
Abstract
Background:
Serum thyroglobulin (Tg) is a key tumor marker in papillary thyroid carcinoma (PTC), but its reliability may be compromised by the presence of antithyroglobulin antibodies (TgAb). Utilizing the assay-specific limit of quantification (LOQ) may enhance the detection of TgAb-related interference compared with the traditional reference limit. This study evaluated postoperative TgAb levels based on LOQ as a surrogate marker for tumor monitoring in PTC.
Methods:
A total of 1039 patients with PTC (≥1 cm) who had undetectable unstimulated serum Tg (<0.2 ng/mL) 6–12 months after total thyroidectomy with radioactive iodine (RAI) ablation therapy (2009–2012) were retrospectively analyzed. Simultaneously measured TgAb levels were classified using both the reference limit (60.0 U/mL) and LOQ (43.4 U/mL) into three groups undetectable (<43.4 U/mL), borderline (43.4–60.0 U/mL), and elevated (>60.0 U/mL).
Results:
The median age was 48.2 years, and 188 (18.1%) were male. The median tumor size was 1.5 cm, and lymph node metastases were present in 705 patients (67.8%). During a median follow-up of 12.0 years, recurrence occurred in 4.8%. Based on initial TgAb level, patients were classified as undetectable (65.6%), borderline (23.5%), and elevated (10.9%), with corresponding 10-year progression-free survival rates of 97.9%, 94.6%, and 88.5%, respectively (p < 0.001). Multivariable analysis revealed a significantly higher recurrence risk in the borderline group compared with the undetectable group (adjusted hazard ratio, 2.01; confidence interval, 1.03–3.96; p = 0.043). In the borderline group, TgAb became undetectable in 75.0% of patients over 6.3 years, whereas those who remained borderline exhibited a higher recurrence rate of 12.9% (p = 0.01).
Conclusions:
TgAb levels above the LOQ were associated with a higher recurrence risk in patients with PTC with undetectable Tg after RAI treatment. Classification of TgAb positivity based on the LOQ may improve prognostic assessment compared with evaluation using conventional reference limits. Further studies are needed to validate our findings and refine TgAb thresholds.
Keywords
Introduction
Serum thyroglobulin (Tg) is routinely used as a tumor marker for postoperative surveillance in differentiated thyroid cancer (DTC). The American Thyroid Association (ATA) also recommends the concurrent measurement of antithyroglobulin antibodies (TgAb).1,2 The development of highly sensitive Tg assays has improved analytical sensitivity and measurement stability at low detection limits.3–5 However, structural recurrence may occur without a corresponding increase in serum Tg levels. One major cause of this discrepancy is interference from TgAb, which is detected in up to 25–30% of patients with DTC.6,7 Notably, such interference may occur even at borderline TgAb levels, defined as detectable but below the assay’s reference limit.8,9 This reference limit was originally established for diagnosing autoimmune thyroid disease and may not be optimal for identifying interference in Tg assays.10,11 Moreover, the lack of standardized guidelines for TgAb interpretation further complicates disease monitoring.
TgAb assays vary in sensitivity and in the absolute concentrations they report, which may lead to underdetection in certain cases.10,12 Consequently, various thresholds have been proposed to define TgAb positivity.8,10,11 Among these, the limit of quantification (LOQ), defined as the lowest concentration measurable with acceptable bias and imprecision, typically within a total allowable error of ≤30%, has gained attention as a reliable parameter.13–15 Compared with conventional assay reference limits, the LOQ enables more accurate detection of low-level TgAb, with reduced variability and improved reproducibility.8,12 Unlike functional sensitivity (FS), the LOQ does not require long-term clinical validation. As such, recent expert consensus has recommended the LOQ as a practical and feasible alternative to FS, which demands more complex methodology and greater resources.6,13,14,16,17
Borderline TgAb levels, defined as detectable but below the assay’s reference limit, are often interpreted as positive in DTC; however, their clinical significance remains uncertain.6,8,17 Few studies have directly investigated their prognostic value. One study reported that borderline TgAb levels, defined according to FS, were not associated with an increased risk of tumor persistence or recurrence in patients with low- to intermediate-risk papillary thyroid carcinoma (PTC). 18 Similarly, another study found no association between borderline TgAb levels above the FS and disease recurrence. 19 In contrast, the prognostic relevance of dynamic changes in TgAb levels has been demonstrated more consistently. A previous study showed that in patients with undetectable Tg but positive TgAb, early postoperative changes in TgAb concentrations may serve as a prognostic indicator of recurrence. 20 A meta-analysis further confirmed that persistent or increasing TgAb levels were associated with a higher risk of cancer persistence or recurrence compared with decreasing levels. 21
This retrospective study evaluated the prognostic significance of postoperative detectable TgAb levels defined according to analytical sensitivity. The analysis included patients with PTC who underwent total thyroidectomy (TT) followed by radioactive iodine (RAI) ablation and had undetectable unstimulated serum Tg levels. Longitudinal changes in TgAb concentrations were further assessed to determine their clinical utility for monitoring disease status in PTC.
Methods
In this retrospective study, 3145 consecutive patients with PTC who underwent TT followed by RAI treatment between 2009 and 2012 at Asan Medical Center, Seoul, Korea, were initially screened. A total of 1832 patients with a primary tumor size <1 cm, 161 patients with unstimulated Tg ≥ 0.2 ng/mL at 6–12 months after ablation, 25 patients with thyroid bed uptake on the initial diagnostic whole body scan, and 88 patients with incomplete clinicopathological data were excluded. Finally, 1,039 patients with undetectable unstimulated Tg (<0.2 ng/mL) and available TgAb measurements obtained 6–12 months after RAI ablation were included in this study (Fig. 1). The study protocol was approved by the Institutional Review Board of Asan Medical Center, Seoul, Korea (IRB No. 2024-1318). The requirement for informed consent was waived owing to the retrospective nature of the study.
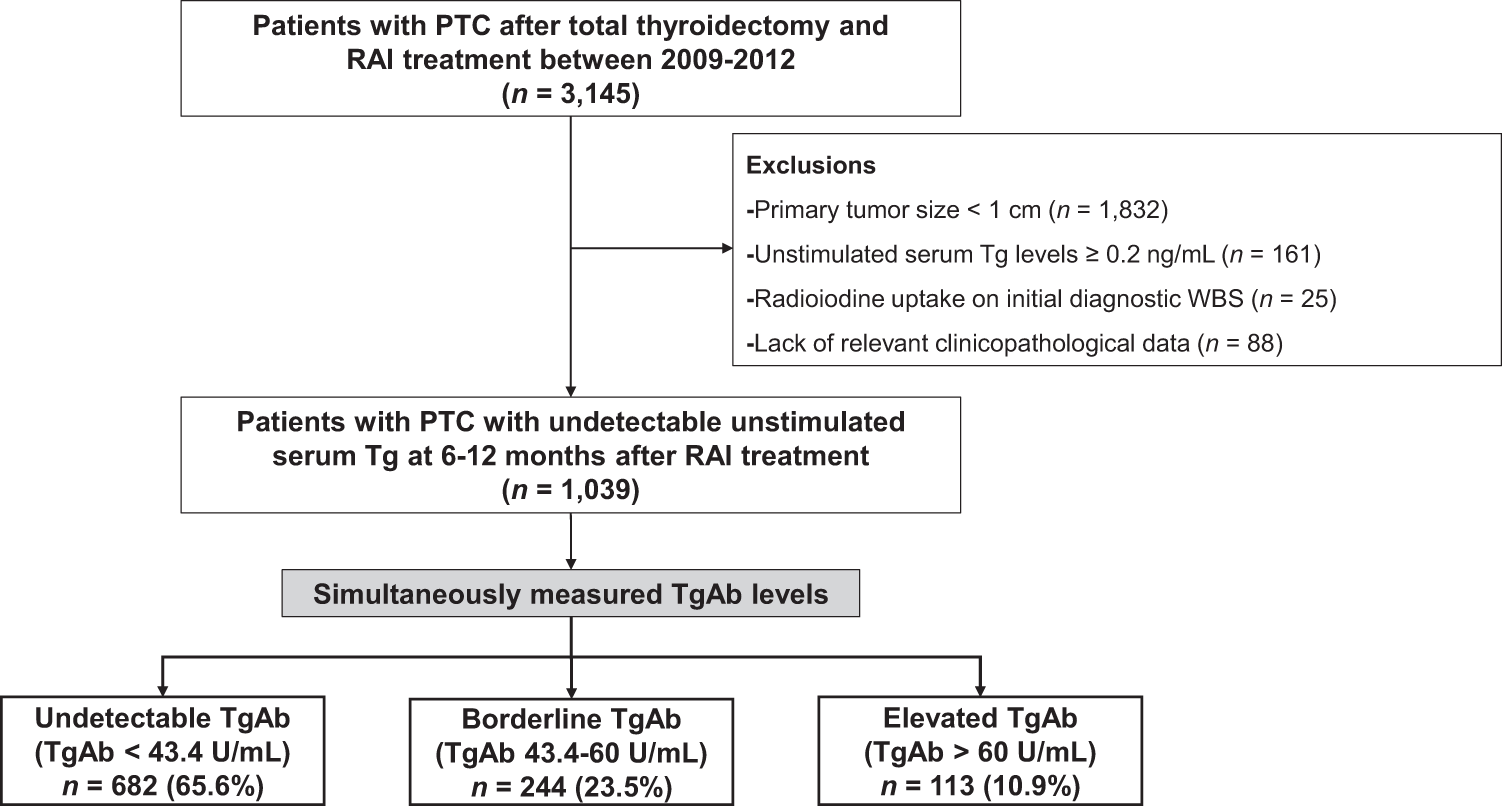
Flow diagram of patients. PTC, papillary thyroid carcinoma; RAI, radioactive iodine; Tg, thyroglobulin; TgAb, antithyroglobulin antibody; WBS, whole body scan.
A radioimmunoassay (RIA) was used to measure serum Tg (Tg-pluS RIA kit; BRAHMS AG, Henningsdorf, Germany), with an FS (coefficient of variation of 20%) of 0.2 ng/mL and an analytical sensitivity of 0.08 ng/mL, as determined in the laboratory. Serum TgAb levels were measured using a radioligand assay (ANTI-TGn RIA kit; BRAHMS) with an FS of 33 U/mL; TgAb positivity was defined as a value exceeding 60 U/mL (the reference limit). According to the Clinical and Laboratory Standards Institute (CLSI) guideline EP17-A, 22 the limit of blank (LOB) was determined by repeated measurements of four blank samples using two different reagent lots (A and B), yielding a total of 132 measurements. The limit of detection (LOD) was derived using the Cochrane G test based on 128 repeated measurements of four low-concentration samples near the LOD value (9.2 U/mL) provided by BRAHMS. The LOQ was established as the concentration at which precision was within 20%, based on repeated measurements of 10 samples near the LOD over 5 days with 19 replicates. Among these samples, the LOQ was determined to be 43.4 U/mL, representing the highest concentration meeting the ≤20% imprecision criterion, and was comparable to the manufacturer-reported LOQ of 42.4 U/mL. Pathological evaluation was performed by an experienced thyroid pathologist with over 10 years of clinical experience. Pathologically confirmed lymphocytic thyroiditis was defined by the presence of diffuse lymphocytic and plasma cell infiltration, oxyphilic cells, and the formation of lymphoid follicles and reactive germinal centers. The infiltration was required to occur in a normal region of the thyroid gland, distinct from the site of PTC.
Patients were categorized into three groups: undetectable TgAb (<43.4 U/mL; below the LOQ), borderline TgAb (43.4–60.0 U/mL; detectable but below the reference limit), and elevated TgAb (>60.0 U/mL). Follow-up occurred every 6–12 months and included measurements of Tg and TgAb, clinical examinations, and neck ultrasonography (US). Levothyroxine therapy was administered to all patients to maintain serum thyrotropin levels within the target range. In cases of increasing Tg or TgAb, or when clinical suspicion of recurrence arose, additional imaging studies beyond neck US, such as 18F-fluorodeoxyglucose positron emission tomography or chest computed tomography, were performed to localize normal or malignant thyroid tissue. Recurrence was defined as the appearance of structural disease after complete ablation of thyroid remnants, confirmed by cytological or histopathological examination, and/or the detection of distant metastases on imaging. 23
All statistical analyses were performed using R software, version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org). Continuous variables are presented as medians with interquartile ranges (IQRs) and were compared using the Kruskal–Wallis test. Categorical variables are presented as numbers (percentages) and were compared using Pearson’s χ 2 test or Fisher’s exact test, as appropriate. Post hoc analyses were evaluated using the Holm–Bonferroni correction method. Progression-free survival (PFS) rates were analyzed using the Kaplan–Meier method and visualized with GraphPad Prism version 10.4 (GraphPad Software, San Diego, CA, USA; http://www.graphpad.com), with comparisons performed using the log-rank test. The Cox proportional hazard model was used for univariate and multivariable analyses to evaluate relevant risk factors, with hazard ratios (HRs) and confidence intervals (CIs) calculated. All p-values were two-sided, and p < 0.05 was considered statistically significant.
Results
Patient characteristics
Baseline characteristics of the study population are summarized in Table 1. The median age at diagnosis was 48.2 years (IQR 39.2–55.2), and 188 (18.1%) were male. Regarding pathological subtypes, classical PTC was diagnosed in 1030 patients (99.1%), whereas the remaining 9 patients (0.9%) had the follicular subtype. The median primary tumor size was 1.5 cm (IQR 1.2–2.0). Extrathyroidal extension (ETE) was observed in 776 patients (74.7%), including microscopic ETE in 524 patients (50.4%) and gross ETE in 252 patients (24.3%). Among patients with gross ETE, 221 (87.7%) had T3b disease with strap muscle invasion, whereas 31 (12.3%) had T4 disease, including invasion of the recurrent laryngeal nerve in 22 patients, trachea in 7, esophagus in 1, and carotid artery in 1. Lymph node (LN) metastases were present in 705 patients (67.8%), with 494 (47.5%) classified as N1a and 211 (20.3%) classified as N1b. Extranodal extension (ENE) was detected in 162 patients (15.6%) and pathologically confirmed thyroiditis in 325 patients (31.2%). The median follow-up period was 12.0 years (IQR 10.9–13.2), with an overall recurrence rate of 4.8% (50/1,039). Locoregional recurrence occurred in 47 patients, including 14 (29.8%) in the thyroid operative bed or central neck LNs and 33 (70.2%) in the lateral neck LNs. Distant recurrence was identified in 3 patients, involving the lungs and skin. Notably, one patient with persistently borderline TgAb levels developed skin recurrence on the arm at 9.6 years of follow-up despite undetectable Tg levels.
Baseline Characteristics of Patients
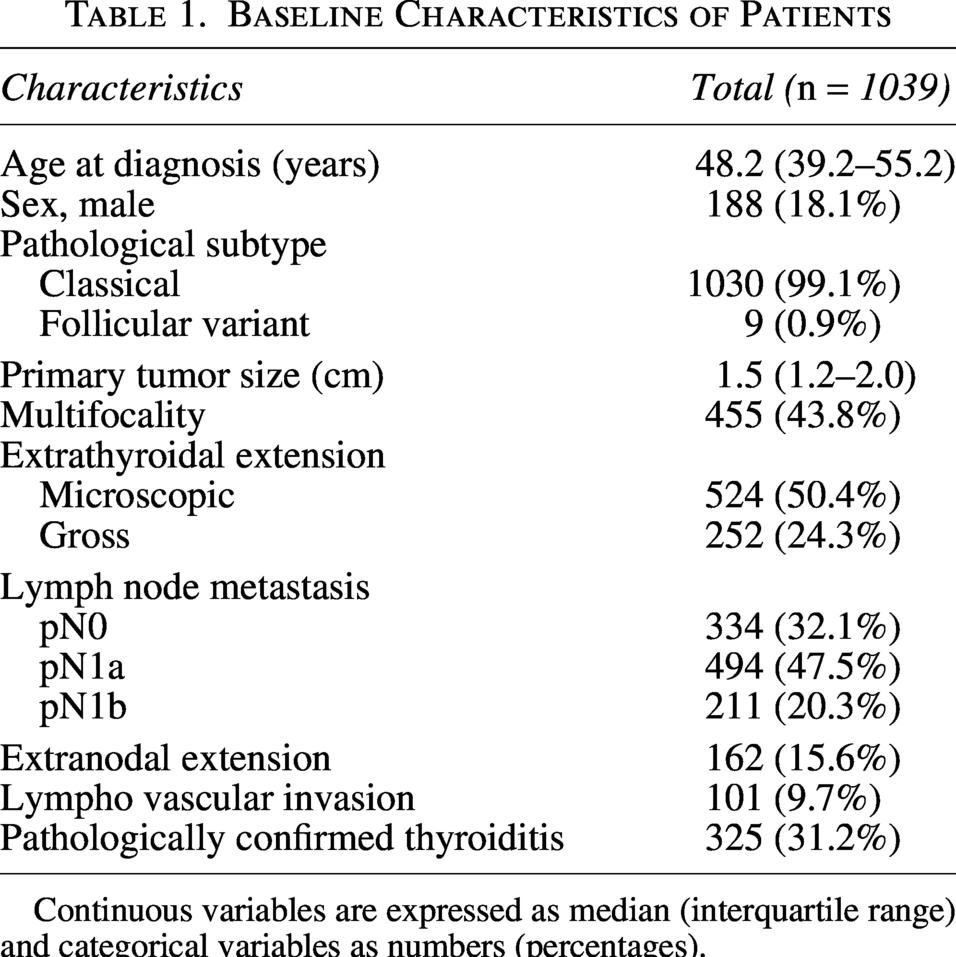
Continuous variables are expressed as median (interquartile range) and categorical variables as numbers (percentages).
Clinicopathological factors correlated with TgAb levels
Clinical and pathological characteristics stratified by TgAb levels are presented in Table 2. The distribution of patients according to TgAb levels was as follows: undetectable (<43.4) in 682 (65.6%; CI 62.7–68.5), borderline (43.4–60) in 244 (23.5%; CI 21.0–26.1), and elevated (>60.0) in 113 (10.9%; CI 9.0–12.8) patients. All patients, regardless of TgAb status, had Tg < 0.2 ng/mL, and 95.4% (991/1,089) had Tg equal to the analytical sensitivity of the assay (0.08 ng/mL). No significant differences were observed between groups in age, primary tumor size, ETE, or lymphovascular invasion. Male sex differed across TgAb groups (p = 0.01), being more frequent in the undetectable [Odds ratio (OR) 2.61; CI 1.39–5.46] and borderline groups (OR 2.02; CI 1.05–4.42) than in the elevated group. Multifocality was more frequent in the elevated TgAb group (p = 0.008) than in the undetectable (OR 1.83; CI 1.23–2.74) and borderline groups (OR 1.44; CI 1.11–2.26). Lateral neck LN metastases and the presence of ENE were more common in the borderline and elevated TgAb groups (p = 0.004 and p = 0.021, respectively). Post hoc analysis revealed significant differences between the undetectable and borderline TgAb groups, with higher rates in the borderline group for both lateral neck LN metastasis (OR 1.11; CI 1.03–1.64) and ENE (OR 1.16; CI 1.04–2.00). Pathologically confirmed thyroiditis was also more frequent in the borderline and elevated TgAb groups (p < 0.001), being highest in the elevated group compared with the undetectable (OR 5.31; CI 3.51–8.12) and borderline groups (OR 2.55; CI 1.62–4.06).
Clinicopathological Factors Correlated with Antithyroglobulin Antibody (TgAb) Levels
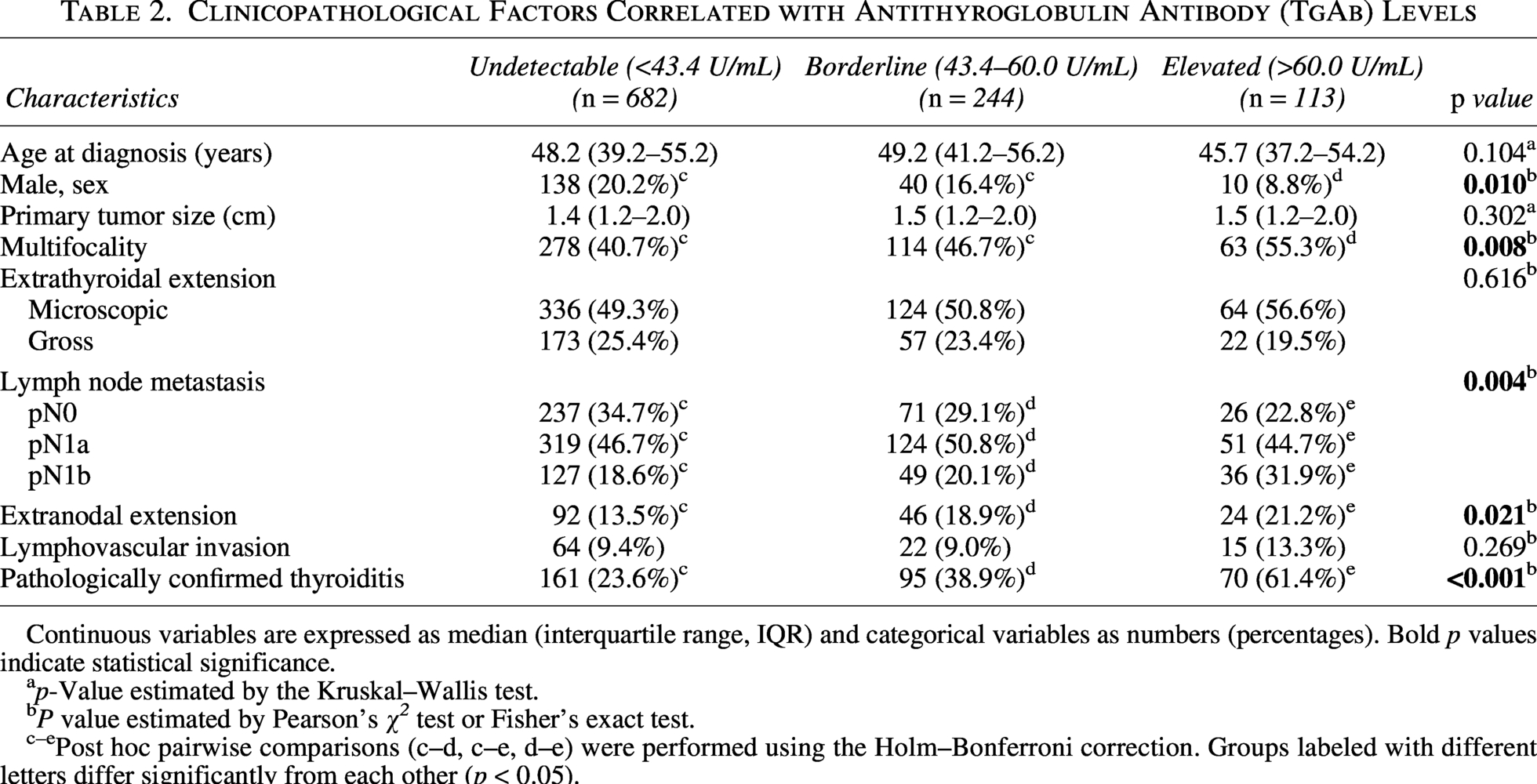
Continuous variables are expressed as median (interquartile range, IQR) and categorical variables as numbers (percentages). Bold p values indicate statistical significance.
p-Value estimated by the Kruskal–Wallis test.
P value estimated by Pearson’s χ 2 test or Fisher’s exact test.
c–ePost hoc pairwise comparisons (c–d, c–e, d–e) were performed using the Holm–Bonferroni correction. Groups labeled with different letters differ significantly from each other (p < 0.05).
Association of structural recurrence with TgAb levels
As shown in Figure 2, the risk of disease recurrence differed significantly among the groups. The 10‐year PFS rates were 97.9%, 94.6%, and 88.5% in the undetectable, borderline, and elevated groups, respectively (p < 0.001). Among 15 patients in the borderline group who developed recurrence, 11 (73.3%) maintained negative serum Tg levels (<0.2 ng/mL) at the time of recurrence detection, whereas all 16 patients with recurrence in the elevated group also had negative Tg levels. Clinicopathological factors associated with disease recurrence are summarized in Table 3. In univariate analysis, male sex, larger primary tumor size, LN metastases, ENE, lymphovascular invasion, and detectable TgAb groups were identified as significant prognostic factors for recurrence. In multivariable analysis, male sex (HR 2.08; CI 1.10–3.94; p = 0.025), primary tumor size (HR 1.29; CI 1.03–1.61; p = 0.028), LN metastases (HR 7.73; CI 1.83–32.66; p = 0.005), presence of ENE (HR 2.03; CI 1.12–3.67; p = 0.019), and detectable TgAb groups remained significant risk factors for predicting recurrent disease. Compared with the undetectable group, the crude HRs for recurrence were 2.21 (CI 1.12–4.34; p = 0.022) in the borderline group and 5.09 (CI 2.55–10.09; p < 0.001) in the elevated group. After adjustment for sex, tumor size, LN metastases, and ENE, the adjusted HRs were 2.01 (CI 1.03–3.96; p = 0.043) in the borderline group and 5.93 (CI 2.20–12.23; p < 0.001) in the elevated group.
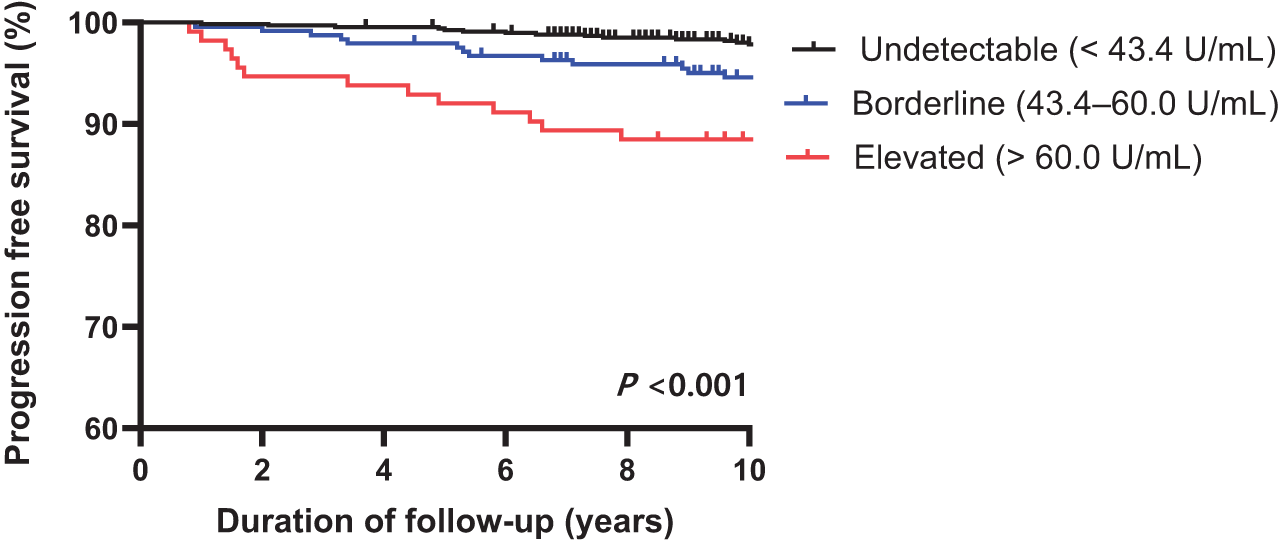
Kaplan–Meier survival curves for progression-free survival based on TgAb levels. TgAb, antithyroglobulin antibody.
Association of Recurrent Disease with Variable Clinicopathological Factors
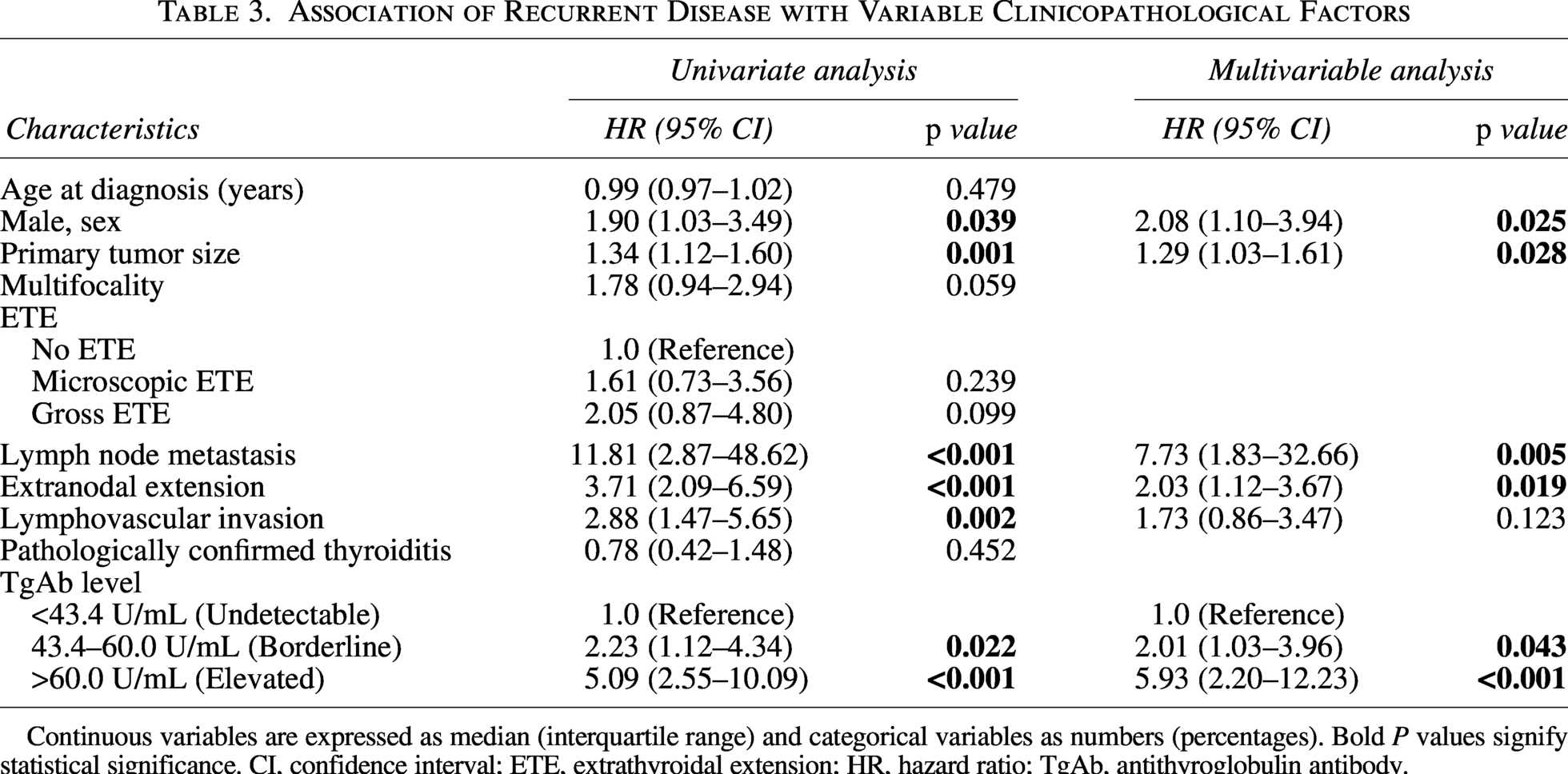
Continuous variables are expressed as median (interquartile range) and categorical variables as numbers (percentages). Bold P values signify statistical significance. CI, confidence interval; ETE, extrathyroidal extension; HR, hazard ratio; TgAb, antithyroglobulin antibody.
Longitudinal changes in TgAb levels during follow-up
Longitudinal changes in TgAb levels between 6 and 12 months post-ablation and the last follow-up were evaluated. Among the 244 patients with initially borderline TgAb, 183 (75.0%) became undetectable at the last follow-up, over a median period of 6.3 years (IQR 3.6–7.8). Of the remaining patients, 57 (23.4%) continued to have borderline TgAb, and only 4 (1.6%) progressed to elevated TgAb (Fig. 3A). Recurrences occurred in 1/4 patients (25.0%) who progressed to elevated TgAb, 7/57 (12.3%) who remained borderline throughout follow-up, and 7/183 (3.8%) who became undetectable. Among the seven recurrences in the persistently borderline group, five (71.4%) had undetectable Tg levels at the time of recurrence. The risk of disease recurrence in the initially borderline group varied significantly according to TgAb dynamics, with higher recurrence observed in patients with persistently borderline TgAb compared with those who became undetectable (p < 0.001; Fig. 4). The 10-year PFS rates were 97.6% in patients who became undetectable and 87.1% in those with persistently borderline TgAb levels.
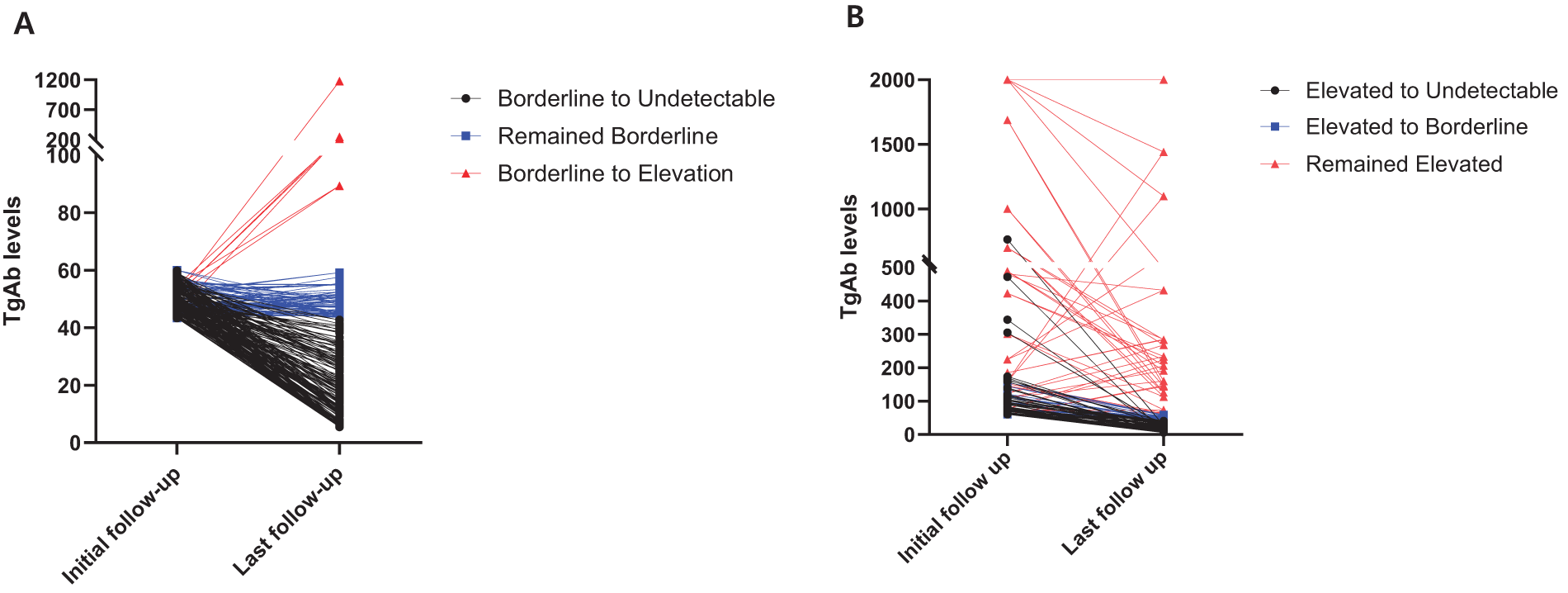
Longitudinal trends in TgAb levels.
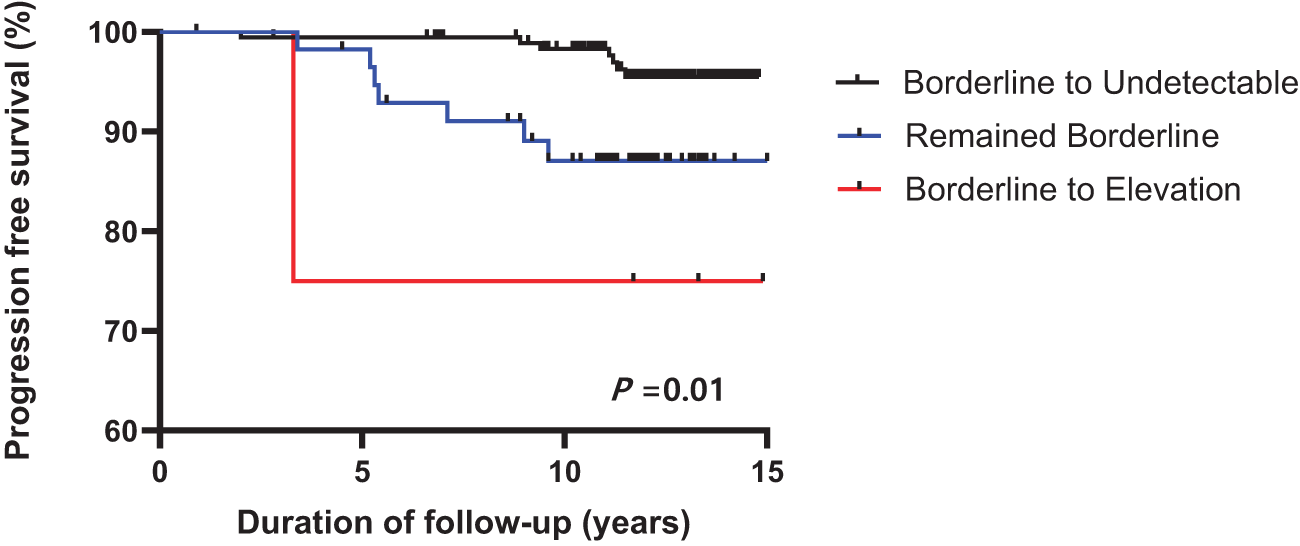
Kaplan–Meier survival curves for progression-free survival according to TgAb dynamics in patients with initially borderline TgAb levels. TgAb, antithyroglobulin antibody.
Among the 113 patients with initially elevated TgAb, 76 (67.3%) became undetectable, 20 (17.7%) remained elevated, and 17 (15.0%) shifted to borderline (Fig. 3B), representing a lower rate of conversion to undetectable status than that observed in the initially borderline group.
Discussion
This study evaluated clinical outcomes in patients with undetectable unstimulated serum Tg, stratified by TgAb levels measured 6–12 months after RAI treatment. Borderline TgAb levels above the LOQ were significantly associated with an approximately twofold higher risk of recurrence compared with undetectable TgAb levels. Longitudinal analysis demonstrated that persistently borderline TgAb was associated with a markedly increased recurrence risk exceeding 12%, even in patients with negative Tg levels. These findings confirm the role of TgAb positivity based on the LOQ as an independent risk factor for recurrence in multivariable analysis. Considering the known interference of TgAb and the present results, defining TgAb positivity according to the LOQ may provide a more appropriate approach. This strategy may improve postoperative risk stratification in RAI-treated patients with PTC by providing more precise and clinically meaningful prognostic information.
In this study, patients with borderline TgAb levels had an approximately 6% risk of recurrent disease, which is relatively high considering that these patients would have been classified as having an excellent response to initial therapy under the conventional reference limit in the current risk stratification system. 1 Moreover, recurrence occurred in over 12% of patients who maintained borderline TgAb levels throughout follow-up, a rate comparable to that observed in the initially elevated TgAb group. Furthermore, Tg remained undetectable at the time of recurrence in 71% of these patients. These findings suggest that even stable, borderline TgAb levels may indicate clinically meaningful assay interference, potentially masking Tg elevation and allowing tumor progression without a corresponding increase in Tg. This observation aligns with recent reports demonstrating that the presence and concentration of TgAb can lower measured serum Tg levels, possibly reflecting TgAb-mediated increases in Tg metabolic clearance. 24 While some studies have suggested that lower TgAb thresholds may increase the likelihood of false-positive interpretations and therefore advocated higher cutoff values to improve specificity for clinically significant disease and mitigate inter-assay variability,6,25,26 the present findings support the use of LOQ-based lower cutoff values. This approach may enhance the detection of TgAb-associated analytical interference that correlates with recurrence risk.
The clinical significance of detectable TgAb and its role in risk stratification of patients with DTC remains a subject of debate. Although the present study demonstrated a higher recurrence rate among patients with detectable TgAb, one study reported only a 2.2% recurrence rate in patients with persistently borderline TgAb. 18 Similarly, another study found that TgAb positivity defined by analytical sensitivity was not associated with tumor features or clinical risk profiles. 25 In contrast, the current findings indicate that detectable TgAb is significantly associated with aggressive pathological features, including lateral neck LN metastases and ENE, both recognized as strong predictors of recurrence in PTC. Importantly, detectable TgAb remained a significant risk factor even after adjustment for other clinical variables. These findings are consistent with a previous meta-analysis demonstrating that TgAb positivity is associated with an increased risk of LN metastases and disease persistence. 21
Based on these observations, patients with undetectable unstimulated serum Tg and TgAb levels below the LOQ, considered negative, may be managed with a less intensive follow-up strategy. This approach aligns with the 2025 ATA guidelines, which state that in patients with low-risk DTC showing unstimulated Tg (<0.2 ng/mL) and undetectable TgAb, lifelong thyroid cancer monitoring is likely unnecessary. 2 The low recurrence rates and excellent survival outcomes observed in DTC further support the gradual de-escalation of monitoring intensity over time. In contrast, detectable TgAb levels, particularly when persistently stable or increasing during follow-up, may warrant additional diagnostic evaluation. Because most cases with detectable TgAb levels exhibited a declining trend, continued monitoring is warranted until TgAb becomes undetectable. The overall management strategy proposed in this study is in agreement with recent expert consensus recommendations. 17
TgAb interference varies widely across patients due to TgAb heterogeneity, is influenced by assay design and test reagents, and correlates poorly with TgAb concentration.8,27 Currently, no available method can reliably overcome TgAb interference while maintaining adequate analytical sensitivity. The proportion of samples classified as TgAb-positive varies substantially across assays due to wide inter-assay variability.6,12 In clinical practice, applying the limit of detection or FS to define TgAb positivity would markedly reduce the clinical usefulness of Tg, as most patients would exceed these overly sensitive cutoffs. 25 Therefore, the assay-specific LOQ was used as a practical lower detection threshold, acknowledging that manufacturer-recommended cutoffs are primarily established for diagnosing thyroid autoimmunity. Each laboratory may consider verifying or establishing its own performance characteristics under local conditions before clinical implementation and measure TgAb longitudinally using the same assay.
The clinical relevance of Hashimoto’s thyroiditis (HT) and circulating TgAb in PTC remains unclear. In the present study, histopathological evidence of HT was more frequently observed in TgAb-positive patients but was not associated with an increased risk of recurrence. In patients with HT, TgAb, particularly specific immunoglobulin subclasses, have been linked to an increased risk of PTC progression. 28 More recently, HT has been suggested to contribute to both PTC development and improved prognosis through modulation of gene expression, activation of shared signaling pathways, and alteration of the tumor microenvironment. 29 Positive TgAb levels may originate from underlying HT or tumor-related inflammation, which may partly explain the inconsistent findings regarding the role of thyroid autoimmunity in PTC. Therefore, the presence of HT alone should not be considered a benign explanation for persistent TgAb positivity, and surveillance strategies should not be modified solely based on this finding.
This study has several limitations. First, its retrospective design may have introduced inherent selection bias, including potential imbalances in tumor subtype distribution and aggressive histological variants. We were unable to re-evaluate the pathological specimens according to the most current diagnostic criteria, and lymphovascular invasion was reported without distinction between lymphatic and vascular components. In addition, the relatively strict pathological criteria used to diagnose lymphocytic thyroiditis may have led to underrecognition of mild cases. The rate of gross ETE in our cohort remained relatively high even after re-review of all operative records for patients classified as having gross ETE. This finding may reflect the single-center design, and referral bias inherent to a tertiary referral center enriched for higher-risk patients,30,31 as well as selection bias related to the inclusion of only RAI-treated patients. Second, a single TgAb assay method (RIA) was used throughout the study period; therefore, comparisons with other commercially available assays, including more sensitive immunometric assays, were not performed. Reliance on a single assay-specific LOQ does not fully capture the complexity of TgAb interference and should be interpreted within the context of laboratory-specific conditions at our institution; therefore, it may not be directly applicable to other TgAb assays. Third, baseline (preoperative and preablation) TgAb levels were not assessed, precluding comparative analyses and evaluation of the potential impact of RAI therapy on subsequent TgAb dynamics. Finally, our cohort consisted exclusively of patients who underwent TT followed by RAI therapy, which may limit the generalizability of our findings to PTC patients managed without RAI or to those with thyroid bed uptake on post-therapy whole-body scanning. Despite these limitations, the study is strengthened by a uniform patient cohort, consistent Tg and TgAb assays, and a prolonged follow-up period. Further large-scale and multi-institutional prospective studies are needed to confirm the reproducibility of our findings and to further refine clinically meaningful TgAb thresholds.
In conclusion, defining TgAb positivity based on analytical sensitivity may provide more sensitive and clinically relevant information than conventional reference limits–based assessment in patients with PTC after RAI treatment. This approach, which incorporates sensitive TgAb classification and monitoring of TgAb dynamics, could improve prognostic assessment in patients with undetectable serum Tg by serving as a surrogate marker.
Authors’ Contributions
C.A.K.: Conceptualization (lead), formal analysis (lead), writing—original draft (lead), writing—review and editing (equal). Y.-I.K.: Methodology (lead), writing—review and editing (equal). D.Y.L.: Methodology (lead), writing—review and editing (equal). S.-H.L.: Methodology (lead), writing—review and editing (equal). J.-S.R.: Methodology (supporting), writing—review and editing (equal). W.B.K.: Investigation (supporting), writing—review and editing (equal). W.G.K.: Conceptualization (supporting), investigation (supporting), writing—review and editing (equal). T.Y.K.: Supervision (lead), conceptualization (lead), writing—review and editing (equal). M.J.J.: Supervision (lead), conceptualization (supporting), writing—review and editing (equal).
Footnotes
Author Disclosure Statement
Authors have no conflicts to disclose.
Funding Information
C.A.K., Y.-I.K., D.Y.L., S.-H.L., W.B.K., J.-S.R., W.G.K., and T.Y.K. have no funding to declare. M.J.J. reports funding from the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (grant number: RS-2025–16064551).