
Abstract
Background:
The nPulse™ Vybrance™ Percutaneous Electrode System delivers nanosecond pulsed field ablation (nsPFA), a nonthermal technology that permeabilizes cell membranes while preserving surrounding structures. As a novel therapeutic approach in the United States, nsPFA may offer a nonsurgical alternative for symptomatic benign thyroid nodules (BTNs). This study evaluates the short-term clinical outcomes and safety of nsPFA treatment performed in a clinic setting, focusing on changes in nodule volume and treatment-related complications.
Methods:
A retrospective chart review was conducted of 38 patients (48 symptomatic BTNs) treated with nsPFA. Benign cytology was confirmed via fine-needle aspiration biopsy. Since some patients underwent nsPFA of multiple BTNs, analysis of volume reduction was performed at the nodule level using a repeated measures approach, which accounts for within-patient correlation when estimating average changes over time.
Results:
Average nodule volume reduction at 1, 3, 6, and 12 months was 49.0% [confidence interval (CI) 42.5–55.4], 53.5% [CI 48.6–58.4], 51.8% [CI 45.2–58.5], and 50.2% [CI 34.9–65.5], respectively. Primary nodules received a median of 37 low-voltage and 24 default-voltage cycles, with additional nodules requiring fewer total cycles. No procedural or post-procedural complications were observed. All patients reported symptomatic improvement, often as early as 2 weeks following treatment. Three patients with toxic nodules and one with a nontoxic nodule were initially on antithyroid medication; all successfully discontinued antithyroid medication within 1 month of nsPFA. Subsequent thyroid function monitoring showed no abnormalities across patients with toxic and nontoxic nodules.
Conclusions:
This study represents the first reported clinical series of nsPFA outcomes for thyroid nodules in North America and the first in the world in a clinic setting. Early findings suggest that nsPFA is a promising, minimally invasive alternative to surgery for symptomatic BTNs, offering significant volume reduction and an excellent safety profile. The rapid symptomatic improvement and durable volume reductions during limited follow-up support further investigation. The modest sample size, retrospective design, and loss to follow-up at later time points may affect the interpretation of sustained effectiveness. Larger, prospective studies with extended follow-up are warranted to validate these results, assess long-term outcomes, and compare procedural environments.
Keywords
Summary of the Problem
Thyroid nodules are highly prevalent, affecting approximately 50% of adults in the United States. 1 Most are benign and asymptomatic; however, a subset of benign thyroid nodules (BTNs) cause dysphagia, dyspnea, discomfort, autonomous hormone production, cosmetic deformities, or growth-related distress.1,2 These BTNs may significantly impact quality of life and often require intervention.1–3 Surgical thyroidectomy remains the standard treatment for symptomatic BTNs but poses substantial risks, recovery time, and operative costs, prompting interest in less invasive alternatives.1–3
Thermal ablation techniques, including radiofrequency ablation and microwave ablation, can be performed under local anesthesia to provide meaningful volume reduction and symptom relief. 4 However, they are limited by thermal diffusion and the heat-sink effect, which compromise precision near critical structures and increase risks of residual tissue, regrowth, and collateral injury.4,5
Pulsed field ablation (PFA) is a nonthermal technique that uses controlled electrical fields to induce selective cellular apoptosis while sparing surrounding tissue.6,7 Nanosecond PFA (nsPFA) delivers nanosecond pulses that permeabilize intracellular organelle membranes, offering highly localized cytotoxicity and enhanced nerve preservation.7–9 The nPulse Vybrance Percutaneous Electrode (PE) System, formerly the CellFX® PE System (Pulse Biosciences, Hayward, CA), is the first nsPFA platform approved for soft tissue ablation by the U.S. Food and Drug Administration (FDA).8,10
Early nsPFA for symptomatic BTNs evidence suggests favorable safety, efficacy, and precision, and clinic-based nsPFA may provide substantive cost and resource-utilization advantages over operating-room-based ablation. This study presents the first clinical series in North America and the first clinic-based series in the world performed with local anesthesia only in an outpatient setting. The primary objective was to evaluate safety, thyroid function stability, and volume reduction rate (VRR) following nsPFA for symptomatic BTNs. Secondary aims included exploring associations between treatment parameters, nodule characteristics, and clinical outcomes.
Methods
A retrospective, single-institution cohort study was approved by the Sarasota Memorial Health Care System Institutional Review Board (IRB#: 00002932) with a waiver of informed consent for research due to minimal risk. Patients treated with nsPFA by the Principal Investigator, a high-volume thyroid surgeon, from May 2024 through June 2025 were included. Data on voltage setting (default-voltage vs. low-voltage) and number of pulse cycles were collected to evaluate associations with VRR, thyroid function, and complications. Patients were informed of management options and early feasibility data from Spiezia et al. prior to consent.9,10
Eligibility criteria
Inclusion criteria: age ≥18 years; at least one BTN with Bethesda II cytology from fine needle aspiration biopsy per American Thyroid Association (ATA) guidelines for ablation; and symptomatic nodules causing compressive symptoms, cosmetic concerns, or autonomous function. 1
Exclusion criteria: Suspicion of malignancy, prior thyroid surgery or ablation, contraindications to clinic-based procedures, or incomplete records. 1 In multinodular cases, nontarget secondary or tertiary nodules with a baseline volume <1 mL were excluded from analysis.
nsPFA procedure
Procedures were performed in a clinic setting with local anesthesia (1% lidocaine) using the nPulse Vybrance PE System. Anxiolytic (alprazolam) and/or muscle relaxant (cyclobenzaprine) were administered as needed for anxiety, discomfort, or muscle contractions. Hydrodissection (5% dextrose) was used discretionarily to limit electrical field progression and associated muscle and nerve stimulation and discomfort. 5
Under ultrasound, a bipolar electrode was inserted using a 13-gauge needle (n = 9) and an 18-gauge (n = 29) after FDA clearance. 10 Eight-second pulses were delivered, and voltage was adjusted for nodule size, composition, location, and patient tolerance. 9 The Position, Pulse, Proceed method was utilized.4,9 Treated tissue became hyperechoic from electrolysis, enabling clear identification from untreated areas. 11 The operator provided continuous procedural explanation, encouraging patient feedback to assess comfort. Pre- and postprocedure laryngeal ultrasound assessed vocal fold motion. Patient tolerance guided treatment completeness, and all patients were monitored for regrowth.
Data collection
Variables included demographics, nodule characteristics, pre-/postprocedure antithyroid medications (methimazole or propylthiouracil [PTU]), pre-/postprocedure thyroid function, pre-/postprocedure ultrasound nodule dimensions, anxiolytic and/or muscle relaxant administration, operator-observed muscle contractions, patient-reported intraprocedural discomfort, voltage setting, cycle number, procedure-related complications or adverse events, nodule VRR, and patient-reported symptomatic relief. Available data were collected for 2-week and 1-, 3-, 6-, and 12-month follow-up visits. VRR was calculated using the ATA-recommended half-cube formula. 12
Statistical methods
Descriptive statistics summarized demographic and baseline clinical characteristics. Repeated-measures methods were used to estimate the average VRR at each time point and evaluate potential predictors of VRR in exploratory analysis. This approach accounted for the correlation among the multiple nodules within patients and longitudinal time points. Significance was defined as p < 0.05. Statistical analyses were performed using SAS statistical software version 9.4 (SAS Institute Inc., Cary, NC).
Results
A total of 38 subjects (48 nodules) were included. The cohort was 89.5% female with a median age of 55.5 years (interquartile range [IQR]: 42, 68) and the median body mass index of 25.4 kg/m2 (IQR: 22.7, 34.2). Median baseline thyrotropin (TSH) was 1.1 mIU/L (IQR: 0.9, 1.7), and median free thyroxine (fT4) was 1.1 ng/dL (IQR: 0.9, 1.2). The median procedure duration was 52 minutes (IQR: 35, 66). Four subjects received antithyroid medication before treatment; three had toxic nodules, and one was treated for concomitant hyperthyroidism (Table 1).
Baseline Characteristics, Procedural Parameters, and Treatment Outcomes
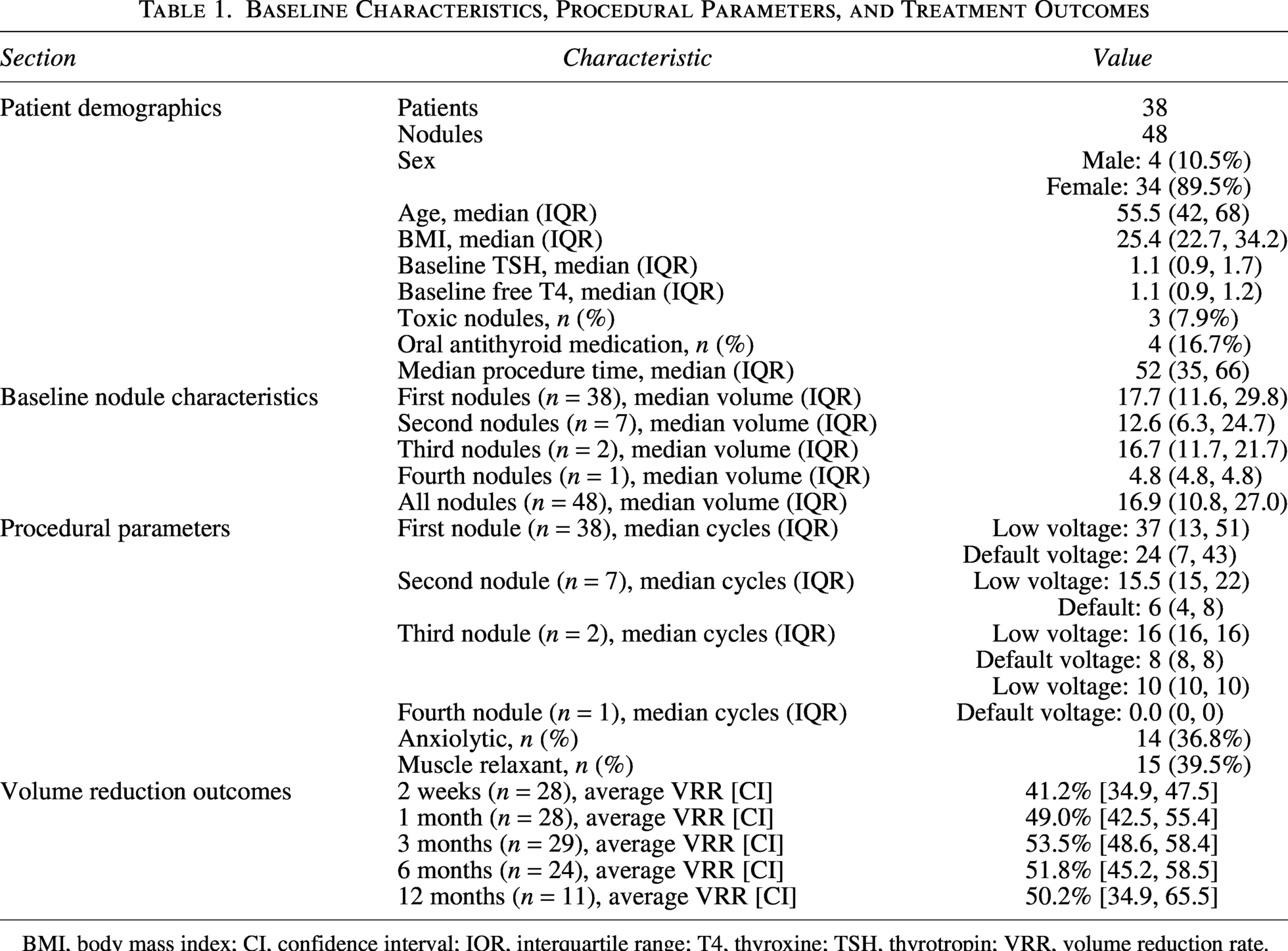
BMI, body mass index; CI, confidence interval; IQR, interquartile range; T4, thyroxine; TSH, thyrotropin; VRR, volume reduction rate.
The median baseline nodule volume (n = 48) was 16.9 mL (IQR: 10.8, 27.0). Nodules were ordered by size, with the first nodules being the largest. The median baseline volume of the first nodules was 17.7 mL (IQR: 11.6, 29.8), of the second nodules was 12.6 mL (IQR: 6.3, 24.7), and of the third nodules was 16.7 mL (IQR: 11.7, 21.7) (Table 1). One subject had four treated nodules (the fourth nodule = 4.8 mL). Skeletal muscle contractions occurred in all patients, varying by anatomical region. No complications were observed.
At 1 month, 92.0% of patients with available data had normal TSH, and 92.3% had normal fT4. At 6 months, all available thyroid lab values were normal. Patients with toxic nodules discontinued antithyroid medications within 1 month. No patient required surgery or repeat nsPFA.
Median numbers of cycles delivered to primary nodules were 37 low-voltage (IQR: 13, 51) and 24 default-voltage (IQR: 7, 43). Secondary, tertiary, and quaternary nodules received fewer total cycles (Table 1). Average nodule VRR was 41.2% at 2 weeks [confidence interval (CI) 34.9–47.5], 49.0% at 1 month [CI: 42.5–55.4], and 53.5% at 3 months [CI: 48.6–58.4] and remained stable above 50% thereafter, measuring 51.8% at 6 months [CI: 45.2–58.5] and 50.2% at 12 months [CI: 34.9–65.5] (Fig. 1 and Table 1). Average VRR increased significantly post-2 weeks [p < 0.001 vs. 1, 3, 6, and 12 months, 4 degrees of freedom (df) test] and remained ∼50% from 1 month onward (p = 0.39 vs. 3, 6, and 12 months, 3df test). Two nodules coalesced by 6 months, precluding individual VRR calculation; a combined VRR of 46.5% was calculated using summed baseline volumes. There was no significant difference in average VRR between 13 and 18 g needles (p = 0.63). Later averages should be interpreted according to smaller samples.
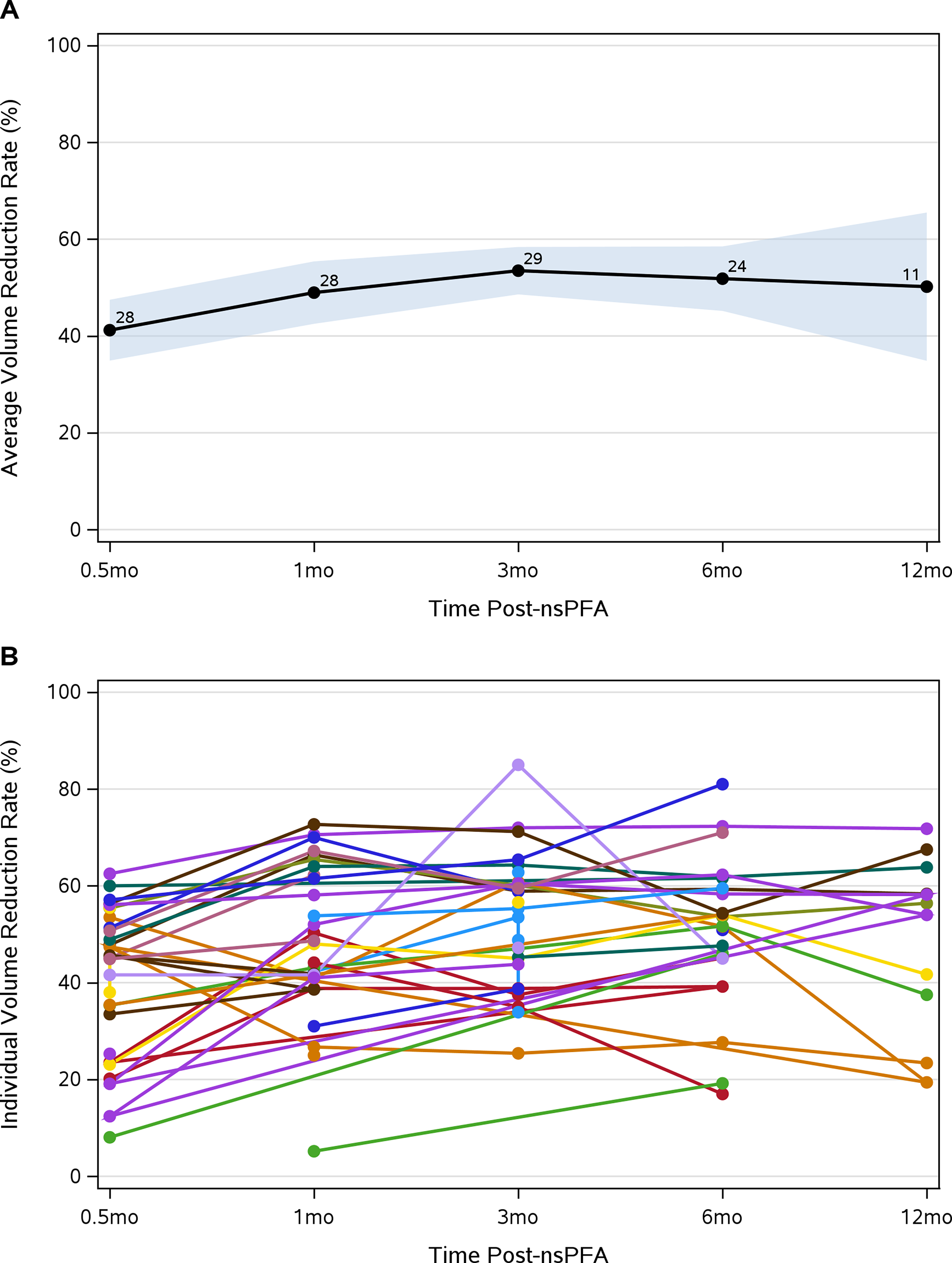
Average
Key Concluding Messages
This first North American and first clinic-based global series demonstrates that nsPFA can safely and effectively treat symptomatic BTNs in awake patients. No complications occurred, and VRR was rapid, stabilizing at ∼50% from 1 month. Short-term reduction is comparable to thermal ablation, although it appears to occur earlier and taper thereafter. Similarly, symptomatic improvement was early, and patients receiving antithyroid medication discontinued treatment with stable thyroid function across toxic and nontoxic nodules.
These findings complement but differ from the prospective early feasibility study by Spiezia et al. Their sedated procedural environment may have enabled higher ablation density, reflected in greater average 1-month VRR (71.1%). In contrast, tolerance, anxiety, and real-time communication in awake patients limited cycle number and voltage. While 1-year outcomes in fully treated nodules suggest durable responses, these findings underscore how procedural environment and patient experience may influence ablation completeness.
Despite encouraging results, challenges remain, and additional data are needed for long-term conclusions. This real-world clinic-based series provides early insight into a procedure with clear clinical and economic advantages and elucidates knowledge gaps that merit further investigation of treatment parameters and procedural settings to optimize clinical outcomes, patient experience, and satisfaction.
Need for More Research
This study is limited by its retrospective, single-operator design. Insufficient follow-up data may limit the conclusiveness of durability assessments, and the absence of a control group restricts comparison with established ablation modalities. Additional constraints include procedural variability, data availability and subjectivity, sample size, and follow-up duration.
Future work should include prospective, multi-institutional studies with larger cohorts, longer follow-ups, and standardized approaches to adjunctive medications, needle gauge, voltage delivery, and patient-reported outcomes to strengthen clinical assessments. Additional clarity on the influence of procedural environment, voltage selection, and cycle number on long-term efficacy is essential. Refinement of treatment parameters and collaboration with industry partners to optimize energy delivery may enhance the patient experience, treatment completeness, and volume reduction. Larger nodules demonstrated greater volume reduction, suggesting a dose–response behavior that could guide protocol refinement. Characterizing the procedural learning curve will be important to facilitate reproducibility and broader adoption. Finally, parallel evaluations of nsPFA under sedation or general anesthesia could clarify which procedural setting provides the better balance of efficacy, cost, and patient experience.
Authors’ Contributions
I.C.I.: Writing–original draft (lead), conceptualization (lead), and review and editing (equal). C.M.: Writing–original draft (supporting) and review and editing (equal). M.M.: Review and editing (equal). T.S.K.: Formal analysis (lead) and methodology (equal). R.P.T.: Writing–original draft (equal), conceptualization (equal), and methodology (lead).
Footnotes
Acknowledgments
The authors would like to acknowledge the Kolschowsky Research and Education Institute, Research Division, First Physicians Group, Thyroid and Parathyroid Center, Division of Head and Neck Endocrine Surgery, and Head and Neck Surgery, Brian D. Jellison Cancer Institute at Sarasota Memorial Health Care System for their assistance and resources provided for the study. Additionally, they would like to thank the Sarasota Memorial Healthcare Foundation for providing the funding to conduct the study.
Author Disclosure Statement
I.C.I., C.M., M.M., and T.S.K. report no conflicts of interest. R.P.T. is a consultant with Pulse Biosciences, Inc.; however, data collection and analysis were conducted independently by the research team.
Funding Information
I.C.I., C.M., M.M., and T.S.K. report no funding. R.P.T. received funding from the Sarasota Memorial Healthcare Foundation. No specific grant number is available.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.