
Abstract
Background:
Mutations in the promoter region of TERT (TERTp) in thyroid nodules with indeterminate cytology are quoted to confer a high (∼80–95%) probability for thyroid carcinoma when detected on genomic classifier (GC) ThyroSeq. TERTp mutations may also occur in benign and low-risk thyroid neoplasms, and the risk of malignancy (ROM) in nodules harboring TERTp mutations without BRAFV600E is unknown. We analyzed the ROM and the surgical diagnosis in a retrospective cohort of thyroid nodules with TERTp treated at two academic medical centers.
Methods:
From 2323 patients with ThyroSeq GC performed on preoperative fine needle aspiration samples, 52 cases (2.3%) were identified harboring TERTp mutations without coexisting BRAFV600E .
Results:
The surgical diagnosis was obtained from resection (n = 51) or biopsy (n = 1, anaplastic thyroid carcinoma). The ROM was 65%. The reviewed diagnoses were benign/low-risk neoplasms in 18 (35%), carcinoma-American Thyroid Association (ATA) low/intermediate-risk in 14 (27%), and carcinoma-ATA high-risk in 20 (38.5%). All 18 benign or low-risk neoplasms had their tumor capsule submitted entirely, and 78% underwent total thyroidectomy. The molecular alterations were substratified into four groups: TERTp alone (n = 21, 40%), TERTp + RAS (n = 18, 35%), TERTp + other non-RAS mutation (n = 8, 15%), and TERTp + RAS + other alterations (n = 5, 10%), and the ROM for each group was 57%, 78%, 50%, and 80%, respectively. The frequency of a high-risk malignancy, which would often lead to a recommendation for total thyroidectomy, was 9.5%, 44.5%, 37.5%, and 80%, respectively. The frequency of high-risk carcinomas was significantly higher when a nodule harbored TERTp and other concomitant alterations (48%) compared with TERTp alone (9.5%; p = 0.006).
Conclusions:
Thirty five percent of TERTp nodules without BRAFV600E are benign/low-risk thyroid neoplasms, leading to their overtreatment. The incidence of high-risk carcinomas increases in TERTp-mutated nodules with the presence of additional mutations. If the indolent histology found in these lesions is confirmed at the behavior level, lobectomy may be sufficient for the initial management of TERTp thyroid nodules without BRAFV600E as long as there is no aggressive clinical or imaging feature. This will spare many patients from the side effects of total thyroidectomy.
Introduction
Telomeres are repetitive DNA sequences that cap the ends of chromosomes and protect them from damage. 1 Telomere shortening after successive cell divisions triggers cellular senescence. 2 Most malignancies achieve immortality by activating the normally silent human TERT gene (hTERT) that encodes telomerase reverse transcriptase (TERT), which maintains telomere length. 2 One mechanism of TERT activation is the presence of two highly recurrent mutations (C228T and C250T) in the promoter region of the hTERT gene. 1,2 TERT promoter (TERTp) mutations have been detected in thyroid carcinomas of follicular cell origin, especially in aggressive forms of the disease such as poorly differentiated and anaplastic thyroid carcinomas. 3,4 Moreover, many studies have shown that the presence of TERTp is associated with aggressive behavior in thyroid carcinomas. 5,6 This correlation with aggressive clinicopathological features has been well established in thyroid tumors with concomitant BRAFV600E and TERTp that are always malignant. 7
In the last decade, preoperative molecular analysis of fine needle aspiration (FNA) specimens has been extensively used and investigated in the United States. TERTp mutations in thyroid nodules with indeterminate cytology are thought to confer a high probability of thyroid carcinoma when detected on certain commercially available genomic classifiers (GCs). 8 For example, reports from the ThyroSeq assay version 3 indicate an 80% risk of carcinoma with isolated TERTp and >95% when TERTp co-occurs with a RAS mutation. Importantly, several publications, as well as the ThyroSeq marketing materials, suggest that the detection of TERTp in FNA samples should lead to more aggressive initial treatment, such as total thyroidectomy. 6,9 –13 However, TERTp mutations were reported in benign and low-risk thyroid neoplasms without BRAFV600E , and the risk of malignancy (ROM) in nodules harboring TERTp mutations without BRAFV600E is not well characterized. 14,15 In order to better stratify patients for initial therapy and avoid overtreatment (such as total thyroidectomy) and its side effects, it is necessary to have a comprehensive analysis of the histopathology of preoperatively detected TERTp without BRAFV600E . Toward that goal, we studied the ROM and the histopathologic diagnosis of a retrospective cohort of thyroid nodules with TERTp treated at two major academic medical centers.
Materials and Methods
Study cohort and inclusion criteria
The medical records of Massachusetts General Hospital (MGH), Boston, MA, and Memorial Sloan Kettering Cancer Center (MSKCC), New York, NY, were searched for all preoperative FNA samples genotyped using the ThyroSeq GC (Sonic Healthcare USA ThyroSeq Laboratory, Rye Brook, NY) from 2010 to 2024 for MSKCC and from 2016 to 2025 for MGH. After excluding cases with BRAFV600E , 52 patients were identified harboring TERTp mutations with or without other non-BRAFV600E mutations (Fig. 1). These cases are the subject of this report. The study was approved by the Institutional Review Board of MSKCC (IRB 17-103) and MGH (2012P001024-04).
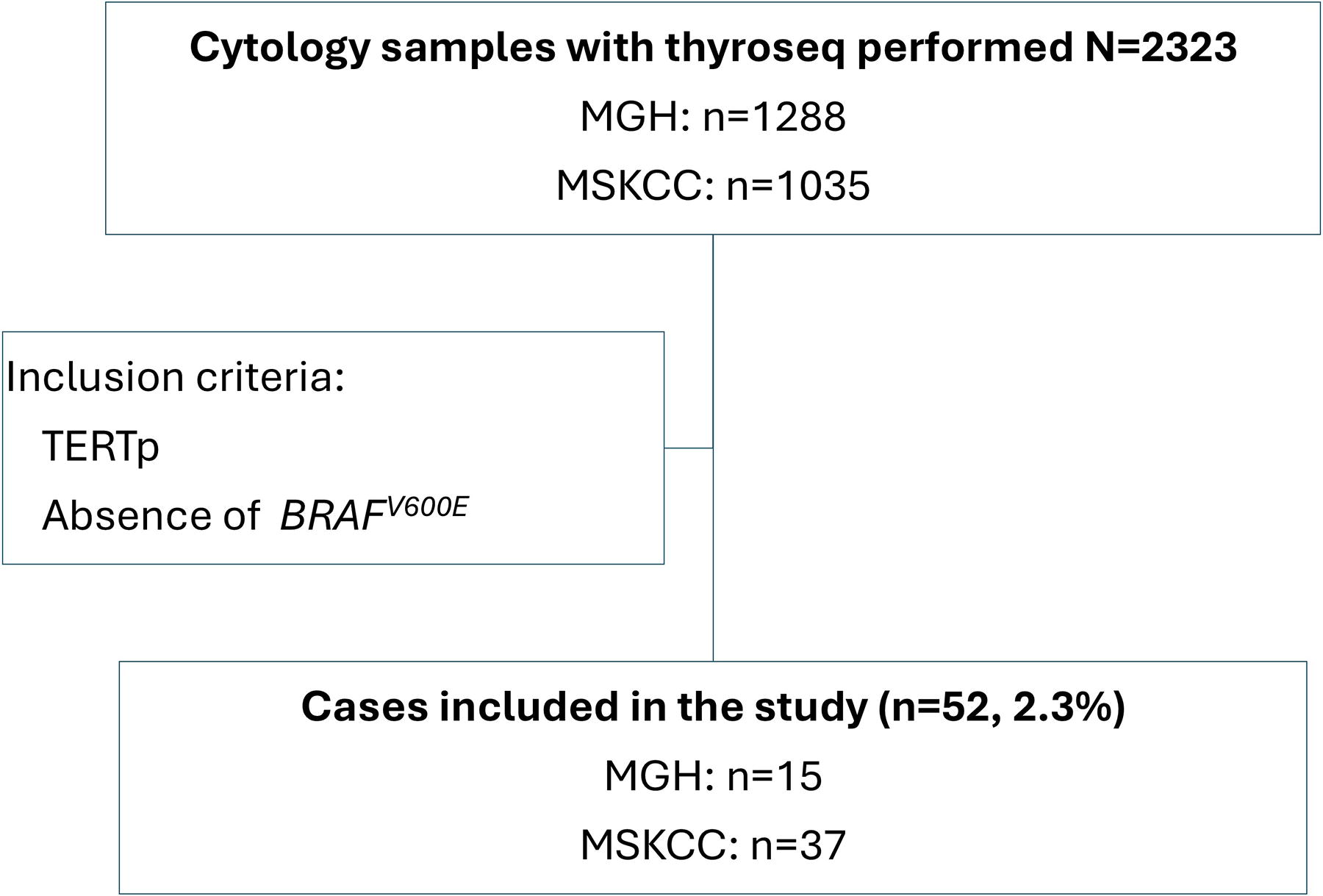
Flow diagram of the participants in the study. MGH, Massachusetts General Hospital; MSKCC, Memorial Sloan Kettering Cancer Center.
Clinical, radiological, histopathologic, and molecular data
Clinical and radiological data were obtained from the medical records. Cases with at least 1 year of follow-up were considered as informative for outcome analysis. In both centers, patients are followed according to the American Thyroid Association (ATA) guidelines. For carcinoma, ultrasound (US) and serum thyroglobulin are performed at 6 months, every 6 months for 2 years and then every year. Benign nodules are generally followed less intensely with just US every year.
The histology slides from the thyroid resections were routinely diagnosed by endocrine pathologists in both centers. They were then rereviewed by endocrine pathologists (B.A.A. and R.A.G.) with 3- and 25-years’ experience, respectively. The tumors were diagnosed according to the fifth edition of the World Health Organization (WHO) classification of thyroid tumors. 16 The pathological stage was assessed according to the eighth edition of the American Joint Committee on Cancer. 17 Angioinvasion was diagnosed using the criteria proposed by WHO fifth edition as “invasion of vessels within the tumor capsule or beyond, with intravascular tumor attached to the vessel wall, or admixed with fibrin or covered by endothelium.” 16
Tumors were subdivided into benign/low-risk neoplasms, ATA low-/intermediate-risk carcinoma, and ATA high-risk carcinoma categories. Based on the most recent WHO classification, the benign/low-risk neoplasms are follicular nodular disease, follicular and oncocytic adenoma, noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) and follicular tumor of uncertain malignant potential (FT-UMP). 16 Low-/intermediate-risk carcinoma definition was mainly based on the one used for the latest ATA low-/intermediate-risk category 18 except for the number of foci of blood vessel invasion cutoff (the latter based on the WHO classification). Among other criteria, the following carcinomas were considered low/intermediate risk: (1) encapsulated follicular and oncocytic carcinoma, minimally invasive or with focal (<4 foci) of angioinvasion; (2) invasive encapsulated follicular variant of papillary thyroid carcinoma (FVPTC), minimally invasive and/or with focal (<4 foci) of angioinvasion; and (3) papillary thyroid carcinoma (PTC) with low volume nodal disease. 18 In addition, encapsulated noninvasive papillary carcinomas with high-grade features (high mitotic count and/or tumor necrosis) were also included in the low-/intermediate-risk category since they were shown to have overall an indolent outcome. 19 The high-risk cases fulfilled the criteria for the ATA high-risk group and/or harbored high-grade/anaplastic histology. These cases included, among other criteria, the presence of oncocytic and follicular carcinoma, widely invasive or with extensive angioinvasion (≥4 foci), high-grade differentiated and poorly differentiated thyroid carcinoma, and anaplastic thyroid carcinoma. ATA high-risk cases were also those cases with distant metastasis at presentation, gross extrathyroidal extension, extensive vascular invasion, and those with large (≥3 cm) metastatic lymph nodes. 18 The cases classified as benign/low-risk neoplasms in each center were reviewed by both the MGH and MSKCC pathologists in a blinded fashion.
The molecular genotyping results, including the allelic fraction, were retrieved from the ThyroSeq report (Sonic Healthcare USA ThyroSeq Laboratory). Ten carcinomas’ cases had their paraffin-embedded tumor tissue genotyped using next-generation sequencing (NGS) assays, and these data were retrieved from the NGS reports. Seven cases from MSKCC were genotyped using MSK-IMPACT targeted NGS 20 and three MGH cases using snapshot (MGH Center for Integrated Diagnostics) (n = 2) and personal genome diagnostics (Labcorp, Burlington, NC) (n = 1) NGS platforms.
Statistical analysis
The ROM was calculated. Additionally, the ROM and clinicopathologic features were compared between nodules harboring TERTp alone and those with TERTp and other concomitant alterations using Fisher’s exact test (p < 0.05 considered significant). Data are expressed as median with interquartile range (IQR) for continuous variables.
Results
Incidence of TERTp mutations
From 2323 (MGH: n = 1288, MSKCC: n = 1035) patients with ThyroSeq GC performed on preoperative (FNA) samples, 52 cases (2.3%) were identified harboring isolated TERTp or TERTp co-occurring with other non-BRAFV600E mutations.
Clinical features, FNA, and therapy
Median (IQR) age at diagnosis in years was 64 (53–73) with females constituting 43 (65%) of all cases (Table 1 and Supplementary Table S1). ThyroSeq genotyping analysis of the FNA showed an isolated TERTp mutation in 21 (40%) of patients, co-occurring TERTp and RAS mutations in 18 (35%), TERTp associated with non-RAS mutations in 8 (15%), and three concomitant mutations (being TERTp, RAS, and other) in 5 (10%). Patients presented with histologically confirmed nodal metastases in two (4%) of cases, and gross extrathyroidal extension was identified in one (2%) patient. Distant metastases were found at presentation in three (6%) of individuals. Most patients 39 (75%) underwent total thyroidectomy, and 12 (23%) patients were initially treated with lobectomy/isthmusectomy. Radioactive iodine (RAI) therapy was administered in 17 (33%) of cases. Median follow-up was 46 months.
Cohort Characteristics of 52 Patients with Promoter Region of TERT-Mutated Thyroid Nodules
In four cases, nodule size was not available by ultrasonography.
IQR, interquartile range; M1, distant metastasis at presentation identified by biopsy or imaging; pN+, pathological nodal metastasis present; TERT, telomerase reverse transcriptase; US, ultrasound.
Histopathology according to risk categories
Median (IQR) tumor size (cm) in the resection was 3.5 (2.6–5.0). Benign/low-risk (i.e., nonmalignant) neoplasms comprised 18 (35%) of all TERTp-mutated cases and were mostly oncocytic and follicular adenomas (Table 2) (Figs. 2 and 3). The oncocytic adenomas comprised 11 of 18 (61%) of noncarcinoma cases. Seventeen (32.5%) of all TERTp-mutated cases were low-/intermediate-risk carcinomas, with the majority (11 of 17, 65%) lacking angioinvasion. The low/intermediate group included three cases of encapsulated noninvasive FVPTC with high-grade features. These three tumors had the histology of encapsulated PTC follicular variant with high mitotic count (five or more per 2 mm2) but lacked invasion. One case also had tumor necrosis. The entire capsule of the carcinoma was submitted for microscopic examination in these three cases. All cases with a diagnosis of benign/low-risk neoplasms (n = 18), and low-/intermediate-risk carcinomas (n = 17) had their tumor capsule submitted entirely for microscopic examination. High-risk carcinomas constituted 32.5% of all cases (n = 17), with 59% of the cases (n = 10) showing high-grade non-anaplastic thyroid carcinoma (high-grade differentiated: n = 6 and poorly differentiated: n = 4). Of the 19 cases initially classified as benign/low-risk neoplasms, there was concordance in the diagnosis of a benign/low-risk neoplasm between MGH and MSKCC in 18 of 19 cases. The discrepant case was classified as FT-UMP in one center and encapsulated PTC, solid subtype, noninvasive in the other center. It was finally categorized as carcinoma for this study.
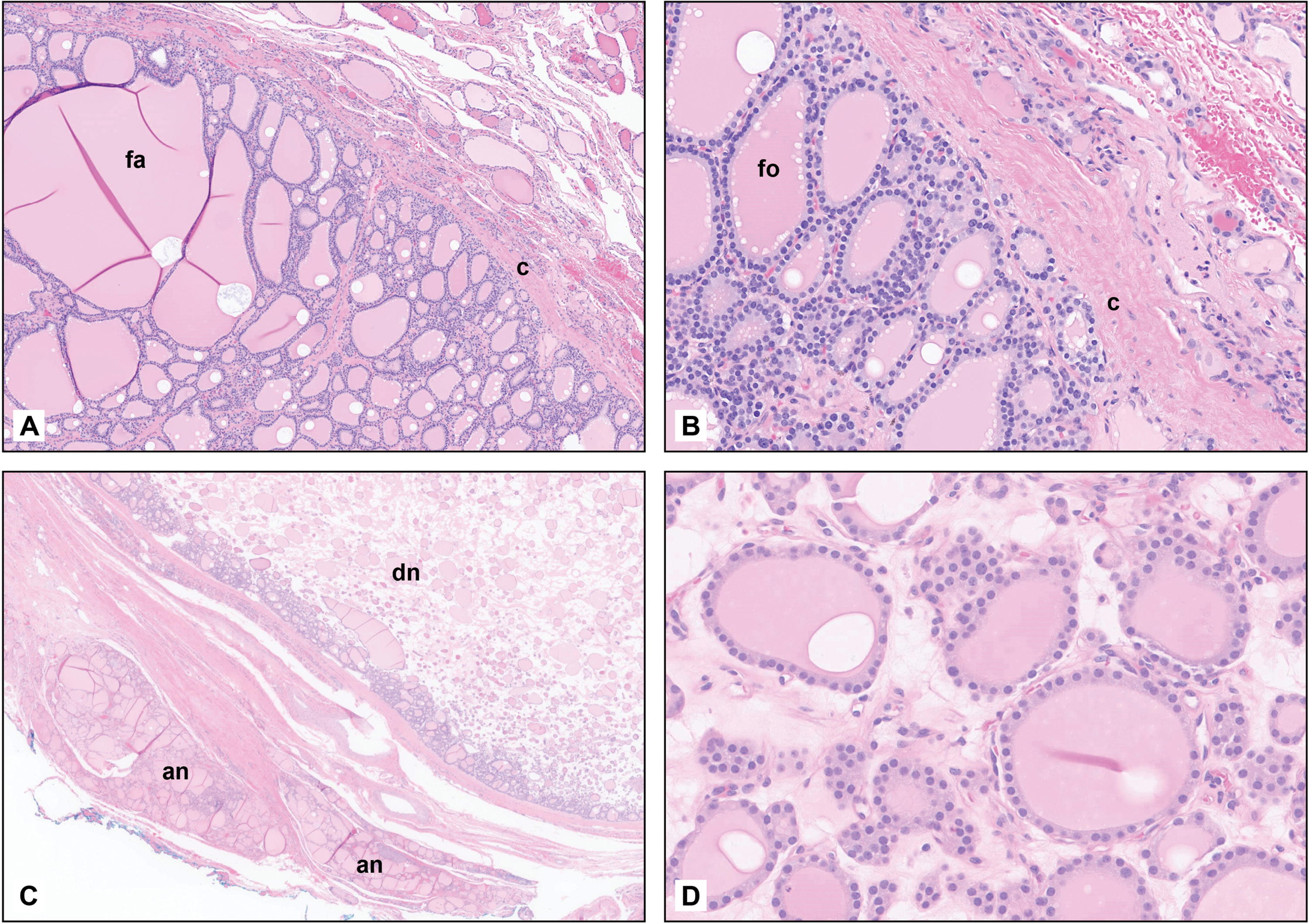
Histological pictures of a 1.2-cm follicular adenoma (fa) containing TERTp and EIF1AX p.A113_splice mutations in a 77-year-old male treated with lobectomy.
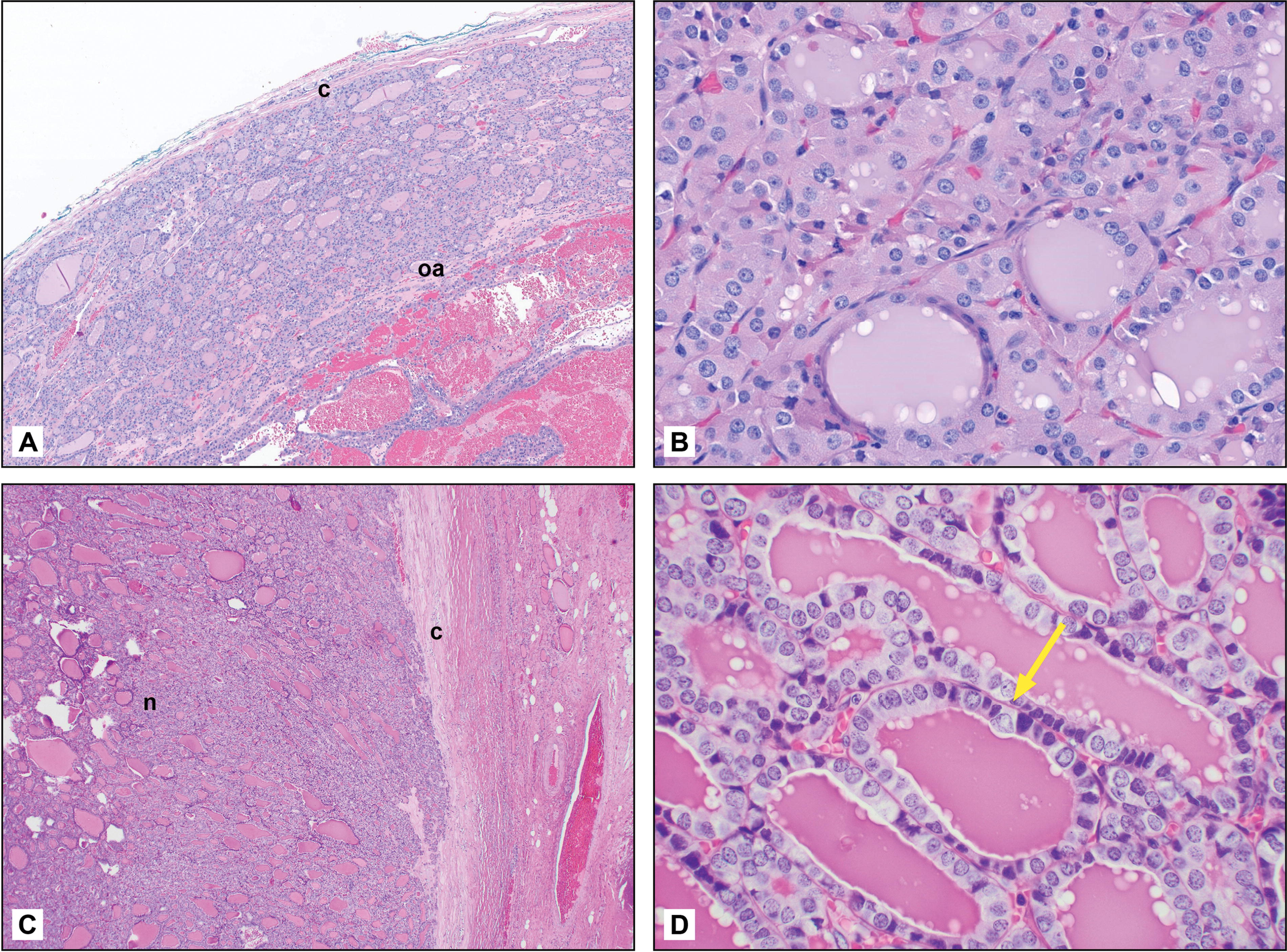
Histological pictures of a 3.3-cm oncocytic adenoma (oa) carrying TERTp, NRAS p.G12V, and EIF1AX p.A113_splice mutations in a 53-year-old male treated with total thyroidectomy.
Histopathologic Features and Risk Classification of 52 Patients with TERT Promoter Mutated Nodules
EFVPTC, encapsulated follicular variant of papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; FT-UMP, follicular tumor of uncertain malignant potential; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; OTC, oncocytic thyroid carcinoma; PTC, papillary thyroid carcinoma.
Histopathology and risk categories according to the mutation profile
The actual TERTp mutations were as follows: C228T (46, 88%); C250T (10, 8%); and A202T (1, 2%) (Table 2 and Supplementary Table S1). The frequency of high-risk carcinomas is significantly higher in tumors with TERTp and co-occurring mutations (15 of 31, 48%) than in those displaying only TERTp mutations (2 of 21, 9.5%, p = 0.006). Patients with tumors containing TERTp coupled with other mutations had a higher rate of high-grade follicular cell-derived non-anaplastic and anaplastic carcinomas (12/31, 39%) than patients with TERTp only (1 of 21, 5%) (p = 0.008). There was also a significantly higher proportion of high-grade follicular cell-derived non-anaplastic carcinoma in patients with two or more mutations (9/31, 29%) than in those with isolated TERTp (1of 21, 5%) (p = 0.04). There was no significant difference in tumor size, encapsulation, presence, and extent of angioinvasion between patients with isolated TERTp mutations and those with TERTp co-occurring with other mutations (p > 0.05). Within patients with carcinoma, there was no difference in pathological stage and angioinvasion between those with TERTp alone and those with TERTp associated with other mutations (p > 0.05).
The ROM according to each mutational group is displayed in Table 3. There was a higher ROM in nodules harboring TERTp and other concomitant alterations (71%) compared with those with TERTp alone (57%), but it was not significant (p = 0.37). Allelic fraction for TERTp mutations was reported in 37 cases, and in 35 (95%), it was >10%.
Risk of Malignancy According to the Underlying Molecular Alterations in Thyroid Nodules with TERT Promoter Mutations Without BRAFV600E Detected in Preoperative Fine Needle Aspiration
ROM, risk of malignancy.
Correlation between ThyroSeq and tissue genotyping
Nine of the 10 cases had TERTp mutation found in both FNA and paraffin-embedded tumor samples. One PTC solid subtype had TERTp detected in the ThyroSeq (allelic fraction 32%), but not in the tissue genotyping snapshot assay.
Overtreatment and outcomes
Of the 18 patients with benign/low-risk neoplasms, 14 (78%) had undergone total thyroidectomy, and thus, 27% of all cases were likely to have been overtreated (Table 4). None of the benign/low-risk neoplasms with adequate follow-up (more than 1 year) recurred. The median (IQR) of follow-up in these cases was 32 (24–43) months. In addition, one minimally invasive oncocytic carcinoma (isolated TERTp, 1.6 cm in a 54-year-old female) underwent total thyroidectomy and could be considered overtreated at diagnosis, as per the most recent ATA guidelines. Overall, 15 (29%) of the 52 cases were likely to have been overtreated—defined as having more extensive surgery than was required by the ultimate pathological diagnosis. Eight patients had recurrence or progression of their disease. Their histotype and mutational profiles were as follows: three anaplastic carcinomas (two with TERTp + RAS + TP53, one TERTp + RAS); two poorly differentiated thyroid carcinomas with angioinvasion (one TERTp + RAS + MSH3, one isolated TERTp); one high-grade PTC, columnar subtype (TERTp and AKT1), one classical PTC (isolated TERTp); and one minimally invasive oncocytic carcinoma (isolated TERTp). Four patients died of the disease. Three of these patients were the abovementioned anaplastic carcinoma, and the fourth one was the abovementioned poorly differentiated carcinoma with angioinvasion and isolated TERTp mutation.
Clinicopathological and Molecular Characteristics of Benign/Low-Risk Neoplasms (Noncarcinomatous)
FTA-P, follicular adenoma with papillary architecture; FT-UMP, follicular tumor of uncertain malignant potential; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; LT, lobectomy; NED, no evidence of disease; TT, total thyroidectomy.
Discussion
The incidence of TERTp mutations in this study (2.3%) is very close to the one (1.7%) in a large cohort of 50,734 indeterminate FNA genotyped by ThyroSeq. 11 This suggests that the frequency of TERTp mutations and the performance of this assay are consistent in FNA of indeterminate nodules. In our cohort of TERTp mutations without BRAFV600E , a significant minority of patients (18, 35%) had noncarcinomatous tumors (benign/low-risk neoplasms). TERTp mutation was also found in benign tumors by Abi-Raad et al. in a multi-institutional study of 32 patients whose FNA was genotyped by ThyroSeq. 14 Of their 27 patients carrying TERTp without BRAFV600E , 18.5% of tumors were benign. 14 The presence of TERTp mutation in benign/low-risk neoplasms is surprising since TERTp was shown to be a late event in tumor carcinogenesis, being more prevalent in high-grade non-anaplastic and anaplastic thyroid carcinomas than in papillary thyroid carcinoma. 21 Except for our series and the ones of Abi-Raad et al. 14 and Boaventura et al., 22 most studies reported the absence of TERTp mutation or single cases of TERTp mutations in cohorts of benign thyroid neoplasms. 3,23 –25 However, this could be due to bias since benign tumors are not routinely genotyped. One possible explanation for the finding of this mutation in benign thyroid lesions is that the TERTp mutation may precede the acquisition of the malignant histologic phenotype. In support of this hypothesis is a case of follicular adenoma reported by Wang et al. in a 69-year-old female. 25 The tumor was histologically a 4-cm follicular adenoma carrying a TERT p.C228T and a NRAS p.Q61R mutations that traveled to distant sites, causing the patient’s demise. 25 The authors, however, do not provide information on the sampling of the capsule of that adenoma. 25 Assuming the capsule of the tumor was entirely submitted for microscopic examination, a metastasizing TERTp-mutated “follicular adenoma” seems to be an extremely rare occurrence, even if it carries another non-BRAFV600E mutation. Indeed, all 12 benign/low-risk neoplasms in the current study with follow-up, and all 5 benign tumors in the one of Abi-Raad et al. did not recur. 14 In both series, all benign/low-risk neoplasm tumors had their entire capsule submitted for microscopic analysis. 14 Furthermore, in both our series and the one of Abi-Raad et al., many benign tumors were found to have TERTp mutations co-occurring with other non-BRAFV600E mutations, and even those did not recur. 14 These additional alterations were in NRAS, EIF1AX, and BRAF (non-p.V600E mutation). One oncocytic adenoma had three mutations (TERTp, NRAS, and EIF1AX). In the series of Abi-Raad et al., two benign tumors carried additional mutations each in HRAS and EIF1AX. 14 Since many authors suggest the performance of radical surgery in patients with TERTp mutations detected preoperatively, 6,10 –13 it is not surprising that 78% of our cases with benign/low-risk neoplasms underwent total thyroidectomy. In view of the available data in the series herein and the literature, these TERTp-mutated benign/low-risk neoplasms appear to have been overtreated.
Although half of our TERTp-mutated noncarcinomatous neoplasms carried another mutation, the presence of an additional mutation increases the rate of an aggressive malignancy. The frequency of high-risk carcinomas as well as the one of high-grade non-anaplastic and anaplastic carcinomas was significantly higher in tumors with TERTp and co-occurring mutations (48% and 39%, respectively) than in those displaying only TERTp mutations (9.5% and 5%, respectively). These data are in congruence with previous studies on the subject, showing more aggressive carcinomas in patients with TERTp co-occurring with other molecular alterations. 14,26,27 The strong correlation between the presence of coexisting TERTp mutations and high-grade carcinoma is, however, not a perfect one since in addition to benign cases with co-occurring mutations, we encountered seven low-/intermediate-risk carcinomas carrying multiple mutations. Of note, these low-/intermediate-risk carcinomas had their entire capsule submitted for histological examinations. In addition to the 14 noncarcinomatous neoplasms treated by total thyroidectomy, one 1.6 cm minimally invasive oncocytic carcinoma underwent total thyroidectomy and could be considered to have been overtreated. Overall, 15 (29%) of patients in this cohort can be considered overtreated.
The vast majority (75%) of patients who relapsed had aggressive histological features. Indeed, out of the eight patients who recurred, six harbored an anaplastic or a high-grade non-anaplastic thyroid carcinoma. Five of these six patients carried multiple mutations. Although histological typing of the tumor appears very powerful and superior to preoperative genotyping in predicting outcome in these series, it is not absolute. Indeed, one of the patients who recurred had a minimally invasive oncocytic carcinoma, and the other was a classical PTC of 1.2 cm with both carrying an isolated TERTp mutation. Eleven of our 13 cases diagnosed as high-grade carcinoma/anaplastic had indeterminate FNA. The finding of TERTp in these cases may have been one of the factors that led to one-stage total thyroidectomy instead of an initial lobectomy in many of those patients. However, the patients would have ended up getting a complete thyroidectomy based on the histological findings if a lobectomy only was performed.
Based on the above data, it seems prudent to base the extent of treatment not solely on the preoperative finding of TERTp mutation in an indeterminate FNA but rather on the combination of clinical, imaging, and molecular features. If the indolent histology found in some of these lesions is confirmed at the behavior level by studies with longer follow-up, lobectomy may be sufficient for the initial management of TERTp thyroid nodules without BRAFV600E as long as there is no aggressive clinical or imaging feature. This is especially relevant in cases with isolated TERTp mutations, given the low probability (9.5%) that nodules with isolated TERTp mutations will be found to harbor high-risk features on surgical pathology analysis that would warrant completion thyroidectomy under current ATA clinical practice guidelines. This will spare many patients with benign/low-risk neoplasms from the side effects of total thyroidectomy, including recurrent nerve injury, hypoparathyroidism, and lifelong thyroid hormone replacement therapy. Completion lobectomy can be performed if the tumor is aggressive upon microscopic examination of the diagnostic lobectomy specimen.
Footnotes
Acknowledgment
The authors thank James Fagin for reviewing this article.
Authors’ Contributions
B.A.A.: Writing, formal analysis, and critical review (equal). R.I. and A.A.: Formal analysis and critical review (equal). P.M.S., M.R.T., and L.G.T.M.: Review and editing and conceptualization (equal). B.X.: Formal analysis and review and editing (equal). R.A.G.: Writing, formal analysis, and conceptualization (lead).
Disclaimer
The content is solely the responsibility of the authors and does not necessarily reflect the official views of the National Institutes of Health.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
R.I., A.A., M.R.T., B.X., L.G.T.M., and R.A.G. receive funding from Cancer Center Support Grant of the National Institutes of Health/National Cancer Institute under award number P30CA008748. B.A.A. and P.M.S. report no funding.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.