
Abstract
Background
Physiotherapist is a professional who knows human movement and ergonomics, but can be subject to work-related musculoskeletal disorders (WRMDs).
Objective
To determined WRMDs epidemiology in physiotherapists working in Portugal, describing the most frequent locations, types and mechanisms of injuries, and the associated risk factors.
Methods
The sample was constituted by 1828 physiotherapists, being 1194 (65.3%) female, aged 21–66 years. A questionnaire was used for data collection. Data were analyzed using logistic regression.
Results
WRMDs prevalence throughout professional practice, in the last 48 h and in the 12-month period were, respectively: 54.6%, 15.9%, 38.1%. In the last 12 months, 1294 injuries were measured. The injury proportion was 0.38 (CI95%:1.83–2.59) and injury rate was 0.035 injuries per 1000 h of Physiotherapist practice. The most common WRMDs types were low back pain (375; 32.72%), neck pain (26.35%) and tendinopathy (183;15.97%), most common in the shoulder (124; 67.8%). The most frequent injury mechanisms were repetitive tasks (452; 21.64%) and exhaustion from long hours of work without rest (266; 12.73%). Women were 2.13 (CI95%: 1.71–2.64;p < 0.001) more likely to develop WRMDs, physiotherapists aged 30 years or older were 1.23 (CI95%::1.01–1.50;p = 0.042), those who practiced physical exercise had 1.31 (CI95%:1.07–1.61;p = 0.010) more probabilities, those classified as overweight had 1.29 (CI95%:1.03–1.60;p = 0.024) more chances and physiotherapists who treated 50 or more patients per week were 1.37 (CI95%:1.13–1.67;p = 0.002) more likely to have WRMDs.
Conclusions
There was a high prevalence of WRMDs in the analyzed sample. It is necessary to implement labor strategies in order to reduce the risk of injuries.
Introduction
In Portugal, there are approximately 14,000 physiotherapists who provide services in the public, private, and social sectors, making Physiotherapy the third largest healthcare profession in Portugal and Europe. 1
World Physiotherapy 2 describes Physiotherapy as a profession that provides services to individuals and populations with the aim of developing, maintaining, and restoring maximum movement and functional ability throughout the lifespan, working in promotion, prevention, treatment/intervention, and rehabilitation.
To perform their duties, physiotherapists engage in many hours of intensive work, including patient transfers, mobilizations, manual therapy techniques, and repetitive movements throughout the day, which can lead to injuries. Despite being the most suitable professionals with extensive knowledge in injury prevention, physiotherapists are not immune to the occurrence of musculoskeletal injuries. They may fail in the execution of therapeutic techniques used in patient treatment or adopt irregular body positions that overload the musculoskeletal system. 3
The Constitution of the Portuguese Republic defines a work-related accident as one that occurs at the workplace and during the time the worker performs their duties, resulting directly or indirectly in a bodily injury, functional impairment, or illness that leads to a reduction in work capacity. 4
Work-related diseases are defined as multifactorial illnesses in which the work environment plays a partial role in causation, including non-communicable chronic diseases that affect working populations. 5 Work-related diseases and injuries burden healthcare systems, reduce productivity, and can negatively impact household income. 6
The systematic review conducted by Vieira et al. 7 revealed a prevalence of work-related musculoskeletal disorders among physiotherapists at some point in their professional lives ranging from 53% to 91%, with the lower back being the most affected body part, followed by the cervical region, thumbs, upper back, and shoulders. The tasks most commonly associated with the development of these disorders were manual therapy, lifting, and transferring patients.
Several studies indicate that the lifetime prevalence of work-related musculoskeletal disorders (WRMDs) in physiotherapists ranged from 55% to 91%8–12 and the prevalence in the 12-month period ranged from 40% to 91%.8,9,12,13
More recent studies, such as those by Rahimi et al. 14 evaluated a sample of 319 physiotherapists aged between 21 and 73 years, in which 94% of physiotherapists reported the presence of injuries in a 12-month period and the study by Khairy et al. 15 identified that 82.6% of physiotherapists, in a sample of 501 individuals aged between 24 and 63, suffered injuries in a two-year period. Abaraogu et al. 16 examined 126 physiotherapists (mean age: 31.98) and a total of 280 injuries were recorded over a 12-month period and 65 injuries over a 7-day period. Kakaraparthi et al. 17 evaluated a sample of 113 physiotherapists (mean age: 30.5), identifying a total of 291 injuries in a period of 12 months.
Bae and Min 18 evaluated 788 physical therapists in South Korea and found that 94.5% reported having suffered some injury in their work practice. In the study by Iqbal and Alghadir 19 69 participants from India were evaluated and it was found that the prevalence of work-related injuries was 92%.
The study by Abolfotouh et al. 3 evaluated 259 rehabilitation professionals (physiotherapists and occupational therapists) and found that 74% reported low back pain in the past year. This pain was responsible for work absences in 33% of the professionals, with an average of 1.38 (±2.96) days of absence in the past year. Most professionals (75%) sought healthcare services due to the pain, and 39% requested rest days and/or medical leave.
In Portugal, studies evaluating injuries among physiotherapists are scarce and involved a very small sample and the practice of the profession of physiotherapists may be different between different countries. Therefore, the aim of this study was to determine the epidemiology of WRMDs in physiotherapists working in Portugal, describing the most frequent injury locations, types, and mechanisms, as well as the associated risk factors.
Methods
The study design was descriptive-correlational and cross-sectional.
The study was approved by the Health Ethics Committee of the Algarve University Hospital Center, Portimão unit. All participants were informed of the study's objectives and that they could withdraw at any time without any consequences. The anonymity of responses was ensured. Informed consent to participate in the study was obtained from all participants.
Population
The population consisted of physiotherapists practicing in Portuguese territory, of all genders. As of the current date, there are 12,553 physiotherapists registered with the Professional Council of Physiotherapists.
The sample size was determined using an estimated mean injury prevalence of 50% and assuming an error margin of 3% with 95% confidence interval (CI). Using these assumptions, the minimum sample size contained 984 physiotherapists.
The inclusion criteria involved physiotherapists working in public, private, and social sectors, with at least one year of professional practice, a minimum of 5 h of work per week, working under any regime, and who freely agreed to participate in the study.
Measurement instrument
The measurement instrument consisted of a digital questionnaire divided into two parts: sociodemographic characterization of the population and aspects related to professional practice, as well as questions regarding the occurrence of injuries.
Since there are no known validated questionnaires on this topic, this questionnaire was developed and evaluated by a group of three physiotherapists with PhDs, lecturers and researchers. Additionally, the questionnaire was subjected to a pretest, administered to 10 physiotherapists, to identify any potential issues and to measure the completion time.
The questionnaire was administered in a single instance by previously trained physiotherapy students, in person to the physiotherapists’ workplaces. Additionally, the questionnaire was distributed through social media and email to the interest groups of the Portuguese Association of Physiotherapists with the physiotherapists themselves responding, and was completed via phone calls to the physiotherapists’ workplaces by trained physiotherapy students.
The first part of the questionnaire included questions about: age, gender, weight, height, workplace, professional practice context, region of professional practice (according to the Nomenclatura das Unidades Territoriais para Fins Estatísticos – NUT II), year of graduation, years of professional practice, years of uninterrupted professional practice, number of weekly working hours, number of working days per week, break time including lunch, average number of patients per hour/day, physical exercise/sport practice at least twice a week, and if they practiced any exercise, they were to specify the average weekly exercise time in minutes, and finally, the pathological conditions of the patients they attended. The last questions considered a time frame of the past 12 months. Regarding the question of patients’ pathological conditions, physiotherapists highlighted all the pathological conditions they had worked with most in the last 12 months, and could indicate more than one answer option. For example, in the last 12 months, physiotherapist “X” worked only with patients with musculoskeletal and neurological conditions. Furthermore, when asked about the context of the workplace and professional practice, physiotherapists could indicate more than one answer option.
The second part of the questionnaire focused on the presence of injuries related to professional practice during the following periods: throughout the entire practice, in the last 48 h, and in the last 12 months. Only physiotherapists who reported injuries in the past 12 months continued to fill out the questionnaire, indicating the number of injuries, the type of injury, location, mechanism of injury, place where the injury occurred, whether they underwent any treatment, and if so, they had to specify the type of treatment received, the inactivity time caused by the injury, and the current status of the injury.
An injury was defined as any condition or symptom that occurred as a result of professional practice as a physiotherapist and had at least one of the following effects: the physiotherapist had to stop their work activity for at least one day; if they did not have to stop working, they had to modify their activity (fewer working hours, reduced effort intensity, decreased ability to perform certain technical gestures or maneuvers); they sought advice or treatment from healthcare professionals to address the condition or symptom.
Data analysis
The software used for the statistical analysis of the data was the Statistical Package for Social Sciences (SPSS), version 29.0.
In the initial approach, descriptive statistics were performed. Next, a binary logistic regression (Enter method) was conducted to test the influence of the variables used in this study on the presence of injury, with each variable being analyzed separately. Subsequently, a final multivariate model was developed (Forward Likelihood method). CI were calculated for both models.
In the analysis using body mass index (BMI), individuals classified as underweight were excluded, and individuals with overweight and obesity were grouped into a single category.
The validity, goodness of fit, and predictive capability of the binary logistic regressions were assessed using the Omnibus test, Hosmer-Lemeshow test, and Nagelkerke's correlation coefficient.
The level of statistical significance was set at 0.05.
Results
The sample consisted of 1828 physiotherapists, of which 1194 (65.3%) were female and 634 (34.7%) male, aged between 21 and 66 years (33.06 ± 8.40). The year of graduation of the physiotherapists ranged from 1971 to 2022. The weight of the physiotherapists ranged from 40 to 135 kg (67.58 ± 12.69) and height from 1.32 to 2.02 meters (1.69 ± 0.91), with a BMI ranging from 15.79 to 41.91 Kg/m2 (23.65 ± 3.33). According to the BMI classification, 41 (2.2%) physiotherapists were classified as underweight, 1259 (68.9%) as having a normal weight, 444 (24.3%) as overweight, and 84 (4.6%) as obese.
1168 (36.9%) physiotherapists reported engaging in some form of physical exercise at least twice a week, while 660 (36.1%) did not engage in any exercise. The weekly duration of physical exercise ranged from 15 to 1200 min (208.96 ± 140.67).
Most of the physiotherapists worked in the Northern region of Portugal (612; 33.48%), followed by the Central region (447; 24.45%), Lisbon Metropolitan Area (341; 18.65%), Algarve (340; 18.60%), Alentejo (36; 1.97%), Autonomous Region of the Azores (34; 1.86%), and Autonomous Region of Madeira (18; 0.98%).
Table 1 presents the nominal and numerical variables related to the professional practice of physiotherapists. Some physiotherapists worked in more than one work place, in different practice contexts, and worked with patients with different pathologies. Therefore, in these questions, physiotherapists could select more than one answer option, justifying the total obtained in each of these sections, exceeding the sample value.
Variables related to professional practice of physiotherapists.
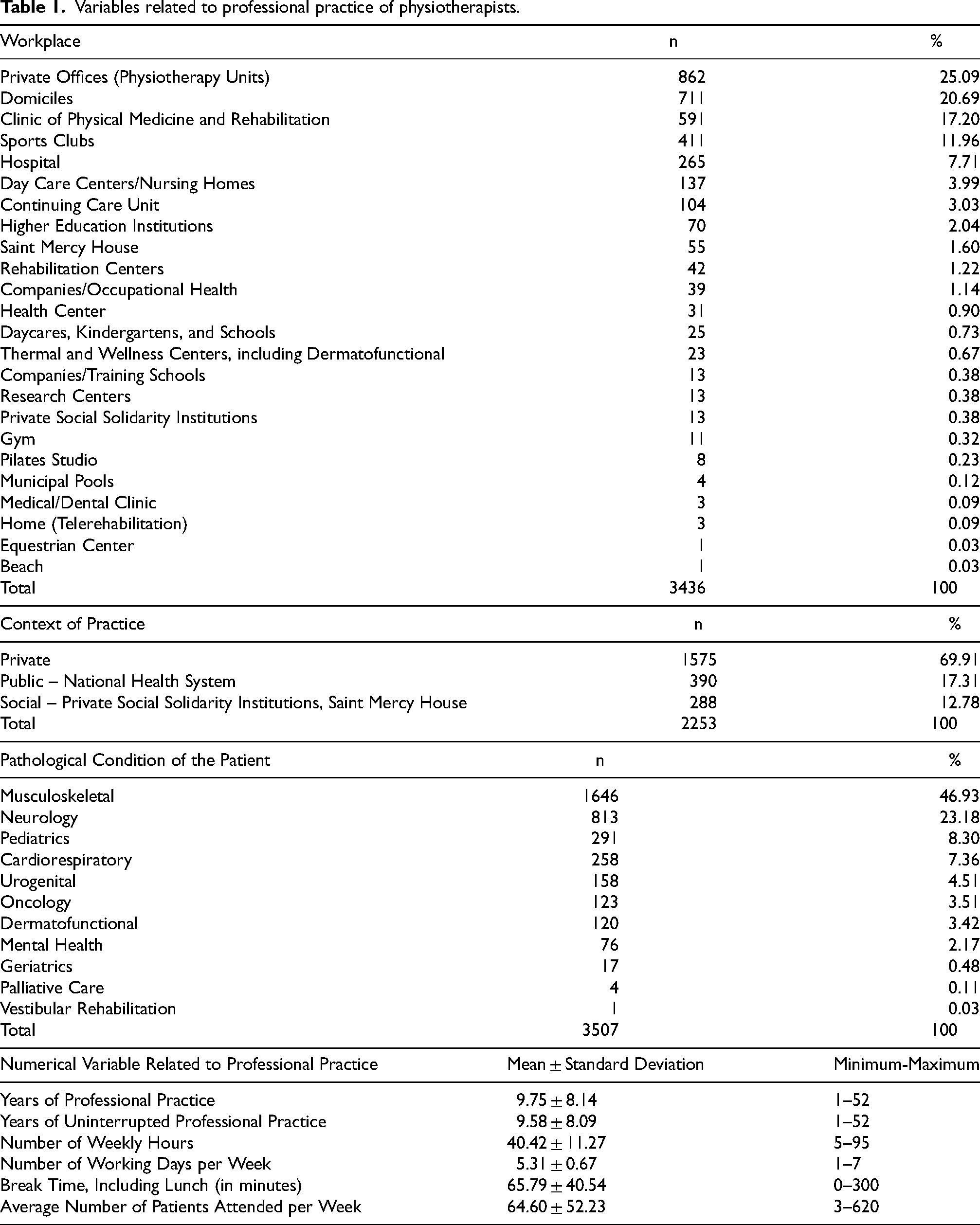
Table 2 presents the prevalence values of WRMDs in physiotherapists during 3 different periods.
Prevalence values of WRMDs in physiotherapists.

Of the physiotherapists who experienced WRMDs at some point during their entire professional practice (998; 100%), 366 (36.67%) suffered 1 injury, 343 (34.37%) had 2 injuries, 180 (18.04%) had 3 injuries, and 109 (10.92%) physiotherapists reported having 4 or more injuries, totaling 2028 injuries.
Of the physiotherapists who experienced WRMDs in the last 12 months (696; 100%), 289 (41.52%) suffered 1 injury, 253 (36.35%) had 2 injuries, 117 (16.81%) had 3 injuries, and 37 (5.32%) physiotherapists reported having 4 or more injuries, totaling 1294 injuries. Since the physiotherapists could only characterize a maximum of 3 injuries, the following results will refer to 1146 injuries.
Figure 1 presents the absolute and relative frequencies of the anatomical locations where WRMDs occurred.
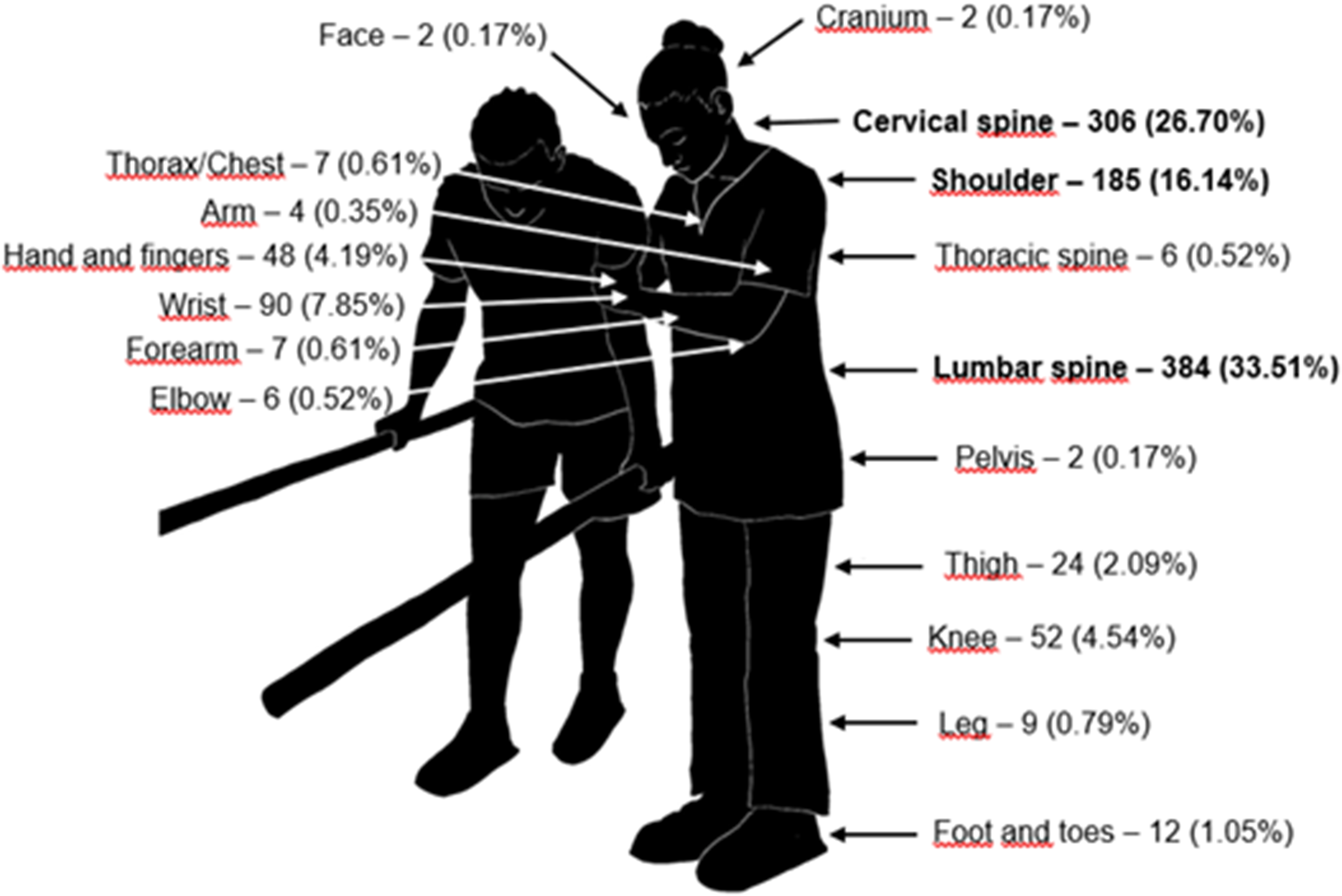
Location of WRMDs.
The value of injury proportion was 0.38 (CI 95%: 1.83–2.59) and the injury rate was 0.035 injuries per 1000 h of Physiotherapist professional practice. The average number of injuries per Physiotherapist was 0.63. The average of injuries per injured Physiotherapist was 1.65.
Table 3 presents the association between the type and location of the injury, showing the percentage values of the different types of WRMDs. This table presents the total values according to the type of injury and the total number of injuries presented (including all types of injuries) was 1146.
Type and location of WRMDs.
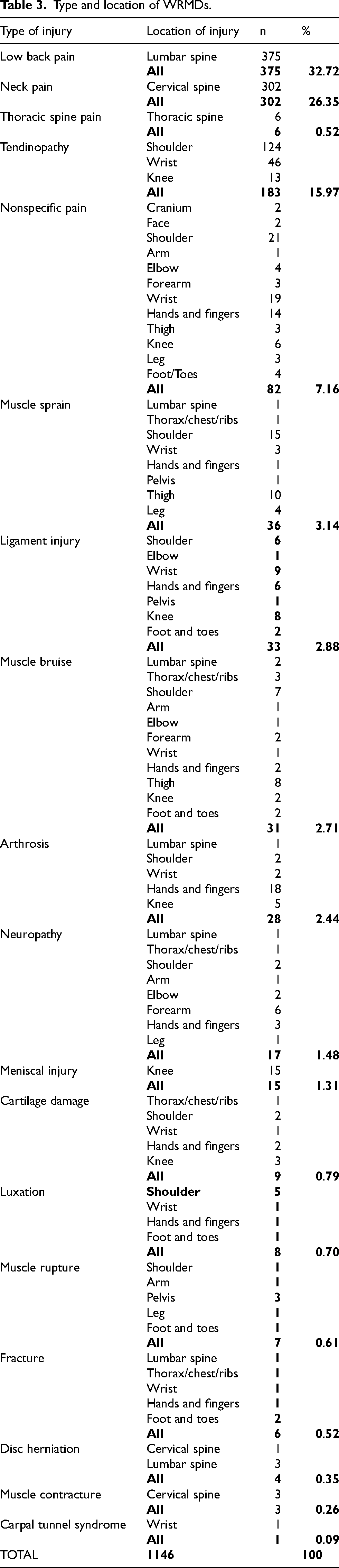
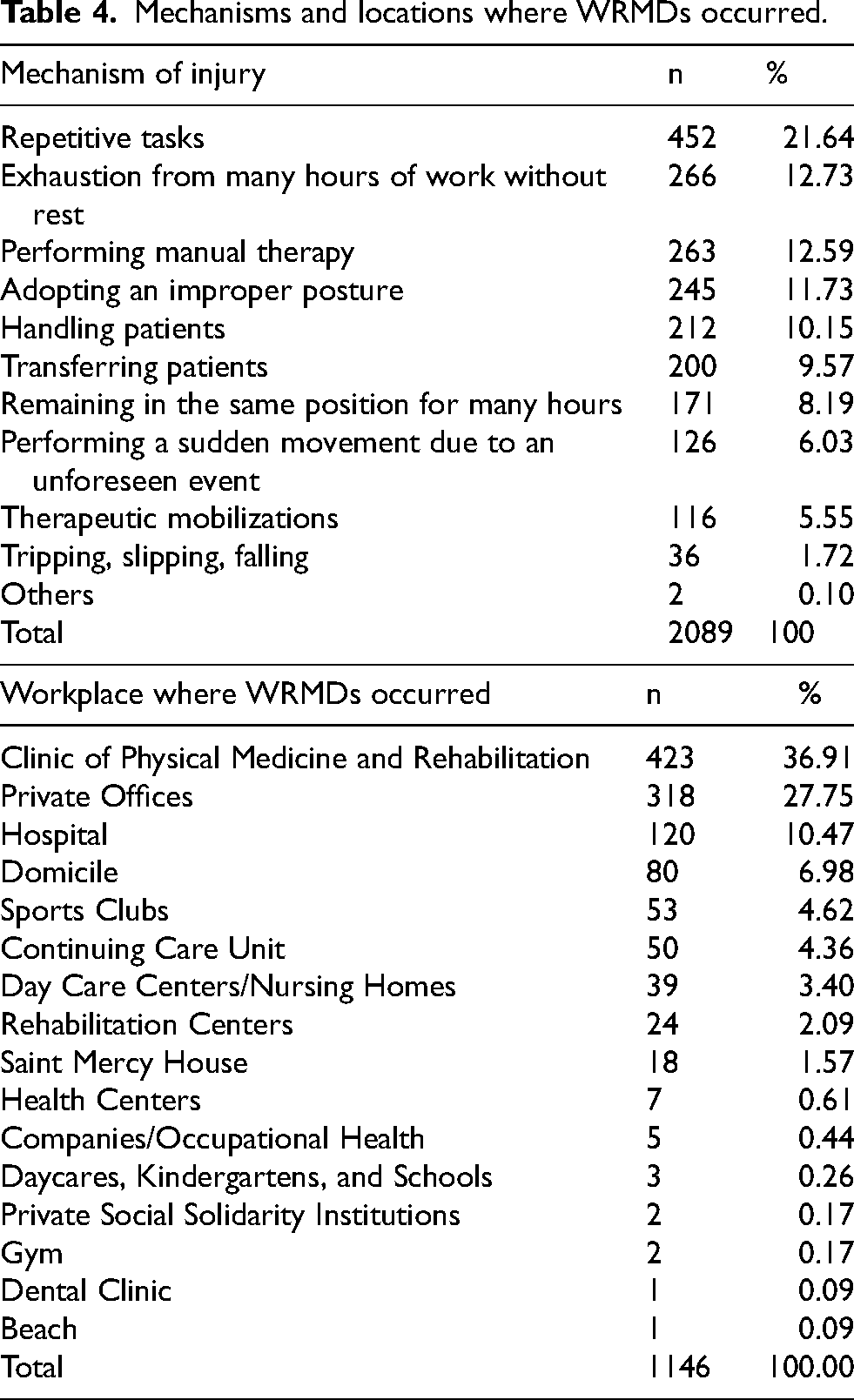
Table 4 presents the absolute and relative frequencies of the mechanisms that caused WRMDs in physiotherapists and the locations where WRMDs occurred. Physiotherapists could report more than one mechanism of injury for each declared WRMD.
Mechanisms and locations where WRMDs occurred.
Most of the WRMDs were subjected to some type of treatment (798; 69.63%), while 348 (30.37%) injuries were not treated. Physiotherapists could select more than one type of treatment for each injury. The types of treatment performed were: Physiotherapy by a professional colleague (485; 36.36%), self-treatment by the physiotherapist (228; 17.09%), medication (201; 15.07%), rest (163; 12.22%), osteopathy (143; 10.72%), non-conventional therapies (acupuncture, reiki, shiatsu) (52; 3.90%), immobilization (38; 2.85%), surgery (17; 1.27%), and others (7; 0.52%).
Most of the WRMDs did not cause any days of professional inactivity, although they did affect work activities (1056; 92.15%). Thirty-seven (3.23%) injuries caused professional inactivity between 3 to 7 days, 32 (2.79%) injuries caused up to 2 days of inactivity, 17 (1.48%) more than 30 days, 3 (0.26%) between 8 and 14 days, and 1 (0.09%) injury caused between 15 to 30 days of professional inactivity.
Regarding the current status of WRMDs, 577 (50.35%) injuries no longer cause pain or other symptoms and the physiotherapist is fully recovered, 349 (30.45%) injuries still cause pain or other symptoms but the physiotherapist is not undergoing treatment, 128 (11.17%) injuries still cause pain or other symptoms and the physiotherapist is undergoing treatment, and 92 (8.03%) injuries do not cause pain or other symptoms but the physiotherapist is undergoing treatment and/or is limited in their professional practice due to the injury.
Table 5 presents the relationship between the presence of WRMDs in the 12-month period and the variables analyzed in this study. The final model was considered mathematically valid with a relatively good predictive capacity (Omnibus, Hosmer-Lemeshow, and Nagelkerke tests: p < 0.001; p = 0.760, and R2 = 0.058).
Relationship between the event, the presence of WRMDs, and variables about non-modifiable sample factors and the professional physiotherapist practice characteristics.
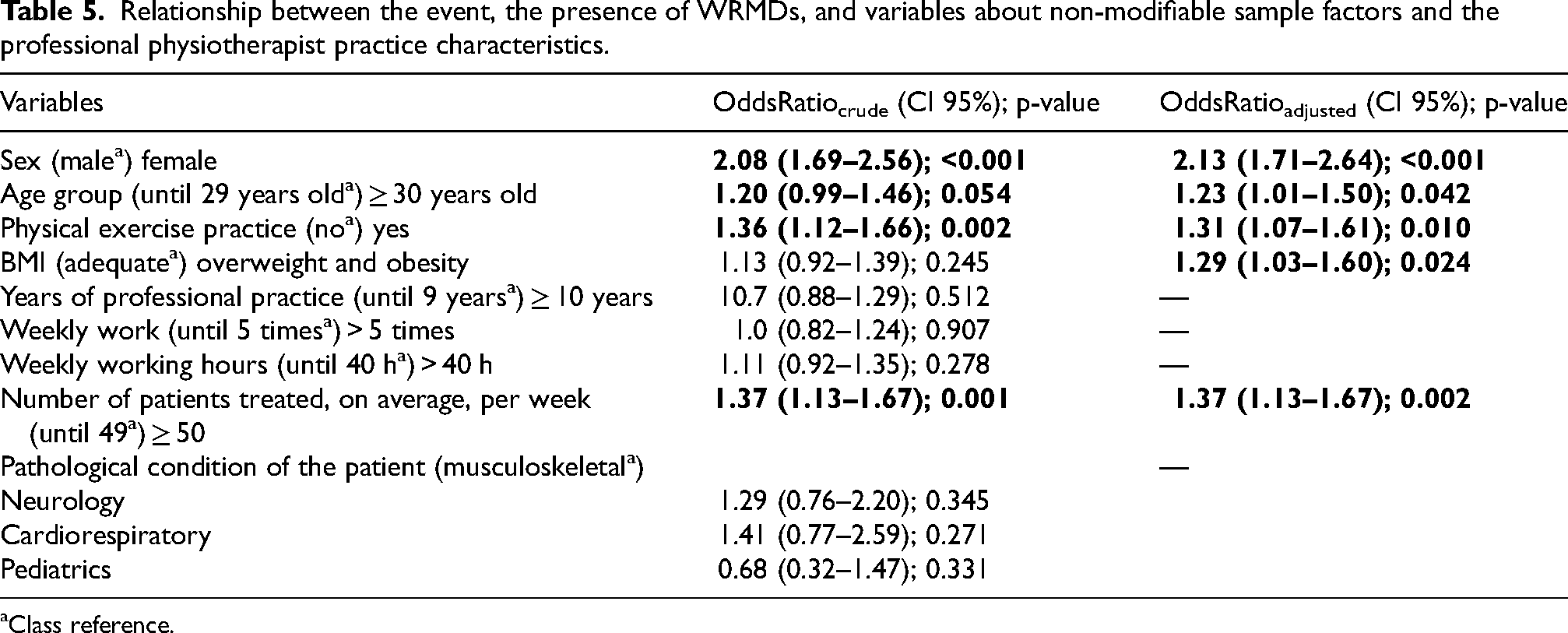
Class reference.
It was found that women were 2.13 times (95% CI: 1.71–2.64; p < 0.001) more likely to develop WRMDs compared to men, physiotherapists aged 30 years or older were 1.23 times (95% CI: 1.01–1.50; p = 0.042) more likely to have WRMDs compared to younger physiotherapists, physiotherapists who engaged in some form of physical exercise were 1.31 times (95% CI: 1.07–1.61; p = 0.010) more likely to develop WRMDs compared to those who did not exercise, physiotherapists classified as overweight or obese according to BMI were 1.29 times (95% CI: 1.03–1.60; p = 0.024) more likely to present WRMDs compared to those with an adequate BMI, and physiotherapists who attended to 50 or more patients had 1.37 times (95% CI: 1.13–1.67; p = 0.002) more chances of having WRMDs compared to those who attended to fewer patients.
Discussion
The data obtained in this study revealed a high prevalence of WRMDs among physiotherapists working in Portugal, considering a higher sample of the population of this country. In 2011, Rodrigues and Pedro 20 evaluated 378 physiotherapists and found that 300 (79.47%) physiotherapists reported the presence of symptoms (pain, discomfort or numbness) in various anatomical regions in the last 12 months. The study by Holder et al. 21 evaluated 667 physiotherapists and physiotherapist assistants from the American Physical Therapy Association 1996 active membership list and found the presence of musculoskeletal injury in the past 2 years in 32% of the sample, a value similar to that obtained in this study, which evaluated a 1-year period (39%). Another study conducted by Alrowayeh et al., 22 which evaluated 212 physiotherapists working in the State of Kuwait, found an annual prevalence of 47.6%.
Higher prevalence values of injuries were observed in the study by Alnaser et al., 23 which evaluated 321 physiotherapists from the State of Kuwait and found a 48% prevalence of WMSDs over a 12-month period, and in the study by Islam et al., 24 which evaluated 62 physiotherapists working in Bangladesh and found that 97% complained of work-related pain. Vieira et al. 25 evaluated 121 physiotherapists from Florida and found a 96% prevalence over a 12-month period. Rozenfeld et al. 12 evaluated 112 Israeli physiotherapists and the lifetime prevalence of WMSDs was 83%, while the values obtained in our study were 55%.
The comparison of our results with studies from other countries is difficult, as there may be variations in the roles of physiotherapists between countries, as well as the workload and other factors that could influence the presence of injuries.
The data from this study revealed that physiotherapists are highly exposed to WRMDs, probably because they are in direct contact with patients, which often requires significant physical effort to perform tasks related to patient care such as transferring, lifting, and positioning patients. Additionally, they must perform repetitive movements using manual techniques that overload the musculoskeletal system and maintain improper positions for prolonged periods.21,26 The combination of these factors with attending to a large number of patients in a day can increase the risk of developing injuries.
The most frequent types of WRMDs observed in this study were low back pain (33%), neck pain (27%), and tendinopathy (16%), with the most common anatomical locations for the latter being the shoulder (68%) and wrist (25%). Abolfotouh et al. 3 evaluated 259 physiotherapists and occupational therapists in Saudi Arabia and revealed a one-year prevalence of low back pain in 73.7% of the sample.
The study by Holder et al. 21 found that the most frequent types of injury were muscle strain (69%), ligament sprain (28%), and vertebral disk involvement (16%), differing from the results obtained in this study. The study by Alnaser et al. 23 also presented divergent results, where the most frequent type of injury was muscle spasm (51%), followed by muscle strain (17%), tendinopathy (16%), and ligament sprain (7%). Comparing the results between studies is challenging due to the different classifications of injury types used in the various studies.
The presence of work-related low back pain can be explained by the application of extreme loads in the work environment or the improper execution of manipulative techniques used in patient treatment, as well as by patient transfers, gait training, repositioning, and performing repetitive tasks that may be carried out in an improper body position.3,7,27
The development of neck pain can be associated with work-related stress, 28 with the physiotherapist being required to attend to a large number of patients in short periods, without delays, while providing quality service. Both low back pain and neck pain have multiple risk factors, including psychological and behavioral factors. 29 Lundberg et al. 30 showed that work-related stress was associated with muscle tension and pain symptoms, which were evaluated through measures such as blood catecholamine levels, heart rate, electromyography, and blood pressure.
Tendinopathy is possibly associated with performing repetitive tasks without adequate rest intervals. The physiotherapists in the sample of this study reported an average of 1.1 h of break time over 40.4 weekly hours. Repeated movement can cause inflammation of the tendons and other musculoskeletal structures.
Our results revealed that the most affected anatomical locations by WRMDs were the lumbosacral spine (34%), cervical spine (27%), shoulder (16%), and wrist (8%). Similar results were found in the study by Mansour et al., 31 which evaluated 139 physiotherapists from Jordan and revealed the presence of musculoskeletal complaints in the cervical spine (100%), lumbar spine (97.9%), shoulder (96.5%), and wrist (24.1%). Holder et al. 21 identified the most frequent injury locations as the lumbar spine (62%), upper back (23%), wrist and hand (23%), with the shoulder accounting for 14% of injuries.
Alnaser et al. 23 also found that most physiotherapists reported WMSDs in the lumbar spine (55%), followed by the wrist and hand (20%), neck (11%), and shoulder (0.7%). The study by Islam et al. 24 found that the most affected locations were the lumbar spine (90%), cervical spine (72% of cases), wrist (58%), and shoulders (55%), but this study also included occupational therapists in its sample. Alrowayeh et al. 22 identified the most affected locations as the lower back (32%), neck (21%), upper back (19%), shoulder (13%), hand/wrist (11%), and knee (11%). Rozenfeld et al. 12 revealed that the lumbar region accounted for 50.7% of injuries.
The most frequent mechanisms of injury in this study were performing repetitive tasks (22%), lack of rest breaks during the workday leading to exhaustion (13%), and performing manual therapy techniques (13%). Physical exhaustion after work was occasionally reported by 49.5% and frequently by 37.5% of the 62 physiotherapists and 39 occupational therapists who comprised the sample in the study by Islam et al.. 24 Performing manual therapy techniques (26%) and patient transfers (25%) were the most common mechanisms of injury in the study by Alnaser et al. 23
The systematic review conducted by Vieira et al. 7 found that performing manual therapy and lifting and transferring patients were the tasks most commonly associated with the development of WRMDs in physiotherapists. The study by McCrory et al. 32 found that the causes of injury occurrence were frequent bending/twisting movements, excessive effort during patient handling activities, inadequate lifting devices, and lack of ongoing training for the use of mechanical lifting devices. However, this latter study included 67 physiotherapy assistants in its sample, in addition to 170 physiotherapists.
Holder et al. 21 found that patient transfers (30%), lifting patients (25%), responding to an unexpected or sudden movement by a patient (24%), and performing manual therapy were the most frequent mechanisms of injury. Performing manual therapy techniques accounted for 21% of the injuries, performing repetitive tasks accounted for 15% of the injuries, and working after being physically fatigued accounted for 13% of the injury mechanisms. The study by Salik and Özcan 11 verified that the highest risk factor causing injuries was transferring the patient (15%).
The workplaces where the highest number of WRMDs were reported in this study included Clinics of Physical Medicine and Rehabilitation (37%), private offices (28%), hospitals (11%), and patients’ homes (7%). It is noteworthy that most physiotherapists worked in these locations where the highest number of injuries occurred: private offices (25%), domiciles (21%), Clinics of Physical Medicine and Rehabilitation (17%), and hospitals (8%). Despite 12% of the sample's physiotherapists working in sports clubs, these were not considered as locations where the highest number of WRMDs occurred. The study by Holder et al. 22 reported more injuries in outpatient settings (64%), hospitals (63%), and specialized nursing facilities (52%), and the systematic review conducted by Vieira et al. 7 found that physiotherapists working in hospitals had a higher prevalence of WMSD. Alnaser et al. 23 reported that most injuries occurred in general hospitals (32%) and rehabilitation hospitals (30%).
In Portugal, it is believed that patient care at domicile may involve fewer working hours, as most physiotherapists provide domicile care in addition to their professional practice at another location. Despite this, the domicile was considered a place where a significant number of WRMDs occurred. This may be due to the fact that patients’ homes are often not equipped with ergonomic structures, such as height-adjustable beds, which can lead to increased physical effort for the physiotherapist and improper working postures. Future studies are necessary to evaluate the number of working hours and the types of patients physiotherapists attend to at home, as well as the working conditions, to assess their association with the presence of WRMDs.
Regarding the logistics of Clinics of Physical Medicine and Rehabilitation, these generally involve a high patient-to-hour ratio, leading to greater work overload, which is different from the practice of physiotherapy in private offices, where the number of patients is usually lower, but the time spent with each patient is higher and individualized, also resulting in a significant physical work demand. As for hospitals, although the number of patients treated may be lower compared to Clinics of Physical Medicine and Rehabilitation, it is believed that this location was associated with a higher number of WRMDs due to the type of patients treated, who are more dependent in terms of mobility and require greater physical effort from the physiotherapist. Clinics of Physical Medicine and Rehabilitation also treat neurologically dependent patients, but most cases in clinics are musculoskeletal.
Most physiotherapists treated patients with musculoskeletal conditions (47%), followed by neurological patients (23%), pediatric patients (8%), and those with cardiorespiratory conditions (7%). The reference class chosen for binary logistic regression was musculoskeletal conditions. It was observed that physiotherapists who primarily worked with neurological patients were 1.29 times more likely to develop WRMDs, and those working with patients with cardiorespiratory conditions were 1.41 times more likely to have WRMDs, compared to physiotherapists who primarily worked with musculoskeletal conditions. However, this analysis did not achieve statistical significance. The study by Nordin et al. 33 found that physiotherapists working in pediatrics had the highest prevalence of injuries (87.5%), followed by those in cardiorespiratory (71.4%), musculoskeletal (71.4%), and neurology (70%).
Regarding the treatment of WRMDs, most physiotherapists in this study sought treatment from a colleague, as well as self-treatment. The study by Abolfotouh et al. 3 revealed that 50.3% of physiotherapists and occupational therapists were treated by a physiotherapist and 25.1% by doctors. The systematic review by Vieira et al. 7 and the study by Alrowayeh et al. 22 also revealed that most physiotherapists sought physiotherapy as a treatment for their injuries, preferring either self-treatment or treatment by a colleague.
The current status of most WRMDs in this study revealed that they no longer cause pain or other symptoms, and the physiotherapist considered themselves fully recovered (50%). However, 42% of the injuries still caused pain or other symptoms to the physiotherapist.
Despite the high number of WRMDs reported in this study, most did not cause physiotherapists to interrupt their professional practice (92%), although it did affect their practice in some way. The study by Holder et al. 21 reported that 79% of physiotherapists made changes to their work habits, improving their body mechanics (50%), increasing the use of other personnel (43%), and frequently changing their work position (24%), without limiting their contact time with patients (92%) or the area of practice after sustaining an injury (85%). Additionally, 8% of physiotherapists who participated in the latter study stated that they would consider a job change because of their injury or the risk of sustaining another injury.
The systematic review conducted by Vieira et al. 7 revealed that 7% to 47% of injured physiotherapists took time off due to WMSDs, and the study by Alnaser et al. 23 found that 33% of physiotherapists reported lost workdays due to their injuries, with a total of 337 days lost over a 12-month period.
Abolfotouh et al. 3 found that 52.5% of their sample had intense lower back pain lasting one day or more, 22.4% had chronic lower back pain, 23.9% had lower back pain that caused work absence, and 18.5% had lower back pain requiring medical attention. Lower back pain was responsible for work absence in 32.5% of the physiotherapists and occupational therapists who comprised the sample.
The results obtained from the binary logistic regression revealed that female physiotherapists were 2.13 times more likely to develop WRMDs (p < 0.001) when the influence of other variables was included in the model. Similar data was observed in the systematic review conducted by Vieira et al. 7 and other studies.33,34 The study by Alrowayeh et al. 22 found a higher prevalence of low back pain and neck pain in female physiotherapists. The higher presence of musculoskeletal injuries in women can be explained by the differences in size and strength compared to men, where women have a biomechanical disadvantage in handling physical stress that can lead to the development of WMSDs.7,27 Furthermore, women exhibit certain physiological characteristics, particularly hormonal variations and differences in connective and muscle tissue structures.35,36 The greater laxity of these tissues, related to estrogen levels, may explain why these tissues are less capable of withstanding functional pressure, leading to a higher development of musculoskeletal injuries. 36
Older physiotherapists (aged 30 years or older) also showed a higher likelihood of developing WRMDs (1.23 times; p = 0.042) compared to younger physiotherapists, as did those who had been working for 10 years or more. However, the latter analysis did not show statistical significance in the Enter model of logistic regression and was removed from the analysis by the Forward-LR method. Age is a factor related to the development of injuries, characterized by the aging of osteo-myotendinous structures.
Divergent data was observed in the study by Holder et al., 21 which found that the highest prevalence of injuries was among younger physiotherapists, aged between 21 and 30 years, as well as in the study by Adegoke et al., 22 which found a higher prevalence of injuries in physiotherapists under 30 years old. The study by Abolfotouh et al. 3 found that physiotherapists and occupational therapists with less than 10 years of experience were significant predictors of low back pain. The study by Alrowayeh et al. 22 revealed that more than 26% of physiotherapists aged between 20 and 40 years reported complaints in the lower back region, while only 5% of those over 40 years old reported these complaints.
Physiotherapists who engaged in physical exercise at least twice a week were 1.31 times more likely to develop WRMDs compared to those who were sedentary. Since exercise is considered a protective factor against the development of injuries, future studies are suggested to determine the type, intensity, and frequency of exercises, as well as the implementation of warm-up and cool-down periods in exercise practices associated with WRMDs. The study by Alrowayeh et al. 22 did not find a statistically significant association between the presence of WMSDs and the practice of exercise.
In the analysis of BMI, according to the Enter method with the entry of each variable one at a time, no statistical significance was obtained. However, in the Forward-LR model, this analysis achieved statistical significance (p = 0.0024), where it was observed that physiotherapists classified as overweight and obese were 1.29 times more likely to develop WRMDs compared to those classified with an adequate BMI. Adegoke et al. 34 revealed that the presence of injuries was associated with a low BMI, and Mansour et al. 31 found that the total exposure to musculoskeletal complaints was positively correlated with BMI. Nordin et al. 33 found that physiotherapists with a BMI between 18 and 25 Kg/m2 accounted for 70.2% of the injuries, those with a BMI above 25 Kg/m2 accounted for 80% of the injuries, and physiotherapists with a BMI below 18 Kg/m2 had 55.6% of the injuries.
Another variable that showed statistical significance in the logistic regression models was the number of patients each physiotherapist attended per week. It was found that physiotherapists who attended a higher number of patients (50 or more patients) were 1.37 times more likely to develop WRMDs compared to those who attended a smaller number of patients. As previously mentioned, a higher number of patients does not necessarily represent a higher workload for the physiotherapist, as it also depends on the type of pathological conditions these patients present, as well as the time spent attending to each patient. In other words, a physiotherapist may have a higher number of patients, but most may present musculoskeletal conditions, whose treatment can be mainly carried out using electrotherapy and thermotherapy resources, and the effective time the physiotherapist is performing any manual technique or transfer may be reduced. Conversely, a physiotherapist may have a smaller number of patients but spend 1 h or more per session, possibly with patients with greater functional limitations, thus requiring more physical effort from the physiotherapist. Therefore, future studies could evaluate the association between the type of patient and their pathological condition, as well as the time spent attending to each specific patient, with the presence of WRMDs.
Limitations
The study presented limitations such as the presence of recall bias among participants, despite the fact that the information was collected from a period one year prior. Additionally, there was a lack of control over some variables that could have interfered with the results, such as hormonal issues related to the woman's cycle, such as menstruation and pregnancy. The data collection method may have caused some biases such as selection bias, making it difficult to access the study for those who did not have internet access or who did not answer calls from unknown numbers, response bias where the answers could have been influenced by the method of collection or the environment and non-response bias due to the lack of time available to participate in the study, for example. Despite the high sample size, the sampling method was non-probabilistic, which may not represent the diversity of the population.
Conclusions
This was the first study conducted with Portuguese physiotherapists involving a high sample of the population, and it was also evaluated a very high number of these professionals compared to published international studies.
The data from the present study revealed a high prevalence of WRMDs in different periods within the analyzed sample. The most frequent types of WRMDs were low back pain, neck pain, and tendinopathy, with the most common anatomical locations being the lumbar and cervical spine and the shoulder. The most frequent mechanisms of injury were performing repetitive tasks, exhaustion from many hours of work without rest, and performing manual therapy.
The non-modifiable risk factors associated with WRMDs were being female and being aged 30 years or older, while the modifiable factors were engaging in physical exercise, being overweight, and attending to a high number of patients.
Therefore, it is necessary to implement occupational measures such as providing or increasing the break time between patient appointments, which could be an active break including techniques of active mobilization and muscle stretching. Another strategy could be to alternate work between patients who are more and less physically demanding.
Footnotes
Acknowledgments
To the physiotherapists who answered the questionnaire, to the 1st and 4th year students of the Physiotherapy Course of Escola Superior de Saúde Jean Piaget do Algarve who helped with data collection, to the Musculoskeletal Physiotherapy Interest Group (GIFME) for disseminating the study Interdisciplinary Centre for the Study of Human Performance (CIPER), to professors Raul Oliveira from the Human Kinetics Faculty, University of Lisbon (UL) and Adérito Seixas from the Fernando Pessoa University, Portugal for their help in preparing and evaluating the questionnaire applied to the participants. To Inês Adrião for creating the figure.
Ethics
The study was approved by the Health Ethics Committee of the Algarve University Hospital Center, Portimão unit. All participants were informed of the study's objectives and that they could withdraw at any time without any consequences. The anonymity of responses was ensured.
Authors’ contributions
All authors were responsible for the conception and design of the study and data collection; BM was involved in the processing and statistical analysis of data; all authors were involved in the drafting of the manuscript; and all authors contributed to the interpretation of the data for the work and revising it critically for important intellectual content. All the authors finally approved the manuscript. BM was responsible for the integrity of the work as a whole. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.