
Abstract
Background:
Mild thyroid eye disease (TED) is the most common form of TED, yet it is the least studied. Uncertainties about the natural history and prevention, and underfunding for clinical research, are an obstacle to improving the management of this important group of patients.
Summary:
The available evidence suggests that the prevalence of mild TED can reach up to two-thirds of all cases, depending on the expertise of the assessor and the criteria used for diagnosis. Prevalent symptoms and signs of mild TED predominantly arise from lid changes, soft tissue involvement and ocular surface disease, but disease presentation is heterogeneous and in some patients proptosis and eye motility changes may be underrated with the current classification. Little is known about the impact of the various manifestations of mild disease on patients’ risk of progression and quality of life (QoL). Although in most patients with mild TED the disease remits spontaneously, some patients progress, and a significant proportion evolve to persistent, inactive TED. Current therapeutic options for these patients are based on scarce, low-to-moderate quality and sometimes conflicting evidence, resulting in significant differences in the management of mild TED in different countries and by different specialists. Among the most recommended therapeutic interventions, selenium supplementation was mainly studied in selenium-insufficient populations with active mild TED and it lacks efficacy in longstanding, inactive disease. The use of immunosuppressive drugs and targeted therapies for mild TED are commonly reported by surveys of medical professionals in a clinical setting, but the indication and efficacy of these agents in mild TED remain unclear.
Conclusions:
Mild TED has a significant psychosocial and functional burden that should be reconsidered and addressed by local, systemic or surgical treatments in an individualized manner. Given the overall effect on QoL and the socioeconomic impact, it is of immediate importance to highlight the knowledge gaps and the need for research in mild TED.
Introduction
Thyroid eye disease (TED) is an autoimmune condition that affects 20–40% of adult patients with Graves’ disease (GD).1,2 The clinical presentation of TED has become less severe over the past decades 3 and at present, 77% of TED cases are of mild severity. 4 In children, nearly all cases of TED are mild. 5 The trend toward milder TED may be related to an earlier recognition and treatment of both hyperthyroidism and TED, as well as a greater utilization of micronutrient supplements, 6 decreased smoking, 7 and less frequent use of radioiodine. 8
Although the majority of mild TED cases remit spontaneously, a significant proportion of patients progress or evolve to persistent, inactive TED.9–11 Currently, therapeutic solutions for these patients are based on limited evidence and the most recent recommendations for mild TED12,13 tend to be rather general and leave important questions unanswered. Despite the “mild” clinical presentation, several clinical studies showed a significant decrease in quality of life (QoL) indicating a measurable psychosocial and functional burden even in the absence of more severe manifestations of the disease of significant diplopia or optic neuropathy.14–17 The negative impact on QoL is consistent across different ethnic groups, extends beyond the active phase and is an indication for specific treatment in mild TED. Unlike other patients with thyroid diseases, TED patients do not recover immediately from their disease-related work disability and in the long-term they are at risk of sickness absence (HR 2.08), reduced capacity to return to work (HR 0.52) and disability pension (HR 4.40). 18 Given the overall effect on QoL and the socioeconomic burden, it is of immediate importance to highlight the knowledge gaps and the need for research in mild TED.
Materials and Methods
This narrative review synthesizes current evidence on epidemiology, clinical presentation, diagnosis and management of mild TED. The research questions were prespecified and the search strategy included a literature search in PubMed using the following keywords—“Thyroid Eye Disease” [Mesh] OR “Graves Ophthalmopathy” [Mesh] OR “Graves Orbitopathy” AND mild OR “mild disease” AND “treatment” OR “diagnosis” OR “Quality of Life” OR “Selenium”. No filters were applied to specify the type of article or the year of publication. Citations within the articles were also explored, if they appeared relevant to the current review. The final reference list was selected by the authors after assessing its relevance in this review. The review was conducted in accordance with the Helsinki Declaration and was approved by the local Ethics Committee (Comité d’Ethique Hospitalo-Facultaire des Cliniques Universitaires St-Luc, Université Catholique de Louvain, Brussels, Belgium).
Review
What was the genesis of the current definition of mild TED?
The NOSPECS classification proposed in 1969 was one of the earliest systems for staging TED without making a distinction between severity and activity. 19 NOSPECS did not explicitly categorize severity of TED into mild and other categories. Likewise, the VISA system introduced in 2006 does not define mild TED. 20 The European Group on Graves’ Orbitopathy (EUGOGO) proposed a broad classification for severity into mild, moderate-to-severe, and sight-threatening in 2008, 21 based on consensus. The aim was to encourage referral of patients to specialist centers and to facilitate appropriate therapeutic decision-making. The inclusion in the definition of mild TED of the condition that the disease should have only ‘minor impact on daily life, insufficient to justify immunosuppressive or surgical treatment’ was intended to emphasize the importance of QoL and of balancing efficacy against safety, at a time when the immunosuppressive treatment of TED consisted predominantly of oral glucocorticoids (GCs). This was not a classification intended to be used in clinical research. Indeed, in the only randomized placebo-controlled trial (RCT) on mild TED published by EUGOGO, 17 the inclusion criteria for mild disease made no reference to QoL. Over the years, the EUGOGO definition of mild TED has probably served its purpose in avoiding patient harm, although there are no data to support this proposition. The drawback of the EUGOGO definition is that in the context of scientific discourse (as opposed to practical management of an individual patient), the clause “minor impact on daily life insufficient to justify immunosuppressive or surgical treatment” can cause confusion. Moreover, the clinical signs of TED should be regarded as a continuum of the disease spectrum; so putting artificial borders between mild, moderate, and severe TED may deprive patients of appropriate care. 22
What is the current definition of mild TED?
The most widely used classification for the severity of TED in the past 10 years is that proposed by EUGOGO. According to this classification, mild TED refers to patients whose eye disease has minimal impact on daily life to justify immunomodulatory treatment or surgery. 12 These patients have one or more of the following features: minor lid retraction <2 mm, mild soft-tissue involvement, exophthalmos <3 mm above normal for race and gender, and no or intermittent diplopia and corneal exposure responsive to lubricants. 12 However, these severity criteria are not universally used. A 2020 meta-analysis of the overall prevalence of TED in patients with GD 23 emphasized that 22 of the 57 included studies did not use any of the recommended classifications to diagnose TED, leading to reporting bias.
It is interesting that the definition of moderate-to-severe TED proposed by EUGOGO in 2008 21 has received wide acceptance and currently, several RCTs that are actively recruiting utilize that definition. In contrast, a clear definition of mild TED based on objective criteria that is widely accepted by the academic community is lacking.
What are the common features of mild TED?
Mild TED is a heterogeneous disorder, with symptoms and signs arising from lid retraction, periocular soft tissue changes, proptosis, eye muscle dysfunction and ocular surface disease (OSD). However, data on the prevalence of each mild TED manifestation is scarce in the literature, with most of it coming from the EUGOGO RCT. 17
Overall, lid signs are the most common signs in TED, with an estimated prevalence of lid retraction and lid lag of 57% and 59%, respectively.23,24 However, most studies do not report prevalence by TED severity category. Typically, in mild TED, eyelid retraction may be intermittent, and the shape of the eyelids tends not to develop the severe lateral flare commonly found in more severe disease due to fibrosis of the lateral horn of the levator.
Soft tissue changes in mild TED can lead to subtle facial disfigurement. Mild soft tissue involvement, categorized according to EUGOGO Color Atlas, can be present in up to 65% of the eyes affected by mild TED. 17
There are limited data sets of normal exophthalmometry values in different ethnicities and defining mild disease on the basis of proptosis “less than 3 mm above normal for race and gender” is contentious. No individual patient is likely to conform to an ethnic stereotype, so the use of premorbid photographs is a more indicative guide to the degree of orbital change.25–28
The majority of mild TED patients don’t present with eye muscle motility disturbance, but 4–11% of them can have intermittent diplopia. 17 It is important to differentiate binocular TED-related intermittent diplopia from restricted extraocular muscle movement from monocular diplopia due to tear film disturbances, uncorrected refractive error or intraocular pathology. The former typically worsens with peripheral gaze. Uniocular duction and field of binocular single vision assessment, along with MRI imaging for extraocular muscle involvement can complement the clinical picture. However, few MRI studies focus on the distinction between mild and moderate-to-severe TED groups (Fig. 1) and the natural history of diplopia in mild TED remains unknown.
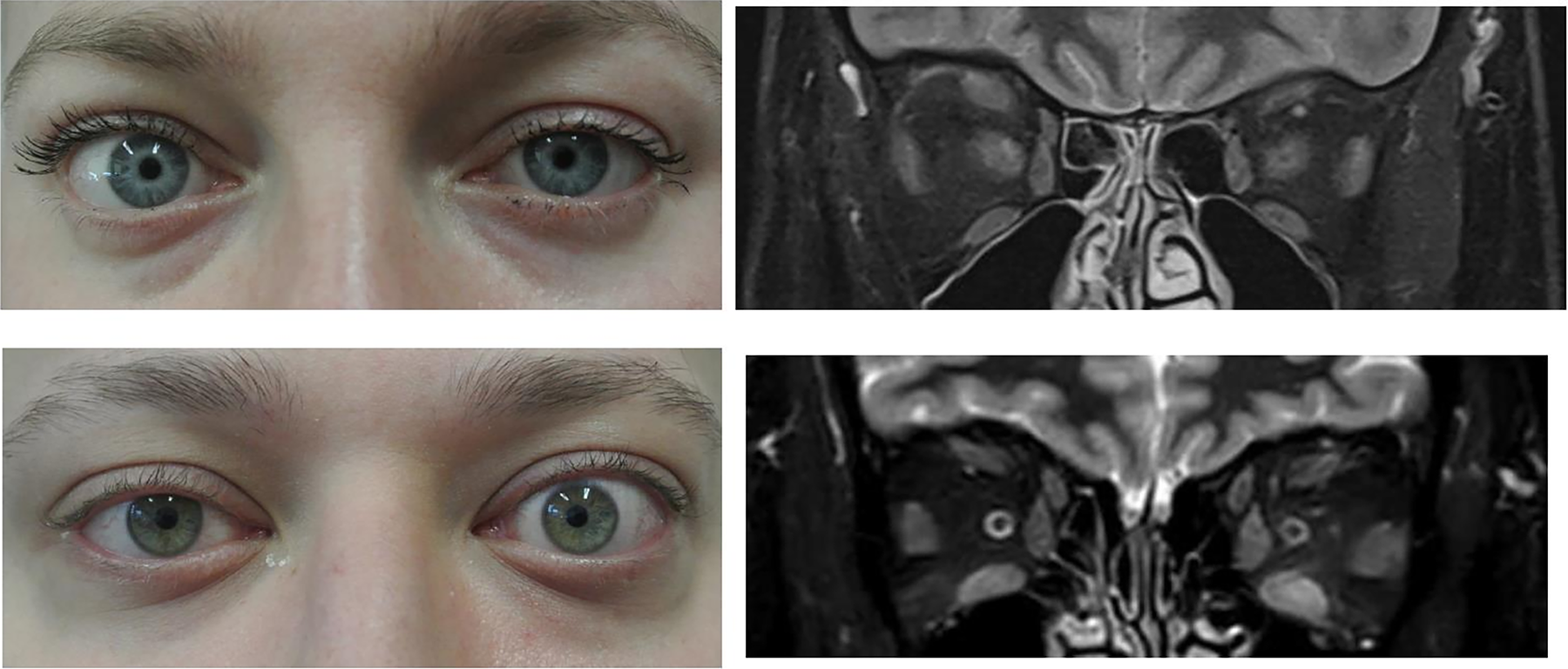
Clinical features of mild thyroid eye disease (TED). Upper images: recent, asymmetrical, mild TED in the right eye (lid changes); on MRI—no eye muscle involvement. Bottom images: recent, asymmetrical, mild TED in the left eye (lid and soft tissue changes); on MRI–eye muscle enlargement involvement. TED, thyroid eye disease; MRI, magnetic resonance imaging.
Finally, OSD can affect up to 65–95% of TED patients. 29 Multifactorial causes include exposure from eyelid retraction, proptosis, a proinflammatory tear film and reduced tear production causing both evaporative and aqueous-deficient dry eye. 29 Patients often report dryness, grittiness, burning, or foreign body sensation, and intermittent blurred vision. Photophobia and excessive tearing can also occur. The OSD Index (OSDI) can provide additional insight into symptom severity, impact on daily activities, environmental exacerbating factors, and a quantitative response to intervention. Although OSDI has been studied mainly in relation to TED activity, 30 one study found OSDI scores significantly higher (worse) in patients with moderate-to-severe active TED compared with mild non-active cases (p = 0.0006). 31 Another study found moderate-to-severe and sight-threatening TED had a higher meibum quality score compared with normal values in mild TED (higher scores indicating reduced function), but no significant differences in meibum expression, tear break-up time, tear production (Schirmer’s test), and Oxford grading score. 32 More studies are needed to correlate OSD parameters with both TED severity and activity. The initial approach to treatment centers on four key aspects: (i) supplementing tear production, (ii) reducing inflammation, (iii) correcting any underlying eyelid malposition, and (iv) making environmental modifications such as using humidifiers or occluding the eyes overnight.
How does mild TED affect QoL of patients?
The GO–QOL is the only validated QoL instrument for all severities of TED with established content construct and cross-cultural validity and a well-defined minimal important change. 33 GO–QOL score range from 0 (full limitation) to 100 (no limitations). Several observational studies and one randomized clinical trial showed mean GO–QoL visual functioning scores ranging from 77.8 ± 16.6 to 82.2 ± 2.2 and mean GO–QoL appearance scores from 74.0 ± 19.8 to 86.0 ± 17.6 in mild TED patients at diagnosis,14–17 indicating a measurable psychosocial and functional burden even in the absence of more severe manifestations of the disease. Females and younger patients have lower appearance but not visual functioning scores. 34
While the GO–QOL questionnaire is effective at detecting change in greater TED severities, its ability to capture subtle improvements or changes in QoL among patients with mild TED may be limited due to a ceiling effect.16,34 In clinical practice, this limitation highlights the need for alternative or complementary patient-reported outcome measures that are more sensitive to variations in the less severe spectrum of the condition and could provide a more accurate assessment of treatment efficacy, ensuring that improvements are not overlooked due to the insensitivity of the standard instrument. The association between depression and TED severity is inconsistent, 35 but one study found that moderate to severe TED patients scored significantly higher for depression on the Profile of Mood States compared with those with mild disease. 36
Apart from changes in the appearance and visual function, it should be remembered that other modifiable factors could also affect the QoL in mild TED patients, such as: (i) dysthyroidism (both hyper—and hypothyroidism), 37 (ii) smoking, 38 (iii) psychological and social burden, and (iv) other factors including comorbidities (Fig. 2). Thus, it is important to evaluate patients with TED using a holistic approach, not solely based on eye examination.
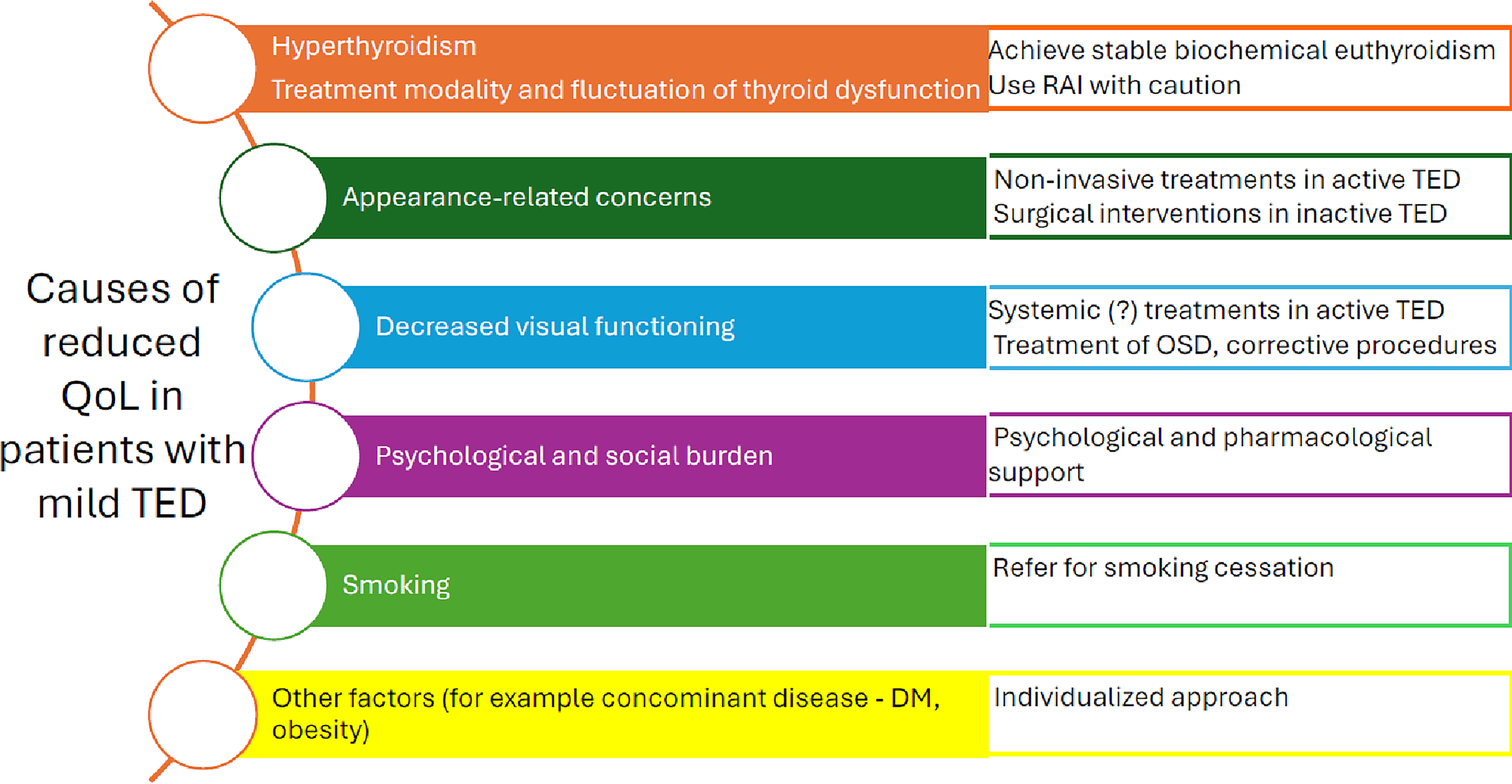
Possible causes of reduced quality of life in patients with mild TED and suggested interventions. DM, diabetes mellitus; OSD, ocular surface disease; QoL, quality of life; RAI, radioiodine.
What is the socioeconomic burden of mild TED?
In a retrospective economic study on TED from the United States, Smith et al. defined six health states of varying TED severity and assigned utility values. 39 Two health states were more closely associated with mild TED—small proptosis without diplopia and intermittent or inconstant diplopia with small proptosis. The utility value for no diplopia/small proptosis was the highest, with a mean of 0.60 (CI, 0.54–0.67), while a slightly lower value of 0.52 (CI, 0.45–0.58) was observed for intermittent or inconstant diplopia with small proptosis. 39 These findings suggest that patients with more severe proptosis/diplopia are more likely to have detrimental associations with QoL.
Ponto et al., analyzing correlations between direct costs and clinical features in a hospital cohort of German patients, found that costs were associated with disease severity but not specifically with diplopia or the costs of mild TED (mean cost: €332; range: €857–€1,078; p = 0.016). 40 The authors also found that the frequency of work disability increased with the severity of diplopia occurring 20.9% (23 of 110) in patients without diplopia, compared with 41% (11 of 27) with intermittent, 42% (25 of 58) with inconstant, and 74% (14 of 20) with constant diplopia (p = 0.001). By extrapolation, patients with mild TED could fall within the first two categories.
What is the natural history of mild TED?
Few studies have documented the natural history of mild TED. In a prospective study, 59 patients attending a combined thyroid-eye clinic in Newcastle upon Tyne, UK 9 were assessed every 3 months using NOSPECS criteria for a median follow-up of 12 months. All of these patients were deemed not to require surgical or immunosuppressive treatment, and most had mild TED. The majority of patients improved spontaneously (64%), and only 13.5% progressed to immunosuppressive treatment. More recently, in a retrospective Italian study of 65 patients with untreated TED, the majority of which was mild, 51% spontaneously improved, and 15% moderately or significantly worsened after a median follow-up of 40 months. 10 In a large prospective series of 364 newly diagnosed patients with GD treated with antithyroid drugs in a tertiary center, 20% of patients had mild and inactive TED at presentation according to EUGOGO criteria. 11 Of these, 43 patients were followed for 18 months and only one progressed to moderate-to-severe form, while 58% of patients had complete remission 11 (Fig. 3). In the seminal study by Marcocci et al., 17 the observations in the placebo group aligned with previous data: 35–36% of mild patients improved spontaneously, 36–39% remained unchanged, and 26% worsened. The main message of these studies is that up to 60% of mild TED patients remit spontaneously, but a significant proportion of them carries a meaningful risk of progression or persistent disease.
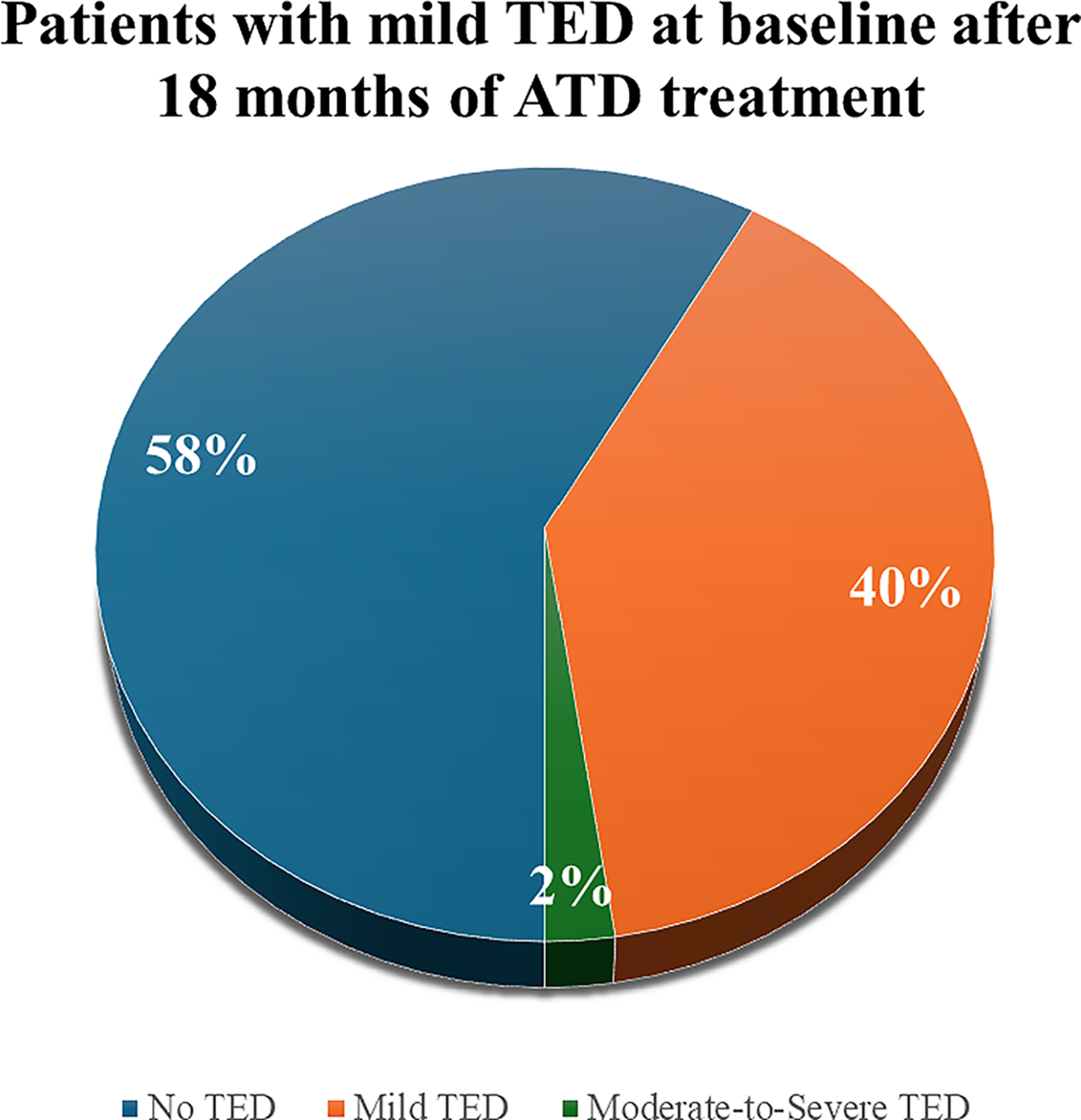
Natural history of mild TED. Data were derived from ref. 11 Among 43 patients with mild TED at baseline, who completed the 18-month follow-up during or after ATD treatment, 58% experienced complete remission of eye signs, 2% progressed to moderate-to-severe TED, and 40% still had mild inactive TED. ATD, antithyroid drugs.
Can mild TED progression be predicted?
Major factors associated with the progression of TED in general (older age, male sex, thyroid dysfunction, radioiodine treatment without steroid prophylaxis, smoking, TSH receptor antibody levels) were also incriminated in the progression of mild TED in some,41–46 including a very large retrospective series of more than 4000 TED patients, 42 but not all studies. 10 The predictive value of some of these and other parameters for developing TED was prospectively assessed in a EUGOGO study of 348 patients with untreated GD. 47 During the 18 months of antithyroid drug treatment, 15% of these patients developed mild TED, mostly during the first 12 months, and only 2% moderate-to-severe TED. Four of the baseline parameters (Clinical Activity Score-CAS, TRAb, duration of hyperthyroid symptoms, and smoking) were found to be significant in forming a predictive score that was better at predicting those patients who will not develop overt TED than those who will (positive and negative predictive values were 0.28 (95% CI 0.20–0.37) and 0.91 (95% CI 0.87–0.94) respectively). 47 In another prospective controlled study of GD patients without TED, TRAb and FT3 levels combined with a score based on the results of visual function tests and of orbital ultrasound showed a high positive (73%) and negative (72%) predictive value in identifying patients at risk of developing overt TED. 48 The severity of soft tissue involvement and presence of diplopia, but not smoking nor radioiodine, were associated with TED progression in the Olmsted County prevalence study. 49
In some, 50 but not all studies, TED patients have lower selenium levels than patients without TED, supporting the hypothesis that relative selenium insufficiency may be an independent risk factor for the development of clinically significant orbitopathy in patients with GD. However, there were no differences in active TED occurrence or the need for immunosuppressive treatment for TED in a study of 430 patients newly diagnosed with GD in a borderline low selenium area, randomized to receive 200 µg selenium or placebo for 24–30 months, but the study was not powered for this outcome. 51
The difficulty in predicting which patients will progress to more severe forms of TED is driving the need to identify new risk markers. Total and LDL-cholesterol are higher in GD patients with TED when compared with patients without TED and elevated LDL cholesterol levels were associated with TED activity and severity. 52 Although some European and Asian observational studies have reported protective effects of statin administration on TED occurrence, one Asian study showed that these benefits appear to be greater for patients with moderate-to-severe TED and when statins are initiated within one year of GD diagnosis. 53 However, prospective RCTs testing the efficacy of statins in GD or mild TED are not available.
Gut microbiota has emerged as a novel immunomodulator of autoimmune thyroid disease, and although influenced by geographic differences, the microbiome signature appears to differ in mild TED from more severe forms and GD without orbitopathy. 54
Can mild TED be prevented?
Smoking cessation, the rapid control of thyroid dysfunction (preferably with antithyroid drugs in patients at high risk for TED progression) and the treatment of the OSD are general measures recommended for all TED patients in order to prevent disease progression. 12 Since up to 60% of patients with mild TED experience spontaneous remission, local and lifestyle measures and watchful monitoring are generally recommended. 13 Smoking cessation was the most frequent recommendation for the management of active mild TED in a survey of European and American TED specialists. 55 According to current recommendations, mild TED without risk factors can be managed outside TED expert centers, unless progression occurs.12,13
What are the most important clinical trials for mild TED?
In contrast to moderate-to-severe TED, very few multicenter RCT have been conducted or are planned in this field. The imprecise definition, heterogeneous clinical presentation and self-limiting course of the disease make such studies difficult to perform.
Available RCTs on mild TED predominantly focused on selenium supplementation. The rationale behind selenium administration in TED comes from its antioxidant (via incorporation in thioredoxin reductase and glutathione peroxidase) and immunomodulatory effects.56,57 In a blinded placebo-controlled multicenter trial conducted in Europe, including geographic areas of possible selenium deficiency, patients with active, mild TED of short duration (<18 months) were randomized to receive for 6 months either selenium selenite (100 µg twice a day) or pentoxifylline or placebo. 17 After 6 months of therapy, improvements in GO–QOL scores, soft tissue signs (CAS) and lid aperture were noted with selenium therapy, but not with placebo, and persisted for an additional 6 months after therapy was stopped. Moreover, the rate of worsening of TED was lower in the selenium group than in the placebo group (7% vs. 26%, p = 0.01). Selenium supplementation had no significant effect on proptosis and eye muscle dysfunction. Similar results were obtained in a placebo-controlled RCT performed in Mexico, although the study may have been subject to methodological flaws.58,59 The Mediterranean diet, naturally enriched in selenium as well as in many antioxidants with anti-inflammatory properties, might also have a beneficial effect on soft tissue involvement and eyelid aperture in patients with mild TED. 60
One double-blind randomized trial compared the efficacy of orbital irradiation with sham irradiation in mild TED. 61 However, mild disease in this study was defined as having a mild extraocular eye muscle motility disturbance (mostly elevation) with or without mild/moderate eyelid swelling or proptosis of 24 mm or less, which does not correspond fully with the current definition. Radiotherapy was effective in improving eye muscle motility and decreasing the severity of diplopia. Importantly, worsening of the TED could not be prevented by radiotherapy, which occurred in 14% of the irradiated and 16% of the sham-irradiated patients. To the best of our knowledge, there are no RCTs concerning immunosuppressive treatments in mild TED. 62
Regarding rehabilitative procedures, various noninvasive (including triamcinolone and botulinum toxin injections) and surgical interventions (including orbital decompressions, strabismus, and eyelid surgery) have been shown to be effective, improving QoL in patients with TED, regardless of its severity.63–68 However, the interpretation of available data is often limited by a small number of RCT, methodological heterogeneity and lack of standardized endpoints, incorporating both functional and aesthetic outcomes.
Did the clinical practice guidelines concerning management of mild TED change across time?
Clinical practice guidelines (CPG) can only summarize the best available evidence, which is scarce and of low/moderate quality in mild TED. For this reason, during the last two decades, the recommendations concerning the management of mild TED did not change significantly12,21,69,70 and a watchful strategy combined with the control of risk factors is generally recommended (Table 1).
Selected Clinical Practice Guidelines concerning Management of Mild TED (apart from Smoking Cessation, Normalizing Thyroid Status, and Local Lubricants Usage)
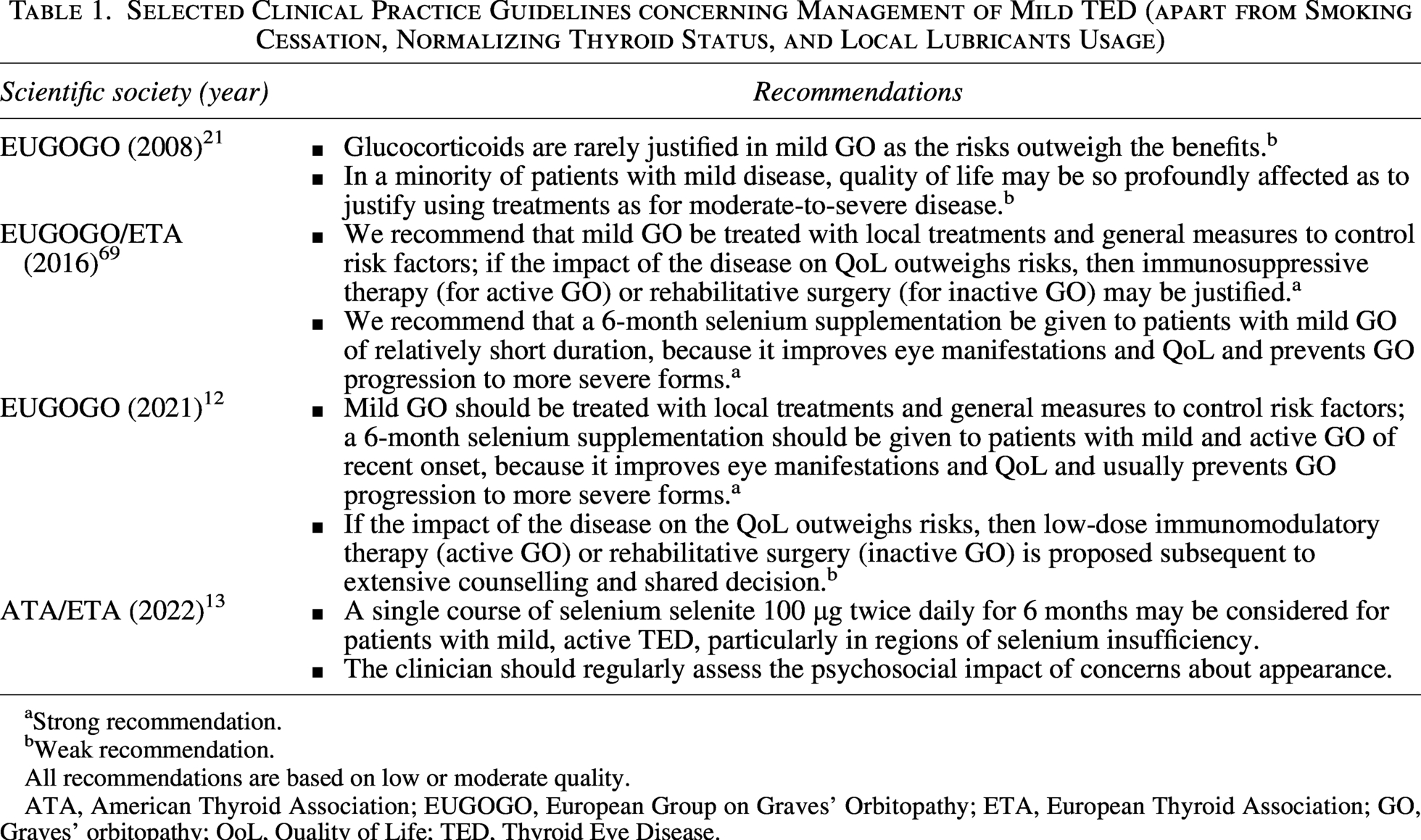
Strong recommendation.
Weak recommendation.
All recommendations are based on low or moderate quality.
ATA, American Thyroid Association; EUGOGO, European Group on Graves’ Orbitopathy; ETA, European Thyroid Association; GO, Graves’ orbitopathy; QoL, Quality of Life; TED, Thyroid Eye Disease.
The only pharmacologic intervention for active mild TED mentioned in CPG is selenium supplementation. A course of sodium selenite at a dose of 100 μg twice daily (equivalent to 91.3 μg of elemental selenium twice daily) for 6 months is either recommended (strong recommendation) or suggested (weak recommendation) (Table 1). The difference in recommendations reflects the lower quality and conflicting evidence of the selenium trials conducted so far.17,58,59,71 The strongest evidence favoring selenium administration came from the EUGOGO trial, which gave rise to the belief that in patients residing in selenium-insufficient areas, this treatment may improve eye manifestations (CAS and palpebral aperture) and QoL, and prevent TED progression to more severe forms. The major limitation of this trial 17 was the lack of evaluation of baseline selenium levels. The clinical relevance of selenium treatment was therefore called into question when a multicenter, randomized, open-label trial conducted in South Korea—a region known to be selenium-sufficient—failed to demonstrate a significant improvement in GO–QOL scores among the 84 patients with mild-to-moderate TED who were randomized to receive either selenium (200 µg/day) in combination with a vitamin B complex or the vitamin B complex alone for 6 months. 71 In long-standing, inactive, mild TED, there is no evidence that selenium is effective.
Although mild TED is traditionally defined as having insufficient impact on daily life to warrant immunomodulatory or surgical intervention, even minimal lid retraction, soft tissue involvement, proptosis and eye muscle dysfunction and OSD can have a negative impact on patients’ self-esteem and self-awareness. 72 In selected cases with a significant impact on QoL and/or with a progressing disease, “low-dose immunomodulatory/immunosuppressive therapy” (active TED) or rehabilitative surgery (inactive TED) is recommended/suggested subsequent to shared decision making. Unfortunately, details concerning “low-dose immunomodulatory therapy” (including which agent, what dose and how long) are missing in all CPG’s. In systemic reviews, it is sometimes stated that occasionally, mild TED may be managed as moderate-to-severe TED. 4 Moreover, individualized corrective procedures in mild TED should be considered in centers that have experience and expertise in those techniques.
How is mild TED managed in real life?
According to CPG, patients with mild TED without risk factors, whose eye symptoms are improving following normalization of thyroid status and local lubricants, can be managed outside TED referral centers.12,13 Patients with mild TED comprise 40–50% of referrals to EUGOGO centers.3,42 A 2003 study found that 44% of mild TED patients in referral centers received TED specific treatment (corticosteroids, radiotherapy or lanreotide/octreotide), with 5% and 17% having surgery in active and inactive disease. 24 More concerningly, the use of quantifiable QoL assessments in routine clinical practice appears to be low (21% in one survey) making it more difficult to justify intervention. 73
With limited clinical trial data, medical surveys can help to collect insights from professionals and patients about the management of mild TED and highlight important regional and professional differences (Table 2). Looking at selected treatment options: (i) selenium supplementation was recommended by 24 − 91%, (ii) oral steroids by 10 − 30%, (iii) intravenous steroids by 5 − 44%, (iv) orbital glucocorticoid injection by 10 − 81% and (v) teprotumumab by 0–10% of physicians. The wide variation in the use of immunosuppressive drugs and targeted therapies for mild TED, despite their unclear efficacy and use outside the recommended indications, highlights the need for more evidence-based strategies.
Selected, Recent Surveys Analysing the Management of Mild TED
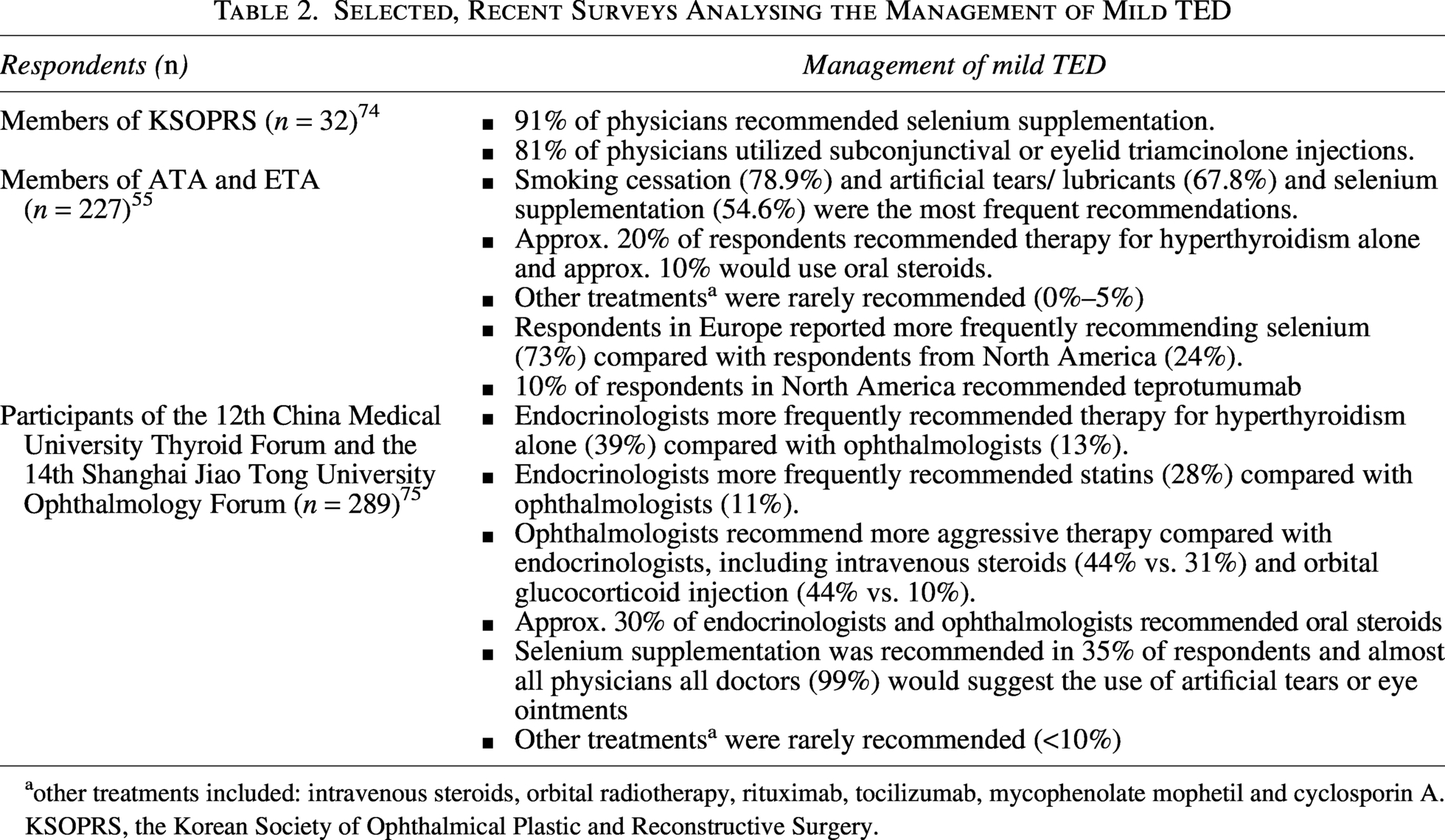
other treatments included: intravenous steroids, orbital radiotherapy, rituximab, tocilizumab, mycophenolate mophetil and cyclosporin A.
KSOPRS, the Korean Society of Ophthalmical Plastic and Reconstructive Surgery.
Future research
Identifying knowledge gaps in the management of mild TED provides a foundation for further research aimed at improving scientific guidance. Future research should focus on preventing the development and progression of mild TED, as well as on assessing and treating the condition. The use of selenium and its applicability in a global context and the importance of addressing metabolic stressors must be clarified. Further studies are required to confirm whether the expected benefits of using new drugs that target TSH receptor antibodies in GD 76 will also extend to TED prevention. In a resource-limited health care landscape, it is unlikely that multidisciplinary TED care would be available to all mild TED patients and whether the new artificial intelligence-driven image capture technologies would result in a paradigm shift of detecting and predicting an adverse TED course. 77 More targeted treatment of the ubiquitous OSD, may positively impact on patients’ QoL in addition to addressing the typical disfiguring manifestations. 78 Most importantly, future research should address whether local or topical treatment remains the preferred, cost-effective and safe option against the emerging systemic targeted biological therapies.79,80
Conclusions
Mild TED is a heterogeneous disease. Although it is the most common form of TED, the level of evidence for the current recommended therapies is weak, resulting in significant differences in management in different countries and by different specialists. While the majority of cases of mild TED will remit spontaneously, therapeutic interventions could be justified in the remaining significant number of patients with longstanding or progressing disease, and to improve the quality of life. The wide variation in the use of systemic treatments and surgery for mild TED in real-life settings may reflect the perception that a higher proportion of these patients experience a significant functional impairment and reduced QoL than could be expected based on the current definition of mild TED. Future research should identify patients with mild TED who could benefit more from experienced, multidisciplinary management.
Authors’ Contributions
M.-C.B.: Conceptualization (co-lead); writing—original draft (co-lead); writing—review and editing (equal). T.B.: Conceptualization (co-lead); writing—original draft (co-lead); writing—review and editing (equal). V.L.: Writing—original draft (equal); writing—review and editing (equal). P.P.: Conceptualization (supporting); writing—original draft (equal); writing—review and editing (equal).
Footnotes
Author Disclosure Statement
M.-C.B.: member of EUGOGO Executive Committee, speaker fees and honoraria for advisory boards of Amgen. T.B.: EUGOGO member; speaker fees and/or honoraria for advisory boards of Amgen, Argenx, Berlin-Chemie, Lundbeck and Merck. V.L.: Member of EUGOGO Executive Committee; speaker fees and/or honoraria for advisory boards of Amgen, Argenx, Roche and Viridian, Institutional Support from Amgen, Argenx, Sling, Lassen & Viridian. P.P.: EUGOGO member.
Funding Information
No funding sources to declare.