
Abstract
Background
There has been a growing interest in defining the educational environment in medical and dental institutes that includes different measures to rate and improve it. Evidence suggests that the educational environment directly impacts teaching, learning, well-being, and students’ involvement and their successful professional performance. The Undergraduate Clinical Education Environment Measure (UCEEM) is widely used in medical and allied health sciences institutions to evaluate students’ perceptions of their clinical learning environment.
Objectives
This study aimed to characterize and contrast how students in two Saudi Arabian dental institutes’ bachelor's degree programs perceive their clinical learning environment, to assess how the academic year influences the student behavior and perception as well as find out the strengths and weaknesses of each of the five domains of the questionnaire used in this study.
Methods
This was a cross-sectional survey study that was conducted from 15th October 2023 till 15th December 2023. Students from two Saudi Arabian colleges - College of Dentistry, Jouf University, and College of Dentistry, Qassim University who met the selection criteria were included in the study using the convenience-sampling method. A 38-item modified UCEEM questionnaire, piloted and tested for reliability and internal consistency, consists of 38 items congregated into five overarching dimensions and was mailed to the third-, fourth- and fifth-year UG students and interns of College of Dentistry, Jouf University, and Qassim University. The modified version was developed through quantitative data from various core groups, comprehensive dialogues with students, and the clinical committees of both colleges. Mann Whitney U and Kruskal-Wallis tests were performed.
Results
The survey achieved a response rate of 69.0%. Among the respondents, there were 85 (57.8%) males and 62 (42.2%) females, aged between 23 and 32 years. The mean total score for all students was 138.45. Notably, students from Qassim University gave significantly higher scores than the students of Jouf University (p = 0.01). Furthermore, students from Qassim University provided higher ratings for most of the overarching dimensions of experiential learning as compared to the students of Jouf University.
Conclusion
The significant differences between universities highlight the need for tailored interventions to improve the quality of clinical education, particularly in areas related to supervision and experiential learning. We recommend implementing continuing education programs for supervisors to enhance their pedagogical competencies in overseeing students’ clinical practice.
Introduction
Clinical environment refers to the surgical/medical workplace in which the professional student completes his/her clinical training in addition to their non-clinical curriculum. The clinical environment is vital as it enables the direct application of theoretical knowledge to practice, the development of clinical skills, and the establishment of problem-solving and clinical reasoning abilities. Clinical environment is generally governed via the interaction of various collaborator bodies and institutional architecture environment. 1 Students are among the principal stakeholder bodies in this environment and research has shown that the learning environment significantly influences their needs and adds to their learning, execution, and accomplishment.2–5
Maintaining an excellent learning environment requires constant monitoring and assessment. Since there has been a lot of diversity in the perception of the education environment by the students and faculty, the identification of educational elements or part of the educational variables is necessary. One such example is the changes in curriculum design over time intentionally or unintentionally that lead to changes in the educational environment. 6 Changes from traditional didactic design to student-centered problem-based learning curriculum create numerous educational environment changes. According to Ong et al., non-traditional classroom seating enhances learning effectiveness, adaptability, and creativity of students. They concluded that a positive course experience can motivate students while fostering creativity and improving learning outcomes. 7
Attainment of knowledge in a clinical setting is a complex phenomenon that requires a balance between healthcare delivery and academic learning. The student-supervisor relationship serves as the cornerstone of the clinical learning experience and is critical to achieving learning outcomes. 8 However, the limitation to clinical productivity is undermined by inadequate management support, supervisor time for clinical teaching and skills, preparation, feedback shortage from the students, and other factors, such as the number of students in each clinical setting and patient availability. The clinical environment is negatively impacted by a lack of treatment quality, patient concerns, and student's life conditions. Ahmad et al. conducted a study to assess the level of anxiety and identify anxiety-provoking factors among clinical dental students. They found that the primary factor causing clinical anxiety was the fear of failing the final examination. 9 Thus, the clinical learning environment needs maintenance and continuous assessment. 5
Research exploring the clinical learning environment has predominantly been carried out in various healthcare disciplines such as medicine, nursing, and physiotherapy.6,8 These studies often report positive perceptions rather than negative ones. 10 Brown et al. 11 and Irfan et al. 12 used the Dundee Ready Education Environment Measure (DREEM) questionnaire which is a universally accepted tool to assess knowledge about learning environment in medical institutes, although it does not specifically focus on the clinical learning environment.
Various tools have been introduced in the literature to gauge the condition of the learning environment. However, most of them are not designed for the initial purpose of measuring the quality of the clinical environment. 13 It also does not differentiate between undergraduate- and postgraduate students.14,15 The Undergraduate Clinical Education Environment Measure (UCEEM) tool was recently introduced to determine undergraduate medical and dental students’ perception of the quality of the clinical environment in clinics/hospitals. 16
Dentistry program is unique in a way that the students start their pre-clinical learning in second academic year and are promoted to clinical courses in a competency-based clinical environment in the third academic year of their study which is followed till the fifth academic year and internship year. In most of the clinical undergraduate dental programs, the clinical learning environment is of utmost importance.
Undergraduate dental degree program at Jouf University and Qassim University, Saudi Arabia is modular-based blended with both horizontal and vertical as well as spiral integration. Clinical learning starts from the third year with clinical courses in the dental clinics. 17 Dental students either perform a significant section of their clinical training within the same university campus clinics or at other hospitals under different supervisors, primary health care and private clinics. Thus, the conditions for the clinical experience are quite diverse for the students.
To date, limited studies have compared the clinical learning environments of two institutions within a cohort of healthcare professional students and examined their perceptions of these environments. Against this background, the current study was undertaken to describe and compare student beliefs of their clinical learning environment across two undergraduate programs and to assess how academic years influence the student's behavior and perception as well as to find out the strengths and weaknesses of each of the five domains of the questionnaire used in this study. This is particularly important as clinical training is a crucial component of professional health education.
Materials and methods
Study design
A cross-sectional survey study was designed and conducted in accordance with the guidelines for strengthening the reporting of observational studies in epidemiology (STROBE). Ethical approvals were obtained from the local committee of bioethics, Jouf University (2-04-44) and IRB Qassim University (22-05-01)
Study duration
15th October 2023 till 15th December 2023.
Inclusion and exclusion criteria
Third, fourth- and fifth-year dental students and interns were included in the dental program offered by Jouf University and Qassim University. The students who were unwilling to participate were excluded.
Participants’ selection and characteristics
Students from two Saudi Arabian colleges who met the selection criteria were included in the study using the convenience-sampling method. The dental undergraduate program at these institutes is 5 years with 1 year of compulsory internship. Annual admission in the first year per year varies between 20-40 students (male and female) in the College of Dentistry, Jouf University, and 12-18 (male only) students in the College of Dentistry, Qassim University.
Undergraduate program at both universities has 179 h of credit (3 semesters per year) including compulsory, elective, and free hours. The first two years mostly cover pre-clinical education (e.g., basic medical sciences, physiology, anatomy, biochemistry, and dental materials). The general structure of the study plan is 179 credits, and it is divided into four sections with 114 (63.7%) compulsory courses, 12 (6.7%) elective courses, and 6 (3.35%) free credit hours. The basic sciences and Islamic courses offered by the university consist of 12 (6.7%) credit hours. Clinical settings are included from the third academic year and followed till the fifth year with 5, 12, and 15 credit hours, respectively. In total, 33 weeks (about 7 and a half months) of clinical courses (excluding exam weeks) are merged into professionalism, continuous assessment, intervention, health care, and critical thinking, treatment planning, research, and scientific methods. The sixth year, i.e., the internship year is fully based on clinical/hospital settings of 5 days per week (17 credits).
Research tool and questions
UCEEM
This is an autogenous-driven, closed-ended analysis tool of subjects relevant to the clinical learning environment. This inventory is developed through quantitative data from various core groups, comprehensive dialogues with students and the clinical committee, and with the main stack holders. It serves as a practical, applicable, and comprehensive tool for assessing the clinical or hospital workplace as a learning environment for undergraduate medical and dental students. Additionally, it can function as an effective tool for benchmarking and evaluating clinical learning environments in various contexts. The original questionnaire includes 38 items, each scored on a five-point Likert scale ranging from 0 to 4. The scale is defined as follows: 0 = strongly disagree, 1 = disagree, 2 = neutral, 3 = agree, and 4 = strongly agree. 14 The questionnaire was modified after personal correspondence with the author to suit our environment.
The revised version consists of four overarching themes namely:
Preparedness for student entry (13 items; score range: 13–65) Opportunities for learning in and through work and quality of supervision (14 items; score range: 14–70) Workplace interaction patterns and student inclusion (9 items; score range: 9–45) Equal treatment (2 items; score range: 2–10)
For all themes and items, a higher score indicated a more positive response.
Other than these questions, background data (gender, ages and academic year) was also collected.
Procedure
Two senior faculty members with expertise in survey research performed the face and content validation of the questionnaire. To determine how well respondents could comprehend and reply to the offered questionnaire, pilot research was carried out with 10 randomly chosen participants from the study site. For this questionnaire, reliability analysis showed Cronbach's alpha coefficients ranging from 0.949 to 0.954 for various sections, which were considered relatively high and internally consistent. The students selected for pilot research were not included in the final sampling.
Third-, fourth-, and fifth-year undergraduate dental students and interns were the target population, and the participants were selected by convenience sampling. Students were invited to fill in the questionnaire in the first and second semesters due to varying degrees of clinical experience. Participants were sent an online questionnaire link of the study via university E-mail address of the principal investigator. Participants were asked to fill in the questionnaire for their existing academic year placing. In case of no response, three remembrances were sent via university E-mail between 5 to 10 weeks (about 2 and half months) following the first E-mail. Participants were assured that the survey results would be presented or published only in aggregate form, ensuring the confidentiality of their personal information.
Statistical analysis
Data was analyzed using the Statistical Package for the Social Sciences version 20.0 (IBM Corp, Armonk, NY, USA). Descriptive data analysis was done using frequency tables and number and percentage for each of the research instrument's items. They were also summarized as mean and standard deviation. Since the response to each item was measured on a 5-point Likert scale, the Mann-Whitney U test, a non-parametric test, was used for intergroup comparisons. The Kruskal-Wallis test was employed to compare UCEEM scores across different academic years. The level of statistical significance was set at p ≤ 0.05.
Results
Participants
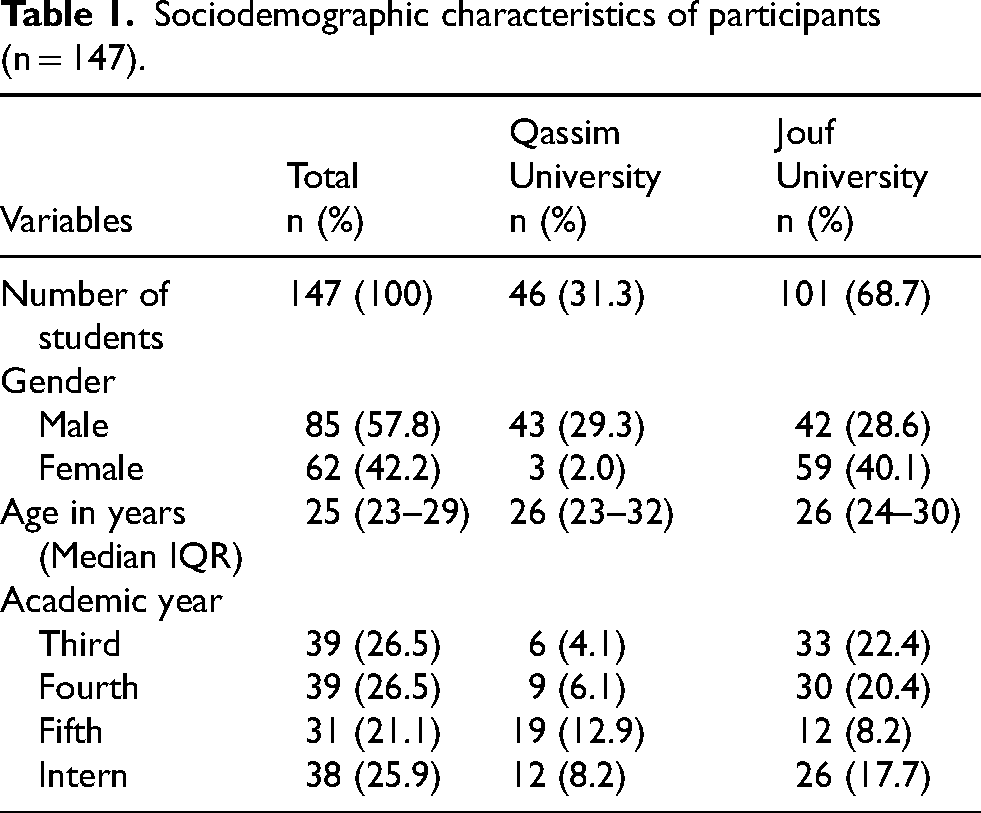
A total of 147 students (out of 213 students) responded to the survey, which corresponded to a response rate of 69.0%. The samples consisted of 85 (57.8%) males and 62 (42.2%) females in an age range between 23-32 years. There were 39 (26.5%) third year students, 39 (26.5%) fourth year students, 31 (21.1%) fifth year and 38 (25.9%) respondents were interns. Table 1 depicts the sociodemographic characteristics of all the participants.
Sociodemographic characteristics of participants (n = 147).
UCEEM scores
Mean total scores for all students was 138.45 (SD: 38.82; range: 109–168), with Qassim University giving the scores significantly higher than the students of Jouf University (p = 0.01).
The mean score for the overarching dimension of experiential learning, based on the subscales of opportunities to learn in and through work, quality of supervision, and preparedness for student entry, was 97.86 (SD: 28.38; range: 81–115). Qassim students provided significantly higher ratings for this dimension as compared to the students of the Jouf University. Qassim students rated two items significantly higher than the students of Jouf University did. One of the items belonged to the subscale “preparedness for student entry": “My supervisors are familiar with the learning objectives” (p = 0.01). Another item belonged to the subscale “opportunities to learn in and through work and quality of supervision": “I have the opportunity to put my theoretical knowledge into practice in this placement” (p = 0.03).
The mean score for the overarching dimension of social participation, based on the subscales of workplace interaction patterns, student inclusion, and equal treatment, was 40.59 (SD: 10.44; range: 41–46). Qassim students provided significantly higher ratings for this dimension than the students of Jouf University did (p = 0.01). Regarding an item, “As a student, I am received in a positive way by the staff here”, the students of Qassim University had provided significantly higher response than the students of Jouf University (p = 0.01).
A summarized form of the data on the total UCEEM, overarching dimension, the subscale scores are presented in Table 2.
Mean and standard deviation (SD) of UCEEM total scores, scales, and items for all students (n = 147).

* Statistically significant.
Comparison between academic years and UCEEM scores
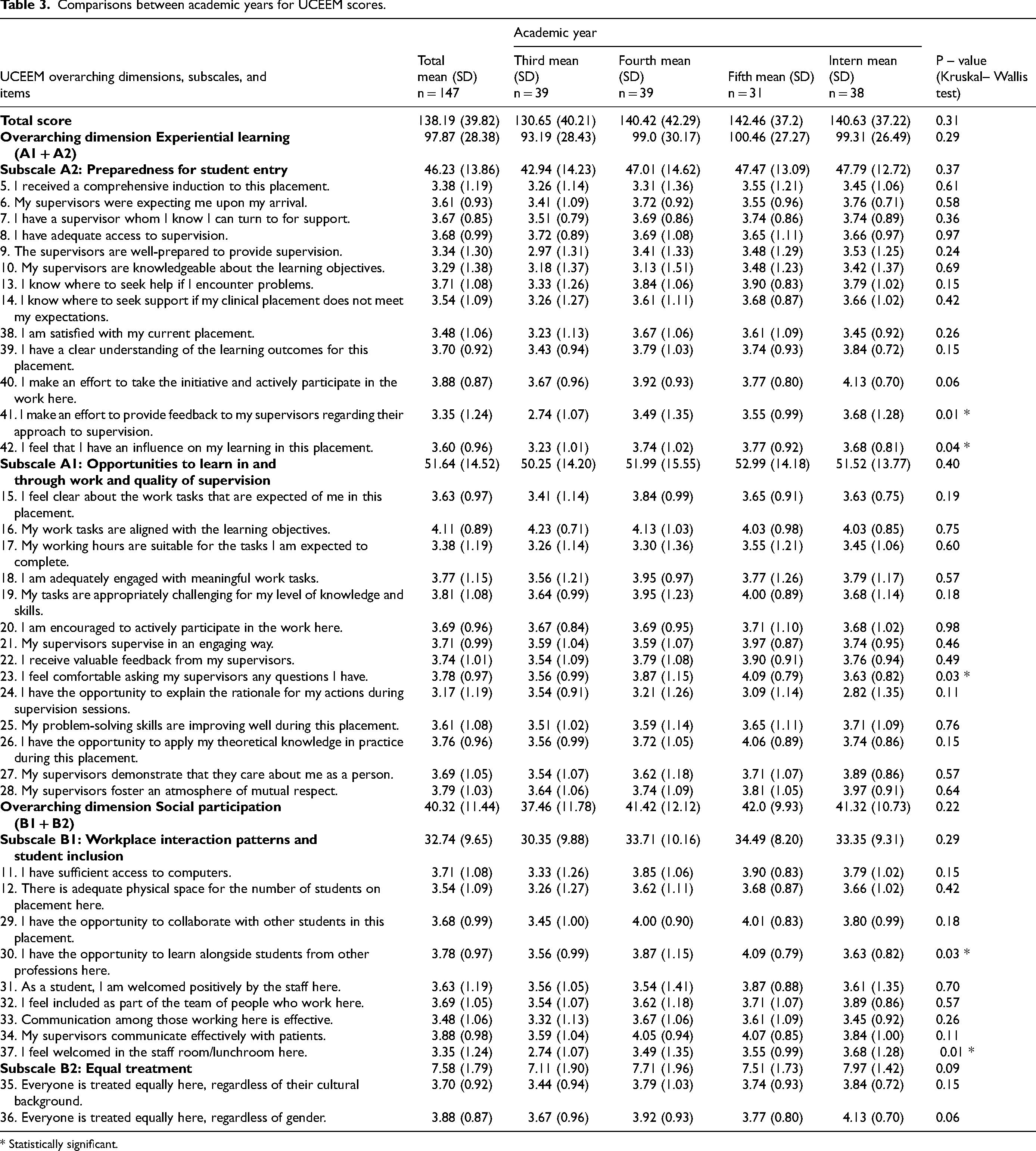
There were statistically significant differences between academic years within each program (Table 3). However, the mean score and standard deviation (138.19 ± 39.82) for the overarching dimension of experiential learning and its subscales showed minimal variation between the academic years.
Comparisons between academic years for UCEEM scores.
* Statistically significant.
In subscale A2, preparedness for student entry, the students at both colleges score significantly high rating to item no. 41 (“I try to give feedback to my supervisors about their way of supervising”) and item no. 42 (“I feel I have influence over my learning in this placement”) showed statistically significant differences, with p-values of 0.01 and 0.04, respectively. Similarly, within subscale A1, “opportunity to learn in and through work and quality of supervision,” students scored significantly higher (p = 0.03) for item no. 23 (“I feel able to ask my supervisors any question I wish”).
Discussion
This study aimed to assess the student's perception of their clinical education environment and professional development by using modified UCEEM online questionnaire. This is the first study to our knowledge that used UCEEM in dental settings in Saudi Arabia.
The primary reason for employing the UCEEM tool in this study was its strong psychometric properties across various contexts. 16 The total UCEEM scores and the scores of the overall arching dimensions were high showing the positive student perception across both institutes. In our study, only 2.5% of total UCEEM items score ≤3 which represent areas of improvement and around 10.5% of total UCEEM items score ≥4 representing strong areas indicated that overall, the general clinical learning environment perception was positive. Students from Qassim University showed significantly higher scores for their clinical learning environment compared to Jouf University. This finding is consistent with previous studies, such as those by Wilson et al., which emphasized that differences in institutional resources and faculty engagement can greatly affect students’ learning experiences. 18 The current study's emphasis on experiential learning reflects findings from Alrashidi et al., who argued that effective hands-on experiences enhance student preparedness and confidence in clinical settings. 19
This study was designed to evaluate the overall learning outcome and the individual overarching dimensions. At the item level, the students score the item ‘supervisory familiarity with the learning objectives’ significantly low with the mean score of 3.02 (1.33). This aligns with the work of Keshavarzi et al., who noted that clear communication of learning goals between supervisors and students is crucial for fostering an effective educational environment. 20 However, this contrasts with the studies conducted by Courtney-Pratt et al. 16 and Benamer et al., 21 which included more than 100 responses and found that familiarity with the learning objectives was higher compared to our study. It is likely that the clinical students in our study interact with a considerable number of supervisors during their clinical rotations. This may lead to differing opinions on clinical cases based on individual clinical experiences, potentially causing some confusion among students regarding the learning objectives. Supervision structure does not differ significantly between the settings within the institutes and between two colleges, which contrasts with suggestions published by the previous studies but is not the scope of this study. Nevertheless, it is essential that the learning outcomes guide the content of the curriculum. Supervisors’ familiarity with the course's learning goals will enable them to better identify students’ learning needs and ensure they receive relevant clinical exposure.
Clinical placements provide students with the opportunity to gain exposure to their future profession and learn through interdisciplinary clinical interactions. Our results for the overarching dimension of “social participation,” which includes the subscale of workplace interaction patterns and student inclusion, indicated that Jouf students scored this item relatively lower compared to Qassim students. Overall, the score was significantly lower, particularly in areas related to perceptions of staff reception and collaborative learning opportunities. These findings are in consistent with the research by Hays et al., which emphasized the importance of inclusivity in educational settings. 22 However, these results contrast the numbers shown by Strand et al. who found high scores for these subscales. 14 The current study's results indicate that fostering an environment where students feel welcomed and included is vital for their overall satisfaction and engagement, reflecting the broader literature on the impact of social dynamics on learning.
The role of clinical supervisors in training students is pivotal, particularly regarding their familiarity with the learning outcomes of the course. 17 Research indicates that supervisors’ understanding of these objectives is essential for effective student training. 21 In our study, the subscale of the UCEEM titled “My supervisors are familiar with the learning objectives” received notably low scores. In contrast, the score reflecting student interaction with supervisors was significantly higher, suggesting that while students may engage actively with their supervisors, they feel that these supervisors lack familiarity with the course's specific learning goals. This finding is in contrast from the work of Benamer et al., which reported reduced UCEEM scores in various areas such as workforce equity of treatment, workplace interactions, student inclusivity, and student entry preparation. Their study employed a comparative design between public and private institutions, highlighting contextual factors that may influence the perceived effectiveness of clinical supervision. 21 This contrast emphasizes the need for further investigation into how supervisor familiarity with learning outcomes affects student experiences across different educational settings. The disparity in findings underscores the complexity of the supervisory relationship and its impact on training efficacy. Recognizing these complexities is crucial for developing strategies that enhance the training process and ensure that supervisors are adequately prepared to meet educational objectives.
The academic-year distribution revealed that third-year students scored significantly lower on the item “I feel able to ask my supervisors any question I wish” compared to other students. This disparity is likely attributable to their recent introduction to clinical placements, where they are still familiarizing to competency-based practices and getting to know their clinical supervisors. Additionally, the presence of different supervisors for various specialties may contribute to the lower scores, as students require time to familiarize themselves with each supervisor's approach and expectations. 23
In summary, the findings of this study indicated generally positive feedback while highlighting specific areas for improvement, particularly in supervisor familiarity with learning objectives and fostering social inclusivity.
Limitations
When evaluating the findings, certain study limitations should be considered. The study may contain some elements of under-reporting bias, as with any questionnaire-based survey. Limitations may also include the cross-sectional design, non-respondent bias, and respondents’ tendency to select socially acceptable answers, as seen in questionnaire surveys. Interns are posted based on a rotation basis of four-month duration in different clinical setups (Hospital or Primary health care centers), thus they do not have identical clinical experience. Furthermore, interns were investigated about their clinical experience indiscriminately, so different variations in the clinical environment cannot be evaluated.
We therefore recommend conducting multi-center studies that can provide data on the dental specialization and career options from the graduates of different dental colleges in Saudi Arabia.
Conclusion and recommendations
The significant differences between universities highlight the need for tailored interventions to improve the quality of clinical education, particularly in areas related to supervision and experiential learning. We recommend the implementation of continuing education programs for supervisors to enhance their pedagogical competencies in supervising students’ clinical practice. To assess the clinical learning experience of the student participants, effective interventions are required. Additional research is required to assess the effectiveness of any given intervention.
Footnotes
Acknowledgements
We thank Deanship of Graduate Studies and Scientific Research, Jouf University for funding this research.
Ethical approval
Ethical approvals were obtained from the local committee of bioethics, Jouf University (2-04-44) and IRB Qassim University (22-05-01).
Informed consent
Participants provided written informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Deanship of Graduate Studies and Scientific Research at Jouf University under grant no. (DGSSR-2023-01-02163).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The dataset used in the current study will be made available on request from Prof. Dr Mohammed Ghazi Sghaireen, msghaireen@ju.edu.sa.