
Abstract
Background:
International guidelines now recommend adopting individualized approaches which consider patient preferences when deciding the extent of surgical resection for low-risk differentiated thyroid carcinoma (LRDTC). Information-sharing must be methodical to help patients make informed decisions without feeling overwhelmed by information. Understanding the factors influencing decision-making is therefore essential.
Methods:
Semi-structured interviews were conducted between May 2023 and June 2024 at two large tertiary referral centers in England, United Kingdom. Consecutive sampling via the multidisciplinary team meetings was used to identify patients newly diagnosed with LRDTC measuring 1–4 cm without adverse features, choosing between hemithyroidectomy and total thyroidectomy, or, if diagnosed following hemithyroidectomy, active surveillance and total thyroidectomy. Clinicians directly involved in their care were approached and recruited, with six consultant thyroid surgeons (five male, one female), and two thyroid cancer nurse specialists (both female), agreeing to participate. All had experience managing over 10 LRDTC patients annually.
Transcripts were analyzed using the framework method of thematic analysis.
Results:
Twenty-four patients were identified, and 19 agreed to participate (13 female, 6 male). Information-sharing was often perceived as a didactic process, leaving patients overwhelmed with complex clinical details. Both groups emphasized tailoring information to meet patients’ needs and delivering it in bite-sized portions to enhance comprehension. Key factors influencing individual decisions included a desire among most patients to minimize the number of, and extent of, surgical procedures, the need to preserve the thyroid gland and avoid hormone supplementation, and the patient’s ability to accept the cancer recurrence risk. Although autonomy was paramount for patients, providers’ recommendations still significantly impacted the final decision. Some clinicians expressed concern that multiple treatment options might confuse patients, instead entrusting decision-making to the multidisciplinary team meetings.
Conclusions:
This study identified essential information needs for LRDTC treatment decision-making, which can help inform the development of decision-support tools. Multidisciplinary team discussions may need to evolve to allow greater flexibility and support individualized decision-making.
Background
The incidence of differentiated thyroid carcinoma globally is rising, without a corresponding rise in mortality. 1 Total thyroidectomy (TT) followed by radioactive iodine therapy has traditionally been the mainstay treatment for tumors larger than 1 cm. 2 However, over the past decade, this orthodoxy has been challenged by studies demonstrating that survival rates for low-risk tumors measuring between 1 and 4 cm are not influenced by the extent of surgical resection. 3 As such, international guidelines now recommend adopting an individualized approach that considers patient preferences when determining surgical treatment plans.4,5
In practice, shared decision-making (SDM) on the management of low-risk differentiated thyroid carcinoma (LRDTC) can be challenging, and recommendations on structuring these discussions are lacking. A meta-ethnography study has shown that patients with LRDTC are often dissatisfied with the amount and type of information they receive, while clinicians fear that the complexity and nuances of the treatment options may overwhelm patients. 6 Additionally, they struggle to explore and address patients’ concerns and preferences. Consequently, the treatment provided may not reflect the patient’s true values and long-term wishes. Most data on this topic are retrospective, introducing recall bias and the possibility that respondents’ attitudes to decision making may change based on their eventual outcomes.
We conducted a prospective qualitative study in which patients newly diagnosed with LRDTC and their health care providers shared their experiences and perspectives on treatment decision-making between hemithyroidectomy (HT) and TT. We aimed to explore the key information needs necessary for individualized decision-making. This study also examined the roles of patients, providers, and multidisciplinary team (also called tumor boards) recommendations, in treatment decision-making. To our understanding, this is the first study to prospectively investigate patient decision-making in newly diagnosed patients within the context of the UK National Health Service.
Materials and Methods
Study design
In-depth semi-structured interviews were conducted from May 2023 to June 2024, collecting data from patients newly diagnosed with LRDTC, consultant thyroid surgeons, and thyroid cancer specialist nurses (TCNSs). Separate topic guides were created for each group.
The study was conducted in two large NHS thyroid cancer tertiary referral hospitals in England, United Kingdom. Ethical approval was obtained from the NHS Health Research Authority (REC 22/NS/0157), and research was conducted in accordance with the Declaration of Helsinki (2013). All participants provided written informed consent. The Consolidated Criteria for Reporting Qualitative Research Publication Guidelines were used for study design and reporting. 7
Participants
Patients with low-risk papillary or follicular thyroid carcinoma, with a tumor size between 1 and 4 cm without adverse features, and not taking thyroid hormone supplementation, were eligible to participate. Adverse features were defined by American Thyroid Association guidelines and included aggressive histological features, larger tumor size, and vascular invasion or lymph node metastases. 8 If the diagnosis was established preoperatively through fine-needle aspiration cytology (FNAC), the recommended management according to multiple international guidelines was either an HT or a TT.4,5 If the cancer diagnosis was confirmed by histopathology following an HT, the treatment options would include a completion thyroidectomy or active surveillance. Eligible patients were identified prospectively from the local thyroid cancer multidisciplinary team meeting lists and were invited face-to-face to participate by the researcher (W.Y.). Participation was voluntary. Patients were informed of the study’s role in improving future patients’ care. Demographic data (age, gender, level of education, and employment status) were collected from the patients prior to the interviews.
Six consultant thyroid surgeons and two TCNSs of the eligible patients’ direct care team were approached and recruited for interviews. All participants signed written consent forms before taking part in the study.
Sampling and data saturation
Consecutive sampling was used to recruit patient participants. A prospective data saturation calculation, involving a base size of four interviews, a run length of two interviews, and a new information threshold of ≤5%, was employed to determine the final sample size. 9 Based on this calculation, saturation was achieved after 19 patient interviews. Due to the limited number of clinicians involved, a data saturation calculation was not conducted.
Qualitative analysis
Interviews were performed online (MS Teams) or face-to-face by W.Y. Interview guides were created by W.Y. and S.W. (Supplementary Appendix SA1) and pilot-tested on patients from a thyroid cancer support group. All interviews were audio recorded and transcribed verbatim, and returned to participants for comments. Field notes were taken contemporaneously. Transcripts were organized using the qualitative software QSR NVivo 12®. The framework method of thematic data analysis was employed, using a combination of deductive and inductive analysis. 10 Two researchers (S.W. and W.Y.) independently read the first six patient interview transcripts and four health care provider interview transcripts.
Analytical frameworks were created and applied to index the subsequent transcripts. These frameworks were revised iteratively until all transcripts were coded. During data analysis, patient and health care provider interview data with similar themes were grouped together, giving rise to dimensions and forming the basis of the final themes.
To ensure the reliability and reproducibility of the coding, another researcher (Q.Y.L.) independently coded three transcripts. The coded transcripts were compared between researchers (Q.Y.L. and W.Y.). Discrepancies in the coded transcripts were discussed and resolved. Researcher Q.Y.L. subsequently coded an additional three transcripts, and a 95% intercoder agreement was achieved. Participants were given the option to review the findings.
S.W. is a principal research fellow in health outcome research with experience in framework data analysis. Q.Y.L. is a post-doc research fellow in health outcome research with experience in framework data analysis. W.Y. is an otolaryngology resident doctor and PhD student, who has received formal teaching in qualitative research and has experience in qualitative research.
Results
In total, 24 eligible patients were identified and approached. Three patients declined to be interviewed and two were uncontactable for an interview. Twenty-five semi-structured interviews (median length 45 minutes, range 20–77 minutes) were conducted between May 2023 and June 2024. Participants included 19 patients, 6 consultant thyroid surgeons, and 2 TCNSs. The recruitment process is demonstrated in Figure 1.

Flowchart demonstrating recruitment process of clinicians and patients.
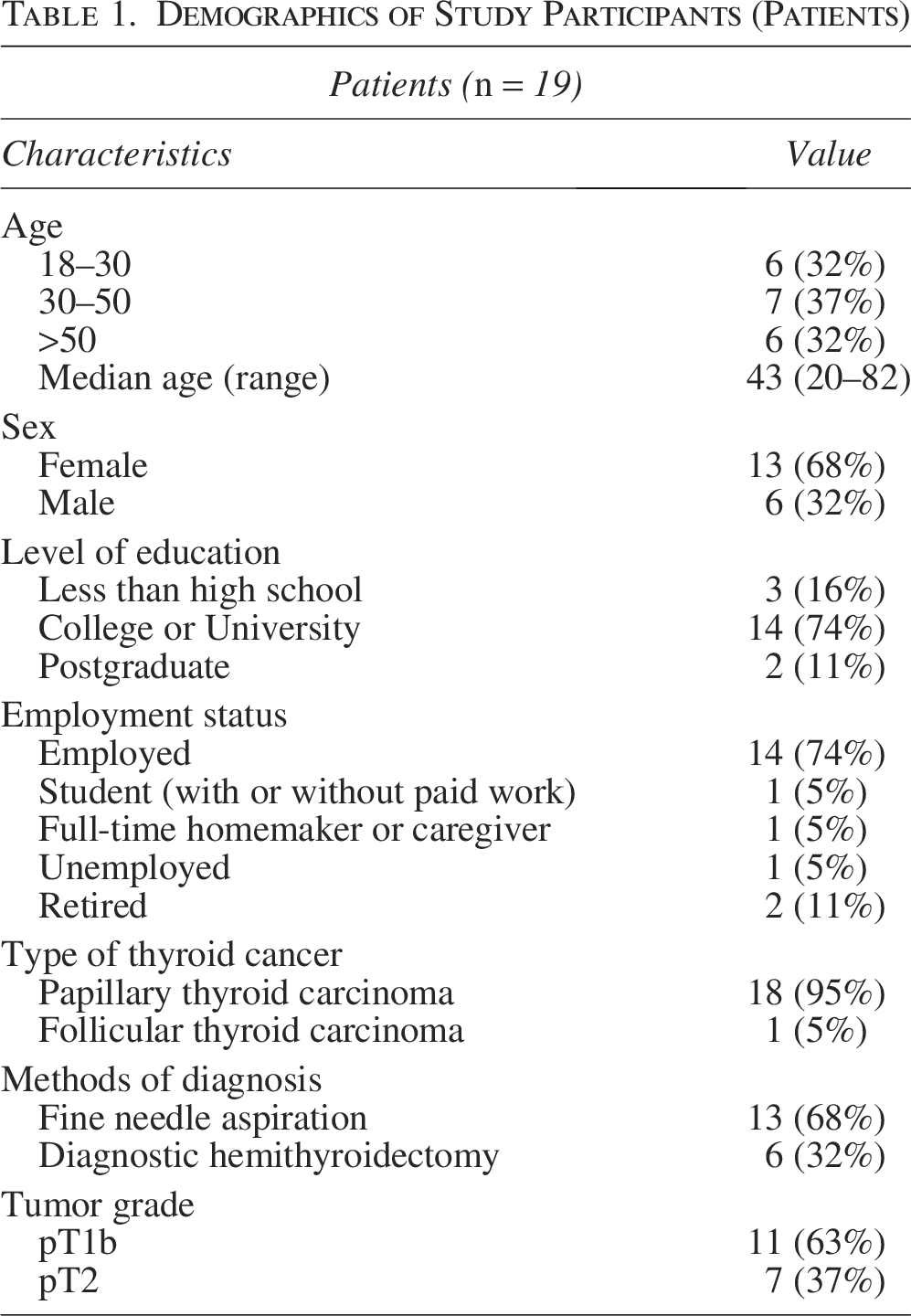
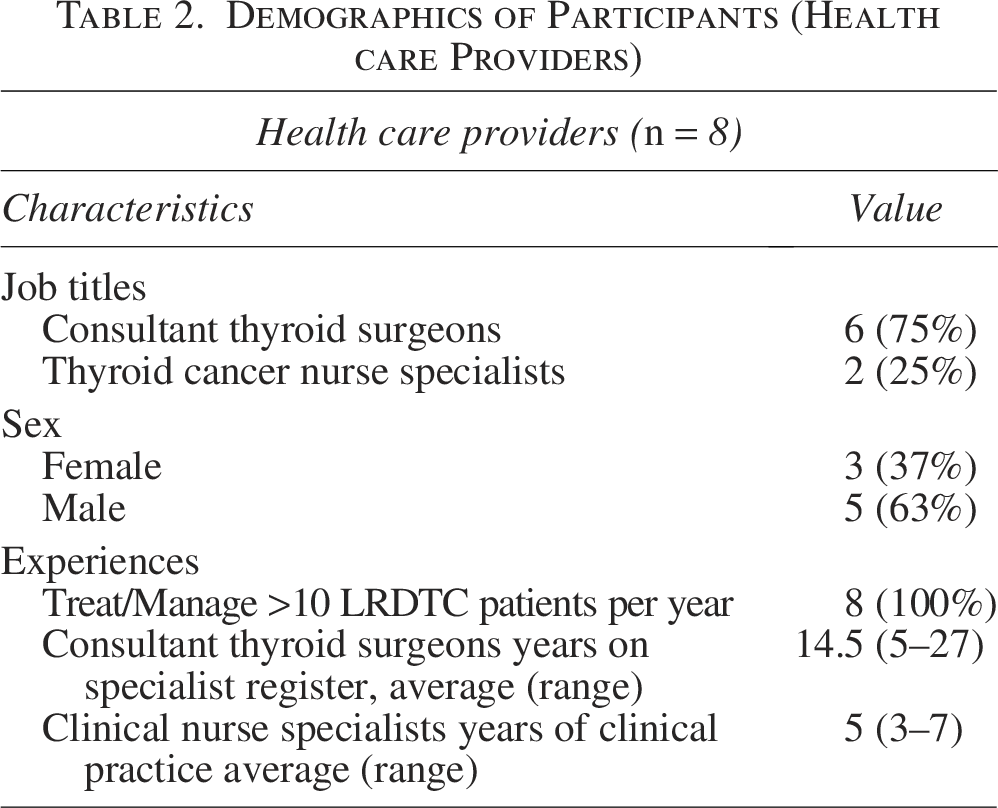
Most patients were female, under 50 years old, employed, and held undergraduate degrees. Patients were recruited from an urban environment. All clinicians managed more than 10 LRDTC patients per year. The demographics of the participants are presented in Tables 1 and 2.
Demographics of Study Participants (Patients)
Demographics of Participants (Health care Providers)
When discussing diagnosis and treatment decision-making for LRDTCs, three key themes were developed from patients and their providers. Each theme is explored below and summarized in figures, which include participants’ quotes. The full analytic frameworks are displayed in Supplementary Appendix SA2 and Supplementary Appendix SA3.
Inadequate information sharing
Vast amounts of information were provided to patients during consultations, including available treatment options, their risks, benefits, and uncertainties. Unfortunately, many patients felt that the information-sharing process was insufficient for decision-making. Some reported difficulties in comprehending the clinical information and its relevance to their daily lives.
Some patients also felt there was a lack of interaction during information delivery. They revealed that clinicians were often eager to share all the information at once, leading to a didactic “very fast presentation of information,” as opposed to a two-way conversation where patients had the opportunity to ask questions. In some cases, this information was delivered shortly after patients received their cancer diagnosis. Consequently, the patients’ ability to process the information was affected by the negative emotions associated with the diagnosis.
Most providers recognized that patients’ information needs varied by age, background, and educational level, and tailored the information accordingly. Some avoided overwhelming patients with too much information initially, allowing them time to process the diagnosis. Information would be reiterated and explained in more detail during a second clinical consultation, to which patients were encouraged to bring a friend or family member.
Another source of information for patients was information booklets (produced by Macmillan Cancer Support) issued by the providers. Overall, mixed reviews were reported by both patients and providers. While the thyroid cancer booklet was largely praised for its clarity and abundant information, some content (e.g., regarding radiotherapy and chemotherapy) was outdated and not directly relevant to patients’ situations. A few patients abandoned the booklet completely after finding it too overwhelming to digest. Many patients wished the information were formatted in bite-sized pieces and arranged in diagrams or comparison tables instead of long paragraphs. A summary of themes is demonstrated in Figure 2.
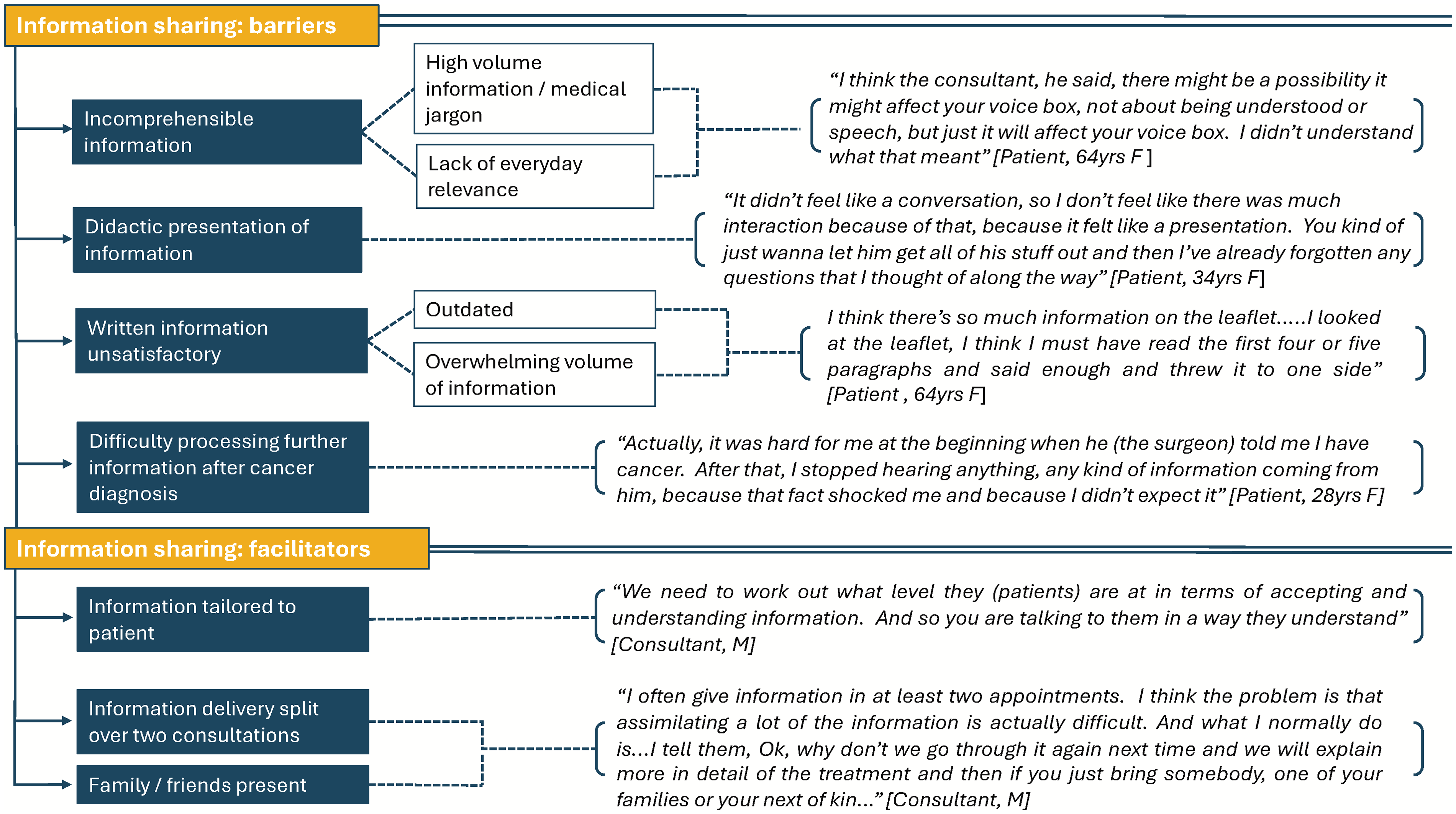
Visual summary of barriers to, and facilitators of, effective information sharing for patients making thyroidectomy treatment decisions, including indicative quotations.
Patients highlight three factors informing their decision-making: a desire to avoid a second operation, the desire to preserve the thyroid gland, and the ability to accept the risk of future cancer recurrence
The majority (15 out of 19) of patients opted for an HT. Both the patients and the providers identified three key factors that significantly influenced the treatment decision-making process. These themes are summarized in Figure 3.

Visual summary of key factors information patient decision-making regarding the management of low-risk differentiated thyroid cancers, including indicative quotations.
First, a key priority for many patients was minimizing the number of, and extent of, surgical procedures. All but one patient diagnosed through histopathology from thyroid lobectomy declined a second operation to remove the remaining thyroid gland. Many opposed having two operations in quick succession, especially if they had endured a challenging recovery from the initial operation. For patients whose diagnosis was confirmed by pre-operative FNAC, most preferred a step-by-step approach and chose HT over TT.
The second key factor that influenced patients’ treatment decision-making was a desire to preserve the thyroid gland and avoid long-term thyroid hormone replacement therapy. Many were concerned about their ability to adjust to the new medication and the effects of having imbalanced hormone levels. However, providers found that this was less of an issue for patients who were already on hormone replacement therapy prior to any surgical intervention, because “they take the drugs anyway, that probably would have pushed [them] towards completion surgery.”
Finally, the decision regarding treatment between HT and TT was influenced by the patient’s ability to accept the risks and consequences of a potential future cancer recurrence. Interestingly, nearly all patients in this study declined TT, as they believed that any cancer recurrence could be effectively treated if it occurred. However, the providers also described a group of patients who would unequivocally choose TT. This group are more risk-averse toward cancer recurrence and also struggles with the uncertainty of potentially needing a second operation should they choose HT.
During the interviews, patients also expressed their concerns about potential surgical complications, especially changes in voice, as these could impact their functionality and future quality of life. Concerns regarding calcium homeostasis, fertility and family planning, the treatment’s effects on pre-existing comorbidities, and long-term quality of life were also frequently raised during consultations.
Patients desire autonomy, clinicians have mixed attitudes to facilitating this if this does not align with multidisciplinary team meeting recommendations
All patients who participated in this study were informed about the treatment options of HT and TT (or completion thyroidectomy and active surveillance if diagnoses came after HT). Fifteen of the 19 patients felt their providers maintained a neutral position and did not sway them toward either treatment. The remaining four patients were strongly recommended one of the two treatment options by their providers. This recommendation was often guided by the local thyroid cancer multidisciplinary team discussion. While three patients were agreeable to the suggested plan, one strongly disagreed and changed the management decision.
Autonomy was paramount for patients; most believed they decided on their treatment themselves, and even those who sought advice from family and friends still felt they were in control of the final decision. Despite this, the provider’s recommendation remained a fundamental part of patient decision-making. When asked whether they would alter their choice if providers recommended a different treatment than they had chosen, most indicated they would change or seriously consider changing their decision, even though they still felt in control.
Clinical equipoise regarding treatment decision-making for LRDTC is well-known among the providers. Half of the providers involved in the study supported patients in making their own decisions, while the other half believed the thyroid cancer multidisciplinary team recommendation should lead the decision-making process. They feared that offering multiple treatment options would confuse patients and increase their anxiety, while the multidisciplinary team recommendation would alleviate patients’ decision-making burden while providing a safety net for the providers. When patients chose a treatment that did not align with the multidisciplinary team recommendation, these providers would present the case back to the multidisciplinary team meeting for approval before commencing the treatment.
These themes are summarized in Figure 4.

Visual summary of conflicting factors for patients and clinicians regarding treatment decision making for low-risk differentiated thyroid cancer, including indicative quotations.
Discussion
This qualitative study explored key elements of the treatment decision-making process for LRDTC. The views and experiences of patients and providers were collected prospectively to provide a comprehensive understanding of information needs during this process. This study highlights key patient priorities during these discussions, including specific operative risks and a desire to minimize repeated operations. It provides specific practical points for the design of future decision-making tools and highlights a discrepancy between how different clinicians interact with multidisciplinary team recommendations.
Effective communication of treatment options along with their associated risks, benefits, and uncertainties between healthcare providers and patients has become a priority as patients assume collaborative roles in decision-making. 11 Unfortunately, our study revealed that many patients were dissatisfied with the information-sharing process. Communicating health information can be challenging, with needs differing by gender, age, cultural background, educational level, disease stage, and coping style.12,13 The aim of information-sharing should not be to convey every detail of treatment, but to provide information tailored to the patients’ specific needs.14,15 When providers meet these needs, patients feel reassured, less anxious, and more optimistic about the treatment process and outcomes. 15 Our study has highlighted that there is a desire for written information that is specific to the patient, up to date, succinct, with a mixture of text and diagrams or flowcharts.
This study has identified three essential factors that informed the patient’s treatment decision-making between HT and TT: (1) a preference to minimize the number of, and extent of, operations; (2) the need to preserve the thyroid gland and avoid long-term thyroid hormone replacement medication; and (3) the patient’s ability to accept the risk of cancer recurrence. These were similar to findings from a scoping review conducted by Wei et al. (2021), which suggested that the risk of cancer recurrence or spread, the need for hormone replacement therapy, and voice change were the main factors informing decision-making between active surveillance, thyroid lobectomy and TT. 16 The consistency of patients’ responses on this matter in both retrospective and prospective studies demonstrates that these issues are of paramount importance to patients and must be addressed in consultations.
In our study, voice change was identified as a primary concern by patients. However, it was not a decisive factor when choosing between HT and TT. On the other hand, whether the patient may require an immediate completion thyroidectomy due to unexpected pathological findings, such as angioinvasion or extrathyroidal extension, can significantly influence the patient’s choice regarding the extent of surgical treatment. It is essential that patients are made aware of this downstream risk when decisions involve the choice of HT. In a survey study by Karcioglu et al. (2022), many thyroid cancer survivors indicated that they were unaware that subsequent treatment options, such as the necessity for a completion thyroidectomy or radioactive iodine, would depend on the outcomes of the preceding steps. 17 Similarly, recent work by Underwood et al. (2024) found that when discussing surgical options surgeons tend to focus on oncological outcomes and surgical risks, and less commonly discussed the possibility of needing thyroid hormone supplementation or completion thyroidectomy without patient prompting, 18 two areas which our study has highlighted are hugely influential to patients. Aligning the agendas of patients and clinicians in these discussions to ensure these critical points are discussed is essential to allow genuine SDM to take place and subsequently improve treatment satisfaction.
Most patients in this study had treatment options presented to them in a balanced manner. Autonomy was highly valued by patients during decision-making. However, their choices could be easily influenced by the providers’ recommendations. This is consistent with our previous systematic review, where patients reported that clinicians’ recommendations were the most significant factor affecting their ultimate decisions. 6 Unfortunately, clinicians’ advice is often shaped by their impressions of a patient’s anxiety and risk tolerance. As a result, the treatment received may not reflect patients’ values and long-term goals. 6
Lastly, this study highlighted an interesting contrast between a group of clinicians who more comfortably supported patients with SDM, and those who believed the multidisciplinary team recommendation should lead the decision-making. The latter worried presenting patients with alternative options would confuse them and exacerbate their anxiety. Elwyn et al. (2017), who described the three-talk model of SDM, argued that SDM is the solution to this concern, rather than the cause. 19 This is because SDM takes into account the extent to which patients want involvement in decision-making. Gu et al. (2024) highlight this spectrum, finding some patients wanted to take a more “paternalistic approach” in which treatment decisions were led by clinicians, while others—notably, younger patients—want to have more autonomy over their decision making. 20 Patients may wish to be informed about the options without necessarily wanting to bear full responsibility for the decisions; SDM accommodates this approach. 21
Currently, multidisciplinary team discussions are regarded as best practice in decision-making for cancer patients worldwide. 22 However, multidisciplinary team meetings tend to focus primarily on the biomedical model of disease, often overlooking the patient’s psychosocial information and perspective on treatment.23,24 Rather than determining which valid treatment options are available, most multidisciplinary team discussions revolve around debating the ‘best’ treatment for a patient. As a result, multidisciplinary team discussions may pose a barrier to implementing SDM as they hinder providers from focussing on patients’ values and preferences. 24 When multiple treatment options with similar oncological outcomes are available, patients’ values should guide decisions, and multidisciplinary team discussions should encourage flexibility and support individualized decision-making.
Strengths and limitations
A major strength of this study is the integration and synthesis of data from patients and healthcare providers to gain a comprehensive understanding of the current decision-making process for managing LRDTC. The convergence of information from various sources is also useful for testing and establishing data validity. 25 Furthermore, the prospective study design ensured that the decision-making process was fresh in the patients’ memories, minimizing the recall bias associated with delayed interviews, which might also be influenced by their eventual clinical outcome. To the authors’ knowledge, there is no prospective data collected on this topic within the context of a European healthcare system and very little internationally. 26
Limitations of the study include a relatively small sample size of health care providers and patients primarily from similar backgrounds (English-speaking, relatively young, and well-educated). Consequently, the approaches to SDM may differ from those of clinicians in other cancer centers, and it is possible that patients with different backgrounds or in other settings may have varying information needs and concerns. As the participants were recruited from two high-volume tertiary-care centers, there is also the potential for referral bias, while the nature of the recruitment adds the risk of volunteer bias. These centers may have better organizational infrastructure and resources to support regular ultrasound-guided monitoring, which might contribute to why patients involved in the study chose more conservative treatment options.
Future research
Decision support tools, such as patient decision aids, can enhance SDM by providing patients with relevant information and clarifying their values regarding the outcomes of options. 27 Currently, only a few decision support tools exist in the literature, all developed using data collected retrospectively.28–30 In contrast, this study prospectively gathered information from newly diagnosed LRDTC patients engaged in SDM. Using this data, we have developed two decision support tools for decision-making on the extent of surgical resection for LRDTC, which we believe will better meet the needs of thyroid cancer patients. These tools will first undergo rigorous testing.
Conclusion
The traditional, paternalistic paradigm of healthcare delivery is rapidly disappearing, with a growing emphasis on SDM centered on patients’ values, needs, and preferences. This qualitative study has provided important insight into the information needs of patients involved in treatment decision-making for LRDTC. It identifies three key factors in the decision-making between HT and TT, which will aid in developing a thyroid cancer patient decision aid. As patients become increasingly involved in their health decisions, the focus of multidisciplinary team discussions may need to shift towards providing available, valid treatment options rather than solely determining the “best” treatment option.
Authors’ Contributions
W.Y.: Conceptualization (lead), drafting (equal), revision and editing (equal), data acquisition (equal), data analysis (equal), and data interpretation (equal). O.S.: Drafting (equal), revision and editing (equal), data analysis (equal), and data interpretation (equal). S.N.R.: Conceptualization (support), revision and editing (support), data analysis (support), and data interpretation (support). S.W.: Revision and editing (support), data analysis (support), and data interpretation (support). D.S.K.: Conceptualization (support), revision and editing (support), data analysis (support), and data interpretation (support).
Footnotes
Acknowledgments
The authors thank all patients, patient advocates, and thyroid clinicians who participated in this study.
Author Disclosure Statement
No conflicts of interest to disclose.
Funding Information
No relevant funding to disclose.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.