
Abstract
Background:
Thyroid disease in pregnancy, preconception, and postpartum is a common and clinically relevant problem. Since the publication of the American Thyroid Association (ATA) guidelines in 2017, substantial new clinical and scientific evidence has become available. The aim of these guidelines is to provide clinicians, patients, researchers, and policymakers with evidence-based recommendations on the care of women with thyroid disease before, during, and after pregnancy.
Methods:
The clinical questions addressed were informed by prior ATA guidelines, stakeholder feedback, a global needs assessment, and input from the multidisciplinary task force. Systematic literature searches were conducted with the support from a medical librarian and evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation framework. Recommendations were formulated based on the quality of evidence, balance of benefits and harms, patient values, feasibility, and equity. Where data were limited, Good Practice Statements were formulated. The task force included representatives from 10 international societies as well as patient advocacy groups and a methodologist.
Results:
The updated guidelines include recommendations on thyroid function testing, iodine supplementation, thyroid autoimmunity, hypothyroidism, hypothyroxinemia, hyperthyroidism and Graves’ disease, thyroid nodules and cancer, and postpartum thyroid dysfunction for women with infertility, pregnant women, and women during postpartum and/or lactation. Recommendations are presented using recommendation tables, additional practical considerations are highlighted in boxes, and background information is provided in the text, tables, and figures per disease entity and chronological subset.
Conclusions:
These 2026 ATA guidelines provide updated, evidence-based recommendations for the diagnosis and management of thyroid disease in women during preconception, pregnancy, and postpartum. While acknowledging that much of the evidence remains of low-to-moderate quality, these guidelines represent current best practices and consensus among international experts from different fields, offering an optimized framework for individualized patient care.
A. Introduction
This document is an update of the 2017 American Thyroid Association (ATA) guidelines for the diagnosis and management of thyroid disease during pregnancy and postpartum. 1 Since the release of the 2017 guidelines, substantial new data have improved our understanding of gestational thyroid physiology; definition of (ab)normal thyroid function tests; quantification of thyroid-disease-related risks; and the harms, benefits, and optimal timing of treatment options for thyroid conditions preconception, in pregnancy, and postpartum.
We established three main goals at the start of the process of updating the guidelines. The first goal was to improve the impact of the guidelines. To achieve this, we first formed key collaborations with 10 international societies, including those that represent obstetricians, fertility specialists, surgeons, and patients with thyroid disease. Representatives of these societies were then invited to serve as committee/writing group members to optimize the content and readability of the document among these disciplines. Second, we wanted to modernize the appearance of the guidelines. To achieve this goal, we intentionally avoided using the text of previous guidelines as a starting point, opting instead to depart from the traditional question-based outline that has generally characterized ATA guidelines since 2006. 2 We also had access to a professional graphic designer and, in our writing process, prioritized clinical pearls and data most relevant for clinicians, shortened recommendations, and included more flowcharts. Third, we wanted to strengthen the evidence-based approach of the guidelines. To achieve this goal, we followed a “blank canvas” approach in which we searched the full literature, not solely focusing on studies published since the previous guidelines, set up a framework of systematic literature searches with the help of a medical librarian, and worked in close consultation with an expert methodologist to adhere to the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework. These modifications, combined with the results of new studies, form the basis for the changes in these updated guidelines as compared with their previous iteration.
With the exception of some subcategories, the quality of most evidence that supports the recommendations in this guideline remains low. Thus, besides the changes noted above, we now include the category of Good Practice Statements (GPSs) for recommendations that the writing committee deemed important but for which the lack of data does not allow for a formal certainty of evidence rating according to the GRADE framework. In addition, we also now highlight practical considerations for clinical management in separate figures and boxes. Finally, we communicate absolute rather than relative risks as much as possible.
These guidelines have been endorsed by:
American Association of Clinical Endocrinology American College of Obstetricians and Gynecologists Asia and Oceania Thyroid Association Endocrine Society European Board and College of Obstetrics and Gynaecology European Society of Endocrinology European Society of Human Reproduction and Embryology European Thyroid Association International Association of Endocrine Surgeons Iodine Global Network Latin American Thyroid Society Thyroid Federation International
B. Methods
The guidelines writing group consisted of 20 individuals: 18 physician-scientists with thyroid expertise representing seven international societies, 1 physician-methodologist, and 1 patient representative. The committee members were selected for their established expertise in thyroidology spanning the life stages of preconception, pregnancy, and postpartum. Each member belonged to up to two out of a total of six working groups within the different chapters in this guideline (one working group for each of the Sections from C to I, with the exception of one combined working group for Sections D and H). The composition of the writing committee was also determined from multiple collateral relationships that the co-chairs and the ATA had developed with 10 international scientific societies representing key stakeholders in thyroidology, general endocrinology, obstetrics and gynecology, and reproductive endocrinology, from which representatives were invited to serve. The chairs of the guideline committee were Tim Korevaar and Angela Leung (ATA), with the ATA represented by Erik Alexander, Chrysoula Dosiou, Sun Lee, Spyridoula Maraka, Kara Meister, Lilah Morris-Wiseman, Caroline Nguyen, and Zhongyan Shan. The Latin American Thyroid Society was represented by Gabriela Brenta. The European Thyroid Association was represented by Sofie Bliddal. The Asia and Oceania Thyroid Association was represented by Haixia Guan. The Endocrine Society and the Iodine Global Network were represented by Elizabeth Pearce. The European Society of Endocrinology was represented by Kristien Boelaert. The American College of Obstetricians and Gynecologists was represented by Sarah Kilpatrick. The American Society for Reproductive Medicine was represented by Jennifer Eaton. The European Society of Human Reproduction and Embryology was represented by Rima Dhillon-Smith. Our patient representative and member of the Thyroid Federation International was Bente Julie Lasserre. Finally, these guidelines were also supported by Roger Chou, a methodologist.
Task force chairs were proposed by the ATA Board of Directors. Both Task Force Chairs and Members were selected for their expertise and evaluated for potential conflicts of interest (COI) by the ATA Guidelines and Statements Committee and the Board of Directors. Any potential financial competing interests were declared (see the Author Disclosure Statement), and, where appropriate, individuals were not involved in the final approval of recommendations for which a potential or perceived conflict was identified. Competing interests were re-evaluated annually by the Task Force chairs and members. The opinions expressed herein are those of the authors, and the Task Force had complete editorial independence from the ATA. Except for the methodology consultant (R.C.), who received consultant fees from ATA, no individual Task Force members received funding from the ATA or from industry for work on this statement.
To inform the key content of the guidelines, we distributed a needs assessment questionnaire to the ATA membership from February to March 2022, to solicit suggestions and affirm content deemed most timely to the research needs and current clinical practice of the field. Input was gathered from a total of 388 respondents from across the globe (Europe 33%, North America 31%, Asia 25%, South America 8%, Africa/Australia both 1%), mostly attending physicians (48%), clinical practitioners (90%) (composed of 40% endocrinologists, 26% obstetricians/gynecologists, 24% reproductive medicine specialists, and the remainder as primary care clinicians, surgeons, etc.). The respondents provided 15 proposed topics and 11 main outcomes of interest that were used to inform the overall outline of the guidelines, organized as 122 PICO (population, intervention, control, outcome) questions with corresponding inclusion and exclusion criteria for the selection of relevant literature. For each of the six working groups (topics represented by Sections C–I), we identified a set of the most clinically relevant outcomes utilizing input from the needs assessment questionnaire and priority voting by the working group members. We subsequently performed a series of systematic literature reviews together with the Erasmus University Medical Center Medical Library (Elise Krabbendam, Biomedical Information Specialist) in consultation with the committee’s methodologist (Roger Chou, MD; see supplemental material). We first performed an overarching systematic literature review (April 12, 2022, and again on February 1, 2024) that included all predefined exposures and outcomes mentioned in the PICO questions, with the aim of identifying randomized trials and meta-analyses only. We then selected the one to four most important PICO questions for each working group (based on group consensus) for a question-specific systematic literature review with the aim of identifying any relevant literature regardless of study type. Literature for the remaining questions was identified through individual literature searches following an online PubMed training course. The results of the included studies were then entered into a data extraction table that also included quality rating metrics (Supplementary Table S1). During the time between systematic literature searches and submission to the journal, additional relevant studies were added per the insights of the committee. For all systematic literature search outputs, studies eligible for inclusion were independently assessed for suitability by two committee members (title and abstract screening, full-text screening, and quality assessment for overarching search), and any disagreements were resolved by discussion with a co-chair (Supplementary Table S2). The publication process consisted of reviews by, and comments from, the ATA Guidelines and Statements Committee, ATA Board of Directors, the ATA membership at large, and the membership of endorsing societies before the article was submitted to Thyroid which then underwent peer review.
The methods and output were based on guidance provided in the GRADE series.1,2 After defining the key clinical questions and performing corresponding systematic literature searches to identify relevant literature, we created an overview of (average) effects on relevant outcomes and rated the quality of the evidence for each. The quality (certainty) of the evidence supporting each recommendation was classified as very low, low, moderate, or high using the GRADE approach, based on study design (randomized trials or nonrandomized studies) and the GRADE domains (limitations/risk of bias, inconsistency, imprecision, indirectness, and publication or reporting bias). The strength of each recommendation was defined as strong (text worded as “should”) or conditional (text worded as “may”) and was based on the quality of the evidence, the balance of desirable and undesirable outcomes, potential impact of individual values and preferences on decisions, and other factors (acceptability, feasibility, cost/resources, and equity). The meaning of a strong recommendation is that all reasonably informed persons (clinicians, policymakers, and patients) would desire the management in accordance with the recommendation. For a conditional recommendation, most persons would still act in accordance with the guideline, but a substantial number would not, for example, conditional on patient preferences. Where applicable, this is expanded upon in the general text. An alternative to graded recommendations was GPSs, which were reserved for situations for which direct evidence on benefits and harms was unavailable or lacking, but there was high certainty of benefit based on indirect evidence, and there was consensus that not following the GPS would be inconsistent with the standard of care. Operationally, a GPS is similar to a strong recommendation (i.e., should be followed in all or almost all situations). 3 Consensus was sought for all recommendations and reached unanimously for the vast majority of recommendations. 4 For the exceptions, we followed an informal consensus process as based on a predefined 75% approval rate from the committee members who were ATA members, with all dissensions summarized in Supplementary Table S3. It should be noted that the recommendations are general guidance and should be adapted for each individual patient scenario, based on local resources/expertise and shared decision-making between the patient, clinician, and other health care team members.
C. Thyroid Physiology and Thyroid Function Testing
Thyroid function tests are among the most frequently ordered laboratory tests in otherwise healthy women of reproductive age.5–7 Specifically for women planning pregnancy, pregnant women, or those who are postpartum, there is generally a lower threshold to perform thyroid function testing. This is partly because, during these specific life phases, normal symptomatology can overlap with that of thyroid disease, while simultaneously, there is a peak in the prevalence of common thyroid disorders (such as Graves’ disease and thyroiditis). Furthermore, most health care practitioners are aware that overt thyroid disease is associated with adverse fertility and pregnancy outcomes. Due to an increased testing frequency, mild thyroid function test abnormalities are commonly identified in women of reproductive age. It remains difficult to distinguish whether these represent early-stage thyroid disease or nonpathogenic thyroid function test abnormalities, especially because of changes in thyroid physiology and an increase in analytical variations around ovarian stimulation in assisted reproductive technology (ART), pregnancy, and postpartum. Therefore, thyroid function testing strategies and interpretation preconception, in pregnancy, and the postpartum period should anticipate the physiological and analytical alterations of thyroid function parameters to optimize clinical care.
Thyroid physiology before, during, and after pregnancy
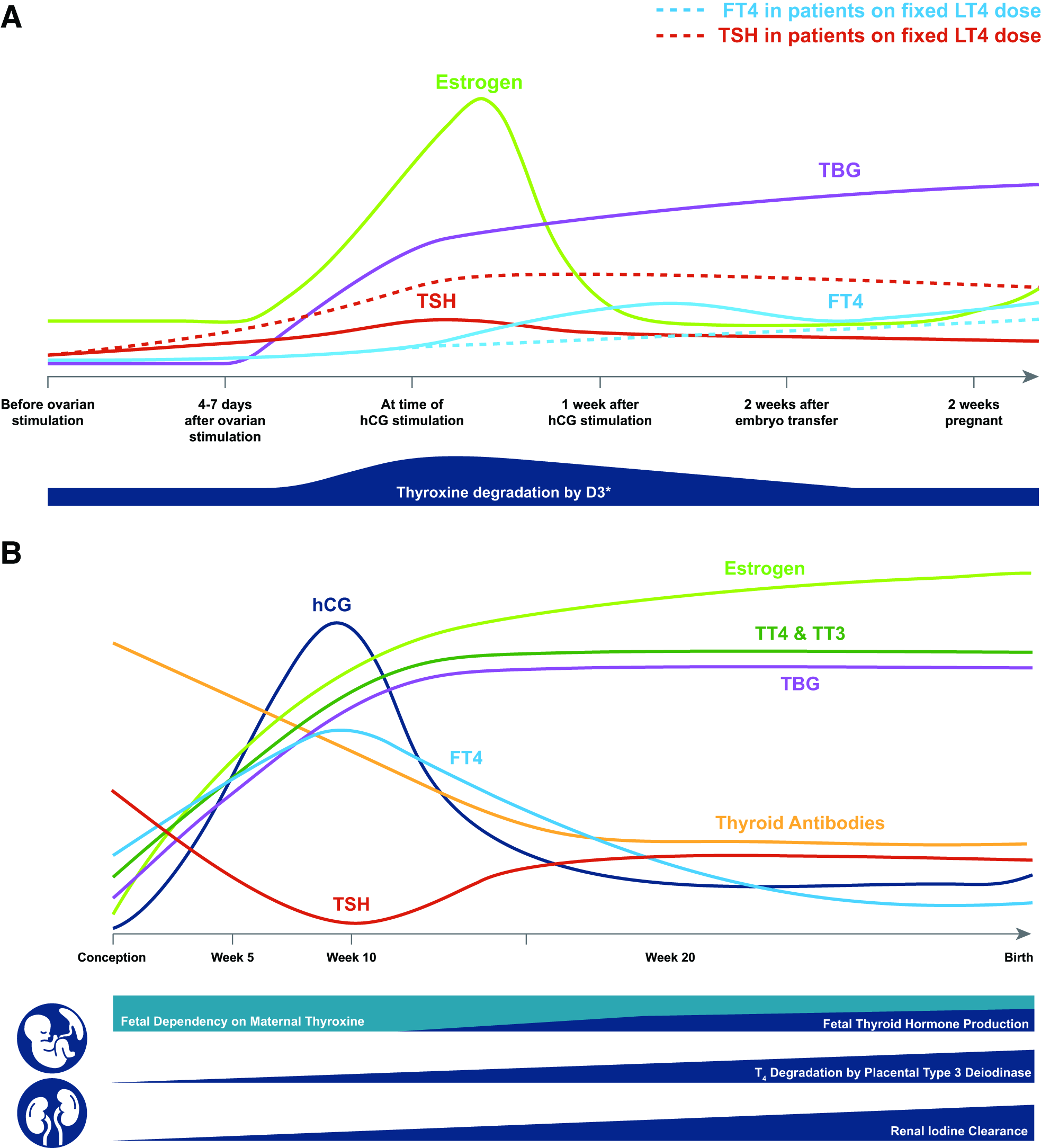
Thyroid parameters are not meaningfully impacted during a normal menstrual cycle. During ovarian stimulation for fertility treatment, the increase in estrogens causes an increase in type 3 deiodinase activity and thyroxine (T4)-binding globulin (TBG) concentrations which necessitates increased thyroid hormone production and causes a slight rise in thyrotropin (TSH) concentrations (Fig. 1A).8–11 Pregnancy itself is also associated with changes in thyroid physiology that make the interpretation of thyroid function tests different in pregnant compared with nonpregnant individuals (Fig. 1B). For example, TBG increases from week 7 of gestation to reach a peak by approximately week 16 and stabilizes thereafter, 12 and logically, total thyroid hormone concentrations (T4 and triiodothyronine [T3]) follow this same pattern. As pregnancy progresses, there is an increase in the transfer of maternal T4 to the fetal compartment, an increase in T4 degradation by type 3 deiodinase expressed in the placenta, and an increase in renal iodine excretion. Furthermore, through its affinity for the TSH receptor, human chorionic gonadotropin (hCG) stimulates thyroid hormone production with peak stimulatory effects around the end of the first trimester. 10 The healthy thyroid system adapts to these alterations through changes in thyroid hormone production, iodine uptake, and regulation of the hypothalamic–pituitary–thyroid axis.8–10 The net effect of all physiological changes is a slight transient increase in fT4 and a decrease in TSH that is most pronounced at the end of the first trimester. Thus, in normal physiology, a TSH below 0.4 mU/L occurs frequently.13,14 Furthermore, the immune tolerance of pregnancy, necessary to tolerate the allogeneic fetus, is associated with a decrease in thyroid antibody concentrations as gestation progresses. This explains why Graves’ disease can become quiescent during pregnancy and why thyroperoxidase antibody (TPOAb) positivity is less common in the third trimester than preconception. 15 Nevertheless, from 28 weeks onward, there is a considerable increase in active transplacental IgG transport, and cord blood concentrations can ultimately increase to those of the mother.16–18 The subsequent immune system rebound that occurs postpartum is a precipitating factor for postpartum thyroiditis (PPT) and de novo or relapsed Graves’ disease. 15
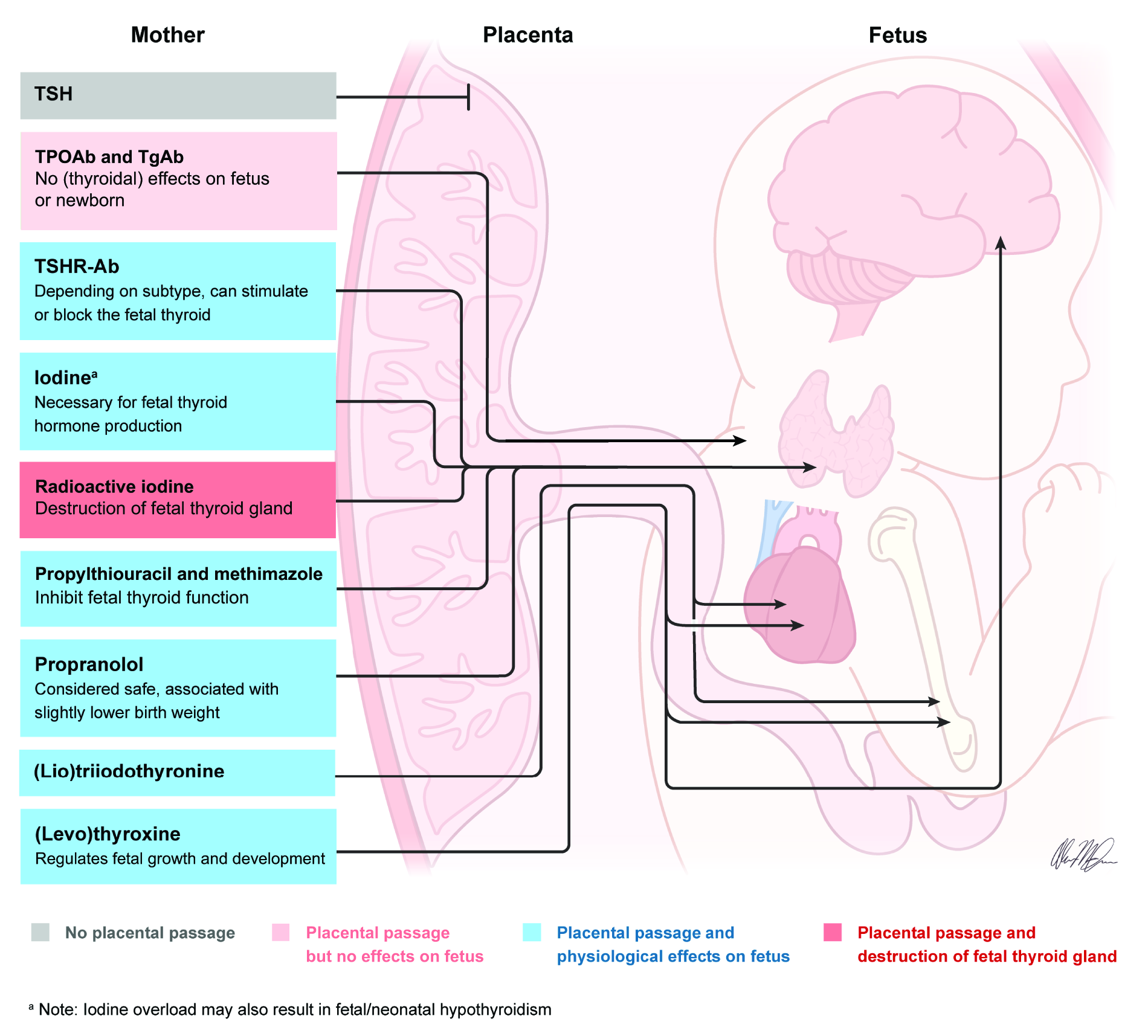
Transplacental passage of thyroid parameters and drugs. Maternal TSHR-Ab, iodine, radioactive iodine, the antithyroid drugs (propylthiouracil and methimazole), propanolol, and the thyroid hormones [(lio)thyronine and (levo)thyroxine] all traverse the placenta and have the potential to induce direct effects to the fetus. Maternal TPOAb and TgAb can also traverse the placenta but do not affect the fetus. Maternal TSH does not cross the placenta. TPOAb, thyroperoxidase antibody; TgAb, thyroglobulin antibody; TSHR-Ab, thyrotropin receptor antibody.
In specific subgroups, physiological processes may have a different effect on clinical parameters. For example, in women with hypothyroidism using levothyroxine (LT4) and who are undergoing ovarian stimulation, the increase in TBG caused by high estrogen concentrations can cause a clinically relevant increase in TSH (mean: +1.50 mU/L) that persists into pregnancy and may necessitate an earlier or larger LT4 dose increase as compared with women with hypothyroidism who conceive naturally. 19 Another example is twin pregnancies, in which there is a higher hCG concentration as compared with singleton pregnancies, causing a greater stimulation of thyroid hormone production, resulting in lower TSH and higher fT4 concentrations.20,21 Yet, for a twin pregnancy in a hypothyroid woman using LT4 (in which no or very little thyroidal response to hCG stimulation can be anticipated), LT4 consumptive factors have a larger impact on thyroid physiology (i.e., larger volume expansion, larger fetal T4 transfer, higher type 3 deiodinase activity due to higher estradiol and a larger placenta) which could necessitate a larger LT4 dose increase as compared with a singleton pregnancy. A final example is TPOAb-positive women, who are known to have a slightly higher mean TSH and a higher risk of overt hypothyroidism, partly because of an impaired thyroidal response to hCG stimulation during early pregnancy.22–25
Knowledge regarding placental transfer of thyroidal factors is key to understanding normal physiology and pathophysiology, as well as the risks and benefits of various treatment modalities. As shown in Figure 2, thyroid hormones, thyroid antibodies, iodine, and antithyroid drugs (ATDs) all traverse the placental barrier.
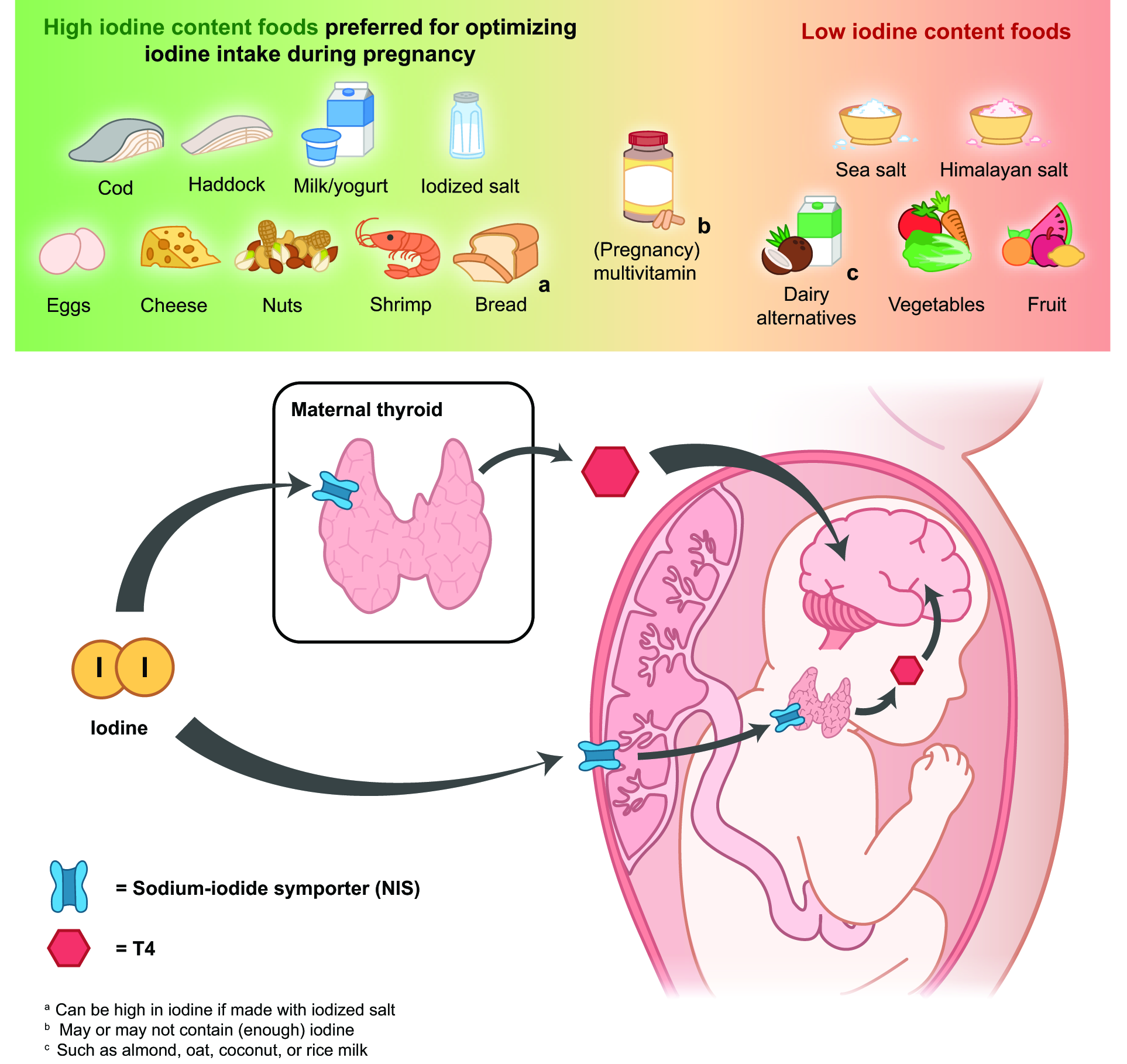
Iodine availability during pregnancy. Examples of supplements and foods with high and low iodine content are shown. Iodine is taken up by the NIS at the basolateral membrane of the thyroid follicular cell in both the mother and fetus, as needed for thyroid hormone production, for which requirements are higher during pregnancy. NIS, sodium/iodide symporter.
Analytical considerations
Pregnancy-specific physiology can also affect thyroid function assay performance, a basic understanding of which is beneficial to health care practitioners. In addition to the aforementioned physiological changes, other changes, such as an increase in free fatty acids and a decrease in albumin concentrations,26–28 may influence the performance of fT4 immunoassays. It is known that these could result in falsely lower serum fT4 concentrations in a method-specific manner, especially during the second half of pregnancy.13,29–31 Recent data have renewed the favorability of the use of fT4 measurements analyzed via analog immunological methods early in pregnancy as compared with alternative options. Most notably, fT4 measured via analog methodology better correlates with TSH in the first trimester than total T4, 32 and fT4 has also been associated with maternal and child outcomes, a finding which has not been demonstrated for other test methodologies.32–35 These findings suggest fT4 analog measurement is an appropriate marker of thyroid function in the first half of pregnancy. 36 The use of a laboratory and trimester-specific fT4 reference interval would likely eliminate any pregnancy-specific analytical changes 37 and is thus the preferred method for fT4 interpretation during pregnancy. However, such reference intervals cannot be effectively transferred amongst differing manufacturers or testing platforms and may not be widely available.
When pregnancy and trimester-specific reference intervals for fT4 are unavailable, alternative strategies for interpreting or assessing thyroid hormone availability during pregnancy can be considered, taking into account the advantages and disadvantages of each strategy. One option would be to use nonpregnancy reference intervals for fT4, taking into account that this will likely lead to small differences in diagnosis, including more diagnoses of overt hypothyroidism and isolated hypothyroxinemia, especially after the first trimester. 38 Another option is to use direct methods for measurement of fT4, such as equilibrium dialysis or ultrafiltration combined with liquid chromatography/tandem mass spectrometry. However, direct methods are not free from technical problems and are significantly more laborious, time-consuming, expensive, and less widely available. Comparisons of direct methods with commonly used immunoassays have yielded heterogeneous results.30,37,39,40 Another option is to use the fT4 index, which is defined as the total T4 adjusted for protein binding using the thyroid hormone binding ratio. 41 This formula assesses whether the amount of total T4 present in serum can be accounted for by the amount of binding protein present. The fT4 index has limited availability, and gestational reference intervals are typically not established. Furthermore, the calculations may be insensitive to the dynamic changes of gestational thyroid function. 41 Another option that could be considered is to use the total T4, adjusting for the increase expected by the TBG rise. Considering the changes of serum total T4 through pregnancy, the reference interval for total T4 can be adjusted by increasing the nonpregnant reference limits by 5% per week, beginning with week 7, and plateauing at a 50% increase from week 16 of pregnancy onward. 12
Importantly, maternal TSH remains the best marker of maternal thyroid status during pregnancy. TSH measurement by third generation immunoassays is not affected by the pregnancy-associated binding protein changes. However, different immunoassays may give different TSH results as is well-established in nonpregnant populations. 42 Therefore, when there is concern over the correct interpretation of fT4 concentrations, the TSH result should be prioritized during evaluation. The general principle that the intraindividual thyroid function test variation is smaller than that between individuals also applies in pregnancy.43,44 Therefore, it is optimal to use the same TSH and/or fT4 assay, or an alternative described above, for follow-up over the course of pregnancy.
Except for the characterization of hyperthyroidism, the relevance of measuring serum free or total T3 in pregnancy is generally low, as there is no clear association between these biochemical markers and adverse pregnancy or child outcomes other than gestational diabetes mellitus.45–47 In addition, maternal free or total T3 concentrations may not reflect T3 status in the fetal brain. 48 When T3 estimates are needed, it is reasonable to apply the same considerations as described above for free and total T4 estimates for interpretation. Considerations for free and total T3 measurements in hyperthyroidism during pregnancy are discussed in Box 5.
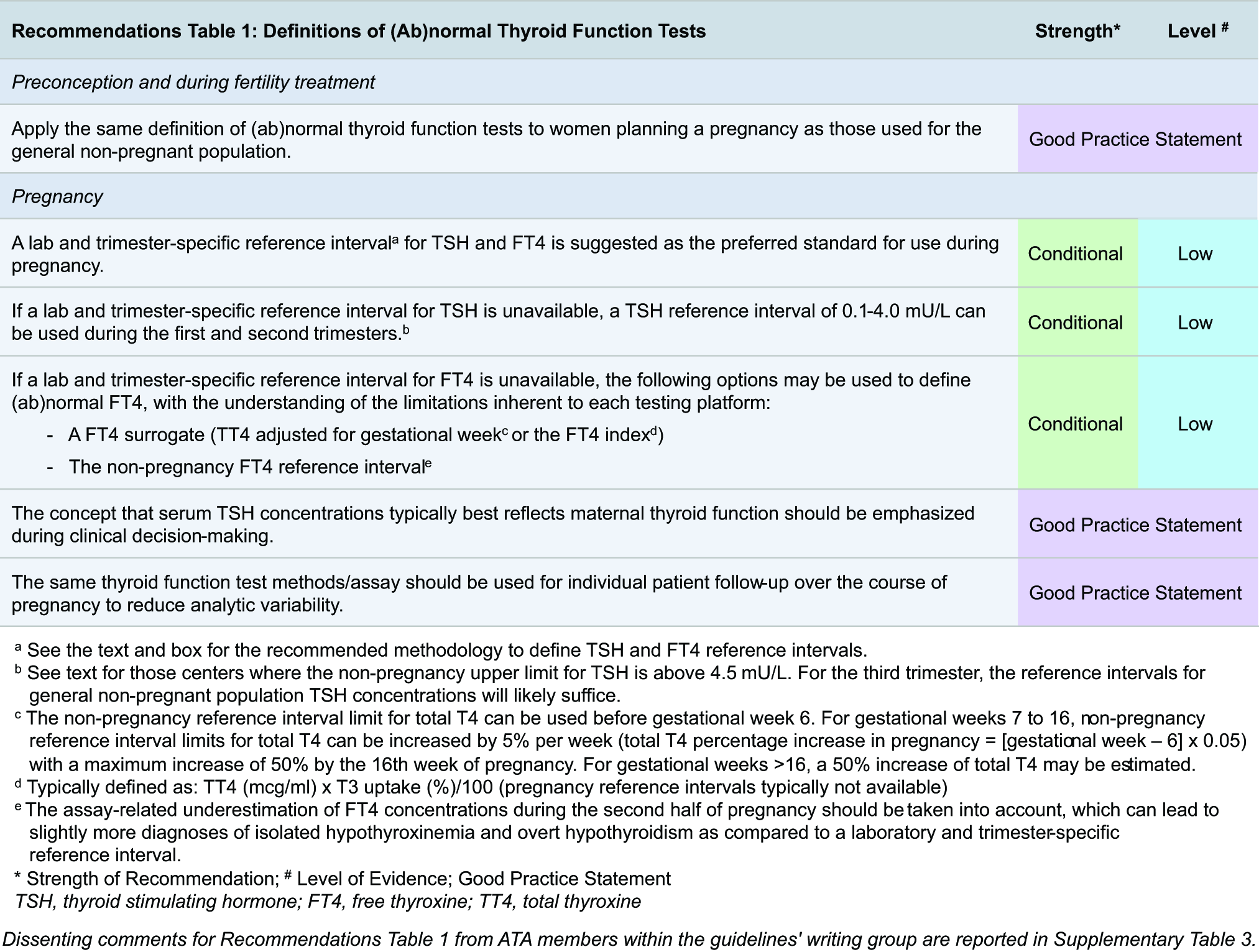
Definition of (ab)normal thyroid function tests
For women planning pregnancy or those who are postpartum, thyroid dysfunction is defined according to local reference intervals for TSH and fT4 used for the general population. During pregnancy, physiological and analytical alterations can be accounted for through the use of laboratory and trimester-specific TSH and fT4 reference intervals. Recommendations on the definition of an abnormal TSH and fT4 in pregnancy (Box 1) should be used to guide clinical practice and cannot replace clinical evaluation, risk assessment, and patient involvement through shared decision-making. Gestational TSH and (f)T4 measurements should be interpreted with the understanding of the limitations inherent to each reference interval. There remain considerable intra-assay and intralaboratory differences in TSH and, especially, fT4 measurements, despite (local) standardization efforts. 49 Laboratory and trimester-specific reference intervals are a statistical estimation of normal variation within a population. These do not incorporate the risk of adverse outcomes but remain the preferred method until risk-based intervals become available. The committee acknowledges, however, the fact that trimester- and laboratory-specific reference intervals are currently unavailable in the majority of hospitals worldwide. In such cases, clinicians can be guided by the knowledge of the physiological changes that occur in healthy pregnant women with a decrease in TSH, especially in the first trimester. The 2017 ATA guidelines, after reviewing the significant geographic and ethnic diversity of TSH concentrations in pregnancy, recommended the following TSH cutoffs in the absence of laboratory and trimester-specific TSH reference intervals: reduction of the lower reference range by 0.4 mU/L and the upper reference range by 0.5 mU/L in the first trimester, followed by a gradual return to the nonpregnant range in the subsequent trimesters. Based on expert opinion and an extrapolation of average values from reference interval studies, this committee agrees that this is acceptable and would correspond, for the typical patient, to a first-trimester reference interval of 0.1–4.0 mU/L.38,50 An upper limit of 4.0 mU/L is about 0.5 mU/L lower than the nonpregnancy upper TSH limit for most assays. It would be reasonable for centers where the nonpregnancy upper limit is well above 4.5 mU/L to deduct 0.5 mU/L from the upper TSH limit instead.38,50 Owing to the large interassay differences in absolute fT4 concentrations, recommendations for absolute fT4 reference intervals are not feasible, but considerations for different alternatives are discussed above.
The abovementioned alternative strategies (e.g., a fixed TSH upper limit of 4.0 mU/L or deducting 0.5 mU/L from the nonpregnancy upper limit) were proposed with the aim to approximate laboratory- and trimester-specific TSH reference intervals in pregnancy. 1 However, recent studies have shown that these alternatives tend to misclassify a substantial number of patients. For example, for overt hypothyroidism in the first trimester, use of a fixed TSH upper limit of 4.0 mU/L would identify 46.1% of all women with overt hypothyroidism but identify the remainder as either euthyroid (11.9%), subclinically hypothyroid (36.8%), or with isolated hypothyroxinemia (5.2%), as compared with a laboratory with trimester-specific reference intervals. 38 However, it is still uncertain if this misclassification will cause clinical harm. These numbers are similar when the subtraction approach is used (46.1%, 13.5%, 35.2% and 5.2%, respectively). 38 Furthermore, recent data on the natural course of thyroid function test abnormalities during pregnancy suggest that mild cases (slightly increased TSH) of overt and subclinical hypothyroidism may be transient in approximately half of all cases.51,52 This may suggest that future disease definitions and/or treatment indications could be improved by accounting for the persistent of disease upon remeasurement.
Thyroid function testing indications

Thyroid function tests are some of the most frequently ordered laboratory tests. In women without known thyroid disease, infertility, or recurrent miscarriage, the indications for thyroid function testing for those planning pregnancy or those who are postpartum are similar as for the general population. During pregnancy, defining a thyroid function testing indication is complicated by the concept that thyroid disease symptoms overlap with those related to a normal pregnancy and also because mild forms of thyroid disease can present without symptoms. Because thyroid hormone demands are increased in pregnancy, risk factors for maternal thyroid dysfunction can be specific to gestation. Furthermore, the risk of thyroid disease according to general (nonpregnancy) risk factors may be larger during pregnancy as compared with a nonpregnant state. Therefore, we recommend that risk factors for thyroid disease during pregnancy (Table 1) are used to determine the indication for thyroid function testing during pregnancy.
Risk Factors for Thyroid Dysfunction During Pregnancy
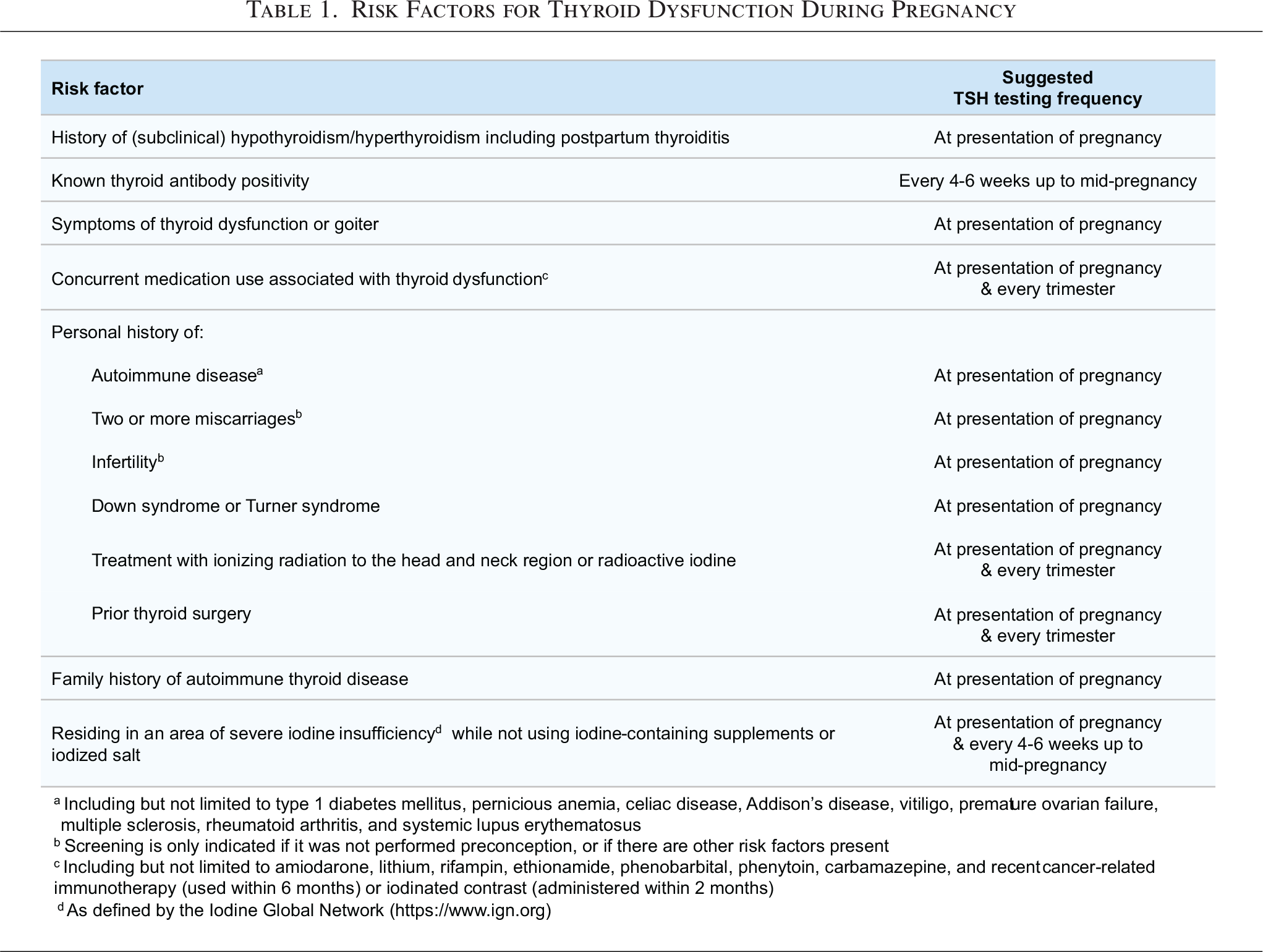
Various studies have shown that risk factors recommended in the previous version of these guidelines would lead to screening of 55–78% of all pregnant women, while detection rates varied between 75% and 85% for overt hypothyroidism and between 54% and 60% for subclinical hypothyroidism.53–56 In an effort to optimize these numbers, we commissioned two studies to validate previous risk factors 57 and to identify new risk factors for thyroid function test abnormalities and TPOAb positivity. 58 For the risk factors we recommend, the selection of some was supported by good volume and high-quality data (thyroid antibody positivity), while the selection of other risk factors was based on reasonable extrapolation of data from nonpregnant populations (e.g., medication use, Down/Turner syndrome, prior radiation/thyroid surgery, history of autoimmune disease, iodine deficiency, family history of autoimmune thyroid disease) or expert opinion (remainder). For women with a history of infertility or recurrent miscarriages, we recommend thyroid function testing if this has not already been performed preconception, unless there are other risk factors present, recognizing that women with such history are frequently tested before conceiving. Three specific risk factors were considered but not added as a thyroid function testing indication. A past medical history of a single miscarriage is common and often attributable to nonthyroidal risk factors, and current data are insufficient to consider it as a risk factor for thyroid disease during pregnancy. While BMI and age were recognized as risk factors for thyroid disease during pregnancy (for overt hypothyroidism/isolated hypothyroxinemia and subclinical hypothyroidism, respectively), the absolute risk differences were small and identification of an objective dichotomous cutoff for these variables remains difficult. 57
It is important to note that the risk factors that are considered an indication for thyroid function testing during pregnancy are not exhaustive. Furthermore, the use of this set of risk factors will not enable the identification of all women with thyroid dysfunction, specifically overt hypothyroidism. Therefore, these risk factors should be used to supplement general clinical reasoning. Similar to the US Preventive Services Task Force recommendations for the general population, 59 there is insufficient evidence to recommend routine thyroid function testing (universal screening) in women planning pregnancy, in pregnant women, or in women during the postpartum period. Detailed overviews of the pros and cons of routine thyroid function testing are described elsewhere.60,61
D. Iodine
Iodine is a trace micronutrient required for thyroid hormone production. There are approximately 15–20 mg of iodine in the human body under normal conditions, with over 70% of this contained in the thyroid gland. 62 Adequate iodine availability is particularly important in pregnancy, when thyroid hormone requirements are higher, renal iodine excretion is increased, and there is additional demand for iodine from the developing fetus (Figs. 1 and 2). 63 Iodine intake should ideally be optimized preconception. For this topic, there is abundant low-to-moderate quality evidence but only sparse high-quality evidence to support recommendations. The committee has assessed all meta-analyses and randomized trials to form recommendations for this subsection, which were often supported by data from single-center observational studies.
Epidemiology and physiology
In 2023, there were 18 countries with insufficient dietary iodine intake out of 127 countries worldwide with available nationally representative data, corresponding to approximately one-third of the world’s population64,65; the most current global iodine status data are available from the Iodine Global Network. 65 In the United States, data from the National Health and Nutrition Examination surveys show that a substantial portion of pregnant women are iodine insufficient, with median UICs as a population biomarker for iodine status declining since the early 2000s.66–69 There is strong evidence that severe maternal iodine deficiency in pregnancy and its effect on thyroid status are associated with adverse obstetrical outcomes, as well as increased risks of maternal and neonatal hypothyroidism, perinatal and infant mortality, low child intelligence quotient (IQ), and child neurocognitive impairment.70–74 Data on the adverse effects of mild-to-moderate iodine deficiency in pregnant women are less clear. Mild-to-moderate iodine deficiency has not been associated with adverse obstetric outcomes.73,75,76 Observational data show associations between mild/moderate iodine deficiency and impaired fetal brain development.77,78 Children of pregnant women with mild-to-moderate iodine deficiency before 14 weeks’ gestation had lower IQ scores in a dose-dependent manner. 79 Adequately powered randomized controlled trials examining child neurodevelopment have not been performed in mild-to-moderate iodine-deficient pregnant women,80,81 but it is biologically plausible that neurodevelopmental effects observed in milder forms of iodine deficiency can be extrapolated from the literature on severe iodine deficiency. However, in small randomized controlled trials, use of iodine supplementation for women with mild-to-moderate iodine deficiency has not resulted in clinically relevant alterations in maternal and neonatal thyroid function.80–85 The sodium/iodide symporter (NIS) plays a crucial role in mediating iodide uptake required not only for thyroid hormone synthesis in both the maternal and fetal thyroid gland but also for the placental transfer of iodide. As such, some of the nutritional effects associated with maternal iodine deficiency could also result in fetal iodine deficiency (Fig. 3).
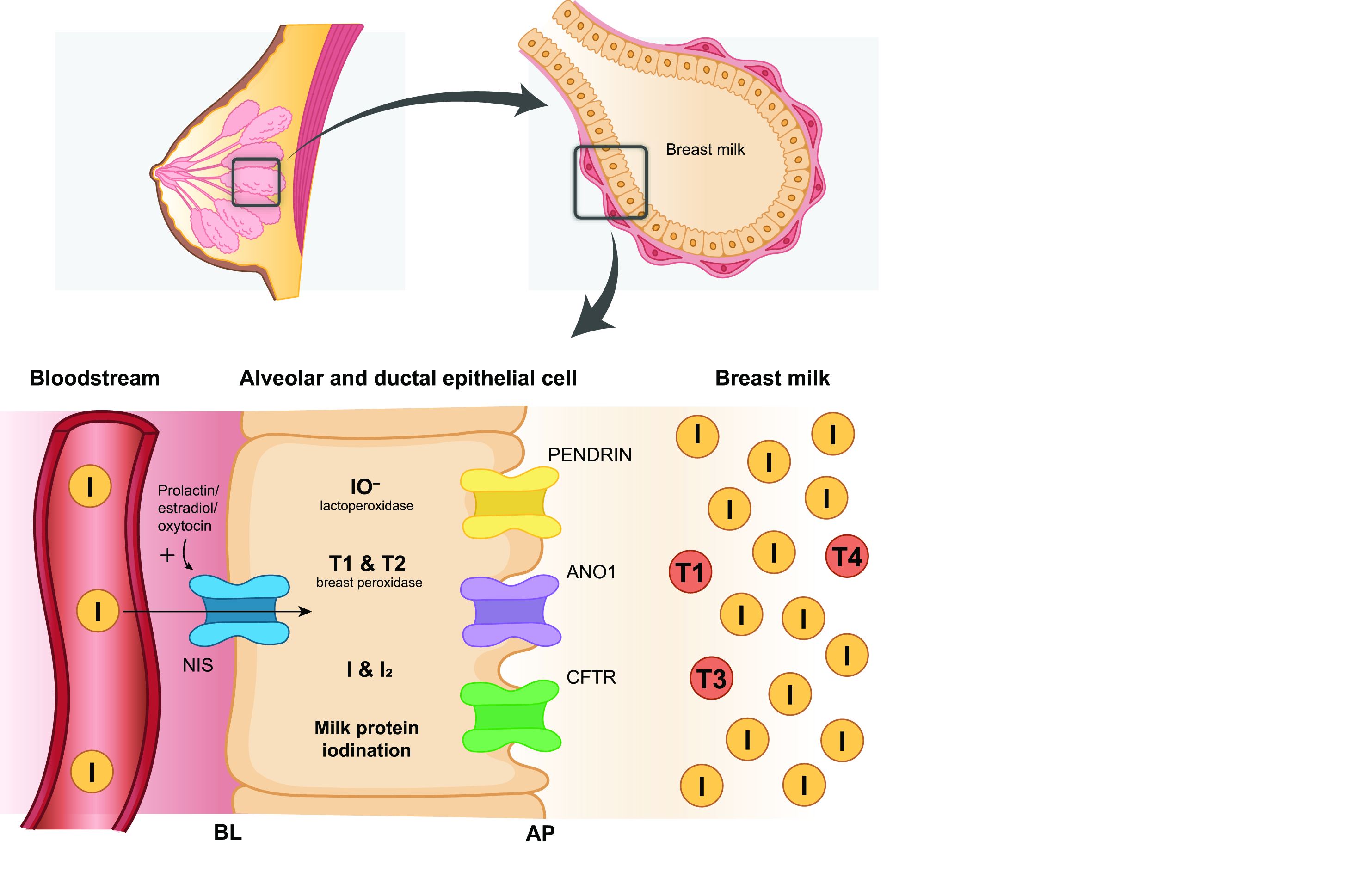
Thyroid hormone and iodine content in breastmilk. Although the World Health Organization suggests a median UIC threshold of >100 mcg/L to indicate adequate iodine nutrition in lactating women, UIC alone may not fully reflect the iodine status of this group, as UIC tends to be lower in lactating women compared with nonlactating women, since iodine is excreted both in urine and breast milk. NIS and Pendrin are expressed in lactating mammary cells and facilitate the uptake of iodine from maternal circulation into breastmilk. Iodide transport across the apical epithelial membrane also occurs through transporters that include ANO1 and CFTR. Limited data suggest that iodine occurs in various forms in breastmilk, mostly iodide (∼77%) and other organic materials like iodinated milk proteins (∼11%). It also occurs in thyroid hormones, predominantly T1 (∼7–25%) but very little T4 or T3 (∼1%; no data on T2). 354 The maximum methimazole/carbimazole content of breast milk is 0.1–0.2% of the maternal dose, and for PTU, this is <0.1%.342,343 AP, apical; ANO1, anoctamin-1; BL, basolateral; CFTR, cystic fibrosis transmembrane conductance regulator; PTU, propylthiouracil; T3, triiodothyronine; T4, thyroxine; UIC, urinary iodine concentration.
Clinical presentation and evaluation
The clinical presentation of iodine deficiency would be reflected as hypothyroidism and its sequelae. It is important to note that there are no validated biomarkers to assess chronic iodine intake on the individual level. Instead, iodine status is measured across populations and is usually assessed by median spot or 24-hour UICs; median UIC values between 100 and 199 mcg/L indicate population iodine sufficiency among nonlactating, nonpregnant women, while median UICs between 150 and 249 mcg/L indicate optimal iodine nutrition in pregnant populations.
Other available measures for assessing population iodine status include serum or whole-blood thyroglobulin concentrations and neonatal TSH concentrations. 86 Serum or whole-blood thyroglobulin values have been proposed for assessing iodine status of populations of pregnant women, 87 but there is currently no consensus on their threshold values, and poor harmonization between assays further limit their utility.86,88 Neonatal TSH concentrations may be available in regions where these measurements are used to screen for congenital hypothyroidism and may be higher in iodine-deficient regions. The prevalence of neonatal TSH concentrations greater than 5.0 mU/L should be <3% in iodine-sufficient regions. 89 However, the timing of assessing neonatal TSH relative to the neonatal TSH surge, as well as the use of iodophor cleansers at the time of delivery, may limit the utility of neonatal TSH as a marker for population iodine nutrition. Finally, there is a substantial degree of intraindividual variation in the ability of the thyroid gland to adapt to insufficient iodine availability, even in those living in severely iodine-deficient regions. Therefore, serum thyroid function tests are not considered sensitive indicators of population iodine status in most groups, including pregnant and postpartum women. 90
Although the World Health Organization suggests a median UIC threshold of >100 mcg/L to indicate adequate iodine nutrition in lactating women, UIC alone may not fully reflect the iodine status of this group, as UIC tends to be lower in lactating women compared with nonlactating women, since iodine is excreted both in urine and breast milk (Fig. 4). 91 Thus, spot breast milk iodine concentrations have also been considered as a biomarker of iodine status in lactation. Breast milk iodine content (BMIC) reflects recent iodine intake, but there is intraindividual variability. Cross-sectional studies have suggested that a median BMIC range of 100–200 mcg/L is considered adequate in lactating women 92 ; however, no formal minimal threshold has been established. As such, the optimal metric for assessing the iodine status in populations of lactating women is currently unclear. 92
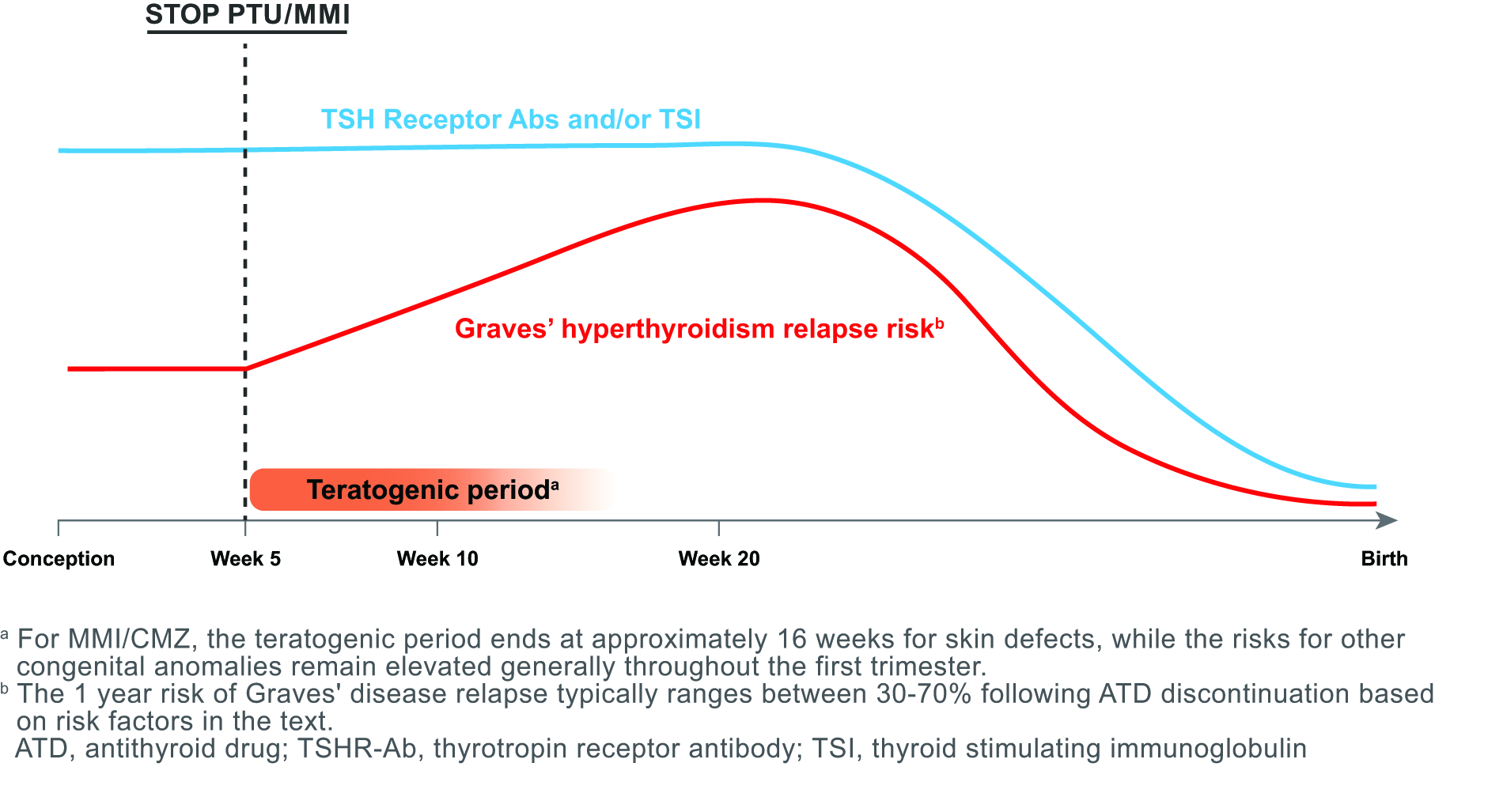
Strategy for ATD discontinuation upon pregnancy confirmation. Factors important for considering when maternal ATD may be successfully discontinued in pregnancy include the duration and dose of ATD use, maternal TSH concentration, signs of Graves’ disease burden (i.e., thyroid eye disease, goiter), and the maternal TRAb and/or TSI concentration. The 1-year risk of Graves’ disease relapse typically ranges between 30% and 70% following ATD discontinuation based on these risk factors.
Treatment and management
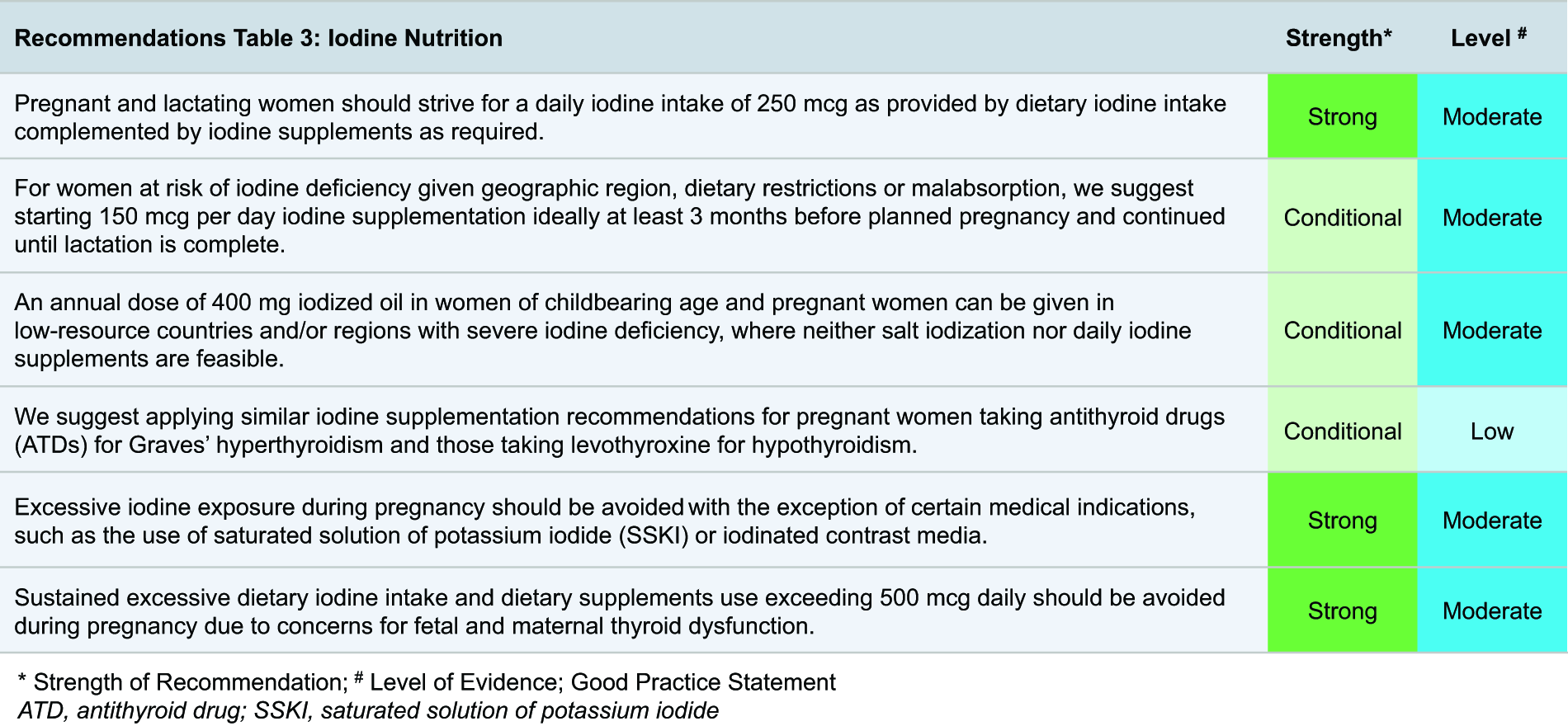
Pregnant and lactating women are recommended to receive a total of 250 mcg iodine daily as provided by iodine supplements and/or dietary iodine intake. 91 Ensuring adequate iodine status as a public health measure is best achieved when iodine supplementation is advised for women in general during these life stages, not just those residing in at-risk areas. However, strategies for optimal iodine intake vary by geographic region. Iodine supplementation of 150 mcg/day should be advised in all women preconception, in pregnancy, and lactation (unless there is high iodine intake evident due to traditional dietary habits) and ideally beginning at least 3 months before conception. Women may need higher amounts of supplementation if at increased risk for iodine deficiency based on information about population iodine status in the region or dietary patterns in the woman (Fig. 3; e.g., not using iodized salt, not ingesting dairy foods, following a vegan diet). 93 The supplemental iodine doses reported in the literature to assess their effects on obstetric and offspring outcomes have ranged from 50 to 300 mcg/day, in line with the range of region-specific background dietary iodine intakes of the various populations studied.72,80,81 In low-resource countries and regions where neither salt iodization nor daily iodine supplements are feasible, the most vulnerable populations for iodine deficiency can be protected by providing an annual dose of 400 mg iodized oil to pregnant women and women of childbearing age.91,94 It should be noted that this should not be used as a long-term strategy or in regions where other options for adequate iodine nutrition are available.
Finally, excess iodine exposure during pregnancy should also be avoided, except in preparation for the surgical treatment of Graves’ disease (when saturated solution of potassium iodide may be used) and when potassium iodide is used as an alternative treatment for Graves’ disease during pregnancy (in which potassium iodide of up to 50 mg/day has been described).95,96 Clinicians should carefully weigh the risks and benefits when ordering medications or diagnostic tests that will result in high iodine exposure (e.g., amiodarone or iodinated contrast media) during pregnancy. Amiodarone is currently classified by the US Food and Drug Administration to pose possible human fetal risk, although it is recognized that its potential benefits may warrant use of the drug in pregnant women. In particular, sustained excessive dietary iodine intake and dietary supplements use exceeding 500 mcg daily should be avoided during pregnancy, due to concerns for fetal and maternal thyroid dysfunction. 97
E. Thyroid Dysfunction and Infertility
The approach to assessment and management of thyroid disease in women with infertility and/or recurrent miscarriages is largely similar to that for the general population. However, this group may benefit from a more proactive approach to diagnosis and treatment. There are notable differences between women with infertility (or those planning fertility treatment) and the general population, including several key distinctions: (1) the window of opportunity to conceive is often shorter for women with infertility, (2) there are time constraints imposed by fertility treatments, and (3) fertility treatments are associated with increased thyroid hormone demand. Optimal thyroid care requires timely diagnosis following the first presentation of a thyroid function test abnormality, as well as anticipation of pregnancy-specific physiological alterations in thyroid function, disease, and treatment. For this topic, there is abundant low-to-moderate quality evidence but only sparse high-quality evidence to support recommendations. The committee has assessed all meta-analyses and randomized trials to form recommendations for this subsection, which were often supported by data from single-center observational studies. Dependent on the availability of evidence, some recommendations specifically mention women with recurrent miscarriages if data were available. While the group of women with recurrent miscarriages was not specifically defined during the design of the methodology supporting this guideline, it is reasonable to also apply all other recommendations in this subsection to women with recurrent miscarriages.
Thyroid function testing and monitoring in infertility
It is important to emphasize that the definition of thyroid dysfunction in women with infertility or those undergoing fertility treatment is the same as that of the general population and thus should be defined according to local reference intervals that are used for the general population. There are two main arguments that support thyroid function testing in women with infertility or history of recurrent miscarriage. First, overt and subclinical hypothyroidism are part of their differential diagnosis (for infertility mainly, in a woman presenting with irregular menses). Second, it has been proposed that overt and subclinical hypothyroidism could be an indication for LT4 treatment in this specific subgroup, as fertility outcomes may be improved and progression from subclinical to overt hypothyroidism can be avoided.
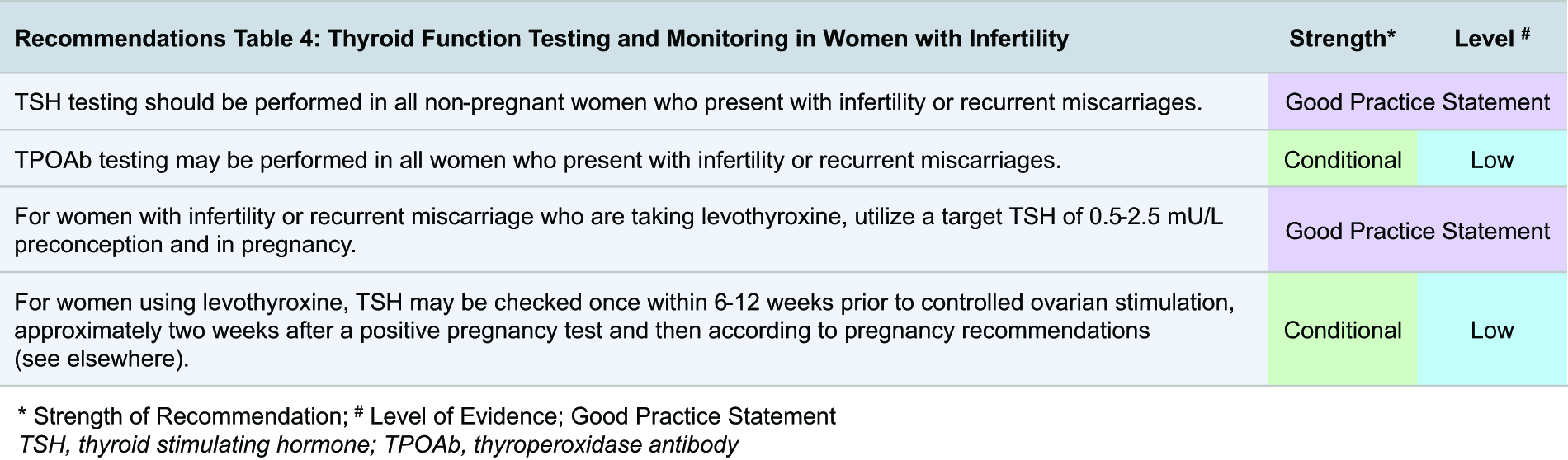
There is value in determining TPOAb status in women with infertility or history of recurrent miscarriage. Approximately 7–9% of euthyroid TPOAb-positive women develop overt or subclinical hypothyroidism during follow-up, mostly in the one year before conception but also during gestation.98–100 Even though LT4 treatment is not indicated for euthyroid TPOAb positivity, TPOAb measurement as part of thyroid function testing is valuable for identifying those more likely to develop hypothyroidism and, therefore, more likely to require LT4 treatment in the near future. The TPOAb status also has some prognostic value for the risk of miscarriage, preterm birth, and PPT. The cost for implementation and a lack of a proven benefit of intervention are the primary arguments against routine TPOAb testing. In view of this, an individualized approach to TPOAb testing may be warranted, where women with a higher likelihood of having antibodies can be considered for testing. This may include women with high-normal TSH concentrations, history of recurrent miscarriages, other autoimmune diseases, or a first-degree relative with thyroid autoimmunity.24,101,102 Robust cost-effectiveness analyses are needed to determine the true cost implications of preconception routine thyroid antibody testing.
For any woman taking LT4 and planning pregnancy, a TSH between 0.5 and 2.5 mU/L is a reasonable treatment target. This strategy creates a margin of safety for maintaining a euthyroid state in anticipation of the increased thyroid hormone demand and LT4 dose adjustments that occur during ovarian stimulation and pregnancy. It is important to note that variations of preconception TSH concentrations within the reference interval do not affect fertility or pregnancy outcomes or the effectiveness of LT4 treatment to a clinically relevant extent.100,103–106
Overt hypothyroidism in infertility
Epidemiology and physiology
The prevalence of undiagnosed overt hypothyroidism in women with a history of infertility or recurrent miscarriages is approximately 0.2%, which is similar to that in women of childbearing age in the general population.101,107 The main risk factor for overt hypothyroidism is thyroid autoimmunity; around 70% of all women with overt hypothyroidism detected in the setting of the work-up for infertility or recurrent miscarriages are TPOAb positive. 101 Furthermore, hypothyroidism is more common in women with other autoimmune diseases. This is particularly relevant for autoimmune diseases that are part of multiple autoimmune endocrinopathies,38,108,109 and it can be beneficial to further investigate any sign of such abnormalities in anticipation of pregnancy. Greater age is also associated with a higher risk of overt hypothyroidism, and there are considerable regional and interpopulation (ethnicity-based) differences in the prevalence of hypothyroidism.38,107,109,110
Clinical presentation, evaluation, and management
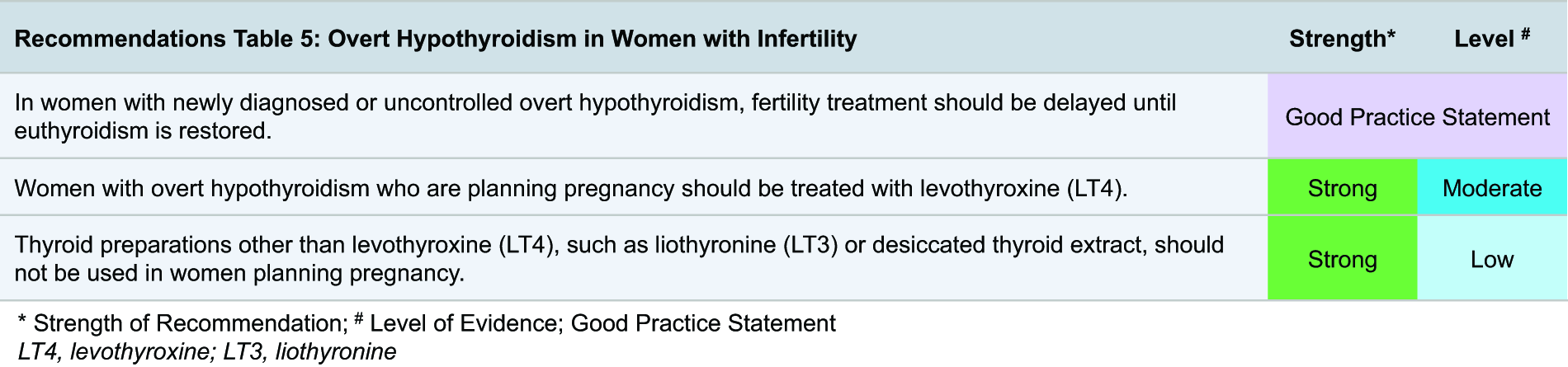
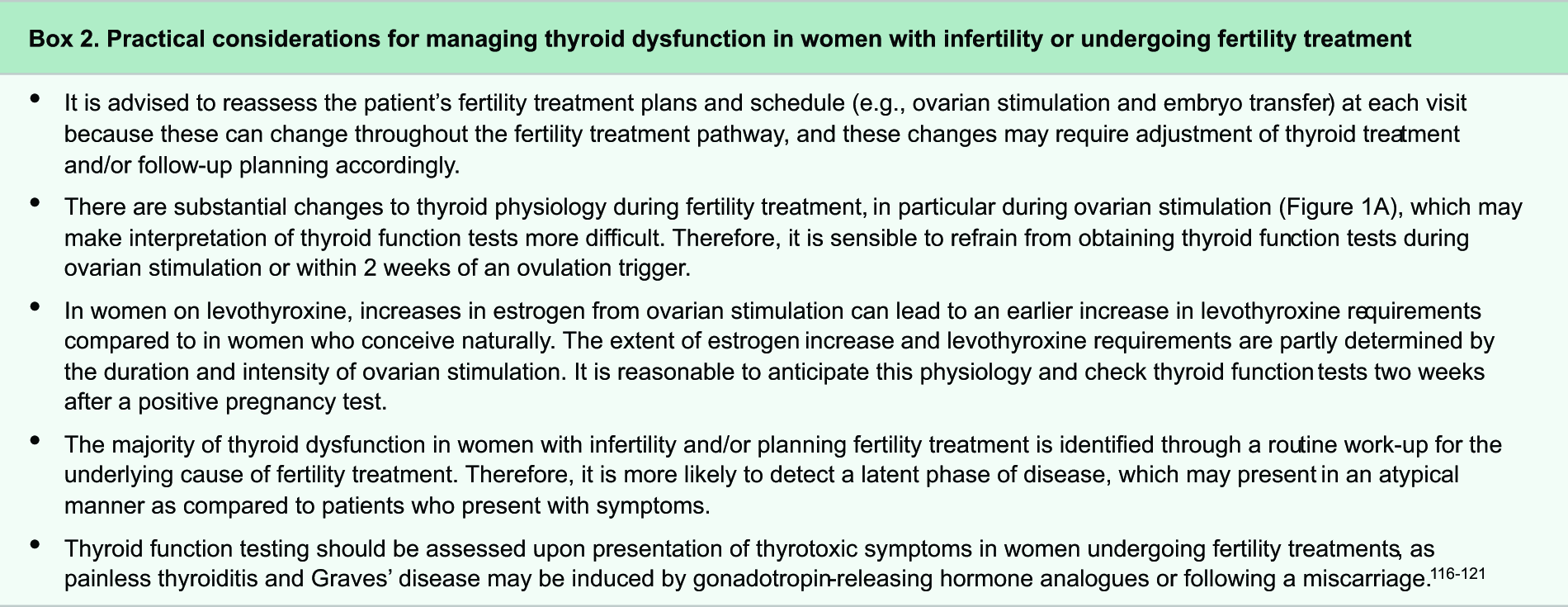
The evaluation and management of overt hypothyroidism in women with a history of infertility is the same as that of the general population, 111 although the clinical presentation may be more atypical (Box 2). Overt hypothyroidism is a well-established risk factor for infertility or recurrent miscarriages through a multifactorial pathogenesis that includes metabolic, endocrine, and menstrual disturbances. 9 Untreated overt hypothyroidism presents with menstrual disturbances in about 23% of cases (mainly as amenorrhea, hypomenorrhea, and menorrhagia), while hypothyroidism accounts for 2–3% of all causes of anovulation.112,113 Data on fertility outcomes in women with untreated hypothyroidism remain sparse as LT4 treatment is usually started without delay. More importantly, women with pre-existing hypothyroidism, who are euthyroid on LT4 treatment, have the same fertility outcomes as those without hypothyroidism.9,114,115 Assessing risk factors for iodine deficiency is helpful to determine an indication for iodine supplementation to prevent maternal and fetal hypothyroidism. Iodine supplementation is preferably started preconception (see Section D). In addition, checking TPOAb status is useful for etiological and prognostic purposes. Women using liothyronine or desiccated thyroid extract preparations should be recommended to switch to LT4 monotherapy before starting fertility treatment to avoid insufficient thyroid hormone availability for the fetal brain (see Section F).
Subclinical hypothyroidism in infertility
Epidemiology and physiology
The prevalence of undiagnosed subclinical hypothyroidism in women with infertility or recurrent miscarriages is approximately 2.4%, which is similar to that of women of childbearing age in the general population.101,120–123 The main risk factor for subclinical hypothyroidism is thyroid autoimmunity; about 40% of all women with subclinical hypothyroidism, detected in the setting of the diagnostic work-up for infertility or history of recurrent miscarriages, are TPOAb positive, and this rises to 80% for those with a TSH >10 mU/L.101,108 Other risk factors include obesity, and considerable regional and interpopulation differences in the prevalence of subclinical hypothyroidism occur.101,107
Clinical presentation, evaluation, and management
The clinical presentation, evaluation, and management of subclinical hypothyroidism in women with a history of infertility are largely similar to those of the general population. 111 The majority of women with infertility who are diagnosed with subclinical hypothyroidism are diagnosed in the work-up for infertility and are asymptomatic. In these women especially, it is difficult to assess whether subclinical hypothyroidism represents normal population variation in TSH or an early form of overt hypothyroidism. Assessing risk factors for iodine deficiency and checking TPOAb status is useful for etiological, therapeutic, and prognostic purposes, as well as determining the frequency of follow-up during a future pregnancy.
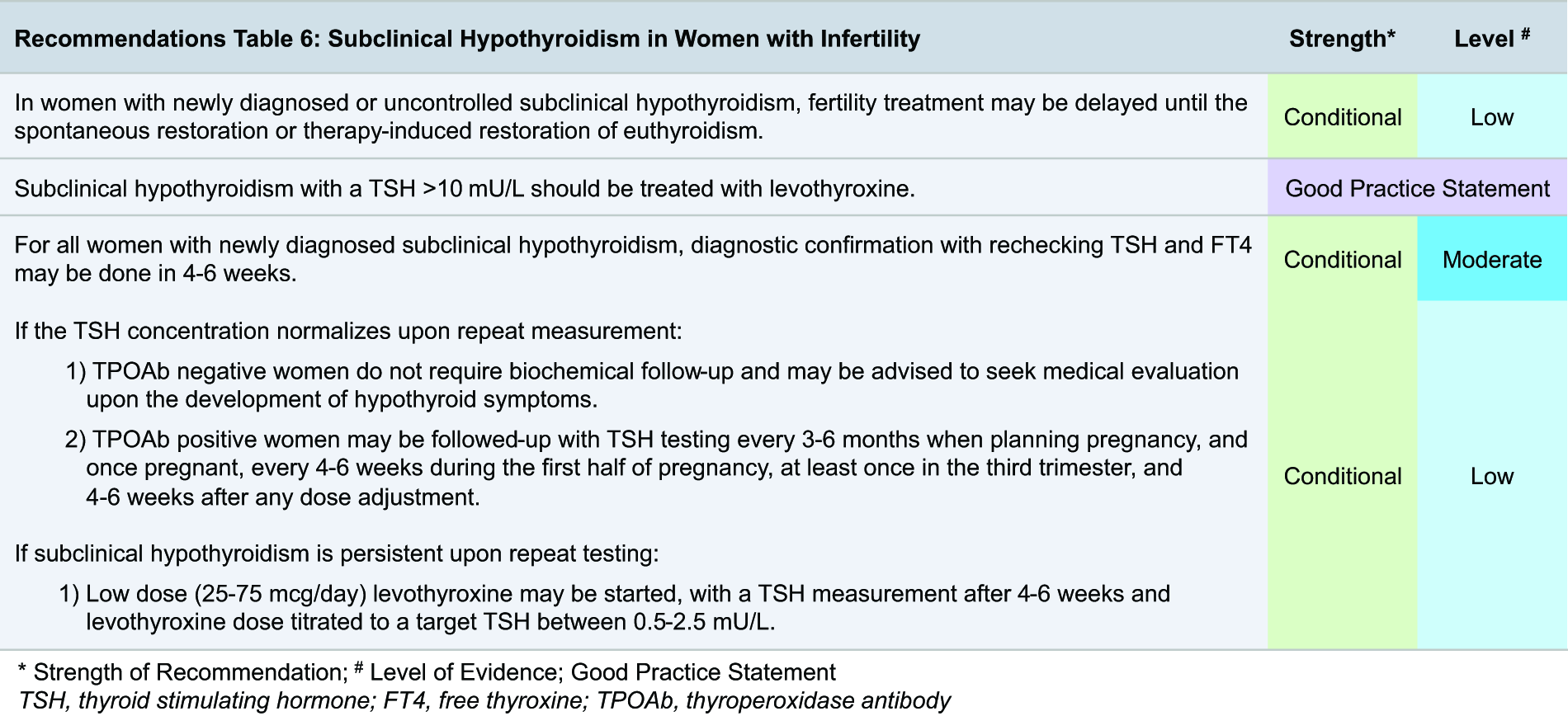
It is well-established that the diagnosis of subclinical hypothyroidism is complicated by large interindividual and intraindividual variations in TSH.124,125 In older populations, up to 80% of mildly increased TSH concentrations may spontaneously normalize upon remeasurement. 126 It is good clinical practice to repeat thyroid function tests after the first identification of subclinical hypothyroidism, because reducing inappropriate LT4 treatment is important to prevent unnecessary patient anxiety, costs, burden on the health care system, and risks related to overtreatment.125,127 In women with infertility, those undergoing fertility treatment, and women with recurrent miscarriages, we recommend aiming for diagnostic confirmation upon first identification of subclinical hypothyroidism by rechecking TSH and fT4 after four to six weeks while delaying fertility treatment. If there is persistent subclinical hypothyroidism, LT4 therapy may be started. In cases of spontaneous normalization of TSH, the TPOAb status can be used to identify patients who may benefit from additional biochemical follow-up. TPOAb positivity is a risk factor for progression to overt hypothyroidism and an indication for TSH monitoring preconception and during pregnancy.98,100,105 For TPOAb-negative women, we advise instructing the patient to seek medical evaluation upon the development of any hypothyroid symptoms. For cases where the physician remains uncertain (e.g., due to a borderline TSH concentration upon retesting, the presence of hypothyroid symptoms, or a high-normal TPOAb titer), it is reasonable to continue evaluation and monitoring, which may include thyroglobulin antibody (TgAb) testing following a shared decision-making approach.
Meta-analyses and narrative reviews, including low-quality studies, conclude that untreated preconception subclinical hypothyroidism in the general population is associated with various mild endocrine changes, 9 a slightly lower chance of conception (absolute difference: −1.4% to −4.5% for increased TSH but <10 mU/L), and a slightly higher risk of miscarriage (absolute difference: +0.4% to +0.7% for increased TSH but <10 mU/L), 104 with similar numbers for women undergoing ART.128,129 In one small, low-quality Korean randomized trial including 64 women, LT4 treatment started on the first day of in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI) treatment in women with subclinical hypothyroidism improved the embryo implantation rate (15% vs. 27%), miscarriage rate (33% vs. 0%), and live birth rate (25% vs. 53%). 130 Women with infertility and those undergoing fertility treatment who have persistent subclinical hypothyroidism preconception could benefit from LT4 treatment as this could prevent progression to overt hypothyroidism, which is especially relevant as there is a state of increased thyroid demand during controlled ovarian stimulation and pregnancy.
The task force recognizes that for certain cases of newly diagnosed subclinical hypothyroidism, verifying persistence is not possible or pragmatic. This can occur in the setting of time constraints related to the age of the patient, the presence of other comorbidities, or due to financial reimbursement related issues. Furthermore, repeat testing may not be deemed pragmatic when there is a low likelihood of TSH normalization. Specific examples would be when the TSH concentration is relatively high (for which the task force suggests a TSH cutoff of 6 mU/L) or when there is concomitant TPOAb positivity.51,52 In those cases, it would be sensible to offer immediately low-dose LT4 (25–75 mcg/day) following a shared decision-making approach.
Thyroid autoimmunity in infertility
This section focuses on TPOAb positivity in women with infertility (considerations related to TgAb positivity in women with infertility can be found in Box 4). TPOAb positivity has a better diagnostic accuracy for hypothyroidism than TgAb positivity and is associated with adverse fertility and pregnancy outcomes, unlike TgAb positivity. Therefore, a TPOAb measurement remains the preferred test to establish or risk stratify for autoimmune hypothyroidism. Assessing TgAb positivity is at the discretion of the physician but can be considered in certain cases (e.g., a euthyroid TPOAb-negative woman with a high-normal TSH and a high risk of thyroid autoimmunity based on previous thyroiditis, concomitant autoimmune disease, or having a first-degree relative with thyroid autoimmunity). Although it is reasonable to also apply recommendations in this subsection to TgAb positive women, this group was not specifically defined during the design of the methodology supporting this guideline.
Epidemiology and physiology
The prevalence of TPOAb positivity in women with infertility or those with a previous miscarriage is around 8–11%, which is similar to that of women of childbearing age and pregnant women in the general population.24,57,101,102,105,106 The prevalence may be about twice as high in women with recurrent miscarriages. 131 Risk factors for TPOAb positivity include other autoimmune diseases, a first-degree relative with thyroid autoimmunity, greater age, obesity, and nulliparity, while smoking is associated with a lower risk and considerable variation is reported by geographical area and/or ethnicity.24,101,102,132 Thyroid autoimmunity can reduce the functional capacity of the thyroid gland, and this can become apparent during states of increased thyroid demand. However, in euthyroid TPOAb-positive women, TSH concentrations during controlled ovarian stimulation are comparable to those in euthyroid TPOAb-negative women. 19
Clinical presentation, evaluation, and management
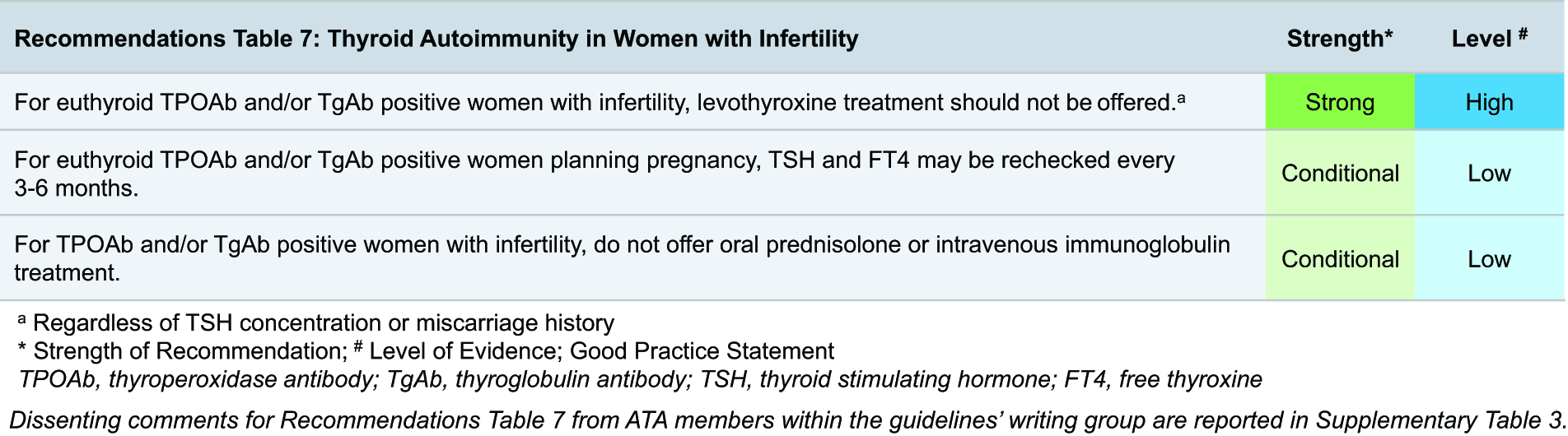
The clinical presentation and evaluation of TPOAb positivity depend on thyroid function and are similar to those of the general population. 111 Euthyroid TPOAb positivity does not present with symptoms. Thyroid autoimmunity is the main risk factor for hypothyroidism. In randomized trials, approximately 7–9% of euthyroid TPOAb-positive women developed (subclinical) hypothyroidism during a 12-month follow-up; cases were mostly detected preconception but also during pregnancy.98–100 Therefore, it seems prudent to recheck TSH every three to six months in euthyroid TPOAb-positive women who are planning a pregnancy.
Euthyroid TPOAb positivity is associated with a higher risk of miscarriage and PPT, and the latter can also occur after a miscarriage.100,105,106,133,134 The absolute risk difference for a miscarriage as compared with TPOAb-negative women ranges from about +2% to +8%, but there are no data for the risk of thyroiditis after miscarriage.105,134–136
Since the publication of the previous version of these guidelines, three high-quality randomized trials have shown that for euthyroid TPOAb-positive women with infertility and or a history of prior/recurrent miscarriage(s), LT4 therapy given during preconception does not improve fertility or pregnancy outcomes.100,105,106 We extrapolated these results, obtained in a high-risk population, to make recommendations for the general population. There were no factors that modified the response to LT4 treatment, including a TSH >2.5 mU/L, previous miscarriage(s), maternal age, or the TPOAb concentration.100,105,106,135,137,138 This suggests that the mechanism underlying the higher risk of miscarriage and other adverse fertility outcomes in euthyroid TPOAb-positive women is not mediated through changes in thyroid hormone availability and remains to be elucidated. It is plausible that thyroid antibodies are a reflection of a more general susceptibility to autoimmunity and that other autoimmune processes are underlying the higher risk of pregnancy complications. 139 However, there are currently no data to support a dietary intervention or the use of immune modulatory medications, such as glucocorticoids, intravenous immunoglobulins, or selenium, to improve obstetric outcomes or lower the risk of developing hypothyroidism (during pregnancy).
Subclinical and overt hyperthyroidism in infertility
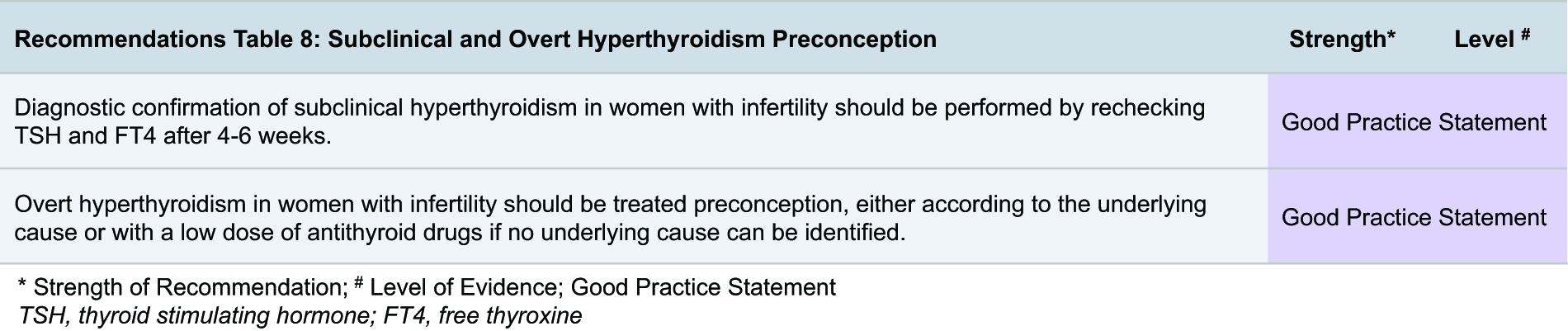
The epidemiology, physiology, clinical presentation, evaluation, and management of preconception subclinical and overt hyperthyroidism are discussed in Section G. For this subsection, we briefly highlight two considerations specifically for women with subclinical or overt hyperthyroidism who are planning pregnancy in the setting of infertility and/or recurrent miscarriages. First, it is relevant to assess the schedule and timing of fertility treatments since (age-dependent) time constraints may warrant a faster diagnostic and/or therapeutic route than usual care. This concept applies to any woman with thyroid disease who is planning pregnancy but can be more relevant for those with subclinical and overt hyperthyroidism owing to the required diagnostics and longer time to reach euthyroidism. Second, for sporadic cases in which the TSH remains persistently suppressed to <0.1 mU/L and both fT4 and T3 are normal, yet no clear underlying cause can be identified after a regular work-up, intensified follow-up during preconception and pregnancy can be considered to identify the possible progression of hyperthyroidism at an early phase. Alternatively, it may be reasonable to consider low-dose propylthiouracil (PTU) preconception. The goal of this approach would be to normalize the TSH concentration prior to pregnancy. This is based on expert opinion and supported by a large observational study showing that a suppressed TSH is associated with a delayed time to pregnancy in untreated women. 104 PTU can be stopped upon a positive pregnancy test to reduce the risk of fetal birth defects associated with PTU exposure, and the patient should be instructed to do so immediately or seek contact upon a positive pregnancy test. If only cryopreservation of oocytes or embryos is planned without the anticipation of an embryo transfer in the immediate future, ATDs can be continued before and during the fertility preservation treatment.
F. Hypothyroidism, Thyroid Autoimmunity, and Hypothyroxinemia Preconception and In Pregnancy
The approach to hypothyroidism during pregnancy differs based on the timing of the diagnosis (preconception vs. gestational) and the magnitude of the thyroid function test abnormality (overt vs. subclinical disease and/or degree of TSH elevation). Laboratory values are the main determinant of general management because of the frequent lack of hypothyroid symptoms during pregnancy and the overlap of hypothyroid symptoms with those of a healthy pregnancy. Optimal management requires anticipation of known physiological gestational alterations of thyroid function parameters, as well as knowledge regarding the interpretation of laboratory tests (see Section C). Furthermore, clinicians should be knowledgeable about (absolute) risks of thyroid dysfunction, to provide individualized counseling on the pregnancy complications or adverse child outcomes risks related to (subclinical) hypothyroidism and the potential benefits of LT4 treatment.
Overt hypothyroidism in preconception and pregnancy
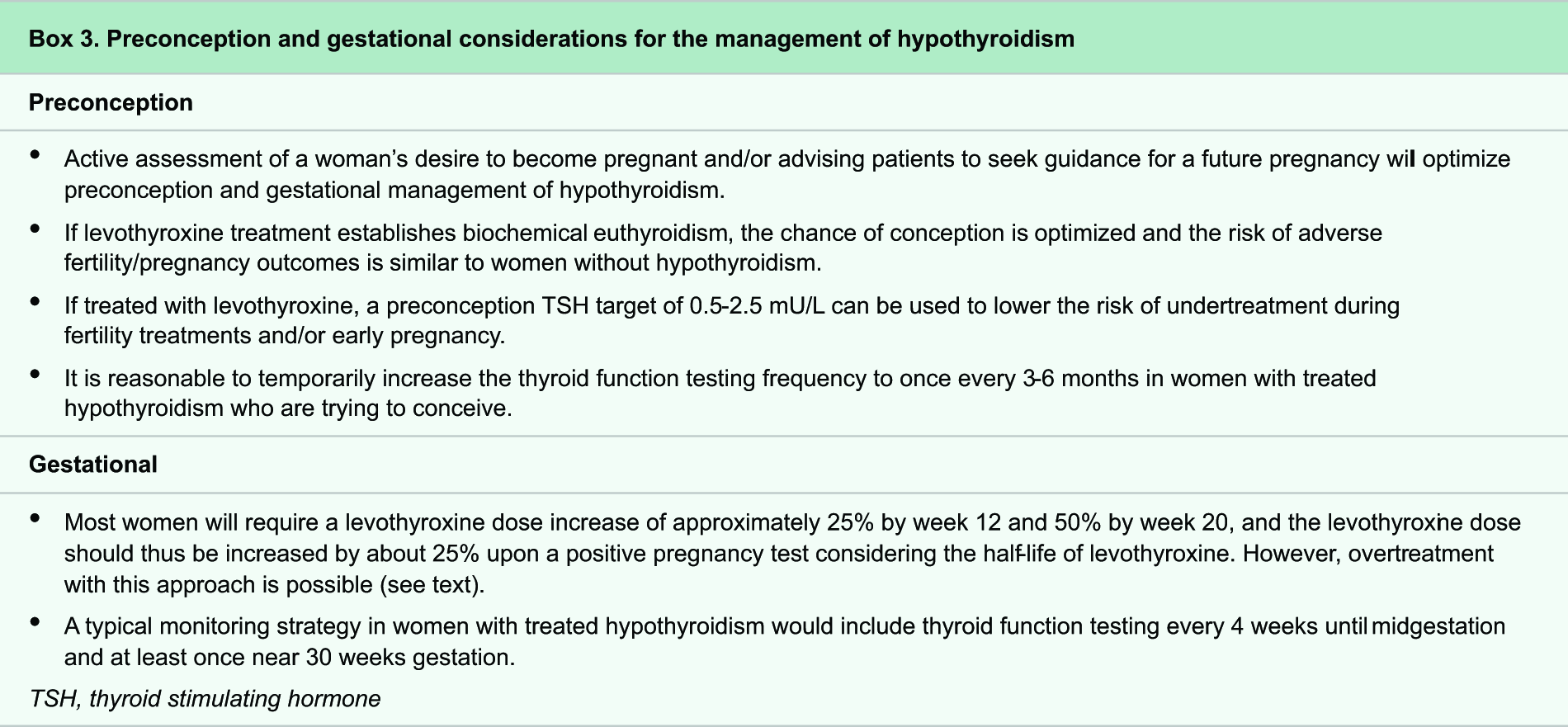
In women known to have hypothyroidism prior to pregnancy, the basis of disease management during the preconception, gestational, and postpartum periods is similar to the general recommendations for nonpregnant patients. Some additional considerations specific to these periods, based on established clinical practice rather than high-quality evidence, are outlined in Box 3. Longstanding overall agreement to treat overt hypothyroidism during pregnancy with LT4 has limited the synthesis of evidence on the risks of untreated hypothyroidism and the benefits of treatment. Most available data on overt hypothyroidism during pregnancy are from studies published 20–30 years ago and therefore include more severe cases than those typically detected in current clinical practice. Nonetheless, LT4 treatment benefits are still considered to outweigh any risks. In general, women with hypothyroidism who remain euthyroid with LT4 treatment have similar fertility, pregnancy, and postpartum outcomes as women without hypothyroidism.
Epidemiology and physiology
The prevalence of overt hypothyroidism is approximately 0.2% of all women of childbearing age,101,107 and new-onset overt hypothyroidism occurs in approximately 0.4–0.5% of all pregnant women,57,110 although the prevalence during pregnancy largely depends on the upper limit used for TSH (laboratory-specific vs. a fixed limit).38,57,110 The main risk factor for hypothyroidism before or during pregnancy is thyroid autoimmunity, with hypothyroidism being more common in women with other autoimmune diseases, especially those autoimmune diseases that are a part of multiple autoimmune endocrinopathies.38,108,109 Greater age is associated with a higher risk of preconception hypothyroidism but not with hypothyroidism during pregnancy, and considerable regional and interpopulation (ethnicity-based) differences in hypothyroidism prevalence occur.38,107,109,110 It remains unknown what proportion of hypothyroidism during pregnancy is pre-existing disease identified for the first time during pregnancy versus gestation-specific hypothyroidism related to the increased thyroid hormone demand of pregnancy.
Clinical presentation and evaluation
The clinical presentation and evaluation of hypothyroidism outside of the perinatal period are summarized in detail elsewhere. 111 Most women diagnosed with overt hypothyroidism during pregnancy are identified when presenting for general obstetric care. While overt hypothyroidism during pregnancy is associated with more hypothyroid symptoms than in euthyroid women, this difference is not large enough to distinguish between the groups, and many women with overt hypothyroidism in pregnancy present without symptoms.140,141 Assessing risk factors for iodine deficiency is helpful to determine an indication for iodine supplementation, since iodine deficiency could cause maternal hypothyroidism and sustained fetal hypothyroidism (Section D). In addition, checking TPOAb status in those with new-onset overt hypothyroidism is useful for etiological and prognostic purposes and for determining the frequency of follow-up during the remainder of pregnancy or during a future pregnancy. Untreated or inadequately controlled hypothyroidism during pregnancy is associated with a higher risk of miscarriage, gestational hypertension, preterm birth, and up to seven points lower mean offspring IQ.142–147 However, it is difficult to quantify these risks for counseling purposes in current clinical practice because these data were collected at least 15–25 years ago and studies may be biased. Within the group of women with overt hypothyroidism during pregnancy, a higher TSH concentration is associated with a higher risk of miscarriage and lower offspring IQ,146,147 but no other factors are known to modify the risk of adverse outcomes. Newly diagnosed overt hypothyroidism during pregnancy is not considered a medical reason for termination of pregnancy.148,149 Women with pre-existing hypothyroidism who adhere to LT4 treatment and/or those with hypothyroidism diagnosed during pregnancy who achieve biochemical control with LT4 have similar risks of adverse pregnancy or child outcomes as women without hypothyroidism during pregnancy.144,145,147–152
Preconception treatment and management
The management of hypothyroidism outside of the perinatal period is summarized in detail elsewhere, 111 and preconception recommendations specifically for women with infertility can be found in Section E. The guidance for the management of overt and subclinical hypothyroidism in women planning pregnancy is summarized in Flowchart 1 and for pregnant women in Flowchart 2. Following an established diagnosis, a logical LT4 treatment target for a woman wishing to conceive is a TSH in the reference interval but below 2.5 mU/L, in order to create a margin of safety for remaining euthyroid in anticipation of a state of increased thyroid hormone demand during pregnancy. The fetal central nervous system is relatively impermeable to T3 and the majority of fetal T3 present in the central nervous system during pregnancy is derived locally from maternal T4 actively transported into the intervillous space. 48 Treatment with liothyronine or desiccated thyroid leads to a relative excess of T3 and relatively low concentrations of T4, which could lower fetal central nervous system T4 and T3 availability.48,153,154 Therefore, women using liothyronine or desiccated thyroid preparations should be recommended to switch to LT4 monotherapy to avoid insufficient thyroid hormone availability for the fetal brain. For switching from combination T3 and T4 therapy to LT4 monotherapy, every 5 mcg of liothyronine may be considered equivalent to 20 mcg LT4. For switching from desiccated thyroid extract to LT4 monotherapy, every 60 mg grain of desiccated thyroid may be considered equivalent to 88 mcg LT4. 155
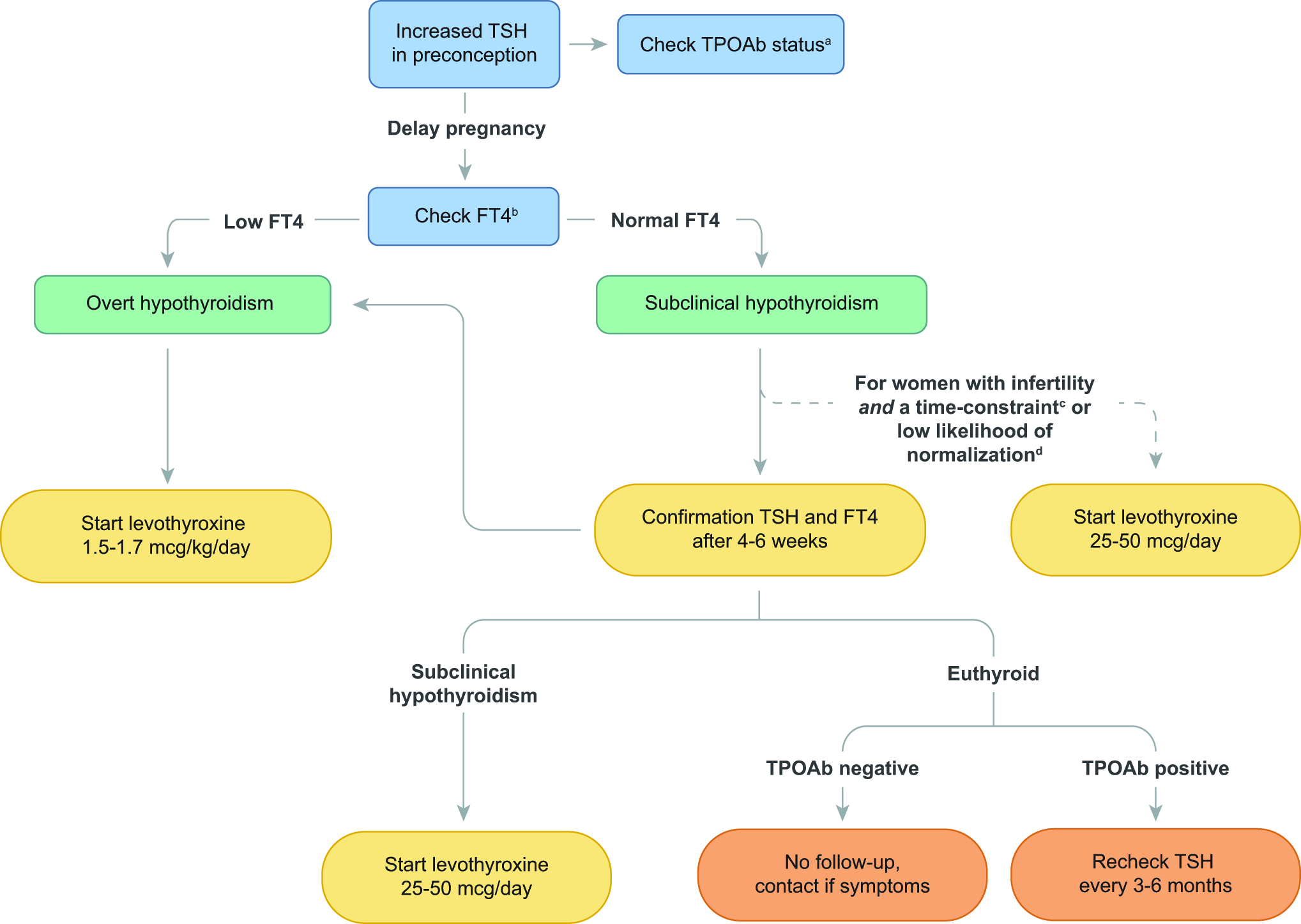
Approach to increased TSH levels in preconception. Green boxes indicate a diagnosis, yellow boxes indicate an action, and orange boxes indicate recommended follow-up. aWomen with a high TSH have a higher risk of TPOAb positivity. TPOAb positivity is associated with a 7–9% risk of developing subclinical hypothyroidism preconception or during pregnancy. TPOAb status can guide screening in a future pregnancy and aid in counseling for postpartum thyroiditis risk. Euthyroid TPOAb positivity is not an indication for levothyroxine (refer to Recommendations Table 7). bOr alternatives as described in the thyroid function testing subsection of this guideline. cFor example, when fertility is already planned or when the chance of a successful pregnancy due to age or comorbidities would be further limited by postponing treatment. dBased on expert opinion, this could be defined, for example, as a TSH concentration >6 mU/L or in case of subclinical hypothyroidism with concomitant TPOAb positivity.
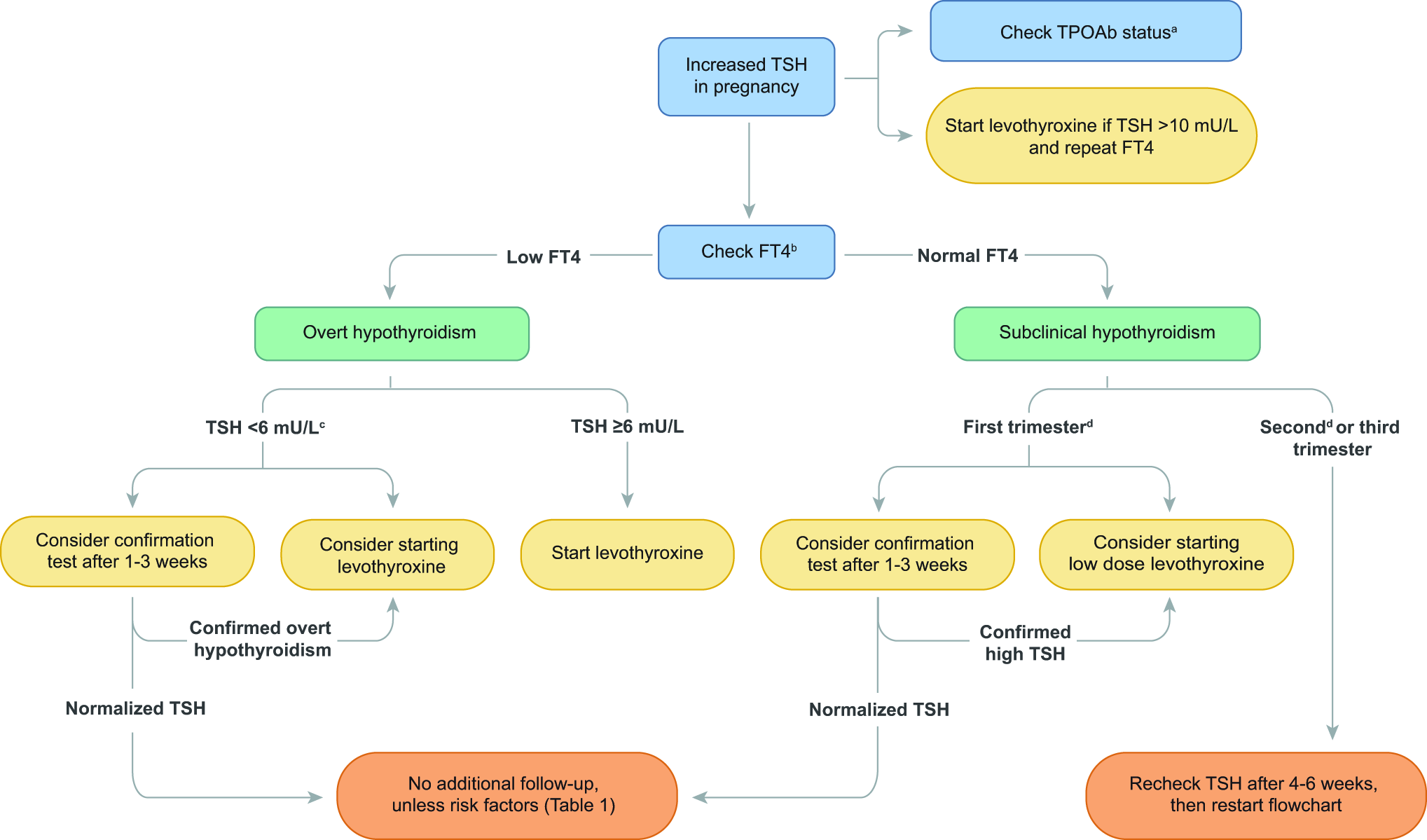
Approach to increased TSH levels in pregnancy. Green boxes indicate a diagnosis, yellow boxes indicate an action, and orange boxes indicate recommended follow-up. aWomen with a high TSH have a higher risk of TPOAb positivity. TPOAb positivity can be used for counseling on postpartum thyroiditis and guide screening in future pregnancies. bOr alternatives as described in the thyroid function testing subsection of this guideline. cFor mild forms of overt hypothyroidism, the risk profile and chance of TSH normalization are similar to those of subclinical hypothyroidism. Therefore, confirmatory testing can be considered using a shared decision-making approach. dThe distinction between the first and second trimester remains arbitrary, and management can be altered if the gestational age is within reasonable proximity on a case-by-case approach.
Gestational treatment and management
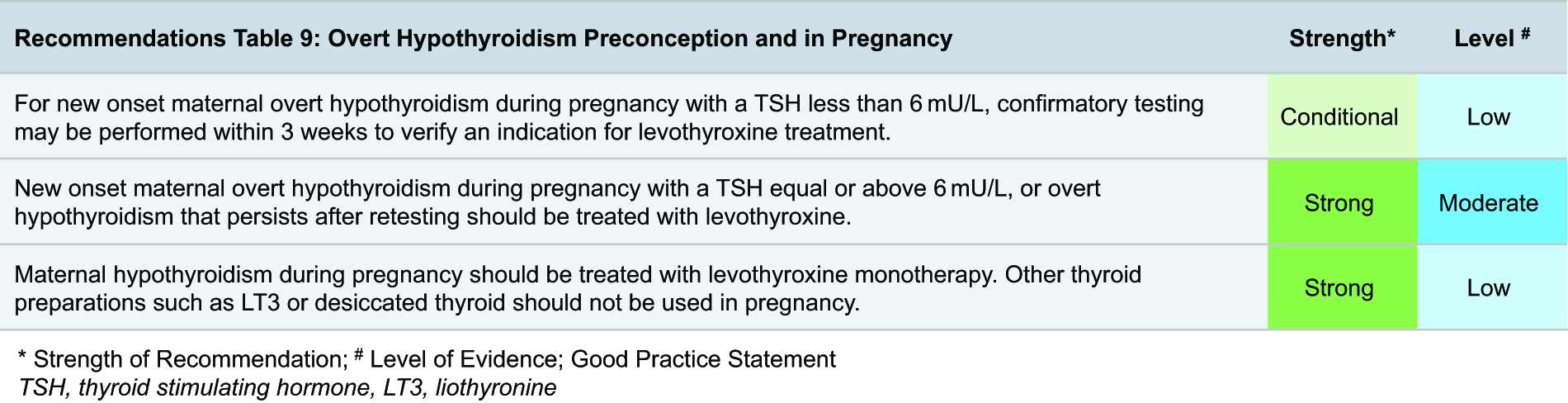
Recent studies showed that mild overt hypothyroidism during pregnancy only persists in less than half of all untreated women upon rechecking thyroid function tests after 1–3 weeks (especially if TSH is <6.0 mU/L), and the persistence is even lower when thyroid function tests are reassessed in the third trimester.51,52 This indicates that for mild overt hypothyroidism during pregnancy, reassessment can be considered before starting treatment. We defined “mild” overt hypothyroidism as a TSH that is elevated above the pregnancy upper limit but less than 6 mU/L based on the possibility of normalizing upon reassessment, low risk of adverse pregnancy outcomes, and expert opinion.33,51,52,146 This recommendation is conditional upon patient preference. A clinical example for this would be if a patient with mild overt hypothyroidism during pregnancy is doubtful or anxious about starting LT4 after counseling on the presumed (minor) risks of remaining untreated or delayed treatment.
In contrast, overt hypothyroidism with a TSH equal to or above 6 mU/L during pregnancy is an indication for LT4 treatment. LT4 doses for newly diagnosed overt hypothyroidism in pregnancy may be estimated with the guidance used for full replacement (1.5–1.7 mcg/kg/day) plus an additional 20–30% dose increase required for gestation. The majority of women using LT4 for overt hypothyroidism will require a dose increase of approximately 25% by week 12 and approximately 50% by week 20 to remain euthyroid.156–158 To reach a steady state, the dose can be increased upon a positive pregnancy test and titrated thereafter, either by increasing the daily dose or by increasing the dose by two LT4 daily dosages per week. If all women undergo a standardized dose increase, there is a slightly higher risk of overtreatment in women with a prepregnancy TSH <1.5 mU/L, women with a prepregnancy LT4 dose >100 mcg/day, and women who increase the weekly dose by two tablets.156–158 Therefore, the preconception TSH and LT4 dose should be taken into account when considering a dose increase and/or the quantity of that increase. At delivery, the LT4 dose can be changed back to the prepregnancy dose, and thyroid function can be tested after six weeks.
Subclinical hypothyroidism in preconception and pregnancy
In women known to have subclinical hypothyroidism prior to pregnancy, there is a lower threshold to start LT4 treatment during preconception or early gestation as compared with subclinical hypothyroidism in nonpregnant populations. A carefully balanced diagnostic, counseling, and treatment strategy is required to optimize potential LT4 benefits while preventing potential harms related to overtreatment and patient anxiety. For this topic, there is abundant low-to-moderate quality evidence but only sparse high-quality evidence to support recommendations. The main foundations of the available evidence are three randomized trials that investigated LT4 for subclinical hypothyroidism during pregnancy. The task force has assessed subanalyses and between-study comparisons from the randomized trials, often supported by observational studies, to form recommendations for this subsection.
Epidemiology and physiology
The prevalence of subclinical hypothyroidism is approximately 2.4–6.0% in women of childbearing age,101,120 and subclinical hypothyroidism during pregnancy occurs in approximately 3.2–3.5% of all pregnant women,57,110 although the prevalence during pregnancy largely depends on the upper limit used for TSH (laboratory-specific vs. a fixed limit).38,57,110 The main risk factor for hypothyroidism before or during pregnancy is thyroid autoimmunity.38,108 Greater age is associated with a higher risk of subclinical hypothyroidism preconception and during pregnancy, and considerable regional and interpopulation differences in subclinical hypothyroidism prevalence occur.38,101,107,110 It remains unknown what proportion of subclinical hypothyroidism during pregnancy is pre-existing disease identified for the first time during pregnancy versus gestation-specific subclinical hypothyroidism related to the increased thyroid hormone demand associated with pregnancy.
Clinical presentation and evaluation
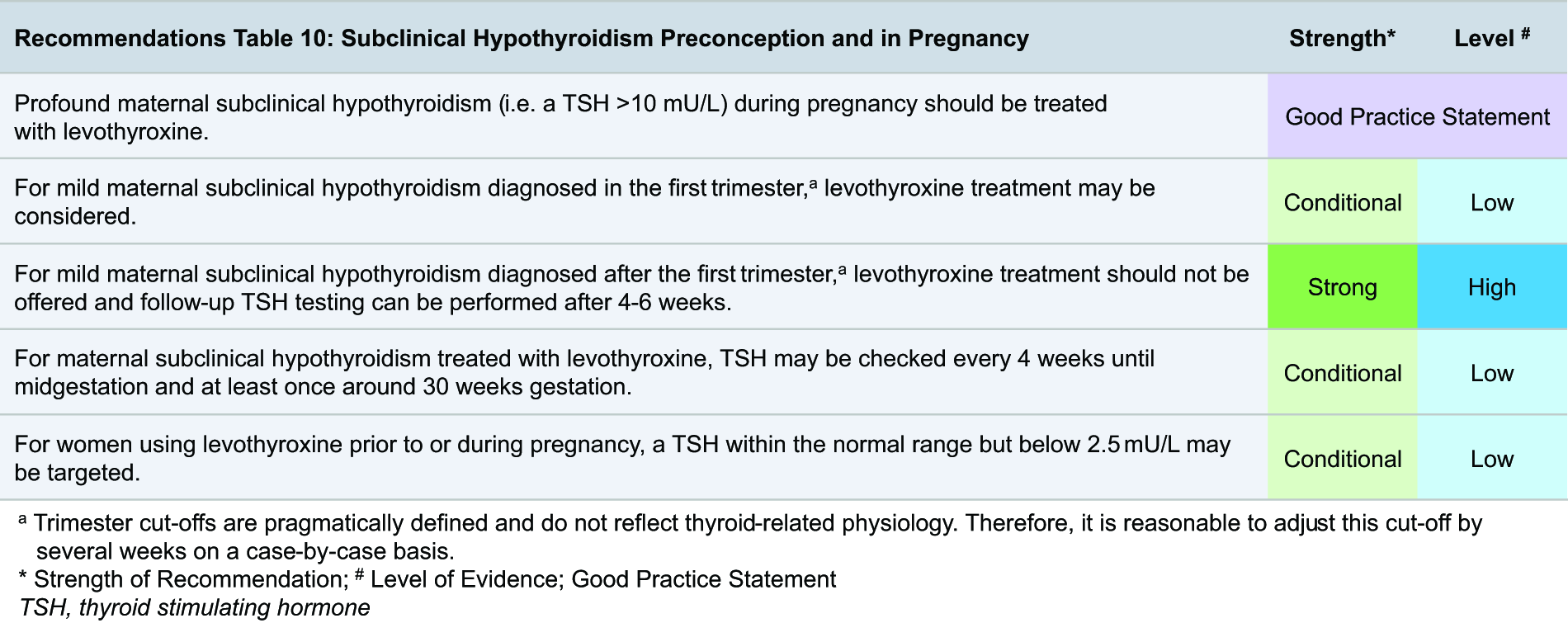
The clinical presentation and evaluation of subclinical hypothyroidism outside of the perinatal period are summarized in detail elsewhere. 111 The majority of women diagnosed with subclinical hypothyroidism during pregnancy are identified when presenting for general obstetric care and have no hypothyroid symptoms.57,140,141 Assessing risk factors for iodine deficiency and checking TPOAb status is useful for etiological, therapeutic, and prognostic purposes as well as assessing the frequency of any follow-up during the remainder of pregnancy or in future pregnancies. Untreated subclinical hypothyroidism is associated with a higher risk of miscarriage, pre-eclampsia, placental abruption, preterm birth, and small for gestational age.33,34,159–161 The absolute risk difference for these pregnancy complications as compared with euthyroidism ranges between +1 to +5%.33,34,159–161 Within the group of women with subclinical hypothyroidism during pregnancy, a higher TSH concentration, earlier gestation at diagnosis, and TPOAb positivity are not associated with a clinically relevant higher risk of adverse outcomes.33,34,159–162 Therefore, although untreated subclinical hypothyroidism is associated with only small absolute increases in adverse pregnancy and child outcomes, this does not preclude consideration of LT4 treatment in selected circumstances. In these settings, treatment decisions are driven primarily by timing of diagnosis (preconception or early gestation), risk of progression during pregnancy, and patient values and preferences, rather than by a large anticipated reduction in absolute risk.
Treatment and management
The management of subclinical hypothyroidism outside of the perinatal period is summarized in detail elsewhere, 111 and recommendations for women with infertility can be found in Section E. For women with subclinical hypothyroidism who are planning pregnancy, postponing pregnancy and repeating thyroid function tests after four to six weeks before attempting pregnancy should be preferred, rather than immediate LT4 treatment, given that thyroid function tests will normalize for a large number of women. If subclinical hypothyroidism persists upon retesting, or if a 6- to 12-week waiting period is not feasible, then LT4 treatment can be started at a low dose (e.g., 50 mcg/day). A logical LT4 treatment target for a woman with a wish to conceive is a TSH in the reference interval to ensure adequate thyroid hormone availability, but below 2.5 mU/L to create a margin of safety for remaining euthyroid in anticipation of a state of increased thyroid hormone demand during pregnancy. Women using liothyronine or desiccated thyroid preparations should be advised to switch to LT4 monotherapy to avoid insufficient thyroid hormone availability for the fetal brain (see subsection on overt hypothyroidism in pregnancy). 48
Limited data from one small, randomized trial and several observational studies support the concept that LT4 treatment for subclinical hypothyroidism diagnosed during the first trimester can be beneficial. In an Iranian randomized trial that treated the highest proportion of patients in the first trimester (62% and 52% in TPOAb-positive and TPOAb-negative women, respectively), LT4 treatment was associated with a lower rate of preterm birth compared with no treatment (5.3% vs. 24.9% in TPOAb-positive women; 7.3% vs. 19% in TPOAb-negative women). In this trial, there was also a higher median offspring gross motor development score (60 vs. 57.5 points on the Ages and Stages Questionnaire) but no corresponding effects on other neurocognitive domains at age 3 years.137,163,164 Notably, the positive results were only obtained if subclinical hypothyroidism was defined using a TSH cutoff of >4.0 mU/L, but there was no LT4 benefit if subclinical hypothyroidism was defined using a TSH of >2.5 or >3.0 mU/L. In a large trial performed in the United Kingdom and Italy (Controlled Antenatal Thyroid Screening [CATS] trial), high-dose LT4 (150 mcg/day) started at a median 12 weeks’ and 3 days’ gestation did not improve obstetric outcomes (personal communication with authors) or offspring IQ at age 3 years. 165 In a large US National Institutes of Health trial, LT4 treatment started on average at 17 weeks’ gestation did not improve obstetric outcomes or offspring IQ at age 5, and LT4 effects did not meaningfully differ according to the timing of treatment initiation (before or after 17 weeks). 166 The concept that the first trimester is a more opportune period for LT4 treatment benefits as compared with later stages of pregnancy is supported by some observational studies investigating miscarriage and offspring IQ or brain morphology,35,159,167 but not by studies investigating other outcomes, such as preterm birth. 33 Trimesters are pragmatically defined and do not reflect thyroid-related physiology; therefore, it is reasonable to adjust these trimester-specific recommendations in this guideline by several weeks on a case-by-case basis (example scenarios: delayed diagnosis due to late entry into prenatal care; an initial or follow-up abnormal TSH result shortly after the end of the first trimester rising TSH concentration or progression toward overt hypothyroidism shortly after 12 weeks’ gestation).
For starting LT4 in women with subclinical hypothyroidism during the first trimester, we advise a shared-decision-making approach that includes counseling on the potential risks of untreated subclinical hypothyroidism and the lack of conclusive evidence for the benefits of LT4 treatment, as summarized in Flowchart 2. Furthermore, recent studies showed that subclinical hypothyroidism during pregnancy only persists in 41% of all untreated women upon rechecking thyroid function tests after about 3 weeks (especially if TSH is <6.0 mU/L), and in 25% when thyroid function tests are reassessed in the third trimester.51,52 This indicates that reassessment can be considered before starting treatment. A clinical example for this would be if a patient with subclinical hypothyroidism during pregnancy is doubtful or anxious about starting LT4 after counseling on the presumed risks of remaining untreated or delayed treatment. When the decision is made to defer LT4, repeat thyroid function testing can be performed within three weeks to exclude progression to overt hypothyroidism. When the decision is made to start LT4 therapy, the optimal dose is one that is high enough to normalize TSH but low enough to prevent potential overtreatment. The concept of potential harm related to LT4 overtreatment and the recommendation to start with 25–75 mcg/day depending on the TSH concentration and weight of the patient are based on data from randomized trials and personal experiences of the writing group.35,100,105,106,168–172 For example, women who were included in the CATS trial and showed biochemical or clinical signs of overtreatment (using LT4 150 mcg/day) had children with more symptoms of attention-deficit/hyperactivity disorder and behavioral difficulties but similar anthropometric, metabolic, and neurocognitive outcomes.168–170 Similar to the management of overt hypothyroidism during pregnancy, a treatment target of TSH in the reference interval, but below 2.5 mU/L to create a safety margin for undertreatment, can be used. In contrast to overt hypothyroidism, for subclinical hypothyroidism diagnosed preconception, there are no data to support a standard 25% LT4 dose increase upon a positive pregnancy test. Based on the personal experience of the writing group, either a small dose increase (e.g., 12.5 mcg/day) or a reflex dose change based on thyroid function testing every 4 weeks during the first half of pregnancy, both yield satisfactory results. After delivery, an LT4 cessation trial should be strived for to prevent unnecessary chronic LT4 use. A shared decision on the cessation trial itself and also its timing can be made taking into account the TSH at diagnosis, TPOAb status, breastfeeding, and future pregnancy planning, while noting that the benefit of LT4 on breastfeeding outcomes is based on very limited data.
Thyroid autoimmunity in preconception and pregnancy
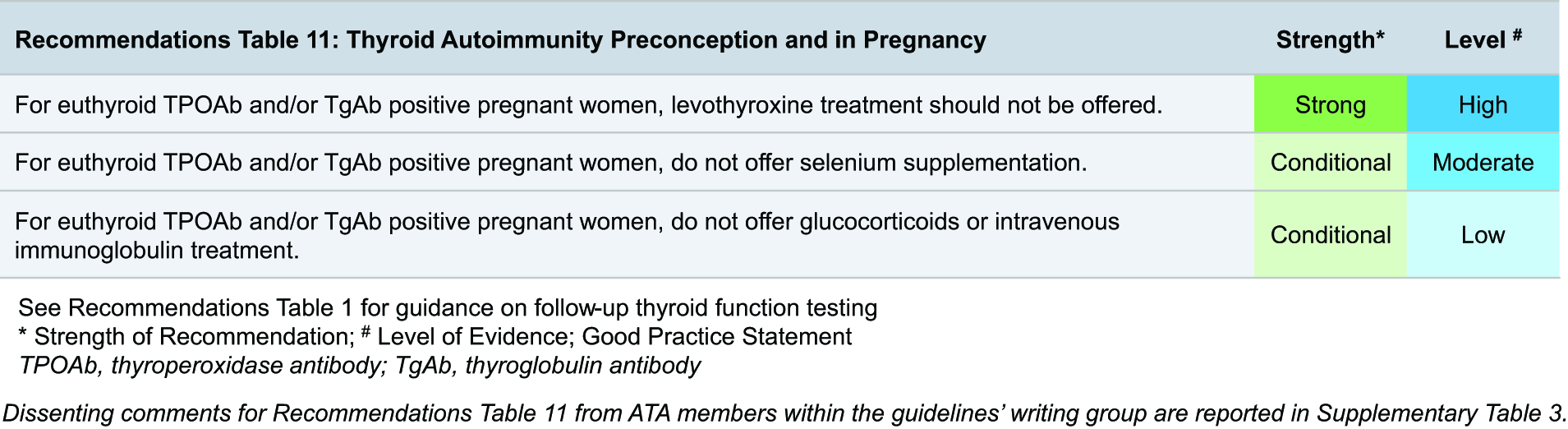
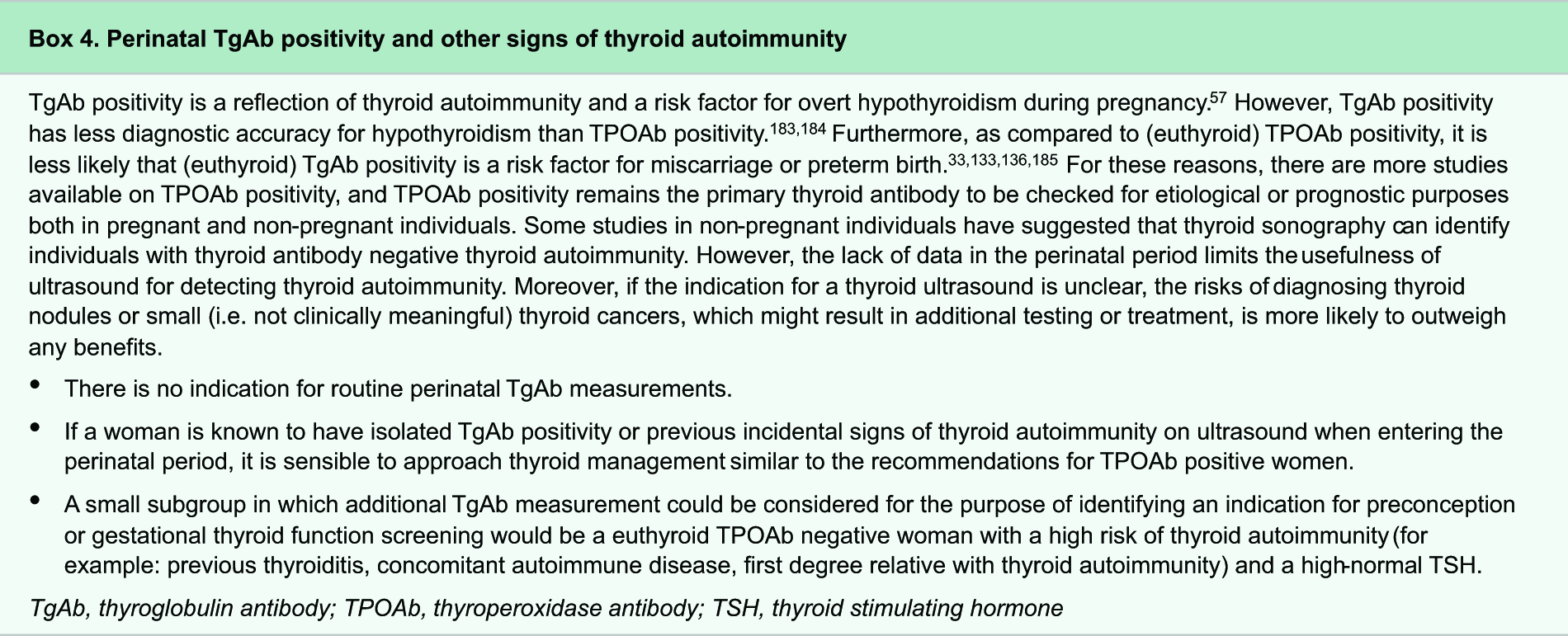
This section focuses on TPOAb positivity; considerations on TgAb positivity can be found in Box 4. Autoimmune hyperthyroidism is discussed below in Section G. The interpretation of TPOAb positivity in the perinatal period is similar to that outside of pregnancy, in the sense that euthyroid TPOAb positivity should be considered a risk factor for thyroid disease rather than a disease entity in itself. However, increased thyroid hormone demand makes pregnancy a window of increased risk of new onset, or progression of, hypothyroidism in women with thyroid autoimmunity, thus warranting active screening and follow-up. Recommendations in this subsection are based on a large body of prospective cohort studies and multiple randomized trials.
Epidemiology and physiology
The prevalence of TPOAb positivity in women of childbearing age and pregnant women ranges between 5% and 15% (worldwide average 9%).57,101,102 Risk factors for TPOAb positivity have poor discriminative ability and include other autoimmune diseases, a first-degree relative with thyroid autoimmunity, greater age, obesity, and nulliparity; in addition, ethnic differences also exist.101,102,132 Thyroid autoimmunity can reduce the functional capacity of the thyroid gland, which can become apparent during pregnancy as thyroidal stimulation by hCG is impaired in the majority of TPOAb-positive women.22,23,25 In line with this physiology, TPOAb positivity is the most important risk factor for hypothyroidism during pregnancy. Of all TPOAb-positive women, 4% have overt hypothyroidism and 18% have subclinical hypothyroidism during pregnancy (as compared with 0.4% and 3.2% for TPOAb-negative women, respectively). 57 As pregnancy progresses, TPOAb concentrations can decrease by 60% due to gestational immunotolerance, 25 and this can change the TPOAb status from positive during early pregnancy to negative during the third trimester in up to 16% of cases.51,52 Furthermore, women with a TPOAb concentration just below the positivity cutoff have slightly higher TSH and lower fT4 concentrations during pregnancy, as compared with women with TPOAb concentrations below the 80th percentile. 173 Therefore, when the initial titer of TPOAb status is in the high-normal range of the reference interval during pregnancy, follow-up of thyroid function tests similar to what is advised for TPOAb-positive women can be considered.
Clinical presentation and evaluation
The clinical presentation and evaluation of TPOAb positivity during the perinatal period are related to hypothyroidism and similar to those outside of the perinatal period, which is summarized in detail elsewhere. 111 Pregnant women with euthyroid TPOAb positivity do not present with symptoms, but have a higher risk of miscarriage and preterm birth.33,100,105,106,133,140,141 The absolute risk difference as compared with TPOAb-negative women ranges from about +2% to +8% for miscarriage, and about + 2 to + 3% for preterm birth.33,105,134–136 There are no known factors that modify these risks in euthyroid TPOAb-positive women.
Treatment and management
Since publication of the previous version of these guidelines, three randomized trials have shown that for women with euthyroid TPOAb positivity, LT4 therapy started either preconception100,105,106 or in early pregnancy 137 does not improve adverse obstetric or newborn outcomes. We extrapolated these negative results, obtained in a high-risk population (a large proportion of women had infertility or a previous miscarriage), to also make recommendations that include the general population. There were no factors that modified the response to LT4 treatment, including a TSH >2.5 mU/L, previous miscarriage(s), maternal age, or the TPOAb concentration.100,105,106,135,137,138 Thus, the slightly higher risks of adverse pregnancy outcomes (especially miscarriage and preterm birth) in TPOAb-positive women do not seem to be modified by LT4 treatment. Since this also suggests that the mechanism underlying the higher risk for TPOAb-positive women is not related to changes in thyroid hormone availability, the underlying mechanism remains to be elucidated. It is plausible that thyroid antibodies are a reflection of a more general susceptibility to autoimmunity and that other autoimmune processes are underlying the higher risks of pregnancy complications. 139 However, there are currently no data to support a dietary intervention or the use of immune-system-altering medications such as glucocorticoids, intravenous immunoglobulins, or selenium to improve obstetric outcomes or risk for (gestational) hypothyroidism.174–180
Isolated hypothyroxinemia in preconception and pregnancy

Isolated hypothyroxinemia is predominantly a pregnancy-specific thyroid function test abnormality with an unclear etiology. Recommendations in this subsection are based on a large body of prospective cohort studies and two randomized trials.
Epidemiology and physiology
The prevalence of isolated hypothyroxinemia in women of childbearing age is about 0.2% and ranges between 2.0% and 2.2% in pregnant women.57,101,110 The prevalence is higher when laboratory and pregnancy-specific reference intervals are used in the first trimester (0.75% vs. 2.1%), but similar across definitions in the second trimester. 38 The etiology of isolated hypothyroxinemia is not clear, but risk factors include iodine deficiency, iron deficiency, higher BMI, greater age, twin pregnancy, exposure to endocrine disruptors, and angiogenic factors,57,184 but not TPOAb positivity. 185 Furthermore, it can also be attributed to changes in fT4 assay performance during pregnancy, leading to falsely low fT4 concentrations in some women. 184
Clinical presentation and evaluation
During pregnancy, most women diagnosed with isolated hypothyroxinemia are identified when presenting for general obstetric care. While isolated hypothyroxinemia is associated with more hypothyroid symptoms than euthyroidism, this difference is not large enough to distinguish these two biochemical states clinically.140,141 Isolated hypothyroxinemia is associated with a higher risk of premature rupture of membranes, gestational diabetes mellitus, (very) preterm birth, large for gestational age, and a lower offspring IQ.33,34,186–189 The absolute risk difference, as compared with euthyroid women, ranges from about +2% to +4% for obstetric outcomes and an average of two to four points lower offspring IQ.33,105,134–136 There are no known factors that modify these risks in women with isolated hypothyroxinemia. The differential diagnosis for isolated hypothyroxinemia may include central hypothyroidism, and screening for symptoms of deficiency or excess of pituitary hormones and/or apoplexy/hypophysitis may be considered. However, central hypothyroidism has a very low incidence, especially in patients lacking risk factors or related symptoms. Therefore, in the absence of central hypothyroidism risk factors (such as a history of previous hypothalamic or [infiltrating] pituitary disease or cranial irradiation) or symptomatology, no further routine diagnostics seem warranted.
Treatment and management
Two randomized trials showed that for women with isolated hypothyroxinemia, LT4 therapy started in the second trimester does not improve obstetric or offspring neurocognitive outcomes, regardless of TPOAb status or iodine intake.165,166,169,170,190 There are no data from randomized trials on early pregnancy LT4 treatment for isolated hypothyroxinemia. Isolated hypothyroxinemia in early pregnancy persists upon reassessment in only 18% of cases.51,52 Follow-up thyroid function testing after two to six weeks can be considered for isolated hypothyroxinemia diagnosed around the first trimester to exclude progression to hypothyroidism, as early isolated hypothyroxinemia is less likely to be related to fT4 assay interference or fT4 reference interval definitions compared with later pregnancy. Because iron and/or iodine deficiency are risk factors for isolated hypothyroxinemia, it is reasonable to assess iron status and risk factors for iodine deficiency in women with isolated hypothyroxinemia.
G. Hyperthyroidism Preconception, In Pregnancy, and Postpartum
The diagnostic approach and management of thyrotoxicosis in women during preconception, pregnancy, and lactation requires careful consideration and a management plan tailored to the individual patient. The most relevant considerations relate to the goal of restoring euthyroidism as quickly as possible, while mitigating the risks of treatment during this vulnerable period. In addition, the unique overlap of clinical signs, symptoms, and laboratory tests with physiological alterations of thyroid parameters during gestation can be challenging in the care of the pregnant hyperthyroid woman.
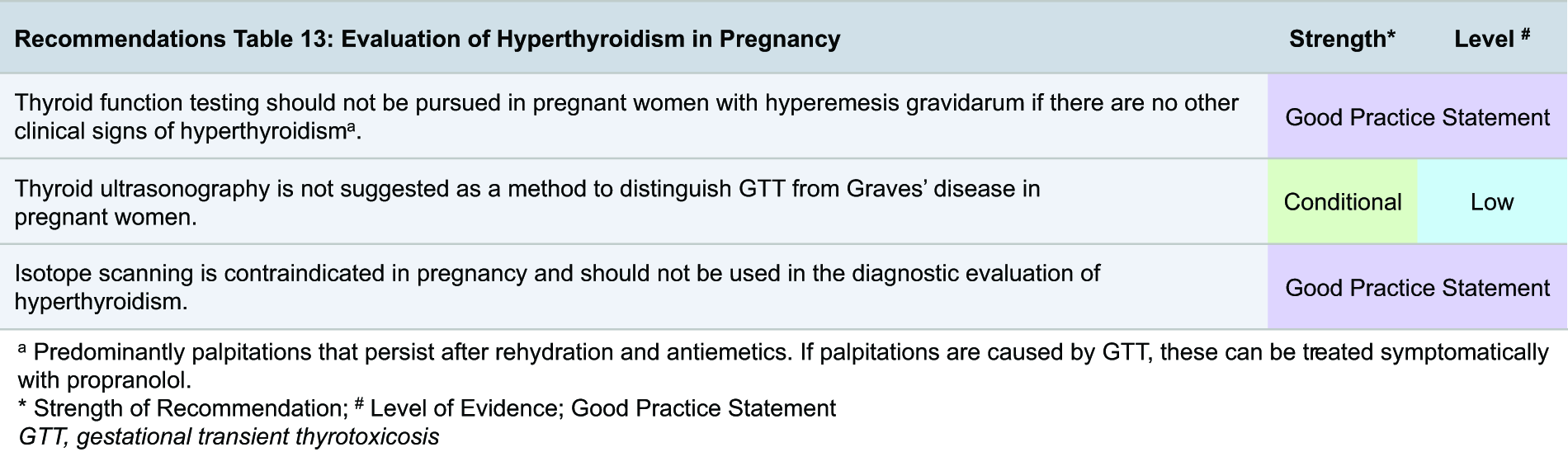
Epidemiology and physiology
A suppressed serum TSH concentration is frequently encountered in early gestation, when the hCG concentration rapidly increases through placental production. Gestational transient thyrotoxicosis (GTT) is the physiological condition resulting from the weak thyroid-stimulating effect of hCG on TSH receptors, typically manifesting as a suppressed TSH and mildly increased fT4 concentrations. Upon the presentation of biochemical hyperthyroidism in pregnancy, GTT should be distinguished from other less common hyperthyroidism etiologies, including (new onset or recurrent) Graves’ disease. Other etiologies of thyrotoxicosis in pregnant women are exceedingly rare and include toxic multinodular goiter and toxic adenoma, the thyrotoxic phases of subacute painful or painless thyroiditis, TSH-secreting pituitary adenoma, struma ovarii, functional thyroid cancer metastases, and germline TSH receptor mutations that are hypersensitive to hCG. 191 Thyrotoxicosis can also result from overtreatment with thyroid hormone replacement or the intentional or unintentional intake of thyroid hormone. 192
The prevalence of GTT varies widely, due to the heterogeneity in the definition of GTT, overlap with other reasons for a suppressed TSH in pregnancy, and the inclusion of women with hyperemesis gravidarum in some studies.8,193,194 It is estimated that the general prevalence of GTT ranges from <1% to 11% during pregnancy, 195 depending on the geographic region. GTT occurs in up to 66% of women with hyperemesis gravidarum. 196 Data on mild hyperthyroidism (usually due to GTT) during pregnancy are reassuring, as it is not associated with higher risks of adverse pregnancy or birth outcomes, such as preeclampsia, gestational hypertension, preterm birth, and small for gestational age.34,160,197,198
Graves’ disease is the most common cause of nonphysiological, pathological thyrotoxicosis in women of childbearing age, occurring in approximately 0.4% of women during preconception and 0.2% during pregnancy. 199 Autonomous thyroid nodules (ATNs), including multinodular goiter, have an estimated yearly incidence of 1–18 per 100,000 among nonpregnant women aged 20–39 years,200,201 while the prevalence of coexisting ATNs and Graves’ disease (termed the Marine–Lenhart syndrome) in nonpregnant individuals was 0.26% in a study from Japan, an overall iodine-sufficient region. 202
Clinical presentation and evaluation
Women may come to attention during preconception and pregnancy for abnormal thyroid function tests checked in response to hyperthyroid symptoms or during routine prenatal care. Guidance for the evaluation of a decreased TSH in women planning pregnancy is summarized in Flowchart 3. Hyperthyroidism found during preconception should generally be evaluated and treated in the same way as in individuals not planning pregnancy, 203 with the added consideration of fertility treatment if applicable.
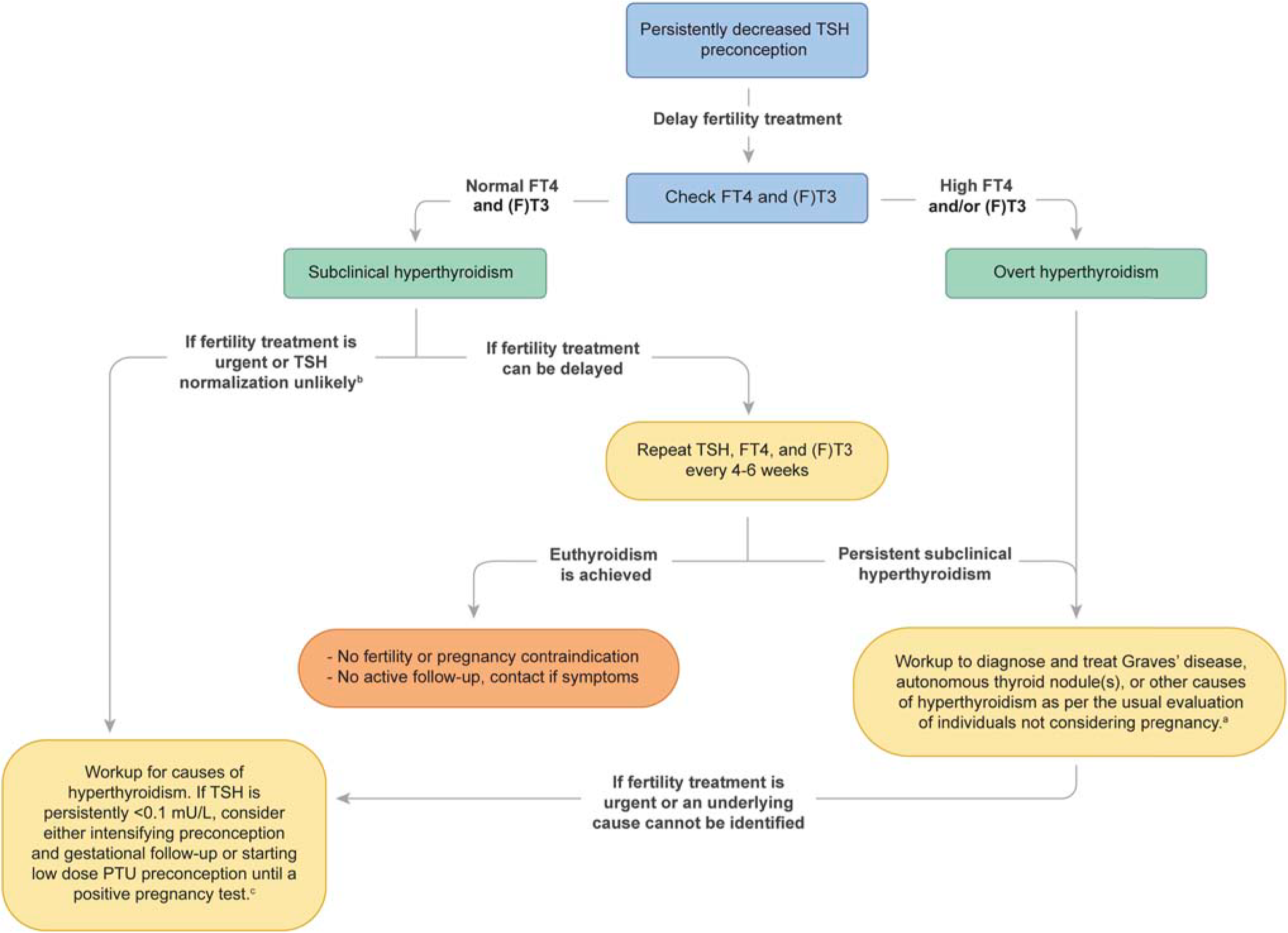
Approach to decreased TSH levels in preconception. Green boxes indicate a diagnosis, yellow boxes indicate an action, and orange boxes indicate recommended follow-up. aIdeally, the treatment for the etiology of hyperthyroidism should be completed and euthyroidism restored (confirmed by two TSH concentrations in the reference range at least six weeks apart) before fertility treatment begins. bFor example, if the TSH has been persistently <0.1 mU/L. cRefer to “Subclinical and Overt Hyperthyroidism in Infertility” in Section E.
The evaluation of hyperthyroidism in a pregnant woman presents distinct challenges. It is important to distinguish Graves’ disease in pregnancy from other causes (Table 2). GTT is more common in states associated with high hCG concentrations, such as early pregnancy, hyperemesis gravidarum, 196 and multiple gestation pregnancies. 198 In contrast, women with untreated Graves’ disease during pregnancy would be expected to have persistently low TSH concentrations, persistently increased fT4 concentrations after the first trimester, 204 and hyperthyroid symptoms that have often times been present before pregnancy. Positive serum TRAb and/or TSI titers, the presence of thyroid eye disease, and a family history of Graves’ disease and/or personal or other family history of autoimmunity also support the diagnosis of Graves’ disease. It should be noted that serum TRAb and TSI concentrations are used interchangeably in this text, as there are no data to show superiority or differences in the upper limit of normal clinical decision cutoffs between the two. In women with hyperemesis gravidarum and no other clinical signs of hyperthyroidism, the relatively frequent occurrence of GTT, as well as the likely absent need for symptom treatment, supports the general lack of benefit of routinely checking serum thyroid function.
Distinguishing Between Gestational Transient Thyrotoxicosis (GTT) and Graves’ Disease
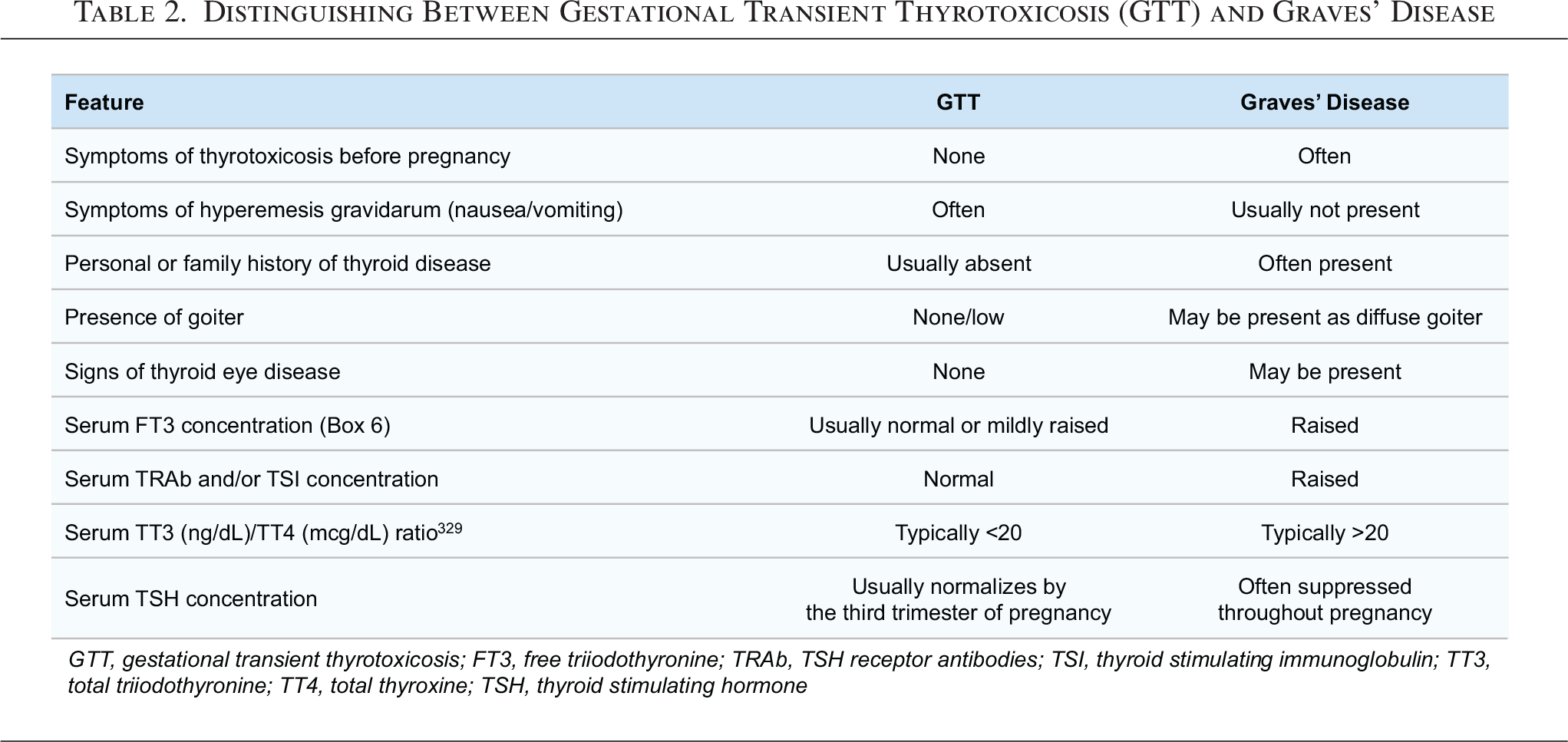
Guidance for the evaluation of a decreased TSH in pregnant women without known thyroid disease is summarized in Flowchart 4. Pregnant women with suppressed TSH concentrations should initially have a fT4 concentration measured, followed by serum TRAb or TSI levels if the fT4 concentration is elevated. A (f)T3 measurement can be considered if the fT4 is normal and distinguishing subclinical hyperthyroidism from overt hyperthyroidism would change management, or to help distinguish the etiology of hyperthyroidism (Box 5 and Table 2). A typical approach to a pregnant woman with a decreased TSH concentration and a concurrently normal fT4 and (f)T3 concentration (i.e., subclinical hyperthyroidism) is to repeat serum thyroid function every two to four weeks until the TSH normalizes (as most cases of GTT will). If subclinical hyperthyroidism persists into the third trimester or evolves into overt hyperthyroidism, additional follow-up and/or reconsideration of the hyperthyroidism diagnosis should be considered. Those with persistent overt hyperthyroidism, particularly after 20 weeks’ gestation, should undergo TRAb and/or TSI testing, followed by treatment or ongoing monitoring as indicated. There is no role of thyroid ultrasonography as a method to distinguish GTT from Graves’ disease in pregnant women owing to their similar thyroidal mechanism of action.
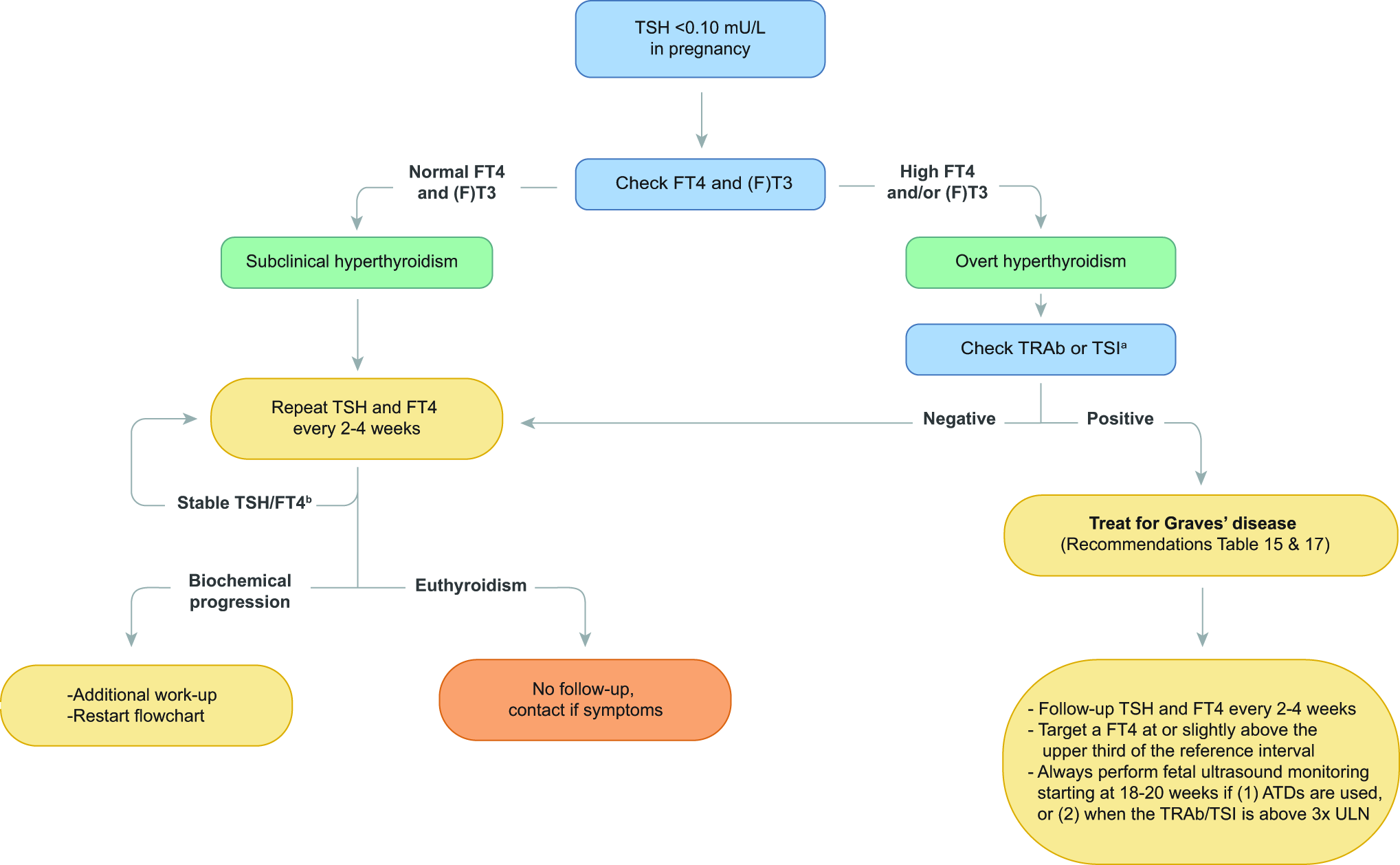
Approach to decreased TSH levels in pregnancy. Green boxes indicate a diagnosis, yellow boxes indicate an action, and orange boxes indicate recommended follow-up. (f)T3 = serum free and/or total T3 (see Box 5 in these guidelines). aFor women with a clear presentation of hCG-induced hyperthyroidism/gestational transient thyrotoxicosis (e.g., with a nonfully suppressed TSH, twin pregnancy, or hyperemesis gravidarum without extrathyroidal signs of Graves’ disease), it is reasonable to follow up with a TSH and fT4 in two to four weeks before checking TRAb and/or TSI. bAssess for a palpable thyroid nodule. If present, then follow biochemical progression and consider ATDs depending on the severity of hyperthyroidism. For example, repeat TRAb and/or TSI, (f)T3 measurement, thyroid ultrasound, and postpartum diagnostic imaging. TSI, thyroid-stimulating immunoglobulin.
For women with preexisting ATNs who become pregnant, there is a lack of rigorous data regarding the patterns of thyroid function changes during gestation, but the physiologically greater thyroid hormone needs during pregnancy may result in gradual improvement of the hyperthyroidism, even potentially resulting in normal thyroid function tests as pregnancy progresses. Thyroid hormone production in individuals with ATNs depends on iodine availability, emphasizing the need to be cautious with excess iodine intake and exposure during pregnancy. It is not possible to confirm an ATN as the etiology of hyperthyroidism in pregnancy, given the inability to perform nuclear medicine uptake and scanning during this period. For the evaluation of hyperthyroidism in lactation, guidance regarding radiopharmaceutical use is found in Section I.
Preconception management of hyperthyroidism (Graves’ disease)
Women of childbearing age with newly diagnosed hyperthyroidism should be assessed for their desire to conceive in the near future. About 20% of women with hyperthyroidism present with menstrual disturbances and hyperthyroidism is associated with reduced fertility, although thyrotoxic women remain ovulatory. 9 In a hyperthyroid woman desiring pregnancy, regardless of the underlying cause, the biochemical goal is to restore and maintain euthyroidism (confirmed by at least two sets of normal thyroid function tests obtained at least six weeks apart) before attempting conception.
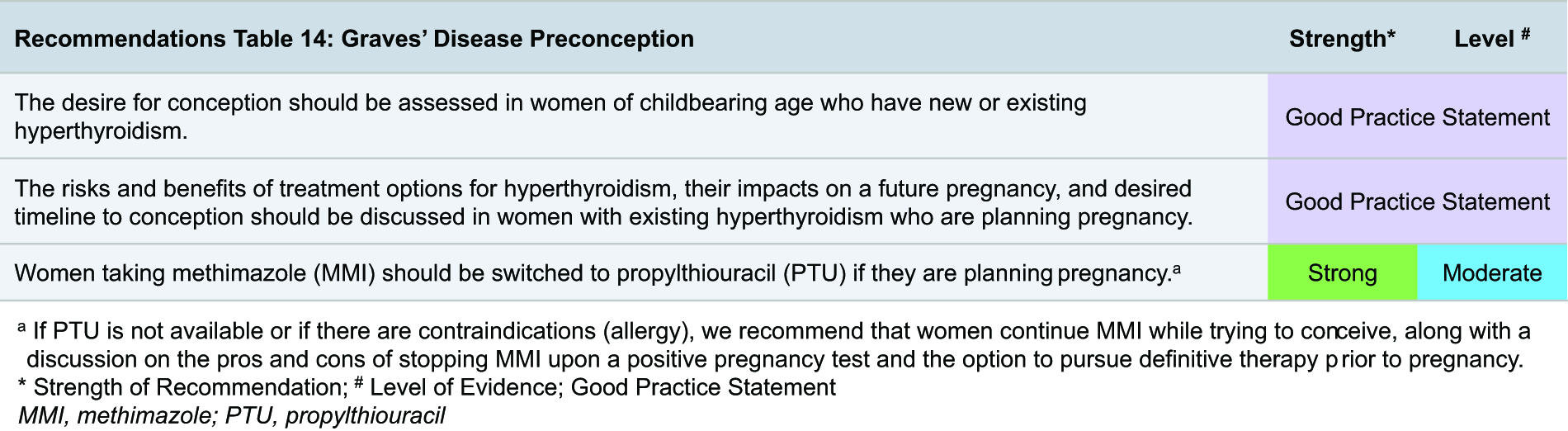
Small studies show that correction of hyperthyroidism improves fertility, although this may be related to the restoration of menstrual cycle regularity. There are no high-quality studies comparing the relative impact of specific treatment modalities for Graves’ disease on fertility; one small prospective study describes the improvement of menstrual irregularity in hyperthyroid women upon ATD initiation. 208 Our understanding of the risks and benefits of thyroid surgery and 131I treatment in Graves’ disease on fertility is primarily derived from their use in women with a history of differentiated thyroid cancer (DTC) (also see Section H), with mostly reassuring findings for effects on ovarian reserve, transient amenorrhea, and pregnancy rates following these therapies.209–212 Although supporting data are limited, it is reasonable to expect that once euthyroid, fertility and fecundity for women with a history of treated Graves’ disease are similar to those without a history of Graves’ disease.
The management of hyperthyroidism due to Graves’ disease during preconception presents unique considerations (Table 3). Options for treatment with ATDs, 131I therapy, or total thyroidectomy should be discussed through a shared decision-making process. The choice and timing of these management decisions should weigh the pros and cons of the treatment options on fertility, the health of a future pregnancy and the fetus, and general maternal health. Women who are already taking methimazole (MMI) should be advised to switch to PTU (if available) once they are actively trying to conceive. If PTU is not available, the lowest effective dose of MMI can be used for the shortest duration possible. The relative risks of MMI and PTU during preconception and pregnancy are discussed below (subsection on ATDs).213–215 While being treated with an ATD, women should be instructed to contact their clinician immediately should they become pregnant.
Advantages and Disadvantages of Treatments for Preconception Graves’ Disease
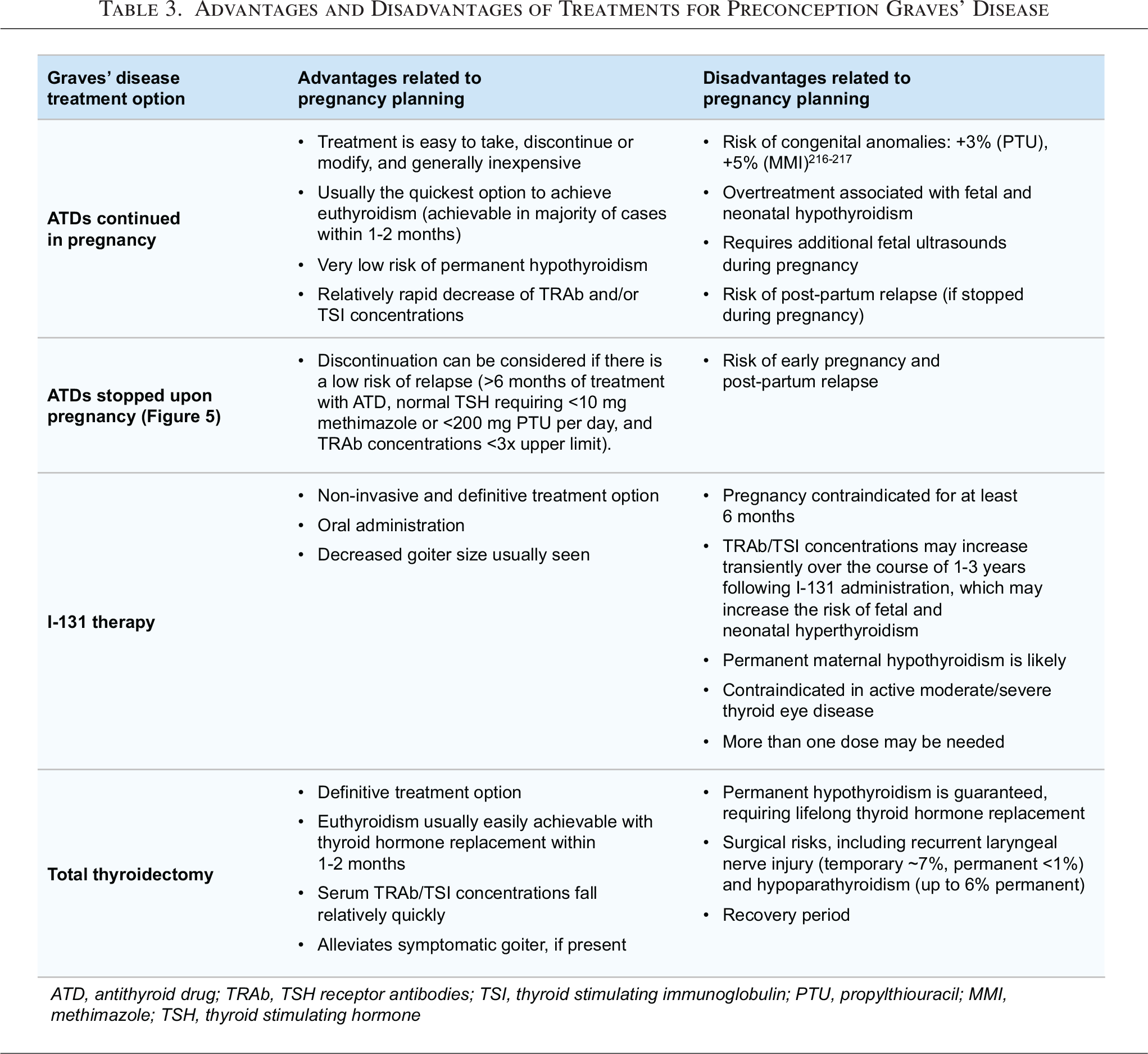
Women with Graves’ disease who are considering radioactive iodine (RAI) treatment before conception should be counseled that serum TRAb and/or TSI concentrations will likely increase after RAI administration, which is associated with an increased risk of fetal and neonatal hyperthyroidism. 213 In pregnancy, however, the risk of fetal and neonatal hyperthyroidism is negligible if the serum TRAb and/or TSI concentrations are <3-fold the upper limit of normal.213,216 Attempting pregnancy could be considered if preconception serum TRAb and/or TSI concentrations are <3× the upper limit of normal or slightly above this threshold as TRAb and/or concentrations are expected to further decline during pregnancy as a result of increased immune tolerance. However, no guidance can be provided on a specific, safe preconception TRAb, and/or TSI concentration cutoff, as the expected decrease of individual TRAb and/or TSI concentrations in pregnancy is difficult to predict. Women who receive preconception 131I treatment for Graves’ disease should be advised to defer pregnancy for at least six months to minimize the potential adverse effects of radiation (as extrapolated from data on 131I treatment for DTC). 217
Finally, some women may elect to undergo total thyroidectomy for the definitive treatment of Graves’ disease before pursuing pregnancy. Postoperative hypothyroidism should be managed with LT4 to ensure stable euthyroidism (confirmed by two consecutive normal thyroid function tests six weeks apart), along with attaining a TRAb and/or TSI concentration that minimizes the risk of fetal/neonatal hyperthyroidism before attempting to conceive.
Gestational management of GTT and Graves’ disease
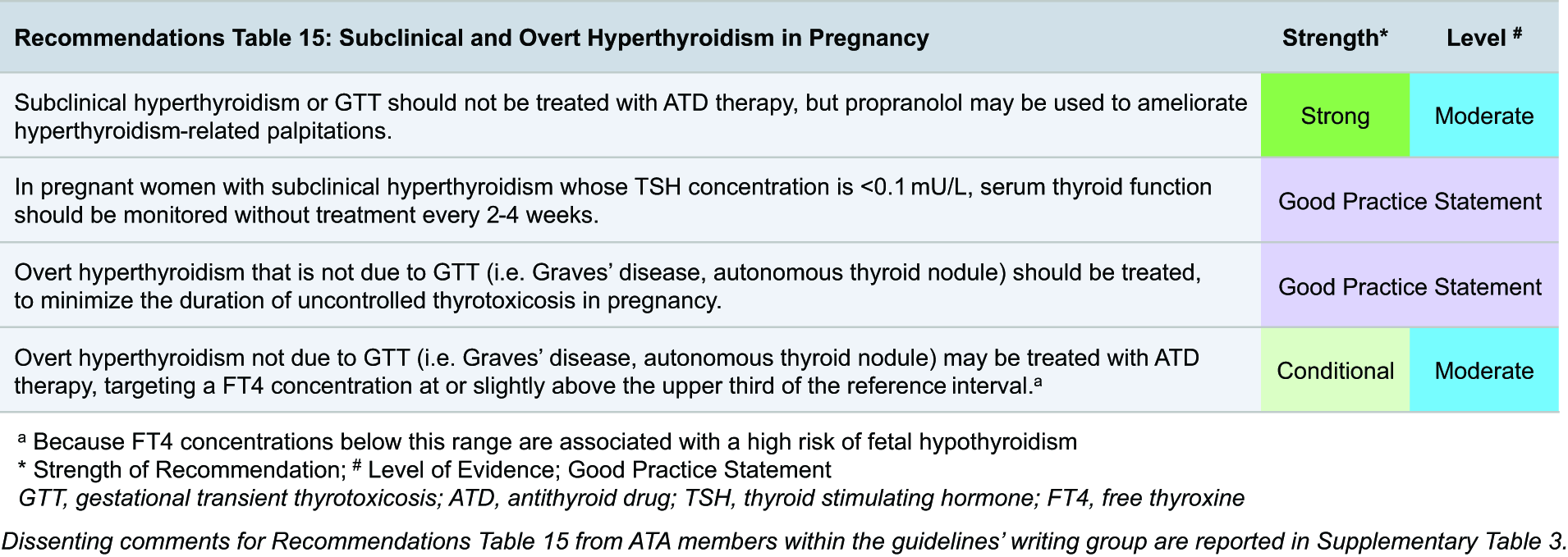
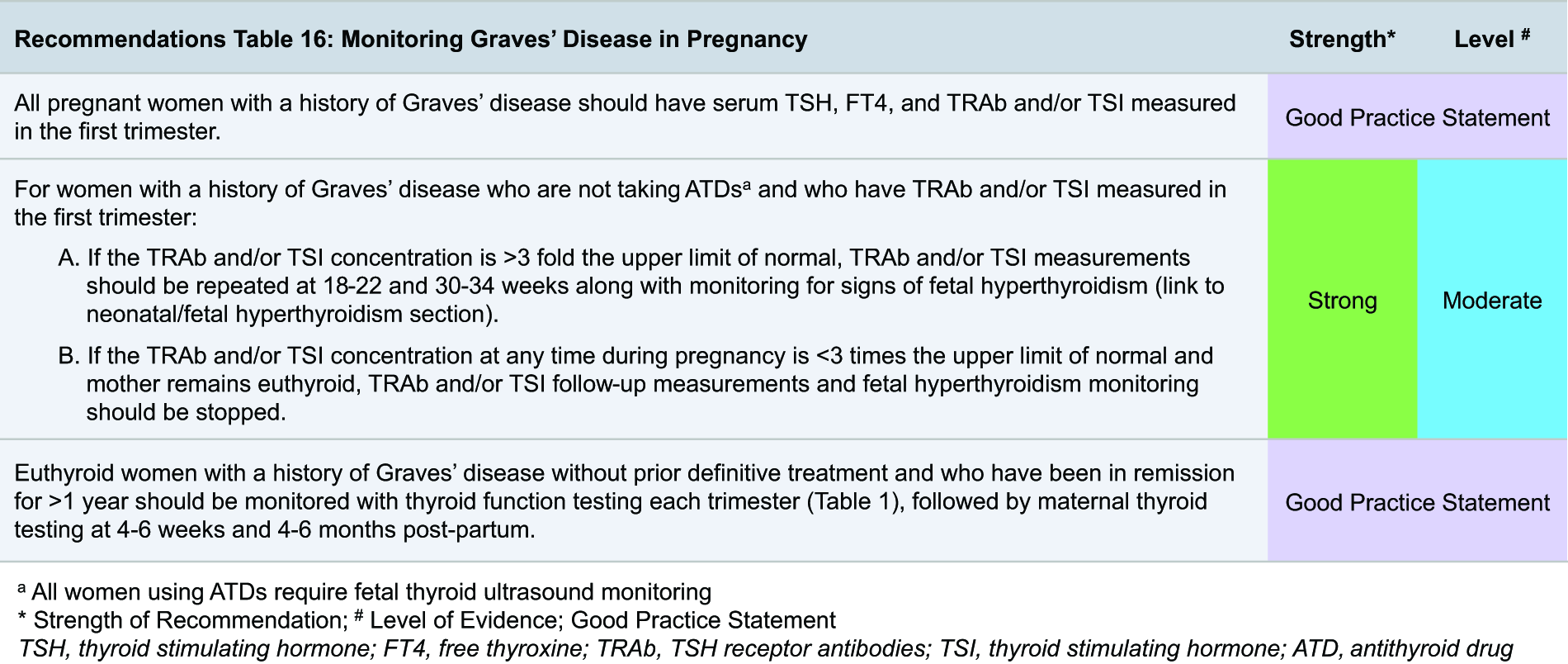
Subclinical hyperthyroidism in pregnant women generally does not require treatment, as the majority of such cases are attributable to GTT. Observational studies have not shown an association between untreated subclinical hyperthyroidism in pregnancy and adverse obstetric outcomes.33,34,160,187,218,219 GTT is typically self-limited and can be managed supportively with adequate hydration, control of hyperemesis if present, and alleviation of thyrotoxic symptoms with propranolol in the same routine doses as those used outside of pregnancy. ATD therapy should generally not be used for the treatment of subclinical hyperthyroidism. If GTT is particularly severe, low-dose PTU could be considered through shared decision-making and counseling about the harms and benefits of its use in pregnancy (see subsection below on ATD use in pregnancy).
For Graves’ disease during pregnancy, the risks of obstetric and medical complications are related to the control of maternal hyperthyroidism and the duration of euthyroidism throughout gestation.222,223 Poor control of thyrotoxicosis caused by Graves’ disease has been associated with pregnancy loss, pregnancy-induced hypertension, intrauterine growth restriction, stillbirth, seizure disorder among offspring,34,204,223–225 and thyroid storm and congestive heart failure in the mother during gestation. 226 In women without Graves’ disease, the association of hyperthyroidism in the first half of pregnancy with adverse pregnancy outcomes is not consistent, and absolute risk differences are small.33,160,204,224,225,227–229 An important difference is that for Graves’ disease, hyperthyroidism is likely more severe and lasts longer. Accordingly, women with Graves’ disease who have overt hyperthyroidism at initial presentation or develop overt hyperthyroidism during pregnancy should be promptly treated, with the main goal to minimize the severity and duration of thyrotoxicosis.
Management options for Graves’ disease in pregnancy (Table 4) include observation alone, ATD therapy, and total thyroidectomy in cases of uncontrollable hyperthyroidism or thyroid storm (Box 6). Limited data suggest that long-term use of saturated solution of potassium iodide (SSKI) may be an alternative option for the management of Graves’ disease in iodine-sufficient populations, particularly if there is a higher risk or contraindications (i.e., allergies) to the usual therapies.96,213,230–232 Fetal thyroid ultrasound, fetal heart rate monitoring, and regular communication with the obstetrician or maternal-fetal medicine subspecialist are key for optimal risk assessment. The combination of persistently positive serum TRAb and/or TSI concentrations without a functioning maternal thyroid gland (such as after thyroidectomy and possibly after RAI therapy if it was administered preconception) can be particularly challenging and may require combined therapy with ATDs (to treat the fetus) and LT4 (to maintain maternal euthyroidism).
Risks and Guidance for Treating Graves’ Disease During Pregnancy
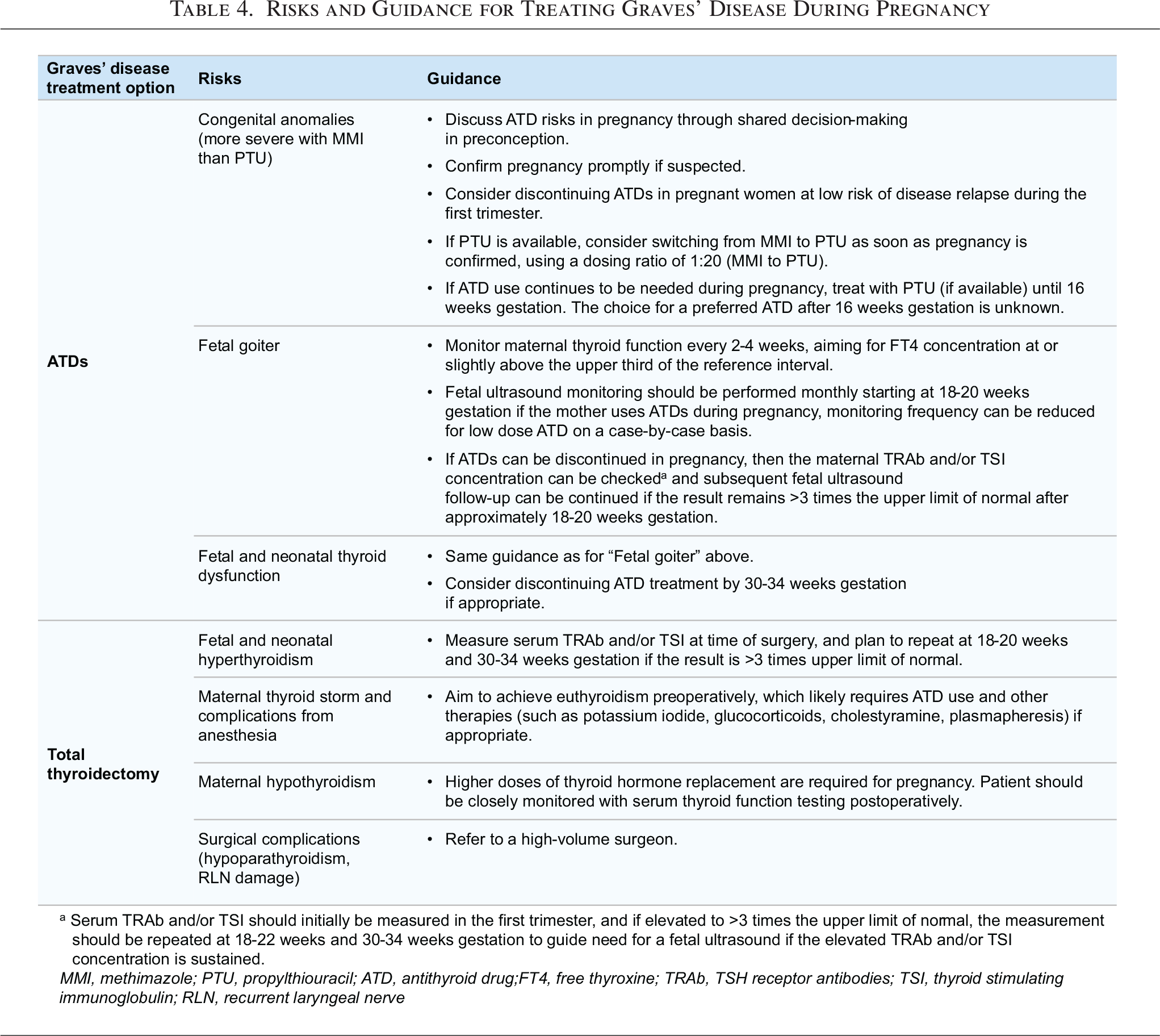
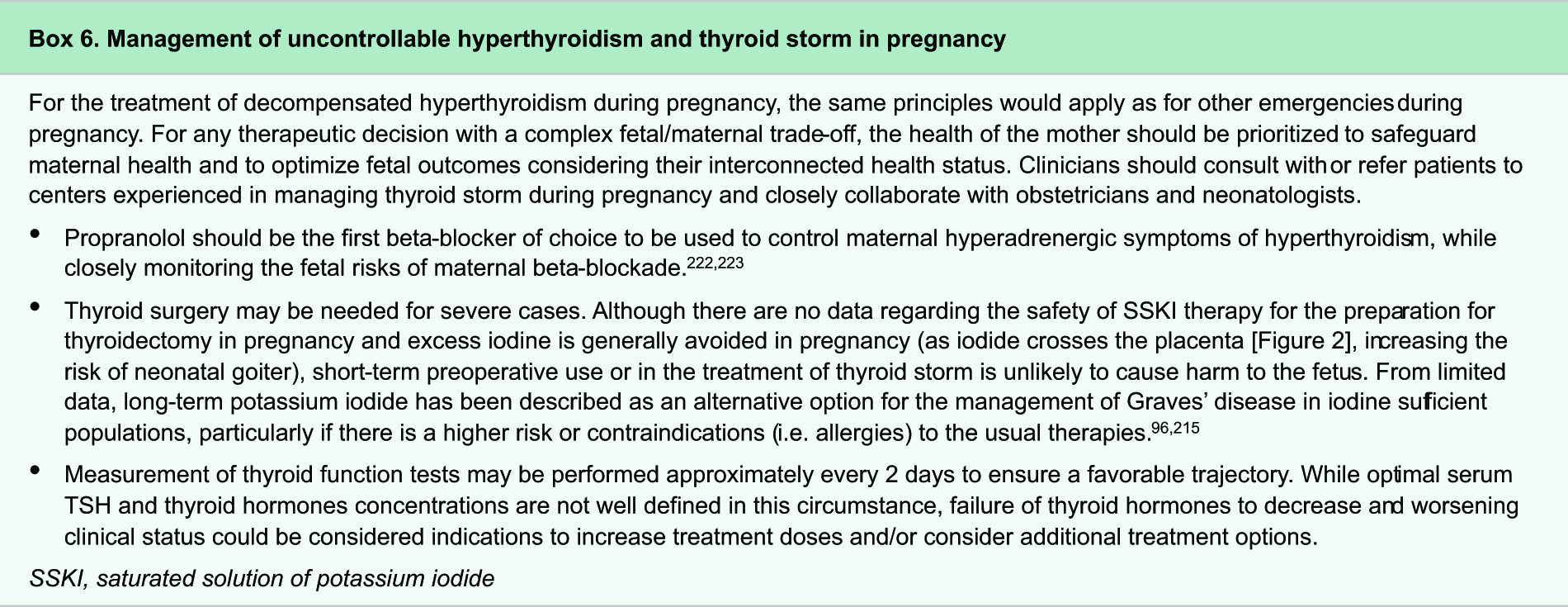
ATD treatment of Graves’ disease in preconception and pregnancy
Women receiving ATD therapy for Graves’ disease should confirm pregnancy promptly if suspected and contact their physician, at which time discontinuation of ATD should be considered (Fig. 5). Upon ATD discontinuation, the risk of Graves’ hyperthyroidism relapse is 30–70%, depending on the duration of treatment and severity of the disease at diagnosis. However, as the average time to Graves’ hyperthyroidism relapse is about three months, there is a good possibility that the teratogenic window has passed when it is necessary to restart ATDs. Small studies have suggested that low-dose ATD use, stable thyroid function for >6 months before pregnancy 233 (preferably with serum TSH >0.35), and negative serum TRAb and/or TSI concentration 234 confer the highest chance of remission after ATD withdrawal. After discontinuing ATDs in pregnancy, serum TSH, fT4, and clinical examination may be monitored every one to two weeks in the first trimester, then every two to four weeks in the second and third trimesters. The choice of which ATD may be the safest to continue should be considered, based on data of ATD risks during pregnancy as discussed below.
Risks of antithyroid drugs during pregnancy. The relative and absolute risks, as well as examples of affected organ systems and severity of congenital malformations, associated with maternal antithyroid drug use during pregnancy are summarized from data reported in two large epidemiological studies. CMZ, carbimazole; MMI, methimazole.
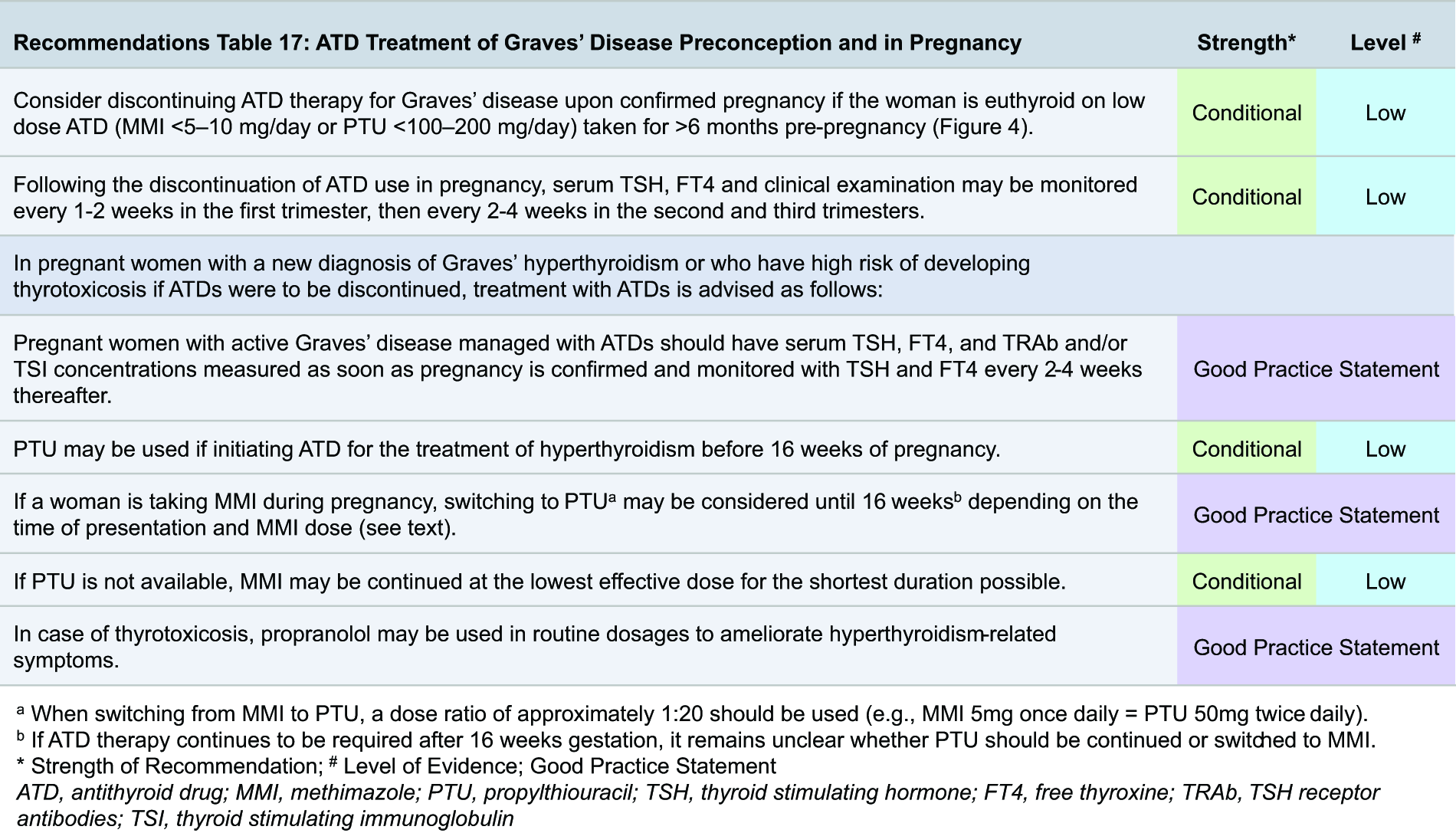
During pregnancy, if the woman is not a candidate for discontinuation of ATDs, she should receive close monitoring with attempts to decrease the dose or even discontinue ATDs in the second half of pregnancy or, in certain cases, be considered for thyroidectomy. Associated risks of continuing ATD use in pregnancy are important to consider, with congenital malformations being the most relevant (Fig. 6). Three large cohort studies from Denmark and South Korea have shown that both carbimazole (CMZ)/MMI and PTU use in pregnancy are associated with a higher risk of embryopathies, compared with women without Graves’ disease.214,215,235 In the South Korean cohort, the absolute risks for the prevalence of congenital malformations per 1000 live births increased by 8.8 cases (CI, 3.92–13.70 cases) in the women who took PTU alone, 17.1 cases (CI, 1.94–32.15 cases) for those who took MMI alone, and 16.5 cases (CI, 4.73–28.32 cases) for those who took both PTU and MMI, compared with pregnant women who were not prescribed an ATD. 215 In addition, the types of abnormalities appear to be milder in those who receive only PTU (i.e., face/neck and urinary tract deformities) compared with those seen with MMI (i.e., deformities spanning seven organ systems; see Fig. 6). 236 Therefore, if PTU is locally available, it is preferred over MMI as ATD therapy in the first trimester.
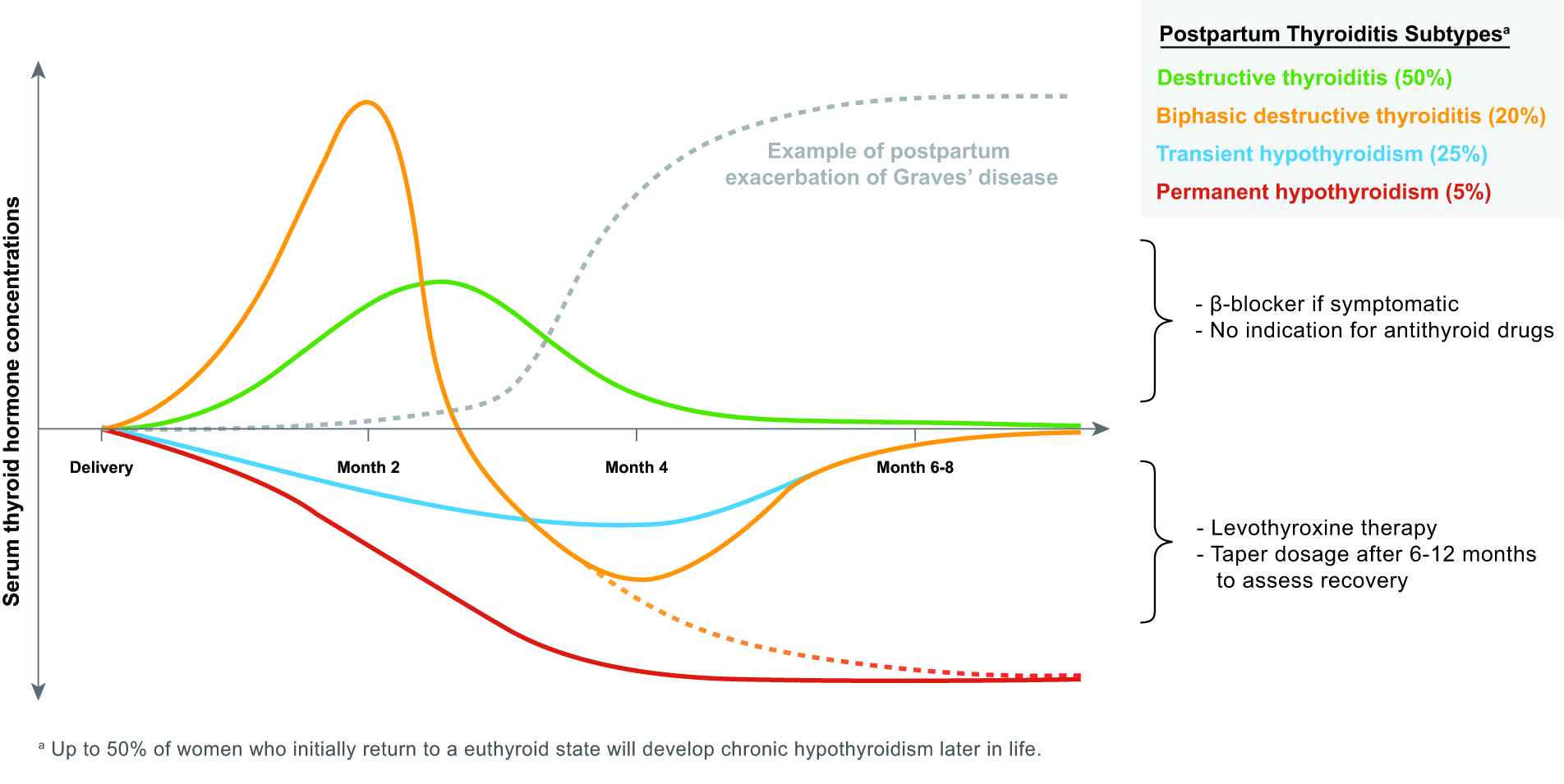
Trajectories of postpartum thyroiditis subtypes. The typical trends of serum thyroid hormone concentrations seen in various subtypes of postpartum thyroiditis are summarized. During the thyrotoxic phases of the destructive subtypes, antithyroid drugs are not indicated, as the underlying etiology is not increased thyroid hormone production (as compared with the postpartum recurrence or exacerbation of Graves’ disease, shown in the gray dotted line). During the hypothyroid phase of thyroiditis, a short course of thyroid hormone replacement may be considered in women with profound symptoms of hypothyroidism, with the plan to taper or stop the dose after 6–12 months.
These studies also showed that the risk of congenital malformations did not differ for pregnancies where MMI was switched to PTU in the first trimester versus those where MMI use was continued throughout the first trimester, suggesting that switching from MMI to PTU may not meaningfully impact the congenital malformation risk.214,215,235 In these studies, the switch to PTU in most women happened well into the first trimester (median time, 44 days from pregnancy start in the Danish study 235 but unknown in the Korean study, as the switch between prepregnancy and first trimester was based on prescription data alone 215 ) after the typical time in which the most sensitive aspects of organogenesis have already been completed. It is therefore possible that MMI exposure in early pregnancy was the driving factor underlying these results. In the Korean study, the cumulative MMI dose of >495 mg and longer duration of its use were associated with increased risk of malformations, whereas there were no such associations for PTU. 215 These data suggest that for those women who continue to require ATD therapy in pregnancy who were not switched to PTU before conceiving, switching from MMI to PTU may lower the risk of congenital abnormalities, especially when switched early in the first trimester or when using a high MMI dose. When switching from MMI to PTU, a dose ratio of approximately 1:20 can be used (e.g., MMI 5 mg/day is equal to PTU 50 mg twice daily). If ATD therapy continues to be required after 16 weeks’ gestation (the time of skin closure), it remains unclear whether PTU should be continued or switched to MMI. As both medications are associated with potential adverse effects and switching between the two may potentially result in a period of suboptimal control, we are unable to make a recommendation regarding the choice of a preferred ATD after 16 weeks’ gestation.
Women who require continued ATD treatment in pregnancy should be closely monitored with thyroid function testing (serum TSH and fT4 as soon as pregnancy is confirmed and every two to four weeks thereafter) and serum TRAb and/or TSI testing in the first trimester. At each assessment, the decision to continue conservative management of Graves’ disease (i.e., holding the ATD and observing) should be guided both by clinical signs/symptoms and thyroid function tests.
Finally, there are limited data on ATD treatment and risks of adverse obstetric outcomes. Both MMI and PTU treatment of Graves’ disease lower the risk of miscarriage, preterm delivery, and low birth weight compared with no use of ATDs or uncontrolled hyperthyroidism despite ATD use. 224 The available data regarding ATD risks in women of childbearing age relate mostly to hepatotoxicity and pancreatitis; although there have been sparse case reports of fulminant hepatic failure associated with PTU use but not MMI in pregnancy, there seem to be no overall differences in hepatotoxicity between women treated with PTU in pregnancy compared with those not exposed to an ATD. 237 There are no data regarding the risks of agranulocytosis and pancreatitis in pregnancy, but they are likely to be similar to those of nonpregnant populations.238–240 Baseline liver function tests and a white blood cell count should be obtained whenever an ATD is started, similar to the recommendations for ATD use in nonpregnant individuals. 203
Thyroid surgery for Graves’ disease in pregnancy
The decision to recommend total thyroidectomy for Graves’ disease in pregnancy should be reserved only for exceptional circumstances. 222 Indications include a severe intolerance to ATDs or the inability to control hyperthyroidism with maximum doses of ATDs, which could result in life-threatening hyperthyroidism to the mother and/or hyperthyroidism or hypothyroidism in the fetus (e.g., the latter is more likely if high-dose ATDs are needed to control maternal hyperthyroidism, as in cases of thyroid storm in pregnancy). If thyroid surgery is required imminently, β1-selective blockers should be used to the extent needed to control maternal hyperadrenergic symptoms of hyperthyroidism, and other therapeutic options (such as potassium iodide, glucocorticoids, cholestyramine, plasmapheresis) should be considered on a case-by-case approach in a multidisciplinary setting, also taking into account general drug preferences during pregnancy (e.g., using hydrocortisone instead of dexamethasone). Women should be counseled that there are increased risks of surgical complications with thyroid surgery during pregnancy, compared with the nonpregnant state; better surgical outcomes of thyroidectomy during pregnancy are associated with operations performed by high-volume surgeons, compared with low-volume surgeons. 241

Risk of Graves’ disease relapse in pregnancy
Limited data suggest that euthyroid women in pregnancy with a history of remitted Graves’ disease have generally similar risks of adverse pregnancy and offspring outcomes to those without a Graves’ disease history, with the exception of increased fetal and neonatal hyperthyroidism risks213,242 in women who have persistently increased serum TRAb and/or TSI concentrations (which may occur after a total thyroidectomy or previous preconception 131I treatment).224,225
For women with a history of Graves’ disease that is in remission following previous treatment, disease recurrence is rare due to pregnancy-specific immune tolerance, especially if serum TRAb and/or TSI titers are less than threefold the upper limit of normal.213,216 Although women with a history of Graves’ disease that is now in remission (including those who have received a course of ATD) have a low risk of Graves’ disease relapse in pregnancy, they should have continued monitoring of thyroid function each trimester and postpartum after three to six months or when developing new thyrotoxicosis symptoms.
Risks of fetal and neonatal hyperthyroidism associated with maternal Graves’ disease
The risks of fetal and neonatal hyperthyroidism are related to maternal TRAbs that cross the placental barrier (Fig. 2) through the neonatal fragment crystallizable receptor (FcRn) and stimulate the fetal thyroid gland. Monitoring for fetal and neonatal hyperthyroidism should be performed if the TRAb and/or TSI concentrations are above three times the upper limit of normal. This also includes, for example, euthyroid pregnant women with a history of past Graves’ disease who were definitively treated with a total thyroidectomy or 131I. In particular, risks of fetal and neonatal hyperthyroidism are higher in cases when the woman received 131I therapy within two years of conception, as the maternal TRAb concentrations are likely to still be elevated. 243 The indications for monitoring of fetal and neonatal hyperthyroidism in pregnant women with Graves’ disease are summarized in Table 5.
Monitoring Fetal and Neonatal Hyperthyroidism in Pregnant Women with Active or Past History of Graves’ Disease
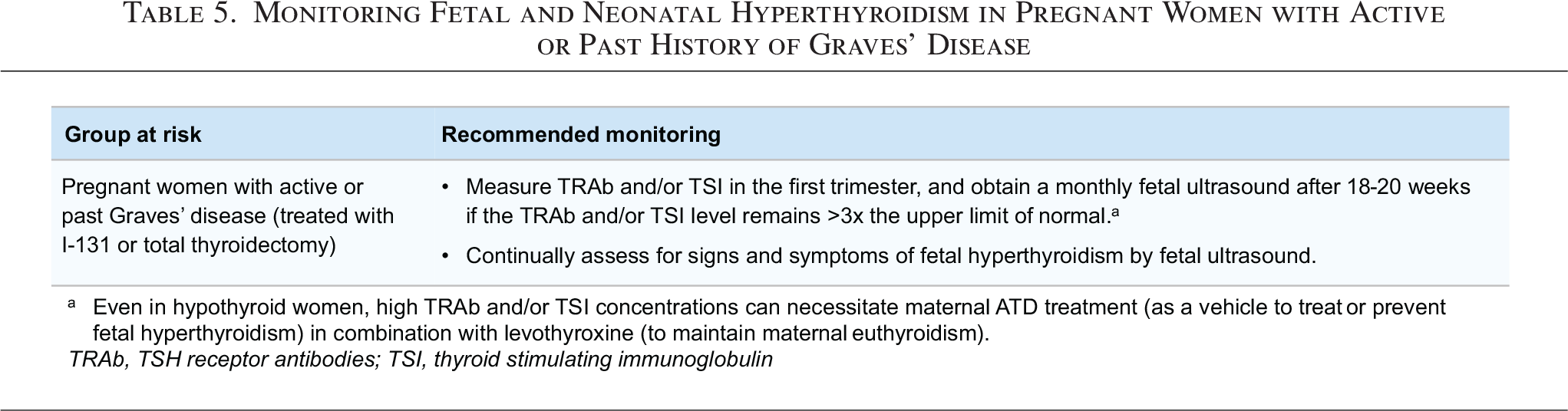
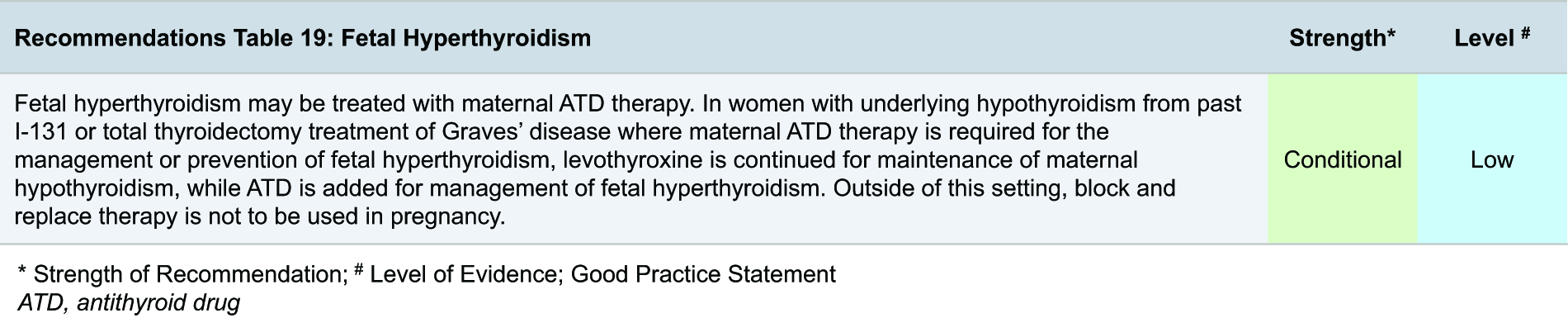
Signs of fetal and neonatal hyper- and hypothyroidism are summarized in Tables 6A and 6B. If fetal goiter is found by ultrasound but the diagnosis remains unclear, amniotic fluid or umbilical cord sampling may be considered at 20–24 weeks’ gestation. Although umbilical blood sampling better reflects fetal thyroid status than amniotic fluid sampling,244–246 it is associated with a 1–2% risk of fetal death, 247 and its benefits must be weighed against this risk. Meanwhile, amniotic fluid sampling is associated with a 0.1% risk of rupture of membranes, and normal fetal thyroid function tests obtained through this route do not completely exclude fetal thyroid dysfunction. 248 All cases of fetal and neonatal hyperthyroidism are considered high-risk pregnancies and should be managed by a multidisciplinary team.
Signs and Symptoms of Fetal and Neonatal Hyperthyroidism (A) and Hypothyroidism (B)
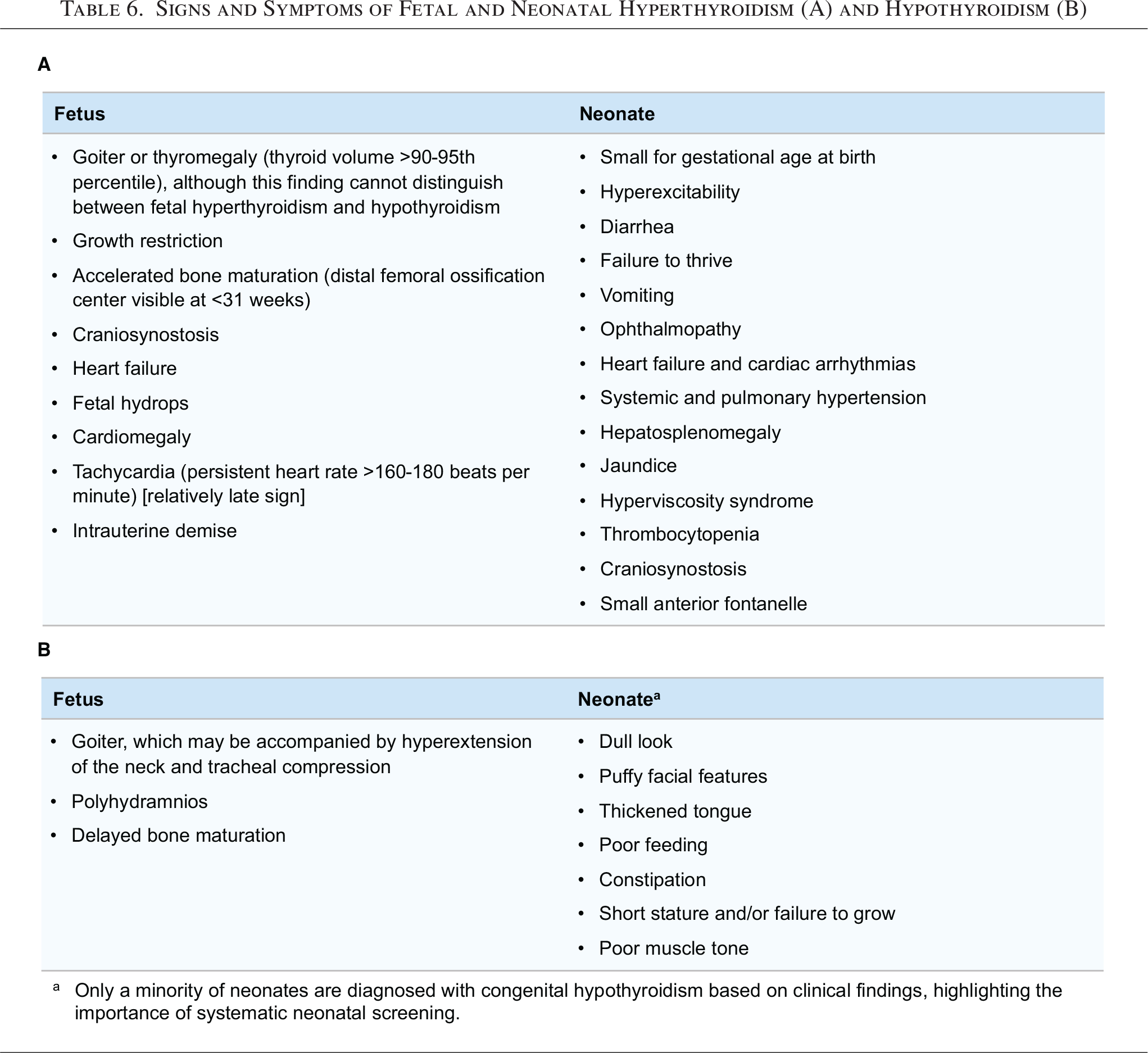
For confirmed cases of fetal hyperthyroidism, treatment largely consists of maternal ATDs. In women already receiving LT4 replacement for iatrogenic hypothyroidism from past 131I treatment or thyroidectomy, maternal ATDs should be given in addition to LT4, as ATDs cross the placenta to impact the fetal thyroid gland (Fig. 2).
Infants born to women with Graves’ disease who have maternal serum TRAb concentrations >3× upper limit of normal should be closely followed and monitored for neonatal thyroid dysfunction.216,243 If the mother is receiving ATDs, their infants may be initially euthyroid at birth but can become thyrotoxic when the effect of the ATDs dissipates, due to the relatively longer half-life of TRAb and/or TSI compared with that of ATDs. Risk assessment and follow-up strategies should be made in a multidisciplinary setting involving the endocrinologist, obstetrician, maternal fetal medicine subspecialist, and pediatrician. Neonatal Graves’ hyperthyroidism may require ATD treatment and may present with fluctuating hypothyroidism or hyperthyroidism in case of combined stimulating and blocking TRAb. However, treatment is likely to be short-term, as remission of neonatal Graves’ disease is common by 20 weeks of life, 249 and remission by 48 weeks after birth is nearly always observed. 250 Neonates born to a mother with poorly controlled Graves’ disease may also develop primary or central hypothyroidism that would require LT4 replacement at birth or upon withdrawal of maternal ATD use.251–253
Postpartum management of Graves’ disease
In the postpartum period, there is a swift normalization of the immune system after the period of prolonged immune tolerance in pregnancy. While serum TRAb and TSI concentrations in women with Graves’ disease decline gradually during pregnancy, they are anticipated to increase in the postpartum period, thereby conferring a 25–55% estimated risk of Graves’ disease relapse after delivery. 254 In addition, some data, though not all, report an increased prevalence of new-onset Graves’ disease in the postpartum period.255–258 Guidance on the evaluation and management of hyperthyroidism during lactation can be found in Section I.
Autonomous thyroid nodules
Epidemiology and physiology
Overt hyperthyroidism may arise from the presence of an ATN during pregnancy, although this is exceedingly rare. There are no robust data on the risks of adverse pregnancy outcomes in women with ATNs. It is relevant to note that in women with an ATN (either with or without ATD treatment), the maternal thyroid function is not a marker of fetal thyroid status (which is opposite to women with Graves’ disease, because in hyperthyroidism due to an ATN, there are no TRAb/TSI that stimulate fetal thyroid hormone production).
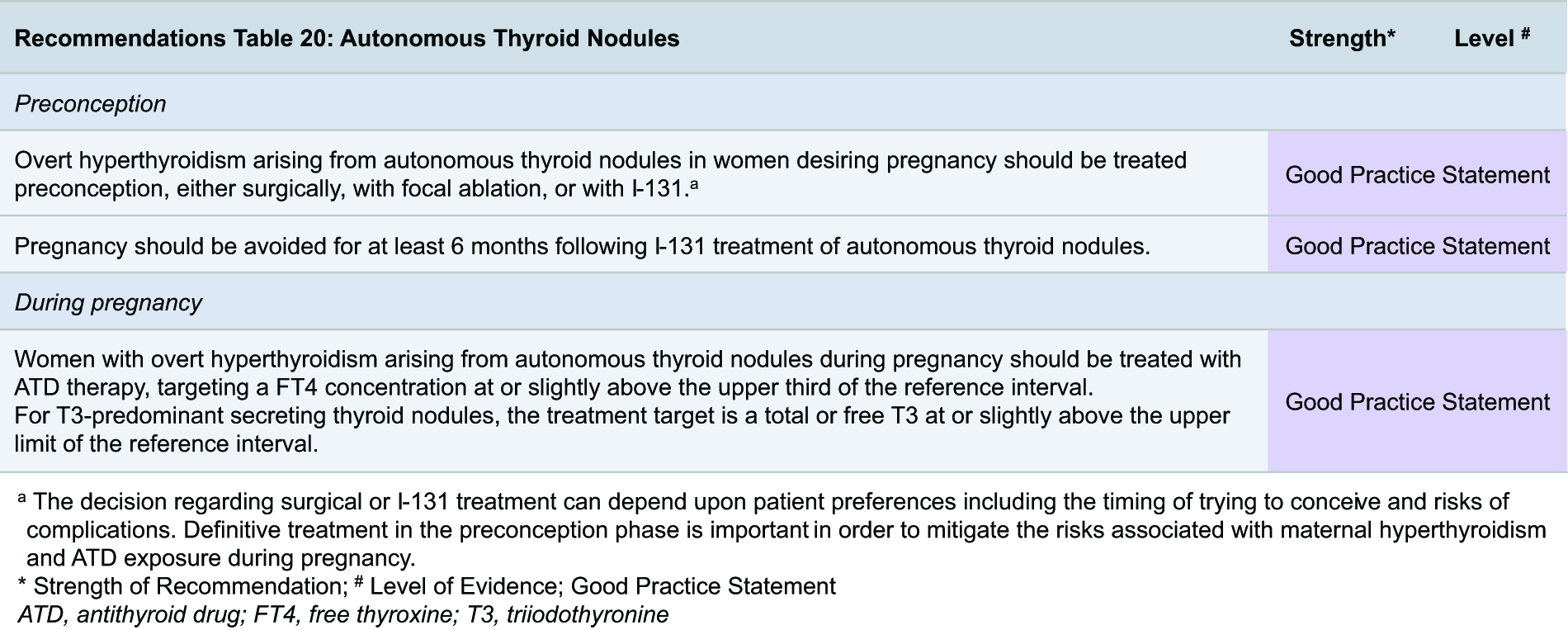
Clinical presentation and evaluation
The evaluation and definitive treatment of hyperthyroidism arising from a suspected ATN is difficult during pregnancy and, therefore, should ideally be completed prior to conception. In the rare case when an ATN is suspected during pregnancy, biochemical evaluation and clinical suspicion are the primary diagnostic tools, as thyroid scintigraphy is contraindicated. The typical presentation is the identification of a thyroid nodule by palpation that is associated with persistent suppressed TSH or hyperthyroidism after the first trimester in TRAb and/or TSI negative pregnant women, which may take the form of predominant T3 thyrotoxicosis. In the postpartum setting, guidance about radiopharmaceutical use for the diagnostic evaluation of ATNs during lactation is found in Section I.
Treatment and management
Women with overt hyperthyroidism due to ATNs should be advised to undergo definitive therapy before conception. There are limited data regarding treatment-specific effects for ATNs on future fertility outcomes, pregnancy outcomes, or fetal/child outcomes. Overt hyperthyroidism arising from autonomous thyroid nodules in women desiring pregnancy should be treated preconception, either surgically, with focal ablation, or with 131I. If thyroid surgery is pursued, the woman should be counseled to have at least two consecutive postoperative normal thyroid function tests obtained at least six weeks apart before conceiving. Pregnancy should be avoided for at least six months following 131I treatment of ATNs, owing to a higher risk of miscarriage and birth defects (as extrapolated from data on 131I treatment for DTC). 217 Also after 131I treatment, stable thyroid function (at least two consecutive postablative normal thyroid function tests obtained at least six weeks apart) should be confirmed before conceiving. ATDs would not provide definitive correction of the hyperthyroidism arising from ATNs and, similar to guidance for the general population, 203 should not be used as long-term therapy in women desiring pregnancy.
During pregnancy, remission of hyperthyroidism resulting from ATNs is not expected, in contrast to Graves’ disease, although the hyperthyroidism may become quiescent due to concurrently increased thyroid hormone needs during gestation. The available evidence regarding treatment options for hyperthyroidism resulting from ATNs during pregnancy is limited, but therapy should largely be medical. During the first trimester, beta-blocker treatment at the lowest effective dose may be used for symptomatic control, and considerations similar to those for GTT can be applied. Should the overt hyperthyroidism from ATNs be persistent, particularly after the first trimester, ATD treatment may be considered, weighing the risks of untreated or undertreated maternal hyperthyroidism against the risks of fetal and neonatal thyroid dysfunction. If employed, ATD therapy should be given to target serum fT4 concentrations to the upper third of the reference interval or slightly above, 207 along with monthly fetal ultrasound monitoring. The fetus is at higher risk of developing hypothyroidism with maternal ATD therapy given for an ATN, compared with Graves’ disease, due to the absence of TRAb and/or TSI in this scenario, which would have counteracted the effect of ATD on the fetal thyroid.
Thyroid surgery for the treatment of ATNs should be reserved in pregnancy only for exceptional circumstances, 222 similar to the surgical indications of Graves’ disease in pregnancy. It is important to note that previous hemithyroidectomy or RAI treatment is an indication for TSH testing upon a positive pregnancy test (Table 1). Finally, there is emerging evidence regarding the safety and efficacy of using minimally invasive techniques such as RFA and ethanol ablation in the treatment of ATNs in pregnant patients. One case series described the restoration of euthyroidism following percutaneous ethanol injection therapy in 2 pregnant women with ATNs, 259 which could be considered in refractory cases or if the risks of using ATDs outweigh the benefits. There are limited studies reporting the use of thermal ablative techniques (during pregnancy preferentially with a bipolar probe or monopolar probe and grounding pad) in this setting, and their comparative efficacy and safety during pregnancy versus thyroid surgery are unknown. Treatment of ATNs using 131I is contraindicated in pregnancy. Guidance about radiopharmaceutical treatment of ATNs during lactation is found in Section I.
H. Thyroid Nodules and Cancer Preconception, In Pregnancy, and Postpartum
Thyroid nodules and thyroid cancer found during preconception, pregnancy, and lactation present unique challenges to both the clinician and the mother. Weighing the pros and cons of pursuing a more immediate plan to make a definitive diagnosis and potentially implement treatment, versus delaying these decisions to either after pregnancy and/or the peripartum period, is pivotal. Shared decision-making is needed to determine which diagnostic tests and treatment interventions should be performed more urgently and to what extent they may adversely impact the mother, fetus, and/or maintenance of pregnancy if carried out. Due to the general absence of high-quality evidence regarding the evaluation and management of women with thyroid nodules and thyroid cancer during preconception, pregnancy, and lactation, this committee has generally combined the available low-quality data in pregnant women with practice recommendations that are in place for nonpregnant individuals to provide guidance on this topic.
Epidemiology and physiology
Observational studies drawn from both iodine-deficient and -sufficient regions report a similar prevalence of thyroid nodules between pregnant and nonpregnant women,260,261 with estimates ranging from 9% to 33% upon screening, but of which only a minority (∼6%) are clinically significant. 262 Greater age, 263 and associated with this, higher parity, 264 are the most relevant risk factors for the detection of a thyroid nodule during pregnancy. For thyroid nodules detected during pregnancy, their size, total number, and frequency of suspicious sonographic features are similar to those of nonpregnant women. 261 Limited data suggest that the prevalence of nonautonomous thyroid nodules increases with each trimester of pregnancy. 263 There are no rigorous data regarding the prevalence of ATNs in pregnant women, but it is understood that they are generally more likely to be present in those living in iodine-deficient regions. 265 ATNs (including multinodular goiter) have an estimated yearly incidence of 1–18 per 100,000 among nonpregnant women aged 20–39 years.200,201
In women with a known history of or new diagnosis of thyroid cancer prior to pregnancy, most of the literature supports that pregnancy itself does not adversely affect overall thyroid cancer outcomes. The size of a thyroid tumor may increase slightly during pregnancy, but the increase is usually not clinically significant.266,267 Diagnosis during pregnancy does not appear to be associated with the presenting stage of thyroid cancer, 268 and for most patients diagnosed with DTC during pregnancy, delaying treatment until postpartum does not appear to impact achieving an excellent response to therapy. 269 Furthermore, the physiology of pregnancy does not appear to be associated with thyroid cancer progression or recurrence in pregnant women with DTC who have previously received initial treatment (i.e., surgery with or without RAI therapy). The risks of recurrence, clinically significant progression of DTC, and progression-free and overall survival are generally similar between nonpregnant patients and pregnant patients who have a history of or are diagnosed with DTC during pregnancy.270–273 Progression of DTC during pregnancy is predicted by the presence of a structurally or biochemically incomplete response to therapy at the time of conception, 274 similar to the considerations of DTC risk used for the nonpregnant patient. Women at high risk for disease progression or immediate complications during pregnancy include those with distant metastatic disease and/or grossly invasive DTC on neck ultrasound or other imaging.
Clinical presentation and evaluation
Thyroid ultrasonography remains the most accurate and sensitive tool for the detection or confirmation of a palpated thyroid nodule in women during preconception or pregnancy. Upon discovery of a thyroid nodule, serum TSH should be measured to rule out possible hyperthyroidism arising from an autonomously functioning thyroid nodule. The definitive diagnosis of an autonomously functioning thyroid nodule cannot be made during pregnancy, given the contraindication to any radioisotope use, including scintigraphy and the common occurrence of physiological (subclinical) hyperthyroidism (Section C).
For nonfunctioning thyroid nodules detected during preconception and pregnancy, evaluation for malignant risk is generally similar to that of nonpregnant individuals. Obtaining a history of risk factors for thyroid cancer, as well as assessment for any relevant syndromic or familial risks, should be performed. There is a possible positive association between higher parity and the risk of thyroid cancer, but this is likely not clinically significant, and studies are complicated by residual confounding factors (age, breastfeeding, thyroiditis, obesity, other factors).275,276 If indicated by sonographic risk criteria, fine-needle aspiration (FNA) biopsy to evaluate the malignant potential of a thyroid nodule should be completed prior to pregnancy. The patient may be counseled to maintain contraception until the planned evaluation and/or treatment are complete, although the clinical suspicion for advanced disease and possible decreased reproductive potential of the patient should be weighed in this consideration. If the patient is pregnant when a nodule is identified, FNA biopsy may be performed after shared decision-making, taking into account subsequent management options of its results.
The anticipated slight enlargement of the thyroid gland during pregnancy (especially during the first trimester)261,263,277 should be considered when evaluating the malignant risk of a thyroid nodule. For nontoxic thyroid nodules, the sonographic risk of malignancy (estimated by tools such as the ATA thyroid nodule risk stratification system 278 and American College of Radiology Thyroid Imaging Reporting and Data System criteria) 279 is not different between pregnant and nonpregnant individuals. However, since overall survival appears not to differ if surgery is performed during or after delivery in pregnant women with thyroid cancer, patient preference for the timing of FNA biopsy (i.e., during pregnancy or postpartum), as well as sonographic features, should be taken into account. For pregnant women who undergo FNA biopsy and are found to have a cytologically indeterminate thyroid nodule, pregnancy is neither associated with a higher rate of malignancy nor the initial stage of thyroid cancer.268,271,280 As molecular marker tests of cytologically indeterminate thyroid nodules have not been validated for use in pregnancy, their diagnostic performance is unknown in this setting.
Management of benign thyroid nodules
Recommendations for the management of ATNs during preconception and pregnancy are discussed in Section F. Appropriate evaluation and treatment (thyroid surgery and/or thermal ablative therapies) of benign, nonfunctional thyroid nodules should ideally be completed prior to pregnancy (refer to the ATA 2026 thyroid nodule guidelines). While thyroid surgery does not change the outcome of a future pregnancy, untreated or incompletely treated postoperative hypothyroidism and hypocalcemia secondary to permanent maternal hypoparathyroidism would increase the obstetrical and offspring risks of pregnancy (see Section F). For pregnant women with nonfunctional thyroid nodules that become symptomatic during pregnancy (e.g., associated compressive symptoms to the anterior neck or rapid nodule growth), shared decision-making should weigh the risks and benefits of these therapies during pregnancy.
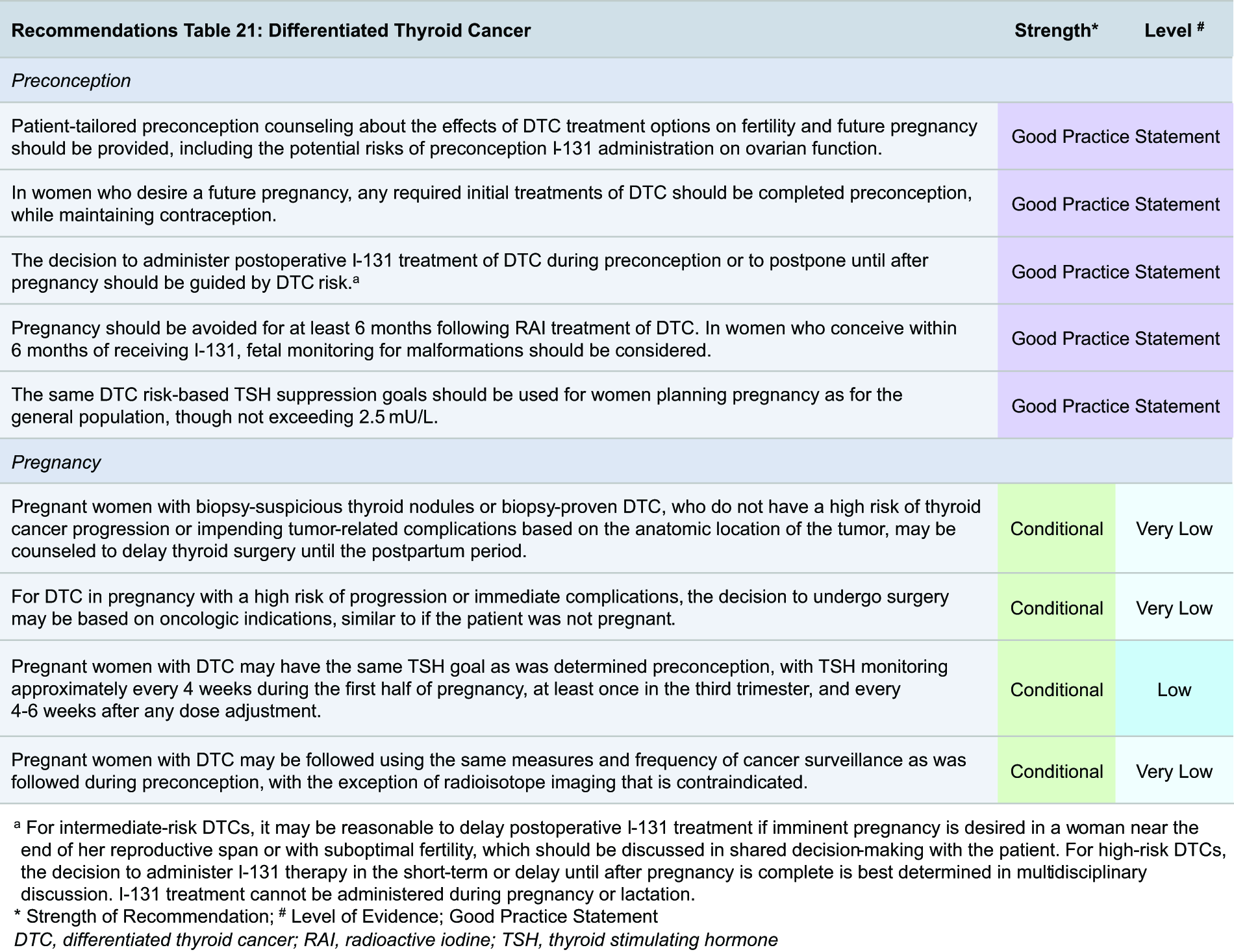
Management of DTC preconception and in pregnancy
Women of childbearing age with a new diagnosis of DTC who desire pregnancy should be counseled on the potential effects of thyroid cancer treatment (e.g., the extent and risks of thyroid surgery, possible postoperative 131I treatment, and extent of TSH suppression) on fertility and future pregnancy (Tables 7 and 8). Data regarding the efficacy and safety of ablative and targeted systemic therapies in this population are extremely limited.
Guidance for the Management of DTC Preconception
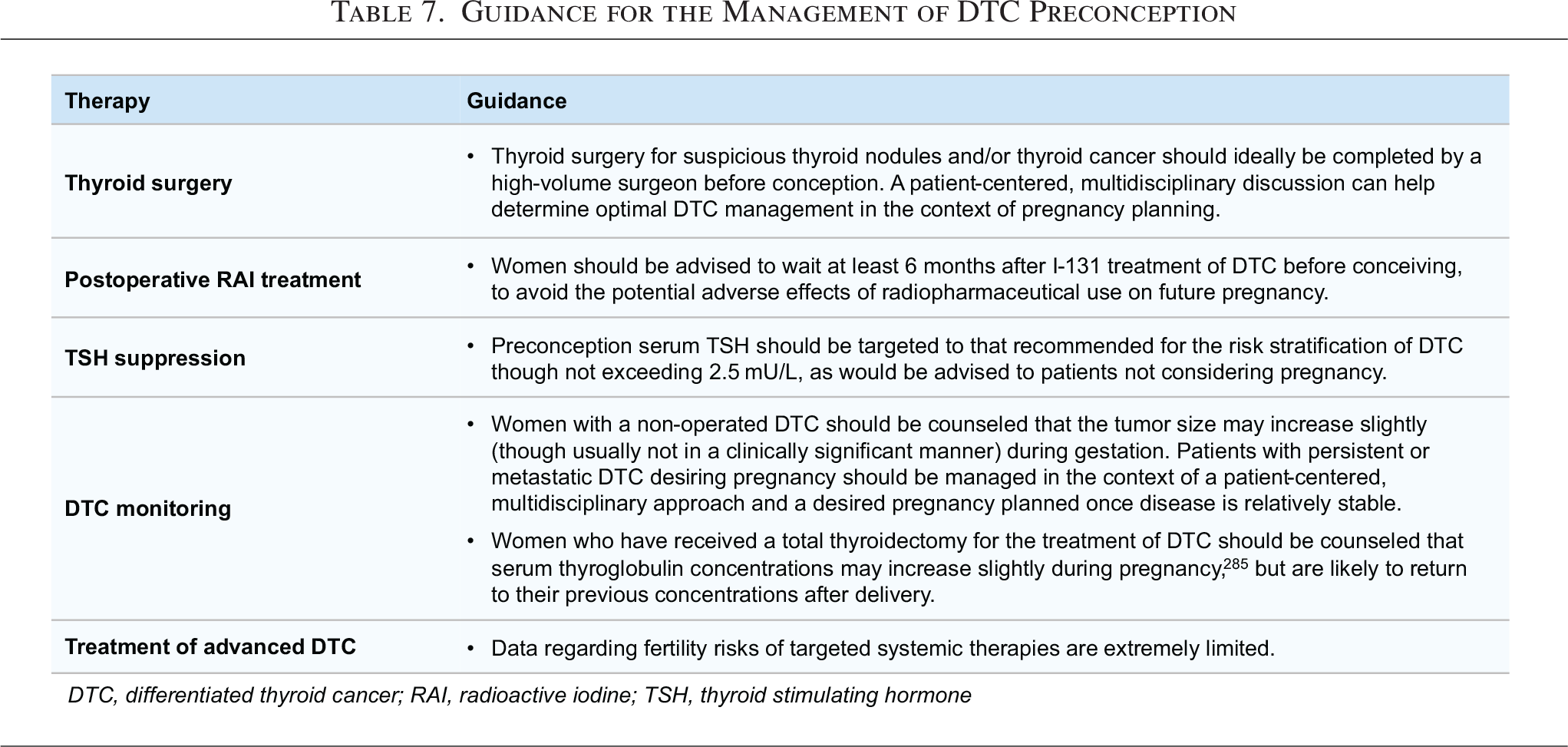
Guidance for the Management of DTC in Pregnancy
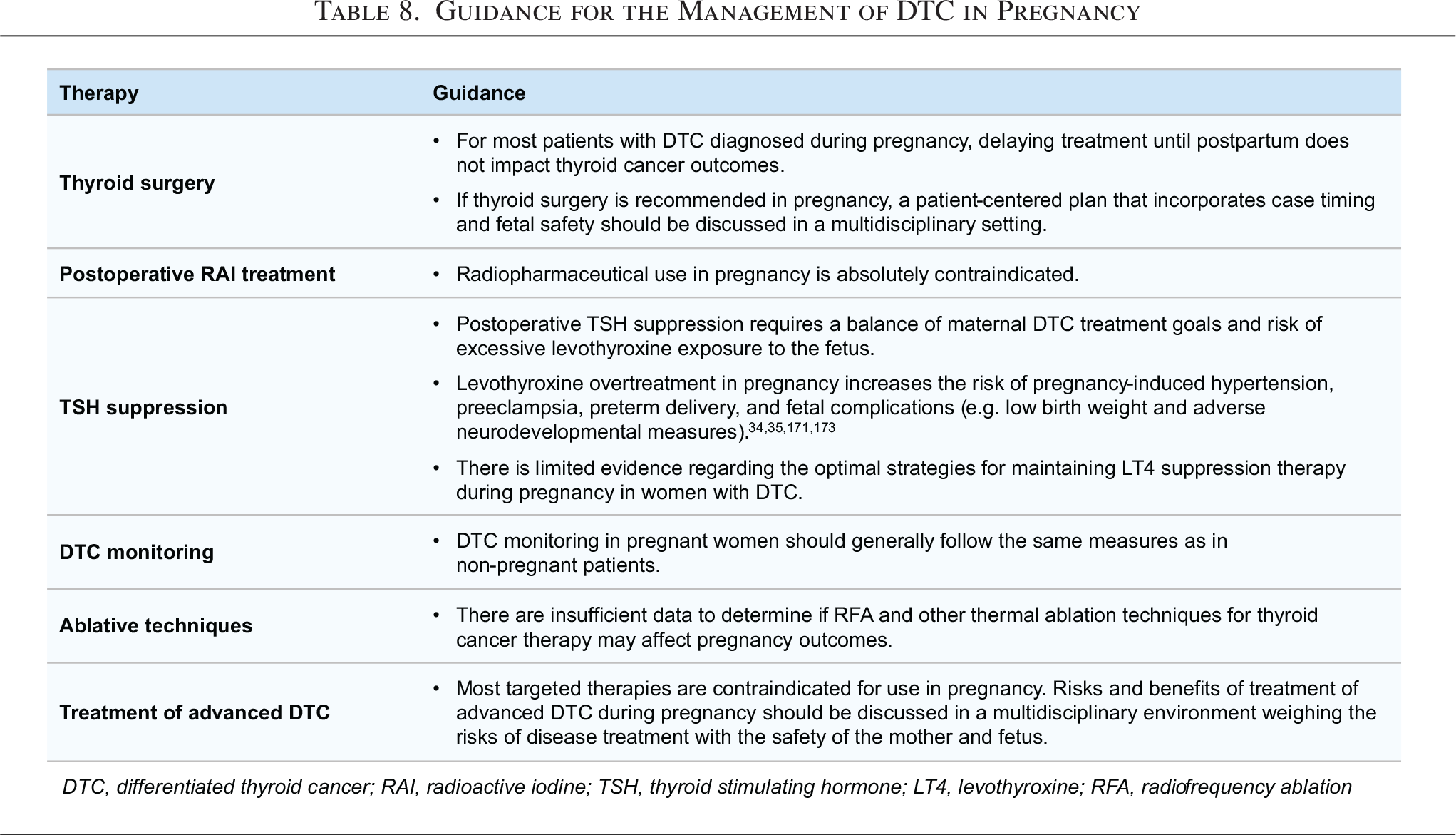
In women undergoing IVF/ICSI, limited data suggest that prior treatment of papillary thyroid cancer (PTC) is associated with a reduction in the number of retrieved oocytes per cycle and a lower number of high-grade embryos compared with women who have not received treatment for PTC, in analyses adjusted for age, BMI, concomitant fertility factors, and ART protocols. 281 One small study has reported that women undergoing IVF/ICSI were more likely to have a clinical pregnancy or live birth following hemithyroidectomy, compared with those who had a total thyroidectomy. 282 Otherwise, there appear to be no independent risks from postoperative RAI treatment or TSH suppression on ART outcomes. No data are available regarding the potential risks of advanced DTC therapies (i.e., targeted systemic therapies) in women undergoing ART.
Thyroid surgery
Surgery for thyroid nodules and/or thyroid cancer during preconception is generally considered safe and is not associated with the health of a future pregnancy. 284 In women with biopsy-proven DTC who have not yet undergone treatment and who become pregnant, there is typically little urgency to perform immediate thyroid surgery before delivery. The vast majority of low-risk DTC (microPTCs) monitored by active surveillance remains stable in size or even becomes smaller during the gestational period, with only 8% growing ≥3 mm during gestation. 267 Therefore, for most women diagnosed with DTC during pregnancy, it is generally reasonable to delay thyroid surgery until the postpartum period for the benefit of both the mother and fetus. If there is a high risk of thyroid cancer progression or impending complications from the tumor, urgent thyroid surgery can be safely performed regardless of trimester, 285 although the second trimester remains preferred, with the surgical plan ideally discussed in a multidisciplinary setting to optimize case timing and fetal safety. Preoperatively, for pregnant women already receiving LT4, the dose may be increased by 25–50 mcg/day, depending on their body weight and preoperative TSH level. For pregnant women who are not already taking LT4 and planned to undergo a hemithyroidectomy, starting LT4 50 mcg once daily either immediately postoperatively or upon the results of a TSH measurement 4 weeks after surgery may be considered. For pregnant women who are not already taking LT4 and planned to undergo a total thyroidectomy, LT4 should be started immediately after thyroid surgery at 1.5–1.7 mcg/kg/day, plus an additional 20–30% dose increase as required for gestation.
Permanent hypoparathyroidism may occur in up to 7% of patients undergoing total thyroidectomy, with a higher risk in patients with thyroid cancer, those undergoing neck dissection, and those undergoing thyroidectomy with a low-volume surgeon. 286 Hypoparathyroidism can be a risk for obstetric complications, such as preterm birth and congenital anomalies compared with women without hypoparathyroidism. 287 Maternal hypocalcemia due to hypoparathyroidism can result in fetal secondary hyperparathyroidism with bone demineralization, uterine contractions, and increased risk of miscarriage. 288 These potential maternal and fetal complications should be considered when planning the extent of thyroid surgery in patients desiring pregnancy.
Postoperative 131I treatment
The considerations regarding the optimal timing of postoperative 131I treatment in women who wish to conceive relate primarily to fertility and pregnancy outcomes. Studies of individuals with DTC have inconsistently shown that a slight delay of 131I administration (defined as >3 months postsurgery) may increase the risk of an incomplete response to DTC treatment,289,290 although there do not appear to be any differences in overall survival.291–293 Limited studies report inconsistent associations between the administration of 131I and ovarian reserve (as defined by serum anti-Müllerian hormone [AMH] concentrations). A meta-analysis 211 showed lower AMH concentrations212,294–296 and slightly earlier menopause after RAI administration in some studies, including in women aged >35 years compared with those aged <35 years and in women who have received multiple 131I treatments, while other data report that postoperative RAI remnant ablation and TSH suppression do not appear to impact the efficacy of ART or result in lower serum AMH concentrations ascertained at 3–12 months after 131I treatment for DTC. 282 Reassuringly, permanent ovarian failure is extremely unlikely after 131I treatment. 297
Observational studies have reported lower pregnancy rates among women who received 131I ablation for DTC, compared with those who have not received 131I,298,299 while other data show that there are no differences in pregnancy rates nor increased risks of miscarriage, preterm birth, stillbirth, or congenital malformations related to the use of 131I.211,300,301 Data suggesting the association between pregnancy loss and 131I administration may be related to the timing of 131I treatment. Some studies have shown increased rates of pregnancy loss occurring within the first 12 months after 131I administration (although many did not distinguish between spontaneous or therapeutic abortion), 300 while a large population-level South Korean study showed that pregnancy loss is observed only if conception occurs <6 months after 131I administration. 217 Although there does not appear to be an increase in congenital anomalies among women who conceive within six months of 131I therapy for thyroid cancer, 301 the higher rates of abortion may conceal the true risk of congenital anomalies, and these data must be interpreted in the context of a patient’s baseline obstetric risk. Finally, there is a lack of conclusive evidence regarding the impact of 131I treatment on later offspring development and growth, regardless of whether women undergo ART or conceive naturally following the 131I dose. Taken together, current evidence suggests that waiting at least six months after 131I treatment before attempting pregnancy would alleviate most pregnancy-related risks associated with 131I administration. The potential impacts of 131I administration on fertility and on later offspring adverse effects are less clear.
TSH suppression
Pregnancy planning is best done when the serum TSH concentration is at the target goal of DTC management that was established preconception,302,303 while taking into account the considerations surrounding thyroid surgery as summarized above in the “Thyroid Surgery” subsection. Women with DTC who have already undergone thyroid surgery and become pregnant should continue LT4, but balancing the potential maternal oncologic risks of inadequate TSH suppression and excess T4 exposure to the fetus requires thoughtful clinical care and monitoring. It has been understood that mildly decreased TSH concentrations during pregnancy may be similar to the physiological effects of hCG and that subclinical hyperthyroidism rarely poses a risk to pregnancy. 218 However, there are newer data that suggest possible risks if preconception TSH concentrations (i.e., measured 6–12 months before pregnancy) are abnormal. In two large population-level observational studies, abnormal TSH concentrations (defined in this cohort as <0.10 or >2.49 mU/L) in women during preconception were associated with delayed time to achieve pregnancy and increased risks of spontaneous abortion, preterm birth, small for gestational age, birth defect, and perinatal infant death.103,104 Preconception TSH concentrations <0.1 mU/L, but not those above, were associated with a longer time to pregnancy over a one-year period. 104 In general, it is reasonable to target the same TSH goal in pregnancy as was determined preconception, according to risk stratification of the DTC, and monitor TSH with the same frequency as in the pregnant woman without DTC (see Section F).
Monitoring of DTC during pregnancy
Given the evidence presented above demonstrating that the physiology of pregnancy does not appear to be associated with clinically significant progression of DTC or progression-free or overall survival,270–273 DTC monitoring in pregnant women should generally follow the same measures as nonpregnant patients. Women with structural or biochemical DTC or metastatic disease have similar risks of progression during pregnancy as nonpregnant women.270,304 Furthermore, disease progression during pregnancy can be predicted by disease behavior prior to pregnancy. 305 These considerations should be discussed with a multidisciplinary treatment team to permit reasonable monitoring during pregnancy in such patients. Women with grossly invasive DTC on neck imaging preconception are at the highest risk for disease progression or immediate complications during pregnancy, similar to these risks in nonpregnant individuals.
Treatment of advanced DTC with targeted systemic therapies
There are insufficient data to determine if therapies for advanced thyroid cancer may affect fertility or pregnancy outcomes. Data on the use of thermal ablative techniques, including RFA, ethanol ablation, and laser ablation, for the treatment of thyroid cancers in pregnancy are extremely sparse.
Management of thyroid cancer in lactation
Although there are fewer direct risks of maternal DTC treatment options to the breastfed infant compared with the fetus during pregnancy, several considerations are pertinent to consider. Thyroid surgery performed during lactation is considered generally safe, as only clinically insignificant amounts of anesthetic drugs are transferred into breastmilk and are not thought to pose a danger to the breastfeeding infant. Current guidelines from the United States and United Kingdom advise that lactating women who undergo surgery can begin breastfeeding as soon as they are awake enough to hold the baby, 285 which is different from prior recommendations advising the disposal of breastmilk for 24 hours after receiving anesthesia. Considerations regarding postoperative 131I ablation and the treatment of maternal postoperative (± postablative) hypothyroidism in breastfeeding women are discussed in Section I.
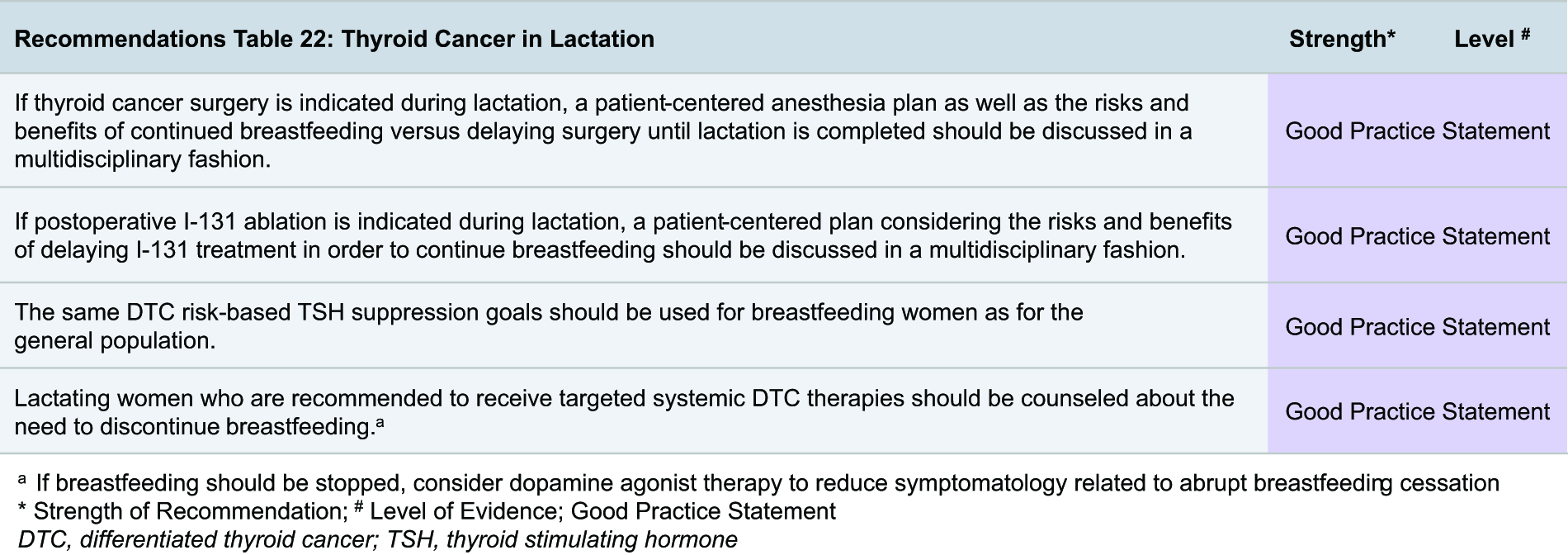
Finally, there are no data on the use and safety of RFA for the treatment of thyroid cancer during lactation. The concentrations of targeted systemic therapies in human breastmilk, or if there may be adverse effects of maternal targeted therapy use on breastmilk production or the health outcomes of the breastfed child, also remain unknown. Serious adverse reactions of maternal use of these therapies to the breastfed infant remain an undetermined possibility.
Medullary and advanced thyroid cancers
The relatively rare scenario of a newly diagnosed medullary or advanced thyroid cancer in a pregnant woman requires careful consideration, balancing the risks and benefits of treatment options during this critical life stage. All decisions should be made in the context of a multidisciplinary team, including a maternal fetal medicine subspecialist if available, on a case-by-case basis, weighing the risks and benefits to the mother and the fetus.

Clinical presentation and evaluation
Serum calcitonin testing in the setting of a thyroid nodule should only be performed if there is a specific indication to do so (i.e., family history of either medullary thyroid carcinoma, MEN2, or a known RET gene mutation). Of note, relevant positive history and physical examination findings in a pregnant woman with thyroid nodules could be related to genetic abnormalities (i.e., MEN2, Cowden’s disease, familial adenomatous polyposis, Carney complex) and may be an indication for newborn screening. The presentation of a poorly differentiated or anaplastic thyroid cancer in a woman during preconception or pregnancy is expected to be similar to that of the general patient with advanced thyroid cancers.
Treatment and management
Patients with MTC should be advised to undergo usual treatment, including thyroid surgery and any recommended genetic testing, prior to pregnancy. The risk of MTC progression in pregnant patients who have received their initial treatment preconception is similar to that of nonpregnant women; thus, the same surveillance strategies can be applied in pregnancy. However, it is important to note that serum calcitonin concentrations may be altered during pregnancy. Studies of serum calcitonin concentrations followed longitudinally in pregnant patients without MTC are inconsistent; while some report that calcitonin remains similar to the nonpregnant patient, 306 others report significant calcitonin elevation during the second trimester of pregnancy that continues through lactation. Serum calcitonin concentrations can increase as much as two to three times the upper limit of normal during pregnancy and remain elevated during the postpartum period, especially if breastfeeding.86,307,308 In contrast, serum carcinoembryonic antigen concentrations appear to remain stable during pregnancy and may be a more reliable tumor marker until lactation is complete. The pentagastrin stimulation test for patients with suspected MTC and normal serum calcitonin concentrations is contraindicated in pregnancy. 309
Data on patients with unresectable or poorly differentiated/anaplastic thyroid cancer or metastatic MTC desiring conception or during pregnancy are scarce. It is generally advisable, when possible, to apply the same urgency to the treatment of poorly differentiated/anaplastic thyroid cancer in pregnant women as in nonpregnant women. External beam radiation therapy can be considered in the setting of a locally advanced thyroid cancer, with a preference to use this treatment during the first trimester to minimize fetal exposure. Based on animal studies, tyrosine/multikinase inhibitors have the potential to cause fetal harm when administered in pregnancy. The pregnancy risks of checkpoint inhibitors used to treat some thyroid cancers are classified as either the inability to rule out harm (as seen with ipilimumab) or even fetal death (as seen with anti-PD1 inhibitors) in animal studies, with extremely limited human data reporting an increased risk of prematurity and low birth weight with their use. 310 The World Health Organization pharmacovigilance database of 91 pregnancies exposed to immune checkpoint inhibitors in pregnancy to June 2022 reported no increased incidence of adverse pregnancy, fetal, and/or newborn outcomes, compared with other anticancer treatments. 311 As the available human data regarding the potential effects of these drugs are sparse, pregnant women should be advised on the risks of embryotoxicity, fetotoxicity, and teratogenicity. These agents should generally not be advised in most pregnant patients, but in those with advanced disease, their potential benefits in stabilizing tumor burden may outweigh their exposure risks.
I. Thyroid Dysfunction Postpartum
Postpartum thyroiditis
PPT is defined as a characteristic pattern of (transient) autoimmune thyroid dysfunction occurring within 12 months after delivery, although it may also occur after a pregnancy loss (Fig. 7). The classic triphasic pattern of PPT, similar to other forms of thyroiditis, comprises an initial period of destructive thyrotoxicosis arising from painless release of preformed thyroid hormone from the inflamed thyroid gland, usually appearing between one and six months postpartum. This is followed by a hypothyroid phase that usually occurs between four and eight months postpartum, in which typical symptoms of hypothyroidism may occur in some individuals, and is followed by the last phase when there is gradual restoration of euthyroidism over another two to three months.
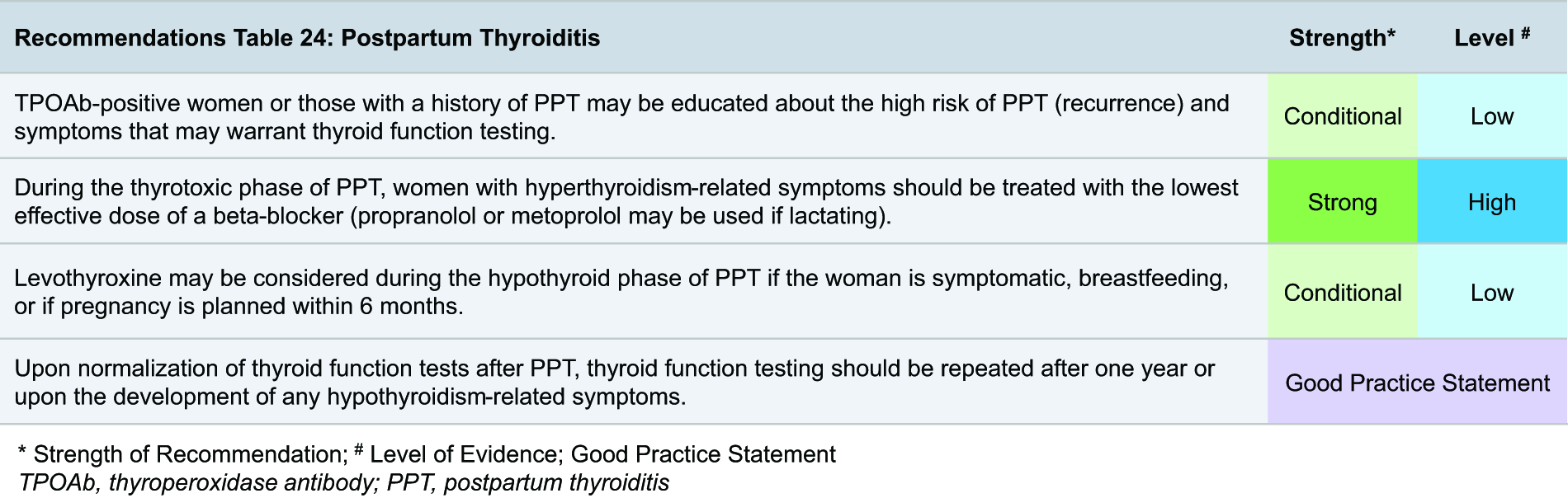
Epidemiology and physiology
The estimated prevalence of PPT is 8%, although this estimate is based primarily on observational studies that have focused on clinically apparent disease, 312 much of PPT is likely to be unidentified. Risk factors for developing PPT include a history of PPT, known thyroid autoimmunity (as defined by serum TPOAb positivity 313 or heterogeneous echotexture by thyroid ultrasound), personal history of autoimmune disease, and a family history of autoimmune thyroid disease. The most prominent risk factor is TPOAb positivity (in studies assessed in the first trimester), increasing the risk of PPT to 33–50%. 314 The autoimmune basis of PPT reflects the rebound of the immune system seen in the postpartum period, when the relative immune suppression of recent pregnancy is no longer present. Women with a history of PPT have a 70% risk of recurrent PPT in a future pregnancy 315 and should be appropriately counseled if further pregnancies are desired. In longitudinal studies, 10–50% of women in whom the hypothyroid phase of PPT initially resolves will ultimately go on to develop permanent hypothyroidism.316,317
Factors associated with an increased risk of developing permanent hypothyroidism are multiparity, thyroid hypoechogenicity on ultrasound, greater severity of the initial hypothyroidism, serum TPOAb positivity, higher maternal age, and a history of pregnancy loss.317,318 PPT can occur following pregnancy loss and in women with pre-existing hypothyroidism, specifically those with Hashimoto’s hypothyroidism who do not have a completely atrophic thyroid gland.319,320 LT4 given to TPOAb-positive pregnant women at 4–38 weeks’ gestation did not change the course of PPT, and LT4 is generally not recommended in this setting for the prevention of PPT. 321 Studies regarding selenium supplementation in TPOAb-positive euthyroid pregnant women show mixed results and mostly are of small cohorts in Europe,322,323 where background selenium nutrition may be suboptimal324,325; thus, we do not advise routine selenium supplementation for the prevention of PPT. Because of the potential risk of long-term hypothyroidism following PPT, even if LT4 was not required in the hypothyroid phase of PPT, we recommend that women with a history of PPT undergo serum thyroid function testing at one year or upon the development of any hypothyroidism-related symptoms.
Clinical presentation and evaluation
It is important to distinguish between the thyrotoxic phase of PPT and Graves’ disease, given the differences in their natural history and recommended management.326,327 The timing of the presentation following birth, biochemical differences, and other clues in the diagnostic evaluation are helpful in differentiating the two entities (Table 9). Serum TRAb and/or TSI positivity, highly specific and sensitive biomarkers of Graves’ disease, and a total-triiodothyronine:total-thyroxine ratio of >20 328 are confirmatory for Graves’ disease in most cases. In contrast, the onset of thyrotoxicosis in the first six months, shorter duration, and milder signs and symptoms of thyrotoxicosis are more suggestive of PPT. If these factors are not able to determine the etiology, conservative follow-up should be considered, and in severe cases, a thyroid nuclear uptake scan can be considered, although the potential consequences related to breastfeeding (including a decrease in specificity and need to temporarily discard breastmilk during the scan) need to be taken into account.
Distinguishing Between the Thyrotoxic Phase of Postpartum Thyroiditis (PPT) and Graves’ Disease
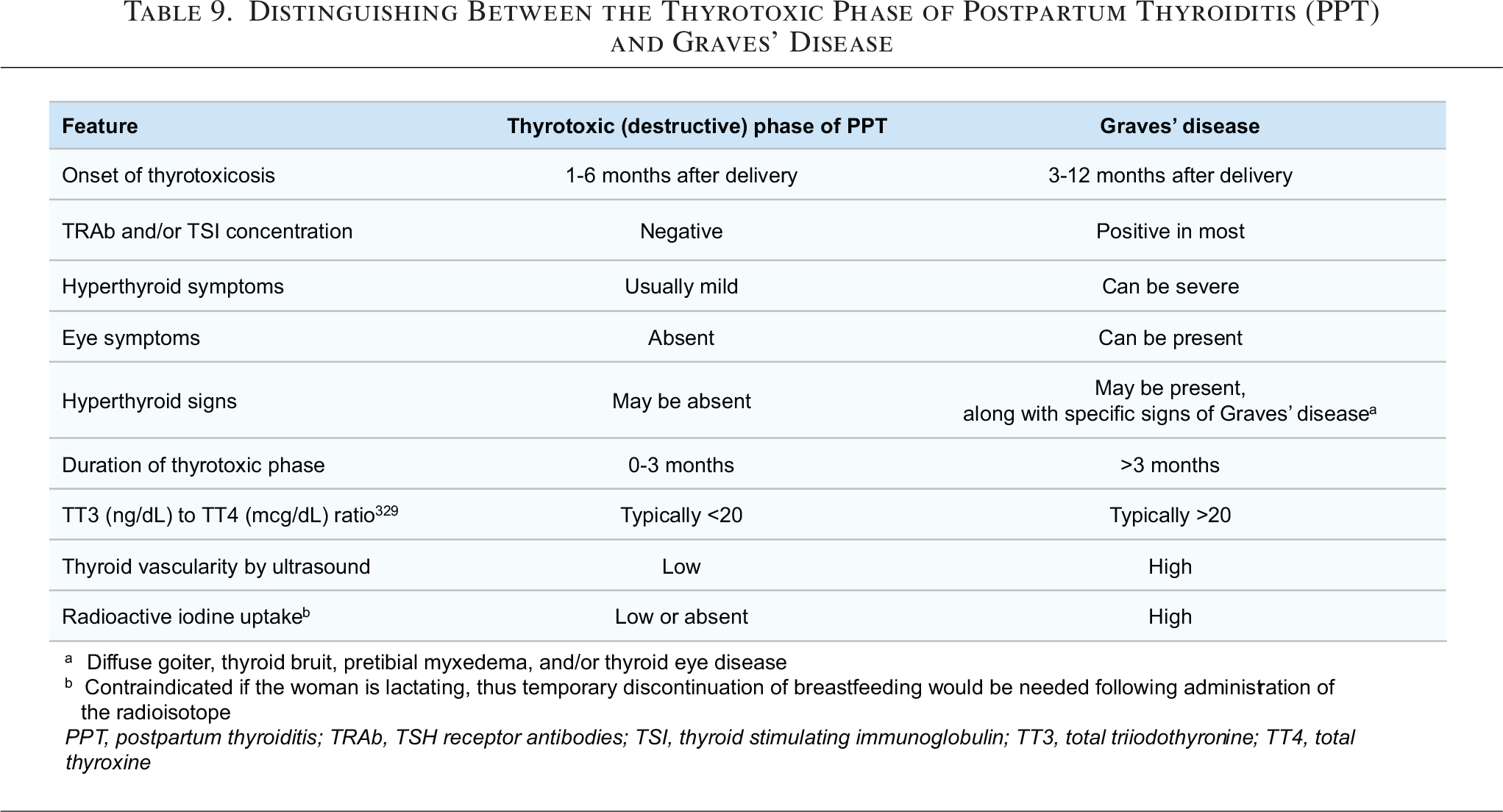
Although the time course of the phases and the clinical presentation of PPT vary, women may be symptomatic and come to attention during only the thyrotoxic or hypothyroid phase or both. A recommended algorithm for the evaluation and management of postpartum thyroid dysfunction is shown in Flowchart 5. Finally, it should be noted that postpartum depression may arise following PPT in some women, which has been studied in various observational cohorts.329–331 Although there is substantial heterogeneity in the available literature and there are overlapping symptoms between the conditions, there appears to be no association between PPT, thyroid autoimmunity, and risk of postpartum depression.332–334 If a woman develops depression in the postpartum period, thyroid function testing should be obtained in accordance with general population screening recommendations.
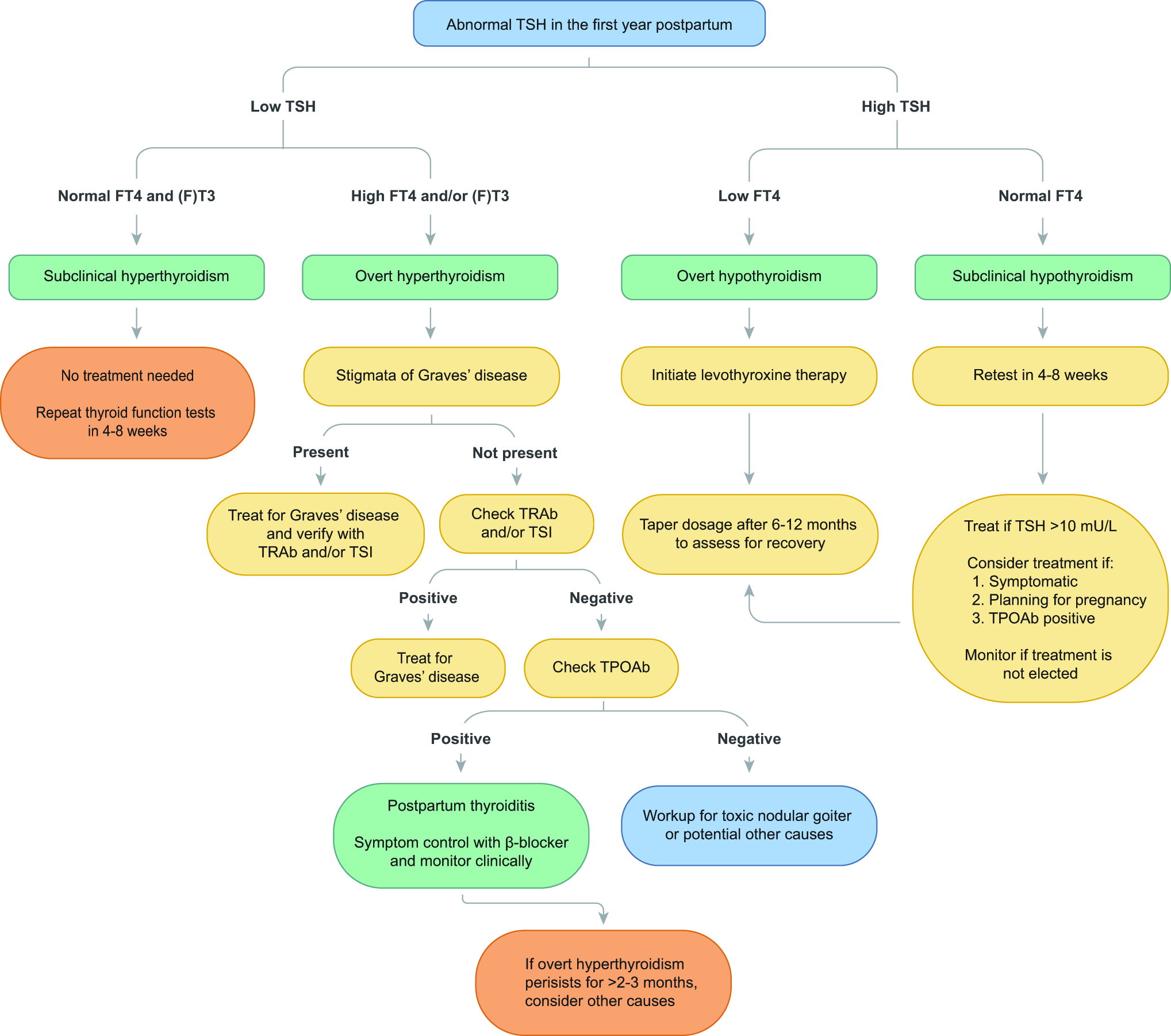
Approach to abnormal TSH levels in postpartum. Green boxes indicate a diagnosis, yellow boxes indicate an action, and orange boxes indicate recommended follow-up.
Treatment and management
During the thyrotoxic (destructive thyroiditis) phase of PPT, women with hyperthyroid symptoms may be treated with the lowest effective dose of a beta-blocker, which will typically be required for a few weeks. Propranolol and metoprolol are deemed safe in lactation. ATDs should not be used in the treatment of the thyrotoxic phase of PPT, as the underlying mechanism is not increased thyroid hormone production.
Treatment with LT4 for the hypothyroid phase of PPT should be given if the woman has hypothyroid symptoms, breastfeeding, or if she is actively trying for another pregnancy within six months. It should be noted that the benefit of LT4 on breastfeeding outcomes is based on limited data, and breastfeeding should be viewed primarily as a contextual factor that may influence shared decision-making for LT4 use postpartum, alongside symptom burden, severity of thyroid dysfunction, thyroid autoimmunity, and future pregnancy planning. If LT4 is started for symptomatic control, a trial of tapering or stopping the LT4 should be routinely considered after one year postpartum in women not planning another pregnancy soon, to determine if LT4 is still needed, since the hypothyroid phase of PPT is often transient. If LT4 treatment is not given or delayed during the hypothyroid phase of PPT, serum thyroid function should be rechecked every four to eight weeks until euthyroidism is restored or sustained hypothyroidism necessitates the initiation of LT4; women should be counseled to use adequate contraception until thyroid function has normalized. After a self-limited episode of PPT, the patient can be instructed to seek medical evaluation upon the development of any hypothyroid symptoms.
Other postpartum thyroid dysfunction
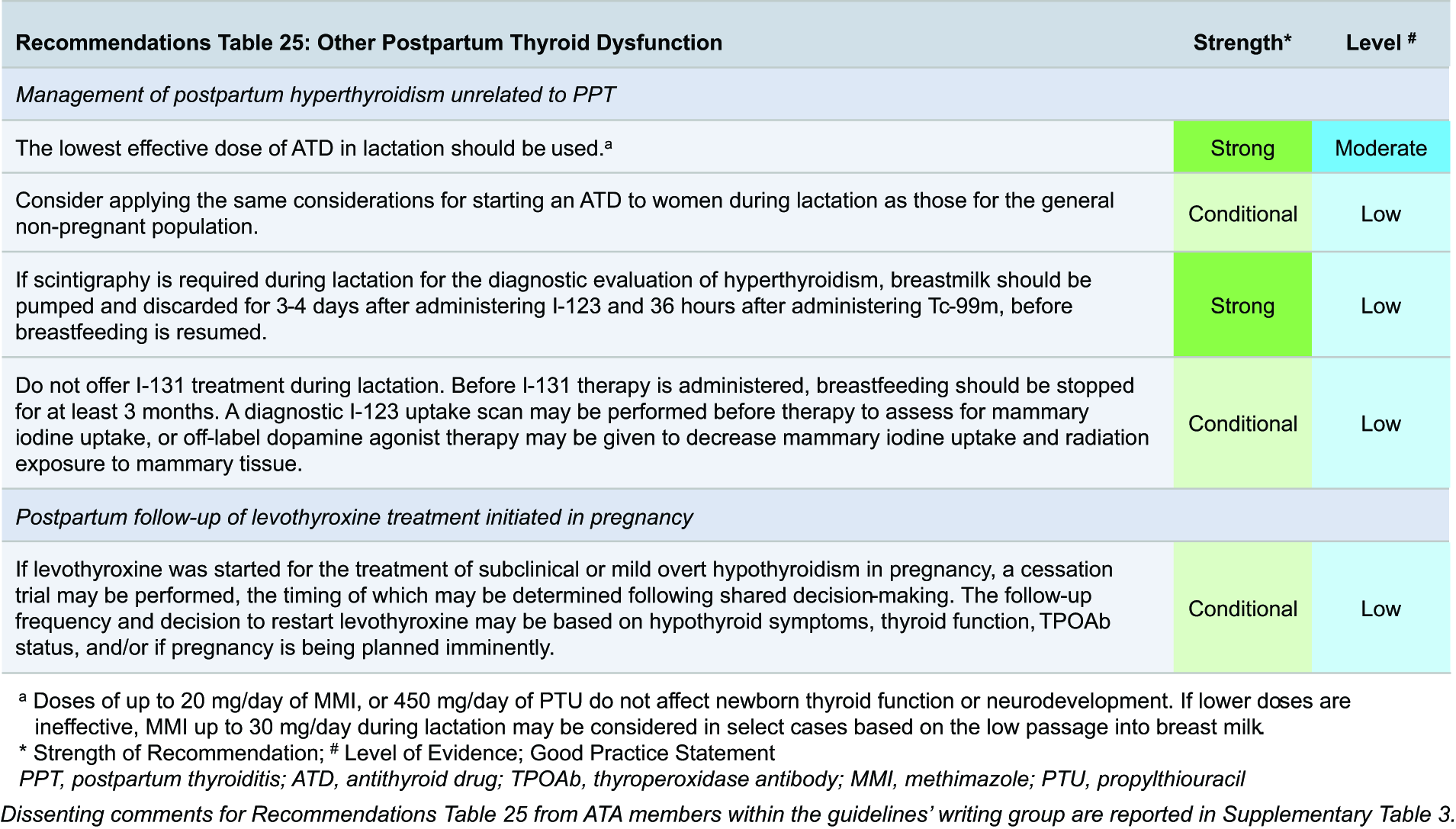
The role of thyroid function in breastmilk production and the potential of thyroid dysfunction to affect milk production, duration of lactation, or frequency of lactation are unclear, but clinically relevant adverse effects are unlikely. Some animal studies have reported impaired lactation following the use of PTU, but human data are sparse. There are small studies of deficient lactation in women with hypothyroidism, but these studies either included women already treated with levothyroxine 335 or who had the onset of lactation failure preceding the diagnosis of hypothyroidism. 336 Given the uncertainties around the available evidence, we are unable to recommend for or against screening for thyroid dysfunction in women having difficulty with lactation. Evaluation for Sheehan’s syndrome may be considered in case of a lack of breastmilk production after hypotension. Similarly, we are unable to recommend for or against the treatment of hypo- and hyperthyroidism for the strict purpose of improving milk production; in this scenario, lactating women with overt thyroid dysfunction should be treated in accordance with the usual care of nonlactating patients.
Radiopharmaceutical use in lactation
The use of diagnostic radiopharmaceutical agents during lactation should be limited to strict indications, given their proven excretion into human breast milk that would expose the mother to direct radiation to mammary tissue (from increased NIS expression during lactation [Fig. 4]) and the breastfed infant to ingested isotopes from breast milk intake. It should also be noted that the avid RAI uptake directed to breast tissue may impair RAI activity in the thyroid bed and the rest of the body.
Lactating women should stop breastfeeding for 3–4 days (although some groups recommend up to 7 days) after the administration of 123I and 36 hours after the administration of 99Tc pertechnetate. 339 Pertechnetate is generally preferred over 123I due to its shorter half-life. During the temporary stoppage of breastfeeding, all breast milk should be expressed and discarded after the administration of either pertechnetate or 123I. The pumping of breastmilk will increase the biological elimination of the radiopharmaceutical from the breast, decrease overall radiation exposure to the breasts, and facilitate continuation of breastfeeding after scanning. In addition, frequent expression of breast milk will help the mammary gland continue milk production. The woman can be counseled that a reserve of breast milk may be expressed prior to the dosing of the radiopharmaceutical agent, which can be used to feed the nursing infant until she can resume breastfeeding.
131I therapy has a relatively long half-life (approximately 8 days) and should not be given to lactating women. If there are no other options and 131I must be considered, the pros and cons of waiting at least three months after cessation of lactation to avoid radiation exposure to the breast should be discussed in a multidisciplinary setting. To aid in the timing of using radiopharmaceuticals (particularly 131I given its long half-life) for diagnostic scanning and/or treatment, a dopamine agonist to decrease breastmilk production and minimize radiation exposure to the breast may be considered,340–344 with the pros and cons of doing so to be discussed in a multidisciplinary setting. Breastfeeding should not resume after 131I administration. 345
Treatment and management of hyperthyroidism during lactation
As radiopharmaceuticals may be useful in the diagnosis and management of hyperthyroidism during lactation, guidance on their administration can be found in the section immediately above. If ATD treatment of hyperthyroidism is needed during lactation, limited observational and interventional clinical studies show that CMZ doses up to 15 mg/day, MMI doses up to 20 mg/day, and PTU doses up to 750 mg/day (with more robust data for PTU doses up to 450 mg/day) are not associated with thyroid dysfunction in breastfed infants.346,347 Breastmilk ATD concentrations are very low compared with maternally ingested doses (for PTU 0.025%, and for MMI 0.14%, of the oral dose).348,349 The up to sevenfold difference in breastmilk PTU and MMI concentrations may be related to their pharmacokinetic properties; PTU has greater protein-binding in serum than MMI, characteristics that may potentially inhibit its transfer into lipid-rich breastmilk. 350 Only one small study has evaluated infant IQ and neuropsychological measures in breastfed infants of mothers taking ATDs and reported no differences compared with a control group. 347 MMI is generally preferred over PTU, due to the risk of PTU-associated hepatotoxicity and the convenience of once-daily dosing. The considerations related to starting ATD treatment for the goal of correcting hyperthyroidism in lactation are generally the same as those outside the lactation setting. 346
Finally, potassium iodide may be considered an alternative management option of Graves’ disease during lactation, which has been described in iodine-sufficient regions such as Japan. Because iodine is excreted into breast milk and there is a risk of neonatal hypothyroidism, though potassium iodide therapy during breastfeeding requires active infant thyroid function test monitoring. 351 The pediatrician should be consulted to monitor serum thyroid function if there are clinical signs of thyroid disease in breastfed infants whose mothers have received SSKI within the past two months.
Treatment and management of hypothyroidism during lactation and postpartum period
In women with preexisting hypothyroidism, the increased LT4 dose requirement during gestation is a physiological function of pregnancy itself. Therefore, following delivery, the maternal LT4 dose can generally be reduced to that used prepregnancy, and serum TSH assessed six weeks thereafter. However, adjusting the LT4 to the prepregnancy dose may not be appropriate for all women. 352 Women who did not require a full dose of LT4 preconception, or those who have had a considerable weight gain during pregnancy, are more likely to require an LT4 dose that is higher than their preconception dose.
Subclinical hypothyroidism in pregnancy is often transient. Women who were started on LT4 in gestation, especially if the hypothyroidism was mild (i.e., TSH <6 mU/L), may be offered a trial of tapering or discontinuing LT4 (particularly if the dose is ≤75 mcg/day) shortly after delivery. Alternatively, this trial may also be deferred until after the initial newborn period, when there is likely less baseline fatigue. Should LT4 be discontinued or its dose decreased postpartum, serum TSH should be evaluated in approximately six weeks. 353 Pooled data from two randomized controlled trials have reported a 13.5% and 15.6% incidence of overt hypothyroidism when women who had subclinical hypothyroidism at 8–20 weeks’ gestation were universally screened for thyroid dysfunction at 1 and 5 years postpartum, respectively. 313
J. Future Research Directions
In the 2017 version of these guidelines, there were 13 suggested research directions, from which new data have considerably impacted the current guidelines for 4 of these. Below are the updated suggested research directions:
Further studies to determine risk-based reference intervals for thyroid function tests in pregnancy. Studies assessing the cost-effectiveness of thyroid function and thyroid antibody screening in women with a history of miscarriage or infertility. Studies assessing clinical (preconception) risk factors for thyroid disease during pregnancy. A comprehensive study to assess the iodine status of pregnant and lactating women in the United States. Studies to determine safe upper limits for iodine ingestion in pregnancy and lactation. Studies quantifying the risk of subfertility, success of fertility treatment, and/or progression to overt thyroid disease during pregnancy in women with preconception subclinical thyroid dysfunction or thyroid autoimmunity. A randomized trial of early LT4 intervention (preconception or early pregnancy, i.e., 6–10 weeks’ gestation) in women with either subclinical hypothyroidism or isolated hypothyroxinemia to determine effects on adverse pregnancy outcomes and child IQ. Studies assessing the effect of LT4 on adverse pregnancy outcomes in different subgroups of euthyroid TPOAb-positive women to establish potential intervention strategies. Prospective studies on the risk of adverse pregnancy and offspring outcomes for women with active Graves’ disease during pregnancy. Studies on serum (f)T3 and (f)T4 monitoring target concentrations in women with Graves’ disease treated with ATD. Studies evaluating the safest timing of administration of different ATDs for management of hyperthyroidism in pregnancy. Studies assessing novel ways to differentiate fetal hyperthyroidism from fetal hypothyroidism when a fetal goiter is detected. Studies investigating the impact of postpartum and pre-existing thyroid dysfunction on lactation.
Authors’ Contributions
T.I.M.K.: Conceptualization, methodology, writing of initial draft, and review/editing; A.M.L.: Conceptualization, methodology, writing of initial draft, and review/editing; E.K.A.: Methodology and review/editing; S.B.: Methodology and review/editing; K.B.: Methodology and review/editing; G.B.: Methodology and review/editing; R.C.: Methodology and review/editing; R.D.-S.: Methodology and review/editing; C.D.: Methodology and review/editing; J.L.E.: Methodology and review/editing; H.G.: Methodology and review/editing; S.J.K.: Methodology and review/editing; B.J.L.: Methodology and review/editing; S.Y.L.: Methodology and review/editing; S.M.: Methodology and review/editing; K.D.M.: Methodology and review/editing; L.F.M.-W.: Methodology and review/editing; C.T.N.: Methodology and review/editing; E.N.P.: Methodology and review/editing; Z.S.: Methodology and review/editing.
Footnotes
Acknowledgments
The committee wishes to thank Elise Krabbendam, MSc, for her help with the systematic literature searches. We thank Yindi Liu, MD; Joris Osinga, MD; and Arash Derakhshan, MD PhD, for their help on performing commissioned studies.50,58 We also thank Yindi Liu, MD, and Freddy Toloza, MD, for updating the literature search outputs and Stine Linding Andersen, PhD, for providing requested subanalyses verifying results for different disease definitions. 52 We also thank the ATA staff, in particular Kelly Hoff and Becky Schierman, for their help and support.
Funding Information
Author Disclosure Statement
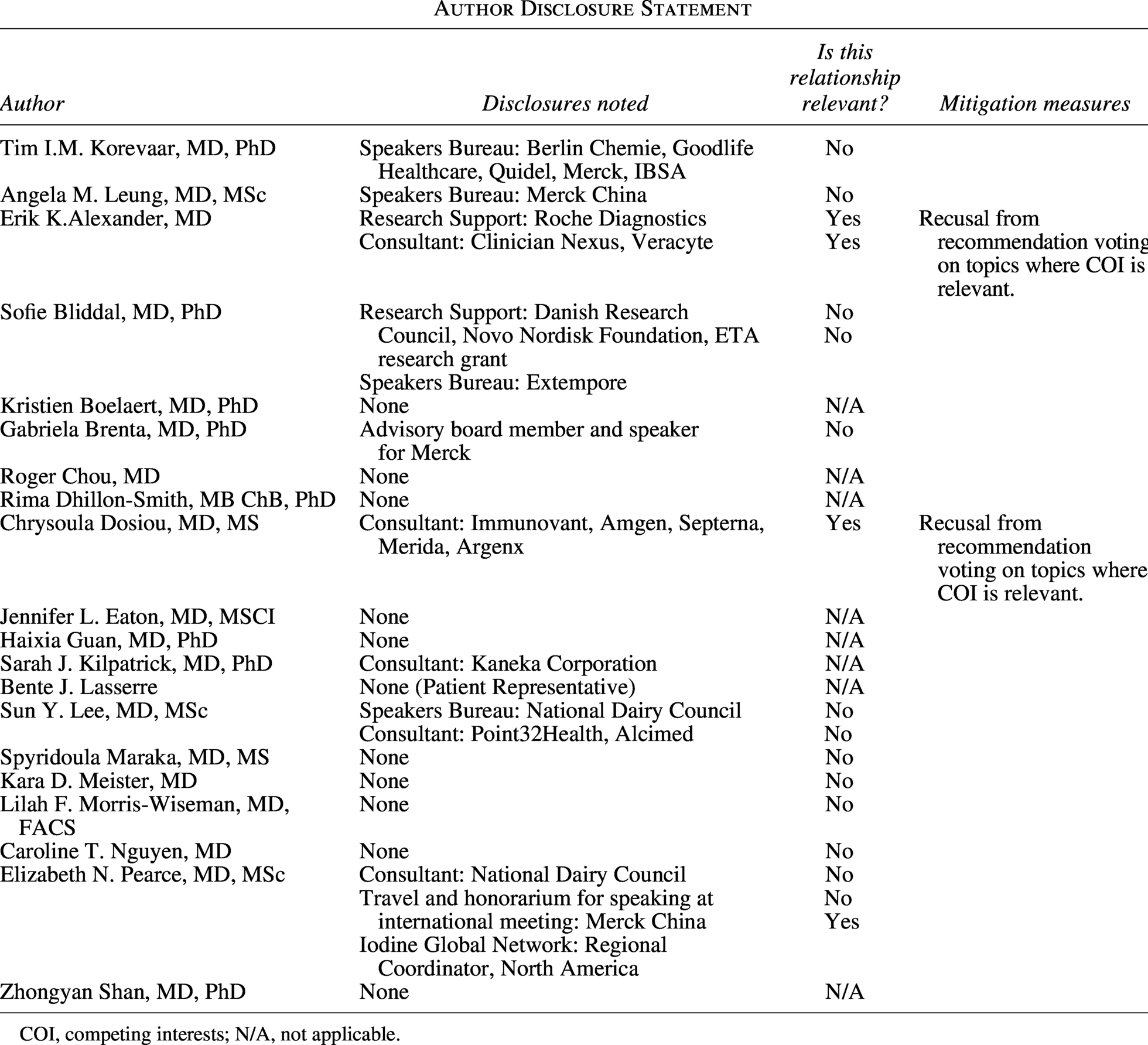
| Author | Disclosures noted | Is this relationship relevant? | Mitigation measures |
|---|---|---|---|
| Tim I.M. Korevaar, MD, PhD | Speakers Bureau: Berlin Chemie, Goodlife Healthcare, Quidel, Merck, IBSA | No | |
| Angela M. Leung, MD, MSc | Speakers Bureau: Merck China | No | |
| Erik K.Alexander, MD | Research Support: Roche Diagnostics |
Yes |
Recusal from recommendation voting on topics where COI is relevant. |
| Sofie Bliddal, MD, PhD | Research Support: Danish Research Council, Novo Nordisk Foundation, ETA research grant |
No |
|
| Kristien Boelaert, MD, PhD | None | N/A | |
| Gabriela Brenta, MD, PhD | Advisory board member and speaker for Merck | No | |
| Roger Chou, MD | None | N/A | |
| Rima Dhillon-Smith, MB ChB, PhD | None | N/A | |
| Chrysoula Dosiou, MD, MS | Consultant: Immunovant, Amgen, Septerna, Merida, Argenx | Yes | Recusal from recommendation voting on topics where COI is relevant. |
| Jennifer L. Eaton, MD, MSCI | None | N/A | |
| Haixia Guan, MD, PhD | None | N/A | |
| Sarah J. Kilpatrick, MD, PhD | Consultant: Kaneka Corporation | N/A | |
| Bente J. Lasserre | None (Patient Representative) | N/A | |
| Sun Y. Lee, MD, MSc | Speakers Bureau: National Dairy Council |
No |
|
| Spyridoula Maraka, MD, MS | None | No | |
| Kara D. Meister, MD | None | No | |
| Lilah F. Morris-Wiseman, MD, FACS | None | No | |
| Caroline T. Nguyen, MD | None | No | |
| Elizabeth N. Pearce, MD, MSc | Consultant: National Dairy Council |
No |
|
| Zhongyan Shan, MD, PhD | None | N/A |
COI, competing interests; N/A, not applicable.
Author Disclosure Statement
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.