
Abstract
Background
Work disability is a major public health challenge, with various health conditions leading to long-term sickness and early retirement, placing a substantial burden on individuals and society.
Objective
This systematic review aimed to identify key health-related risk factors for work disabilities, highlighting the importance of early prevention strategies.
Methods
A systematic literature search was conducted in 06/2023 using MEDLINE via PubMed, EMBASE via OVID, and CINAHL via Cochrane Library Trials. Two independent reviewers screened abstracts and reviewed full-text articles describing risk factors for work disabilities. Data extraction followed PRISMA guidelines, with the databases searched using synonymous keywords for “risk factors” and “work disability”.
Results
Of the 61,872 articles identified, 17 met the inclusion criteria. The studies identified several health-related risk factors leading to work disabilities. The most frequently reported conditions were common mental disorders and musculoskeletal disorders, often leading to short- or long-term sick leave. The review highlighted that health-related risk factors frequently co-occur and interact, suggesting that work disability is rarely due to a single factor. The quality of the included studies varied, and many relied on self-reported data, which can introduce bias.
Conclusion
(Chronic) conditions, particularly mental and musculoskeletal disorders, are significant risk factors for work disability. Primary and secondary prevention measures, such as rehabilitation are crucial to mitigate the need for disability retirement. Future research should focus on prospective cohort studies and a thorough scientific investigation of potential intervention factors to provide decision-makers with information on cost-effective prevention programs.
Keywords
Introduction
Technological advancements and automation have profoundly reshaped the labor market, reducing the need for physical labor in industrialized countries. The reduction in physical labor, coupled with insufficient physical activity, has been linked to increased mortality and reduced longevity.1,2 The shift necessitates changes in the health system and working environments to address new health challenges.
The evolving labor market, along with demographic changes, significantly impacts the health system. As life expectancy rises and the workforce ages, there is an increased demand for healthcare services, particularly in nursing and rehabilitation.3–6 Coordinated efforts from employers, governments, and other relevant stakeholders are required to promote workability up to the statutory retirement age. Effective prevention and rehabilitation measures are crucial in reducing the necessity for disability pensions. A systematic review has demonstrated the importance of occupational rehabilitation in improving return-to-work outcomes for individuals suffering from back pain. 7 By 2030, the demographic change will become even more evident, as the baby boomer generation (1959–1968) begins turning 70, leading to a surge in retirements. 8 This development will necessitate an increased labor force and prompt discussions about raising the retirement age to manage potential costs. 9 Promoting work ability until the statutory retirement age requires a coordinated effort by employers, governments, trade unions, and other relevant stakeholders.
The COVID-19 pandemic has heightened public awareness of health-related lifestyles and the importance of medical checkups, underscoring the need for studies on preventive health measures that can identify risk factors early and prevent work disability.10,11 For instance, the National Institute for Health and Care Excellence (NICE) guidelines on long covid (2020) advocated for more interventions and studies to be able to offer the best possible treatment to long COVID patients. 12
This increased interest in health-related lifestyles requires greater support from studies on preventive checkups that screen a large number of the population for health-related risk factors.13–15 The majority of these risk factors are modifiable, meaning they can be influenced by the individual. These include behaviors such as smoking, an unhealthy diet, and a lack of physical activity leading to conditions like high blood pressure and obesity.16,17 Additionally, unchangeable factors such as gender or age can also pose significant risks. 18
This study defines health-related risk factors for work disability as conditions that elevate the risk of developing diseases, potentially resulting in the premature termination of a worker's career. Identifying these factors is crucial for developing targeted prevention programs that enhance work retention and overall workforce health. According to a survey from the Robert Koch-Institut (RKI) in 2020, 12 the increase in cardiovascular diseases, pulmonary diseases, diabetes, and arthropathy creates a high need for innovation to secure the individual's ability to work.14,19 Moreover, the prevalence of obesity has risen substantially in recent years, especially among young male adults. 20 The number of pulmonary diseases, particularly bronchial asthma, has increased, especially in the younger generation, with one in every 10 people diagnosed with asthma. 11 Furthermore, the prevalence of diabetes among those aged 55–74 is anticipated to expand from 2.4 million to 3.9 million people, implying a 79% increase in healthcare costs. Since 2003, musculoskeletal diseases in individuals over 50 have increased by 6%. During the COVID-19 pandemic, young adults and children experienced an increase in depression and anxiety.21–23
In summary, these challenges facing public health likely denote a lower quality of life and higher costs for the social and health care systems, such as statutory pension insurance.24,25 People who are not working for various health-related or other reasons reported significantly higher numbers for anxiety, depression, health-related problems, and a lower quality of life.26–28 Thus, focusing on preventive and rehabilitative measures is crucial to ensure that people can maintain a healthy working life, reducing the risk of health-related retirement. However, further information on which risk factors to target these preventative efforts is needed.
Therefore, this systematic review aimed to provide an overview of potentially relevant health-related risk factors for the primary outcome of work disability to influence, for example, prevention and rehabilitation measures and adapt working conditions as needed.
Methods
A systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.29,30 The review protocol was registered with the International Prospective Register of Systematic Reviews (CRD42023422118).
Eligibility criteria
In our systematic review, we implemented a stringent set of inclusion and exclusion criteria to ensure the quality and relevance of the included studies.
Search methods for identification of studies
The authors selected relevant studies published from 2000 until June 2023, by searching the electronic databases MEDLINE via PubMed, EMBASE via OVID, and CINAHL via Cochrane Library Trials. The search of all published studies was conducted from May to July 2023. The keywords for the investigation were identified using the knowledge of the contributing authors. We applied the English language, and the search keywords included “risk factors” and “work disability” (see Table 1). The terms were carefully selected by identifying which terms have previously been used in related studies. The precise search strategy for the databases was:
Search domains and terms.
Search: (risk factor [Title/Abstract]) OR (determinants [Title/Abstract]) AND (work disability [Title/Abstract]) OR (sick leave [Title/Abstract]) OR (unemployment [Title/Abstract]) AND (2000:2023[pdat])
Study selection
The authors used EndNote 20.5 to assess and document the full reports on inclusion or exclusion according to the predefined selection criteria. Studies were selected independently by two reviewers (LK and LC). We considered all potentially eligible studies. Initially, the titles and abstracts were screened and full reports from potentially relevant studies were retrieved. Disagreements were resolved by discussion and where agreement could not be reached, a third reviewer was consulted (BW).
Data collection and extraction
Data extraction was performed by LK and LC and checked by BW. Both independent raters reviewed full-text versions of the articles and articles were retained if they met inclusion criteria. The agreement on inclusion and exclusion assignment was unanimous. Data extracted from the studies included the following information: lead author, time of data collection, study design, sample size, demographic characteristics (age, gender), measurement, and diagnosis as a determinant for work disability, confounding factors, and reported outcomes. All data required to answer the research questions were published within the papers, so no contact with authors was necessary. These results were recorded in the following table.
Quality assessment and risk of bias
The risk of bias was assessed using the QUIPS (Quality in Prognostic Studies) assessment tool.32,33 This tool evaluates prognostic studies for bias within six domains: (I) study participation, (II) study attrition, (III) prognostic factor measurement, (IV) outcome measurement, (V) study confounding, and (VI) statistical analysis reporting. A score of low, moderate, or high is assigned to each domain. Two authors (LK and LC) independently applied the QUIPS assessment tool, and a third author (BW) provided input as needed for consensus. Ideally, studies were considered to be of low risk of bias. That was the case when the items were rated as low or moderate on all of the six domains, with at least four rated as low. A study was scored a high risk of bias if two or more of the domains were scored as high. The remaining studies were scored as moderate. 33
The methodological quality of several studies34–41 was assessed using the Jadad scale. 42 All other studies are not Randomized Controlled Trials (RCT) and we therefore refrained from using the Jadad scale. Two reviewers (LK and LC) performed the assessment independently, and discrepancies between reviewers were resolved by discussion for consensus. Studies achieving 3 or more points (from a maximum of five) were considered to be of high quality, while studies scoring below three were considered to be of low quality.
Ethics and data analysis
The study did not involve contact with humans, so the need for ethical approval was waived. A meta-analysis of health-related risk factors was considered inappropriate due to the high heterogeneity in the definition of the risk factors between the studies. Accordingly, a narrative synthesis of studies was conducted.
Results
The literature search resulted in a total number of 61,872 hits. After marking records as ineligible by automation tools and duplicate removal, 2290 hits were screened on the title and abstract. This resulted in 69 full-text articles that were assessed for eligibility, of which 38 articles did not meet the inclusion criteria. Of the remaining 31 articles, 14 were eliminated, leaving 17 articles that met the inclusion criteria. Figure 1 provides a visual representation of the literature screening process.

PRISMA diagram showing a selection of studies for systematic review.
Characteristics of included studies
The characteristics of the included articles are presented in Table 2.34–41,43–51 Variations in definitions and measurements of work disability were evident. The included studies reported disability due to illness and sick leave. Of the 17 included studies, most studies (n = 9) were prospective or retrospective cohort studies.35,44–51 One included study was a cluster analysis. 43 The remaining studies (n = 7) were RCTs.34,36,38–41,49 Studies were executed in eight different countries, all of them in Europe. There was considerable variation across studies regarding sample size. The sample size ranged from 96 up to 13,007 subjects.
Characteristics of included studies.
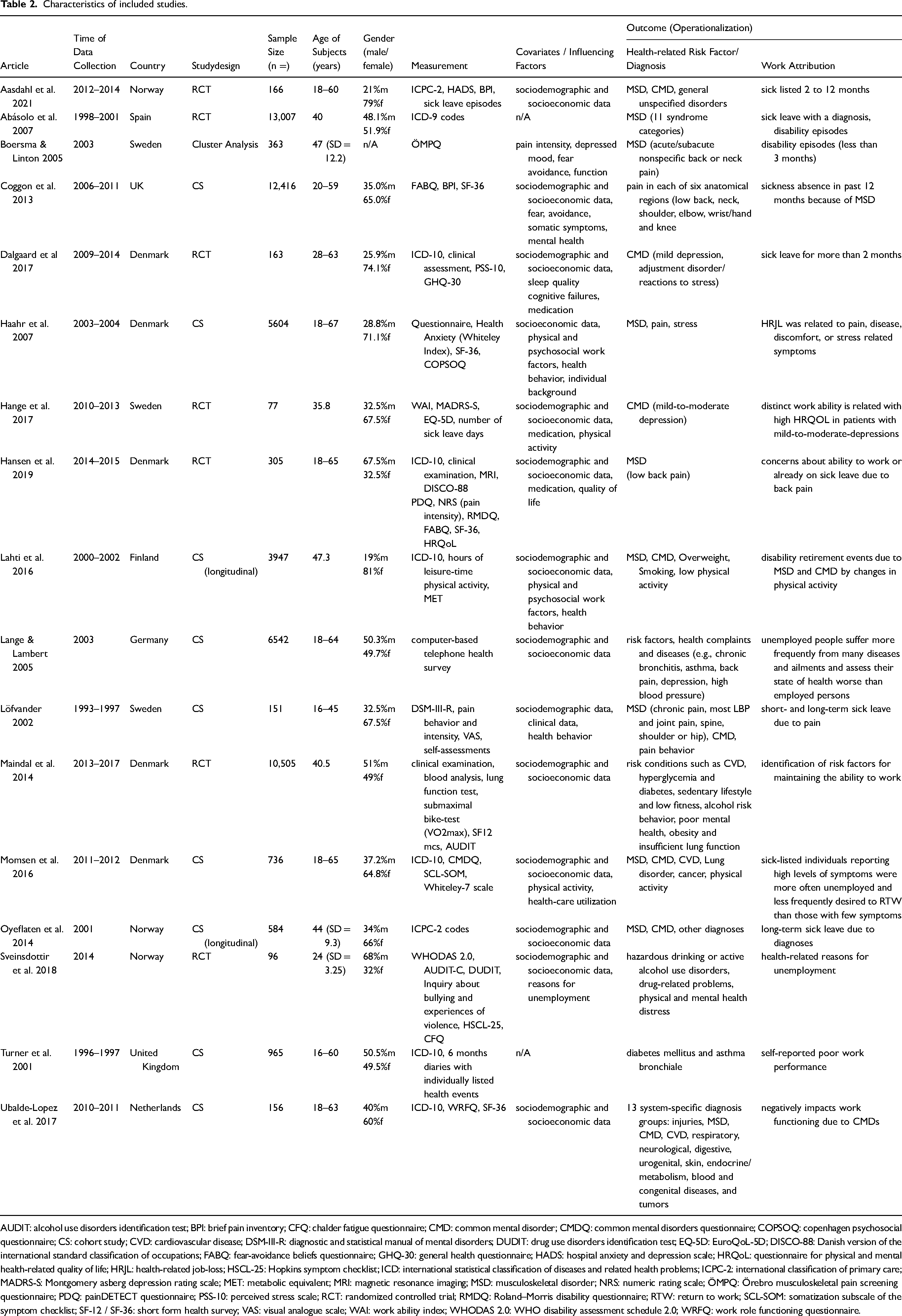
AUDIT: alcohol use disorders identification test; BPI: brief pain inventory; CFQ: chalder fatigue questionnaire; CMD: common mental disorder; CMDQ: common mental disorders questionnaire; COPSOQ: copenhagen psychosocial questionnaire; CS: cohort study; CVD: cardiovascular disease; DSM-III-R: diagnostic and statistical manual of mental disorders; DUDIT: drug use disorders identification test; EQ-5D: EuroQoL-5D; DISCO-88: Danish version of the international standard classification of occupations; FABQ: fear-avoidance beliefs questionnaire; GHQ-30: general health questionnaire; HADS: hospital anxiety and depression scale; HRQoL: questionnaire for physical and mental health-related quality of life; HRJL: health-related job-loss; HSCL-25: Hopkins symptom checklist; ICD: international statistical classification of diseases and related health problems; ICPC-2: international classification of primary care; MADRS-S: Montgomery asberg depression rating scale; MET: metabolic equivalent; MRI: magnetic resonance imaging; MSD: musculoskeletal disorder; NRS: numeric rating scale; ÖMPQ: Örebro musculoskeletal pain screening questionnaire; PDQ: painDETECT questionnaire; PSS-10: perceived stress scale; RCT: randomized controlled trial; RMDQ: Roland–Morris disability questionnaire; RTW: return to work; SCL-SOM: somatization subscale of the symptom checklist; SF-12 / SF-36: short form health survey; VAS: visual analogue scale; WAI: work ability index; WHODAS 2.0: WHO disability assessment schedule 2.0; WRFQ: work role functioning questionnaire.
Quality assessment and risk of bias
A summary of the quality assessment using the Jadad scale scores is shown below. The Jadad scale could only be applied to selected studies because the tool is explicit for RCTs. The total scores of the studies (n = 7) ranged from a minimum of 1 point to a maximum of 4 points. One study had low quality (1 point) 41 because of the high risk in terms of randomization, blinding, and an account of all subjects. Four studies had a medium to high quality (3 points).34,36,38,39 The subjects were randomly assigned into groups and the randomization was accomplished using a computer-generated random number list, but the fate of all subjects in this study is not described (e.g., drop-outs, screening failure). In conclusion, two studies showed a high quality on the Jadad scale (4 points)37,40 because they were methodically very well performed and described.
The risk of bias was assessed using QUIPS (Quality in Prognostic Studies). A summary of the risk of bias is shown in Figure 2. According to the QUIPS evaluation, more than half of the studies showed a moderate risk of bias. The most common moderate score presented in domain five is “study confounding”. The percentage agreement between reviewers (LK and LC) was 94% agreement.
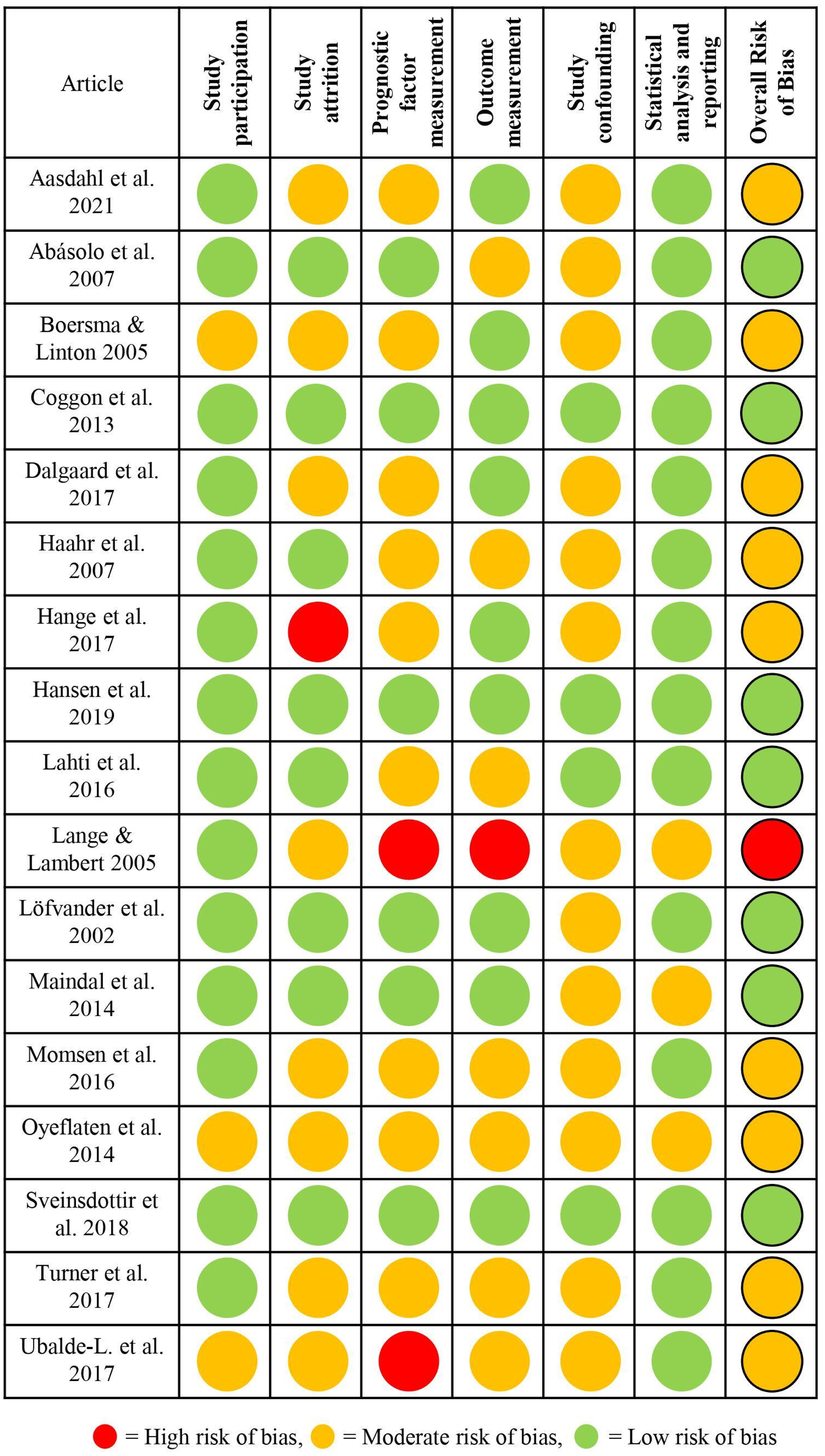
Risk of bias tool.
Health-related risk factors
Health-related risk factors are factors or conditions that increase the likelihood of developing certain health problems or diseases. These risk factors can be behavioral, environmental, genetic, or a combination of factors. Risk factors for work disability are conditions, behaviors, or circumstances that increase the risk that an individual will be unable to perform their occupational tasks due to health issues.
All studies addressed health-related risk factors (e.g., behavior, working environment, physical or psychological complaints, or diagnosed diseases) that led to work disability. To collect data on risk factors, the included studies examined health status, sick leave, and/or work ability. In some studies the diseases were diagnosed by physicians,34,36,38–40,44,46–49 in others, the symptoms were self-reported by the subjects.35–37,41,43,45,50,51 One of the main findings of the systematic review is that the studies primarily examined diseases, and there were fewer studies on other health-related risk factors (such as behaviors or lifestyle-related risk factors). Almost all articles included MSDs (Musculoskeletal Disorders) and/or CMDs (Common Mental Disorders). CMD, where depression, anxiety, and fear were most commonly identified36–39,41,44–47,49–51 Dalgaard et al. reported adjustment disorder/reactions to stress and sleeping problems in addition to depression. 39 Sveinsdottir et al. reported physical and psychological fatigue, maladaptive coping strategies (helplessness and hopelessness), and insomnia as additional categories. 37 CMDs can affect cognitive functioning, concentration, and emotional stability, which are essential for maintaining productivity and effective communication at the workplace.38,46,49
MSDs were the most frequently diagnosed/examined and mentioned, along with CMDs. Commonly mentioned symptoms and diseases concerning the musculoskeletal system were (low) back, neck, and/or shoulder pain.34,35,37,38,40,43–47,49–51 Abásolo et al. grouped the ICD-9 codes into 11 syndrome categories and presented them more in detail (back pain, neck pain, tendinitis, sciatica, muscular pain, microcrystalline arthritis, peripheral osteoarthritis, inflammatory diseases, knee pain, carpal tunnel syndrome, other (e.g., osteoporosis, joint infections or tumors). 34 MSDs can limit physical functioning, making it difficult to perform tasks that require physical effort or stamina. In all studies, the ability to work was limited in the short or long term due to the illness. The decisive markers were sick leave with a diagnosis of MSD. Abasolo et al. explicitly mentioned that sick leave due to trauma, surgery, or accidents at work was excluded. 34 Haahr et al. found that health-related Job-loss (HRJL) was associated with pain, disease, or discomfort in the neck, back, arms, or legs. 35 Löfvander et al. found that an important risk factor for long-term sick leave was multiple enthesopathy, which often occurs in association with inflammatory joint disease. 50 Many subjects reported chronic pain that limits mobility and flexibility, making it difficult to perform tasks that require bending, lifting, or prolonged standing or sitting. The study by Coggon et al. examined the reasons for international differences in sickness absence among employees. Namely, the risk factors were older age, lower education level, a tendency of somatization, physical strain at work, and prolonged absence due to non-MSDs, but these factors explained only a small part of the more than 30-fold variation in prevalence between occupational groups.51,52 Prolonged absence due to MSDs was more common in groups with higher time pressure at work, lower job control, and more negative beliefs about the work-relatedness of MSDs.51,52
Another condition associated with work disability were cardiovascular diseases (CVDs), which refer to a group of disorders that affect the heart and blood vessels. Some common types of CVDs, such as hypertension (high blood pressure), heart arrhythmias, and coronary artery disease were diagnosed and mentioned in the articles.36,45–47,49
CVDs also play a role in the aftermath of the COVID-19 pandemic raising the awareness of respiratory diseases. Nevertheless, they have also been frequently mentioned in studies before 2019. Lung diseases, asthma bronchiale, and chronic bronchitis were most frequently mentioned as leading to longer-term sick leave.36,45,46,48,49 Turner et al. reported that the participants self-rated their work performance as poor due to the diseases (asthma bronchiale and diabetes mellitus). 48
Most of the aforementioned diseases rarely occur alone, but rather in combination or as a consequence of other diseases, such as obesity.36,44 The causes can be very diverse, but low physical activity and a sedentary lifestyle are the most commonly mentioned risk factors for obesity and can contribute to the development of chronic diseases that eventually lead to work disability.36,44,46 Following on from this, it is noted that unhealthy consumer behavior plays a role, and addictive behavior (smoking and alcohol abuse/binge drinking) is considered a risk factor for several diseases like CVD, lung diseases, and CMD and thus for work disability36,44 particularly among young workers. 37
Some studies also collected blood samples and found that some abnormal blood values, such as increased blood lipid level, hyperglycemia, glycated hemoglobin, and HbA1c (indicative of diabetes) are associated with increased risk for work disability.36,45,48,49
Other individual risk factors have been mentioned in individual studies, e.g., cancer/tumors, gastrointestinal complaints, injuries, skin diseases, neurological diseases, and dizziness, which are less common and usually occur in combination with other complaints.
Therefore, it is of high importance to note that these health-related risk factors often occur in combination and can influence each other. Most of the included studies also emphasized that there is not just one risk factor that is critical to work disability but a multitude of risk factors that need to be carefully evaluated. Identifying and managing these risk factors as soon as they become noticeable can help reduce the risk of disease with improved health and thus lead to a healthier professional career. Figure 3 provides an overview of the diseases and health-related risk factors mentioned in the included studies.

Health-related risk factors for work disability.
Discussion
This systematic review identifies several critical health-related risk factors for work disability. Particular emphasis is put on health-related risk factors that increase the likelihood of an occurrence of mental health disorders and musculoskeletal conditions such as back pain. Additionally, internal diseases like cardiovascular diseases (CVD) and diabetes mellitus are highlighted as significant contributors. These findings have important implications for the development of preventive strategies and interventions aimed at reducing work disability.
Occupational safety and workplace health promotion have become more important in industrialized countries in recent decades. There is a growing interest in the scientific monitoring of prevention programs as well as the effectiveness of interventions.53,54
The objective of the studies examined in this review is to detect diseases that lead to incapacity for work and find out what risk factors contribute to the development of those diseases. Various treatment methods were targeted for this purpose. Many studies have used self-reported questionnaires to be able to reach a high number of subjects (e.g.,34–37,41,43,45,50,51). Other studies have documented diagnoses according to the International Statistical Classification of Diseases and Related Health Problems (ICD), primarily ICD-10.34,38–40,44,46–49 In some of the studies included in the review, physicians’ diagnoses as reasons for work disability were not shown. In some of the studies, the subjects were only screened via questionnaire, which may be less valid compared to a physician's diagnosis. In addition, some of the authors did not use validated questionnaires, some used questionnaires that were not (yet) validated. Therefore, we see a slight reduction in the validity of those studies. Overall, there was a slight discrepancy to be seen regarding the quality of the studies. Further studies should be conducted with a more defined focus on the reasons and risk factors for long-term sickness absence and potentially already checking for the success of intervention factors.
Unfortunately, data from emerging countries are not yet sufficiently available, which is confirmed by the literature included in this review. All included studies were from Europe, which makes the transferability of the results to countries with different workplace patterns difficult. Except for one study that investigated the cultural differences in MSD/pain and used questionnaires in over 18 countries worldwide.51,52 Occupational activities and thus mental and physical stress differ worldwide. A sedentary lifestyle appears to be an important health-related risk factor regardless of whether physical activity was performed or not. 55 The majority of the diseases that have been diagnosed in the studies are associated mainly with sedentary jobs i.e., work on computers, that require little physical activity.56–58 The results may however most likely be extrapolated to other highly industrialized countries. The most commonly identified diseases include mental disorders, back pain, neck and shoulder pain, obesity, and high blood pressure. The mental illnesses mentioned in the studies are possibly related to the individuals’ stress levels due to the high workload, based on a system of modern-quick-paced meritocracy.57,58 Mental health disorders, including depression and anxiety, are major contributors to work disability. The impact of these conditions on work ability is profound, often leading to prolonged absenteeism and reduced productivity. The review underscores the necessity of early identification and intervention for mental health issues in the workplace. Specific risk factors for mental health issues in the workplace include high job demands, lack of control, poor work-life balance, and negative workplace culture. Early predictors include decreased productivity, increased absenteeism, mood changes, and physical symptoms like fatigue and headaches.23,56 Neck and back pain have also been related to a stressful sedentary workplace and desk jobs.59,60 Workplace ergonomics, regular physical activity, and early intervention programs could reduce the incidence and severity of back pain. Respiratory diseases have also come into focus. This is most likely in line with the worldwide increase in airway allergies and an aspect that should be addressed in future prevention programs. Particularly in light of the COVID-19 pandemic, respiratory illnesses are expected to increase in the coming years. The long-lasting impact of the pandemic on employees’ health is still unknown. 61
Even though socioeconomic factors could not be considered, our literature review presents an overview of the diversity of health-related risk factors. In addition to diseases, other factors are also relevant that either lead to incapacity for work or have a negative influence on the return to work (RTW) (e.g., a previous period of unemployment, industrial accident, activity limitations, higher age, being female). 62 Cancelliere et al. examined 56 systematic reviews that addressed RTW in various conditions and injuries. The authors evaluated that the effects that may be associated with positive RTW outcomes were a higher socioeconomic status, strong self-efficacy, and optimistic expectations for recovery and return to work. 62 Støver et al. found in a health survey of work environment and work disability associations among 5749 working people that individuals who report a poor work environment have a higher risk for work disability. 63 Additionally, the social interaction within the workplace plays a crucial role in the RTW process. Tjulin et al. explored the experiences of co-workers and highlighted the importance of social support and positive interactions for successful RTW outcomes. 64 This reinforces the thesis that several factors, such as work environment, socioeconomic status, and behavior, are associated with disability. Coggon et al. examined the prevalence of low back pain and wrist/hand pain in over 18 countries and found that musculoskeletal pain is widespread, but there are large international differences as they can only be partially explained by personal and socioeconomic risk factors.65,66 Certain work environments can exacerbate health conditions such as ergonomic issues (e.g., poor seating and posture or lack of breaks and movement) that contribute to musculoskeletal problems, thus they are presenting an important health-related risk factor.67,68 Employers should take steps to address these health-related risk factors and support employees with health conditions to minimize the impact on work disability.
Aging increases the likelihood of age-related health issues that can affect an individual's ability to meet the demands of their job, thus age can be considered a health-related risk factor and has a reciprocal effect on other health-related risk factors. In older people, physical strength and reaction time could decrease, thus susceptibility to chronic diseases increases. It is important to ensure access to health services when health problems arise. Limited access or even lack of access to healthcare services can result in unmanaged health conditions, leading to worsening symptoms and reduced ability to work. 69
Prognostic factors can be divided into non-modifiable and potentially modifiable factors. The relevant prognostic factors for work disability measured in this review were non-modifiable (e.g., diagnoses) or less easy to modify (therapy-related). However, the assessment of these non- or difficultly modifiable factors remains relevant information for the healthcare system and statutory pension insurance. Rehabilitation therapy becomes necessary when a disease has occurred. Identifying health-related risk factors before the appearance of an illness requires expanded screenings, ensuring long-term health and preserving work ability. 69
Strengths
The main strength of this review is that this is a systematic review regarding explicitly health-related risk factors for work disability. The review should state the diversity of those risk factors. Another strength of this review is the methodological quality, ensured by following the PRISMA guidelines for systematic reviews. An extensive literature search was conducted based on a comprehensive search strategy. 29 By including cohort studies, RCTs, and case-control studies, we are confident that this review presents a complete overview of existing studies on this topic.
Limitations
Despite the extensive search, a potential limitation may be the exclusion of non-English studies and grey literature (research and information produced outside of traditional commercial or academic publishing channels, e.g., government reports, conference papers, white papers, or theses. This limitation suggests that the findings might not fully represent the global body of research on this topic.
Additionally, the heterogeneity of study designs, populations, and definitions of terms across the included studies presents a challenge for drawing definitive conclusions. The variability in methodologies and the use of different diagnostic criteria make it difficult to directly compare and synthesize the results of the studies. Another limitation is the reliance on self-reported data in many of the studies. Self-reported questionnaires, while useful for reaching a large number of subjects, can introduce bias and may not be as accurate as physician-diagnosed conditions. Some studies included in the review used non-validated questionnaires, further reducing the reliability of the findings. This limitation underscores the need for future studies to use validated and standardized assessment tools to improve the accuracy and validity of the data. In addition, the QUIPS tool is a non-validated instrument, which could give room for personal interpretation. Nevertheless, the QUIPS tool is recommended by the Cochrane Methods Prognosis group and designed for prognostic studies addressing all common sources of bias. Based on this, we considered the tool suitable for evaluating the risk of bias.32,70
Conclusion
This systematic literature review suggests that there are multiple health-related risk factors for work disability. Based on this systematic review, the strongest overall risk factors include mental illnesses and back pain. Also, the importance of internal diseases like CVD and diabetes mellitus and related symptoms should not be overlooked. Unlike orthopedic diseases and psychological disorders, internal diseases often evolve unnoticed by the patient or are trivialized like e.g., asthma, which has not been the focus of work-related prevention programs so far. These findings underscore the necessity for screenings, comprehensive preventive strategies and interventions. 15 Early identification of these risk factors is of great importance for better strategies in primary and secondary prevention of disease progress and work disability. Employers, healthcare providers, and policymakers must work together to implement effective prevention and management strategies, fostering healthier and more productive work environments.
To improve the quality of future studies, it is strongly recommended to standardize design and methodology and to conduct more high-quality longitudinal studies. In addition, advocacy for the universal use of consistent terms and definitions is essential to improve clarity and comparability across studies. It is also important to encourage research in different geographical regions, including developing countries. This broader focus will guide future studies and allow for the generalization of results, making the findings more globally applicable. Expanding the scope beyond European countries, as noted in the limitations, will ensure a more comprehensive understanding of risk factors for work disability worldwide.
Footnotes
Abbreviations
Acknowledgments
Not applicable
Ethical considerations
Not applicable
Informed consent
Not applicable
Reporting guidelines
PRISMA guidelines
Author contributions
LK had the idea for the study conception and design, wrote the first draft, and conducted the analyses. LK and LC selected the studies for inclusion and abstracted data. LK wrote the first draft. LC, MH and BW critically revised the paper for important intellectual content. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Registry and the Registration No. of the study
The review protocol was registered with the International Prospective Register of Systematic Reviews (CRD42023422118).