receiving thyroxine therapy should be undertaken every 6–12 months. More frequent serum Tg measurements may be appropriate for ATA intermediate-high or high-risk patients. Measurement of serum Tg on thyroid hormone in patients after lobectomy during initial follow-up is not recommended routinely (see In patients with circulating anti-Tg antibodies, trends of serial TgAb levels using the same assay may be useful to monitor disease. Current Tg immunometric assays (IMA) and radioimmunoassays (RIA) are often affected by TgAb, and Tg liquid chromatography-tandem mass spectrometry (LC-MS/MS) has low sensitivity. These should not be solely relied upon to monitor patients with circulating TgAb levels. Imaging is the primary modality for monitoring in this population.
Serum Tg should be measured 6–12 weeks after total or near-total thyroidectomy in patients with DTC,
243
as discussed in
Serum Tg is measured by immunometric assays, which include competitive RIA and IMA, or by LC-MS/MS assays. 964 In addition to sensitivity and specificity, these assays differ in ease of performance, instruments required, as well as interference from anti-Tg autoantibodies (TgAb), and heterophile antibodies (HAb). 964 The majority of clinical laboratories use Tg-IMA, which involves a solid phase antibody and a labeled antibody targeting a different Tg epitope and can be rapidly performed on an automated high-throughput instrument. It is recommended that Tg assays are calibrated with a standard traceable to the Certified Reference Material−457, now known as BCR-457, European Commission Institute for Reference materials. 965 The use of this Tg standard has significantly reduced the wide inter-assay variability, although even with use of these standards, mean Tg concentration in a cohort of TgAb-negative patients varied as much as two-fold. 966 The BCR-457 standard is a preparation of glandular Tg, and various Tg features, including glycosylation and iodine heterogeneity, can lead to differences in epitopes of circulating Tg detection. 967 Due to this intrinsic variability in Tg detection and the importance in postoperative follow-up, it is recommended that longitudinal measurements are made with the same manufacturers assay, and the same laboratory, if possible.
Immunometric assays are prone to interference from TgAb, which commonly cause falsely low serum Tg measurements. Moreover, variability in TgAb assays may result in falsely negative antibody levels associated with a misleadingly undetectable serum Tg due to the antibodies that are present but not detected. 968 Assays for TgAb have similar variability and lack of concordance, as do Tg assays, 969 and both Tg and TgAb assays may be affected by HAbs. 970
TSH-stimulated serum Tg measurements had been recommended to enhance the sensitivity for persistent or recurrent DTC. Most studies, though, have shown that a basal serum Tg (using assays with a sensitivity of 0.1 ng/mL or lower) on LT4 in patients after total thyroidectomy is adequately sensitive. 971 A meta-analysis of studies of DTC follow-up through 2013 concluded that an undetectable basal Tg level using modern highly sensitive assays had a high NPV, and TSH stimulation was not required. The authors recommended TSH stimulation when Tg levels were detectable. 972 A subsequent systematic review and meta-analysis from papers published from 2003 to 2018 addressed the NPV of serum Tg on LT4 in follow-up of DTC patients who had undergone total or near total thyroidectomy, with or without RAI. 973 The diagnostic performance of serum Tg on thyroid hormone was assessed versus anatomical imaging for structural recurrence both at the time of Tg and during follow-up. The NPV of serum Tg was 99.4% when undetectable on thyroxine treatment, providing support for adequate clinical sensitivity.
In patients with DTC treated with a total thyroidectomy with or without ablative RAI, a low or undetectable basal serum Tg is a reliable indicator of disease status. A retrospective series of patients with low-risk DTC treated with total thyroidectomy but without ablative RAI demonstrated that an unstimulated Tg of <0.5 ng/mL on LT4 was achieved in all patients 2 years after treatment. 974 A retrospective database study examined 773 patients with DTC undergoing 3176 cervical ultrasounds from 1996 to 2012 975 ; in the 6 months following the ultrasound, results were classified as true or false based on further evaluation and the sensitivity, specificity, and PPVs and NPVs. After 10 years, no true positive or false negative ultrasounds were found in patients with a basal Tg <1 ng/mL.
TgAb are present in about 20% of patients with DTC; thus, they have been the focus of several studies trying to identify the optimal approach to measuring serum Tg, minimizing the disruption from TgAb, understanding the significance of TgAb in the original assessment of DTC, and their impact on prognosis for tumor recurrence.976,977 A variety of approaches have been proposed to improve the sensitivity and accuracy of serum Tg measurement, 849 especially in the presence of TgAb. A retrospective multi-institutional series studied 495 patients with Stage I–IV DTC (89% with PTC), comparing various Tg assays and determining the impact of TgAbs on the various assays. 850 The study compared four Tg immunoassays (IA), two Tg RIAs, and two Tg LC-MS/MS assays in patients with or without TgAb. TgAb positivity was observed in 27–58% of patients. The Tg IMA was most sensitive and specific in samples that were TgAb negative. In the presence of TgAb, Tg levels were underestimated by Tg IMA. Tg LC-MS/MS was most likely to measure Tg in the presence of TgAb and was felt to be the most accurate. TgRIA measured Tg in specimens that were TgAb positive, but there were false positives. A study to determine the benefit of Tg LC-MS/MS measurements examined patients with DTC who had undergone thyroidectomy and had a Tg measured by both immunoassay and LC-MS/MS no more than 1 month apart and examined those with TgAbs and with HAb. 851 The investigators observed that a falsely elevated TgIMA with undetectable Tg LC-MS/MS occurred with significant frequency. Tg LC-MS/MS, however, was useful to rule out HAb interference. Tg LC-MS/MS was not effective at detecting low levels of serum Tg in patients with TgAb and structural disease in this study, and the investigators concluded that no current assay design effectively measures serum Tg in the presence of TgAbs. The Tg mini-recovery system, which adds serum Tg with a concentration of about 5 ng/mL to samples with low native concentration to improve recovery, was assessed in 1120 samples from 798 patients with DTC, 20% of whom were TgAb positive. 978 The application of the mini-recovery system did not provide an overall clinical benefit in most patients. Thus, in clinical series, it is not clear that any Tg assay system is fully accurate in monitoring patients with circulating TgAb.
The significance of TgAb measurement in longitudinal follow-up has been assessed in patients treated with or without ablative RAI therapy. Notable is a study of 107 patients with DTC and positive TgAbs, all of whom had tumors <1 cm and who underwent total thyroidectomy without ablative RAI; they were followed for 6 years. 979 TgAb levels fell in most patients, and there was no tumor recurrence. TgAb levels declined even in the absence of RAI. A retrospective review of a database that included 432 patients with DTC (all of whom underwent total thyroidectomy with or without ablative RAI, and 106 [24.5%] had detectable TgAb over a median follow-up of 53 months) 980 included patients from ATA low- (53.7%), intermediate- (26.8%), and high- (19.4%) risk groups. Disease progression in patients with TgAb positivity was compared with those who were TgAb negative. There was no association of initial TgAb positivity with disease progression and no association with response to therapy in the low-risk group. A rising TgAb level, more than an absolute level, was associated with an increased risk of a structurally incomplete response in the intermediate- and high-risk groups. A prospective study of 152 patients with DTC who underwent total thyroidectomy without RAI included patients with TgAbs (41 patients) and without TgAbs (111 patients) who were followed for a median of 2.3 years. 981 The overall risk of recurrence was similar in the two groups, and serum TgAb levels either decreased over time or were stable, increasing in just two patients.
In a study of 110 patients with positive TgAb levels treated with total thyroidectomy and ablative RAI, 982 an increase in the first 6–12 months was a risk factor for worse disease outcomes in patients <55 years, and the median time for TgAb levels to become negative was 15.8 months after surgery. A meta-analysis of 34 studies assessed whether TgAb levels are a reliable prognostic marker for DTC. 981 The studies included were those that had patients with DTC with known TgAb status and included prognostic outcomes. TgAb positive patients, in comparison to TgAb negative patients, had a higher risk of lymph node metastases and cancer persistence but no difference in tumor size, risk of extrathyroidal extension, or cancer mortality. Patients with persistent or increasing TgAb levels had a higher risk of cancer persistence and cancer mortality compared with patients with decreasing TgAb levels. A retrospective study of 76 patients with DTC with elevated TgAb levels after total thyroidectomy but without persistently raised serum Tg IMA level >1 ng/mL or RAI-avid disease examined the association of changes in TgAb levels and clinical outcome. 983 High postoperative TgAb levels and central compartment lymph node metastases were risk factors for an incomplete response, and low levels of TgAb were associated with an excellent outcome. Patients with low levels of TgAb had excellent outcomes, and patients with recurrences had very high baseline TgAb levels >1000 IU/mL. A study of 405 patients with DTC with preoperative TgAb positivity found that elevated TgAb levels were a risk factor for nodal metastases and extranodal extension, and elevated thyroid peroxidase antibodies (TPO) Ab levels were associated with a lower pathological tumor and nodal stage. 984
The importance of de novo TgAbs in patients with DTC that are initially TgAb negative has been studied. The NTCTCSG reported on the significance of de novo TgAb detection from their DTC registry from 1996 to 2012, focusing on patients who were negative at their first postoperative follow-up and over the next 3 years without demonstrating evidence of persistent disease. 985 Overall, de novo TgAb were detected in 5% of patients with DTC, and there was no difference with respect to structural recurrence among these patients compared with patients who remained TgAb negative. In the six patients from the de novo TgAb group who experienced structural recurrence, none were TgAb positive at the time of detection, and TgAbs became positive a median of 2.1 years later. Another retrospective study identified 119 patients with DTC with pre-ablation negative TgAb and evaluated 14 patients (11.7%) that developed de novo TgAbs. 986 The patients with de novo TgAbs did not differ from the TgAb negative patients regarding disease-free survival, although 2 of the 14 patients had structural recurrence.
In a limited number of patients with DTC, structural disease is present, but serum Tg is undetectable, and only TgAb levels are elevated. A retrospective review of 47 patients with PTC and lung metastases who had negative serum Tg and positive TgAb levels compared their outcomes with historical controls.
987
The 5- and 10-year rates of progression-free survival were not lower in the patients that were serum Tg negative and TgAb positive. The strongest predictor of a poor prognosis was loss of 131I avidity in the lung metastases. Finally, as outlined in
Can monitoring be de-escalated or discontinued in patients with low-risk DTC?
▪
For patients with low-risk DTC treated with total thyroidectomy and RAI and a sustained excellent response 5–8 years after initial therapy, routine ultrasound can be discontinued, and patients can be followed subsequently with biochemical markers alone every 1–2 years. Patients with low-risk DTC treated with total thyroidectomy and RAI and sustained excellent response for 10–15 years do not require continued routine biochemical monitoring for thyroid cancer and should be considered to have achieved a complete remission. For patients with low-risk DTC treated with a total thyroidectomy alone and a sustained excellent response 5–8 years after initial therapy, routine ultrasound can be discontinued, and patients can be followed subsequently with biochemical markers alone every 1–2 years. Patients with low-risk DTC treated with total thyroidectomy alone and sustained excellent response for 10–15 years do not require continued routine biochemical monitoring for thyroid cancer and have achieved a complete remission. For patients with low-risk DTC treated with lobectomy, if initial ultrasound is negative, subsequent ultrasounds should be performed every 1–3 years for 5–8 years after initial therapy. Nodules in the residual lobe should be monitored as per ATA thyroid nodule guidelines. For patients with low-risk DTC treated with lobectomy, if postoperative Tg is not markedly elevated (see
Defining complete remission
“Complete remission” is the term used in oncology to define the disappearance of all signs of cancer in response to treatment. This does not always mean that cancer has been cured or will not return. 988 Identifying patients to be in complete remission offers psychological, financial, and medical value to both patients and clinicians.
As recurrence risk declines over time, it is likely that most patients with DTC will achieve “complete remission”; however, this term has not been included in prior ATA DTC guidelines. Clear data to define this term in thyroid cancer are lacking and complicated by the heterogeneity of thyroid cancer management and differences in monitoring and response to therapy. However, the low rates of recurrence and outstanding survival statistics for patients with low-risk DTC support the general concept of de-escalating monitoring intensity over time. As summarized below, data are strongest for patients with low-risk DTC treated with total thyroidectomy, particularly those who also receive RAI. Data are more limited for patients treated with lobectomy, thereby providing a call for more research for this growing population of patients. Further validation studies will be crucial for all groups to help guide long-term monitoring so that we can better avoid unnecessary follow-up and interventions. A recommended approach is summarized in Table 11.
Low-Risk DTC with Excellent Response to Therapy De-escalation Recommendations
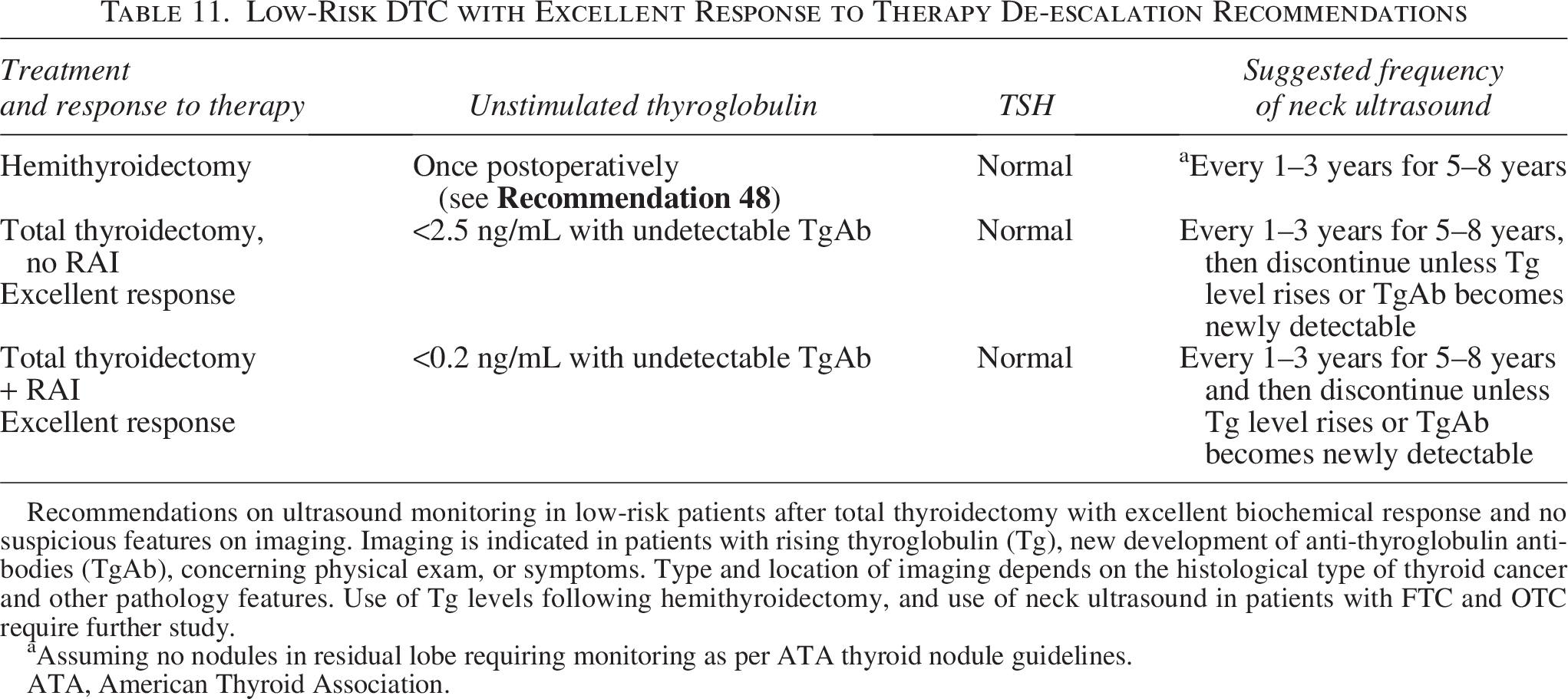
Recommendations on ultrasound monitoring in low-risk patients after total thyroidectomy with excellent biochemical response and no suspicious features on imaging. Imaging is indicated in patients with rising thyroglobulin (Tg), new development of anti-thyroglobulin antibodies (TgAb), concerning physical exam, or symptoms. Type and location of imaging depends on the histological type of thyroid cancer and other pathology features. Use of Tg levels following hemithyroidectomy, and use of neck ultrasound in patients with FTC and OTC require further study.
Assuming no nodules in residual lobe requiring monitoring as per ATA thyroid nodule guidelines.
ATA, American Thyroid Association.
Introduction to de-escalation of long-term monitoring in low-risk DTC
In patients with low-risk PTC treated with total thyroidectomy who have achieved sustained excellent response, lifelong thyroid cancer monitoring is likely unnecessary due to the outstanding long-term prognosis. Lifelong biochemical assessments and neck ultrasounds are associated with financial and psychological burden that may not be justified in many patients in view of the extremely low risk of recurrence long after treatment.989,990 There are no studies to compare lifelong monitoring with an abbreviated course of follow-up, and specific timing of when to stop monitoring is not clear. Recent data on ultrasound monitoring in patients treated with total thyroidectomy for low- and intermediate-risk PTC and excellent biochemical response outlined below suggest that life-long monitoring with ultrasound is not necessary. There are patients in whom continued ultrasound monitoring is appropriate. Patients who have a history of clinical or radiographical recurrence and those with indeterminate or suspicious results on biochemical or imaging assessments should continue to undergo ultrasound monitoring. These data are limited to patients with PTC.
There are less data on de-escalating monitoring in patients with FTC or OTC, but it is important to recognize that recurrence rates are also very low for patients with low-risk FTC or OTC with undetectable Tg levels and negative imaging, as noted in
Ultrasound monitoring after total thyroidectomy for patients with low-risk DTC
Neck ultrasound monitoring is recommended to identify residual and/or recurrent structural disease in the neck and has long been used for routine monitoring for locoregional recurrences. With the more sensitive Tg and TgAb assays (functional sensitivity of 0.1 and 0.9 ng/mL, respectively) now commonplace, the role of continued long-term ultrasound monitoring to detect structural recurrences in low-risk patients after total thyroidectomy for PTC who have excellent biochemical responses has been re-evaluated. Because of variability in both surgical approach and RAI use, it is not possible to formulate a single recommendation. As total thyroidectomy followed by RAI represented the historical standard of care, most of the data come from that patient population. However, more recent studies have demonstrated that total thyroidectomy without RAI in low- risk patients is non-inferior to total thyroidectomy with RAI; thus, fewer low- risk patients have been treated with RAI in recent years. 770
DTC recurrence in the low-risk category is uncommon. When it occurs, the overwhelming majority occurs in the first 5 years after surgery.770,991–995 In addition, patients who have excellent biochemical responses early on are unlikely to develop recurrences. Most of the data reflect monitoring patients with PTC. Some studies described below include patients with low-risk FTC and OTC.
A retrospective analysis reviewed 1020 patients who underwent total thyroidectomy with or without RAI for predominantly low- (61.3%) and intermediate- (35.5%) risk DTC, with 948 patients (93%) observed to be disease-free at initial post-treatment evaluation (<12 months). The duration of study follow-up was 5.1–20.4 years, with a median of 10.4 years. Of these 948 patients, structural recurrences were found in only 13 (1.4%), all of whom had disease confined to the cervical lymph nodes or thyroid bed. Ten of the 13 patients recurred in the first 5 years, and the remaining 3 within the first 8 years. 991
A retrospective study of 501 patients with DTC who underwent total thyroidectomy and RAI found that of the 263 patients with excellent biochemical responses at 17 months (interquartile range [IQR] 14–22), only five (1.9%) patients developed structural disease at 101 months (IQR 71–126). All ATA risk groups were included in this study. 993 Another study retrospectively reviewed 2250 patients who had total thyroidectomy with or without RAI for PTC >1 cm who were biochemically and structurally disease-free on initial follow up. This cohort included higher-risk patients 992 and did not exclude patients with gross extrathyroidal extension (34%), positive surgical margins (9.3%), central (52.9%) or lateral compartment lymph node metastases (15.3%), or unfavorable histologies (1.8%). Structural recurrences were found in only 68 patients (3%), with a time to recurrence of 3.86 years in those with lymph node recurrences and 4.38 years in those with local soft-tissue recurrences or distant metastasis. In a prospective randomized trial of 726 patients with low-risk DTC after total thyroidectomy and RAI, 11 patients (2%) were found to have recurrences: 4 patients with structural disease, 5 patients with rising Tg levels but no evidence of structural disease, and 2 patients with indeterminate findings on ultrasound that were not sent for biopsy at a median of 5.4 years. All patients with structural recurrences had an elevated Tg level. 994 A randomized controlled trial of 730 low-risk patients after total thyroidectomy found recurrences in 31 patients (4%) at 3 years for both those who received RAI and those who did not, with no difference between the groups. Of these patients, five were found to have structural disease on ultrasound. 770 To investigate the need for long-term monitoring in low-risk DTC in patients with excellent biochemical response, 756 patients were retrospectively reviewed at a single institution, all of whom had low-risk DTC and achieved excellent biochemical response (stimulated Tg <1 mcg/L) with total thyroidectomy and RAI. Radiological recurrence was found in 13 (1.7%) patients, with the latest presentation of biochemical recurrence at 59 months. Only seven (54%) of the patients who recurred had a histological diagnosis of PTC, representing <1% of the cohort. 995 While there are reports of recurrences after many more years, these are very rare. 992
Ultrasound of patients at low risk for recurrence who have had excellent biochemical responses has not been found to identify clinically significant disease, but it can increase the number of interventions undertaken based on false positive findings.743,996–999 While most data reflect patients who had RAI as part of their initial therapy, some data include patients who had not received RAI. Two hundred and 26 patients who had total thyroidectomy (with or without RAI) for PTC and who were at low- or intermediate-risk for recurrence with either excellent biochemical response or low-detectable Tg levels (0.21–0.99 ng/mL) at 1 year of follow-up were retrospectively reviewed. Of the 226 patients studied, 171 had (75.7%) an excellent biochemical response at the first year of follow-up. At 3 years of follow-up, only two (1.2%) patients developed indeterminate or suspicious features on ultrasound, and only three (1.8%) patients developed these ultrasound features at last follow-up (median 72 months; range 59–94 months), resulting in an NPV of 98.8% and 98.2%, respectively. Of the 55 patients who had low detectable Tg levels, one (1.8%) developed indeterminate or suspicious features on ultrasound at 3 years, and three patients (5%) had suspicious features at the last follow up (median 86 months; 59–99 months), resulting in an NPV of 98.7% and 94.5%, respectively. Of the six patients whose ultrasounds were not considered reassuring at last follow-up, only one was suspicious, while the other five were indeterminate. All six patients showed an increase in their Tg levels or developed TgAbs. No patient required treatment. 997
Another retrospective cohort of 756 patients treated with total thyroidectomy and RAI for DTC were followed for 11.2 years; structural recurrence was found on imaging in 15 (2%) patients, 13 (85%) of whom experienced it within 5 years of surgery. All had rising Tg or TgAb levels. Six (40%) of the 15 patients who recurred had FTC or OTC. Of the nine (1.2%) patients with recurrence and PTC histology, two had high-risk disease, with the remaining seven having low- or intermediate-risk pathologies. 1000 A retrospective review of 76 patients with T1N0 to T4N1b PTCs followed by RAI with postoperative Tg levels <1 ng/mL and negative antibodies found 18 (23.7%) patients with suspicious ultrasound findings during 2–7 years of routine neck ultrasound monitoring. None of these patients proved to have recurrent disease by either pathological assessment or clinical follow-up and instead were determined to have false positive imaging results. 996
Yang et al. reported a cohort of 90 patients with intermediate-risk PTC who underwent total thyroidectomy with RAI treatment and who had Tg levels <1 ng/mL in the absence of antibodies and either negative or atypical features on postoperative ultrasound. Over a median follow-up of 10 years (range 1–15 years), nine (10%) patients developed suspicious features on ultrasound that represented clinical disease requiring intervention, and none of these patients had ever attained excellent biochemical response as defined by the 2015 ATA guidelines. Fifty-one (56.7%) patients developed new atypical features on ultrasound in the course of follow-up that led to biopsy (3 patients, 3.3%), WBS (6 patients, 6.7%), cross-sectional imaging (10 patients, 11.1%), or further ultrasound monitoring (47 patients, 52.2%), with none ultimately found to have recurrent disease. 998
Just two studies have included patients who did not receive RAI. A review of 171 patients with low-risk PTC who underwent total thyroidectomy with or without RAI and excellent biochemical response reported one patient who experienced a structural recurrence, and there were 114 false positive findings; 61% of this study group did not have RAI as part of their initial therapy. 743 The other study retrospectively evaluated 93 patients with low- and intermediate-risk PTC treated with or without RAI with excellent biochemical response and found suspicious ultrasound findings in five patients (5.4%) over a mean follow-up of 2.5 years; all these patients had RAI as part of their initial therapy, and none ultimately were found to have clinically significant disease warranting treatment. Another 19 patients (20.4%) had indeterminate findings on ultrasound at a median follow-up of 4 years, none of whom ultimately demonstrated recurrence by clinical follow-up or on FNA cytology. 999 In a SEER review of 22,000 patients, more intense ultrasound imaging and surveillance were associated with increased intervention but with no impact on patient survival. 1001 Cost analyses of thyroid cancer surveillance have found that the cost to detect recurrence in low-risk patients is up to seven times higher than that performed for intermediate- and high-risk patients. 1002
When should neck ultrasound and other imaging techniques (WBS, SPECT-CT, and 18FDG-PET-CT) be performed during follow-up?
Neck ultrasound
Considerations regarding neck ultrasound after surgery are reviewed in
Diagnostic RAI WBS
▪
Patients who have undergone lobectomy or total thyroidectomy without RAI should not undergo surveillance radioiodine WBS. Patients with DTC who are at low- and low-intermediate risk of recurrence and who have excellent response to therapy do not require routine diagnostic radioiodine WBS during follow-up. ( Patients with DTC who are at intermediate-high and high risk of recurrence can be evaluated with diagnostic radioiodine WBS to evaluate for iodine-avid disease if there is clinical suspicion for recurrence. WBS, if undertaken, can be performed with 123I or low activity 131I. SPECT-CT radioiodine imaging may be performed in addition to planar imaging to anatomically localize the radioiodine uptake and distinguish between likely cancer and nonspecific uptake
Patients whose native thyroid is still in place do not benefit from RAI WBS in efforts to detect recurrence, as the gland remnant is sufficiently iodine-avid to frustrate efforts to identify cancer in other sites. Thus, the utility of follow-up WBS is dubious in patients who have not received (and are not planned to receive) RAI as part of their treatment.
Following RAI ablation or adjuvant therapy, when the post-therapy WBS does not reveal uptake outside the thyroid bed, subsequent diagnostic WBS has low sensitivity and is usually unnecessary in patients who have achieved an excellent response as defined in the 2025 ATA guidelines, particularly for patients with low-risk DTC.1003–1005
A subsequent diagnostic WBS may be indicated primarily in three clinical settings: (i) for patients with abnormal uptake outside the thyroid bed on post-therapy WBS, (ii) for patients whose post-ablation WBS is of limited use because large thyroid remnants with high uptake of (>2% of the administered activity at the time of scan) obscure the detection of lower uptake in neck lymph nodes, and (iii) for patients with rising or elevated TgAb levels (who are at risk of false negative Tg measurement) even when neck ultrasound does not show any suspicious findings; 123I is preferred generally over 131I for these indications for diagnostic body scan because it delivers lower radiation doses to the body and provides better-quality images.
Scintigraphy (131I or 123I ) should include planar images of the whole body. These images may be supplemented with SPECT when available, or spot images of the neck, mediastinum, and on any abnormal focus of RAI uptake when SPECT is not available. A WBS may be performed after the administration of either a diagnostic dose (usually 74–185 MBq, 2–5 mCi of 131I or 123I) or therapeutic administration of 131I. Because of the lack of anatomical landmarks on planar images, it may be difficult to differentiate (i) uptake in remnants of normal thyroid from lymph node metastases (especially when the remaining native thyroid is large), (ii) uptake in lung metastases from rib lesions, and (iii) accumulation of RAI in intestine or bladder from a pelvic bone lesion.
Hybrid cameras combine a dual-head SPECT gamma camera with a CT scanner in one gantry. This allows direct super-imposition of functional and anatomical images. The radiation dose delivered to the patient by the low-dose CT scan is 2–5 mSv, which is much lower than the dose accompanied by the administration of 3.7 GBq (100 mCi) of 131I (approximately 50 mSv). SPECT-CT performed after the administration of a diagnostic or a therapeutic dose (≥1.1 GBq, 30 mCi) of RAI is associated with an increased number of patients diagnosed with a metastatic lymph node and a decreased frequency of equivocal findings.830,832,1006–1010 SPECT-CT may change tumor risk classifications according to the ATA Risk of Recurrence classification and change management in some patients by decreasing the rate of equivocal findings. However, the impact on clinical care in reported series varies widely, from a few percent up to one-third of patients.832,1008–1011 Pursuit of additional imaging studies is not uncommon after identification of a likely disease site through SPECT-CT. As expected, cancers with low or absent uptake of RAI may yield a false negative SPECT-CT.
Positrons are emitted by 124I, enabling PET/CT imaging in patients with DTC. It may be used as a dosimetric and diagnostic tool to localize disease; 124I PET/CT permits accurate measurement of tumor volume and of the uptake and half-life of 124I in each disease site, thereby allowing for a reliable dosimetric assessment. While these lesional dosimetry metrics have demonstrated promise, they have not yet found widespread use owing to the investigational nature of the 124I isotope.1012–1014 Additionally, a few small single-center studies have examined the role of other positron-emitting radiopharmaceuticals in detecting DTC, including [18F]-tetralfuoroborate (TFB), 1015 [68Ga]PSMA-11, 1016 and [68Ga]DOTATATE/DOTANOC. 1017 The role of these novel agents in thyroid cancer remains undefined.
The sensitivity of 124I PET for the detection of residual thyroid tissue and/or metastatic DTC is generally higher than that of a diagnostic planar WBS (99% vs. 66%, respectively).1018–1022 These results were summarized in a meta-analysis, with a pooled sensitivity of 94.2% and specificity of 49.0% 1023 ; 124I PET/CT has not yet been compared with SPECT-CT in a large series of patients; 124I PET/CT is promising but not yet widely available for clinical use.
18FDG-PET/CT scanning
▪
Imaging using 18FDG-PET/CT scanning may be performed in patients with DTC at high risk of recurrence with elevated serum Tg levels, particularly in patients with OTC or aggressive histologies and in patients who have a history of negative RAI imaging. Imaging with 18FDG-PET/CT scanning may also be employed: (i) as a prognostic tool in patients at highest risk for rapid disease progression and disease-specific mortality and (ii) as an evaluation of post-treatment response following systemic or local therapy of invasive disease.
In patients with high-risk DTC with elevated serum Tg levels (generally >10 ng/mL) , particularly those who have negative RAI imaging, 18FDG-PET/CT is primarily employed. In a meta-analysis of 17 studies that included 1195 patients, 1024 the sensitivity of 18FDG-PET/CT was 0.86, specificity was 0.84, and the diagnostic odds ratio was 31. There was high heterogeneity and possibly publication bias, but the reported values are similar to earlier reports in non-iodine-avid DTC. 745 Other factors influencing 18FDG-PET/CT sensitivity include tumor de-differentiation, larger tumor burden, and serum Tg doubling time.1025–1027
In patients with an aggressive histological subtype (e.g., PDTC, tall cell cancers) and OTC, 18FDG-PET/CT is more sensitive; 18FDG uptake in patients with metastatic DTC is a major negative predictive factor for response to RAI treatment and an independent prognostic factor for diminished survival.1028,1029 It may identify lesions with high 18FDG uptake (SUV) that are more aggressive, warranting local treatment or more intensive monitoring. It is complementary to WBS even in the presence of detectable uptake in metastases, because 18FDG uptake may be present in sites with or without 131I uptake. However, 18FDG-PET/CT for patients with recurrent 131I-avid disease has not been widely undertaken, and so its benefit is uncertain.
Aggressive pathological variants may produce only small amounts of serum Tg, so this reference point may not be accurate for those cancers. Shorter Tg doubling time has been associated with increased demonstration of disease through 18FDG-PET/CT, but the “cut-points” vary across reports.1025,1027,1030 For patients with undetectable serum Tg levels in the setting of persistent TgAbs, the “true” Tg cannot be reliably assessed; 18FDG-PET/CT may demonstrate disease in some of these patients.
A meta-analysis from 2019 indicates that the sensitivity of TSH-stimulated 18FDG-PET in detection of disease may not be superior to that of studies undertaken in an unstimulated setting. 1024 False positive results may be found with 18FDG-PET imaging with TSH stimulation. 1031 The frequency of false positive lesions varies from 0% to 39% between series, even with TSH stimulation. These false positive rates justify a FNA biopsy with cytology and Tg measurement in the hub washout for cases where an accessible lymph node is identified by 18FDG-PET/CT (to confirm the presence of thyroid cancer prior to initiating therapy). Detection of lesions in other locations should prompt dedicated cross-sectional imaging of those regions for confirmation and clinical decision-making. Finally, it is important to recognize that 18FDG-PET is insensitive for detecting brain metastases and that standard imaging stops in the mid-thigh. Thus, if there is concern for metastases to brain or below the thighs, brain MRI and extension of images to the feet should be considered.
Is ongoing risk stratification (response to therapy) useful in guiding long-term disease surveillance and therapeutic management decisions?
▪
Ongoing risk stratification (dynamic risk assessment), when used in combination with the initial risk of recurrence, allows the clinician to provide individualized management recommendations while risk estimates evolve over time and should be used to inform timing and type of imaging.
The 2015 ATA guidelines defined an updated risk stratification system (RSS) that has been demonstrated in several studies to be predictive of recurrence. In addition, dynamic risk stratification, which assesses response to therapy over time, has been shown to correlate with initial risk category and initial response to therapy; it can predict future recurrence. The 2015 ATA RSS has been shown to be more predictive of recurrence than the original 2009 ATA RSS. A review of 2425 patients with PTC after total thyroidectomy and CLND at a single institution in South Korea between 1985 and 2009 found the accuracy of the 2015 ATA RSS was superior to the 2009 ATA RSS. Due to the inclusion of small volume micro-metastasis in cervical lymph nodes in the low-risk group by the 2015 guidelines, 258 out of 1913 (13.5%) patients who were designated as intermediate-risk by the 2009 RSS were low-risk according to the 2015 RSS. In the 2015 ATA low-risk group, only 1.1% of patients had recurrences. 1032
In addition, the ATA RSS is a predictor of response to therapy. A retrospective review of 2071 patients in 40 centers with DTC (NIFTP was excluded) reviewed recurrences 1 year after surgery based on their 2015 risk groups. Most patients had a total thyroidectomy, with only 3.5% receiving a lobectomy. Of the entire cohort, 1109 (53.6%) had low-risk, 796 (38.4%) intermediate-risk, and 166 (8%) had high-risk disease. Biochemical recurrence was assessed in patients who had a total thyroidectomy, and structural response was assessed for all patients. Overall, 76.1% of all patients had excellent responses at one year. Incomplete structural responses occurred in 1.5% of the low-risk group, 5.7% of the intermediate-risk group, and 14.5% of the high-risk group, indicating that the 2015 RSS is a strong predictor of response to therapy in the short term. 1033
Data on long-term outcomes were reviewed from 674 patients between 2000 and 2020 with a mean follow-up duration of 6.17 years at a single institution in Saudi Arabia. Of this cohort, 60% were low-risk, 18.8% intermediate-, and 21.2% high-risk based on the 2009 ATA RSS. Of the entire cohort, 68.4% had excellent responses, 9.6% indeterminate responses, 12.3% biochemically incomplete responses, and 9.6% structurally incomplete responses. Of those with excellent response to therapy, 68.1% were low-risk. Those with high-risk disease had structurally incomplete responses at a rate of 61.5%. 1034
Dynamic risk assessment during therapy or monitoring has been validated in several studies. In one review, 2184 patients treated with total thyroidectomy and RAI between 1998 and 2014 were classified by the 2009 ATA RSS and followed with dynamic risk assessment over an average of 7 years. Most patients in the initial high-risk category moved to the low-risk group with excellent responses, and only 6.4% of patients in the low-risk group were recategorized as high- risk during the follow-up period. 1035 Another study, with an average follow-up duration of 10.3 years, found that the dynamic risk stratification system was an independent predictor of structural recurrence. Structural recurrence occurred in 4.7% of patients with an initial excellent response to therapy compared with 17.1%, 58.4%, and 83.9% of patients with indeterminate, biochemically incomplete, and structurally incomplete initial responses, respectively. 1036
In addition to validating the 2015 RSS, some data have indicated that the initial response to therapy may be a better predictor of outcome than the 2015 ATA RSS. 1037 A retrospective cohort of 176 cases of PTC compared outcomes after a median of 7 years for patients stratified by recurrence risk and by initial response to therapy and found that the initial response to therapy had a higher NPV and PPV compared with the ATA RSS system. 1037
Using the proposed integrated approach, most patients achieve excellent response to therapy over time, and their response can be predicted by both initial response and improved dynamically during therapy. A single-center, retrospective cohort of 501 patients with DTC was analyzed after treatment with total/near-total thyroidectomy and RAI ablation and initial follow-up of 6 to 18 months. They were grouped by initial postoperative response to therapy (excellent, indeterminate, biochemical incomplete, and structural incomplete) and followed for a mean duration of 101 months; 258 (66.7%) had excellent, 101 (26.1%) indeterminate, 17 (4.4%) biochemically incomplete, and 11 (2.8%) structurally incomplete responses to therapy. One hundred and fourteen patients (23%) underwent an additional intervention, with 52.6% achieving excellent biochemical responses by the last assessment. At the last assessment, 417 (83.2%) of the entire cohort achieved excellent biochemical response, 1% indeterminate response, 3.6% biochemically incomplete response, and 10.2% structurally incomplete responses. 993
What does each category of dynamic risk assessment mean for patients’ risk of long-term recurrence? At the time of diagnosis, the initial risk of recurrence (Low, Intermediate, High) is determined based on pathology, preoperative and postoperative imaging, and Tg/TgAb levels if applicable, using our DATA framework for initial therapy (Fig. 5). It is used to predict overall risk of recurrence and to help guide therapeutic decision-making and the need for additional surgery, RAI, or more extensive treatment. Over time, dynamic risk assessment performed during the second assessment phase in the DATA framework for monitoring after therapy (Figs. 6, 7) helps further refine risk of recurrence estimates. This can be assessed at every visit and may change over time. Since response to therapy differs for those who have undergone total thyroidectomy or lobectomy and for those treated with total thyroidectomy with or without RAI treatment, such categories have been evaluated separately in some papers, but additional studies are needed.
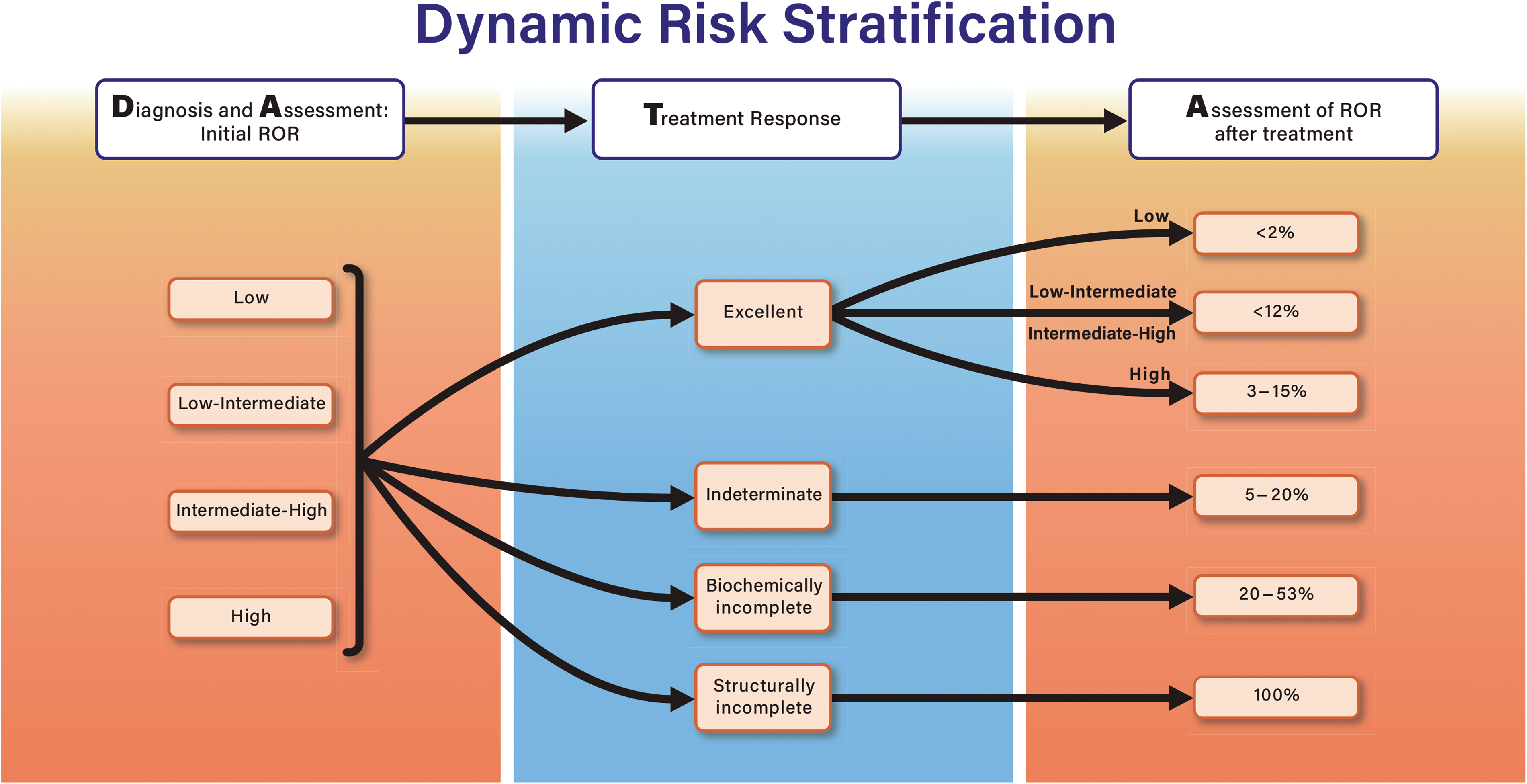
Dynamic risk stratification and DATA after initial therapy. After initial pathology, imaging, and clinical evaluations are used to estimate risk of recurrence (ROR), a treatment decision is made followed by assessing response to therapy leading to a re-estimation of ROR to inform monitoring approaches.
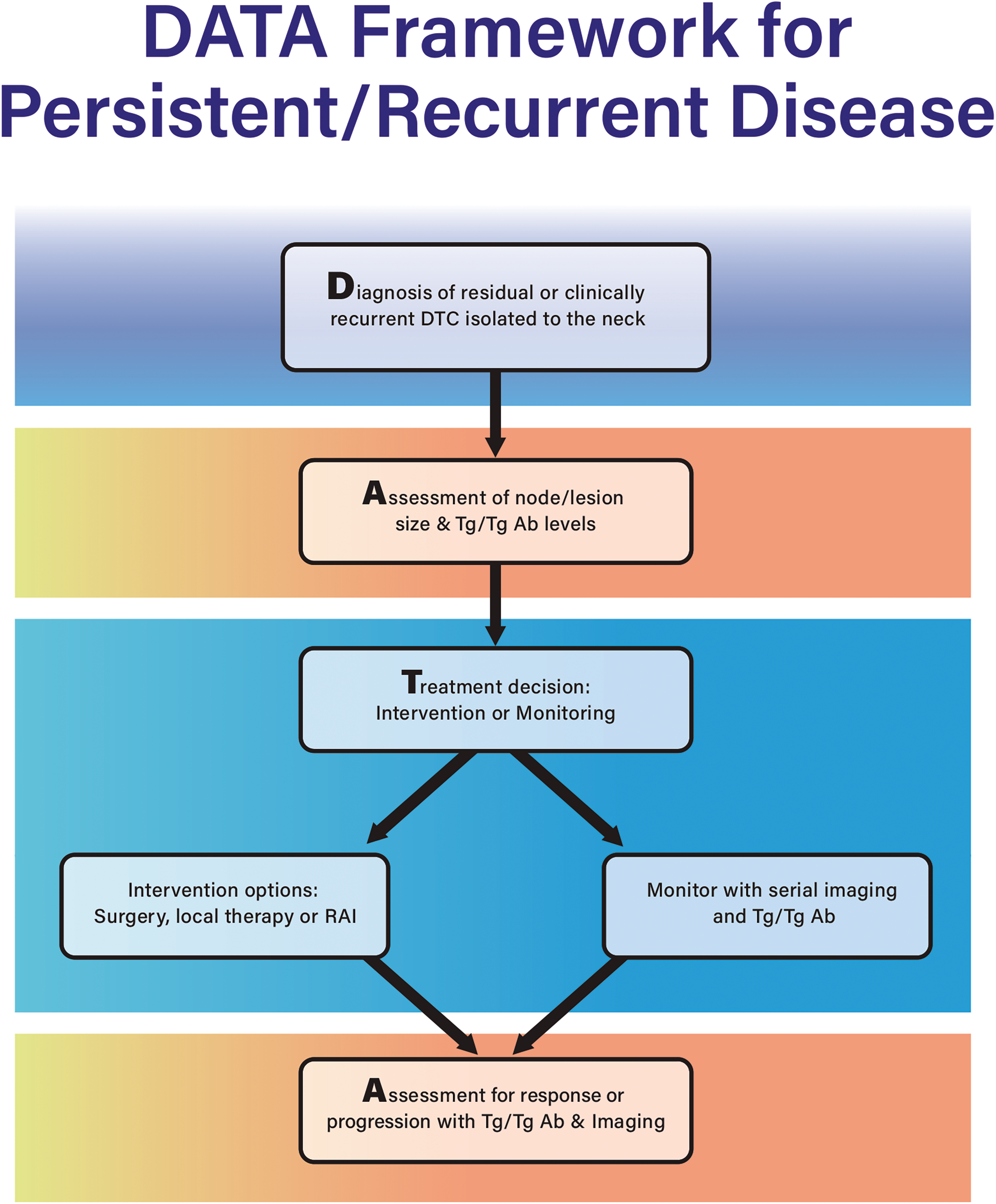
DATA framework when a patient is diagnosed with residual or clinically recurrent localized DTC in the neck.
For patients treated with total thyroidectomy and RAI
When evaluating patients from all initial risk of recurrence categories, those who achieved an excellent response to therapy had recurrence rates of 1–4%.712,729,771,1036,1038–1042 When specifically evaluating low-risk patients who achieved an excellent response, risk of recurrence was 0.2–2%.994,1043 When evaluating intermediate-risk patients, 1–12% developed a structural recurrence.1043,1044 Patients with high risk at initial assignment who achieved an excellent response experienced recurrences 3–15% of the time.602,652,712,1042,1045
For those with an indeterminate response to therapy, recurrence rates range from 5% 1046 to 15–20%.1043,1047,1048 Patients with biochemically incomplete responses to therapy experienced recurrences 20 − 53%1036,1046,1048 of the time. For this category, it is harder to determine true structural disease rates, since biochemically incomplete response was also often combined with structurally incomplete responses to therapy. The combined recurrence rates were as high as 85%.712,729,1036,1038,1041,1043,1048
For those who had total thyroidectomy without RAI
All patients who undergo lobectomy or total thyroidectomy without RAI are low- or intermediate-risk, with rare exception. Hence, these studies do not represent high risk of recurrence patients. Those with excellent responses had recurrence rates of 0–1.6%732,1047,1049,1050 in all studies except Lee et al., where a recurrence rate of 7.4% was observed. 1036
Those with indeterminate responses experienced a 0–5.6% recurrence rate.732,1036,1042,1047,1049,1050 Biochemically incomplete response to therapy was associated with a 0–31.6% rate of recurrence.732,1036,1042,1047,1049,1050 All those categorized as structurally incomplete responses experienced continued presence of disease.732,1036,1042,1049,1050
As shown in Figure 6, recurrence rates for all initial risk of recurrence categories that derive excellent response to therapy are <15%. Those with initial low risk of recurrence with excellent response to therapy have a ≤2% chance of recurrence. Those with initially high risk of recurrence have higher recurrence rates (up to 15%), so they may warrant closer follow-up, but overall, this category experiences low rates of recurrence, which supports de-escalation of monitoring with continued excellent response to therapy. For those with indeterminate or biochemically incomplete responses to therapy, recurrence rates have been reported to be as high as 20% for indeterminate and 53% for biochemically incomplete responses. These data support continued biochemical and imaging follow-up. Those with stable Tg and/or TgAb levels should have ongoing imaging. In contrast, those with rising Tg or TgAb titers should have additional imaging, including cross sectional imaging or PET/CT, to evaluate for progressive structural disease that would warrant intervention.
When and what type of treatment should be performed when there is evidence for locoregional residual, clinically recurrent, or progressive DTC?
▪
A decision to perform a therapeutic compartmental or focused central and/or lateral neck operation in the re-operative setting should be based on a combination of factors. These include extent of prior operation(s), size and anatomic location of new disease, pace of growth, patient factors and preference, and context to overall disease management. Percutaneous ethanol ablation may be considered an alternative therapy for recurrent or residual thyroid cancer, with greatest use in patients at high risk for complications from reoperation. RFA may be considered an alternative therapy in recurrent or residual thyroid cancer, with greatest use in patients at high risk for complications from reoperation.
Depending on the initial tumor risk and the response to initial therapy, imaging-detected locoregional persistent or recurrent disease can occur in up to 30–40% of patients with PTC.
168
Risk for individual patients can be estimated based on the ATA Risk of Recurrence and by category of response to initial therapy (
In prior ATA guidelines, size of a recurrent lymph nodes has been the primary determinant in consideration of surgical intervention. If a metastatic lymph node was >8 mm in the smallest dimension in the central neck or >10 mm in the lateral neck, reoperation was preferred over continued monitoring. The dimensions were selected because they represented the minimal size to be considered suspicious on imaging. Based on these recommendations, Lang et al. studied the effect of central compartment lymph node size on oncologic outcomes and morbidity of reoperative CLND. 1055 In this retrospective study of 130 patients who underwent reoperation, central compartment lymph nodes measuring >15 mm in smallest dimension represented an independent risk factor for biochemical incompleteness (compared to individuals with smaller disease); individuals grouped by disease <10 mm and between 10–15 mm did not differ from one another. Those patients with disease >15 mm had a significantly higher incidence of recurrent laryngeal nerve involvement and a higher rate of temporary, but not permanent, vocal cord paresis. These findings suggest that the previous threshold of 8 mm might potentially be increased to ≥15 mm in the central neck.
Multiple factors in addition to size should be considered when determining if reoperation is appropriate for recurrent disease in the neck, including proximity of metastatic lymph nodes to adjacent vital structures and the functional status of the vocal cords. Patient comorbidities, motivation, and emotional concerns also should be assessed, along with primary tumor factors (high-grade histology, Tg level doubling time, RAI avidity, and 18FDG-PET avidity). In an environment of collaborative transdisciplinary management, metastatic lymph nodes can be monitored for progression in appropriately selected and counseled patients via serial clinical and radiographical monitoring. Surgery or other “rescue” interventions usually can be offered if progression is observed. If disease remains stable, then monitoring can continue. Decisions about when to monitor versus proceed with an intervention should use shared decision-making with the patient and include an experienced multidisciplinary team.
Bulky and/or invasive recurrent disease is generally best treated with surgery.321,1059–1062 The judgment to offer surgery for recurrent nodal disease in the neck should compare two domains: (1) the (increased) risks of revision surgery balanced against (2) resection constituting optimal treatment for macroscopic (gross) nodal disease. An important element in this decision-making process is the availability of expertise in the performance of reoperative thyroid cancer surgery, which is chiefly to be found in referral centers. The decision to treat cervical lymph node recurrences with surgery should be made with consideration of the presence of distant disease and whether progression has been seen. Even in the setting of progressive distant disease, reoperative lymphadenectomy may be indicated to palliate symptoms and/or prevent aerodigestive tract obstruction or invasion. Transdisciplinary coordination of care is key for such complicated patients. Patient perspective and preferences are of paramount importance when weighing risks and benefits. 302 Cytological confirmation of disease can be deferred if the findings will not change management. While cytological confirmation of abnormal radiographical findings prior to resection is generally advised, this may not be necessary (or possible) in every case (e.g., radiographical findings assigned a very high likelihood of malignancy based upon growth or symptoms, or the specific location of the lesion making it difficult/impossible to biopsy).
Reoperation is the most appropriate management for most patients with clinically apparent, macroscopic nodal disease identified via imaging rather than through serum Tg level elevation; meticulous anatomical characterization is crucial to inform the surgical approach.240,241,629 In view of the increased risks of revision surgery, a clearly identified technical goal is mandatory. The risks of operations are strongly informed by the exact location of the recurrence/target node(s) and the extent to which the surgical field in question was previously manipulated. For example, the risks are elevated if there are recurrent central compartment lymph nodes after thyroidectomy, but typically less in the setting of lateral neck dissection following previous removal of a single node (berry-picking). The disease target must be defined by high-resolution anatomical studies such as ultrasound or CT with contrast, and by 18FDG-PET/CT or RAI-SPECT/CT (as opposed to PET or RAI scan alone), to permit best preoperative planning. Ultrasound-guided FNA for cytology and Tg measurement in the aspiration sample should be performed to confirm the nodal recurrence prior to surgery when feasible.
Because of the increased risk of recurrence with ‘‘berry-picking,’’ compartmental dissection is recommended in the primary setting (Recommendation 20)1063,1064 and during reoperation if it proves possible; recurrences in the environment of previous compartmental dissection usually are not amenable to formal lymphadenectomy because node-bearing tissues have been removed. Hence, planned reoperative dissection may be more limited, depending upon the surgeon’s assessment of the safety of the procedure in the context of scarring/distortion of anatomy (from prior surgery and/or radiation therapy) and the likelihood of complications. Revision lateral neck dissection involves Levels II, III, IV, and sometimes V, especially if a less than complete compartmental dissection was previously performed. Reoperative central neck dissection usually includes at least one paratracheal region with prelaryngeal and pretracheal sub-compartments. Bilateral central neck dissection is to be advised only when required by recurrence on both sides of the neck due to risks of bilateral recurrent nerve injury and permanent hypoparathyroidism. In modern series reported according to the most recent response nomenclature, reoperative surgery results in 27–63% excellent responses, 5.7–13.3% biochemically incomplete responses, 10–44% structurally incomplete responses, and 8.6–30% indeterminate responses.1065–1067 Patient age >45 years, aggressive histology, and LNR >0.6 at initial resection were found to be independent risk factors for an incomplete response after reoperation. 1067 In these reports, risk of permanent hypoparathyroidism ranged from 0% to 5.9%, and risk of permanent vocal cord paresis ranged from 0% to 1.3%, suggesting that reoperative central compartment surgery is safe in expert hands.
Percutaneous ethanol ablation for patients with metastatic lymph nodes has been employed as a nonsurgical directed therapy for patients with recurrent DTC. While no prospective comparisons between percutaneous ethanol ablation and surgery for recurrent disease have been performed, a meta-analysis of 27 studies including 1618 patients indicated that surgery has a success rate of 94.8% compared with 87.5% with percutaneous ethanol ablation, but that complications associated with surgery were slightly higher. 1068 Because percutaneous ethanol ablation encourages the clinical team to address an individual lesion rather than pursuing a compartmental approach, reoperative surgery is still considered the first-line therapy for patients with recurrent DTC. As is true with reoperative surgery, percutaneous ethanol ablation is best performed by clinicians with expertise in the technique and ideally should be performed for disease that is cytologically proven based on FNA.
Most published studies are limited to percutaneous ethanol ablation for patients who underwent prior neck dissections with RAI treatment and to individuals who have FNA-proven DTC in a lymph node. The largest study to date included 44 patients treated with ethanol injection for lymph nodes with metastatic PTC; it showed local control in 80% of patients, with a median follow-up of 11.3 years and no major complications.1069,1070 A total of 13 recurrent lesions occurred in 10 patients at the previous ablation site (19% recurrence); most of these were found in the lateral neck. Another study retrospectively reviewed 25 patients who had 37 lymph nodes ablated with a mean follow-up of 65 months. 1071 Most of the lymph nodes shrank, and 46% completely disappeared. Serum Tg levels declined in most patients and entered an acceptable range (<2.4 ng/mL) in 82% of patients without TgAb. There were no serious or long-term complications. One series demonstrated durable responses following ethanol injection, reporting that 87% of 71 lesions responded completely at a mean of 40.5 months. Another study showed a decrease or no growth in 75.6% of the 46 lesions ablated over a mean of 74 months1072,1073; again, there were no long-term complications. Some patients required more than one percutaneous ethanol ablation treatment. These retrospective studies and reviews suggest that percutaneous ethanol ablation is a safe procedure warranting consideration in patients who are poor surgical candidates due to high anesthesia risk, multiple prior operations in the disease bed, or previous neck irradiation.
RFA under local anesthesia for the treatment of recurrent DTC also has been reported over the last several years. As might be expected, the overwhelming majority of studies were undertaken retrospectively. Short-term results (with follow-up periods ranging from 21 to 36 months) of RFA for nodules with a mean maximum diameter of 0.8–1.4 cm were associated with a mean volume reduction that has ranged between 95% and 98%, with complete disappearance of metastatic foci in 61–94% of the cases.1074–1078 A recent meta-analysis revealed that the serum Tg level decreased after RFA; the pooled proportion of reduction in serum Tg levels after RFA was 71.6% [CI 63.5–79.7%]. 1079 Chung et al. reported an experience with 46 recurrent DTC lymph nodes (median largest diameter, 0.84 cm ±0.47) in 29 patients 1080 after a mean follow-up of 80 months. The study observed that the tumor volumes exhibited a mean reduction of 99.5% and complete tumor disappearance in 91.3% by the final evaluation. There were significant reductions in Tg levels, and there were no delayed complications noted.
Choi et al. examined patients with local recurrences after primary surgery and compared the efficacy and complication rates between the RFA (n = 96; 67% central, 33% lateral) and revision surgery groups (n = 125; 43% central, 57% lateral). 1081 After propensity score adjustment, the recurrence-free survival rates were similar between the two groups (p = 0.2), as was the decrease in mean serum Tg levels post-treatment (RFA p = 0.891 and surgery p = 0.963). They showed no significant differences between groups with respect to procedural complications and voice changes. Overall complications were significantly more frequent in the surgery group (RFA, n = 7; surgery, n = 27; p < 0.001); 13 of 70 surgical patients experienced permanent hypocalcemia, but no patient in the RFA cohort was similarly affected.
As with percutaneous ethanol ablation, multiple treatment sessions often are required. Immediate complications include discomfort, pain and sensation of heat, hematoma, and changes in voice. 1082 A meta-analysis evaluating safety of RFA in recurrent DTC found overall and major complication rates of 10.98% and 6.71%, respectively. 1083
Both percutaneous ethanol ablation and RFA appear to be most useful for patients at high surgical risk rather than as an equivalent alternative to resection of metastatic disease.1082,1084 Preliminary findings using ultrasound-guided laser ablation for treatment of cervical lymph node metastases have been reported.1085–1087 There has not yet been a randomized trial comparing observation with these minimally invasive techniques in the setting of small lesions. Such studies are necessary to determine their optimal use. Additional experience is needed interpreting radiographical response to the therapies and whether they are superior to monitoring.
Should RAI therapy be used for the treatment of isolated cervical lymph node metastases?
▪
Additional RAI therapy for identified isolated cervical lymph node metastases may be considered after local therapy has been performed or if local therapy is not feasible.
Hirsch et al. retrospectively studied the effect of a second RAI treatment in a cohort of patients with DTC with incomplete biochemical/structural response to initial treatment with surgery and RAI in the absence of distant metastases. 1088 For the incomplete biochemical response cohort, 44 of the 60 patients with evaluable data (73.3%) still had an elevated Tg level 1–2 years after the second RAI treatment. For the incomplete structural response cohort who underwent re-treatment with RAI alone (median lesion size 11.6 mm), no significant change in stimulated or unstimulated Tg levels ensued 1–2 years after the second RAI treatment. Three of 47 (17.6%) patients had resolution of their nodes based on imaging follow-up 1–2 years after the second RAI dose. Of the remaining 44 patients, 10 (22.7%) showed locoregional structural progression, 2 (4.5%) showed a decrease in nodule size, and 26 (59.0%) experienced stable disease. These data suggest limited benefit of a second RAI treatment in patients with DTC with biochemical or structural evidence of persistent locoregional disease. Hung et al. retrospectively evaluated use of RAI after reoperation for recurrent or persistent disease. 1089 Of 102 patients undergoing reoperation, 50 (49.0%) received additional RAI. Median Tg levels at all timepoints studied were similar between the reoperation with RAI group and the reoperation without RAI group (Tg before reoperation, 3.3 ng/mL vs. 2.4 ng/mL, respectively; Tg after reoperation, 0.6 ng/mL vs. 0.2 ng/mL; and Tg after RAI, 0.5 ng/mL vs. 0.2 ng/mL; all differences were nonsignificant). Structural recurrence after reoperation occurred in 18 of 50 patients (36%) in the reoperation with RAI group and 10 of 52 patients (19%) in the reoperation without RAI group. In multivariable analysis accounting for clinicopathologic characteristics and Tg levels before reoperation, administration of RAI after reoperation was not associated with the rate of a second structural recurrence, suggesting limited benefit of this approach. Piccardo et al. found RAI after reoperation for DTC recurrence was significantly associated with better progression-free survival in patients with a suppressed Tg of >1 ng/mL. 1090 It should be noted that the evidence to support this recommendation is low quality, and prospective studies could be helpful in identifying patients for whom repeated RAI may be appropriate.
Should external beam radiation therapy be used in isolated cervical node metastases?
▪
EBRT using modern techniques such as IMRT and stereotactic radiation may be considered for locoregional recurrences that are not surgically resectable or when there is extranodal extension or involvement of soft tissues.
Stereotactic body radiotherapy (SBRT) can be used to treat isolated metastatic foci, but it does not have a role in most patients with resectable lymph node metastases. As outlined in detail in
What preparation and dosing strategies should be used for RAI therapy for locoregional and/or distant metastases?
▪
Empirically administered amounts of 131I >5.5 GBq (150 mCi) that have high potential to exceed toxicity parameters should be avoided in patients >70 years or with renal failure. Such patients should be evaluated with dosimetry to confirm safety prior to RAI administration if doses >5.5 GBq (150 mCi) are being considered. Dosimetry-guided RAI (either lesional or maximum tolerated activity) may be considered in patients with locoregional or metastatic disease when administered activities >5.5 GBq (150 mCi) are considered. rhTSH-mediated elevation or LT4 withdrawal may be utilized to prepare patients with distant metastatic disease who are being treated with RAI.
The optimal therapeutic activity for treatment of locoregional or distant metastases remains controversial.760,1091–1094 In general, activity selection strategies include imaging-adapted, risk-based fixed dosing, or dosimetric approaches including MTA or lesional dosimetric methods.781,1095–1100 The primary advantage of a fixed dosing strategy is its relative ease and straightforward application, while use of lesional dosimetry potentially allows for more precise administration of biologically guided activity to be based on the patient’s unique tumor burden and physiology. In the MTA dosimetry approach, serial blood sampling and/or imaging are used to determine the maximum safely administered activity, which has been empirically determined to be a dose not >2Gy (200 rads) to the blood, and not >4.44 GBq (120 mCi) retained in the whole body 48 hours post-administration (or 2.96 GBq, 80 mCi in the case of patients with diffuse lung metastases).781,875 With the lesional dosimetry approach, pre-therapy imaging is used to prescribe a predicted radiation dose to thyroid remnants or sites of metastatic disease. 1101 Use of dosimetry for administered activity is favored in patients with renal insufficiency,1102,1103 children,1104,1105 older patients (>70 years of age), and/or patients with extensive pulmonary or bony metastases.
Comparison of outcomes among these methods is difficult, and no prospective randomized trial has delineated the optimal approach. One retrospective study concluded that patients with locoregional disease were more likely to respond after dosimetric therapy than after empirical dosing. 784 Another study demonstrated improved efficacy of administration of dosimetric maximal activity after failure of empirical dosage. 1106 Arguments in favor of higher activities cite a positive relationship between the total uptake per tumor mass and outcome, 1107 while others have not confirmed this association. 1108 The study by Deandreis et al. demonstrated equivalent overall survival benefit between MTA-guided dosimetry therapy and empirical treatment, although this work was limited by its retrospective design and major differences between the study populations.1109,1110 In specific settings (i.e., patients with radiation-induced DTC after Chernobyl), radioiodine treatment may be associated with good outcomes even in high-risk patients with metastatic disease. 1111 In principle, improved imaging methods including 124I PET and 123I/131I SPECT have the potential to augment the accuracy of dosimetric methods.1112,1113 Considering cost and logistics with multi-time point dosimetry, simplified dosimetry methods have been proposed.1112,1114,1115 These typically employ a simplified single time-point measurement after administration of a diagnostic dose of 123I, 124I, or 131I to estimate maximum tolerated dose.
The efficacy of RAI therapy is related to the mean radiation dose delivered to neoplastic foci and to the radiosensitivity of tumor. 1116 Radiosensitivity is higher in patients (i) who are younger, (ii) with small metastases from PTC or FTC, and/or (iii) with RAI uptake but no or low 18FDG PET uptake.
The maximum tolerated absorbed radiation dose, commonly defined as 200 rads (cGy) to the blood, is potentially exceeded in a significant number of patients undergoing empirical treatment. In one study, 1–22% of patients treated with RAI according to dosimetry calculations would have theoretically exceeded the MTA had they been empirically treated with 3.7–11.1 GBq (100–300 mCi) of 131I.
783
Another study found that an empirically administered activity of 7.4 GBq (200 mCi) would exceed the MTA in 8–15% of patients <70 years and 22–38% of patients ≥70 years.
782
Administering 9.25 GBq (250 mCi) empirically would have exceeded the MTA in 22% of patients <70 years and 50% of patients ≥70 years. These estimates suggest a need for caution when administering empirical activities >3.7–5.55 GBq (100–150 mCi) to older patients and those with renal failure; they support the recommendation that patients in this group undergo dosimetrically guided therapy. Patients should be counseled about the potential risks and benefits of RAI as noted in
While patients with distant metastases have traditionally been prepared for RAI therapy using thyroid hormone withdrawal, rhTSH can be used as an alternative for many patients. RhTSH preparation for RAI has been recommended for select patients with underlying comorbidities that make iatrogenic hypothyroidism potentially risky; these patients include those with pituitary disease who are unable to raise their serum TSH and patients for whom a delay in therapy must be avoided. Generally, such patients should be given the same or higher activity than would have been delivered had they been prepared with thyroid hormone withdrawal. This activity selection strategy is supported by studies demonstrating enhanced detection of metastases in patients undergoing thyroid hormone withdrawal compared to rhTSH preparation.1117,1118 The amount of radiation delivered to a metastatic lesion per mCi administered may be different for preparation with thyroid hormone withdrawal versus rhTSH, but the amount of radiation delivered to the critical and noncritical organs also may be different. Plyku et al. performed a study in which both stimulation methods were deployed in four patients, with marked differences in absorbed radiation doses in normal tissues. 1118 These findings warrant further study.
There are no randomized controlled trials comparing outcomes of preparation with thyroid hormone withdrawal therapy to rhTSH-mediated therapy for treatment of distant metastatic disease, but there is a growing body of non-randomized studies reporting use of rhTSH to prepare patients in this context.
1119
Gomes-Lima et al. demonstrated similar survival in patients with metastatic DTC prepared with rhTSH and thyroid hormone withdrawal in a retrospective cohort study of 55 patients.
1120
Small comparative studies have suggested that the radiation dose to metastases is lower with rhTSH than following withdrawal.1118,1121 Many of these case reports and series report disease stabilization or improvement following rhTSH-mediated RAI, but it is unclear whether the efficacy of this preparation is comparable to that of thyroid hormone withdrawal. Extreme or prolonged elevations of TSH may acutely stimulate tumor growth and volume of metastatic disease.1122,1123 With brain metastases or metastases close to the spinal cord or superior vena cava, swelling can compromise neurological function or produce superior vena cava syndrome. If brain or spinal canal metastases are detected, EBRT prior to RAI and high-dose corticosteroid therapy are recommended to limit the risk of acute tumor swelling (see
What RAI dosing strategies should be used for patients with pulmonary metastases?
▪
Pulmonary micrometastases can be treated with RAI therapy, and this may be repeated if the disease continues to concentrate RAI and clinically respond. RAI dosing for pulmonary micrometastases should either be empiric (3.7–7.4 GBq, 100–200 mCi, or 3.7–5.55 GBq, 100–150 mCi for patients >70 years) or estimated by dosimetry to limit whole-body retention to 2.96 GBq (80 mCi) at 48 hours with 200 cGy to the bone marrow. Radioiodine-avid macronodular metastases can be treated with RAI, and treatment can be repeated when objective benefit is demonstrated. RAI dosing either may be empiric (3.7–7.4 GBq, 100–200 mCi, or 3.7–5.55 GBq, 100-150 mCi for patients >70 years) or informed by whole-body dosimetry to limit whole-body retention to 2.96 GBq (80 mCi) at 48 hours with 200 cGy to the bone marrow.
For patients with pulmonary metastases, key criteria for therapeutic decisions include (i) size of metastatic lesions (e.g., macronodular typically detected by chest radiography, micronodular typically detected by CT, lesions beneath the resolution of CT); (ii) avidity for RAI and, if applicable, response to prior RAI therapy; and (iii) stability (or lack thereof) of metastatic lesions. 1124 Pulmonary pneumonitis and fibrosis are rare complications of high activity treatment, and they can be severe or even fatal. 1125 Dosimetric approaches to the selection of therapeutic activity with a limit of 2.96 GBq (80 mCi) whole-body retention at 48 hours with 200 cGy to the bone marrow should be considered in patients with diffuse pulmonary uptake to reduce these risks. 875 If pulmonary fibrosis is suspected, then appropriate periodic pulmonary function testing and consultation should be obtained. Pulmonary fibrosis may limit the ability to re-treat metastatic disease with RAI. 1126
Patients with pulmonary micrometastases (<2 mm, generally not seen on CT imaging) that are RAI-avid have the highest rates of complete remission after treatment with 131I.1127–1130 These patients may be treated and re-treated with RAI up to every 6–12 months, if disease continues to concentrate RAI and to respond clinically, and if pulmonary side effects are not encountered.
Macronodular pulmonary metastases that are iodine-avid also may be treated with RAI. Factors to consider are disease response to treatment, patient age, and the presence or absence of other metastases.1127,1128 Patients with solitary pulmonary metastases may be considered for surgical resection or radiation therapy, although the risk–benefit ratio for surgery is unclear.
A precise definition for “clinical response” is challenging in view of the wide variation observed in disease presentation and response to therapy. A meaningful response to RAI is generally a significant reduction in serum Tg level and/or the size (or rate of growth) of structurally apparent disease. Reduction in serum Tg level when RAI uptake does not fall or when there is a simultaneous increase in tumor size suggests cancer refractory to RAI or inadequate treatment. In the presence of widespread metastases, especially in bone, additional RAI may temporarily inhibit progression, but it is unlikely to result in cure, and the risks of bone marrow suppression or pulmonary fibrosis should engender caution when considering repeated RAI administrations. Absolute neutrophil count and platelet counts are markers of bone marrow suppression, and pulmonary function testing including diffusing capacity of the lungs for carbon monoxide can be markers of pulmonary toxicity. Other approaches should be employed once RAIR disease is encountered (see
The likelihood of long-term benefit of RAI in patients with elevated Tg levels and negative diagnostic WBS is low. 1131 While some reduction in serum Tg may be observed after empirical therapy, one analysis concluded there was insufficient evidence to support this assertion. 1132 In one small retrospective series of patients with structural disease but negative diagnostic WBS, additional RAI therapy was associated with stability of disease in 44% of patients and progression of structural disease in 56% of patients. 1133
What RAI dosing strategies should be used for patients with bony metastases?
▪
RAI for iodine-avid bone metastases has been associated with improved survival and should be employed. The activity administered could be given either empirically (3.7–7.4 GBq, 100–200 mCi) or as determined by dosimetry.
RAI for patients with bone metastases is generally not curative, but many patients with RAI-avid bone metastases experience benefit.1128,1134,1135 The dosimetrically determined administered activity of 131I may be beneficial in comparison to empirical dosing,
1107
but this has not been shown in prospective, controlled studies. In addition to improved survival, some patients receiving RAI also may have palliation of bone pain.
1136
As outlined in
When should empirical RAI be considered for Tg-positive, RAI diagnostic scan-negative patients?
▪
In the absence of structurally demonstrable disease, patients with stimulated serum Tg <10 ng/mL after thyroid hormone withdrawal or <5 ng/mL with rhTSH (indeterminate response) can be followed with thyroid hormone therapy alone, reserving additional treatment for emergence of rising serum Tg levels over time or other evidence of structural disease progression. Empiric (3.7–7.4 GBq, 100–200 mCi) or dosimetrically determined RAI therapy may be considered in patients with more significantly elevated or rapidly rising serum Tg levels where imaging (e.g., cross sectional imaging and/or 18FDG-PET/CT) has failed to reveal tumor amenable to directed therapy. If persistent nonresectable disease is localized after empiric administration of RAI, and there is objective evidence of significant tumor reduction, then repeated RAI therapy can be considered until the tumor has been eradicated or the tumor no longer responds to treatment. (
There is no recognized cutoff value for a serum Tg level above which a patient empirically should be treated with RAI. Most studies have reported primarily on patients after LT4 withdrawal with Tg levels ≥10 ng/mL; it has been suggested that a corresponding level after rhTSH stimulation would be 5 ng/mL.1131,1138–1140 Patients with a suppressed 1141 or stimulated 1142 serum Tg level of ≥5 ng/mL are unlikely to demonstrate decline without therapy, and they have higher rates of subsequent structural recurrence. In addition, a rising serum Tg level heralds clinically apparent disease, particularly if the rise is rapid.1143,1144
If serum Tg levels suggest persistent or recurrent disease but diagnostic RAI WBS is negative and structural or 18FDG-PET/CT imaging do not reveal disease amenable to directed therapy (surgery, thermal ablation, EBRT, alcohol ablation), then empirical therapy with RAI (3.7–7.4 GBq, 100–200 mCi) or dosimetrically determined RAI activities can be considered for two purposes: (i) to aid in disease localization and/or (ii) as therapy for unidentified disease. This approach may disclose the location of persistent disease in up to 50% of patients.1139,1145,1146 However, the reported range of success is wide. From a therapeutic perspective, more than half of patients with negative diagnostic WBS experience a fall in serum Tg levels after empirical RAI therapy,1140,1147,1148 but improved survival has not been shown with empirical therapy in this setting.1131,1138,1139 There is evidence that Tg levels may decline without therapy in a proportion of patients with Tg levels <10 ng/mL.713,1094,1138,1141,1144,1149–1153 The most compelling evidence for benefit from empirical RAI therapy is for multiple pulmonary metastases, which are typically not amenable to surgical management or EBRT.1138,1154
How is radioiodine-refractory DTC classified?
▪
RAIR DTC (including OTC) cannot be diagnosed in patients who have not received an ablative or treatment dose of RAI. Patients who meet criteria for RAI should receive ablative or treatment administrations of RAI to determine status. Patients who have RAIR DTC should not receive additional empiric RAI therapy. Other treatments should be considered.
Strong criteria suggesting iodine-refractory DTC include (i) absence of 131I uptake on a post-therapy scan (
Response to RAI therapy can be heterogeneous, and there is a spectrum of responsiveness. There has been controversy in defining response and refractoriness to RAI therapy.760,1155 These controversies were summarized in a recent multidisciplinary meeting and publication that promoted the following statements
1156
:
Characteristics used to classify patients as RAIR should be used to risk-stratify patients about the likelihood that their tumors will respond to RAI. They should not necessarily serve as definitive criteria to mandate whether RAI should be recommended. RAIR criteria will continue to evolve as (a) additional studies address important limitations and technical issues confounding the current literature, (b) techniques for RAI imaging are optimized and standardized, and (c) re-differentiation therapies enhance the effectiveness of RAI.
In clinical practice, patients and clinicians together must make judgments about the appropriateness of continued RAI, and so it is important to provide a framework for treatment planning. We propose the following criteria which may suggest an iodine-refractory state in patients with metastatic DTC: When a patient does not have uptake on post-therapy scans in the setting of structurally apparent disease on imaging, and/or when there is progression of disease fewer than 6 months after treatment, such a patient is unlikely to receive benefit from additional RAI administration.
Supplemental criteria suggesting less RAI sensitivity
No uptake present on a diagnostic 123I or 131I WBS in the presence of otherwise detectable disease. This criterion is known to predict less favorable response to RAI, but some fraction of patients in this category will have a positive post-therapy scan and may still derive some clinical benefit from RAI. Uptake is present in some (but not all) tumor foci on post-therapy WBS. This criterion does not preclude use of RAI but instead suggests that a multimodal treatment approach could be appropriate depending on therapeutic response. RAI alone is not adequate treatment for this subgroup of patients.
Prognosis for patients with DTC is usually favorable, even when metastatic iodine-avid disease is present.
1157
For this reason, RAI is considered primary treatment for RAI-avid metastatic disease. However, a subgroup of patients with DTC with advanced disease do not respond, or become refractory, to RAI; while some of these patients die within 3–5 years, there are also long-term survivors with stable or very slowly progressive disease.
Predictors for tumor response to RAI treatment are presence of 131I uptake, younger patient age, well-differentiated histology, small metastases, and low 18FDG uptake. These parameters are closely related1154,1158,1159 and can predict response to treatment. About two-thirds of patients with metastases demonstrate 131I uptake in them, and only half of such individuals will be cured with repeated courses of RAI.
Less clear is the case of patients with uptake in all known lesions who do not achieve a complete response despite several treatment courses but whose disease remains stable and does not progress according to RECIST criteria (see below). In the absence of randomized studies, it remains controversial whether these patients should be considered iodine-refractory (and thus whether RAI treatment should be abandoned in favor of other treatment strategies). The probability of obtaining a cure with more RAI is low, and the risks of dose-related toxicities may increase (see above). There are several considerations, including response to treatment and absence of tumor progression since a prior treatment, a high or significant level of uptake on post-therapy WBS, low 18FDG uptake, and good tolerance (absence of side effects) from the RAI therapy. It is important to consider patient preparation with low iodine diet and other confounding variables that may lead to misinterpreting the most recent scan as negative.
Which patients with metastatic DTC can be followed without additional therapy?
▪
Patients with RAIR metastatic DTC that is asymptomatic, stable, or minimally progressive, or who have clinically significant comorbidities, can be monitored on TSH-suppressive thyroid hormone therapy with serial radiographic imaging every 3–12 months. In the absence of planned systemic treatment or redifferentiation therapy, molecular testing is not routinely recommended in patients with RAIR residual DTC.
Patients with metastatic RAIR DTC often have an indolent clinical course, with no apparent symptoms or adverse impact from their disease burden for many years. Once RAIR metastatic disease is identified, attention should be directed toward (i) determining the extent of metastasis on imaging studies such as CT, 18FDG-PET/CT, or MRI; (ii) clinically assessing the patient for symptoms, risk of symptomatic progression, and comorbidities; and (iii) determining the rate of progression of radiographically evident lesions. Serial assessment of the size and development of metastatic lesions can be enhanced by applying criteria similar to RECIST version 1.1, as commonly used to assess tumor response in clinical trials.
1160
Representative soft tissue metastatic lesions, typically ≥1 cm, are identified as “targets” on cross-sectional imaging, with the longest diameter of each lesion measured. Disease extent is stable or minimally progressive if the sum of the longest diameters of the target lesions increases less than 20% in the absence of new metastatic foci on sequential imaging. Notably, RECIST 1.1 does not consider bone metastases (other than soft tissue components) to be measurable; thus, the growth of these lesions also should be assessed clinically. No study has identified an appropriate frequency for the optimal timing of serial imaging, but it is reasonable to repeat the imaging studies within 3–12 months based on the disease burden; location of lesions, and other clinical factors, such as histological subtype, rate of change in size over time, and Tg doubling time.1161,1162 More frequent assessment may be considered when metastatic disease is initially identified (before a growth rate has been established) and/or there is a rapid rise in Tg level, and/or there is a change in patient symptoms. Less frequent imaging is possible if a pattern of stability is established. The development of worrisome progressive disease (whether by RECIST 1.1, the appearance of clinically significant new lesions, or impending disease-related symptoms) should prompt consideration of appropriate systemic therapy, optimally with a shared decision-making approach to individualize the treatment decisions (
For patients with RAIR DTC deemed appropriate for systemic treatment, what is the optimal approach to choosing the best therapy?
▪
Tissue-based biomarker testing to identify actionable oncogenic driver alterations in RAIR DTC should be performed prior to initiating systemic therapy for progressive disease.
The treatment landscape for RAIR DTC has evolved considerably over the last decade.1163,1164 Effective systemic therapies for patients with progressive disease have emerged regardless of histological subtype, and new personalized treatments have emerged for genotype-specific subgroups of patients. Oncogenic driver alterations that are potentially amenable to FDA-approved drug treatments are found frequently in RAIR DTC, including NTRK 1&3 fusions, RET fusions, and BRAFV600E mutations.1165,1166 In addition, other gene alterations, such as N/H RAS mutations and ALK fusions, may respond to targeted therapies. Thus, identification of an oncogenic driver may impact the choice of systemic therapy, whether treatment involves FDA-approved agents, clinical trial participation, or off-label treatment options. Toda et al. evaluated the frequency of identifying treatment-driving genomic changes in comprehensive genomic analysis of 552 patients with advanced thyroid cancer (ATC [n = 130], PDTC [n = 55], and DTC [n = 367]) using one of three testing options as part of a cancer-wide national study in Japan. Druggable genomic alterations were identified in 68/130 ATCs (52%), 16/55 PDTCs (29.1%), 1/55 FTC (1.8%), and 260/307 PTCs (85%), not only confirming the value of the testing but also pointing to therapeutic gaps for RAS-mutated thyroid cancers. 1167 This approach is supported by the American Society of Clinical Oncology Provisional Clinical Opinion on somatic genomic testing in patients with metastatic or advanced cancer, which states, “Patients with metastatic or advanced cancer should undergo genomic sequencing in a certified laboratory if the presence of one or more specific genomic alterations has regulatory approval as biomarkers to guide the use of or exclusion from certain treatments for their disease.” 1168 Further support for conducting biomarker testing when considering treatment options (specifically for patients with RAIR DTC) is provided by an AHNS Endocrine Surgery Section and International Thyroid Oncology Group consensus statement. 1169
Several tissue-based multigene panels for next-generation sequencing (NGS) are FDA-approved for biomarker identification. Multigene panel-based NGS assays are recommended over sequential genomic biomarker testing because FDA-approved biomarker-linked therapy is available for more than one biomarker in RAIR DTC.1168,1169 If genomic sequencing results are used in clinical decision-making, such testing is best performed in a certified laboratory. Although concordance across NGS assays is high, platforms differ in the genes analyzed and techniques employed. Because oncogenic kinase fusions play a prominent role in DTC, NGS assays optimized to identify oncogenic kinase fusions, such as RNA-based sequencing and/or anchored multiplex polymerase chain reaction (PCR), are preferred. 1170 In the case of a rapidly progressive cancer, selection of the assay that will return results most promptly may be preferred over a more comprehensive NGS assay, depending on cost, time to obtain results, and availability. For example, rapid testing for a BRAFV600E mutation by either immunohistochemistry or PCR may be prudent in select cases.1171–1176
With the tumor-agnostic availability of immune checkpoint inhibitors (ICI) based on a high tumor mutational burden (TMB-H), NGS testing that provides TMB-H is preferred, although TMB-H DTCs are rare, even when they are RAIR.1177–1179 Similarly, tumor-agnostic indications for ICI therapy for the treatment of microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) tumors are also significant, even though MSI-H or dMMR DTCs are rare. 1180 IHC for PD-L1 to predict possible benefit from ICI therapy is not currently considered a routine biomarker in RAI-refractory DTC, but PD-L1 status may provide useful information in some cases.1181–1183 The measurement of tumor DNA shed into the plasma (circulating tumor DNA [ctDNA]), or “liquid biopsy,” is a powerful emerging tool in oncology, particularly for the identification of genomic driver alterations when tumor biopsy is insufficient for NGS testing. 1184 In the RAIR DTC setting, large analyses validating the clinical utility of ctDNA testing have not yet been performed but may be limited by relatively sparse tumor cell shedding as compared to other cancers, and technical challenges in detecting the presence of kinase fusions.1185,1186 More study, and possibly improved assays, will be needed before measurement of ctDNA in RAIR DTC is validated. As a result, if an archival specimen adequate for tumor-based NGS testing is not available, biopsy of a locoregionally recurrent or metastatic lesion is preferred over ctDNA analysis for NGS testing.
What is the general approach for first-line therapy for patients with progressive RAIR DTC?
While response rates to first-line therapies can be high, and medications can be well-tolerated, no current therapies are curative. The ability of patients to tolerate effective doses of therapies due to side-effects and/or toxicities varies without clear pre-treatment predictors other than known comorbidities. Thus, determination of the best treatment approach for each person with progressive RAI-refractory DTC should be individualized and determined in a shared decision-making model with the patient. Figure 8 outlines the general approach to assist in clinical decision-making as an application of the DATA framework.
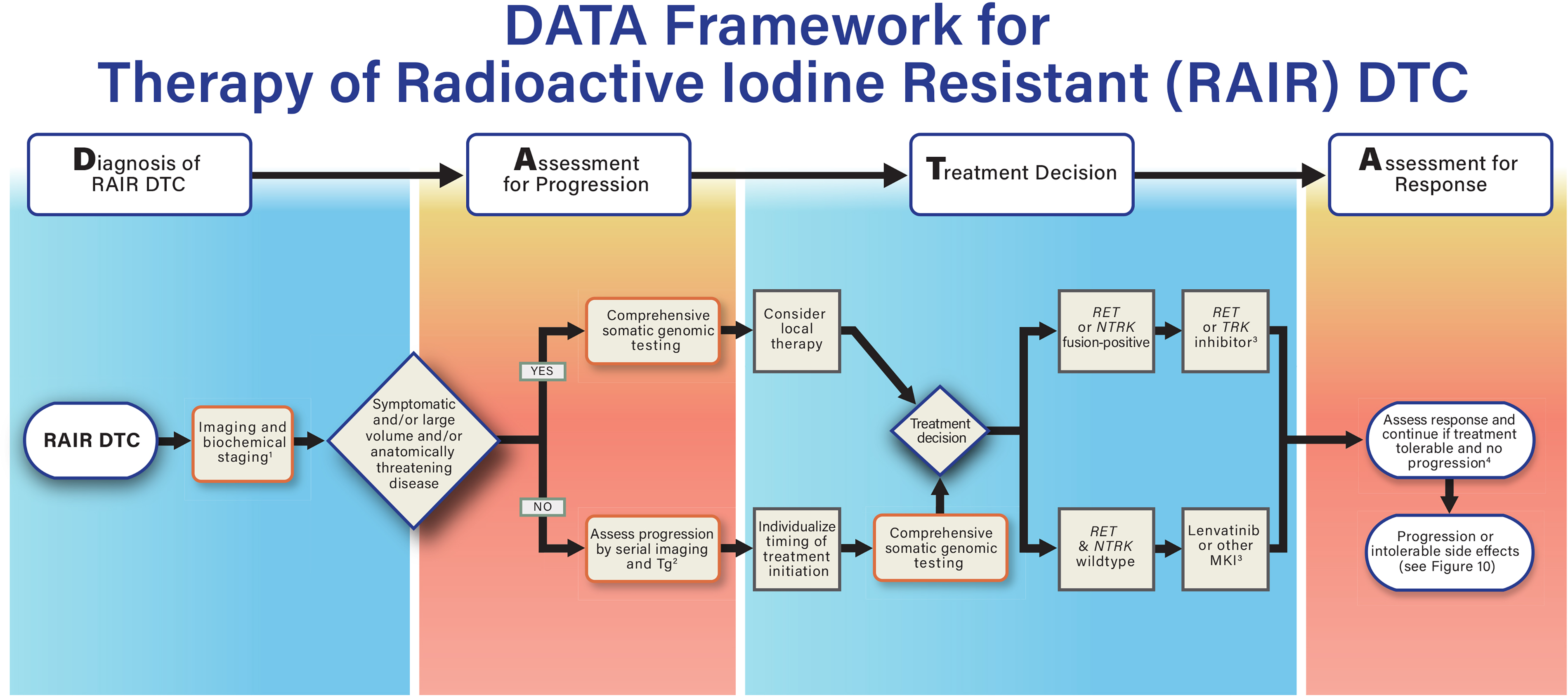
DATA framework for systemic treatment of patients with RAIR unresectable/metastatic DTC. 1) Initial staging may involve CT, MRI, and/or PET/CT. Consider brain MRI to rule out brain metastases. 2) First imaging and Tg monitoring after 2–6 months; timing thereafter is based on rate of progression and/or development of symptoms. 3) First-line gene-specific therapy in most patients with RET or NTRK fusion-positive disease is preferable. Multikinase inhibitors (MKIs) are recommended in general in patients with BRAFV600E or RAS-mutated DTC unless based on comorbidities/side effect concerns, patient preference, or clinical trial options. 4) When treatment is discontinued due to treatment related adverse events (TRAE), consider second-line therapy only after disease progression. CT, computed tomography; MRI, magnetic resonance imaging; NTRK, neurotrophic receptor tyrosine kinase; RAIR, radioactive iodine resistant.
When patients with RAIR DTC without an actionable driver alteration need systemic therapy, what is the best initial treatment?
▪
For patients with progressive RAIR DTC without an actionable biomarker-linked FDA-approved first-line therapy, MKI therapy with either lenvatinib or sorafenib is recommended. In most cases, lenvatinib is the preferred first-line MKI.
Long-term survival outcomes following RAI treatment in patients with RAI-responsive metastatic DTC are excellent. 1154 Therefore, it is critical to confirm whether patients with DTC being considered for systemic therapy have defined RAIR DTC. The DECISION trial was the first large multicenter double-blind placebo-controlled randomized clinical trial studying the MKI, sorafenib, in patients with progressive RAIR DTC. 1187 Kinases inhibited by sorafenib include vascular endothelial growth factor receptors (VEGFR) 1–3, RET, c- and BRAF kinases, and platelet-derived growth factor receptor (PDGFR) β. Key elements of the study design included the enrollment of patients with RAIR DTC with disease progression per RECIST criteria within the past 14 months. Participants were randomized to sorafenib or placebo and treated until they experienced disease progression per RECIST. At that point, participants’ treatments were unblinded and those that had been randomized to placebo were offered crossover to open-label sorafenib. Progression-free survival was the study’s primary endpoint. Secondary endpoints included the adverse event profile, objective response rate and overall survival. DECISION was a positive study, with median progression-free survival significantly improved from 5.8 months with placebo to 10.8 months with sorafenib (HR 0.59 [CI 0.45–0.76]; p < .0001). The objective response rate (all partial responses) was 12.2%, and median duration of response was 10.2 months. There was no difference in overall survival between the two groups. Of note, 71.4% of patients randomized to placebo crossed over to receive sorafenib at the time of disease progression, which may have confounded the ability to detect a difference in overall survival. Adverse events were graded according to Common Terminology Criteria for Adverse Events (CTCAE) v 3.0. The most common adverse events occurring in at least 15% of patients randomized to sorafenib were hand-foot syndrome (HFS), diarrhea, alopecia, rash, fatigue, weight loss, hypertension, anorexia, oral mucositis, pruritus, nausea, headache, cough, and constipation. Grade 3 or higher serious adverse events occurred in 37% of patients randomized to sorafenib. Dose interruption, reduction, and discontinuation occurred in 66.2%, 64.3%, and 18.8% of patients, respectively. Sorafenib was approved by the FDA and other health authorities for the treatment of progressive RAI-refractory DTC.
Exploratory analysis to identify biomarkers predictive of outcomes in DECISION evaluated tumor mutations (BRAF and N/H/K RAS), serum Tg, and plasma protein levels. 1188 No association between tumor mutational status and response to sorafenib was found; however, biomarkers associated with poor prognosis included elevated baseline VEGF and Tg levels, mutations in RAS, and the presence of wild-type BRAF. Additional real-world and pooled analyses detailing retrospective series of patients with RAIR DTC treated with sorafenib generally reported similar efficacy and safety outcomes.1189–1193
SELECT, a randomized phase III trial comparing the MKI, lenvatinib, to placebo in patients with RECIST-measurable RAIR DTC, was conducted shortly after DECISION. 1194 Lenvatinib inhibits VEGF receptors 1–3, fibroblast growth factor receptors (FGFR) 1–4, PDGFRα, and RET and KIT. Three hundred and ninety-two participants with RAIR disease measurable by RECIST v1.1 and having progressed within 12 months were randomized in a 2:1 ratio to lenvatinib 24 mg daily versus placebo. Unlike the DECISION trial, participants were allowed to receive one prior MKI. At the time of disease progression, participant treatments were unblinded, and those receiving placebo were offered crossover to lenvatinib. Progression-free survival, the study’s primary endpoint, was 18.3 months with lenvatinib compared with 3.6 months with placebo (HR 0.21 [CI 0.14–0.31]; p < 0.001). Progression-free survival was updated to 19.4 and 3.7 months, respectively, in a subsequent analysis. 1195 The objective response rate was 64.8% in the lenvatinib group, including four patients with a complete response. The difference in median overall survival between the two groups was not statistically significant (HR for death, 0.73 [CI 0.50–1.07]; p = 0.10), although evaluation of overall survival was confounded because 83% of placebo-arm patients crossed over to receive open-label lenvatinib at the time of disease progression. For patients who crossed over to lenvatinib following progression on placebo, the median progression-free survival on open-label lenvatinib was 10.1 months, and the objective response rate was 52.3%. The progression-free survival benefit with lenvatinib was seen across all histological subtypes and sites of metastasis in subset analyses. Treatment-related adverse events were common and resembled those of sorafenib, with additional side effects such as hypertension, stomatitis, proteinuria, arthralgia, and dysgeusia. Serious adverse events occurred in 49.8% of patients on lenvatinib, six of which were fatal and attributed to lenvatinib. Increases in TSH also were common on lenvatinib, and dose increases in LT4 were common. QT prolongation, arterial and venous thrombotic events, renal and hepatic toxicity, gastrointestinal fistula, gallbladder toxicity and reversible posterior leukoencephalopathy syndrome (RPLS) occurred rarely. Dose interruption, reduction, and discontinuation occurred in 82.4%, 67.8%, and 14.2% of patients, respectively. Lenvatinib was approved by the FDA and other health authorities for the treatment of progressive, RAIR DTC.
In China, a phase III trial similar to the SELECT trial randomized 151 participants with progressive RAIR DTC to lenvatinib or placebo. 1196 Median progression-free survival was significantly longer with lenvatinib (23.9 vs. 3.7 months), and the objective response rate on lenvatinib was 69.9%. The safety profile in this study was like that seen in SELECT, apart from higher rates of hypertension, proteinuria, and dose reduction in the Chinese participants.
In SELECT, circulating cytokines, angiogenic factors, Tg, and tumor BRAF and N/H/K RAS mutational status were examined to identify biomarkers predictive of clinical outcomes. 1197 The lenvatinib progression-free survival benefit persisted across all factors examined. BRAF and RAS mutations were neither predictive nor prognostic in the overall study population; however, in patients on the placebo arm, wild-type BRAF was a poor prognostic factor.
Several “real-world” studies have reported outcomes of patients with RAIR DTC treated with lenvatinib.1191,1193,1198–1206 Results generally have corroborated lenvatinib’s efficacy in terms of response rates and survival. Similar toxicity profiles were seen and considered manageable in most cases with supportive care, dose holds, and dose reductions. However, for older patients, heavily pre-treated patients and those with a poor performance status, dose reductions were more common, and efficacy was not as great as reported in SELECT.
While no randomized controlled trial has been conducted directly comparing sorafenib to lenvatinib in patients with progressive RAI-refractory DTC, attempts to identify the preferred first-line treatment have included systemic review and real-world comparisons.1193,1205,1207 Results of these studies and expert opinion have led to a general consensus that lenvatinib is associated with a longer progression-free survival benefit and higher objective response rate. While the safety profiles of the two drugs are similar, lenvatinib is the preferred first-line drug for most patients in need of (and without contraindications to) treatment.1193,1205,1208
What is the best timing for the initiation of MKIs in patients with RAIR DTC?
▪
Lenvatinib or other therapy should be initiated without delay in patients with symptomatic RAIR DTC for whom local therapy, such as radiation or surgery, is not appropriate. For patients with asymptomatic RAIR DTC that has progressed over the prior 12–14 months and local therapy is not appropriate, if efficacy outcomes are the most important goal of treatment, earlier initiation of lenvatinib may be considered. For patients with asymptomatic progressive RAIR DTC for whom QoL is a major priority, delaying the initiation of lenvatinib and continuing disease monitoring may be most appropriate.
Decisions regarding the optimal timing of MKI initiation in patients with metastatic RAI-refractory DTC can be complex, and shared decision-making with the patient is critical. MKI therapy is not curative and causes toxicity that can affect QoL. In many cases, ongoing disease monitoring by serial imaging and Tg testing, along with TSH suppression, may be appropriate, especially for patients with no impending symptoms and low-volume disease. Other individuals may have a more rapid pace of disease growth, and/or a higher volume of disease. When such patients are symptomatic (or thought to have impending symptoms), delaying the initiation of treatment may be unwise. However, there is a middle ground of patients with RAIR DTC whose disease is relatively aggressive and who will ultimately succumb to progressive disease but nevertheless have disease indolent enough that ongoing monitoring can be considered. To complicate matters, patients may hold different values. For example, some may strongly value QoL over length of life and wish to avoid adverse events from treatment as long as possible, while other patients may wish to treat their cancer aggressively. Multidisciplinary discussion may be useful; personalizing the decision on when to start MKI therapy (considering patient preferences, priorities, and concerns) is imperative.1164,1208
When considering the timing for initiating MKI therapy, one important factor is whether treatment improves overall survival. In the DECISION (sorafenib) and SELECT (lenvatinib) phase III trials, evaluation of the overall survival benefit with treatment is challenging, as both trial designs incorporated crossover to open-label MKI therapy for placebo patients at the time of disease progression. Nonetheless, two exploratory SELECT analyses indicated that an overall survival benefit was observed in two subsets of participants: namely, in patients age 65 and older and in patients with lung metastases.1209,1210 In SELECT, 71 of the 392 participants enrolled were older than 65 years. 1209 The progression-free survival benefit from lenvatinib versus placebo was maintained for participants both ≤65 and >65 years of age; however, an overall survival benefit was experienced in participants >65 years, even though the rates of crossover from placebo to open-label lenvatinib were similarly high in both groups (85% and 89%, respectively). Two hundred and twenty-six participants enrolled in SELECT harbored lung metastases. 1210 In participants with lung metastases of any size, no overall survival difference was seen in the lenvatinib compared with placebo arms. However, when a cutoff for lung metastasis of ≥1 cm was used, overall survival was significantly improved from 33.1 months in those randomized to placebo to 44.7 months in those randomized to receive lenvatinib (HR 0.63 [CI 0.47–0.85]; p = 0.0025).
Additional exploratory analyses from SELECT may provide further guidance related to the timing of initiation of lenvatinib. Performance status and neutrophil-to-lymphocyte ratio (NLR) are general markers of more advanced disease in patients with cancer. In SELECT participants randomized to lenvatinib, progression-free survival was improved in those with a performance status of 0 versus 1 and in participants with a low versus high NLR. 1211 Similarly, efficacy outcomes were superior in participants with a lower, compared with a higher, tumor burden.1212–1214 These findings suggest that for patients with progressive RAIR DTC who highly value the efficacy of treatment, it may be advantageous to initiate lenvatinib before the individual’s performance status, NLR, and tumor burden worsen. This must be balanced against an individual patient’s risk of side effects (which include treatment-related mortality), prior tumor treatments, comorbidities, and concerns regarding decline in QoL.
Patient-reported outcomes were evaluated in a multicenter expanded access program of lenvatinib among 39 patients with RAIR DTC not included in SELECT. 1215 Patients completed the European Organization for Research and Treatment (EORTC) QoL Questionnaire-Core 30 and the pain visual analog scale (VAS) at baseline and monthly for 6 months. Adverse events were graded according to CTCAE v4.0. The most common adverse events were similar to those reported in SELECT. Overall, after initiating treatment no statistically significant difference in the QoL was found. Patients reported slight improvements in general health and in emotional and cognitive status, but also a slight worsening of physical role and social functioning. Pain, dyspnea, insomnia, and constipation improved, while fatigue, nausea and vomiting, appetite loss, and diarrhea worsened. An overall reduction of the level of pain was found on the Pain VAS. While this study did not reveal a clear adverse impact on patient QoL after initiating lenvatinib, the authors speculated that the impact of treatment-related fatigue, anorexia, weight loss, and stomatitis represented a major challenge for patients on treatment.
Further investigation is needed to define the optimal timing for initiating MKI therapy. For example, discrete-choice experiments and conjoint analysis are needed to ascertain patient preferences related to MKI therapy, including thoughts on the optimal time to initiate therapy, balancing the potential impact on QoL with efficacy benefits from treatment, and identifying desired supports to enhance the patient experience during therapy.
When initiating lenvatinib treatment for RAIR DTC, what is the best starting dose?
▪
For most patients with progressive RAI-refractory DTC initiating lenvatinib, 24 mg once daily is the recommended starting dose; a lower starting dose may be indicated in selected patients. Dose holds and dose reductions are important strategies for managing adverse events related to lenvatinib.
The high rates of treatment-related adverse events, dose holds, and dose reductions encountered in SELECT led to investigation of the best starting lenvatinib dose for patients with RAIR DTC. A follow-up noninferiority study comparing the FDA-approved dose of 24 mg daily to 18 mg daily was performed, with a primary efficacy endpoint of objective response rate at 24 weeks, and primary safety endpoint of ≥ grade 3 adverse events. 1216 One hundred and fifty-two participants with progressive RAIR DTC were enrolled. At 24 weeks, the objective response rate in the 18 mg starting-dose arm was 40.3% [CI 29.3–51.2] compared with 57.3% [CI 46.1–68.5] in the 24 mg starting-dose arm. Surprisingly, ≥ grade 3 treatment-emergent adverse event rates were similar in both treatment regimens: 61.3% in the 24 mg arm and 57.1% in the 18 mg arm, a difference of −4.2% [CI −19.8 to 11.4]. The authors concluded that the approved lenvatinib starting dose of 24 mg daily is important for optimizing lenvatinib treatment but should be accompanied by dose reductions when necessary. The best starting dose for lenvatinib should be individualized, particularly in patients with comorbidities. In patients with severe renal impairment (creatinine clearance <30 mL/min) or liver dysfunction (Child-Pugh C), the recommended daily starting dose is 14 mg once daily. A lower recommended starting dose also may be advisable for patients with hypertension that is challenging to manage. Hypertension must be well controlled prior to initiating lenvatinib. Additional guidance on lenvatinib dosing was provided by an analysis of the impact of dose interruptions in SELECT. 1217 Scheduled planned drug holiday schedules also have been explored with some evidence for continued treatment efficacy, but this strategy has not been studied as a comparative trial. 1218 While lenvatinib improved progression-free survival compared with placebo regardless of the duration of dose interruptions, the magnitude of benefit was greater among patients for whom dose holds consumed less than 10% of the total treatment time (compared with those with dose holds longer than 10%) of total treatment duration. This highlights the importance of toxicity management so that dose interruptions are reduced to a minimum among those patients for whom the efficacy of treatment is the most important goal.
How should adverse events in patients receiving VEGFR MKI therapy be managed?
▪
Prevention, amelioration, and timely management of adverse events are required for patients treated with MKIs. Patients initiating MKI therapy should be evaluated at baseline and no less often than every 2 weeks for the first 2 months of treatment to manage adverse events and then generally at 1- or 2-month intervals thereafter.
Appropriate supportive care, including timely identification and management of adverse events, is essential to minimizing dose interruptions, dose reductions, and optimizing treatment for patients with RAIR DTC during MKI therapy. Adverse event prevention and careful management reduce the impact of treatment-related adverse events on patient QoL.1208,1219 Many of the MKI-related adverse events may be ameliorated by preventive care and proactive lifestyle modification.1220–1222 Thus, there is emerging interest in “prehabilitation,” or proactive preparation for patients with RAIR DTC for whom MKI therapy is planned to improve patient QoL, facilitate adherence to treatment, minimize the need for dose holds and reductions, avoid treatment discontinuation, and thereby optimize patient outcomes. Specialized consultation, including dietary, dental, dermatology, podiatry, and psychosocial supportive care, may limit the risks and discomforts that patients experience.
Hypertension is a common complication of all VEGFR MKIs.1220–1222 If untreated, MKI-associated hypertension can progress rapidly and lead to hypertensive emergencies, including RPLS. Blood pressure must be well controlled prior to initiating MKI therapy. In SELECT, treatment-emergent hypertension was found at a median of just 2 weeks after beginning lenvatinib. 1223 Thus, patients should monitor blood pressure at home daily after starting treatment. When hypertension does emerge, antihypertensive therapy should be initiated promptly to avoid RPLS, acute kidney injury, and heart failure. Studies evaluating the optimal approach to MKI treatment-emergent hypertension have not been conducted, but calcium channel blockers, angiotensin-converting enzyme inhibitors, beta blockers, diuretics, and angiotensin II antagonists all have been prescribed. 1223 Because treatment-emergent hypertension was associated with an overall survival benefit in SELECT, optimal medical management of this potentially serious adverse event is preferred over treatment discontinuation. Dose reductions may be needed in antihypertensive treatment-refractory cases. In patients with treatment-emergent hypertension for whom antihypertensive therapy has been initiated or increased, providers must remember to take the VEGFR MKI half-life into account when the MKI is held. The half-life of lenvatinib is short. When lenvatinib is held, even for a short period, antihypertensive therapy also may require adjustment.
HFS involves painful hyperkeratotic lesions and blistering concentrated on the palms of the hands and soles of the feet.1220–1222 It is more common with sorafenib but also can be seen with lenvatinib, other VEGFR MKIs, and some other chemotherapeutic agents. Patient education regarding keeping hands well-moisturized (with fragrance- and alcohol-free products) and feet dry, avoiding sun exposure and extreme hot or cold temperatures, and wearing well-cushioned shoes can reduce exacerbation of MKI-related HFS. Treatment of hyperkeratotic areas and calluses on the hands and feet is essential. These lesions should be removed before treatment initiation and during therapy. The use of a 10% urea-based cream can be beneficial. If HFS emerges during treatment, 20–40% urea-based creams can be applied to affected areas, and periodic podiatry checks may be considered. In the case of more severe toxicity, topical or systemic glucocorticoids, antibiotics, and analgesics may be needed.
Diarrhea is a common adverse event with VEGFR MKIs1220–1222 and when associated with anorexia, stomatitis, and weight loss, it can be particularly challenging for patients. Patients should keep a symptom diary; alter diet to limit diarrheagenic foods; maximize intake of high-protein, low-fat, and low-fiber foods; and maintain hydration and electrolyte intake. Probiotics and consultation with a dietician may be helpful. Over-the-counter antidiarrheals, such as loperamide, may be needed. If loperamide is ineffective, diphenoxylate/atropine is recommended.
Because MKIs can alter TSH levels, particularly in patients who have undergone thyroidectomy, TSH and free T4 must be monitored periodically and thyroid hormone replacement therapy adjusted to maintain the appropriate level of TSH suppression. Serum electrolytes (including calcium) and blood counts also require monitoring. Proteinuria is a common MKI-related laboratory abnormality that should be monitored. QTc prolongation is a class effect of MKIs, necessitating EKG evaluation before initiating treatment and periodically during treatment. VEGFR MKIs may rarely cause cardiomyopathy. Baseline echocardiogram or other nuclear cardiac function study should be considered in selected patients at increased risk, such as those with significant histories of hypertension, coronary artery disease, or diabetes. Rare but potentially life-threatening treatment-related adverse events include gastrointestinal perforation, fistula formation, bleeding, and thromboembolic events. Patients with certain comorbid illnesses, such as poor cardiac function, recent acute cardiac syndrome or stroke, uncontrolled hypertension, colitis, diverticulitis, intestinal perforation, recent bowel surgery, tumor invasion of the trachea, esophagus or great vessels, hemoptysis, or other bleeding disorder, may be precluded from safely receiving a VEGFR MKI. Treatment alternatives may need to be considered.1221,1224
It is important for clinicians and patients to recognize that combined studies from patients with many cancers describe a 1–2% mortality rate from adverse events associated with lenvatinib. Several of these studies were collated from clinical trials for a variety of cancers using high-dose therapy and undertaken prior to gaining substantial clinical experience. 1225 Data from real-world thyroid cancer clinical practice are needed to optimize selection of patients for therapy and to enhance early recognition of symptoms.
What is the preferred approach to second-line therapy for patients with RAIR DTC?
▪
Cabozantinib should be offered as second-line therapy for patients with RAIR DTC without an actionable oncogenic driver alteration who have progressed on or did not tolerate, prior MKI therapy, if they desire ongoing treatment, and do not have a contraindication to therapy.
The first evidence for clinical benefit with MKI treatment in the second line was demonstrated in SELECT. 1194 Ninety-three of the 392 participants enrolled (25.3%) had received one prior MKI. In this subset of second-line participants, efficacy of lenvatinib was similar to first-line participants, with median progression-free survival of 15.1 months and objective response rate of 62.1%. Cabozantinib, an MKI targeting VEGFR2, c-MET, RET, and other kinases, was studied in a single-arm, multicenter phase II trial enrolling participants with RAIR DTC who had progressed after no more than two prior MKIs. 1226 The primary endpoint, objective response rate, was 40%. Following this, COSMIC-311, an international double-blind, phase III trial investigating cabozantinib in previously treated RAIR DTC, was launched. 1227 Participants were allowed to receive up to two prior VEGFR MKIs, and they were randomized in a 2:1 ratio to cabozantinib 60 mg daily or placebo. At the time of disease progression, treatments were unblinded, and those receiving placebo were offered crossover to open-label cabozantinib. The study design incorporated two primary endpoints, objective response rate per RECIST v1.1 and progression-free survival. One hundred and eighty-seven participants were enrolled. Most had received either lenvatinib or sorafenib as their most recent therapy. The objective response rate with cabozantinib was 15%, which did not meet the prespecified criteria for statistical significance. However, with cabozantinib, median progression-free survival was not reached [CI 5.7 months—not estimable] compared with a median progression-free survival of only 1.9 months with placebo [CI 1.8–3.6 months] (HR 0.22 [CI 0.13–0.36]; p < 0.0001). Based on these data, the FDA-approved cabozantinib for the second-line treatment of patients with RAIR DTC who experience disease progression while receiving a VEGFR MKI. Prescribers should be aware that the cabozantinib formulation studied in COSMIC-311, Cabometyx, differs from the cabozantinib formulation, Cometriq, studied in medullary thyroid carcinoma. The most common adverse events in COSMIC-311 were HFS, diarrhea, and fatigue. Dose reductions for toxicity were required in 56% of patients, and 5% of patients discontinued cabozantinib due to intolerable adverse events.
Several other VEGFR MKIs have been studied in RAIR DTC, either in the first line or beyond. All the agents studied have demonstrated clinical activity and generally acceptable safety profiles. These include sunitinib, pazopanib, axitinib, and vandetanib.1199,1228–1233 These agents are FDA approved for other malignancies, but they have not garnered health authority approvals for the treatment of RAIR DTC. However, there may be patient-specific reasons justifying their use in select cases.
Several studies in China have explored additional MKIs for activity in RAIR thyroid cancer. Donafenib was studied in a small, randomized phase II trial examining two different doses. The objective response rate was 13% in both dose arms, but progression-free survival seemed longer with the higher dose (15.0 vs. 9.4 months, respectively). 1234 Apatinib showed encouraging activity in phase II and real-world settings, leading to the phase III REALITY study.1235–1237 In REALITY, 92 participants were enrolled and randomized to apatinib or placebo. The objective response rate with apatinib was 54.3%, and median progression-free survival was 22.2 months compared with 4.5 months with placebo. Additionally, 113 patients with RAIR DTC were enrolled in a randomized phase II trial of anlotinib compared with placebo. 1238 There was a significant improvement in median progression-free survival, from 8.4 months in the placebo arm to 40.5 months with anlotinib. Neither of these agents are available for prescription or approved by the FDA for thyroid cancer therapy in the United States.
For patients with NTRK fusion-positive RAIR DTC, what is the optimal first-line therapy?
▪
In patients with progressive RAIR DTC harboring an oncogenic NTRK fusion, NTRK-targeted therapy is recommended in the first line.
Neurotrophic receptor tyrosine kinase (NTRK) genes, NTRK 1/2/3, code for tropomyosin receptor kinase (TRK) proteins, TRK A/B/C. 1239 NTRK gene fusions are oncogenic driver alterations seen in multiple pediatric and adult malignancies, including thyroid cancer. A few rare malignancies harbor very high rates of NTRK gene fusions (>90%), whereas NTRK fusions may be seen at low rates of <1% in many more common cancers, including non-small cell lung cancer (NSCLC), colorectal carcinoma, and melanoma. The prevalence of NTRK gene fusion in PTC is approximately 7%. 1240 NTRK fusions are seen rarely in more aggressive follicular cell-derived thyroid cancers and ATC. NTRK fusions occur more frequently in PTCs diagnosed in children and young adults, at approximately 25%.1240,1241 NTRK 3 fusions are most common in thyroid cancer, followed by NTRK 1 fusions. NTRK 2 fusions have not yet been identified in thyroid cancer. Importantly, both NTRK 1 and 3 have multiple 5′ fusion partners, which is an important factor in choosing the best NGS test used to identify these alterations.
Larotrectinib is a potent and selective oral small molecule pan-TRK inhibitor. It was studied in a phase I–II program involving children, adolescents, and adults with NTRK fusion-positive malignancies. In the initial report, 55 adults and children with 17 different NTRK fusion-positive tumor types were enrolled and included in the primary analysis. 1242 The adult dose administered was 100 mg twice daily. The objective response rate by RECIST v1.1, the primary endpoint, was 75%. At the time of data cutoff, median duration of response and progression-free survival had not been reached, but the 1-year progression-free survival rate was 55%. Most adverse events were only grade 1 or 2. Of the grade 3 or higher treatment-related adverse events, the most common were anemia, increased transaminases, weight gain, and decreased neutrophil count. There were no grade 4 or 5 treatment-related adverse events. Only 15% of patients required dose reduction. Larotrectinib is approved by the FDA and other health authorities for the treatment of NTRK fusion-positive malignancy.
Updated results in 159 participants with NTRK fusion-positive cancers were subsequently reported. 1243 The objective response rate for the entire cohort was 79%; 16% of participants experienced a complete response. Median progression-free survival was 28.3 months. Thirteen participants had brain metastasis at enrollment, including four participants with thyroid cancer. Of these, nine (75%) responded. Of the 159 participants, 24 (16%) had thyroid cancers (RAI-R DTC or ATC), making thyroid cancer the most common adult tumor type enrolled. The most recently published results in NTRK fusion-positive thyroid cancer details outcomes of 29 thyroid cancer participants. 1244 Twenty patients had PTC, two had FTC, and seven had ATC. NTRK 3 fusions were slightly more common than NTRK 1 fusions. In the 21 patients with evaluable DTC, the objective response rate was 86%, including two participants with a complete response. In the participants with DTC, responses were durable, with median duration of response, progression-free survival, and overall survival not yet reached.
Entrectinib was developed as an MKI targeting TRK A, B and C, as well as the ROS1 and ALK kinases. Entrectinib was studied in a phase I/II program and an integrated analysis of 54 adult participants harboring NTRK 1, 2, or 3 fusion-driven cancers was reported. 1245 The cohort included five participants with thyroid cancer. The objective response rate of the NTRK fusion-positive patients of all tumor types was 57%, with a 7% complete response rate. One of the five thyroid cancer participants experienced a partial response. Median progression-free survival for the whole cohort was 10 months. Forty percent of patients required dose reduction, and 4% of patients discontinued entrectinib due to treatment-related adverse events. These data led to FDA approval for entrectinib for NTRK fusion-positive solid tumors and ROS-1 fusion-positive NSCLC.
The most recent updated analysis of entrectinib in adults with NTRK fusion-positive solid tumors is available in abstract form. 1246 This cohort included 150 patients with sarcoma, NSCLC cancer, secretory carcinoma, thyroid cancer, and other cancers. The objective response rate for the entire cohort was 61.3%, with a median progression-free survival of 13.8 months. Ten of the 16 (62.5%) participants with thyroid cancer responded. The median duration of response across tumor types ranged from 5.6 to 44.2 months.
In a rare tumor setting such as NTRK fusion-positive advanced thyroid cancer, opportunities to conduct clinical trials are limited. Nonetheless, in view of the available data, larotrectinib appears to be the preferred agent for treating patients with NTRK fusion-positive advanced thyroid cancer. Similarly, no robust data are available to help decide when to initiate gene-specific therapy. Because the studies were “basket trials” for patients with multiple tumor types, RAIR disease criteria for patients with thyroid cancer were not specified, and while the protocols required measurable disease by RECIST v1.1, disease progression prior to enrollment was not required. Immediate initiation of treatment may not be necessary in patients with NTRK fusion-positive thyroid cancer with low-volume disease that is asymptomatic and very slowly progressive, even if RAIR. However, when patients have clinically meaningful disease progression, the risk–benefit calculation involved in considering the initiation of treatment differs from that with VEGFR MKI therapy, due to the relatively favorable toxicity profile of larotrectinib and entrectinib. Future study devoted to optimizing the role for TRK-specific treatment in NTRK fusion-positive thyroid cancer, including involving the patient voice in decision-making, is needed.
For patients with RET fusion-positive RAIR DTC, what is the optimal first-line therapy?
▪
In patients with progressive RAIR DTC harboring an oncogenic RET fusion, RET-targeted therapy is recommended in the first line.
REarranged during Transfection (RET) codes for a receptor tyrosine kinase that, when activated by its ligand, signals through several pathways, including the RAS-MAPK and PI3K-AKT pathways.1247,1248 RET is activated in thyroid cancers via two distinct mechanisms: point mutations in MTC and gene fusions in DTC. While CCDC6 (coil-coil domain 6) and NCOA4 (nuclear coactivator 4) are the most common 5′ fusion partners with RET in thyroid cancers, more than 25 5′ fusion partners have now been identified. As with identifying NTRK fusions in thyroid cancers, the fact that RET also has numerous 5′ fusion partners makes it critical to select an NGS assay optimized for identifying oncogenic gene rearrangements with all possible 5′ fusion partners when conducting biomarker testing for treatment decision-making. RET fusions occur in approximately 10–15% of PTCs but are more common in pediatric and young cases and in radiation-induced thyroid cancers.261,1249–1254 RET fusions are less common in PDTC or ATC.
Many VEGFR MKIs, such as cabozantinib, lenvatinib, sorafenib, and vandetanib, inhibit RET along with other kinases, including VEGFR 1–3. 1255 MKIs have been studied in multiple RET-driven cancers with mixed success. Activity led to approvals of vandetanib and cabozantinib in MTC.1256–1259 It is thought that the efficacy of VEGFR MKIs in RET-driven cancers is limited by insufficient anti-RET activity ascribed to the dose-limiting adverse events. In RET-driven cancers treated with vandetanib and cabozantinib, acquired resistance can arise due to the emergence of on-target RET V804M/L mutations. This mutation at the “gatekeeper” residue blocks drug binding in the kinase pocket, leading to loss of treatment efficacy. 1260
Selpercatinib is an oral highly specific and potent RET kinase inhibitor, with limited off-target activity against other kinases, especially VEGFR2. 1260 The drug was designed to inhibit the wildtype RET kinase present in RET fusion-positive cancers, as well as to inhibit all the known RET mutations present in MTCs. Selpercatinib also was designed to overcome the RET V804M/L “gatekeeper” resistance mutations and has good central nervous system penetration. LIBRETTO-001 was a phase I/II clinical trial enrolling adolescents and adults with RET-driven NSCLC, advanced thyroid cancers and other solid tumors.1261,1262 Three thyroid cancer cohorts enrolled participants with (i) RET-mutant MTC previously treated with vandetanib and/or cabozantinib, (ii) RET-mutant MTC who had not received prior vandetanib or cabozantinib, and (iii) RET fusion-positive DTC. Radiographical tumor progression was not an explicit inclusion criterion, although systemic therapy had to be warranted. Objective response rate was the primary endpoint. Nineteen participants with RET fusion-positive DTC were enrolled, 13 with PTC, 3 with PDTC, and 1 with OTC (2 with ATC also were enrolled). Six (32%) of the participants with DTC had brain metastases. Six distinct 5′ RET fusion partners were involved, with CCDC6 and NCOA4 being the most common. The objective response rate in NMTC was 79% [CI 54–94], including a partial response in one of the two patients with ATC. The 1-year duration of response was 71% [CI 39–88], and 1-year progression-free survival 64% [CI 37–82].
Consistent with selpercatinib’s specificity for the RET kinase, the drug was overall well tolerated. Most adverse events were grades 1 and 2. The most common grade 3 or 4 treatment-related adverse events seen in 10% or more of participants were hypertension and increased alanine aminotransferase. There were no deaths attributed to selpercatinib. Similarly high response rates, durability, and tolerability were seen in LIBRETTO-001’s two MTC cohorts and NSCLC cohorts, including in tumors harboring the RET V804M/L gatekeeper resistance mutation and in participants with brain metastases.1261–1263 Selpercatinib received FDA and other health authority approvals. The FDA’s specific approval for selpercatinib is for adults with RET fusion-positive NSCLC, for adult and pediatric patients at least 12 years of age with RET-mutant MTC, and for RET fusion-positive RAI-refractory DTC who require systemic therapy.
Pralsetinib is another RET kinase-specific oral small molecule inhibitor, like selpercatinib, designed to have potent anti-RET activity with minimal off-RET kinase activity. Pralsetinib was studied in ARROW, a phase I/II trial enrolling adults with RET-driven solid tumors and the phase II efficacy results in participants who received the recommended phase II dose, 400 mg once daily, have been reported.1264,1265 Three thyroid cancer cohorts were evaluated, including patients with (i) RET-mutant MTC that previously had received vandetanib and/or cabozantinib, (ii) treatment-naïve RET-mutant MTC, and (iii) RET fusion-positive thyroid cancer. Forty-five percent of the participants with RET fusion-positive thyroid cancer had brain metastases. Of the nine participants with RET fusion-positive thyroid cancer who had measurable disease, eight responses were seen for an objective response rate of 89% [CI 52–100]. The 1-year duration of response was 86% [CI 60–100], and one-year progression-free survival was 81%.
Pralsetinib was well tolerated; adverse events were primarily grade 1 or 2. Grade 3 or higher treatment-related adverse events that occurred in 10% of participants or more were hypertension, neutropenia, lymphopenia, and anemia. Dose interruptions due to adverse events were necessary in 54% of patients, and dose discontinuations due to treatment-related adverse events occurred in 4% of patients. Pralsetinib received FDA line-agnostic approval in patients with RET fusion-positive NSCLC and RET fusion-positive thyroid cancer who require systemic therapy and are RAI-refractory. While the initially accelerated FDA approval for pralsetinib included RET-mutant MTC, its approval was subsequently withdrawn because a required confirmatory phase study would not be feasible.
There are no data available to help guide the decision to initiate gene-specific therapy in RET fusion-positive thyroid cancer. As with TRK-directed therapy, the RET-specific targeted therapies are generally well tolerated. Thus, there is not as strong a rationale to delay initiation of treatment because of concerns surrounding treatment-related toxicity and impact on QoL when patients with RAIR RET fusion-positive DTC have clinically meaningful disease progression.
For patients with ALK fusion-positive RAIR DTC, what is the optimal first-line therapy?
▪
In patients with progressive RAIR DTC harboring an oncogenic ALK fusion, anaplastic lymphoma kinase (ALK)-targeted therapy is recommended in the first line.
Oncogenic kinase fusions involving ALK have been reported rarely in PTCs, PDTCs and ATCs, with higher rates occurring in patients previously exposed to radiation.261,665,680,681,1266,1267 The most frequent 5′ fusion partners with ALK are striatin and echinoderm microtubule-associated protein-like 4, both of which contain coil–coil domains leading to homodimerization, constitutive ALK phosphorylation, and activation. While ALK-targeted therapy has been studied extensively in ALK fusion-positive NSCLC, the rarity of ALK fusion-positive thyroid cancers precludes standard clinical trial approaches. Case reports have detailed impressive efficacy of ALK-specific therapies, such as crizotinib, alectinib, and lorlatinib, in several patients with ALK fusion-positive RAIR DTC.1202,1268–1270
For patients with BRAFV600E mutation-positive RAIR DTC, what is the optimal first-line therapy?
▪
In patients with progressive RAIR DTC harboring an oncogenic BRAFV600E mutation, BRAFV600E-directed therapy may be considered in the first line for patients who are poor candidates for lenvatinib. BRAF-directed treatment is recommended in patients with BRAFV600E mutation-positive RAIR DTC who have progressed on or did not tolerate one or more prior MKI therapies. Currently approved BRAF-directed therapies are not recommended in DTCs harboring non-V600 BRAF alterations.
In view of the high rate of oncogenic BRAFV600E mutations driving PTCs, BRAFV600E-specific targeted therapy is appealing in thyroid cancer. However, to date, large-scale trials investigating BRAF-targeted therapy in BRAFV600E mutation-positive RAIR DTC have not been completed. Several small studies have demonstrated activity with this approach. The BRAF kinase inhibitor, vemurafenib, was evaluated in a multicenter phase II trial involving two cohorts. 1271 Cohort 1 enrolled 26 participants with RAIR PTC harboring BRAFV600E mutations who had not received prior VEGFR MKI therapy and cohort 2 enrolled 25 BRAFV600E mutation-positive participants who had previously received VEGFR MKI therapy. The primary endpoint was the objective response rate, which was 39% in cohort 1 and 27% in cohort 2. Median progression-free survival was 18.2 months [CI 15.5–29.3] in cohort 1 and 8.9 months [CI 5.5–not estimated] in cohort 2. Grade 3 or 4 adverse events were encountered in 66.7% of participants, the most common of which were cutaneous squamous cell carcinoma, lymphopenia, and increased gamma glutamyl transferase.
A multicenter randomized phase II trial compared dabrafenib monotherapy with dabrafenib/trametinib combination therapy for BRAF-mutated RAIR DTC with progressive disease by RECIST v1.1. 1272 Fifty-three participants were enrolled, 26 to the monotherapy arm and 27 to the combination arm. One participant’s tumor had a BRAFK601E mutation; all others harbored a BRAFV600E mutation. Prior treatments with up to three prior MKIs were allowed, and most participants had received at least one prior MKI. The primary endpoint, objective response rate, was defined as the rate of minor, partial, and complete responses. With monotherapy, the objective response rate was 46%. With combination therapy, the objective response rate was 48%. Median progression-free survival with monotherapy was 10.7 months [CI 3.8–34.7] and 15.1 months [CI 12.3–37.3] with the combination. Grade 3 adverse events occurred in 58% of patients receiving dabrafenib and in 48% of patients receiving dabrafenib plus trametinib. There were no grade 4 or 5 adverse events. Dose reductions and discontinuations due to adverse events occurred in 23% and 56%, and 19% and 22% of patients in each group, respectively. Thus, combination therapy was not superior to monotherapy in this randomized phase II DTC trial, a result that differed from the results of randomized phase III data in melanoma.1273–1275
A similar BRAF-targeted approach investigated the BRAF inhibitor, encorafenib, plus mitogen-activated protein kinase (MEK) inhibitor, binimetinib, in a phase II open-label single-arm multicenter Japanese trial enrolling patients with previously treated BRAFV600-mutated thyroid cancers. Eight of 17 patients with DTC (47.1%) experienced an objective response, with a 12-month progression-free survival rate of 79.0%. 1276
Currently, a global randomized, placebo-controlled phase III study evaluating dabrafenib plus trametinib in adult participants with BRAFV600E mutation-positive RAIR DTC (who progressed following prior VEGFR MKI therapy) is underway (NCT04940052). During this trial, dabrafenib plus trametinib has garnered tissue-agnostic FDA approval for adults and children with BRAFV600E mutation-positive solid tumors who have progressed following prior treatment and who have no satisfactory alternative treatment options. This approval was based on the Rare Oncology Agnostic Research and NCI-MATCH program enrolling multiple cohorts treated with open-label dabrafenib plus trametinib, which together accruing 131 adult and 36 pediatric participants with BRAFV600E mutation-positive solid tumors.1277–1281 A total of 54 adult participants (41% [CI 33–50]) experienced an objective response. In the 36 pediatric participants, the objective response rate was 25% [CI 12–42]; duration of response was ≥6 months for 78% of patients and ≥24 months for 44% of patients. The most common (≥20%) adverse reactions in adult patients were pyrexia, fatigue, nausea, rash, chills, headache, hemorrhage, cough, vomiting, constipation, diarrhea, myalgia, arthralgia, and edema.
Reported objective response and progression-free survival rates in small studies do not establish superior outcomes for BRAFV600E-targeted therapy versus lenvatinib for progressive DTC. Thus, lenvatinib in general is considered as first-line therapy for patients with RAIR progressive BRAFV600E-mutated DTC unless contraindications to its use are present or comorbidities suggest higher risk for lenvatinib-related side effects (e.g., fistula formation or uncontrolled hypertension). Dabrafenib plus trametinib is an FDA-approved option for patients with BRAFV600E mutation-positive cancers as second-line therapy. Its use as a first-line therapy may be considered for patients with comorbidities or who are at high-risk for lenvatinib side effects. Many patients with RAIR progressive BRAFV600E-mutated will ultimately be treated with both a MKI and BRAFV600E-targeted strategy. Ongoing studies will better address this important “order of treatment” question.
It is important to recognize that the efficacy of currently approved BRAF kinase inhibitors, which block the signaling of the monomeric BRAF kinase activated by BRAFV600E mutations, is limited to tumors driven by class 1 BRAF mutations, predominately BRAFV600E. 1282 Dabrafenib or vemurafenib has no role in the treatment of tumors harboring BRAF class 2 or 3 alterations (e.g., BRAF mutation at codon 601 or BRAF gene fusions), which signal as dimers, not monomers. Not only are these therapies ineffective at blocking activated BRAF dimers, they can also paradoxically increase BRAF signaling in this context 1283 and drive cancer progression. Newer treatments with broader efficacy across the spectrum of BRAF monomers and dimers, including BRAF non-V600E class 2 or 3 alterations, are under development. 1284
For patients with RAIR DTC harboring other potentially actionable targets, what is the optimal first-line therapy?
▪
In patients with progressive RAIR DTC harboring other potentially actionable non-NTRK/RET/ALK/BRAFV600E targets, enrollment in a clinical trial or first-line lenvatinib is suggested.
Other oncogenic targets potentially amenable to drug therapy can be identified in genomic analysis of RAIR DTC. For example, N/H/K RAS mutations are frequently present in FTCs, FVPTCs, and PDTCs and lead to upregulation of the MAPK signaling pathway.261,674,1285–1287 As such, RAS mutations represent attractive oncogenic targets for pharmacologic intervention. KRAS G12C accounts for approximately 40% of all KRAS mutations in solid tumors, and now two KRAS G12C-specific inhibitors, sotorasib and adagrasib, have received FDA approvals for the treatment of KRAS G12C mutation-positive NSCLC.1288,1289 Both agents have activity limited specifically to the KRAS G12C mutation alone. While not approved for DTC, their use could be considered if this mutation is identified.
Although not a direct inhibitor of RAS signaling, tipifarnib is an inhibitor of farnesyl transferase that can interfere with HRAS protein function, and it has been studied in HRAS mutation-positive malignancies. 1290 This phase II trial in patients with advanced, unresectable or metastatic, relapsed and/or refractory tumors that carry HRAS mutations included 13 patients with thyroid cancer. While promising activity was seen in HRAS mutation-positive head and neck squamous cell carcinoma and other malignancies, none of 13 patients with HRAS mutation-positive thyroid cancer included in the trial responded to treatment.
A broader approach targeting MAPK pathway activation also has been studied, due to the frequency of oncogenic BRAF and RAS mutations. A phase II trial investigated selumetinib, a small-molecule inhibitor of the MEK-1/2 MAPK kinases, in 39 participants with RAIR DTC. 1291 While genotyping was not required for enrollment, 12 of 26 tumors tested for BRAFV600E were positive. With only one response seen, and a median progression-free survival of 8 months, further study was not warranted. More research is needed to exploit the potential for blocking other oncogenic RAS mutations, and several novel approaches are being actively studied.
The PI3K/Akt/mTOR pathway is frequently dysregulated in FTC and PDTC.665,1292–1295 PI3K inhibitors have been developed in oncology, including buparlisib, an oral pan-class I inhibitor. The TUTYREF network conducted a multicenter phase II trial of buparlisib in 43 patients with progressive RAIR FTC and PDTC. 1296 The primary endpoint of this study was the progression-free survival at 6 months, with a 50% progression-free survival at 6 months defined as success. Thirty-five percent of the advanced thyroid cancers studied by NGS testing harbored alterations activating the PI3K pathway. The 6-month rate of progression-free survival with buparlisib was 41.7% [CI 7.7–55.5], but no patients achieved a RECIST-defined response, even though eight patients harbored an activating PI3K alteration. Thus, buparlisib has not undergone further development in DTC,
Targeting mTOR directly has also been explored as a treatment approach for RAI-refractory DTC. Everolimus has been studied in several phase II trials, resulting in objective response rates ranging from 0% to 5%, and median progression-free survival ranging from 9 to 12.9 months.1297–1299 Little activity was seen, even in patients harboring PI3K/Akt/mTOR alterations. The limited activity of everolimus as a single agent has not justified further study. Combined mTOR inhibition with other agents has also been studied. In a randomized phase II trial, the addition of pasireotide long-acting release to everolimus did not improve outcomes. 1300 More promise has been seen with combining mTOR inhibition with VEFGR MKI treatment. A single institution phase II trial of sorafenib plus temsirolimus for patients with advanced DTC enrolled 36 patients. 1301 With 8 of 36 (22%) patients responding, the study did not meet its primary goal of an objective response rate of at least 25%, but it did set the stage for further study. A subsequent single institution phase II trial of sorafenib with everolimus reported an objective response rate of 60% in 28 patients with RAIR DTC. 1302 Nine of these patients had OTC, and seven responded, prompting an Alliance for Clinical Trials in Oncology randomized phase II trial evaluating sorafenib with or without everolimus in patients with RAIR OTC (NCT02143726). This study has completed accrual; results are only available in abstract form. 1303 While progression-free survival was significantly improved with sorafenib plus everolimus, compared with sorafenib alone, objective response rate and overall survival were similar between the two arms. In view of the frequency of PI3K/Akt/mTOR pathway upregulation in advanced DTC and the number of potential pharmacologic opportunities to disrupt this pathway, more studies exploiting this therapeutic target are needed.
What is the approach for patients with progressive RAIR DTC who progress on first-line therapy or cannot tolerate first-line therapy?
While response rates to first-line therapies can be high, and medications can be well tolerated, no current therapies are curative, and treatment resistance is nearly universal. In addition, some patients cannot tolerate the medications due to side effects and/or toxicities. Thus, determination of the timing and type of second-line treatment, and/or whether such therapy should be pursued, requires careful discussion with the patient. Figure 9 outlines the general approach for second-line therapies in the following section as an application of the DATA framework.
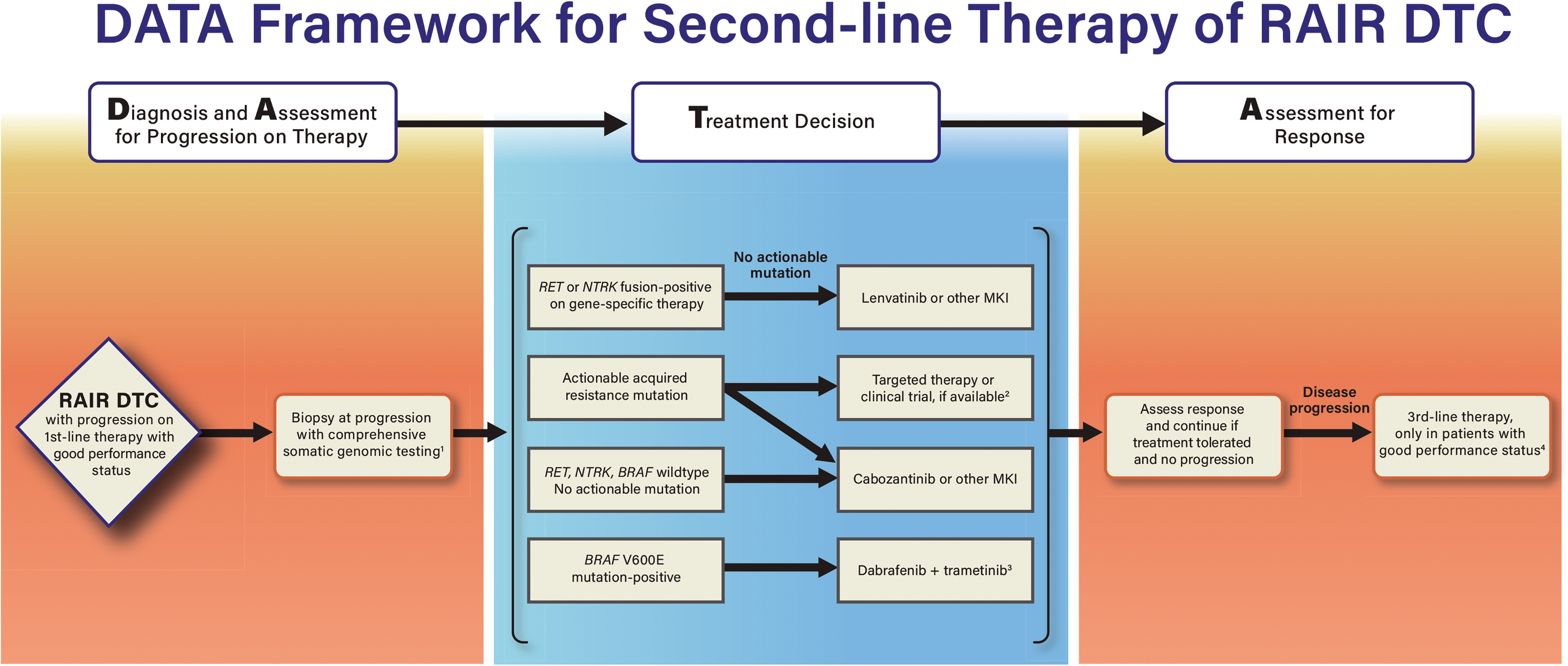
DATA framework for treatment of patients with progression on (or intolerance to) first-line therapy for RAIR metastatic DTC. 1) Biopsy of progressive disease when acquired resistance emerges is advised to evaluate for potentially actionable resistant mechanisms. 2) If targeted therapy or clinical trial is not available, cabozantinib or another MKI may be considered in patients treated with lenvatinib first-line. 3) Dabrafenib plus trametinib is FDA-approved for solid tumors with BRAFV600E mutation who have progressed on prior treatment. Dabrafenib plus trametinib was not superior to dabrafenib alone in progressive DTC; thus, dabrafenib monotherapy may be considered. 4) Enrollment in a treatment clinical trial when available is encouraged. Other third-line options may include lenvatinib, cabozantinib, or sorafenib if not already received. FDA, U.S. Food and Drug Administration.
What is the optimal approach to address disease progression in RAIR DTC on gene-specific therapy?
▪
Whenever feasible, surgical or core tumor biopsy to allow for NGS testing to identify potential molecular mechanisms of acquired resistance should be performed. Surgical or core biopsy is preferred over ctDNA analysis, which may be considered for patients in whom tumor biopsy is not possible.
In the gene-specific treatment setting, there are two basic types of resistance: primary resistance and acquired resistance. Primary resistance is defined by disease progression without an initial response to treatment. Teasing out the mechanisms of primary resistance to gene-specific treatment can be challenging, particularly because large datasets are generally needed to identify predictive biomarkers. Acquired resistance is defined as disease progression during treatment after an initial response. In the setting of gene-specific treatment, patients usually have biomarker testing by an NGS assay prior to beginning treatment. When disease progression occurs, tumor or “liquid” ctDNA biopsies for NGS testing can be performed to search for an acquired alteration (not present in the baseline studies) that may explain the development of resistance.
In NTRK fusion-positive cancers, both on- and off-target mechanisms of resistance to TRK-specific therapies have been identified. 1304 NTRK mutations that alter the conformation of the TRK kinase binding pocket have been found in tumors that have developed acquired resistance. These NTRK acquired resistance mutations are paralogous to mutations responsible for acquired resistance previously described in ALK and ROS1 fusion-positive NSCLCs. Off-target resistance mechanisms also have emerged, typically non-NTRK alterations that upregulate other oncogenic pathways, such as emergence of MET amplification, BRAFV600E mutations, and KRAS hotspot mutations. In the RET-specific treatment setting, similar on- and off-target acquired resistance has emerged.1305–1307 In some patients, despite NGS testing, no mechanism of acquired resistance is identified. More than one acquired resistance mechanism emerges in some patients. Hence, polyclonal resistance may develop, likely because of tumor heterogeneity.1307,1308 Polyclonal acquired resistance presents a particularly difficult treatment challenge.
Next-generation TRK inhibitors have been developed to overcome on-target resistance, and studies are underway. 1309 As is the case when targeting ALK and other oncogenic fusion-driven cancers, sequential TRK- and RET-specific treatments may become necessary to extend the benefits of gene-specific therapy beyond the first line, particularly to address on-target acquired resistance. On the other hand, bypass pathway mechanisms of resistance that activate a secondary oncogenic pathway pose a challenging problem. In theory, therapeutically targeting both pathways with combined gene-specific inhibitors may be possible. In the absence of clinical trials that determine safe combination dosing strategies, tolerability and efficacy, combined targeted therapy options are not generally available.
Oligo-progressive metastatic disease may be seen as a pattern of acquired resistance to gene-specific treatment. A focal approach, such as resection or SBRT (if feasible), plus continuation of the gene-specific treatment may extend the length of clinical benefit of the gene-specific treatment beyond this initial episode of disease progression. 1310 Drug-specific recommendations for holding treatment perioperatively and/or during radiation should be observed.
What is the role of immunotherapy in RAIR DTC?
▪
Immune checkpoint inhibitors or other forms of immunotherapy may be offered in selected cases, such as when tumors harbor a high tumor mutational burden or are mismatch repair deficient.
The success of ICIs across multiple malignancies has prompted interest in using ICIs for the treatment of RAIR DTC. In solid tumor oncology, the lead immunotherapy approaches involve targeting the PD-1/PD-L1 and CTLA4 immune checkpoint axes. Multiple investigations have evaluated biomarkers predictive of response to ICIs across the spectrum of malignancies. 1311 PD-L1 expression in the tumor microenvironment correlates with response in a variety of cancers. In addition, solid tumors that are MSI-H or dMMR have demonstrated high response rates to ICIs. Tumor mutational burden is another strong predictor of response to ICIs.1177,1311,1312 The hypothesis that rich peri- and intra-tumoral infiltration of CD8+ T cells (representing) responds to ICIs whereas “cold” tumors are unlikely to respond has been demonstrated in multiple settings.1313,1314
The strong immunogenicity of normal thyroid tissue, exemplified by Hashimoto thyroiditis and autoimmune-mediated hypothyroidism, prompted early interest in the tumor microenvironment of thyroid cancers. PD-L1 positivity in DTC ranges from 25% to 67% and seems to correlate with more aggressive disease.1178,1181,1182,1315–1317 Analyses of tumor-infiltrating T cells, including regulatory T cells, indicate that some DTCs do indeed harbor a “hot” tumor microenvironment, especially in more aggressive disease.1182,1318,1319 On the contrary, DTCs typically do not demonstrate a high tumor mutational burden. DTCs are rarely MSI-H, though they may uncommonly harbor a dMMR signature.665,1320
Several clinical trials investigating ICIs in advanced thyroid cancer have been conducted. KEYNOTE-028 was a single-arm, multicenter “basket” trial evaluating the anti-PD-1 monoclonal antibody pembrolizumab in PD-L1-positive advanced solid tumors. 1321 Of the 475 patients enrolled, 22 had thyroid cancer. In these 22 patients, an objective response rate of 9% was seen, which was one of the lowest response rates found across the 20 solid tumor types enrolled. Median progression-free survival in the patients with thyroid cancer was 6.8 months. This study incorporated analysis of PD-L1 staining, tumor mutational burden, and T cell-inflamed gene-expression profile. Together and separately, these three biomarkers were predictive of outcomes, but the presence of the biomarkers and correlation with response was not analyzed and reported for the individual cancer histologies. KEYNOTE-158 was a subsequent multicenter phase II basket trial of pembrolizumab in ten different advanced solid tumor histologies.1177,1322 The primary endpoint was objective response rate, and a key exploratory endpoint was the association of tumor mutational burden with response. One hundred and three patients with thyroid cancer were enrolled. The objective response rate was similarly disappointing, with only 6.8% of patients responding. Based on these results, pembrolizumab was not advanced as a standard of care treatment for patients with RAIR DTC. However, based on KEYNOTE-158, the FDA approved pembrolizumab for the treatment of adult and pediatric patients with any type of solid tumor that is unresectable, or metastatic that has progressed on other standard therapies, if that lesion is tumor mutational burden-high (determined by an FDA-approved test). Thus, pembrolizumab may be considered a treatment option for the uncommon RAIR DTC patient with tumor mutational burden-high disease that has progressed on standard of care treatment, such as first- and second-line kinase inhibitor therapy.
Efforts are underway to couple ICIs with other agents that may enhance their efficacy. One successful strategy in several tumor types involves adding a VEGFR MKI to ICI treatment based in promising preclinical data.1323–1325 Definitive clinical trials investigating the addition of VEGFR MKI to ICI therapy have been conducted in several tumor types.1326,1327 In RAIR DTC, several small studies have yielded intriguing data, including a multicenter phase II trial of lenvatinib plus pembrolizumab in two cohorts: patients with treatment-naïve progressive RAIR DTC and patients with RAIR DTC that has progressed on lenvatinib. 1328 While activity of lenvatinib plus pembrolizumab in the first-line patients did not seem superior to the activity of lenvatinib alone (demonstrated in SELECT) when pembrolizumab was added as a salvage approach to patients who experienced disease progression on lenvatinib, the objective response rate was 14%. A second multicenter phase II trial has explored this combination in patients with PDTC and ATC. Early published data and abstract presentation suggest promising activity. 1329 Other early data explored VEGFR MKI treatment with cabozantinib coupled the ICI combination ipilimumab and nivolumab in progressive RAI-refractory DTC; results were less promising. 1330 Investigations aimed at improved understanding of immune control of RAI-refractory DTC and new immunotherapy clinical trials, including investigation of chimeric antigen receptor T cell therapy, are currently ongoing (NCT04420754).
For patients with RAIR DTC, what is the role for kinase inhibitor redifferentiation therapy?
▪
Redifferentiation by MAPK pathway blockade in patients with progressive RAIR DTC harboring targetable mutations may be considered in selected patients. Clinical trial participation is encouraged. Redifferentiation approaches in adjuvant RAI treatment for patients with high-risk, non-gene selected DTC are not recommended.
RAI remains a mainstay of treatment for patients with metastatic DTC. Approaches that re-differentiate thyroid cells to enhance RAI uptake or that increase RAI retention to improve RAI treatment outcomes have long been an area of research and clinical interest. Prior efforts include use of demethylating agents and retinoic acids (for redifferentiation) and lithium (to enhance retention) either have not progressed through clinical trials or have not been shown major impact to date.
One consequence of MAPK pathway upregulation that is particularly common in DTC is suppression of thyroid hormone biosynthesis gene expression. As a result, NIS and TPO expression involved in facilitating iodine uptake and organification are suppressed.1331,1332 Preclinical studies demonstrated that disruption of MAPK can increase 124I uptake in vitro and in vivo in thyroid cancer mouse models driven by BRAFV600E expression.1333,1334 These studies led to a single-institution, single-arm study exploring the pharmacologic inhibition of the MAPK pathway in patients with RAIR DTC to reverse refractoriness to RAI. 1335 In this study, 20 patients with metastatic DTC meeting at least one of three definitions of RAI-refractory disease were treated with the MEK inhibitor, selumetinib, for 4 weeks. During the fourth week, 124I PET was performed. If this scan indicated that at least one lesion was predicted to reach a threshold absorbed dose of at least 2000 cGy, the patient continued selumetinib until receiving up to 11.1 GBq (300 mCi), based on dosimetry. Eight patients met the threshold for RAI. Five of the 20 enrolled patients met criteria for confirmed partial response by RECIST v1.1. Of interest, all five patients with NRAS-mutated tumors met the 124I threshold for treatment, while only one of nine patients with tumors harboring BRAF mutations met the threshold for treatment. One patient with wild type and one patient with RET fusion-positive disease also met criteria for RAI treatment. This pilot study established the proof-of-principle that MAPK inhibition can stimulate RAI uptake in RAIR DTC in a subset of cancers distinguished by MAPK activation. A subsequent multicenter phase II trial investigated selumetinib for redifferentiation in patients with DTC with RAIR RECIST-measurable disease that had progressed within the previous 12 months. 1336 Participants were treated with selumetinib for 28 days, followed by 123I SPECT/CT. Participants deemed to have sufficient RAI uptake continued selumetinib for two more weeks and then received 5.5 GBq (150 mCi). The primary endpoint was progression-free survival at 12 months among patients receiving RAI. A sample size of 60 was planned, but the trial was closed early due to slow enrollment, with only 28 patients evaluable. Eleven (39.3%) were deemed to have sufficient 123I uptake for RAI treatment. In patients receiving RAI, the 12-month progression-free survival rate was 64.8%, which the authors considered promising since all participants had disease progression within 12 months at study entry.
Another small single-institution feasibility study investigating the BRAF inhibitor, dabrafenib, in RAIR BRAFV600E-mutant PTC followed. 1337 This study enrolled 10 patients with RAIR BRAFV600E-mutant PTC who were treated with the BRAF inhibitor, dabrafenib, for 4 weeks. In the last week, patients underwent a low-dose 131I WBS. Those patients with evidence of uptake continued dabrafenib for 2 weeks and received an empirical activity of 5.5 GBq (150 mCi). The primary endpoint was rate of new RAI uptake after treatment with dabrafenib. Six of the 10 patients demonstrated new RAI uptake and received RAI treatment. Of these, two patients met criteria for partial response by RECIST v1.1. Vemurafenib was investigated in a single-institution pilot trial of 12 patients with RAI-refractory BRAFV600E-mutant PTC. Two patients stopped treatment due to toxicity; 124I PET predicted absorption of at least 2000 cGy in at least one target lesion among four patients who were treated with RAI. At 6 months, two of these patients experienced partial response by RECIST v1.1. Beyond evaluating vemurafenib’s potential to increase RAI uptake in BRAFV600E mutant tumors, this study also studied mechanistic questions of redifferentiation. Three patients underwent paired pre- and on-vemurafenib biopsies on which RNAseq was performed and BRAF/RAS and thyroid differentiation scores (TDS) were determined. Paired biopsies confirmed pharmacologic reprogramming by inhibition of MAPK output that was accompanied by increasing BRAF/RAS TDS scores. 1338
A single-institution retrospective series of 13 patients with RAIR DTC treated with targeted therapy provides further support for the potential for MAPK blockade to reverse refractoriness to RAI in patients with BRAF- and RAS-mutated DTC. Thirteen patients were treated with either selected BRAF or MEK inhibitors. Nine patients were treated with RAI, three of whom achieved a partial response. 1339 The first multicenter study examining redifferentiation in metastatic disease completed to date is MERAIODE: A Redifferentiation Phase II Trial with Dabrafenib and Trametinib Followed by Radioactive Iodine in BRAFV600E mutation-positive RAIR DTC. 1340 This study enrolled 24 patients who received dabrafenib plus trametinib and underwent diagnostic WBS on day 28. After 35 days, patients received an empirical rhTSH-stimulated administration of 5.5 GBq (150 mCi). The primary endpoint was the objective response rate by RECIST v1.1 at 6 months. It was 38%. The biochemical response rate in patients without TgAb, defined as a suppressed Tg decrease of 50% or more, was 47%. Most adverse events were grade 1 or 2, and no grade 4 or 5 adverse events were seen. MERAIODE enrolled a second cohort of patients with 11N/H/K RAS-mutated RAIR DTC who were treated with trametinib alone followed by an rhTSH-stimulated empirical administration of 5.5 GBq (150 mCi). 1340 Two of the 10 patients evaluable for response at 6 months derived a partial response by RECIST v1.1 criteria.
The mechanisms of resistance to redifferentiation with MAPK inhibition are not fully understood; preclinical models investigating monomeric BRAF inhibition in BRAFV600E mutation-positive DTC have shown a potential role for up-regulation of epidermal growth factor receptor 3 (ErbB3) expression and MAPK and PI3K/Akt pathway reactivation. 1341 This finding led to a small single-institution exploratory study of vemurafenib plus the anti-ErbB3 monoclonal antibody, CDX-3379, for redifferentiation in BRAFV600E mutation-positive RAIR DTC. Seven patients were enrolled. Of the six patients evaluable for RECIST v1.1 response, two experienced a partial response at 6 months. The authors concluded that further evaluation of BRAF-directed therapy with ErbB3 inhibition for redifferentiation is warranted.
While redifferentiation studies thus far have focused mainly on BRAF- and RAS-specific inhibition, case reports have detailed the potential for TRK- and RET-targeted therapies to promote redifferentiation in NTRK and RET fusion-positive RAIR DTC.1342–1344 The rarity of NTRK fusion-positive PTC poses a challenge to execute conventional clinical trials to investigate TRK inhibition for redifferentiation; however, study of RET inhibition for redifferentiation of RAIR RET fusion-positive PTC is now underway (NCT05668962). Currently, redifferentiation therapy is only considered for individuals with tumors harboring BRAF or RAS-mutations.
The potential ability of a MEK inhibitor alone to enhance RAI uptake during initial therapy in patients with high-risk DTC has been studied in a randomized prospective study, ASTRA trial. 778 This was an international multicenter phase III placebo-controlled, double-blind trial that randomized 233 patients with post-thyroidectomy high-risk DTC to receive selumetinib or placebo (in a 2:1 ratio) for 5 weeks. On treatment days 29–31, rhTSH-stimulated 131I (100 mCi/3.7 GBq) was administered, followed by 5 days of selumetinib or placebo. The primary endpoint was complete response rate at 18 months. Post-thyroidectomy high-risk DTC was defined by demonstrating at least one of the following pathological features: primary tumor >4 cm, gross extrathyroidal extension (T4 disease), and at least one metastatic lymph node ≥1 cm or involvement of ≥5 lymph nodes (any size). ASTRA was not an up-front gene-selected trial. Excellent response was determined at 18 months in three consecutive stages: stage I, serum Tg <1 ng/mL without TSH stimulation and neck ultrasound showing no structural disease; stage II, following rhTSH stimulation, serum Tg level <1 ng/mL and no evidence of thyroid cancer on diagnostic WBS; and stage III, no evidence of thyroid cancer by cross-sectional imaging. No statistically significant difference in complete response rate 18 months after RAI was observed (selumetinib n = 62 [40%]; placebo = 5 30 [38%]; OR 1.07 [CI 0.61–1.87]; p = 0.8205). Thus, while not supporting use of MEK inhibitor redifferentiation in a non-genotype-selected but high-risk population, ASTRA has established benchmarks, including a well-thought-out definition of complete response to adjuvant RAI for use in future studies. 778
Despite promising results with improved RAI uptake and tumor response in some contexts, more studies are needed to define the clinical benefit of redifferentiation, potential side effects, and populations appropriate for redifferentiation-directed therapy.
What is the role of cytotoxic chemotherapy in RAIR DTC?
▪
Cytotoxic chemotherapy can be considered in patients with RAIR DTC with metastatic, rapidly progressive, symptomatic, and/or imminently threatening disease not amenable to control through other approaches. Use within the context of a therapeutic clinical trial is preferred.
Although doxorubicin was approved for use in thyroid cancer by the FDA in 1974 and has some utility in ATC, historically, cytotoxic chemotherapy has produced disappointing results when used to treat RAIR DTC. 1345 Cytotoxic chemotherapy, however, may have selective benefit in patients unresponsive to kinase inhibitors. 1346 Data are limited and primarily anecdotal.
What is the optimal approach for patients with oligometastatic RAIR DTC?
▪
For patients with RAIR DTC with solitary or oligometastases (two to five lesions), focal ablative treatment may be considered. Optimal treatment approaches may be best addressed in a multidisciplinary setting.
Surgery, RFA, and PEI are also addressed for patients with locally residual or recurrent DTC in
Oligometastatic disease has been variably defined in the literature. Some define it as two to five metastatic deposits that may be limited to one to two organs, whereas others have proposed more dynamic models incorporating lesions emerging either synchronously or metachronously, and including progressive disease.1354–1358 Traditionally, local treatment for any burden of metastatic disease was considered palliative. However, clinical data supporting a role for aggressive local treatment in improving progression-free and overall survival, deepening response to systemic therapy, and salvaging patients developing solitary/oligo-progressive disease in the course of systemic therapy have emerged.1356,1358–1361 Data elaborated specifically in thyroid cancer are limited; treatment of oligometastatic RAIR DTC has been described primarily in case reports and small series.1362–1367 Because many RAIR DTCs grow slowly, local treatment for oligometastatic disease has the potential to offer significant clinical benefit, which may be difficult to discern.
While no randomized prospective controlled trial has been conducted to evaluate the role of metastectomy in oligometastatic RAIR DTC, several analyses of pulmonary metastectomy demonstrate the potential for a survival benefit with surgery.1366,1367 A single-center retrospective review included 43 patients with RAIR DTC submitted to pulmonary metastectomy; for those who underwent a complete (R0) resection, disease-specific survival at 5 and 10 years was 100% and 77%, respectively. A similarly long survival rate was seen in a SEER registry analysis of patients with thyroid cancer with lung metastasis who underwent resection. 1367 In this analysis, survival benefit was also seen in patients with bone metastasis who underwent resection. Metastectomy in patients with solitary bone metastasis also appears to be associated with excellent long-term overall survival. 1368
SBRT, also termed stereotactic ablative radiotherapy (SABR), is a radiation technique that delivers high doses of radiation to small tumor targets using highly conformal techniques. SABR has been used to treat cancer deposits in the lungs, brain, liver, adrenal glands, and bones, and it has been studied in NSCLC, prostate, breast and colorectal cancers. 1354 One international multicenter phase II trial, SABR-COMET, enrolled patients with multiple solid tumor types.1356,1369 SABR-COMET randomized 99 patients with one to five oligometastases to receive SABR to all metastases versus standard palliative radiotherapy administered for symptom relief or to prevent an impending complication. Median overall survival in the SABR-treated group was 50 months, compared with 28 months in the control arm (stratified log-rank test p = 0.006; HR, 0.47 [CI 0.27–0.81]). While the rate of ≥grade 2 adverse events was higher in the SABR arm, there was no difference in patient-reported QoL. 1370 Phase III trials are now underway, including SABR-COMET-3 (ClinicalTrials.gov identifier: NCT03862911), SABR-COMET-10 (ClinicalTrials.gov identifier: NCT03721341), and the CORE trial (ClinicalTrials.gov identifier: NCT02759783). Enrollment of patients with thyroid cancer into these studies is to be advised.
Thermal ablative techniques, such as RFA, cryoablation, and microwave ablation, have become common treatments for lung metastases and other metastatic sites in various solid tumors.1371,1372 Randomized trials of thermal ablation in RAI-refractory DTC have not been conducted, but a retrospective review of patients with lung metastasis treated across the TUTHYREF network has been reported. 1373 RFA was employed most frequently, followed by cryoablation and then microwave ablation. While most patients had treatment of multiple metastases, one patient with a solitary lung metastasis remained disease-free at last follow-up. Overall survival for all 47 patients treated was 79% [CI 66–91] at 3 years. 1373 Treatment with thermal ablation, whether by cryoablation or RFA, in patients with solitary/oligometastatic bone metastasis has also been shown to yield excellent disease control, especially for lesions 2 cm or smaller.1374,1375
When solitary/oligo-progressive disease emerges during kinase inhibitor therapy, an ablative treatment approach may be considered if the site is amenable. To date, thyroid cancer-specific data are limited, but a single-center retrospective series of patients with ALK/ROS1/RET-rearranged NSCLC with solitary/oligo-progressive disease on TKI therapy treated with radiation, surgery, or percutaneous thermal ablation has been reported. 1361 TKIs were held during local therapy in many, but not all cases, and then resumed after ablative therapy was completed. The authors concluded that this approach facilitated clinically meaningful extension of TKI therapy beyond the initial date of disease progression.
What is the optimal treatment approach for patients with site-specific symptomatic RAIR DTC?
▪
For patients with symptomatic RAIR DTC, local treatment is suggested. Surgery, radiotherapy, and percutaneous thermo-ablative approaches are available to treat individual symptomatic sites of disease.
Patients with symptomatic unresectable and/or metastatic RAIR DTC are optimally reviewed in a multidisciplinary setting. Treatment decision-making should be individualized and consider the overall disease burden, pace of disease progression, symptoms or impending symptoms, and potential anatomical complications. In many cases, treatment goals are palliative. Local therapies, including surgery, cementoplasty/vertebroplasty, radiotherapy or thermal ablation, should be considered for symptomatic or anatomically threatening lesions (such as for the prevention or palliation of airway or aerodigestive tract obstruction or hemorrhage; symptomatic mediastinal, hilar, or lung lesions; and symptomatic bone lesions). 1359 The site of metastases, extent of disease, presence of symptoms or impending functional impact of the metastasis, and the role of RAI should be considered when making treatment decisions.
While prospective controlled trials are lacking, palliative radiotherapy is well tolerated and effective at producing durable local control in many cases. SBRT is generally the preferred modality for lung lesions and may be used for disease locations. One single-institution retrospective series reported outcomes of 53 patients with various thyroid cancer diagnoses treated using palliative radiotherapy. 1376 In this series, 21 patients received SBRT for lung metastases, and 34 patients were treated for bone metastases. In the lung metastases group, median local control of the treated lesion(s) was 187 months, and median progression-free survival and overall-survival were, respectively, 16 and 245 months. In the bone metastases group, median local control of the treated lesion(s) was 98 months, and median progression-free survival and overall-survival were, respectively, 24 and 50 months. Radiotherapy was well tolerated, without significant adverse events. The impact of treatment on symptoms, such as cough, dyspnea, hemoptysis, or pain, was not reported. A second small single-institution retrospective series similarly reported disease control from palliative radiotherapy in DTC. 1377 This group also noted control of symptoms related to the treatment lesions.
Bone metastases in DTC are typically osteolytic and highly destructive to bone structural integrity and cause frequent skeletal-related events (including pathological fracture, spinal cord compression, and pain), impairing QoL and survival.1378,1379 Bone metastases are seen in a higher percentage of patients with FTC, OTC, and PDTC than in patients with PTC.1380,1381 Mutational analysis in a single-institution study revealed TERT promoter mutations in 72% of cases, RAS mutations in 40%, and BRAFV600E mutations in 20%. Median overall survival can be quite long for patients with a solitary bone metastasis, whereas expected overall survival with multisite disease is less than 10 years.1135,1368,1372,1382,1383 Multivariable analysis identified RAI-avidity and treatment with radiotherapy as significant predictors of improved survival.
Symptomatic vertebral metastases are best approached by a multidisciplinary team. Indications for palliative surgery include vertebral metastases associated with spinal cord compression or impending compression and risk of fracture in weight-bearing long-bone metastases.1368,1379,1380 Postoperative radiotherapy is typically administered to reduce the risk of local recurrence. Cementoplasty is a palliative approach involving CT-guided percutaneous injection of poly-methyl methacrylate cement into an osteolytic lesion. The goal of cementoplasty is to fill the defect in order to enhance mechanical stability of the bone and rapidly reduce pain. Cementoplasty may be used alone or in combination with other local treatment such as surgery or external radiation therapy. Cementoplasty may be complicated by cement leakage, although such episodes are usually not clinically significant.1359,1372,1380
Other percutaneous approaches (e.g., RFA, cryotherapy, and microwave ablation) are alternatives to radiotherapy for symptomatic metastases. These techniques can be particularly helpful to salvage sites of disease after progression following prior radiotherapy and for patients who are poor candidates for surgery. Several retrospective series examining the rate of local control of treated lesions, especially lung and bone metastases, and patient survival have been published, but data examining patient-reported outcomes, such as symptom control, are scarce.1372,1373,1384 RFA is more commonly used in treating lung, bone, and liver metastases, although some consider cryoablation preferable for treating bone metastases, because it is associated with less post-procedural pain compared with RFA and avoids electrical conduction. 1359 Advantages of RFA include its minimally invasive nature, repeatability, and low morbidity. RFA has limitations: it should not be used for lesions >3 cm or for lesions in proximity to large blood vessels (which promote heat loss, thus reducing efficacy) or to the pleura (which raises the risk of pneumothorax).
Cryoablation is another local treatment involving percutaneous insertion of one or more probes into the tumor. 1359 Freezing is achieved by circulation of argon under pressure, causing the destruction of cell membranes and denaturation of proteins, leading to cell death. One anatomical advantage of cryoablation is the ability to visualize the zone of freezing. In addition, risk to some anatomical obstacles such as neural tissue can be minimized by temperature control or by using carbon dioxide or saline injection to move structures out of the way. Morbidity is generally limited, and larger tumor volumes can be addressed by the insertion of more than one probe. One drawback is the high cost of the needles and the rare gas.
Microwave ablation, like RFA, uses electromagnetic current to increase intra-tumoral temperature based on micromovement of water molecules.1359,1385 Heating is faster and can achieve higher temperatures than RFA. Theoretical advantages include the possibility of treating lesions >3 cm and avoiding heat loss by thermal convection from adjacent large vessels. Microwave ablation has been studied most extensively in liver metastases, particularly among patients with colorectal carcinoma, but data are emerging with microwave ablation in other metastatic settings, include bone for metastasis.1386–1389
When should bone-directed agents be considered for patients with DTC?
▪
In patients with RAIR DTC with symptomatic and/or multiple bone metastases, treatment with a bone modifying agent is recommended to decrease the risk of skeletal-related events. A bone-modifying agent dosing schedule of every 3 months may be considered due to a reduction in the risk of adverse events, especially osteonecrosis of the jaw, compared with monthly dosing, but may increase the risk of symptomatic skeletal events.
Bone metastases in advanced RAIR DTC are common and are a poor prognostic factor.765,1347 Skeletal-related events, such as spinal cord compression, pathological fracture, need for external beam radiation therapy and/or surgery, and hypercalcemia, are a major cause of morbidity and can cause pain, impaired mobility, and financial burden. Bisphosphonates, particularly zoledronic acid, and the RANKL inhibitor, denosumab, have been studied extensively in patients with solid tumor with bone metastases, but large-scale clinical trials have not been carried out in DTC. One small single-institutional experience studying patients with DTC/bone metastases has been reported. 1137 Patients with thyroid cancer have been enrolled in several randomized controlled trials investigating zoledronic acid.1349–1351 Most data in solid tumors are in patients with castration-resistant prostate cancer, breast cancer, and NSCLC.
Randomized controlled trials in patients with bone metastases from solid tumors have shown consistently that bisphosphonates (e.g., zoledronic acid) reduce the incidence of skeletal-related events, and zoledronic acid is the most effective agent. Common adverse events include nephrotoxicity, acute phase reactions, and hypocalcemia. Less common ones include osteonecrosis of the jaw and atypical femur fractures. In addition, zoledronic acid must be dose-reduced based on renal function and is contraindicated for individuals with a GFR <30 mL/mL due to risks of acute nephrotoxicity.
The RANKL-targeted monoclonal antibody, denosumab, has been studied to prevent skeletal-related events in a range of solid tumors, including breast, prostate cancer, and lung cancers. Noninferiority randomized controlled trials have compared denosumab with zoledronic acid.1352,1353 In addition, several pooled analyses have been conducted.1351,1354 These suggest that denosumab delays time to skeletal-related events and worsening of pain more effectively than does zoledronic acid, but there were no differences in overall survival or disease progression between the two agents. Denosumab has an adverse event profile like that of zoledronic acid overall, including osteonecrosis of the jaw and risk of atypical fractures. Denosumab causes more frequent serious hypocalcemia compared with zoledronic acid but is less nephrotoxic. Additional benefits with denosumab include the convenience of subcutaneous administration (as compared with intravenous administration for zoledronic acid) and reduced need for renal function monitoring. Hypocalcemia is more common in patients with renal failure treated with denosumab.
Cost-effectiveness of denosumab compared with zoledronic acid has been studied. 1355 While the direct cost of denosumab is higher than that of zoledronic acid, this was offset by reduced costs related to bone complications. Quality-adjusted life-year and net monetary benefit analyses favored denosumab from the perspectives of society and payers. Extending the dosing interval from 4 to 12 weeks for zoledronic acid and denosumab, especially to decrease the risk of osteonecrosis of the jaw, has been explored in noninferiority trials.1356–1359 Overall, most data support the 12-week schedule, although concern has been raised regarding a potential risk of increased symptomatic skeletal events with the 12-week dosing schedule that might not be definitively detected in a noninferiority trial. 1360 A head-to-head study, the REDUSE trial comparing every 4-week to every 12-week dosing of denosumab for patients with bone metastases with a primary endpoint of serious skeletal events, is underway (NCT02051218).
Bone-directed agents often are administered for several years in patients with bone metastases, though randomized controlled trials generally have evaluated treatment durations of 1–2 years. A recent systematic review of studies evaluating bone-directed therapies beyond 2 years suggests that the incidence of osteonecrosis of the jaw increases after 2 years, while the rates of clinically significant hypocalcemia and nephrotoxicity were low, and atypical femoral fractures were rare. 1361 However, most data were retrospective and limited to subgroup analyses.
What is the best treatment for patients with brain metastases?
▪
Resection and/or SBRT are the mainstays of therapy for central nervous system metastases. RAI can be considered if central nervous system metastases concentrate RAI. If RAI is planned, SBRT and concomitant glucocorticoid therapy are recommended prior to RAI therapy to minimize the effects of a potential TSH induced increase in tumor size and RAI induced inflammatory response.
Brain metastases typically occur in older patients with more advanced disease and are associated with a poor prognosis. 1390 Surgical resection and SBRT are the mainstays of therapy.1390–1392 There are few data showing efficacy of RAI. For patients with few (one to three) brain metastases, SBRT is as effective as surgery and can be repeated in case of the appearance of new brain lesions. It is usually well tolerated, and brain necrosis that occurs in less than 10% of cases is usually limited and without clinical consequences; thus, patient outcome depends mostly on the progression rate of extracerebral lesions.1393,1394
Stereotactic radiation therapy is preferred to whole brain irradiation because life expectancy in patients with brain metastases may be prolonged, and stereotactic irradiation induces less short- and long-term toxicity compared with whole brain irradiation (fatigue, headache, cognitive decline, and behavioral changes). It may be effective even in patients with multiple brain lesions.
Who should be considered for clinical trials?
▪
Patients should be counseled to consider enrolling in prospective clinical trials based upon specific eligibility requirements for given studies and the likelihood that the patient will benefit from participation. Clinicians considering referral of patients for trials should review available treatment options and eligibility criteria, preferably through discussions with personnel at the trial center and review of materials at the website www.clinicaltrials.gov. (
A therapeutic clinical trial is a systematic investigation of the effectiveness and safety of a new, modified, or combination of treatments, potentially including medications, surgery, radiation therapy, and/or other novel or revised approaches. A broad variety of such trials may be ongoing, and they can generally be identified through online databases such as www.clinicaltrials.gov. Referral recommendations are informed through direct contact with the institutions conducting studies of particular interest to assure trial availability and patient eligibility. Enrollment into clinical trials is associated with lower overall cancer-specific mortality for patients with common cancers, even within contexts in which approved, and “standard of care” therapies already exist. 1395 The reasons for this association are unclear, but there is no evidence to suggest that trial participation is deleterious to patients, and it may be beneficial.
Participation in a clinical trial should be considered in any situation where there is no effective standard of care, or when a standard of care is being compared with a promising new or investigational approach. Adjuvant therapy trials may be appropriate for patients at high risk of recurrence following primary treatment who wish to pursue aggressive therapy. For patients with RAIR DTC that is locally advanced or metastatic, clinical trials are appropriate in the setting of disease that is considered progressive by RECIST criteria. This is particularly true if progression occurred after use of an approved therapy.
Considerations managing pregnant patients with DTC
▪
In most pregnant patients, surgery can be safely delayed until after delivery. Exceptions include rare patients for whom there is concern for significant disease progression. If necessary, surgery may be performed in the second trimester of pregnancy. For pregnant patients diagnosed with DTC during pregnancy, monitoring with neck ultrasound at least once in early second trimester and more often if clinically indicated is appropriate. Cross-sectional imaging using MRI may be performed in selected cases. Imaging modalities that require ionizing radiation should not be performed other than in exceptional circumstances. ( TSH goals for pregnant patients, in general, are the same TSH as determined preconception. Thyroxine dose may be adjusted toward less TSH suppression if there are concerns that excess thyroxine may have an adverse impact on the pregnancy. TSH should be monitored approximately every 4 weeks until 16–20 weeks of gestation and at least once between 26 and 32 weeks of gestation. Monitoring using neck ultrasound and Tg is appropriate for pregnant patients who have an incomplete response to therapy. If cross-sectional imaging is needed, MRI should be performed. Pregnant patients in excellent or indeterminate response categories should be monitored as for nonpregnant patients.
The potential adverse impact of thyroid cancer treatments on pregnancy and fertility, as well as the impact of pregnancy on the onset and progression of DTC, has been the focus of several studies.885,898,1396–1406 Human chorionic gonadotropin (hCG), elevated throughout pregnancy, stimulates the luteinizing hormone/hCG receptor but also is a weak stimulator of the TSH receptor, which is responsible for the increased level of free thyroxine and reduced TSH seen in the first trimester of normal pregnancy. 1396 This endogenous stimulation of the TSH receptor during pregnancy could potentially result in stimulation of the growth of thyroid cancer in pregnancy and drive earlier treatment.
Several studies have examined the impact of pregnancy on the onset and progression of DTC. In women with treated DTC, pregnancy has not been associated with an increased level of progression or recurrence. In a retrospective study of 235 women with DTC with term pregnancies after initial treatment for DTC (1997–2015), structural disease recurrence or progression was seen in only 5% of patients (11/235) when they were evaluated 3–12 months after delivery. 1397 Among the women with no evidence of structural disease before pregnancy, none progressed; among those with structural disease, 29% progressed (11/35), but therapy in the first year was only required in 8% (3/35). A retrospective analysis was performed of 19 women with PTC (most with T1aPTC [68%]) who were diagnosed immediately before or in the early stages of pregnancy and who delayed surgery until after delivery. 1398 Serial neck ultrasounds did not demonstrate clinically significant progression of their tumors. Most women (16/19) underwent elective surgery at a median of 12 months after diagnosis. The predominance of small initial tumors may not make these findings generalizable to women with more advanced DTC.
In a study of 124 women with DTC and lung metastases, outcomes were compared between those who became pregnant (N = 37) and those who did not (N = 87). 1399 There was no difference in the 5- and 10-year progression-free survival in these groups, indicating that even in women with lung metastases, pregnancy was not associated with worse outcomes. A study designed to determine if pregnancy influences thyroid cancer stage and outcome utilized the California tumor registry and identified women with thyroid cancer and a pregnancy 5 years prior to, or 9 months after, the diagnosis. Tumor histopathology, stage, and status at last follow-up and 5-year disease-specific survival were evaluated. No differences in any of the outcomes were identified in 301 recently pregnant women versus 903 matched nonpregnant women. A meta-analysis of 10 studies of women with previously treated DTC who became pregnant showed no overall difference in the risk of recurrence associated with pregnancy, including in two studies of patients with distant metastases. 1400 A propensity score-matched retrospective cohort study of women in China with DTC who became pregnant showed that there was no impact of pregnancy on progression-free survival. 1401
Numerous studies have examined the impact of thyroid cancer treatment on obstetrical complications and outcomes. In a retrospective observational study examining women in South Korea, 7232 women with a diagnosis of thyroid cancer had similar obstetrical complications and outcomes in comparison to a control group of women without thyroid cancer. 1402 The only obstetrical complication that was increased in women with thyroid cancer was postpartum hemorrhage (OR 1.23 [CI 1.15–1.32]). Another retrospective study using data from a large U.S. database (US HCUP-NIS) of women delivering between 1999 and 2014 found no significant differences in obstetrical complications or outcomes in women with thyroid cancer, except for an increase in blood transfusions and venous thrombosis. A retrospective cohort study in China of 154 women with thyroid cancer who had term pregnancies compared with matched controls found no overall difference in obstetrical complications or outcomes, except for an increased risk of invasive placentation. 1403
A long-standing recommendation after RAI therapy for hyperthyroidism or thyroid cancer has been to wait at least 6 months after therapy before becoming pregnant. Several observational studies have provided a basis for recommendations around the timing of pregnancy after 131I therapy. A large retrospective study from Korea, a population-based cohort, utilizing the Health Insurance Review and Assessment database identified 10,842 women with thyroid cancer who then became pregnant.
885
They assessed the impact of surgery or surgery and RAI on obstetrical complications and pregnancy outcomes. Overall, there was no increased incidence if pregnancy occurred greater than 6 months after RAI was given. When pregnancy occurred less than 6 months after RAI was administered, there was a small but significant increase in congenital malformations in the offspring, with an OR of 1.74 [CI 1.01–2.97]. A retrospective study of 212 singleton pregnancies in women with thyroid cancer compared with controls found a higher rate of late miscarriages, but this finding was not significant when adjusted for a higher rate of TPO antibody positivity.
1404
The women with thyroid cancer had greater gestational weight gain but no increase in gestational diabetes, and there was no impact on neonatal thyroid function. RAI therapy should not be administered in recently lactating patients (see
In pregnant women with a new diagnosis of thyroid cancer, or after detection of a recurrence, the impact of delaying thyroid cancer treatment until after delivery has been assessed. Several small retrospective studies have followed pregnant women with thyroid cancer who delayed surgery until after delivery to determine the influence of pregnancy on tumor progression. A study of 19 women with PTC were followed through pregnancy using serial neck ultrasounds. An increase in tumor volume was observed in 26% of women, but there were no clinically relevant changes, and 16/19 underwent elective surgery at a median time of 12 months post-delivery. 1398 An international cohort study highlighted that thyroid cancer constitutes ∼6–10% of cancer diagnoses during pregnancy; in this population, 29/35 (83%) underwent surgery during pregnancy. 1405 Most tumors (57%) were <2 cm in diameter, and lymph nodes were present in 26%. There were no adverse obstetrical or neonatal complications. These studies indicate that in most pregnant women with newly diagnosed DTC or recurrence of their DTC, there is rarely significant progression, and it is safe to defer surgery until after delivery. If there is a decision to move forward with surgery during pregnancy, this appears to be safe. In general, it is recommended in the second trimester.
Thyroxine dose requirements increase in most pregnant women with hypothyroid, especially those who are athyreotic. 898 A concern has been raised whether the higher thyroxine doses of pregnant women with thyroid cancer may impact obstetrical complications. According to a retrospective cohort study of women with thyroid cancer on thyroxine up to 2 years before pregnancy, a TSH <0.10 was associated with an increase in preterm delivery compared with control, with an OR of 2.14 [CI 1.51–2.78]. 1406 Although data are limited, women with DTC and a TSH level in the reference range did not have increased obstetrical complications.
Cancer survivorship
According to the National Cancer Institute of the National Institutes of Health, an individual is considered a cancer survivor from the time of diagnosis, through life. 1407 Cancer survivors can include those free of disease and living beyond cancer treatment, individuals free of cancer experiencing the sequelae of treatment, as well as those living with active tumor. Untoward consequences associated with their diagnosis of cancer are not limited to those with living with side effects of treatment or with uncontrolled cancer. Several aspects affect QoL among thyroid cancer survivors. We focus on those related to a thyroid cancer diagnosis per se; management of hypothyroidism is discussed in other ATA guidelines.
What are long-term survivorship concerns related to initial thyroid cancer therapy?
▪
Patients should be made aware of potential long-term side effects of treatments and monitored with appropriate intervention and/or referrals during follow-up.
Shared decision-making between the patient and the treating clinical team is essential and is particularly important prior to initiating a treatment plan, including active surveillance. Because complications can impact QoL even after a thyroid cancer is in complete remission or during years of stability, the potential for impact on long-term QoL should be discussed and carefully weighed prior to initiating therapy. Potential long-term complications of RAI and those of non-RAI medical therapies are discussed in detail in their individual recommendations. Potential long-term consequences of thyroid cancer surgery include the following.
Hoarseness/voice change
Thyroidectomy with or without central neck dissection involves manipulation of the larynx for intubation to allow for general anesthesia and relevant nerves and muscles that may alter the voice on a temporary or permanent basis. Postsurgical voice change is very common for these reasons, even when relevant nerves such as the recurrent laryngeal nerve and external branch of the superior laryngeal nerve are preserved and deemed to be functional by laryngeal exam. Voice change has been reported in over 30% of patients in the long term, even without nerve injury. 1408 Vocal fold paralysis may occur from nerve injury during surgery. The incidence of vocal fold paralysis after thyroid surgery is variable and may be related to surgeon volume/experience with thyroid surgery. Dhillon et al. 1409 reported a 2.9% incidence of temporary and 0.2% permanent vocal fold paralysis in nerves that could be preserved in a single high-volume thyroid surgeon’s hands. When a patient has a voice change that impacts QoL, referral should be made to a laryngologist who works in tandem with a speech language pathologist to help the patient achieve the best voice possible. 583 In some cases, patients also may experience aspiration, which also can be managed by this team. Bilateral injury to the recurrent laryngeal nerves may result in dyspnea and the need for a tracheostomy. Every effort should be made to avoid this challenging situation by avoiding a total thyroidectomy when the initial thyroid lobe removal results in a known recurrent laryngeal nerve injury.
Hypoparathyroidism
The parathyroid glands may be injured or inadvertently removed during thyroid surgery. The risk of hypoparathyroidism varies with surgeon experience. The rate of temporary hypoparathyroidism has been reported to be 14 − 43%, and the rate of permanent hypoparathyroidism estimated to be 1 − 25%. 1410 Those patients who are not adequately supported with calcium and vitamin D supplements may experience paresthesias in their extremities and in severe cases tetany or cardiac arrhythmia. Even when adequately supplemented, Bergenfelz et al. have reported that patients experiencing permanent hypoparathyroidism after total thyroidectomy for benign disease are at an increased risk for renal insufficiency and a cardiovascular event if they had known cardiovascular disease at the time of thyroidectomy. 1411 Also, compared with patients without permanent hypoparathyroidism, the risk of death was significantly higher among patients with permanent hypoparathyroidism. 1412 Preservation of viable parathyroid glands during thyroid surgery is of critical importance.
Scar/cosmesis
The cervical scar that results from thyroid surgery is a result of multiple factors that are both surgical technique and patient-related. Many studies have reported that the appearance of the cervical scar after thyroid surgery has a significant QoL impact on patients, especially within the first few years after surgery.584,585 Management of the scar and lessening its impact should be a focus for the thyroid surgeon. There are also remote access surgical options available for carefully selected patients that will avoid a neck scar.
Neck tightness and dysphagia
Many patients experience a “tight neck” from scarring and fibrosis that can occur after thyroid surgery (“post-thyroidectomy central compartment syndrome”). If it occurs, this is most noticeable in the first 3 months post-op but may persist longer. This tightness may also result in a globus sensation or dysphagia which mostly reverts back to the preoperative baseline by 2–3 months. 586 Massage and neck range of motion exercises in the immediate postoperative period may help to minimize this effect. 587
How should financial hardship caused by thyroid cancer be addressed?
▪
Patients should be informed that resources exist for patients and families impacted by financial burden due to a diagnosis of thyroid cancer. Clinicians should know that many patients diagnosed with thyroid cancer experience financial burden engendered by the costs of cancer diagnosis, treatment, and monitoring. Clinicians should discuss these topics with patients and their families.
The substantial cost of thyroid cancer care can place a burden on thyroid cancer survivors and their families. Patients diagnosed with thyroid cancer are at risk for financial hardship (i.e., financial toxicity).1413–1415 A study evaluating bankruptcy in Washington State found that patients diagnosed with thyroid cancer are 3.46 times more likely to file for bankruptcy than people without cancer (the second largest difference when compared with other cancer types). 1416 In addition, compared with individuals without cancer, thyroid cancer survivors experience higher unemployment 2 years after diagnosis and lower income at 2 and 4 years after diagnosis. 1417 In one study from the Netherlands, older age, greater fatigue, and lower education were associated with unemployment. 1418 Medical costs can lead to differing financial burdens based on factors such as patient age, socioeconomic status, and race/ethnicity. Prior studies have found that Black and Hispanic patients with thyroid cancer are at elevated risk for food insecurity. 1419 In the United States, younger patient age is commonly associated with more cancer-related financial hardship, likely because older patients have access to Medicare. In contrast, among low-acculturated Hispanic women as compared with high-acculturated Hispanic women, financial hardship has been seen across all age groups. 1420 Financial hardship contributes to poor QoL. In a study of 1743 adult thyroid cancer survivors in the United States, financial difficulties were associated with increased anxiety and depression. 1415 Clinicians should be aware that some patients diagnosed with thyroid cancer suffer financial hardships due to the costs of cancer diagnosis, treatment, and monitoring. Clinicians should employ approaches to testing, treatment, and monitoring that are most cost effective for a patient and reduce the financial barriers to care. 1421 Patient education should address financial services, social work, and when available, care coordinators.
What are the critical psychosocial concerns of thyroid cancer survivors?
▪
Thyroid cancer survivors should be informed that services are available to support psychosocial needs related to having a cancer diagnosis. Clinicians treating patients diagnosed with thyroid cancer should be prepared to help patients manage the psychosocial implications of thyroid cancer diagnosis and management.
Thyroid cancer survivors may have long-term and underaddressed psychosocial concerns, including worse QoL, distress, and cancer-related worry. Although there has been some variability in findings and measures used, several reports show that irrespective of prognosis, many patients with thyroid cancer report worse QoL.468,1422–1424 One study found that self-reported QoL among thyroid cancer survivors is similar or worse than the QoL of survivors with other cancer types. 1425 Patients with thyroid cancer diagnosed at a younger age, with comorbidities, with preexisting depression, who overestimate mortality risk, who have a fear of recurrence, who have persistent disease, and who have side effects or complications from their thyroid cancer treatment are more likely to report worse QoL.941,1426–1435 One study suggested that cancer-related fatigue is associated with both worse QoL and distress. 1436 Another study found that with thyroid cancer, younger patient age, more comorbidities, history of depression, and report of thyroid hormone suppression correlated with moderate to severe post-treatment fatigue. 1437 A recent systematic review suggested that QoL was better in patients undergoing hemithyroidectomy versus total thyroidectomy when measured shortly after the procedure (less than 6 months), but long-term data were less certain, and prospective data are limited. 1438 There are mixed findings surrounding whether more intensive treatment adversely impacts QoL.396,398,1439,1440
One important consideration of measures of QoL has been the need for their validation in patients with thyroid cancer. Recently, the EORTC QoL group has developed and validated a QoL tool for patients with thyroid cancer (EORTC QLQ-THY34), including in a recent phase IV study.1441,1442 Use of this validated scale has the potential to provide important insights to inform better understanding of the their psychosocial well-being.
Distress related to a thyroid cancer diagnosis can remain high for many years after diagnosis.1443,1444 Studies have found that cancer-related worry is prevalent among thyroid cancer survivors; for a substantial proportion of patients, it can become long-standing.990,1443,1445 A study in 941 Canadian cancer survivors found that cancer-related worry was greatest in younger cancer survivors and in patients with confirmed or suspected residual disease. 1443 However, even in 2215 disease-free patients 2–4 years post-diagnosis, there were concerns about death (41%), harms from treatment (44%), impaired QoL (55%), family at risk (58%), and cancer recurrence (63%). Female patients, younger patients, those with a lower education, and racial/ethnic minorities are more likely to report cancer-related worry. 990 Studies suggest that patient worry can impact both clinician and patient treatment choices.1446–1448
Despite clinician awareness of high levels of worry, distress, and worse QoL among thyroid cancer survivors, many clinicians do not pursue management considerations beyond the clinician–patient clinic visit. Hence, many patients report unmet psychosocial support needs.1449–1453 In a survey of 2000 patients with thyroid cancer, just 9% reported receiving support addressing worry about recurrence, 12% counseling to manage distress, and 10% information about coping strategies. 1454 High-quality information resources should be offered to patients, including, but not limited to, details surrounding online support groups (e.g., ThyCa: Thyroid Cancer Survivors’ Association, Inc.), general information on cancer distress (e.g., the NCCN patient guidelines on cancer distress), thyroid cancer–specific information on cancer distress and coping (e.g., ASCO’s Thyroid Cancer: Coping with Treatment and the NCI’s Thyroid Cancer-Patient Version), as well as access to local resources, such as hospital social work and/or psychology services.1443,1455–1458
Authors’ Contributions
M.D.R.: Conceptualization, project administration and supervision, writing—original draft, writing—review and editing, and visualization. J.A.S.: Conceptualization, project administration and supervision, writing—original draft, writing—review and editing, and visualization. Z.B.: Writing—original draft, writing—review and editing, and visualization. L.B.: Writing—original draft, writing—review and editing, and visualization. G.B.: Writing—original draft, writing—review and editing, and visualization. G.A.B.: Writing—original draft, writing—review and editing, and visualization. P.L.B.: Writing—original draft, writing—review and editing, and visualization. R.C.: Methodology, data curation, validation, writing—original draft, writing—review and editing, and visualization. R.R.F.: Writing—original draft, writing—review and editing, and visualization. W.G.: Writing—original draft, writing—review and editing, and visualization. E.G.G.: Writing—original draft, writing—review and editing, and visualization. M.H.: Writing—original draft, writing—review and editing, and visualization. S.M.L.: Writing—original draft, writing—review and editing, and visualization. A.M.L.: Writing—original draft, writing—review and editing, and visualization. J.O.: Writing—original draft, writing—review and editing, and visualization. J.A.R.: Writing—original draft, writing—review and editing, and visualization. B.R.: Writing—original draft, writing—review and editing, and visualization. D.L.S.: Writing—original draft, writing—review and editing, and visualization. R.P.T.: Writing—original draft, writing—review and editing, and visualization. L.J.W.: Writing—original draft, writing—review and editing, and visualization.
Footnotes
Acknowledgments
The task force wishes to thank Ms. Amanda Perl, former Executive Director, American Thyroid Association; Ms. Pam Mechler, current Executive Director of American Thyroid Association; Ms. Kelly Hoff and Ms. Becky Schierman, Assistants to the task force, and Chandler Atchison, research librarian, for their constant help and support, as well as Ms. Vicki Wright for her assistance in article preparation. We would like to thank the members of the ATA Guidelines Steering Committee and the full ATA membership for their careful review and suggestions for the draft article that led to detailed consideration and modifications during final revisions prior to journal submission, as well as our patient advocate (G.B.) who served as a full voting member of the task force.
The following groups reviewed and endorsed the final document: the ATA BOD, American Association of Endocrine Surgeons, Asia Oceania Thyroid Association, American Head and Neck Society, Canadian Society of Otolaryngology-Head and Neck Surgery, China Thyroid Association, Endocrine Society, Endocrine Society of Australia, Guangzhou First People’s Hospital, International Association Endocrine Surgeons, International Federation of Head and Neck Oncologic Societies, International Thyroid Oncology Group, and Latin American Thyroid Society.
Author Disclosure Statement
These guidelines were funded by the American Thyroid Association without support from any commercial sources. MDR and JAS have no significant financial or competing interests to disclose.
DISCLOSURE STATEMENT
| First Name | Last Name | Disclosures Noted | Is this |
Mitigation Measures |
|---|---|---|---|---|
| Matthew | Ringel | None | N/A | |
| Julie Ann | Sosa | Research Support: Subcontract from MD Anderson Cancer Center funded by Exelixis and Eli Lilly for MTC registry. Consultant: Member and ATA representative, Data Monitoring Committee of the Medullary Thyroid Cancer Consortium Registry | No | |
| Zubair | Baloch | None | N/A | |
| Lindsay | Bischoff | None | N/A | |
| Gary | Bloom | Commercial Interest: Eli Lilly travel grant | Yes | Recusal from recommendation voting where COI is relevant. |
| Gregory | Brent | None | N/A | |
| Pamela Lyn | Brock | None | N/A | |
| Robert | Flavell | Commercial Interest: Co-Founder, Tiller Therapeutics. Value < $5000. Commercial Research Grants from Bristol-Myers-Squibb and Fibrogen | No | |
| Whitney | Goldner | Commercial interest: Roche: Site PI of multicenter study| Siemen's: Site PI of multicenter study. Does not get paid directly - research costs are paid to institution. | No | |
| Elizabeth | Gardner Grubbs | Research Support: Elizabeth Grubbs oversees institutional research funding from by Exelixis and Eli Lilly for MTC registry | No | |
| Megan | Haymart | None | N/A | |
| Steven | Larson | Commercial Interest: Commercial research grants from Y-mAbs Therapeutics, Inc., Genentech, Inc., WILEX AG, Telix Pharmaceuticals Limited, and Regeneron Pharmaceuticals, Inc.; Inventor of issued patents both currently unlicensed and licensed by MSK to Samus Therapeutics, Inc., Elucida Oncology, Inc., and Y-mAbs Therapeutics, Inc Serves or has served as a consultant both compensated and uncompensated to Cynvec LLC, Eli Lilly & Co., Prescient Therapeutics Limited, Advanced Innovative Partners, LLC, Gerson Lehrman Group, Progenics Pharmaceuticals, Inc., Exini, Inc., and Janssen Pharmaceuticals, Inc Holding ownership interest/equity in Elucida Oncology, Inc.; and holding stock in ImaginAb, Inc., and Y-mAbs Therapeutics |
Yes | Recusal from recommendation voting where COI is relevant. |
| Angela | Leung | None | No | |
| Joseph | Osborne | Consultant: Siemens Healthineer | No | |
| John | Ridge | None | N/A | |
| Bruce | Robinson | Consultant: Advisory Board for Eisai, Lilly and Exelixis | Yes | Recusal from recommendation voting where COI is relevant. |
| David | Steward | None | N/A | |
| Ralph | Tufano | Commercial Interest and Consultant: Medtronic Category C Commercial Interest and Consultant: Stryker Medical-(terminated 4/1/2023) Pulse Biosciences Category D Commercial Interest and Consultant: RGS Health Care Category B Commercial Interest and Consultant: RGS Health Care Category B |
Yes | Recusal from recommendation voting where COI is relevant. |
| Lori | Wirth | Consultant: Bayer Healthcare Consultant: Blueprint Medicines Consultant: Eli Lilly Research Support: Eli Lilly Consultant: Exelixis Consultant: Coherus Biosciences Consultant: Morphic Therapeutic terminated 12/2021) Consultant: EMD Serono Consultant: Illumina Consultant: Nested Therapeutics Consultant: PDS Biotechnology DSMC Member: PDS Biotechnology Research Support: Ellipses Consultant: Ellipses Research Support: Novartis Consultant: Novartis Consultant: Merck |
Yes | Recusal from recommendation voting where COI is relevant. |
Funding Information
These guidelines were funded by the ATA without support from any commercial sources.
Disclaimer
It is our goal in formulating these guidelines, and the ATA’s goal in providing support for the development of these guidelines, that they assist in the clinical care of patients and share what we believe is current, rational, and optimal medical practice. In some circumstances, it may be apparent that the level of care recommended may be best provided in limited centers with specific expertise. Finally, it is not the intent of these guidelines to replace individual decision-making, the wishes of the patient or family, or clinical judgment.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.