
Abstract
Background
Low back pain (LBP) is one of the common self-reported of musculoskeletal pain among working the population. Nonetheless, its influence on work productivity specifically absenteeism and presenteeism among Malaysian academics remains unknown.
Objective
Therefore, this study aims to investigate the influence of LBP on work productivity among academics.
Methods
This is a cross-sectional study assessing the association of LBP on work productivity (absenteeism and presenteeism) among academics. A self-administered questionnaire was used to obtain the study information. Data was analyzed using linear regression and reported in term of unstandardized coefficient (B) and 95% confidence interval (CI).
Results
A total of 411 academics participated with median age 40.5 years. The mean prevalence of absenteeism and presenteeism due to LBP is 2.3% and 19.89% respectively. Occurrence of LBP and its severity were not significantly associated with absenteeism. Nonetheless, LBP severity and anxiety symptoms were significantly associated with increased presenteeism.
Conclusion
The prevalence of presenteeism due to LBP among academics is notably higher than absenteeism. Increases in LBP severity and anxiety were significantly linked to higher rates of presenteeism. Therefore, academic institutions should implement interactive and sustainable workplace wellness programs to enhance their employees’ health and well-being, which may lead to improve their work productivity.
Introduction
In recent years, low back pain (LBP) is the most reported musculoskeletal pain (MSP), and a major public health issue among the working population. Previous systematic review found that the prevalence of LBP in Malaysia among various types of the working population ranged from 12.4% to 84.6%. 1 The teaching profession has been found to have a higher prevalence of MSP than other occupational groups. 2 A previous systematic review suggested that the prevalence of self-reported MSP among teaching population ranges between 39% and 95%. 3 Recent study by Meaza (2020) found that 65.2% of academics experienced MSP in the past 12 months. 4 LBP is a frequently reported MSP site, followed by the neck and upper limbs.
LBP contributes significantly to years lived with disability (YLD). The Global Burden Disease Collaborators discovered that between 1990 and 2020, age-standardized YLD rates declined by 10.5% (11.1%–10.0%) and 10.4% (10.9%–10.0%), respectively. Despite this modest decrease, LBP remains a leading cause of YLD globally. 5 In addition, it is projected that more than 800 million people worldwide may experience LBP by 2050, compared to 619 million in 2020.
There is clear evidence that LBP negatively affects work productivity. Work productivity is commonly assessed through absenteeism and presenteeism. A previous study reported that 53.34% of Brazilian school teachers experienced absenteeism due to illness. 6 The prevalence of presenteeism among school teachers varies greatly between nations. Previous study found Thai teachers revealed presenteeism, 35.0%; 7 Nicaragua, 65.2%; 8 and Brazilian, 43%. 9 Nonetheless, both studies focused on general illness without specifically examining LBP, despite the growing recognition of LBP as a major contributor to productivity loss. For instance, a large-scale study involving 115,880 Swedish patients who sought care for LBP found that 42% experienced sickness absence or disability pension days, compared to 15% in a reference group without LBP. Moreover, the study reported that patients with LBP had a productivity loss of €8928 over 12 months, significantly higher than the €3499 in the reference group. 10 Further support comes from a previous qualitative study that identified the future ability to continue working becomes one of the significant concerns among employees with LBP. This concern includes the possibility of early retirement, an unenjoyable retirement, increased pain at work, needing to retrain, or being unable to continue in their chosen career. 11 Both absenteeism and presenteeism have significant consequences for individuals’ personal lives, health, and overall productivity, and can adversely impact student learning outcomes, particularly in the academic profession where continuity in teaching and sustained engagement are essential.
However, despite global recognition of LBP’s burden, there is a dearth study focusing on the influence of LBP on work productivity among Malaysian working population especially academics. Most local studies have concentrated on prevalence rather than its influence on work productivity. There is a clear need to update and expand our understanding of this issue in the higher education sector. Therefore, this study aims is to explore the LBP severity on work productivity specifically absenteeism and presenteeism among academics with LBP.
Methods
Study design, study population and sample size calculation
This was a cross-sectional study conducted at a public university with four campuses situated in Northern region of Malaysia. All academics included permanent, contract and expatriate with experienced in teaching at least one semester are considered as eligible participants. Meanwhile, academics who will retire within a year of the study period and who have musculoskeletal diseases with specific pathology evidence, such as tumor, fracture, infection, dislocation, or osteoporosis, were excluded from the study.
The sample size was calculated using the OpenEpi version 3.01 software. This study referred the information from a previous study investigating the work productivity related to MSP among the working population. 12 Given the two-sided significance level (95%), statistical power of 80%, the most sample size calculated is 372. An additional 10% has been added to prevent dropouts and to attain sufficient power. Ultimately, the target sample size is 409.
Data collection and study instruments
Upon receiving ethical approval, a permission request letter, information sheets describing the study, and the ethical clearance from the Medical Ethics Committee of academic institution were sent to the Office of the Rector of the selected branch campuses. A brief meeting was conducted with the Rector and the researcher to explain about the background, objectives, and procedures of this study after obtaining their permission. Universal sampling was employed to recruit academics in these campuses. Participation was completely voluntary.
A self-reported questionnaire was utilized to gather extensive information from participants, encompassing socio-demographic characteristics, work information, lifestyle factors (such as sitting time), the presence and intensity of LBP, psychological symptoms (depression and anxiety), and work productivity. The Work Productivity and Activity Impairment Questionnaire: General Health V2.0 (WPAI:GH) was employed to measure absenteeism and presenteeism related to work productivity, while the presence of MSP was assessed using items adapted from the Nordic Musculoskeletal Questionnaire. Pain intensity was gauged through the Visual Analog Scale, and psychological symptoms were evaluated with translations of the Beck Anxiety Inventory and the Beck Depression Inventory, both tailored for the Malay-speaking population.
Pain catastrophizing was assessed using the Pain Catastrophizing Scale (PCS) and evaluated somatization tendencies through selected items from the Brief Symptom Inventory. Lifestyle factors, particularly sitting time, were measured through one single item from the International Physical Activity Questionnaire. The item measures the duration (minutes per day) of time spent sitting on a usual weekday. This includes time spent sitting at a desk, visiting friends, reading, sitting or lying down while watching television across various contexts including work, home, or leisure.
Statistical analysis
Data were analyzed using using Stata version 13.0 software. Prior to answering study objectives, the normality of the data was assessed using Kolmogorov-Smirnov & Shapiro-Wilk test. For continuous data that normally distributed reported mean and standard deviation (SD), while non-normally distributed reported median and interquartile range (IQR). For categorical, the descriptive results were presented as frequency and percentage.
Linear regression was used to estimate the association of LBP severity on work productivity (absenteeism and presenteeism). Results are reported in terms of unstandardized coefficient (B) and 95% confidence intervals (CI). The p-value < 0.05 was considered statistically significant.
Results
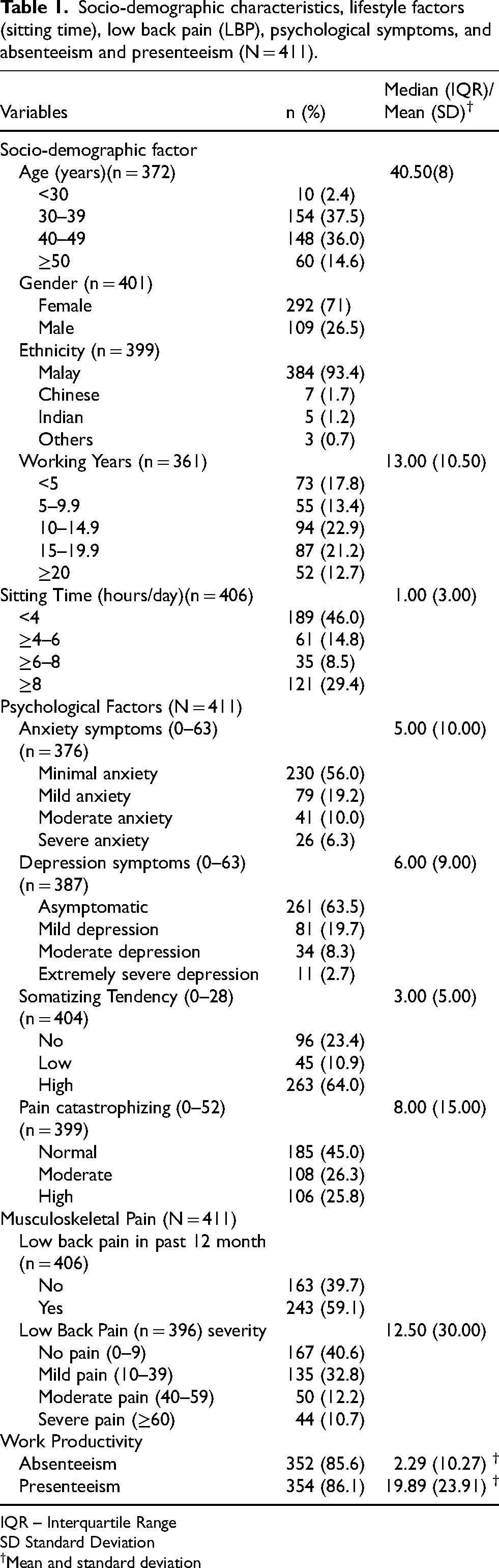
Of the 420 self-reported questionnaires distributed, 411 (97.86%) were returned the questionnaires. Majority of participants were Malays (93.4%) and females (71%) (Table 1). The median (IQR) age was 40.50 (8.0) years. Slightly more than half of the participants had worked for more than 10 years (56.8%), and nearly half (46%) reported sitting less than four hours/day on a usual weekday. Most participants had minimal anxiety symptoms (56.0%), asymptomatic depression (63.5%), and normal pain catastrophizing levels (45.0%). Nonetheless, 64.0% of participants exhibited a high level of somatizing tendency.
Socio-demographic characteristics, lifestyle factors (sitting time), low back pain (LBP), psychological symptoms, and absenteeism and presenteeism (N = 411).
IQR – Interquartile Range
SD Standard Deviation
Mean and standard deviation
In the past 12 months, 59.10% had LBP, with the majority had mild to moderate severity (45.0%). The mean (SD) work time missed due to LBP (absenteeism) and work impairment while present (presenteeism) were 2.29 (10.27) and 19.89 (23.91), respectively.
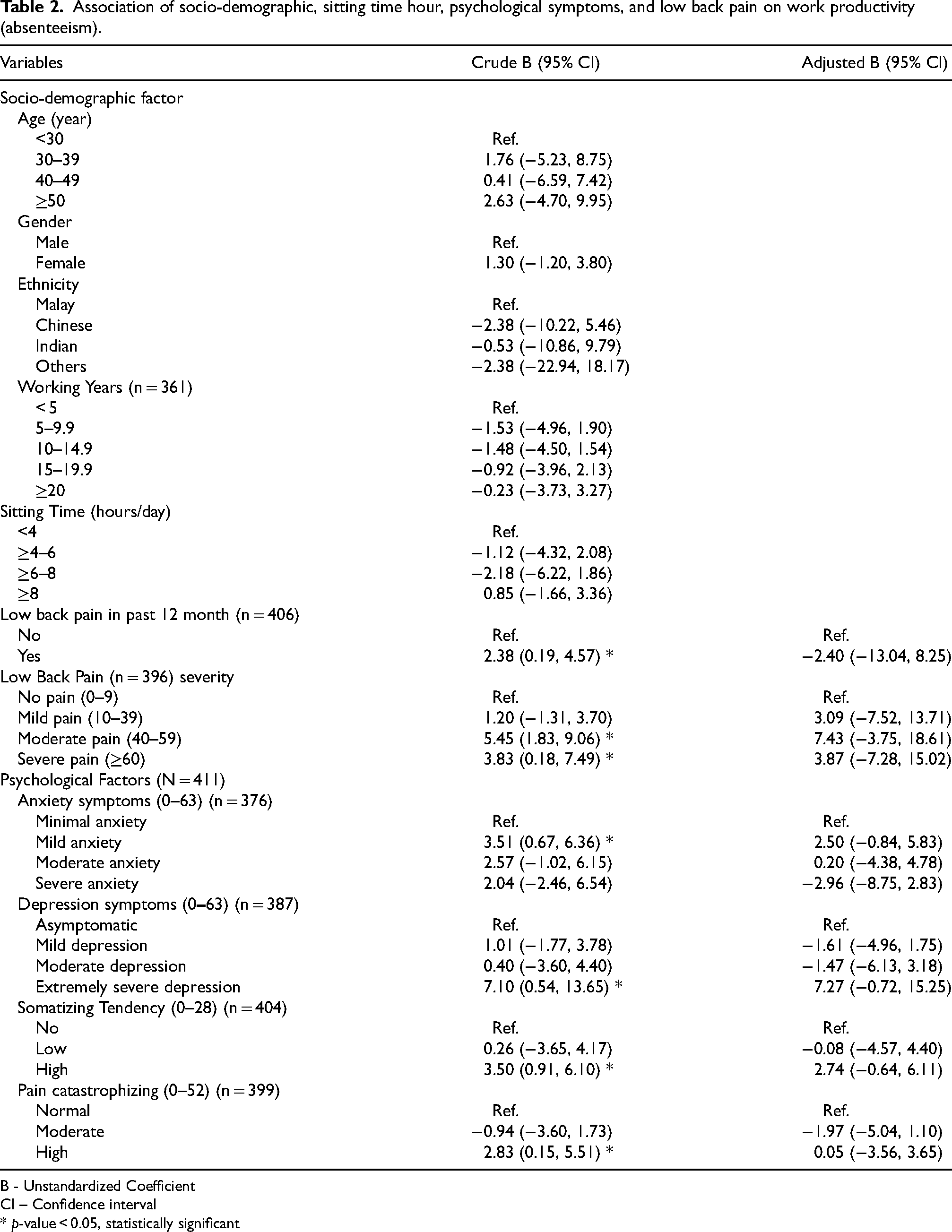
Table 2 shows the univariable and multivariable linear regression analysis on factors associated with absenteeism. In the univariable analysis, higher absenteeism was significantly associated with LBP in the past 12 months with moderate and severe pain, as well as mild anxiety, extremely severe depression, high somatization, and high pain catastrophizing. Participants with LBP had 2.38 units higher absenteeism than those without LBP. Those with moderate and severe LBP had 5.45 and 3.83 higher absenteeism, respectively.
Association of socio-demographic, sitting time hour, psychological symptoms, and low back pain on work productivity (absenteeism).
B - Unstandardized Coefficient
CI – Confidence interval
* p-value < 0.05, statistically significant
Mild anxiety, extremely severe depression, high somatization and high pain catastrophizing were also linked to increase absenteeism. All the significant variables (p < 0.05) were tested simultaneously in the multivariable analysis. However, none of these associations remained significant in the multivariable analysis.
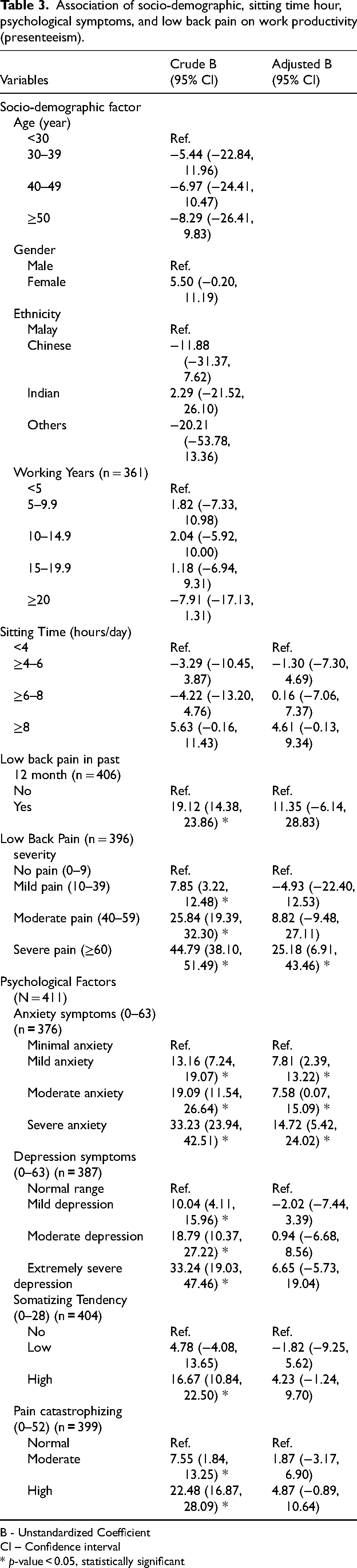
Table 3 presents the univariable and multivariable linear regression analysis on factors associated with presenteeism. In the univariable results, presenteeism was significantly associated with all severity of LBP, all levels of anxiety and depression symptoms, high somatization, and moderate to high levels of PCS.
Association of socio-demographic, sitting time hour, psychological symptoms, and low back pain on work productivity (presenteeism).
B - Unstandardized Coefficient
CI – Confidence interval
* p-value < 0.05, statistically significant
Participants with LBP in the past 12-month had 19.12 units higher presenteeism compared to those without LBP. Specifically, participants with mild, moderate, and severe LBP had 7.85, 25.84, and 44.79 units higher absenteeism, respectively. Compared to those with minimal anxiety, participants with mild, moderate, and severe anxiety, had higher presenteeism scores by 13.16, 19.09, and 33.23 units, respectively. Similarly, participants with mild, moderate, and extremely severe depression had presenteeism scores higher by 10.04, 18.79, and 33.24 units, respectively. Participants with high somatization, moderate, and high PCS had presenteeism scores higher by 16.67, 7.55, and 22.48, respectively.
In the multivariable analysis, there were only severe LBP and all levels of anxiety symptoms were significantly associated with the presenteeism.
Discussion
The aim of this study was to evaluate the association between LBP severity and work productivity specifically absenteeism and presenteeism on academics in Malaysia. A total of 243 participants (59.1%) reported to have LBP. The prevalence identified in this study is comparable to that of previous study conducted within the same working population, which reported rates range from 53.5% to 59.8%.13–15 Nonetheless, a previous local study reported that the 12-month prevalence of LBP among academic in different institutions was lower (33.3%) than current findings. This variation may be due to different distribution of participants’ socio-demographic such as age and working years which might influence the difference prevalence of LBP. Overall, this indicated that the occurrence of LBP was considerably prevalent among academicians.
Current results found that 19% of participants experienced impairment while working (presenteeism) due to LBP. It is challenging to compare the observed prevalence with that of previous studies due to variations in the studied populations and the focus on presenteeism related to different health conditions or diseases. Previous study conducted among different working populations reported that the prevalence of presenteeism among Japanese nurses was 58% which three times higher than current finding. 16 Occupations in caring, helping, and teaching sectors are frequently associated with higher presenteeism likely due to close relationship with care recipients that discourage absenteeism despite illness. 17 Similarly, Mamaye et al. (2024) reported that 35.2% of primary school teachers experienced presenteeism, which is nearly double the prevalence observed in our study. 18 These discrepancies may stem from differences in occupational demands, workplace environments, cultural perceptions of pain, and variations in the measurement tools or definitions of presenteeism employed across studies.
Meanwhile, there were 2% of the participants who missed their work (absenteeism) due LBP. To our knowledge, none of work productivity study has been conducted in similar working population. Interestingly, we found comparable results with previous study among Japanese nurses which reported their absenteeism 3.3%. 19 Absenteeism rate was less than 10% among various working population indicate that missing work due to LBP is low and not a major problem as compared with presenteeism. The low absenteeism related to LBP may be attributed to cultural perceptions regarding LBP management. Many individuals believe that seeking medical treatment for LBP has little effect on their recovery. 20 Additionally, it is postulated that high workloads compel employees to fulfill their responsibilities, as they fear that their absence will increase the workload and stress for their colleagues. Consequently, presenteeism due to LBP is observed to be slightly higher than absenteeism. Future studies should explore this in detail.
In the univariable analysis, the 12-month occurrence of LBP was significantly associated with absenteeism. However, it’s important to note that the risk estimate for absenteeism is not as high as for presenteeism, which is nine times greater. This aligns with findings by Matsudaira et al. (2022), who reported that presenteeism poses a greater concern than absenteeism in terms of prevalence and economic burden. These findings highlight LBP as a major cause of productivity loss, sick leave, and early retirement, especially in occupations like academic work. 21 Nonetheless, the moderate association between LBP and absenteeism suggests that other health issues or contextual factors might also influence decisions to take leave. This suggests that while LBP has some effect on absenteeism, other health and non-health conditions may also contribute to participants taking leave. Subsequently, our current findings also showed significant association between LBP severity and absenteeism. This observation was consistent with the findings by previous study which demonstrated that those who had moderate and severe LBP were prone to have absenteeism compared to those without LBP. 22 In contrast with the previous study, our results found non-significant association between LBP severity and absenteeism in the multivariate analysis. A previous study found that individuals with LBP from low- and middle-income countries often self-manage their condition before seeking medical care. Self-management strategies include traditional home remedies, such as herbal oil massages, over-the-counter drugs, medications available at home, or advice from friends and family. 23 This reliance on self-management could explain why participants with LBP are less likely to take work leave, thus contributing to the observed non-significant association between absenteeism and LBP severity.
Furthermore, we hypothesize that the academic profession’s substantial work demands render the process of applying for leave less meaningful. Academics often feel obligated to fulfill their job responsibilities even while on leave, which undermines the intended benefits of time away from work. Future studies should conduct a more detailed exploration of these dynamics. Additionally, the use of unstandardized instruments to measure absenteeism in both studies may also explain the non-significant association observed between these two variables.
Meanwhile, our results indicated a significant relationship between the severity of LBP and presenteeism in both univariable and multivariable analyses. These findings are consistent with previous studies19–22 which also identified a significant increasing trend in LBP severity and presenteeism. Work productivity is reduced if the workers have poor health condition. 24 It is plausible that individuals who had poor health condition exclusively experiencing severe pain were more likely to suffer functional limitations, feel demotivated to carry out their daily tasks, and experience breakdowns. Consequently, this will lead to a reduced in working productivity.
In the univariable analysis, psychological symptoms specifically mild anxiety and extremely severe depression were found to be significantly associated with absenteeism due to LBP. This finding is consistent with a previous study in India, which also found that greater psychological symptoms severity was linked to higher absenteeism rates. 25 These psychological conditions may contribute to by intensifying pain perception, reduce pain coping skills, and result in physical symptoms like fatigue and sleep disturbances. Furthermore, severe depression can decrease motivation and functional capacity, leading to greater difficulty in managing daily activities and work tasks. Additionally, anxiety and depression may promote fear-avoidance behavior, causing individuals to avoid activities that might worsen their pain, which can lead to physical deconditioning. These psychological factors can also interfere with adherence to treatment plans, prolonging pain, and functional limitations, thereby increasing absenteeism. The compounding stress from dealing with both chronic pain and psychological issues creates a vicious cycle that further exacerbates work absenteeism. Nonetheless, the association between anxiety and depression with absenteeism due to LBP become non-significant in the multivariable analysis. The non-significant association in the multivariable analysis indicates that psychological symptoms and LBP were not the strongest influence on absenteeism in this study population.
On the other hand, results from univariable analysis found that all levels of anxiety symptoms (mild, moderate, severe) and all levels of depression symptoms (mild, moderate, and extremely severe) were significantly associated with productivity loss at work (presenteeism) due to LBP. An increasing trend of risk estimate was also observed as the level of psychological symptoms are increased. The trend is not surprising as previous evidences on the association between psychological symptoms and LBP were established. 26 These findings highlight how the co-occurrence of these conditions further exacerbates the negative effects on academics’ presenteeism. Our results are consistent with prior research by Yokota et al., 27 which identified a notable relationship between the prevalence of depression and work productivity among nurses suffering from chronic pain. Nonetheless, only anxiety symptoms remained significantly associated with presenteeism due to LBP after adjusted all the possible factors. This indicates that the studied participants have significant anxiety issues, which are associated with LBP and reduced work productivity. Therefore, an employee mental well-being program is necessary to address these issues.
Our univariable analysis found that there was significant association between PCS with absenteeism and presenteeism due to LBP. In addition, the risk estimate of presenteeism is relatively higher than absenteeism among participants with PCS. This could be due to the presence of ripple effect of LBP that influence its association between PCS and presenteeism. PCS is considered as one of the most one of the most important psychological correlate of pain chronicity and disability. 28 The association between presence pain with catastrophic thinking and depression leading to decreased work performance. According to Becker et al., 29 it has also been suggested that the neurobiological mechanism by which pain causes decreased performance is the suppression of reward and motivational processes in the brain’s dopamine system. Nonetheless, the association between PCS with presenteeism due to LBP was not statistically significant in the multivariable analysis. This indicates that PCS might not as prominent contributing factors as other psychological factor such as anxiety symptoms. Further study should be considered in looking this into details.
Meanwhile, somatization was significantly associated with absenteeism and presenteeism, consistent with previous research by Bailey et al. 30 However, this association was not significant in the multivariable analysis. Earlier studies indicated that mental health symptoms such as depression, anxiety, and somatization can impair worker functioning. However, the lower prevalence of somatization among academics compared to anxiety accounts for the non-significant association observed in the multivariable analysis.
Although the results provide valuable insights into the effects of LBP on absenteeism and presenteeism among academics in the northern region of West Malaysia, several limitations need to be acknowledged. First, the cross-sectional design limits the ability to establish causal relationships between LBP and study outcomes (absenteeism and presenteeism). Second, this study relied solely on self-report measures which may introduce to recall bias. Nevertheless, the items used have been validated in previous studies, supporting its appropriateness as measurement tools. Additionally, future research should consider including participants’ monthly salaries to better quantify the cost implications of absenteeism and presenteeism, providing organizations with a clearer picture of the impact of LBP on work productivity. Despite these limitations, the study highlights the substantial influence of LBP on reducing work productivity particularly presenteeism. To our knowledge, this study is a pioneering effort in examining the impact of LBP on work productivity, particularly within the Malaysian academic sector.
Conclusion
In conclusion, presenteeism due to LBP is more prevalent than absenteeism among academics. Increases in LBP severity and anxiety were significantly associated with increased presenteeism among academics. Therefore, academic institutions should implementing an interactive and sustainable workplace wellness program to enhance their academics’ health and well-being and subsequently improve their work productivity.
Footnotes
Acknowledgment
We would like to thank all the University administrators and academics for their cooperation and participation in our study. This study was supported by a Universiti Sains Malaysia, Short-Term Grant with Project No: 304/CIPPT/6315622.
Ethics approval and consent to participate
This study was approved by the Medical Ethics Committee of Universiti Sains Malaysia (USM/JEPeM/21120770) and performed in accordance with the principles of the Declaration of Helsinki.
Informed consent
Written informed consent was obtained for publication of this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Short-Term Grant from Universiti Sains Malaysia, Project No: 304/CIPPT/6315622.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets are not publicly available but are available from the corresponding author upon reasonable request.