
Abstract
Background
Waist and back pain are common among healthcare professionals in labor and delivery units due to physical demands and psychological workload. Massage may alleviate symptoms; however, manual massage often lacks feasibility. Automated massage devices may offer an alternative, but evidence among healthcare professionals is limited.
Objective
This study aimed to examine within-group changes in pain, perceived stress, state anxiety, fatigue, and psychological well-being among healthcare professionals following an automated massage application.
Methods
This single-group pretest–posttest quasi-experimental study was conducted with 35 healthcare professionals working in the delivery room of a state hospital. Participants used an automated massage device applied to the waist and back regions during routine break periods for two weeks. Data were collected using the Visual Analogue Scale for pain, the Perceived Stress Scale, the State Anxiety subscale of the State–Trait Anxiety Inventory, the Piper Fatigue Scale, and the Psychological Well-Being Scale. Pretest–posttest comparisons were performed using paired-samples t tests or Wilcoxon signed-rank tests, as appropriate.
Results
Statistically significant within-group reductions were observed in pain, perceived stress, state anxiety, and fatigue scores following the intervention (p < .001). Psychological well-being scores showed a statistically significant increase after the intervention period (p < .001).
Conclusions
In this single-group study, automated massage use was associated with favorable short-term changes in pain, stress, anxiety, fatigue, and psychological well-being among healthcare professionals working in a labor and delivery setting. Further controlled studies with larger samples and longer follow-up periods are needed to confirm these results.
Introduction
Promoting safe and healthy working environments is a key priority emphasized in the United Nations Sustainable Development Goal 8.8, which highlights the importance of protecting workers’ physical and mental well-being. The working environment is a multifaceted concept influenced by physical, psychological, and psychosocial factors, all of which may interact and shape workers’ exposure to occupational risks. 1 Understanding these interrelated dimensions is essential for identifying conditions that may adversely affect health and well-being in the workplace.
Healthcare professionals are among the occupational groups frequently exposed to demanding physical and psychological working conditions. Previous studies have reported that waist and back pain are more prevalent among healthcare professionals compared to many other professions.2,3 In a recent scoping review, Rossetto et al. examined musculoskeletal disorders among healthcare workers and noted that work-related musculoskeletal conditions represent a significant occupational health concern due to their substantial impact on individuals’ quality of life and functional capacity. 2 These findings underscore the relevance of addressing musculoskeletal health within healthcare settings.
Increased workload, insufficient organizational support, and frequent lifting or carrying tasks have been associated with waist and back pain, stress, fatigue, and psychological strain among healthcare professionals. 4 In labor and delivery units in particular, healthcare professionals often work in confined spaces and are required to adopt sudden or prolonged non-neutral postures while managing deliveries, which may contribute to musculoskeletal discomfort, especially in the waist and back regions. 5 Previous research has reported a high prevalence of musculoskeletal pain among obstetrics and gynecology staff. 6 Similarly, studies focusing on midwives have identified waist pain (80.7%) and back pain (71.6%) as the most commonly reported musculoskeletal complaints. 7
The limited availability of easily accessible and practical supportive interventions for managing such pain among healthcare professionals may be associated with adverse physical and psychological outcomes. These may include increased stress and fatigue, reduced work capacity, diminished professional quality of life, and psychological distress, potentially contributing to workforce attrition over time.6,8 A systematic review examining workplace interventions in hospital settings reported substantial heterogeneity in intervention approaches, including ergonomic education, practical ergonomic modifications, stress reduction strategies, workstation redesign, administrative adjustments, and the use of lift equipment and minimum-lift policies. 1 These findings indicate that while various strategies have been explored, the need for feasible and easily implementable supportive interventions in demanding clinical environments remains.
Massage is commonly used as a supportive approach for managing waist and back pain. Previous studies examining manual massage interventions have reported reductions in general pain and perceived stress among nurses.9,10 Although manual massage may be administered by trained practitioners or performed individually, its routine use in clinical settings is often limited by time constraints and the need for additional labor. Consequently, the use of technological and innovative massage devices has been suggested as a potentially more feasible and sustainable alternative.
The existing literature includes a limited number of studies investigating automated massage interventions among healthcare professionals. These studies reported reductions in stress 11 and anxiety 12 among healthcare workers who received short-duration (10–20 min) general body massage using automated massage chairs in specially designed relaxation rooms incorporating environmental elements such as color, scent, and music. However, these interventions primarily focused on whole-body relaxation rather than targeting specific anatomical regions associated with occupational pain.
In contrast to previous studies, the present study applied automated massage during rest periods specifically to the waist and back regions, which are commonly reported as primary sites of pain among healthcare professionals. In addition to pain, fatigue and psychological well-being were also assessed. The automated massage device used in this study was portable and designed for use on targeted body areas without requiring additional personnel or extensive time resources. These characteristics may enhance the practical applicability of the intervention in busy clinical environments.
The aim of this study was to examine changes in pain, fatigue, perceived stress, state anxiety, and psychological well-being among healthcare professionals working in a delivery room following an automated massage application
The hypotheses of the study were formulated to examine within-group changes following the automated massage application:
Methods
Study design
This study was conducted to examine changes in pain, stress, anxiety, fatigue, and psychological well-being levels of healthcare professionals following an automated massage application. A single-group pretest–posttest quasi-experimental design without a control group was employed. Outcome variables were measured before and after the intervention to evaluate changes over time within the same group.
Participants
The study participants consisted of healthcare professionals working in the delivery room of a state hospital located in a province in Turkey. Data collection was conducted in the healthcare professionals’ break rooms within the delivery unit between July 30, 2024, and September 20, 2024.
The study population included all healthcare professionals (midwives, nurses, and physicians) employed in the delivery room during the study period. At the time of the study, a total of 37 healthcare professionals were working in the unit, including 27 midwives, two nurses, and eight physicians. One midwife and one physician were excluded because they were on leave during the data collection period. Consequently, the final sample consisted of 35 healthcare professionals, including 26 midwives, two nurses, and seven physicians.
Inclusion criteria
Healthcare professionals working in the delivery room who voluntarily agreed to participate in the study were eligible for inclusion.
Exclusion criteria
Healthcare professionals were excluded if they worked in units other than the delivery room; had waist or back pain due to known pathological conditions; had any medical condition contraindicating massage to the waist or back region; or were receiving psychiatric treatment at the time of the study.
Data collection tools
Personal Information Form: The Personal Information Form was developed by the researchers based on the relevant literature.10–12 The form consisted of 14 items designed to collect data on participants’ sociodemographic characteristics and occupational features.
Visual Analog Scale (VAS): Pain intensity was assessed using the VAS, a widely used and reliable instrument for measuring current pain severity. The scale consists of a 10-cm horizontal line, with one end indicating “no pain” (0) and the other indicating “worst possible pain” (10). Participants were asked to mark the point on the line that best represented their perceived pain intensity. Pain severity was calculated by measuring the distance (in centimeters) from the “no pain” anchor to the marked point. 13
Perceived Stress Scale (PSS-14): Perceived stress was measured using the 14-item PSS developed by Cohen et al.. 14 Items are rated on a five-point Likert scale ranging from 0 (“never”) to 4 (“very often”), with total scores ranging from 0 to 56; higher scores indicate higher perceived stress. The Turkish validity and reliability of the PSS-14 were established by Eskin et al., who reported a Cronbach's alpha coefficient of 0.84. 14
State Anxiety Subscale of the State–Trait Anxiety Inventory (STAI): State anxiety was assessed using the State Anxiety subscale of the STAI, originally developed by Spielberger et al.. 15 The Turkish adaptation of the scale was conducted by Öner and Le Compte.16,17 The subscale consists of 20 items rated on a four-point Likert scale, with both direct and reverse-scored items. Total scores range from 20 to 80, with higher scores indicating higher levels of state anxiety. The Cronbach's alpha coefficient for the Turkish version has been reported to range between 0.83 and 0.92. 14
Piper Fatigue Scale: Fatigue was evaluated using the Piper Fatigue Scale, originally developed by Piper et al.. 18 Following revisions, the current version of the scale consists of 22 items rated on a 0–10 VAS. The scale assesses subjective fatigue across four dimensions: behavioral/severity, affective meaning, sensory, and cognitive/mood. Higher scores indicate greater levels of perceived fatigue.
Psychological Well-Being Scale: Psychological well-being was measured using the Psychological Well-Being Scale developed by Diener et al., 19 which was adapted into Turkish by Telef. 20 The scale includes eight items rated on a seven-point Likert scale, with total scores ranging from 8 to 56; higher scores reflect higher levels of psychological well-being.
Satisfaction Assessment Form: Participants’ satisfaction with the automated massage application was assessed using a brief Satisfaction Assessment Form developed by the researchers.8,10 The form included items evaluating overall satisfaction with the intervention, willingness to use the application again, and likelihood of recommending it to others. Content validity was established through expert review by four faculty members and three midwives specializing in midwifery, gynecology, and obstetrics nursing.
Data collection
Pretest data were collected prior to the intervention after participants were informed about the study and written informed consent was obtained. The automated massage application was implemented during participants’ routine break periods while working in the hospital.
The intervention was administered during the 4th to 6th working hours of the shift, a period reported by participants as associated with increased fatigue. Each participant used the automated massager for a total of 20 min per session, consisting of 10 min applied to the waist region and 10 min applied to the back region. The application was performed five days per week over a two-week period.
Participants were allowed to use the automated massage device in their preferred rest areas within the delivery unit. Prior to the initiation of the intervention period, all participants were provided with instruction and demonstration regarding the correct use of the massager while seated on a chair or armchair.
All participants received the massage in a 90-degree seated position, thereby ensuring a consistent distribution of body weight and a uniform contact angle. During the application, the researcher was present in the unit and available to provide assistance if needed; however, no manual intervention or individualized adjustment of massage settings was performed beyond ensuring safe and appropriate use.
Posttest data were collected after completion of the two-week intervention period using the same measurement instruments administered at baseline. The automated massage device used in the study was portable and designed for application to the waist and back regions.
Data analysis
Data were analyzed using IBM SPSS Statistics for Windows, version 27. Descriptive statistics, including minimum and maximum values, means, and standard deviations, were used to summarize the data. Pretest–posttest comparisons were conducted using within-group statistical analyses. Paired-samples t tests were applied for variables with normally distributed pretest–posttest difference scores, whereas the Wilcoxon signed-rank test was used for variables that did not meet the normality assumption.
Normality was primarily assessed based on the distribution of pretest–posttest difference scores using the Shapiro–Wilk test, with skewness and kurtosis values examined as supportive indicators. Internal consistency of the measurement instruments was evaluated using Cronbach's alpha coefficient. The level of statistical significance was set at p < .05.
A sensitivity analysis was conducted using G*Power for the primary outcome (Pain VAS) with a paired-samples design. With a total sample size of 35, a two-tailed significance level of α = .05, and 80% power, the minimum detectable standardized mean difference was d_z = 0.49, corresponding to a moderate effect size.
Ethics approval and consent to participate
Ethics committee approval was obtained from the Health Sciences Research Ethics Committee (Ethics committee date: 04/07/2024, ethics no: E.181712) of XXX University. This study was conducted in accordance with the principles of the Declaration of Helsinki, and all patients provided informed consent prior to enrollment. The questionnaire form stated that the participants’ identity would be kept confidential and that participation was on a voluntary basis. After the healthcare professionals who agreed to participate in the study were informed about the purpose and scope of the study, their verbal and written consents were obtained.
Results
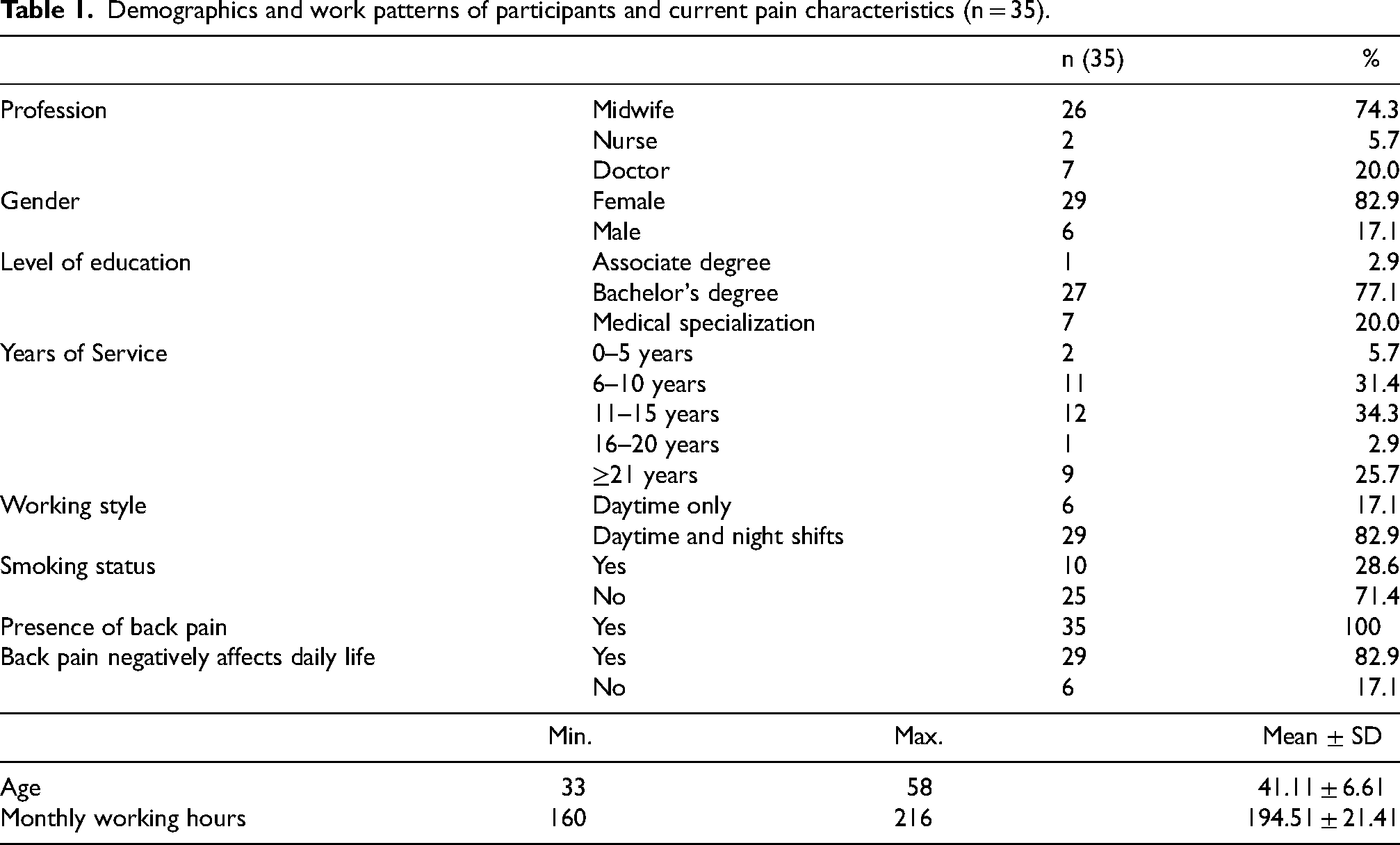
Table 1 presents the demographic characteristics, work patterns, and back and waist pain related findings of the participants. The majority of participants were midwives (74.3%), followed by doctors (20.0%) and nurses (5.7%). Most participants worked both daytime and night shifts (82.9%). All participants reported experiencing waist and back pain, and 82.9% indicated that the pain negatively affected their daily lives.
Demographics and work patterns of participants and current pain characteristics (n = 35).
Within-group comparisons of pain, state anxiety, and fatigue scores are presented in Table 2. The mean VAS pain score decreased from 9.69 ± 0.72 at pretest to 6.06 ± 1.85 at posttest, and this change was statistically significant (t(34) = 11.42, p < .001). Similarly, the mean State Anxiety score measured by the STAI decreased significantly from 49.11 ± 3.31 at pretest to 44.00 ± 3.29 at posttest (t(34) = 12.43, p < .001). The mean Piper Fatigue Scale score also showed a statistically significant reduction, decreasing from 7.30 ± 0.78 before the intervention to 6.68 ± 0.66 after the intervention (t(34) = 7.28, p < .001).
Within-Group comparisons of pain, state anxiety, and fatigue scores using paired-samples t test (n = 35).

Note. t = paired-samples t test. All comparisons represent within-group pretest–posttest analyses.
Table 3 presents within-group comparisons of perceived stress and psychological well-being scores using the Wilcoxon signed-rank test. The (PSS-14) scores decreased significantly from a pretest mean of 46.26 ± 5.76 to a posttest mean of 43.70 ± 5.31 (Z = −4.29, p < .001). In contrast, Psychological Well-Being Scale scores increased significantly from 33.54 ± 9.11 at pretest to 35.89 ± 7.20 at posttest (Z = 3.85, p < .001).
Within-Group comparisons of perceived stress and psychological well-being scores using Wilcoxon signed-rank test (n = 35).

Note. Z = Wilcoxon signed-rank test. All comparisons represent within-group pretest–posttest analyses.
Participants’ satisfaction with the automated massage application was also evaluated. As all participants provided identical responses, no statistical comparisons were conducted. All participants (100%) reported being satisfied with the automated massage, indicated that they would be willing to use it again, and stated that they would recommend it to others.
Discussion
This study examined within-group changes in pain, perceived stress, state anxiety, fatigue, and psychological well-being among healthcare professionals following an automated massage application. The pretest–posttest comparisons indicated statistically significant reductions in pain, stress, anxiety, and fatigue scores, along with an increase in psychological well-being scores after the intervention period. Given the single-group design, these findings should be interpreted as associations observed over time rather than causal effects.
At baseline, all healthcare professionals working in the delivery room reported experiencing waist and back pain, and the majority indicated that this pain negatively affected their daily lives. These findings are consistent with previous studies reporting a high prevalence of musculoskeletal pain among midwives and obstetric healthcare staff. Prior research has shown that waist and back pain are among the most common musculoskeletal complaints in these occupational groups.3,6,7 The present findings align with the existing literature, highlighting the substantial physical burden experienced by healthcare professionals working in labor and delivery settings.
Reductions in pain intensity observed in this study are consistent with findings from previous research on massage-based interventions. Although studies specifically examining automated massage devices are limited, earlier research has demonstrated that manual massage may contribute to reductions in musculoskeletal pain among healthcare professionals and other physically demanding occupational groups.9,21 The current study extends this literature by providing preliminary evidence regarding the potential role of automated massage in similar clinical contexts.
The observed decreases in perceived stress and state anxiety following the intervention are also in line with previous studies evaluating massage-based or relaxation-oriented interventions among healthcare workers. Randomized and non-randomized studies have reported reductions in occupational stress and anxiety levels following manual massage or the use of massage chairs in designated relaxation environments.11,12,22 Although methodological differences limit direct comparisons, the consistency of findings across studies suggests that massage-related interventions may be associated with short-term improvements in psychological outcomes.
Similarly, fatigue levels decreased following the automated massage application in this study. Prior research has reported reductions in fatigue following manual massage interventions in both healthcare and non-healthcare populations, particularly in physically demanding contexts. 23 The present findings are compatible with these reports and suggest that automated massage may be associated with favorable changes in perceived fatigue levels.
An increase in psychological well-being scores was also observed after the intervention period. Previous studies have suggested that massage and relaxation interventions may be associated with improvements in psychological well-being, mood, and mental fatigue. 23 While the mechanisms underlying these associations were not examined in the present study, the findings contribute to the growing body of literature exploring supportive interventions for healthcare professionals’ well-being.
Several strengths of this study should be noted. Standardized and validated measurement instruments were used to assess pain, psychological, and fatigue-related outcomes. In addition, to the best of our knowledge, this study is among the first to explore the use of an automated massage device among healthcare professionals working in a high-intensity delivery room setting. The intervention focused on the waist and back regions, which are commonly reported as areas of discomfort among this population, and was implemented in a real-world clinical environment.
Despite these strengths, the findings should be interpreted in light of the study's limitations, which are discussed in detail in the following section.
Limitations
Several limitations of this study should be acknowledged. First, the sample consisted of a relatively small number of healthcare professionals (n = 35) recruited from a single hospital and a single clinical unit (delivery room). Therefore, the findings cannot be generalized to all healthcare professionals or to different healthcare settings.
Second, the study employed a single-group pretest–posttest design without randomization, a control group, or blinding. As a result, causal inferences cannot be drawn, and the observed changes may have been influenced by uncontrolled factors. In addition, the absence of a control group limits the ability to distinguish intervention-related changes from time-related or contextual effects.
Third, the data were based on self-reported measurement instruments, which may be subject to reporting and response biases. Moreover, the study evaluated only short-term outcomes of the automated massage intervention, and long-term effects were not assessed.
Fourth, the inclusion of multiple outcome measures may have increased the risk of type I error. In addition, no a priori power analysis was conducted, and the study may have been underpowered to detect smaller effects.
Finally, the intervention was implemented in a real-world clinical setting, and although efforts were made to standardize the procedure, individual differences in perception and response to the intervention may have influenced the results.
Given these limitations, the findings should be interpreted as preliminary, and the study should be considered exploratory or pilot in nature. Future research involving larger samples, multicenter designs, randomized controlled methodologies, and longer follow-up periods is recommended to strengthen the evidence base. Qualitative studies may also provide deeper insight into healthcare professionals’ experiences and perceived benefits of automated massage interventions.
Although an a priori power analysis was not performed, a post hoc sensitivity analysis indicated that the study was sufficiently powered to detect moderate within-group changes in the primary outcome; however, smaller effects may not have been detectable.
Conclusion
This study observed favorable short-term changes in pain, perceived stress, state anxiety, fatigue, and psychological well-being among healthcare professionals following the use of an automated massage application. In addition, participants reported high levels of satisfaction with the intervention.
Given the single-group, non-randomized design and the limited sample size, the findings should be interpreted with caution. Rather than demonstrating causal effects, the results suggest that automated massage may represent a feasible and acceptable supportive approach for healthcare professionals working in physically and psychologically demanding clinical environments.
Automated massage devices may offer practical advantages, as they can be used independently without requiring additional personnel or additional time resources. However, conclusions regarding their broader impact on work performance, occupational well-being, or healthcare systems cannot be drawn based on the present study.
Further research employing larger samples, controlled study designs, and longer follow-up periods is warranted to confirm these findings and to better understand the potential role of automated massage as a supportive intervention for healthcare professionals.
Footnotes
Acknowledgments
We would like to thank the health workers who participated.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Osmaniye Korkut Ata University (Ethics committee date: 04/07/2024, ethics no: E.181712).
Informed consent
People who accepted to participate in the study were informed about the study, and their written consent was obtained prior to the study.
Author contributions
Study conception and design: E.Y., S.G.S.; Data collection: E.Y.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing and data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Clinical trial
The trial protocol was registered (NCT06504797).