
Abstract
Background
Night work may be imposed in several work sectors, or chosen by companies because of its economic advantages. However, it may have negative effects on employees’ health.
Objective
To assess the repercussions of night work on sleep, mood and quality of life of employees concerned by night work.
Methods
Cross-sectional and descriptive study conducted in 2023 among night workers in two companies. Sleep disorders, mood disorders and quality of life were assessed by the Spiegel questionnaires, the HAD scale and the SF-12 questionnaire.
Results
A total of 199-night workers were included. Mean age was 36.1 ± 8 years. The median Spiegel score was 20 (IQR: 19–21). Sleep quality was pathological in 4.5% and disturbed in 93.5% of cases. The median HAD score was 16 (IQR: 13–20). Anxiety and depression were present in 10.6% and 32.2% of cases, respectively. The median SF-12 global score was 39 (IQR: 37–41). The overall quality of life was slightly impaired in 43.7% and, moderately impaired in 56.3% of cases. A positive correlation was found between quality of life and sleep quality (r: 0.164; p < 10−3). A negative correlation was found between quality of life and mood disorders (r: 0.164; p < 10−3) and also between sleep quality and mood disorders (r: 0.058; p = 0.001).
Conclusions
Our study highlighted the harmful effects of night work on employees’ sleep quality, mood and quality of life. The mission of the occupational physician is to ensure better adaptation to night work, through an analysis of working conditions and an implementation of protective measures.
Introduction
The most known atypical working hours are shift work, night work and weekend work.1,2 Night work is defined as any work performed between 9 p.m. and 6 a.m., or more regularly, any work whose usual schedule includes at least three hours during this period, at least twice a week. 3
Night work is a significant risk factor for employees’ health, affecting both physical and mental well-being. Night work is associated with neuropsychological disorders such as mood disorders, anxiety, and depression. Chronic fatigue and insomnia are also prevalent among night workers, leading to irritability and cognitive impairments. 4 Night work has been linked to increased cardiometabolic risks, including glucose intolerance and hypertension. There is also evidence suggesting a potential link to breast cancer and immune system vulnerabilities. 5 Night shifts are associated with a higher risk of occupational injuries compared to day shifts. The risk of injury increases with successive night shifts, highlighting the impact of fatigue and reduced alertness. 6
Indeed, the human body is subjected to a circadian rhythm, programed by internal biological clocks. According to the definition of the National Institute of General Medical Sciences, circadian rhythms are physical, mental and behavioral changes that follow a 24-h cycle. 7 The circadian rhythm could act on many physiological activities including food intake, hormonal secretions and the alternation of vigilance and sleep. 8
According to the literature, abnormal sleep patterns can lead to immunological problems, metabolic syndrome, sleep disorders, cardiovascular disease, and depression. 9 The night worker should therefore be able to benefit from special medical supervision. Indeed, this monitoring allows the occupational physician to assess the consequences of night work on the health and safety of the night worker and to anticipate the possible repercussions on his quality of life.
In this context, we conducted a survey of employees working at night in two companies in the industrial region of Ben Arous, Tunisia: an electronic company and an automotive company to assess the impact of night work on the sleep, mood and quality of life of employees concerned by night work.
Methods
Study type and conception
This was a cross-sectional and descriptive study carried out between January and October 2023 among employees working at night in two companies in the governorate of Ben Arous, Tunisia: an electronic and automotive devices company, respectively. The study focuses on this region of Tunisia due to its growing industrial sector and the rising prevalence of night shifts, particularly in the automotive and electronics industries. These sectors are relevant as they often require continuous production and shift work.
Data collection was based on a self-administered questionnaire (Appendix A) including socio-demographic, occupational and medical characteristics.
Population of the study
Employees who had worked at night for at least one year in the two companies and who agreed to answer the questionnaire, were included in the study.
Employees working shifts and those with incomplete questionnaire responses were excluded.
Variables
The following data were collected: sociodemographic characteristics (age, gender), occupational characteristics (sector of activity, job position, professional seniority, adaptation period) and medical history. Quality of sleep and quality of life were measured using validated scales. Quality of sleep was assessed by the Spiegel questionnaire. For the quality of life, we used the SF-12 scale (Appendix B). The selection of “quality of sleep” and “quality of life” as key variables is justified by their direct relevance to the well-being of night workers. Quality of sleep is critical because inadequate sleep can lead to various health issues, including fatigue and decreased cognitive function, particularly affecting those working nontraditional hours. Similarly, quality of life encompasses broader aspects of well-being, including physical, emotional, and social health, making it essential for understanding the overall impact of night work.
Mood disorders such as anxiety and depression were also assessed using the HAD (Hospital Anxiety and Depression scale) (Appendix B).
Measurement tools
Body mass index BMI was used to distribute the population overweight (BMI between 25–30 kg/m2), obese (BMI greater than 30 kg/m2), or normal BMI (BMI less than 25 kg/m2).
Sleep quality was assessed by the Spiegel questionnaire (Appendix B) validated in French which includes six questions relating to the time of falling asleep, sleep quality, sleep duration, nocturnal awakenings and dreams in order to obtain a total score of 30 points.10–12
Sleep quality was classified as normal when it is between 24 and 30 points, disturbed when it was between 15 and 23 points, and pathological when it was less than 15 points.
Mood disorders were measured using the HAD (Hospital Anxiety and Depression scale) (Appendix B) validated in French, 13 allowing to calculate both depression and anxiety scores with thresholds determining three groups: A score less than or equal to 7 corresponded to the absence of an anxious or depressive state, a score between 8 and 10 indicated a doubtful anxious or depressive state, a score greater than or equal to 11 indicated a certain anxious or depressive state.
For the quality of life, we used the SF-12 scale (Appendix B) validated in French. We calculated the following two sub-scores: the Physical Dimension Score (PCS) (by summing the scores of questions 1 to 5 with question 8) and the Mental Dimension Score (MCS) (by adding the scores of questions 7 to 12 except question 8). The PCS and MCS scores are between 0 and 100: 0 represents the worst and 100 the best health. In general, an overall score above 50 indicates a good quality of life, while a score between 40 and 49 indicates a slight impairment, a score between 30 and 39 a moderate impairment, and a score below 30 a severe impairment in quality of life.14–16 The overall SF-12 score is the sum of the two MCS and PCS scores.
Our study employs a quantitative approach as it utilizes a structured survey to gather numerical data on sleep quality, mood, and quality of life among employees working night shifts at two companies in Ben Arous, Tunisia. While there is no comparison group to generalize the findings to a broader population, the focus on measuring specific variables through standardized instruments allows for the identification of patterns and correlations within the surveyed group. This approach provides valuable insights into the experiences of night workers, contributing to the understanding of the impacts of night work on their well-being.
Statistical methods
The data was analyzed using the Software Package for Statistics and Simulation (IBM SPSS version 25). Participant characteristics are described as proportions for categorical variables and means with standard deviations for continuous variables with a normal distribution or median with interquartile range (IQR) for variables not following the normal distribution. The link between two quantitative variables (the SF-12, Spiegel and HAD scores) was studied by the Pearson coefficient, or the Spearman rank correlation coefficient. The correlation coefficient “r” varies from −1 (perfect negative correlation) to +1 (positive correlation) passing through zero (absence of correlation). The difference between two parameters was considered statistically significant when the p-value was less than 0.05.
Ethical considerations
At the time of our study, the information obtained was recorded by the investigator in such a way that the identity of human subjects cannot be easily verified, directly or indirectly through subject-related identifiers. Response to the questionnaire was voluntary.
Results
Socio-demographic characteristics
A total of 199 workers responded to the questionnaire. The mean age was 36, 1 ± 8 years. The most represented age group was (31–40) years in 44.2%. Our population consisted of 175 women (88%) and 24 men (12%) with a sex ratio of 0.13.
Professional characteristics
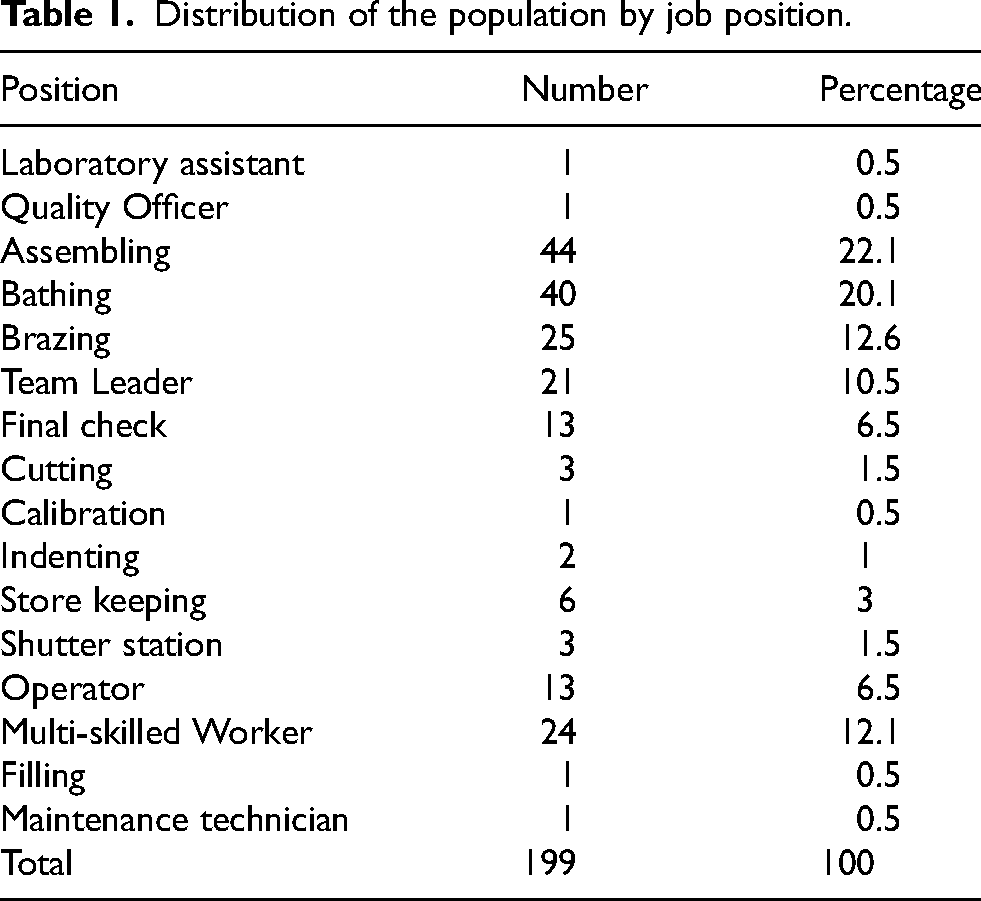
Participants had a median professional seniority of 5 years (IQR: 3–10) with extremes ranging from 1 to 21 years. They worked in the automotive company in 86% and in the electronics company in 14%. They mainly occupied the following positions: assembling (N = 44; 22.1%), bathing (N = 40; 20.1%), brazing (N = 25; 12.6%) and multipurpose workers (N = 24; 12.1%) (Table 1).
Distribution of the population by job position.
The choice of night work was voluntary in 98.5% (N = 196) and, imposed in 1.5% of cases. Median seniority in night work was 3 years (IQR: 2–5) with extremes ranging from 6 months to 20 years. This seniority was less than or equal to 5 years in 74.9% of cases (Figure 1). Our respondents benefited from a period of adaptation to night work in 85.4% (N = 170).
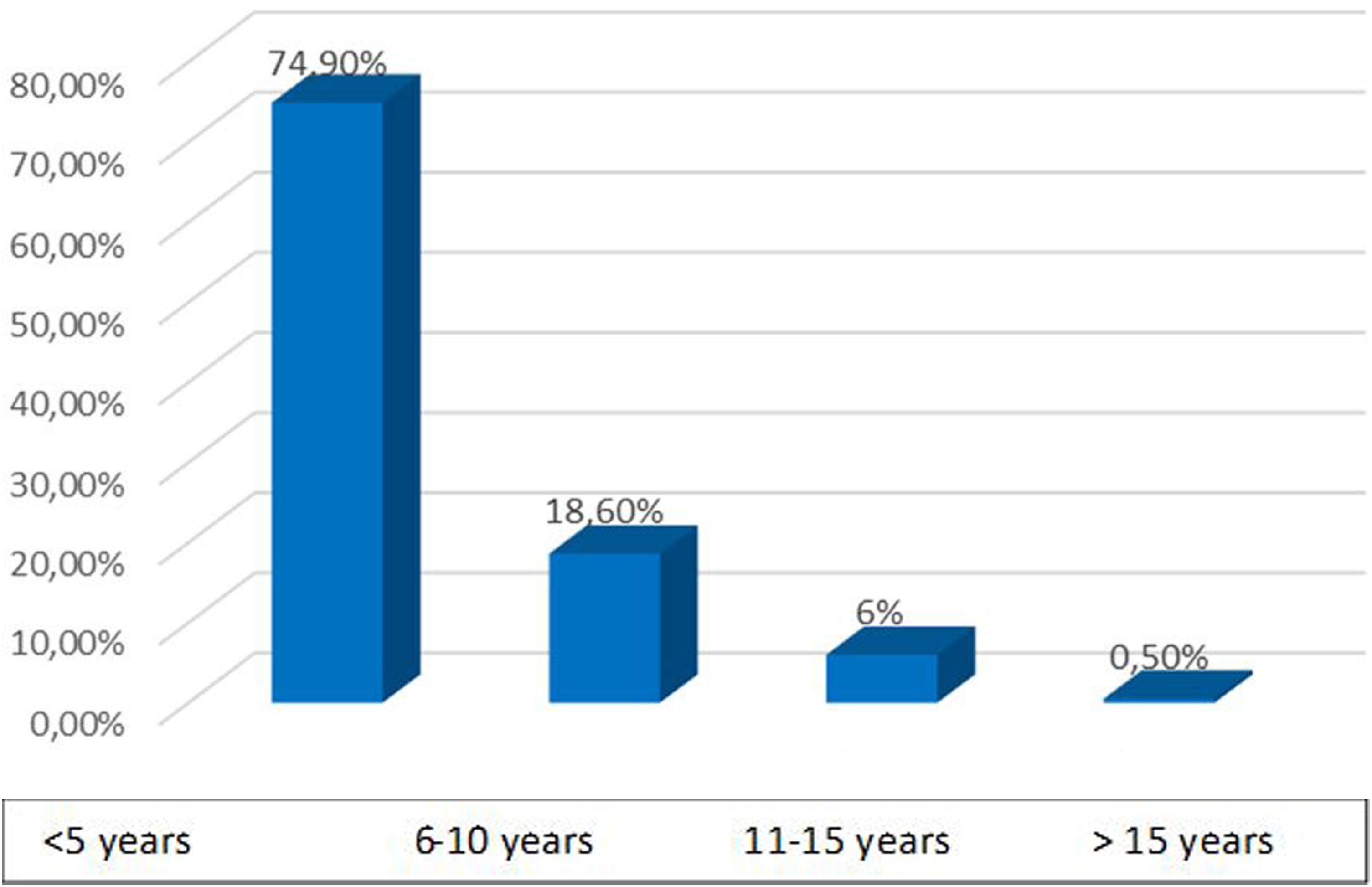
Distribution of the population by length of service in night work (in years).
Medical characteristics of the population
Our participants reported being smokers in 11.6% (N = 23), and alcohol consumers in 2% (N = 4) of cases. A pathological medical history before hiring was found in 11.6% of cases (N = 23) represented mainly by hypertension (N = 5), asthma and rhinitis (N = 3 for each), and primary sterility (N = 3). The medication intake was noted in 8.5% (N = 17). Regular physical activity was reported in 37 cases (18.6%). We found BMI overweight in 39.7% (N = 79) and obesity in 29.1% (N = 58) of cases.
Impact of night work on employees
Effects on dietary patterns
Our participants reported eating on a fixed schedule in 34.2% of cases (N = 68).
Regarding the nature of food, they reported consuming soft drinks in 60.3% (N = 120), coffees in 61.8% (N = 123), treats in 63.8% (N = 127), fruits and vegetables in 84.9% (N = 169).
Diseases diagnosed after hiring
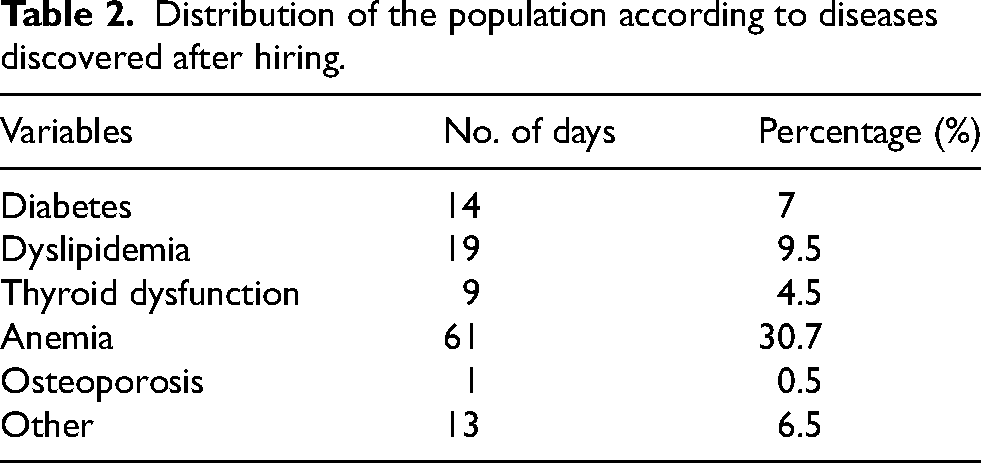
The diseases diagnosed after hiring were mainly: anemia (30.7%), dyslipidemia (9.5%), diabetes (7%) and, thyroid dysfunction (4.5%) (Table 2).
Distribution of the population according to diseases discovered after hiring.
Impact of night work on sleep
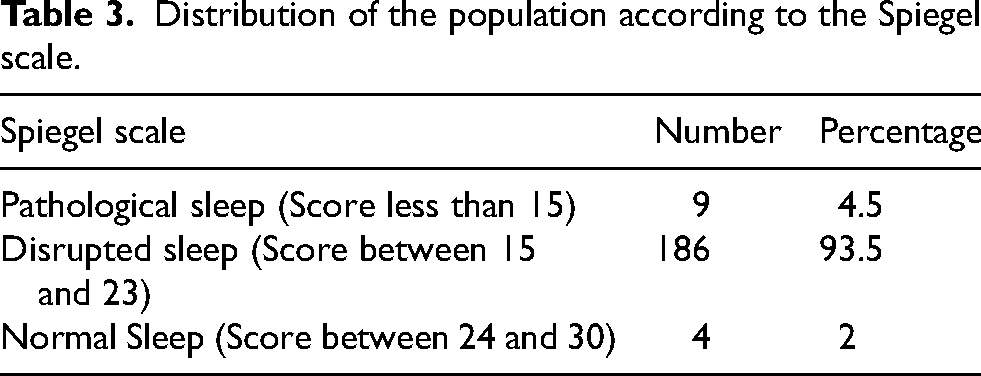
The Spiegel median score was 20 (IQR: 19–21) with extremes ranging from 10 to 26. By identifying the three subclasses of the Spiegel score, night workers showed signs of pathological sleep (N = 4; 4.5%) and disturbed sleep (N = 186; 93.5%) (Table 3).
Distribution of the population according to the Spiegel scale.
We found a delayed sleep onset in 53.3% (N = 106), impaired sleep quality in 18.1% of cases (N = 36), and frequent awakenings in 60.3% (N = 120) with dreams in 40.2% (N = 80).
Impact of night work on mood
The median HAD score was 16 (IQR: 13–20) with extremes ranging from 2 to 32. By identifying the two dimensions of the HAD score, night workers showed signs of definite anxiety (HAD-A score greater than 11) in 10.6% of cases (N = 21). Definite depression (HAD-D score greater than 11) was found in 32.2% (N = 64). The median HAD scores for anxiety and depression were 7 (IQR: 5–9) and 9 (IQR: 7–11), respectively (Figure 2).
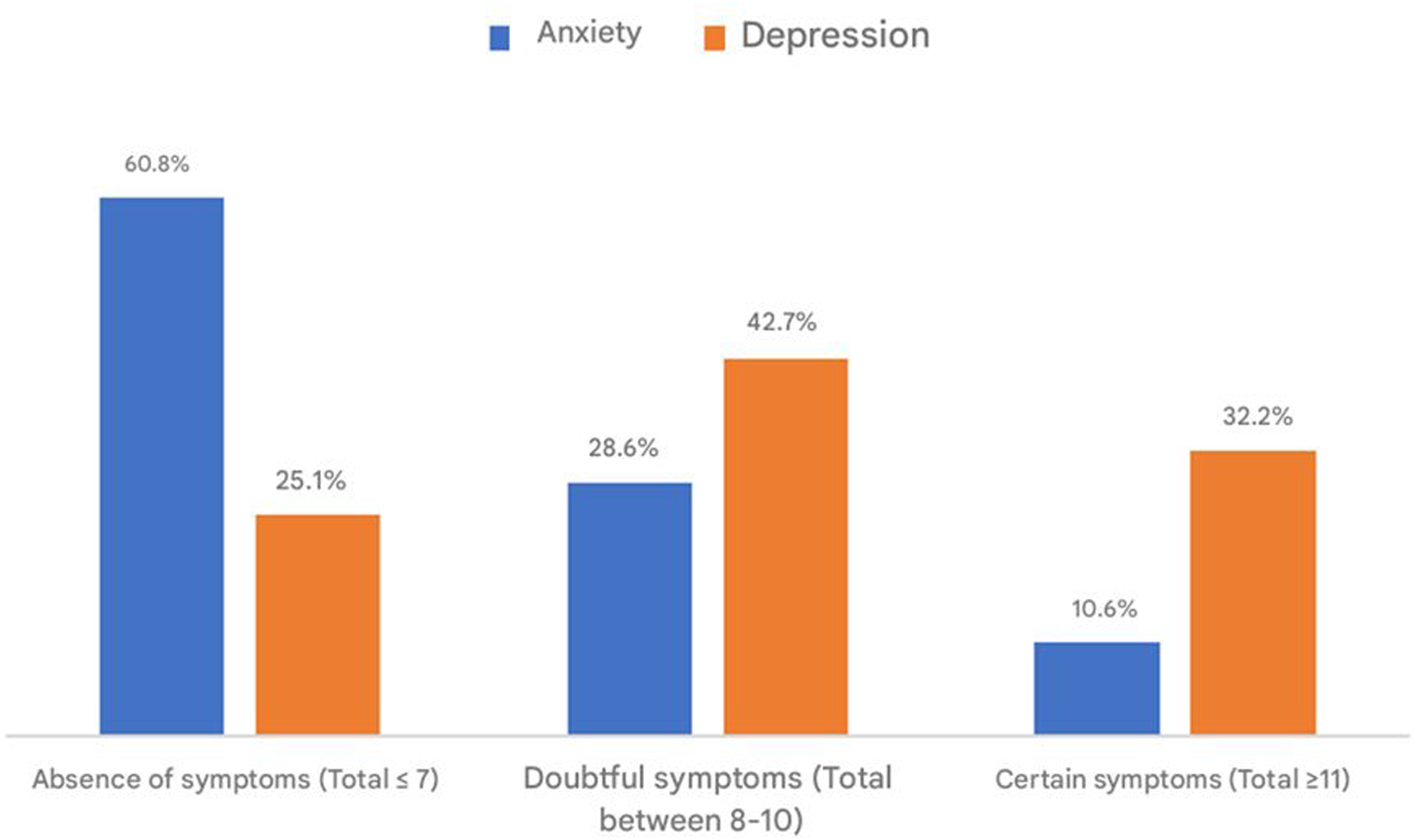
Distribution of the population according to the results of the HAD scale.
Impact of night work on quality of life
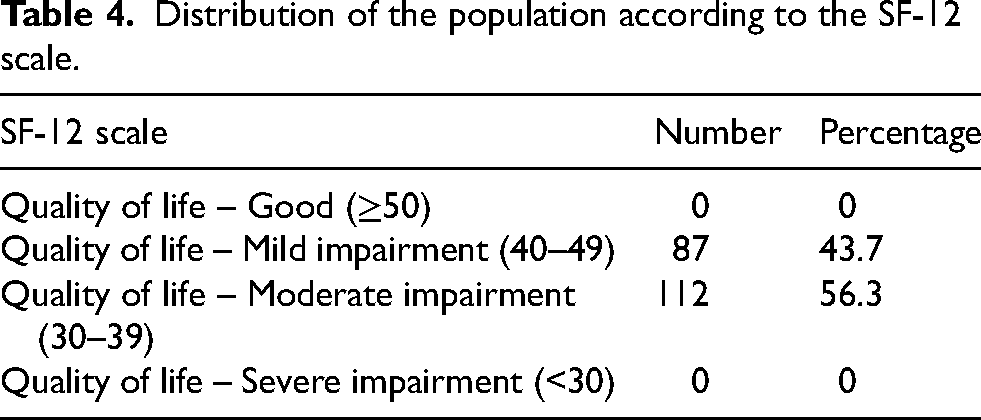
The median overall score on the SF-12 scale was 39 (IQR: 37–41). The median PCS was 17 (IQR: 16–18). The median MCS score was 22 (IQR: 20–23). The overall quality of life was slightly impaired (overall score between 40 and 50) in 43.7%, and moderately impaired in 56.3% of cases (Table 4).
Distribution of the population according to the SF-12 scale.
Analytic study
Quality of life and quality of sleep
In the analytical study, a positive correlation was found between the overall score of SF-12 and the Spiegel score with a statistically significant link (p < 10−3). The correlation coefficient (r) was 0.164 (Figure 3).
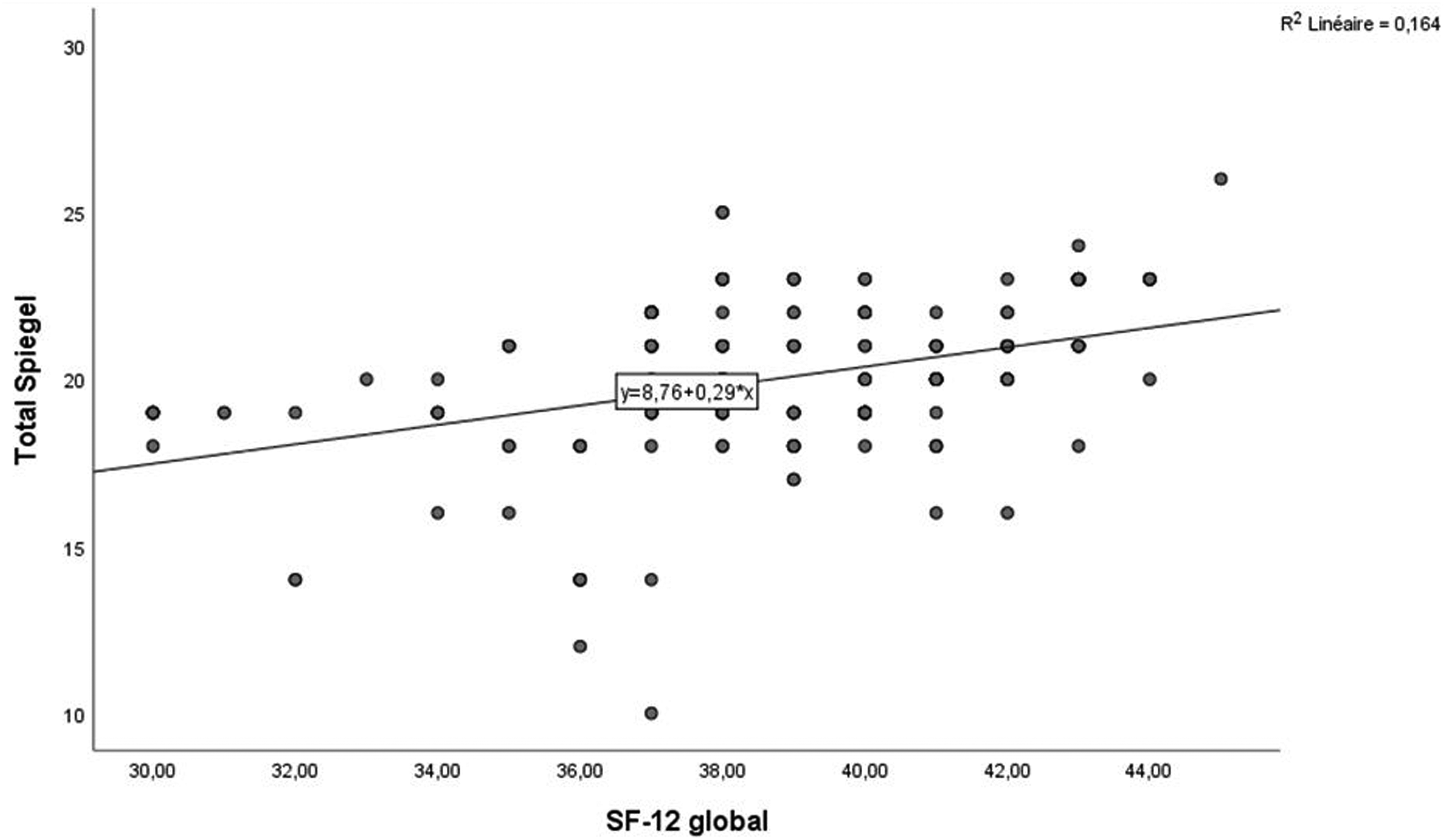
Correlation between SF-12 score and Spiegel score.
Quality of life and mood disorders
A negative correlation was found between the SF-12 score and the HAD total score with a statistically significant relationship (p < 10−3). The correlation coefficient (r) was 0.164 (Figure 4).
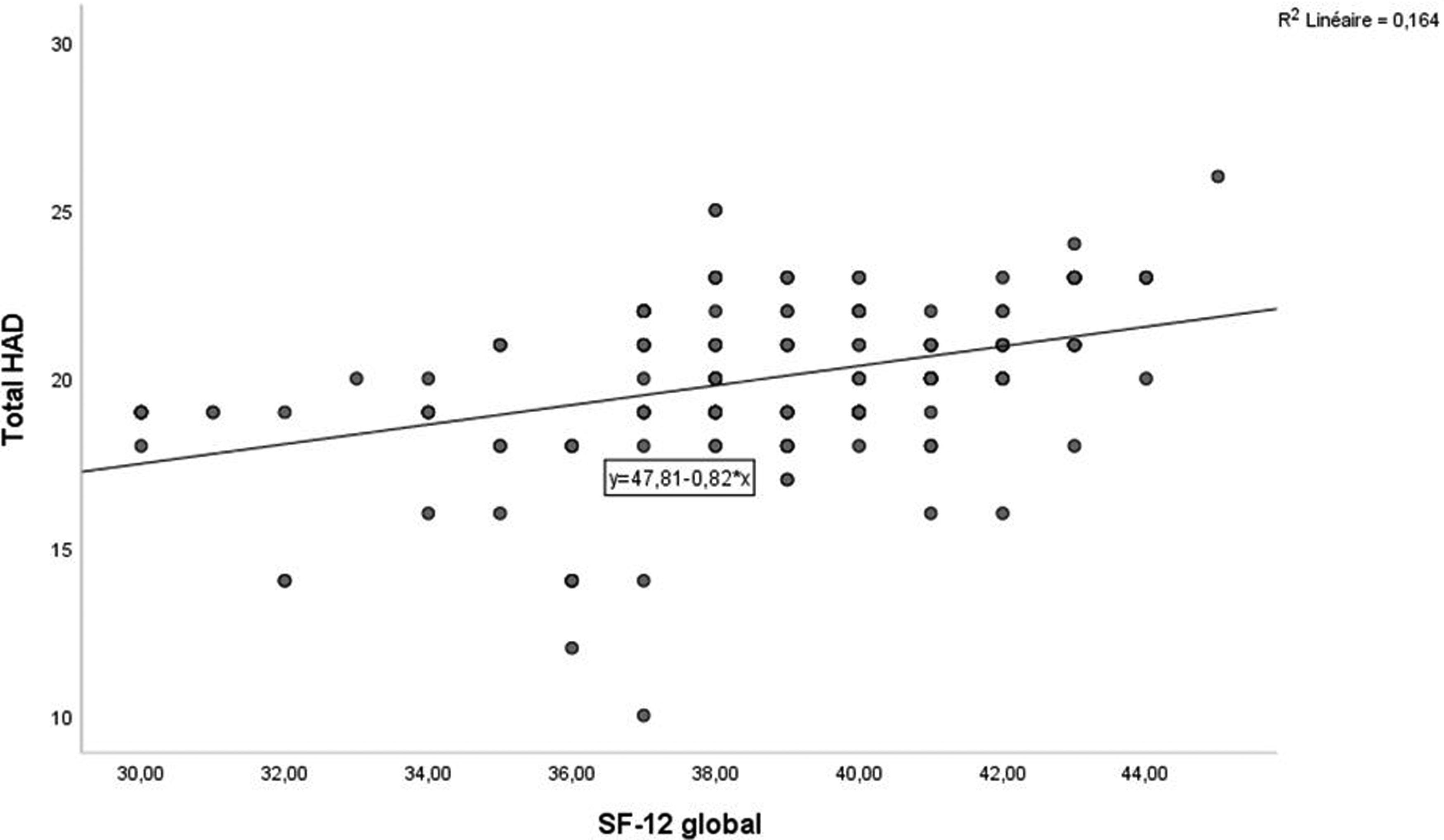
Correlation between SF-12 score and HAD total score.
Sleep quality and mood disorders
A negative correlation was found between the Spiegel score and the HAD total score with a statistically significant link (p = 0.001). The correlation coefficient (r) was 0.058 (Figure 5).
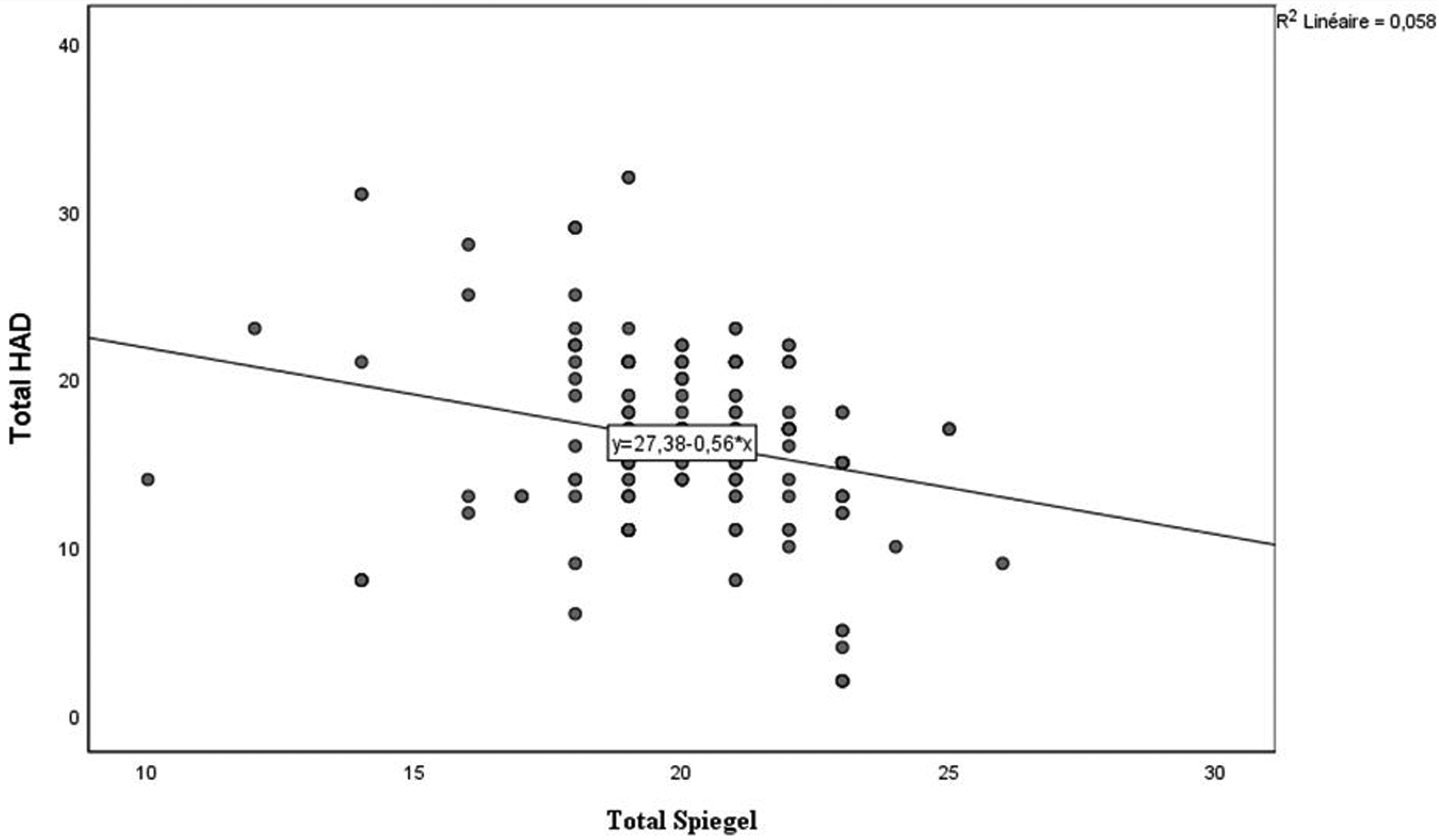
Correlation between the Spiegel score and the HAD total score.
In our analytical study, a positive correlation was found between quality of life and quality of sleep (r: 0.164; p < 10-3). A negative correlation was found between quality of life and mood disorders (r: 0.164; p < 10-3) and also between sleep quality and mood disorders (r: 0.058; p = 0.001).
Discussion
Atypical working hours and particularly night work is beneficial but sometimes necessary for the operation of certain companies and sectors. Indeed, industrialized societies have become increasingly dependent on it. 17
Our study allowed us to assess the repercussions of night work, in particular on the quality of life, mood, sleep and the onset of certain diseases among workers of two large companies in the Ben Arous industrial zone, Tunisia. This study was based on a self-questionnaire collecting socio-demographic, professional and medical characteristics with three valid scales in French, namely SF-12 for quality of life, HAD for screening for anxiety and depression and the Spiegel scale for sleep quality.
Our sample consisted of 199 employees working at night, and had a clear female predominance (88%) with a sex ratio of 0.13. The average age of workers was 36.1 years. Our employees worked in an electronics industry in 86% and 14% worked in an automotive devices manufactory. Participants had a median occupational seniority of 5 years (IQR: 3–10) with extremes ranging from 1 to 21 years. The median length of service in night work was 3 years. The choice of night work was voluntary in the vast majority of cases (98.5%). An adaptation period was respected to assess the initial tolerance to this unconventional schedule in 85.4%.
Night work was imposed and even necessary for certain sectors such as the security sector, health or telecommunications. 18 For economic reasons, some companies in other sectors cannot even remove it. 13 However, it is well known that this atypical work schedule is a nuisance for employees and can even cause them premature wear and tear. 19
In our sample, 11.6% of employees had a chronic disease at hiring including hypertension (N = 5; 2.5%), asthma and rhinitis (N = 3 for each; 1.5%), and primary infertility (N = 3; 1.5%) and diabetes (N = 2; 1%). After a few years of night work, we noticed the appearance of diseases discovered after hiring with modification of the epidemiological profile: 7% of diabetes, 7.5% of dyslipidemia and 4.5% of thyroid dysfunction, and mainly anemia 30.7%. We noted an overweight in 40% of cases and an obesity in 29% of cases.
Eating habits were marked by fixed food intake in 34% of cases, soft drink consumption in 60% of cases, coffee drinking in 62% and, treats in 64% of cases. As for physical activity, it was present in 18% of cases. As for habits, 11.5% of employees were smokers and 2% alcoholic.
Our study suggests metabolic changes that are known effects of night work as well as shift work, already shown by several experimental studies. Indeed, sleep deprivation even over a few days was associated with significant weight gain and the conclusions of the ANSES report with SFRMS consensus group affirmed a probable risk of obesity, type 2 diabetes and a proven risk of metabolic syndrome. 3 The correlation between sleep deprivation and weight gain has been the subject of several studies such as the study by Spiegel et al. carried out in 2004, mainly by increasing the desire for caloric foods and snacking. 20
Moreover, no cases of cancer were detected in our study, although this risk was well elucidated in the literature particularly the risk of breast cancer in women that increased with the accumulation of years of night work, 21 and caused by the disruption of the circadian rhythm and the fall in melatonin levels. 22 Moreover, the IARC had classified night work and shift work as group 2A probable carcinogens because they probably involve circadian disorganization. 23
We assessed the impact of night work on the quality of life, sleep and mood of employees, using the SF-12, Spiegel and HAD scores respectively.
We found that overall quality of life (physical and mental) assessed by SF-12 was slightly impaired in 43.7% and, moderately impaired in 56.3% of cases. Indeed, several repercussions of night work on the employees have been described in the literature. Thus, there is an increase in fatigability, nervousness and irritability, as well as chronic sleep deprivation, deteriorating social life and collective responsibilities, as demonstrated by a study on night workers of hospital staff in Sousse in 2004. 18
For the impact on sleep quality (assessed by the Spiegel score), 4.5% of employees showed pathological sleep signs and 93.5% showed signs of disturbed sleep. Night workers are usually in chronic sleep debt leading to harmful consequences such as profound drowsiness, cognitive slowing, attention lapses and other effects. 24
The HAD scale assessing the impact of night work on the mood of employees allowed us to note signs of certain anxiety in 10.6% and depression in 32.2% of cases. These effects would probably be related to the atypical schedule of work on mental health. This work organization is commonly accepted as a provider of stress, chronic fatigue and would also be responsible for an increased risk of depressive pathology more than anxiety. 8
In our analytical study, a positive correlation was found between quality of life and quality of sleep (r: 0.164; p < 10-3). A negative correlation was found between quality of life and mood disorders (r: 0.164; p < 10-3) and also between sleep quality and mood disorders (r: 0.058; p = 0.001). The correlation coefficient (e.g., r = 0.164) indicates a weak positive correlation between two variables, suggesting that as one variable (e.g., quality of life) increases, the other variable (e.g., sleep quality) tends to increase as well. Despite its weakness, this correlation can be meaningful in the context of well-being, as even small improvements in sleep quality can lead to noticeable enhancements in overall health, such as increased energy levels, better mood, and improved productivity. Over time, these minor positive changes can accumulate, resulting in significant benefits, particularly for individuals in high-stress environments like night work. Thus, our findings underscore the potential for targeted interventions to improve sleep quality and, consequently, overall quality of life.
In a study by Lim et al. comparing night workers to a group not working at night, sleep quality partly explained the association between night work and deteriorating quality of life. 25 In another Chinese study, night work, shift frequency, and sleep disturbance were associated with an increased risk of depression among workers. A subsequent mediation analysis found that the association between night work and depression appeared to be partially mediated by sleep disorders. 26 In a Tunisian study, depression was associated with sleep quality (p = 0.01) among healthcare workers with atypical schedules. These schedules generate sleep and mood disorders according to this study. 27
Our study, which involved 199 employees working at night on a fixed schedule for an average of 3 years in two different industries: one in the electronics sector and the other in the automotive parts manufacturing sector, has strong points. It made it possible to determine the frequency of the repercussions of night work on sleep, mood, and quality of life. The main strength of this study is its real-world evaluation of the long-term effects of fixed night shift work in two industrial sectors in Tunisia's largest industrial zone. By assessing 199 employees over an average of three years, it provides valuable insight into the impact of night work on sleep, mood, and quality of life under actual working conditions. The choice of scales was based on their validity and reliability in order to avoid overestimating the frequency of these disorders. Thus, we found pathological sleep quality in 4.5% and disturbed in 93.5% of cases. Anxiety and depression were certain in 10.6% and 32.2% of cases respectively. The overall quality of life was slightly impaired in 43.7%, and moderately impaired in 56.3% of cases. In the analytical study, a positive correlation was found between quality of life and quality of sleep (r: 0.164; p < 10-3). A negative correlation was found between quality of life and mood disorders (r: 0.164; p < 10-3) and also between sleep quality and mood disorders (r: 0.058; p = 0.001).
The literature review reveals a range of occupational health strategies that have been employed to mitigate the adverse effects of night work. These strategies can be broadly categorized into three main approaches: health assessments and monitoring, personalized interventions, and organizational and policy changes. Our study was based on health assessments and monitoring. Health assessments and monitoring are cornerstone strategies in managing the health risks associated with night work. Occupational physicians play a critical role in conducting regular health checks, which include medical history, physical examinations, and blood tests. 28 These assessments are essential for identifying early signs of health problems such as sleep disorders, cardiovascular diseases, and mental health issues, which are commonly associated with night work. 4
In addition to traditional health assessments, recent studies have emphasized the use of innovative tools such as sleep questionnaires, actigraphy, and biomarker measurements to monitor the health of night workers more effectively. 29 In our study, we used validated questionnaire in their French version, comprehensible by all participants.
However, some limitations of this study deserve to be highlighted, related in particular to the cross-sectional nature of the study. Therefore, the causal link between night work and the various studied factors cannot be formally established. In addition, our study only concerned workers from the two electronics and automotive companies who agreed to participate, thus not considering other sectors and occupational exposures that may interfere with the effects of night work. The inclusion of night workers alone certainly constitutes a selection bias that does not allow the generalization of our results. We cannot incorporate comparative analysis at this stage, but we propose that future research include this aspect to enhance the understanding of night work's impact. By comparing the findings to data from populations working regular shifts or national averages, subsequent studies could provide a clearer context for interpreting the effects on sleep quality and overall well-being. This approach would allow for more robust conclusions and better inform workplace policies aimed at supporting night workers.
Further multi-centre studies would be needed to verify our results across different industry sectors and work schedules to be able to compare results on a wider scale.
Conclusions
The main strength of our study is its real-world evaluation of the long-term effects of fixed night shift work in two industrial sectors in Tunisia's largest industrial zone. By assessing 199 employees over an average of three years, it provides valuable insight into the impact of night work on sleep, mood, and quality of life under actual working conditions. Our study highlighted the harmful effects of night work on employees’ sleep quality, mood and quality of life. Faced with these nuisances, the role of the occupational physician is important in ensuring better adaptation to night work, following an assessment of working conditions and the implementation of measures to protect workers’ health. These assessments are essential for identifying early signs of health problems such as sleep disorders, cardiovascular diseases, and mental health issues, which are commonly associated with night work.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Ethical considerations
Not Applicable.
Informed consent
Participants were informed of the objectives of the study. We obtained their consent. The anonymity of the respondents was respected.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.