
Abstract
Background
Despite the growing popularity of aerial sports, limited research has investigated musculoskeletal (MSK) injury incidence among female acrobatic athletes. Understanding injury prevalence is essential for implementing effective prevention strategies.
Objective
To investigate demographic characteristics, physical activity (PA) levels, and MSK injury occurrence in female aerial acrobatics athletes in the western region of Saudi Arabia.
Methods
Sixty female aerial acrobatics athletes (mean age: 28.66years) participated. We assessed PA using International Physical Activity Questionnaire–Short Form, and data on MSK injury history and sport-specific profiles were collected. Descriptive statistics and Chi-square tests examined correlations between injury occurrence and factors such as age, experience, and type of aerial activity.
Results
Most participants (60%) reported high PA levels. The majority (92%) performed warm-ups and cool-downs routines and mainly exercised under supervision. The current injury prevalence was 20%, with 12 participants reporting ongoing injuries. Common injury sites included the back 8(28.6%), knee 7(25%), and wrist 6(21.4%).
Conclusion
Musculoskeletal injury prevalence among participants was 20%, reporting a current injury related to aerial acrobatics sports. This study revealed low MSK injury rates and high PA levels among female aerial acrobatics athletes, primarily characterized by limited experience. To promote injury prevention, further research is needed with a larger sample and a focus on factors influencing injury frequency such as age, acrobatics type, and upper body strength. In addition, developing a reliable assessment tool designed for aerial acrobatics athletes’ performance is recommended.
Keywords
Introduction
Acrobatic aerial sports, characterized by performing dynamic movements that require the power of upper and lower extremities strength, flexibility, and precision.1,2 Female athletes from gymnastics to aerial arts, display a unique blend of athleticism and artistry movements. 3 Aerial Hammock, Aerial Silks, Aerial Hope (Lyra), and Circus Pole are some examples of aerial acrobatics sports types. However, because of the nature of these sports, with their high-impact landings and complex routines, places athletes at high risk of injuries.2,4
The global rise in sports participation, particularly among female athletes, has led to an increase in both acute and overuse sport-related injuries over the past three decades.5,6 Research has established some injury patterns amongst female sports participants. This includes a higher incidence of stress fractures, particularly in areas such as pelvis, femoral neck, and tarsal navicular compared to men.7–9 Studies on circus arts, a type of sports like aerial acrobatics sports in many aspects, highlighted a high injury rate. For instance, 3.3 injuries per 1000 h of practice were noted among circus arts students, where the majority of the injuries were incurred in the lower back and shoulder. 10 Adult circus artists had a greater injury risks (13 injuries per 1000 h of practice) compared to adolescents (3 injuries per 1000 h of practice). 11 Female gymnasts, who perform similar acrobatic movements, usually complain of shoulder injury, with the prevalence increasing proportionally to extended training duration.4,12 Moreover, aerial acrobatics sports performers are particularly susceptible to spine injury following fall.13,14
There has been a significant rise in sports participation, including acrobatic sports, particularly among women in the Saudi young population. 15 This increased interest in sports and physical activity (PA) which is supported by new government initiatives and action plans to promote women's athletes as part of comprehensive national development strategies. 16 The rising popularity in acrobatic sports, pursued both competitively and for general fitness improvement, is an important contributing factor. 17 As the participation and popularity in acrobatic sports rise, understanding the prevalence and nature of injuries in female acrobatic sports becomes a priority. This is especially crucial for aerial acrobatics athletes, coaches, trainers, and medical professionals.
Despite the growing popularity of aerial acrobatics sports, such as aerial silks, hammock, hoop, and pole, at international and national levels, there remains limited literature addressing the common sites of injury among practitioners. There are numerous studies have identified potential determinants of musculoskeletal pain and injury, including technique, training load, and biomechanics. 15 However, there is a clear lack of comprehensive research examining the influence of physical activity level, age, experience, and other intrinsic and extrinsic predisposing factors on injury risk among female acrobatic athletes in Saudi Arabia. 18 Considering aerial acrobatics as a new sport, is an indicator of the general absence of specialized knowledge and trained experts in Saudi Arabia. This could result in higher chances of injury due to inadequate coaching, training habits, and safety protocols. Therefore, there is a serious need for further research to inform evidence-based injury prevention practices and professional education in this rapidly growing sport discipline. 19
Methods
Study design
This is an observational study.
Participants
For this research we recruited sixty female aerial acrobatics sports athletes between the age of 18 and 45 years old who are actively engaged in acrobatic sports for more than one month. Participants were excluded if they experienced recent fractures or significant musculoskeletal conditions unrelated to acrobatic sports, had certain medical conditions such as diabetes, hypertension, or hyperthyroidism, or were currently pregnant. Recruitment and data collection occurred at a female acrobatic center, chosen for its accessibility, participant diversity, and institutional support. The center provided the researcher with appropriate facilities for data collection, which facilitated participant engagement and ensured the feasibility of the recruitment process.
Outcome measures
Musculoskeletal injuries and sport-specific profiles were assessed with a comprehensive questionnaire filled using Google Forms. To identify musculoskeletal injuries, participants were asked to self-report any injury sustained, and to ensure consistent reporting an explicit definition of “injury” was provided (e.g., any symptom or complaint that resulted from acrobatic sport activity and affected training or performance or required medical treatment). Participants’ experience level was measured subjectively, where participants responded to a single question to rate their experience level (beginner, intermediate, or advanced). The International Physical Activity Questionnaire– short form (IPAQ-SF) used to measure the physical activity level of the participants in the last seven days and categorized them into (low, moderate, and high) based on their responses. The IPAQ-SF has also demonstrated superior test-retest reliability (ICC = 0.80) 17 and established validity as a measure of physical activity. Given the established validity of the International Physical Activity Questionnaire IPAQ in quantifying physical activity, and assuming a correlation with injury occurrence, it may serve as a reliable, evidence-based measure for assessing injury risk by reflecting the direct relationship between physical exertion and musculoskeletal strain. 20
Procedures
All participants read and signed the consent form voluntarily prior to recruitment. Subsequently, personal and demographic information, physical activity level (IPAQ - short form), history of musculoskeletal injuries and sport specific profile were obtained using a Google Forms questionnaire. Our study protocol collected all necessary data during a single visit, minimizing the risk of missing data.
Determination of sample size
The sample size for this research was determined using G*Power software (version 3.1.9.7). Based on an a priori power analysis, with alpha level of 0.05, and power of 0.80, the required sample size was determined to be 57 participants. 15
Statistical analyses
Descriptive statistics including frequencies, counts, means, standard deviations (SD), and percentages (%) were computed for demographic, physical activity, and sport-related profile data using “IBM SPSS Statistics for Windows, version 28 (IBM Crop., Armonk, N.Y., USA)”. The chi-square(r) test was used to test the correlation between the current injuries and (age, type of aerial acrobatics sport, experience level, and physical activity level) at a significant level of (≤ 0.05).
Institutional review board statement
Informed consent was obtained from all participants prior to data collection. This study was approved by the Faculty of Medical Rehabilitation Sciences, King Abdulaziz University ethical review committee (IRB Approval No. FMRS-EC2023-005), ensuring that it conformed to the ethical guidelines of the Declaration of Helsinki.
Results
Participants’ demographics
Sixty female participants were included in the study. The participants’ mean age was (28.6± 6.47 years). A total of 41 (68%) of the participants were within the BMI normal range (Table 1).
Participant's demographics (n = 60).

Participants’ physical activity and sport-related profile
According to the IPAQ's level of physical activities, the majority of participants 60% (n = 36) had high levels of physical activity, whereas 28.3% (n = 17) had moderate levels of physical activity and 11.7% (n = 7) had low levels of physical activity.
The majority of participants (52%) have been practicing aerial acrobatics sports for less than six months, followed by 23.3% who had been participating for more than 18 months (Table 2). Regarding self-rated experience level, 38.3% of participants (n = 23) identified as beginners, 53.3% (n = 32) as intermediate, and 8.3% (n = 5) as advanced.
Aerial acrobatics participants sports profile and injuries.

The most preferred type of Aerial acrobatics types to least, were aerial hoop, aerial hammock, aerial silk, and aerial pole. The most practiced types of aerial acrobatics sport were hoop (n = 42) and hammock (n = 40). Group exercise was the most preferred form of Aerial acrobatics exercises sessions. Additionally, 91.7% (n = 55) of participants performed warm ups and cool downs before and after sessions (Table 2).
Out of 60 participants, only 12 had current Aerial acrobatics related injuries, where the back was the most injured site 28.6% (Table 2). Of these, two participants were beginners, nine were intermediate, and only one was advanced aerialist acrobatic participants. Interestingly, nine out of the 12 injured participants played aerial hoop and hammock exercises.(Figures 1 and 2
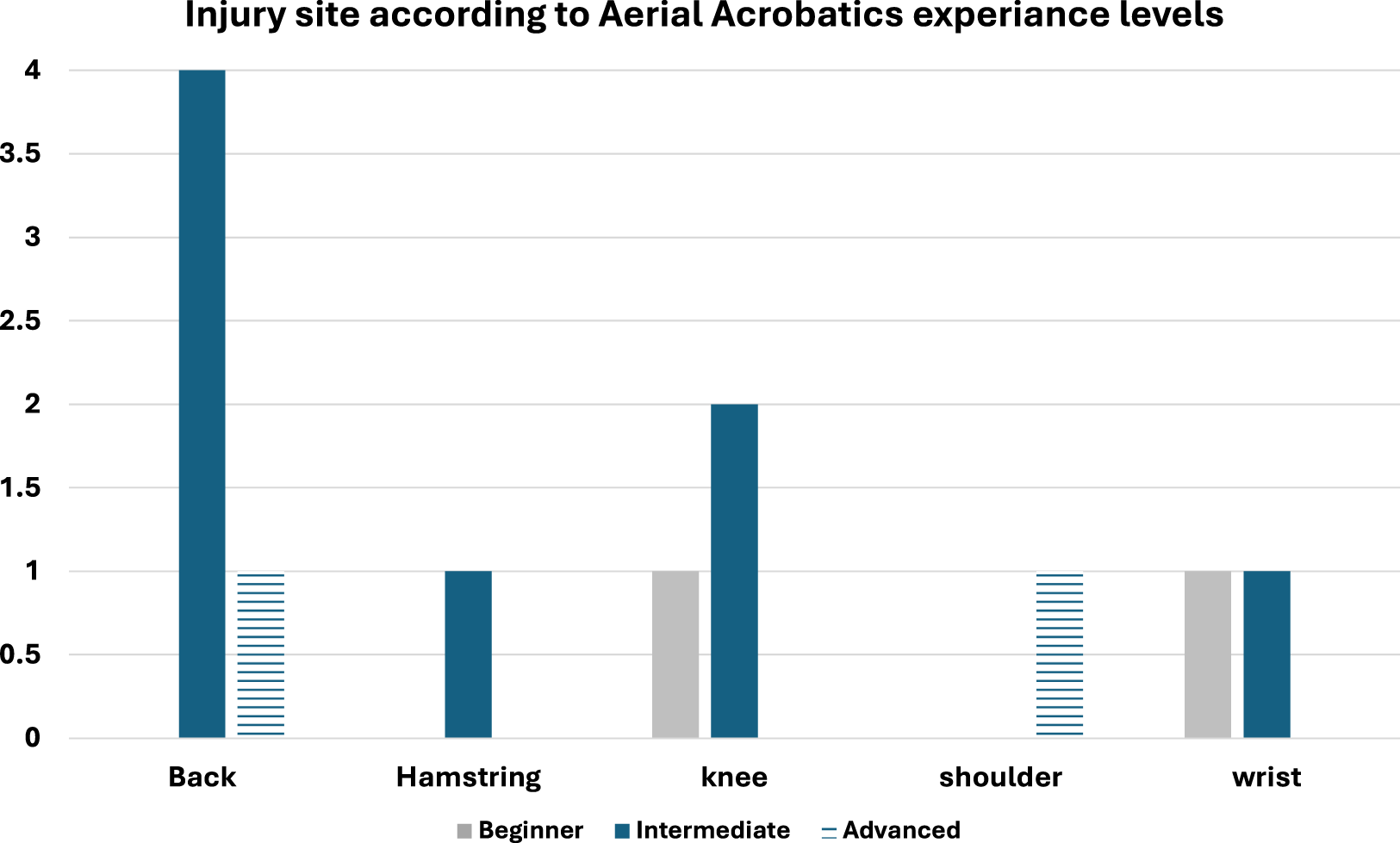
Current injury site according to aerial acrobatics experience level.
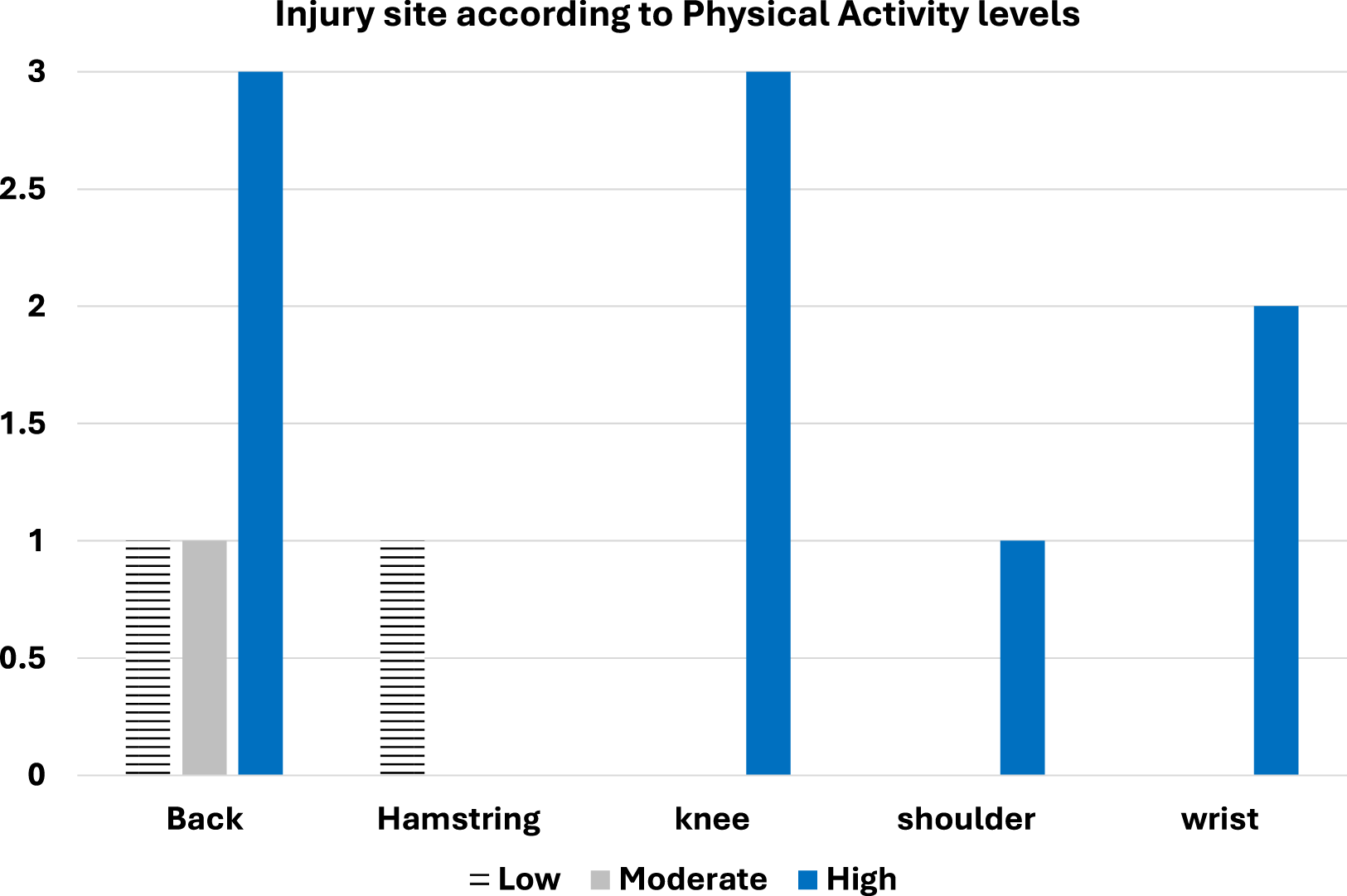
Current injury site according to physical activity level.
Correlation between current injury and demographics, PA, and sport-related profile
Only current injury showed significant correlation (≤ 0.05) with BMI and warming up and cooling down (r = 0.026, 0.031), respectively (Table 3).
Correlation between current injury suffering and other variables.

*Significantly correlated if ≤ 0.05
Discussion
The main purpose of this study was to evaluate the current levels of physical activity PA and current musculoskeletal injuries among female acrobatic athletes in Jeddah, Saudi Arabia. The findings revealed that almost 60% of the sample was adequately active based on the IPAQ-SF results. This result differs from many previous studies carried out within the countries of the Arabian Gulf region, including Saudi Arabia, which reported a larger prevalence of physical inactivity among females. For instance, Al-Zalabani et al. found that quite a large proportion (66.6%) of the women in their study were physically inactive.21,22 While Bajamal et al. 23 found that physical activity levels is low among female adolescents. Barriers to PA include lack of facilities, time constraints, and cultural factors. 24 Despite the fact that the results of the current study are different from those of the majority of earlier studies,25–27 they are comparable to another study by Amin et al., in which 59% of the sample was generally active. 28
To the best of our knowledge, this study is the first to investigate the prevalence of musculoskeletal injuries in women's acrobatic sports in Saudi Arabia. This initial work is vital in bringing awareness and better understanding for these types of injuries in this unique population. Our study identified that 26.7% of participants reported injuries in the last 12 months, with a current injury prevalence of 20%. Despite the unique demands of aerial acrobatics sports, which require strength, flexibility, and coordination, these injury rates are lower than those reported in other acrobatic sports and circus arts. This may be due to high safety measures and supervision by qualified trainers.13,29
During our study, we collected data on previous and current injuries through a survey. The most common injury sites were the back, knee, and wrist, likely due to repetitive weight-bearing activities and sophisticated movements in acrobatic sports. The findings are consistent with the current existing literature on gymnastics and circus arts, which identify the lower limb, upper limb, and spine as common injury sites. In particular, the lower back, shoulder, ankle, and wrist are frequently reported as specific locations of injury.10,12
A few studies have indicated that the risk of injury is increased with age. This is particularly evident in circus arts students aged 15 to 17 years, of whom around 56.4% reported sustaining an injury. 10 Similarly, increased acute and chronic injuries have been noted in those aged 13 years and above. However, our study found no statistically significant relationship between age and the incidence of injury. This may be explained by the comparatively small sample size, that prevents the detection of true associations, if present. It is also possible that the age range of our participants (18–45 years) excluded the younger age groups where the trends of age-related injury may be more pronounced. Alternatively, other confounding factors played a larger role in our specific cohort.
Aerial acrobatics sports include aerial hammock, aerial silks, aerial hoop (lyra), and circus pole. In our research, the most practiced aerial sports disciplines were aerial hoop (70%) and hammock (66.7%), followed by silk (20%) and pole (10%). This popularity is likely because hoop and hammock allow for more points of contact and grip, making them easier to maneuver. However, silk and pole are more challenging due to the continuous climbing required, which may explain their low popularity. Regardless of the type of aerial acrobatics sport, our study found no significant indication of increased injury risk. Furthermore, no previous studies have examined the relationship between specific types of aerial acrobatics sports and injury incidence.
Our results showed that the intermediate-level participants represented the most prominent group (41.6%), followed by beginners (28.3%) and advanced athletes (10%). Surprisingly, intermediate-level participants had the highest rates of injury. This can be explained by a number of behavioral and biomechanical reasons. Behaviorally, intermediate athletes tend to have a basic knowledge of the sport but may overestimate their abilities. This may enhance them to try more advanced skills or higher-risk tricks without sufficient proficiency or supervision. The eagerness to learn new skills and the willingness to take risks, combined with the lack of refined technique and body awareness relative to advanced practitioners, may increase the likelihood of injury.
Biomechanically, intermediate athletes may not yet have developed optimal movement patterns, strength, or flexibility to safely perform more advanced techniques. This may lead to compensatory movements, heightened joint loading, thereby raising the risk of injury. For example, athletes may attempt inversions or drops without sufficient core strength or shoulder stability, consequently placing excessive stress on these areas. Thus, there is a need for more research, involving the use of biomechanical measurements and qualitative interviews. This can fully explain the complex interplay of factors leading to injury risk in this group of participants.
Regarding physical activity levels, our study found no significant correlation between levels of physical activity (high, moderate, or low) and current injuries. This finding contrasts with the results reported by Choe et al. found a significant relationship between the intensity of physical activity and the occurrence of injuries. 30 The discrepancy between our results and previous study may attribute to the differences in the study population and activity types, as our study was specific to the arial acrobatics sports. Although our results demonstrated a higher incidence of injuries in participants who reported always warming up and cooling down, this finding can be explained as the quality and content of the warm-up or cool-down process may opposed to the practice itself. In addition, insufficient long duration of static stretching before activity have previously been demonstrated to be associated with increased injury risk. 31 Moreover, intrinsic and extrinsic risk factors, for example overuse, anatomical predispositions, or could negate the protective effects of warm-up and cool-down practices in specific injury types. 32
Limitations
The results of this study must be seen in the context of several limitations. First, the fact that our participants were women only, further suggests that generalizing our study's findings to general groups may not be appropriate. However, these findings are still an important source of information and practical guidance specifically for young and middle-aged women participating in acrobatic sports. Additionally, there was a lack of previous research on scales measuring physical performance and injury risk in aerial sports. Second, the relatively small sample size (n = 60) may limit the generalizability of the study. Therefore, future research should incorporate larger and more diverse samples and possibly objective measures to verify injuries. Third, the cross-sectional design employed in this study, which gathers data at a single point in time, restricts the capacity to make inferences regarding causal links between variables identified and injury outcomes.
Fourth, the absence of clinical verification of the reported injuries is a major limitation. While information based on self-reported injuries can provide valuable information regarding their prevalence and patterns, clinical evaluations by medical practitioners would provide a more objective and precise description of these injuries. Future research can benefit from incorporating clinical assessments or medical records to corroborate the self-reported injury information. Additionally, there was a lack of previous research on scales measuring physical performance and injury risk in aerial sports
Conclusion
In conclusion, this current study found that Saudi women acrobat athletes engage in high levels of physical activity, suggesting a higher awareness of the relationship between physical activity and overall well-being. Furthermore, our findings demonstrated that the incidence of injuries in aerial sports is low. This could be because of the strict safety protocols at the fitness facility, in addition, the fact that most participants were being watched over by qualified and experienced trainers. The most frequently affected areas were the back, knee, and wrist. Factors, such as age, degree of physical activity, degree of aerial sport experience, and type of aerial sport practiced were also not associated with risk of injury. In addition, Obesity as well as warming up and cooling down factors were associated with increased the risk of injury. Thus, it is recommended to educate new players, clinicians, and trainers about the possibilities of injuries related to previous risk factors to reduce the frequency of injuries in this sports population.
Future studies are encouraged to include longitudinal designs to improve understanding of injury mechanisms across time, include biomechanical evaluations to examine movement patterns and forces, and involve larger and more diverse samples to improve the generalizability of results.
Footnotes
Acknowledgements
The authors want to thank Ms. Ghada Alturk, Loca Studios, and all participants for their valuable contribution to this study.
Ethical considerations
Approval was granted by the Faculty of Medical Rehabilitation Sciences, King Abdulaziz University Ethics Committee (Ref. FMRS-EC2023-005).
Informed consent
Informed consent was obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deanship of Scientific Research (DSR) at King Abdulaziz University, Jeddah, (grant number (GPIP:260-883-2024)).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.