
Abstract
Background
Work, a social determinant of health (SDOH) can both affect and be affected by health.
Objective
To examine literature related to work as a SDOH on cardiovascular and musculoskeletal disease among U.S. workers.
Methods
A literature review was conducted. All studies investigating work-related SDOH on the following cardiovascular (stroke, hypertension) and musculoskeletal disease (arm and leg limbs, pain). Epigenetic influences were also evaluated, as it relates to these diseases.
Results
The core concept of “work” as a SDOH on cardiovascular and musculoskeletal disease has yielded the “bio-ecological work” model, comprised of four main levels of influence: Work Environment, Interpersonal, Psychological, and Intrapersonal. The Work Environmental dimension includes: The health effects of unemployment and job insecurity, the impact of shift work schedules on health, balance between work effort and reward, the psychosocial work environment, the influence of control at work, demands, and decision latitude on worker's health, the link between health and the physical risks and hazards of work. The Interpersonal level consists of: The health implications of balancing work and family responsibilities and social support at work. The Psychological dimension includes perceived discrimination in the workplace and acute work-related stress and chronic disease. And the Intrapersonal level consists of workplace exposures on epigenetics, telomere length, and microRNA molecules.
Conclusion
This work is important to inspire capacity building and research in occupational health, to prevent cardiovascular and musculoskeletal disorders in order to preserve a productive life for the ageing population.
Keywords
Objectives
Examine the literature related to work as a Social Determinants of Health (SDOH) on cardiovascular and musculoskeletal disorders and outcomes among U.S. workers.
Identify the need for future studies related to work as a SDOH on health outcomes.
Introduction
There are critical changes in work and in the U.S. workforce, which have pervasive implications for future health. Work, as a social determinant of health (SDOH), can both affect and be affected by both cardiovascular and musculoskeletal diseases. Additionally, work can result in more rapid onset and progression of both diseases.
Particularly when it comes to cardiovascular and musculoskeletal diseases, work can result in more rapid onset and progression of both diseases. For example, there are well documented causes of cardiovascular disease, which can also lead to unhealthy coping mechanisms. Work outside of traditional daytime hours have been associated with cardiovascular disease (CVD), like high blood pressure and stroke.1–4 Exposure through work with furnaces, boilers, vehicle exhaust, or in areas with poor air circulation can reduce the amount of oxygen carried by blood, damaging the heart.1–4 Research has shown that exposure to high effort and low reward employment associated with double the risk of newly reported coronary heart disease over 5.3 years. 2 Additionally, jobs that require workers to maintain a high level of vigilance to prevent major incidents/accidents present a greater psychological burden. 2
There is also evidence that work can cause premature musculoskeletal disorders. Work-related musculoskeletal disorders are the most widespread occupational health hazard facing the U.S. today. Nearly two million workers suffer work-related musculoskeletal disorders every year, and about 600,000 lose time from work as a result 5 Over the 2021–2022 period, there were 502,380 workplace musculoskeletal disorders that resulted in at least one day away from work. These cases occurred at an annual incidence rate of 25.3 musculoskeletal disorders per 10,000 FTE workers. 6 It is reported that musculoskeletal disorders cost an estimated $213 billion in annual treatment, care and lost wages. 7
The current economic downturn resulting from the COVID-19 pandemic is changing the profile of workers and the nature and structure of work in the United States. This is evidenced in several studies which evaluate the impacts of COVID-19, specifically telework in various work domains on musculoskeletal disease.8–10 Telework or working remotely from home, through making use of the internet, e-mail, and the telephone has numerous advantages, but also has many post-pandemic negative impacts on workers’ health and safety. Telework is a major contributor to the development or aggravation of work-related musculoskeletal disorders where unsuited workstation ergonomics (i.e., working with inadequately placed screens and laptops and sitting in maladjusted seats without usual functionalities and ergonomic support), sedentary behavior and prolonged sitting in non-neutral positions, as well as psychosocial and organizational factors (i.e., extended working hours with fewer rest periods to meet increased work demands; social isolation; lack of support from work colleagues and superiors; blurred work-home boundaries and omnipresence of work; environmental factors such as poor lighting and glare, inadequate room temperature, and ventilation or noise) play a role.8,9 During the pandemic, white-collar and salaried telecommuters were more likely to experience health problems (i.e., anxiety, fatigue, musculoskeletal pain, and headache/eye strain) than daily commuters. And this association varied by gender, with female teleworkers experiencing a greater likelihood of depression and insomnia. 10
Today's workforce is older, more racially and ethnically diverse, and increasingly made up of women. 11 Additionally, the pandemic is disproportionately hurting employment sectors, with ramifications that could be long-lasting. The COVID-19 pandemic has exposed the link between socio-economic inequalities and health outcomes, especially in the area of musculoskeletal diseases 12 and cardiovascular health.13,14
Epigenetic differences resulting from socio-economic inequalities potentially modify cardiovascular and musculoskeletal disorders among other health outcomes. Epigenetics is the modification of DNA without changes in sequence. This can be covalent changes directly to the DNA molecule, such as methylation. Cytosine methylation is well-characterized at cytosine-guanine rich regions, called CpG islands, found primarily in the promoter regions of genes. Cytosine methylation influences gene expression by impeding the RNA polymerase machinery from transcribing the DNA following methylated promoters. DNA methylation on a global scale, and more so in specific regions, has been characterized as indicative of so-called “biological age”. Methylation changes are seen to occur and accumulate over time, and measurements of methylation changes serve as a molecular clock of ageing. Much previous work on biological ageing has focused rather on telomere length. Telomeres serve to protect the ends of linear chromosomes and are eroded over a lifetime of DNA replications. The other primary epigenetic modification occurs within the chromatin, rather than directly on the DNA molecule. DNA is wrapped around histone octamers, allowing its compaction. Because the histone complexes can be moved on DNA molecules, this creates differential compaction of the DNA, physically creating or limiting access to regions of DNA, and thereby modifying gene expression. Histones are acetylated on lysine resides within their “tail” domains, and this acetylation generally opens the chromatin structure, increasing transcription of genes within that region of DNA.
Psychosocial aspects of work can affect health; specifically, the experience of work itself—the social and psychological aspects of working conditions—affect physical health. And for many Americans, work is a major source of opportunity for personal development and building economic stability in their lives. These opportunities are shaped by many characteristics, including job security, scheduling, family responsibilities, the balance of work efforts and rewards, the work environment, control, support, perceived discrimination, physical risks, and acute stress, in making decisions about one's work. For example, occupational segregation accounts for disproportionate mortality rates for Latino/Hispanic and African American/Black workers during the COVID-19 pandemic. Along with this growing demographic diversity, the “twenty-first century workplace” features more multidisciplinary jobs, more collaborative work and reliance on technology, and a shift away from manufacturing jobs. 15 As companies have restructured “knowledge work”—requiring a relatively high level of education or technical training—and service jobs, which have become more predominant.15,16
The Bureau of Labor Statistics projects that the United States workforce will increase by 8.3 million jobs from 2021–2031, in which nearly one-third of new jobs are projected in healthcare and social assistance. 17 Today's workers face greater job uncertainty; they are more likely to have many employers and to be required to enhance or expand their skills over the course of their working careers. These shifts in work may have outpaced knowledge about their implications for the quality of working life and for safety and health on the job. 16 For example, Latinos are disproportionately employed in precarious work conditions that can trigger hypertension risk, which may contribute to cardiovascular disease risk among Latinos. 18 Public health initiatives should promote behavioral interventions in these work settings. 18 Measures to protect workers from physically hazardous conditions remain important, but the current context calls for new integrated strategies that not only will protect workers from major hazards but will promote healthier work and workplaces. To fill this need to better understand health outcomes related to work as a SDOH within the current day context in which we currently live, the aim of this study is to examine the literature related to work as a SDOH on cardiovascular disease and musculoskeletal disease among U.S. workers, and related epigenetic influences that we should begin to look more closely at. This review is important to help inspire capacity building and research in occupational health, to prevent ill-health and to preserve a productive life for the ageing work population. 19
Methods
This study, as a literature review, is exempt from Institutional Review Board approval. The review search included clinical trials, meta-analyses, systematic reviews, reviews, and randomized controlled trials. All searches were limited to English language, humans, and adults 19 + years.
Articles were initially determined to be relevant if they: (1) were a review article; (2) attempted to include occupations and skill work levels represented in sample; and (3) ONLY included the following health domains:
Stroke or hypertension or cardiovascular Musculoskeletal pain (including nonspecific) or musculoskeletal disorder Epigenetics including DNA methylation and telomere length (each of which relate to biological ageing), and the expression of microRNAs
For review, PubMed was searched. A health sciences librarian created the search using a combination of keywords and controlled vocabulary which were generated from the Yale Mesh Analyzer (https://mesh.med.yale.edu/) and WordFreq (https://sr-accelerator.com/#/wordfreq). Keyword alternatives and variations were developed from the terms: psychosocial job stress, occupational health, anxiety, musculoskeletal pain, hypertension, stroke, epigenetics, ageing and employment levels.
This search attempted to capture papers related to studying epigenetics within the context of occupation, without capturing papers relating to, for example, the occupation of promoters by transcription factors. This was additionally filtered to remove duplicates and to include only studies in three broad areas: occupational impact on telomere length, occupational impact on DNA methylation (globally and in specific genes), and occupational impact on microRNA expression.
Results
The core concept of “Work” as a social determinant of health on cardiovascular and musculoskeletal disease, mirrors Bronfenbrenner's Ecological Model (1979),
20
in which multiple levels of influence interact with one another and influence negative health outcomes and disparities. According to the literature, we find four main levels of influence, from the wider exo-system drilling down to the micro-system:
Work Environment (shift work; control at work, demands, & decision latitude; work effort & reward; unemployment & job insecurity; work-related stress) Interpersonal (social, work/family) Psychological (perceived discrimination, stress) Intrapersonal (biological, epigenetics)
This “bio-ecological work” model (Figure 1.) is based on the idea that relationships which individuals have with their family, friends, coworkers and/or supervisors, and work environment impacts their health outcomes—and that these relationships are affected by their work environment, which are in turn affected by broader social, cultural, and political conditions.
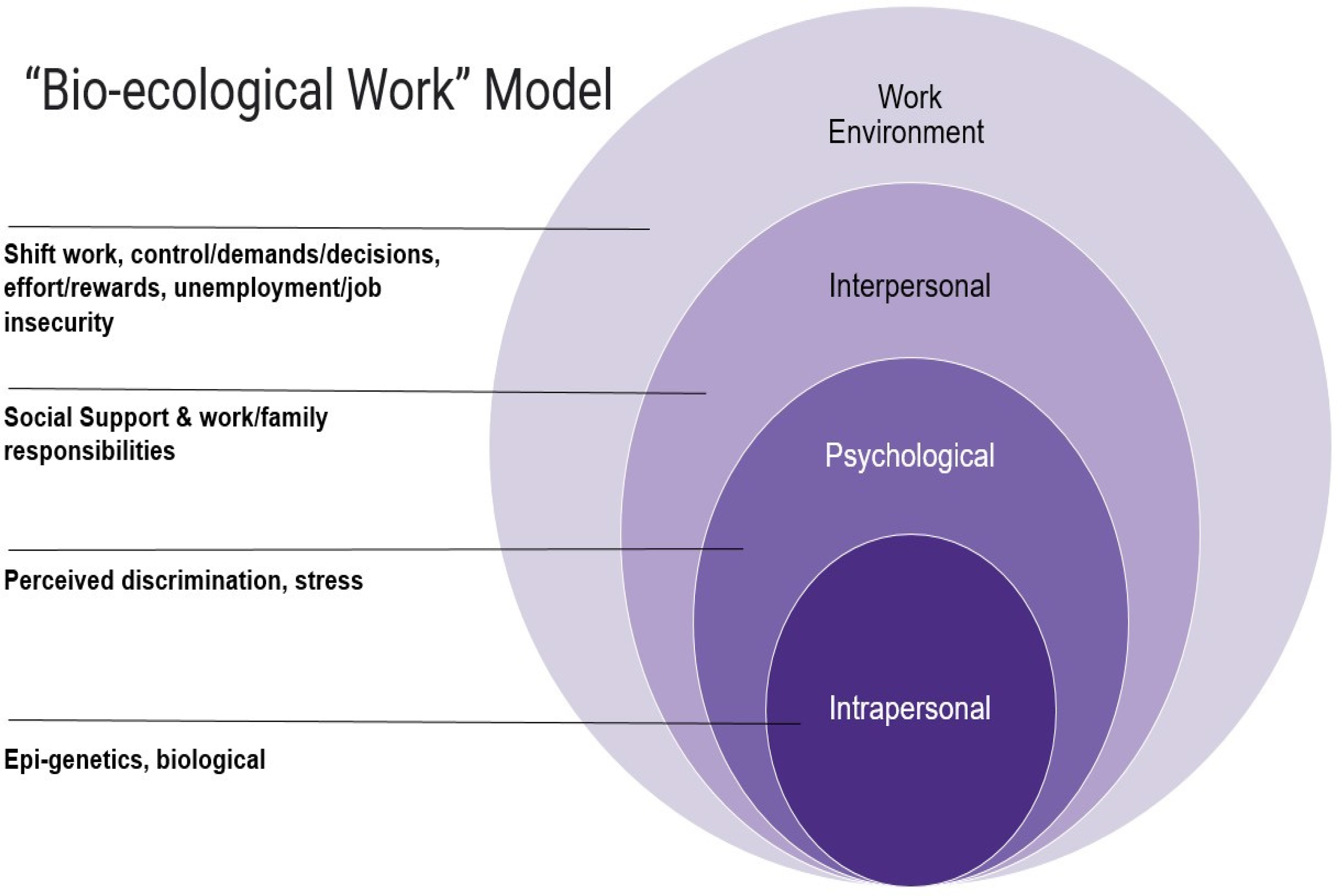
“Bio-ecological work” model.
Work environment level
The health effects of unemployment and job insecurity
A bad or negative work environment can contribute to the risk of CVD including stroke, which is associated with an increased prevalence (OR = 1.29, p < 0.01). 21 Although somewhat sparse, the majority of research studies on job insecurity and unemployment has been restricted to industrialized societies, like the U.S.22,23 Additionally, the specifications on the frequency and length of job insecurity and unemployment are lacking, which make it challenging to fully understand the impact on health. 22 While poor health in and of itself can be a cause of unemployment, studies also show that unemployment appears to be an independent factor of preexisting health effects. 24 Unemployment brings lower income and living standards, which consequently can cause deteriorating physical health because of changes in the ability to afford nutritious food, healthy housing, and/or sufficient medical care. This was particularly evident during the COVID-19 pandemic, when in October 2021, nearly 20 million adults lived in households that did not get enough to eat, 12 million adult renters were behind on rent, expired unemployment benefits, and supply chain problems that contributed to rising prices on common goods. 25
What we do know is that unemployed individuals have a higher prevalence of poor health and excess mortality than their employed counterparts.22,23,26 Unemployment is associated with health issues such as cardiovascular risk factors, being overweight, and having diabetes 27 and it can limit access to health-promoting aspects of work. In addition, those who are already at greater disadvantage with respect to social factors like educational attainment and racial or ethnic group are at greater risk of being unemployed. 24
For those who are employed, job insecurity or even the threat of job loss can contribute to poorer health. 24 Job insecurity has been shown to be associated with elevated risks of hypertension and cardiovascular disease”.28,29 Specifically, job insecurity is significantly associated with elevated hypertension among those employed in healthcare support occupations 30 and public administration industries. 31 The stress associated with the prospect of losing one's job can also lead to risky coping behaviors such as smoking, lack of exercise and forgoing sick or vacation leave, and may place workers at increased risk of work-related injury and illness. 32 In a study of hotel housekeepers, agency-hired workers typically received no benefits, are paid less, and experienced job insecurity, thus having more difficulties in maintaining routine medical visits and purchasing prescription medications. 33 In situations of economic and sociopolitical instability, single women are the most vulnerable, often having little to fall back on in the face of illness, job loss, and increased family care and domestic burdens. 34
The impact of shift work schedules on health
Shift work is typically characterized by employes working outside standard (9:00am to 5:00pm) hours. Because shift work includes night work, the normal sleep—wake cycle circadian rhythm is disrupted, with potential consequences for shift workers’ physical health. 29 Evening and overnight shifts, holding multiple jobs, long work hours and excessive overtime work can be detrimental to health by causing increased fatigue, sleep loss or lower sleep quality, decreased work performance, occupational stress, and disturbances in circadian rhythms.24,35–39 Workers with physically-demanding jobs—including long hours, strenuous occupational physical activity, and irregular working hours—are more likely to experience a stroke, hypertension, or other cardiovascular diseases compared to other workers.29,35–41
The research on working hours and health appears to be evident. Specifically, there is a significant association between stroke and exposure to long working hours for 10 years or more, 41 and regular (non-shift) employment before stroke onset appears to have a positive impact on outcome. 42 It has been shown that longer working hours and an extended duration of strenuous activity during work is associated with increased rates of hemorrhagic stroke.32,41 This issue becomes even more urgent during and after the COVID-19 pandemic, as individuals are working more from home, with the risk of working longer hours and becoming physically inactive. 42 Health promotions advocate for consistent physical activities, breaking up sedentary time and maintaining social relationships, beneficial to public mental health. 42
We also see gender and other demographic differences in health, as it relates to shiftwork. In men, systolic blood pressure was higher in shift workers compared to daytime workers; and in women, weight, body mass index, and the prevalence rate of hypertension in the past medical history were higher in shift workers compared to daytime workers. 36 And for both men and women, rotating shift workers spent less time sleeping both on working days and on non-working days, spent less time with sport activity, drank more coffee and they spent less time working per day, especially in light physical work, compared to daytime workers. 36 In addition, low and middle educational levels were most frequently found among rotating shift workers as opposed to daytime workers where high educational level was more common. 36
The balance between work effort and reward
Perceived balance between a worker's efforts and rewards (in terms of earnings, benefits, esteem, job security and career opportunities) has been shown to influence health outcomes. 24 Effort reward imbalance exposure and high efforts at work has been associated with heart disease 37 and masked hypertension, 43 and for women, effort reward imbalance was associated with higher increases in systolic ABP. 44 Interestingly, all three measures of effort and reward imbalance, job strain, and conflict at work, were more frequently reported among stroke cases. 45 However, the mechanisms by which this imbalance differs, might be due to gender or other demographic factors (i.e., socioeconomic, racial/ethnic factors, etc.) which should be further examined.
The psychosocial work environment
Evidence shows associations between work environment, physical indicators and mental health outcomes. 46 Despite the influence of the work environment, there are still limited studies exploring the work environment comprehensively. Research shows that the work environment can be a risk factor for the development of moderate to severe clinical conditions, predicting absenteeism or intention of leaving the job. 47 Specifically it has been shown that a poor work environment and cardiovascular disease risk factors (obesity or sleep complaints) occur not only when workers are exposed to poor working conditions, but also after retirement. 46
Literature on the psychosocial work environment is still a matter of debate. In particular, the involvement of the main behavioral and clinical risk factors and their relationships with working conditions are not always clear, despite an abundant body of literature. 46 Most studies have investigated the impact of a limited number of characteristics of the work environment on the occurrence of one or a few risk factors, dismissing potential mediating factors. 46 Some of these psychosocial work environment investigations have targeted specific populations, such as nurses, 48 and home care workers, 49 but studies with more robust designs are needed. 47 Nevertheless, more research into the psychosocial work environment is needed to improve the health of working populations. 50
The influence of control at work, demands, and decision latitude on worker's health
Job control, the combination of skill discretion and decision authority, is considered a central component of the psychosocial working environment. 51 Differences in the degree of control that workers feel they have over their working conditions are thought to be a major factor accounting for steep social gradients in health. 24 Jobs characterized by both high psychological demands and high levels of decision-making authority and skill utilization (“decision latitude”) can promote self-esteem and self-efficacy; yet workers whose jobs have high demands offer little decision latitude (what has been called “job strain”), are at higher risk of chronic physical and mental illnesses (such as cardiovascular disease, stroke, hypertension and musculoskeletal pain).24,52
Employes who feel their job gives them little job control yet have high demands have been found to have increased risks and worsened outcomes relating to cardiovascular disease, hypertension, and cerebrovascular disease.28,37,45,53 The same is true of workers who feel that the benefits of their work do not align with their efforts.25,26,34,54,55 Men appear to be more impacted by these psychosocial exposures than women, 53 though women represent an understudied population. 56 Research is needed to determine the impact of the timeframe of these exposures on cardiovascular and cerebrovascular events.
Literature provides evidence of gender and/or age differences in such outcomes. For example, low job control was associated with an increased risk of hypertension among men, but not among women. 53 But low job control was associated with upper-limb pain among women, while high psychological demand was associated with upper-limb pain only among men. 57 The prevalence of upper-limb pain was higher among those women who performed passive work (low demand, low control), active work (high demand, high control), and tasks under high strain (high demand, low control). 57 For women, there appeared to be a relationship between both lower back pain and neck-shoulder pain with job control, revealing that higher levels of job control were related to lower levels of both low back pain and neck-shoulder pain.11,52 Research also found that high emotional demand led to excess risk of workplace injuries, with this risk highest for workers under the age of 30, for males declaring a fear for their own safety or for the safety of colleagues and females who work in an atmosphere of tension with the public, or who have to hide or fake emotions. 12
The link between health and the physical risks and hazards of work
There is widespread awareness that both physical tasks involved in a job and the physical work environment can have important health effects, which has been the traditional focus of occupational health and safety research. Physical factors are social determinants of workplace injury, with the higher the reported exposure to physical risk factors, the higher the risk of workplace injury. 12 There are also other hazardous exposures in the workplace: inadequate ventilation or temperature control which exacerbate allergies or asthma, lead, pesticides, aerosols, ammonia, asbestos, and other cleaning products and workplace-related chemicals which can create long-term exposure can poison and cause serious illness. 58 Park et al. (2019) reported more exposure to physical/chemical and ergonomic hazards and musculoskeletal pain for those in nonstandard employment. 59 Workers with physically-demanding jobs—including long hours, strenuous occupational physical activity, and irregular working hours—are more likely to experience a stroke, hypertension, or other cardiovascular diseases compared to other workers.28,35–40 Individual demographic and work characteristics (i.e., age, gender, type of work, skill level, exposures at work) are important factors related to health outcomes. For example, a higher level of physical exertion is a risk factor among older female eldercare workers, but a moderate level of emotional demands is associated with lower risk among younger workers. 60 Work that is physically demanding and poor workplace conditions are associated with a higher prevalence of pain among both women and men. 57 Additionally, employes with musculoskeletal pain had 4 times higher risk of disability pension compared to those without musculoskeletal pain. 61 However, limited longitudinal studies have identified relevant hazard and risk factors for musculoskeletal pain. 62 To ensure the development of a more nuanced approach to hazard reduction and improved sustainable employment for workers requires a greater understanding of the relationship between work characteristics and musculoskeletal pain. 62
Workers in particular areas of the workforce are at increased risk of work-related injuries and illness: air transportation, nursing, 63 work with motorized vehicles and equipment, trucking services, hospitals, grocery and department stores, and food services account for nearly 30 percent of nonfatal occupational injuries. 64 Physically demanding daily tasks and uncomfortable working positions can lead to physical strain and injury, increasing the risk of long-term absence, mostly due to musculoskeletal pain; and sedentary jobs allow little opportunity for movement and contribute to risk of obesity and chronic diseases like diabetes and heart disease. 64 For example, among standard and nonstandard workers overall, unskilled manual workers were more likely to be elderly, less educated, have a low income, work fewer weekly hours, and have a shorter work duration, service. 65 Sales workers were more likely to be younger, have a shorter work duration, and work in smaller workplaces; and clerks were more likely to be younger and more educated; and managers and professionals were more likely to be more educated. Manual workers were more likely to report exposures to all physical/chemical and ergonomic hazards, and musculoskeletal pain than non-manual workers and have a higher income. 66 Blue-collar workers are more at risk (than white-collar workers), with a significantly higher prevalence of musculoskeletal symptoms 67 and an increased risk of hemorrhagic stroke. 35
Need for future studies
Our analyses reveal the need for prospective/longitudinal design and modeling for predicting workplace injuries so that preventative measures can be preemptively applied to minimize combinations of psychosocial and physical risk factors. For example, objectively quantifying the early signs of pain can have a major impact on functional abilities. Having tools for early detection of musculoskeletal disease pain and functional impairment will allow delivery of preventative approaches at a pre-clinical stage. Wearable sensor technology coupled with custom software and biomarkers of ageing can objectively quantify early signs of pain associated with detrimental impact of functional abilities. Having such tools of early detection of musculoskeletal disease pain and functional impairment will allow delivery of preventative approaches at pre-clinical stage.
Interpersonal level
The physical health and mental health implications of balancing work and family responsibilities
Given the persistent gender imbalance in family care responsibilities among women, 68 and that women are more adversely affected by rheumatic and musculoskeletal diseases compared to men,57,68,69 makes gender in musculoskeletal health a priority area of future research. Within a study group of women, there was a higher prevalence of pain among those exposed to a high domestic workload. 57 For women, supervisor support is protective against lower back pain, but only when work-family conflict is low; whereas for men, experiencing moderately high levels of work-family conflict amplified the negative effects of physically demanding work on lower back pain. 52
The impact of the pandemic continues to affect many workers, with greater concern for safety at work around the COVID-19 infection and related organizational changes affecting their jobs. 70 The literature highlights the nexus of health and gender inequalities associated with the COVID-19 pandemic and the adverse impact on women's health in balancing work and family responsibilities. Women performing work from home and family responsibilities during the lock down seemed to be going through increased physical and mental load. 68 However, social support at work has protective effects on health and has been linked to reduced risk of illness-related absence.71,72 Work environments that facilitate mutual support between coworkers can reduce job stress and provide a buffer against physical stressors related to work. 24 Support from supervisors has additionally been shown to help workers manage their hypertension. 33 Having a good physical work environment and good relationships with management were associated with self-reported musculoskeletal pain in fewer body regions.62,69 If we look at support over time, high work social support in midlife decreased the risk of health-related exit and unemployment. 73 Thus, social support in the workplace can promote health among workers. 74
Need for future studies
While the work-family conflict and health literature are expanding, it is still heavily reliant on cross-sectional research designs particularly among women. 75 A limitation of this area of literature is the lack of a standard definition of “responsibilities.” A more standardized definition of “responsibilities” could include more comprehensive measures with questions about tasks outside the house (for example, grass mowing and snow clearing), taking care of a person with a loss of autonomy, family budget, car maintenance, and playtime with children. 75 Future research should explore the longitudinal health effects on working women.
Despite promising evidence for social support at work, more analysis is needed to fully understand the effects. The benefit of social support may not provide equal benefit, and some groups may even struggle due to the intensity of their social connections and perception of inclusion at work. Further studies are needed to focus on uncovering which function(s) or mechanism(s) of social support are actually beneficial among hard-to-reach and precarious workers who are dealing with enormous life challenges. 76
Psychological level
Perceived discrimination in the workplace
Perceived discrimination refers to an individual's perception of negative attitude, judgment, or unfair treatment due to specific characteristics such as gender, race, ethnicity, and social status. 77 Despite the intent of the victim, the perception of discrimination still causes stress and deleterious behaviors for an individual. Short- and long-term health outcomes stemming from workplace discrimination are similar to those originating from non-work discrimination.14,78–80 Mounting evidence has demonstrated a role of psychosocial stressors such as discrimination in hypertension and cardiovascular disease. 81 The negative impacts of discrimination in the workplace can be both short-term (increasing stress levels, blood pressure and other physiological symptoms) and long-term (leading to musculoskeletal problems, arthritis, heart disease and other physical illnesses). 79 Recent research indicates a potential association between workplace violence (Workplace violence was determined based on self-reported threats, bullying, or harassment at work over the past 12 months, supplemented with additional information regarding frequency) and an increased risk of CVD, which included all forms of heart disease and stroke in the working-age population. 82 Workplace discrimination in particular is also associated with lower overall health and more chronic illness. 79 However, individuals with high perceived control were less negatively affected by workplace discrimination when reporting on their overall health. 79 Although racial composition of workplace may be a mechanism by which high SES increases discriminatory experiences for African Americans, males and females may not differ in this regard.17,19
Acute work-related stress and chronic disease
A working environment can damage health not only through obvious physical hazards, but also through stress. The last couple of decades have seen marked increases in scientific knowledge about causal pathways and physiological mechanisms that help explain the links between social and economic factors and health. 24 Examples include physiologic damage to multiple vital organ systems caused by chronic stress through neuroendocrine and immune pathways.83–86 Stressful experiences, including aspects of the work environment and working conditions, can trigger the release of hormones and other substances in the body which, particularly with stressors over time, can damage immune defenses and vital organs.87,88 This physiologic chain of events can result in more rapid onset and progression of chronic illnesses including cardiovascular disease; the bodily wear and tear associated with chronic stress may accelerate ageing.87,89,90 In addition, work stressors can cause depression and other mental health episodes, 91 and strain from trying to cope with daily events may over time, lead to far more physiological damage than a single stressful event, even if the event is dramatic. Daily hassles can include constant challenges posed by work environments in which a person may feel disrespected, experience microaggressions at work, 92 and feel intimidated or under constant strain trying to balance the demands of work and family responsibilities with inadequate resources and support.
Need for future studies
There is a well-documented association between experienced discrimination and negative psychological symptoms.11,12 However, research has yet to examine whether there is an interaction between race/ethnicity and how the experience of racial discrimination in the workplace moderates an association between discrimination experiences and depression or other negative emotions due to treatment based on race. 14 As such, more research is needed which addresses these issues of equity and inclusion in the workplace. Additionally, it is recommended that research be carried out at short time intervals in order to catch all new cases of depressive and other mental health episodes, and that the study designs clearly accommodate the need to distinguish first-onset from recurrent depressive episodes. 91
Intrapersonal level
Workplace exposures on epigenetics
Health lies at the intersection of the environment and the individual. The genetic makeup of the individual has long been understood to impact health, with numerous polymorphisms contributing, usually each in small ways, to how a person responds to environmental stimuli. More recently, we have come to understand that the converse is also true, in that the environment can shape the epigenome, which in turn influences gene expression in response to the environment. Epigenetic modifications of the DNA, such as opening or closing of chromatin structures mediated by histone modification, and the direct modification of the DNA itself by methylation. DNA methylation, often at C-G rich areas known as CpG islands in the promoters of genes, contributes to gene regulation.
Occupation has been shown many times to influence DNA methylation, both at specific sites and in a more gross manner. Occupational exposures that impact DNA methylation include benzene,93–95 nanoparticles, 96 radiation,97–99 pesticides,100–104 chromate,105–107 nickel,108,109 lead, 110 mercury, 111 per- and polyfluoroalkyl substances, 112 and welding fumes. 113 Even exposures such as noise have been linked to changes in DNA methylation patterns. 114 Exposure to these various insults varies in ways besides occupation, such as with neighborhood and socioeconomic status.114,115 Epigenetic modification of DNA is one of the proposed “hallmarks of environmental insults”. 116 DNA modification, in turn, impacts cardiac health 117 as well as mental health. Differential methylation has been described in depression, 118 stress resilience, 119 and “burnout”. 120 Recently, a comprehensive study looked at the effects of socioeconomic factors on biological ageing as measured by eight different molecular clocks based on patterns of DNA methylation. 121 Biological ageing, as measured by DNA methylation, was only partially explained by smoking, alcohol consumption, and obesity, leaving the socioeconomic status index as a significant influence on ageing.
Epigenetic modification potentially impacts cardiovascular health. Biological age, as determined by DNA methylation-based clocks, is correlated with cardiovascular disease incidence. Using a DNA methylation-based clock, every one-year increase in biological age was found to increase the risk of cardiovascular disease by 4%. 122 Furthermore, studies have shown differential DNA methylation in atherosclerosis. 123 Recently, a study utilizing an NHANES cohort and a DNA methylation-based method showed better performance as a measure of CVD risk than a PCR-based measure of telomere length. 124 As methylation changes with age and exposures, there is the potential for cardiovascular risk factors to mediate their effects through these epigenetic changes. While DNA methylation correlates to cardiovascular disease risk by virtue of measuring biological ageing, there remains the possibility that workplace exposures can more directly affect risk, although this has not often been explicitly explored. As one example, nightshift work has been shown to increase the risk of atherosclerosis. 125 Nightshift work, in a separate study, also showed “suggestive” correlations to differential methylation patterns. 126 Clearly, the relationship between work and cardiovascular disease risk, as mediated by epigenetics, remains an area open to further exploration.
Telomere length
Telomere length serves as another molecular clock. These nucleoprotein complexes serve as the aglets of chromosomes, protecting against the slow erosion that takes place due to the end-replication problem of linear chromosomes. The very ends of chromosomes lose some genetic material at each replication, and thus these repetitive elements have evolved to prevent the erosion of coding DNA. This erosion, and the rate of erosion, can serve as a molecular clock of biological ageing.
Interestingly, several studies have demonstrated an acceleration of telomere erosion in response to social determinants of health (SDOH). Childhood adversity has been associated with shorter telomere length in adults. 122 The socioeconomic status of parents even impacted the telomere length of their children. 123 Lifestyle choices also impact telomere length. 124 Similar to DNA methylation, numerous occupational exposures and the nature of work (such as shift work) have been shown to be associated with reduced telomere length.102,125–141 Biological ageing, as measured by telomere attrition, was accelerated in a longitudinal study in neighborhoods with lower socioeconomic status or worse social environment. 142 Furthermore, vascular ageing has been shown to correlate with telomere length. 143 Vascular injuries have similarly been associated with decreased telomere length. 144 One study found that increased telomere length was associated with workplace learning opportunities. 145 Another study showed a marginal association between maternal stress (including socioeconomic stressors) and shorter telomeres in infants. 146 Interestingly, a 2016 metanalysis indicated that mindfulness exercises were associated with increased telomere length, perhaps serving as an occupational therapy intervention. 147 One study of cardiovascular disease risk in the U.S. examined telomere length in a relatively large sample (963 subjects) 148 ; and found one social factor—home ownership associated with longer telomere length in general, with some differences in significance among ethnic or racial sub-populations. Interestingly, a study of women in the southern U.S. showed that while “chronic stress” led to shorter telomeres, however “perceived stress” may buffer this effect. 148
MicroRNA molecules
A third genetic influence on gene expression is the presence of microRNA molecules. These sometimes are categorized under epigenetic influences because they are thought to impact phenotype solely through controlling the expression of other genes. MicroRNA are 22 nucleotide RNA molecules. Interacting with cognate sequences largely in the 3’ untranslated regions of mRNA molecules, they can either block translation by the ribosome or create double-stranded RNA regions that flag the mRNA for degradation. MicroRNA are encoded by their own genes, similar to mRNA, which puts their expression properly under the field of transcriptomics rather than epigenetics. However, their stability even in peripheral circulation and their changes in response to numerous stimuli gives them great utility as biomarkers.
Several studies have assayed microRNAs as biomarkers of occupational exposures. A pair of 2019 reviews148,149 summarize literature on microRNA expression changes in response to occupational exposures. Exposures to particulate matter, metals, and polycyclic aromatic hydrocarbons have been demonstrated to result in significant changes in the expression of specific circulating microRNAs, although on the whole there are no reliable biomarkers of these exposures. This is largely blamed on the heterogeneity of both exposures and study designs. More recently, Sturchio et al. reviewed the use of microRNAs as biomarkers for the diagnosis and prognosis of mesothelioma, 150 a cancer directly related to occupational and social exposure to asbestos. MicroRNA has been proposed as biomarkers for diverse occupational exposures, including mercury, 151 carbon nanotubes, 152 volatile organic compounds, 153 and even noise. 154 Because microRNAs function through the regulation of other genes, their expression and how it changes between conditions may additionally inform etiology. However, this picture is often obscured by the ability of each microRNA to recognize and regulate many targets mRNA, impacting potentially several cellular pathways.
With specific regards to musculoskeletal and cardiac health, much less is known about the role of microRNAs as biomarkers or mediators of disease. One study showed that miR-143 and miR-145 were both significantly higher in patients with essential hypertension than in age- and gender-matched control patients. 155 Our own recent study further identified changes in microRNA expression associated with lower back function and motion sickness. 156
Need for future studies
Clinical translation of epigenetic biomarker data is complicated by several factors. For one, studies are generally limited in size and difficult to generalize. Differences in the way analyses are performed, such as by RT-PCR or microarray or next generation sequencing, result in data that are not immediately comparable. Additionally, studies assay different biological tissues, such as saliva, tissue, or blood. Variability in sample types, collection methods, nucleic acid isolation methods, assay types, and data analyses all remain standardized. If these challenges can be overcome, then epigenetic biomarkers offer easy-to-assay biomarkers that can potentially inform us about a plethora of exposures, benefiting public health.
Discussion
A literature search is typically a critical and thorough process of information synthesis of existing knowledge. Through careful evaluation and critical summary, we have analyzed the existing body of literature to examine significant aspects of work on health. We considered work as a SDOH on cardiovascular and musculoskeletal diseases, and the associated epigenetic influences. The experience of work itself can affect both physical and mental health on four main levels of influence: the broader work environment, interpersonal relations, psychologically, and interpersonally. This pattern of results is consistent with Bronfenbrenner's Ecological Framework (1979), 20 in which each level influences one another within a whole system. When applied to the system of work or employment among U.S. workers, we see that the wider elements of work conditions (i.e., unemployment or job insecurity, shift work schedules, the psychosocial work environment, work risks and hazards, etc.), interpersonal relationships (i.e., social support, work and family responsibilities), psychological (i.e., perceived discrimination and work-related stress), and intrapersonal (i.e., epigenetics), influencing and being influenced.
Our findings highlight that work is not conducted in a vacuum and it is not only a place you go to obtain income. Work is a complex SDOH that greatly influences health outcomes, and further disparities. Work affects our health; and our health affects our work. The impact of work includes the larger work system, down to exposures on our individual genetics, and many things in between. All of these bio-ecological dimensions are impacted based on race, ethnicity, income, education, and other demographic factors. The most compelling explanation for these findings is that all identified psychosocial aspects of work which were identified in the literature, were represented at every level of the ecological model.
Our analysis reveals gender, racial/ethnic, and occupational (blue-collar vs. white collar) disparities among U.S. workers. Occupational disparities across these dimensions portend different types of work inequities. Ultimately, disadvantaged groups in lower socioeconomic status and educational positions, who are more often in blue collar jobs, do worse health-wise. For example, having a lower education has been associated with a higher risk of poor health. 157 We also see these trends in precarious work (i.e., seasonal jobs, lack of formal contracts, piecework pay), lack of access to health care (i.e., no health insurance or are not offered workers compensation benefits), and inadequate COVID-19 safety issues (i.e., lack of trainings, lack of PPE, low education and/or literacy level), which is often worse for low-income groups. These findings highlight the importance of integrating the bioecological work model into real world solutions and interventions.
Although this present literature review clearly supports the relevance of the bioecological model in examining SDOH on health outcomes, it is important to recognize several limitations of the study. The first limitation concerns the heterogeneity of the literature from the review, in terms of differences in sample populations, differences in disease severity of individuals, different methods and interventions, and different measured outcomes among studies. For example, differences in the sample population demographics (i.e., age, gender, race, and/or comorbidities) may affect the study results. For instance, pooling the data from the original articles was difficult due to heterogeneity in study designs and reported outcomes, 158 and heterogeneity in disease severity. A second limitation is that we only searched the PubMed search engine, which limited our access to literature data and likely biased the literature included in the study. A third limitation is that the search was only limited to English language and only publications over ten years, from 2012 to 2022. A fourth limitation is that inclusion/exclusion guidelines were less rigorous due to the heterogeneity of the sample. A fifth study limitation was that there has been much work done on CVD and epigenetics, but when you limit the review to a role of musculoskeletal work, the body of literature was much smaller. A final limitation of this study was that we selected only arm and leg limbs for musculoskeletal pain/disorders because this review was meant to be broader in nature and less sophisticated than an advanced review, which would be more inclusive of other types of musculoskeletal pain and disorders.
Despite these limitations, results suggest some practical and future research implications.
Use of this bioecological model in practice requires getting the “whole” picture. By addressing not simply the work issues or health issues independently—and taking a broader look at each individual's context and situation, healthcare providers and clinical providers can deliver a higher standard of care. By educating healthcare providers and clinicians about the work-related environment, as well as educating employers about how the work environment can directly impact health and mental health outcomes. Given changes in work, in part due to COVID-19 and elevated risks for those with chronic disease, makes this review especially relevant and timely.
Conclusion
Work is a multifaceted SDOH that greatly influences cardiovascular disease and musculoskeletal disorders; and conversely affects our work. Why and how work impacts these, and other disorders is complex, but likely also involves underlying genetics, changes in an individual's epigenetics (that is, DNA methylation, histone acetylation, telomere lengths, and microRNA status), adaptive/maladaptive biological responses to environmental exposures, and psychosocial and work environment factors. For example, workplace risk factors affect musculature health, while also affecting epigenetic readouts. However, further investigation is required to examine the combination of 1. occupational therapy, 2. gene expression, and 3. other health-related factors as a promising method of managing disease. 159
This review of literature provides a clear need for more robust prospective/longitudinal epidemiological studies. Controlled studies of workplace risk factors should be able to discover epigenetic biomarkers with utility in predicting musculoskeletal health and diseases. These studies should incorporate novel assessment tools, biomarkers to better understand mechanisms, and more definitive/well-validated tools for measuring psychosocial stress/mental health in the workplace. In addition, more detailed qualitative research could provide further insights into the goal-setting experiences among employes in the workplace, health prevention and education. 160 Such an approach will allow application of preventative measures at the preclinical stage. Workplace preventative and detection services can effectively lead to the identification of risk factors, promotion of lifestyle changes and detection of cardiovascular 160 and musculoskeletal diseases. Such services should be integrated into workplace systems to aid the prevention and detection of cardiovascular and musculoskeletal diseases, as well as other chronic conditions. Furthermore, understanding how secondary factors such as social support (positive) and experiences of discrimination (negative) influence the work-health paradigm is paramount. This work is important to help inspire capacity building and research in occupational health, to prevent cardiovascular and musculoskeletal diseases and to preserve a productive life for the ageing work population.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.