
Abstract
Background
Professional quality of life (ProQoL) encompasses the positive and negative experiences associated with one's professional role. Accurate assessment of ProQoL necessitates psychometrically sound instruments.
Objective
This study examined the reliability and validity of the Short Professional Quality of Life Scale (Sh-ProQoL) in a sample of Arab nurses.
Methods
A cross-sectional design was employed using convenience sampling. The study included 200 nurses from hospitals in Dubai. Psychometric evaluation comprised assessments of reliability and inter-scale correlations. Exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were conducted to determine the factor structure. Convergent validity was assessed through average variance extracted (AVE) and Pearson correlation coefficients between the Ar-Sh-ProQoL and external measures: Job Satisfaction (JS), Perceived Quality of Care (PQC), and Intention to Leave (ITL).
Results
The scale and its subscales demonstrated strong internal consistency, with test–retest reliability coefficients of ICC ≥ 0.70. EFA and CFA supported a 3-factor structure for the Ar-Sh-ProQoL, explaining 74.57% of the total variance. Factor loadings from EFA ranged from 0.73 to 0.87, and CFA yielded acceptable fit indices: χ2/df = 1.51, RMSEA = 0.05, GFI = 0.96 and CFI = 0.98. Square root AVE values ranged from 0.87 to 0.88, and AVE values ranged from 0.75 to 0.80, confirming strong discriminant and convergent validity. The scale also showed significant correlations with JS (r = 0.51), PQC (r = 0.45), and ITL (r = 0.48).
Conclusion
The Ar-Sh-ProQoL demonstrated robust psychometric properties and is a valid and reliable instrument for assessing the ProQoL among Arab nurses.Conclusion: The Ar-Sh-ProQoL, consisting of nine items, demonstrated robust psychometric properties and is a valid and reliable instrument for assessing the professional quality of life among Arab nurses.
Keywords
Introduction
The healthcare sector in the United Arab Emirates (UAE) plays a critical role in advancing the nation's strategic goal of delivering high-quality medical services while fostering overall societal well-being. 1 Within this framework, nurses serve as foundational contributors, exerting a substantial influence on both patient outcomes and the broader quality of care provided. 2 Despite their central role, limited attention has been directed toward assessing nurses’ Professional Quality of Life (ProQoL) in the UAE context. ProQoL is a key indicator of mental health, job satisfaction, and clinical performance among healthcare professionals. 3 Elevated ProQoL is associated with increased compassion satisfaction, improved emotional well-being, and enhanced motivation in the workplace—factors that collectively support the delivery of compassionate and effective care.4,5 Conversely, diminished ProQoL—marked by burnout and secondary traumatic stress—is linked to a range of adverse outcomes, including substance use, emotional disengagement, reduced care quality, job dissatisfaction, and increased turnover among nursing staff.6–8
Nursing is inherently demanding, both physically and emotionally, and these demands have a substantial impact on ProQoL. Long working hours, irregular shifts, and routine exposure to pain, trauma, and death place nurses at heightened risk for psychological distress and fatigue. 9 Accordingly, ProQoL has garnered increasing interest among healthcare researchers and administrators due to its implications for workforce sustainability and patient safety. 10 Conceptually, the original Professional Quality of Life Scale (ProQoL), developed by Stamm, comprises 30 items and is designed to capture both the rewarding and adverse aspects of caregiving. It is typically conceptualized along two primary dimensions: compassion satisfaction (CS) and compassion fatigue (CF).11,12 The CF dimension has been further delineated into two constituent subcomponents: burnout (BO) and secondary traumatic stress (STS). 11 However, compassion fatigue has also been characterized as a broader construct that encompasses both burnout and secondary traumatic stress symptoms arising from prolonged exposure to others’ suffering.11,13 Figley 14 defines compassion fatigue as the cost of caring for others or for their emotional pain, resulting from a sustained desire to support individuals experiencing traumatic events. Additional terms used to describe this construct include “empathy burnout,” “vicarious traumatisation,” and “secondary traumatic stress.” Within this conceptual framework, STS is regarded as a central component of compassion fatigue rather than an entirely independent dimension. CS reflects the fulfillment derived from helping others, whereas CF includes the dual burdens of burnout and secondary traumatic stress (STS). Burnout is commonly attributed to systemic stressors, such as excessive workloads and insufficient organizational support, 15 while STS results from repeated exposure to patients’ suffering and trauma. Though distinct, burnout and STS frequently co-occur, compounding their negative effects and undermining both emotional resilience and professional competence. 16 Compassion fatigue has far-reaching consequences, including heightened staff attrition, diminished productivity, increased incidence of medical errors, compromised patient outcomes, and financial burdens for healthcare systems. Notably, burnout has been identified as a major determinant of reduced patient safety and clinical care quality. 17
A variety of instruments have been developed to assess ProQoL, with the most widely adopted being the 30-item Professional Quality of Life Scale (ProQoL). 18 This tool evaluates three core constructs: CS, burnout, and STS, and has been translated and validated in multiple languages and cultural contexts.19–21 Nonetheless, concerns have been raised regarding item clarity and the structural validity of the original scale, prompting calls for more streamlined alternatives. 22 Translation and validation studies have highlighted challenges in the ProQoL's factorial and internal consistency, particularly in the absence of foundational factorial validation prior to its widespread adoption. 23 Meta-analytical evidence suggests that internal consistency problems are more pronounced in studies using translated versions, although factor structure issues have also been reported in the original English version. Moreover, several scholars have recommended a psychometric re-examination of the burnout and STS subscales.19–25
In response to these limitations, the Short Professional Quality of Life Scale (Sh-ProQoL) was introduced in 2020. Comprising nine items across three subscales—CS, CF, and burnout (BO)—this shortened version was initially validated among Spanish palliative care providers. 12 The Sh-ProQoL was designed to retain the theoretical strengths of the original scale while offering improved brevity, clarity, and utility in clinical settings. Despite its conceptual and practical advantages, the instrument has yet to be validated among Arab nursing populations, underscoring the need for rigorous cross-cultural psychometric evaluation. To address this gap, the current study undertook a linguistic and cultural validation of the Arabic version of the Sh-ProQoL (Ar-Sh-ProQoL) as part of a broader research initiative. The primary aim was to examine its reliability and validity, ensuring that the Ar-Sh-ProQoL is both linguistically appropriate and culturally sensitive to the diverse experiences of Arab nurses working in Dubai healthcare settings.
Materials and methods
Aim
The primary aim of this study was to examine the psychometric properties—including reliability and validity—of the Ar-Sh-ProQoL among nurses.
Study design
This was a cross-sectional, methodological study.
Participants and setting
Participants were Arab nurses recruited from various healthcare facilities in Dubai, United Arab Emirates, using a convenience sampling approach. Eligibility criteria included: (a) being a registered nurse aged 18 years or older; (b) having at least one year of clinical nursing experience; (c) full-time employment in a clinical nursing role; and (d) willingness to participate with informed consent. Nurses were excluded if they: (a) were absent during the study period; (b) had less than six months of clinical experience; (c) completed fewer than 80% of the questionnaire items; or (d) declined to participate.
Sample size
Sample size requirements for exploratory factor analysis (EFA) were estimated using a commonly recommended 20:1 subject-to-item ratio. 26 Given the nine-item structure of the ProQoL, a minimum of 180 participants was required. To account for potential non-responses, the sample size was increased by 10%, resulting in a target sample of at least 200 participants, which was achieved.27,28
Data collection
Prior to data collection, all eligible participants received information about the study's objectives and methodology. They were informed that participation was voluntary, that responses would remain confidential, and that data would be anonymized in the final analysis. Written informed consent was obtained from each participant. Following consent, participants completed the Arabic Sh-ProQoL questionnaire. A subsample of 30 nurses was randomly selected to complete the same questionnaire again after a two-week interval, enabling the assessment of test–retest reliability and temporal stability of the instrument in this population.
Instruments
Short professional quality of life scale
The Sh-ProQoL, developed by Galiana et al., 12 comprises nine items distributed across three subscales: burnout (BO), CF, and CS. Each subscale includes three items rated on a 5-point Likert scale ranging from 1 (never) to 5 (very often), with subscale scores calculated by summing the respective items. Scoring thresholds for the CS subscale define scores below 10 as “low,” scores of 11–13 as “average,” and scores of 14 or above as “high.” For the BO subscale, scores of 6 or below are classified as “low,” 7–8 as “average,” and 9 or above as “high.” For CF, scores of 4 or lower indicate “low,” a score of 5 denotes “intermediate,” and scores of 6 or above indicate “high” levels of fatigue.20,29
Intention to leave (ITL)
Intent to leave was assessed using a single item evaluating the likelihood of job departure: “If you had the opportunity to leave your current workplace, would you do so?” Responses were rated on a 5-point Likert scale, where 1 represented “strongly disagree” and 5 represented “strongly agree.” Higher scores reflected a stronger intention to leave one's current position.30,31
Job satisfaction (js)
Job satisfaction was evaluated using a single item: “Considering all things, how satisfied are you working in your current setting?” Responses were captured on a 5-point Likert scale ranging from 1 (“strongly dissatisfied”) to 5 (“strongly satisfied”), with higher scores indicating greater overall satisfaction with one's current role.8,32
Perceived quality of care (PQC)
Perceived quality of care was measured using the item: “How would you rate the unit's nursing care quality in the last three months?” Participants responded on a 4-point Likert scale ranging from 1 (“very low”) to 4 (“very high”), with higher scores reflecting better perceived quality of care provided by the unit.33,34
Translation and cultural adaptation
The Ar-Sh-ProQoL underwent a rigorous forward-backward translation process to ensure linguistic accuracy and cultural appropriateness. The translated and back-translated versions were cross-referenced, and expert reviewers provided feedback to refine content while preserving the original meaning. This process followed the World Health Organization's guidelines for the cultural adaptation of assessment instruments, which include five systematic steps: forward translation, expert review, backward translation, pre-test/cognitive interviews, and final version development. 35 A qualitative pre-test involving 10 nurses was subsequently conducted to assess language clarity and content validity. Based on participant feedback, minor revisions were made to address ambiguous wording. This approach ensured that the final version was linguistically accurate and culturally appropriate for the target population.
Data analysis
Descriptive statistics were used to summarize participant characteristics. Continuous variables were analyzed using means and standard deviations, while categorical variables were reported as frequencies and percentages. Internal consistency of the Ar-Sh-ProQoL and its subscales was assessed using Cronbach's alpha. Test–retest reliability was examined over a two-week interval using intraclass correlation coefficients (ICCs), with values between 0.61 and 0.80 indicating strong agreement and values above 0.81 indicating excellent agreement. 27 Floor and ceiling effects were evaluated by calculating the proportions of participants who obtained the lowest and highest possible scores, respectively. 28
EFA was conducted to assess the dimensionality of the Ar-Sh-ProQoL, using principal component extraction with Varimax rotation to identify the underlying factor structure. Principal component analysis (PCA) with Varimax rotation is widely utilized as a rapid, stable, and practical approach for data reduction and for clarifying simple factor structures, particularly during preliminary analytical stages, and remains one of the most commonly applied techniques in practice due to its strong interpretability. 36
Sampling adequacy and factorability were evaluated using the Kaiser-Meyer-Olkin (KMO) test and Bartlett's test of sphericity. Factors with eigenvalues greater than 1.0 were retained, and items with factor loadings ≥0.40 were considered acceptable. 27
Convergent validity was assessed by comparing composite reliability (CR) values to average variance extracted (AVE) values, and by calculating Pearson correlation coefficients between the Ar-Sh-ProQoL and external measures: JS, PQC, and ITL. Correlations were interpreted as strong (r > 0.50), moderate (r = 0.35–0.50), or weak (r < 0.35). Convergent validity was considered adequate when CR exceeded AVE for each subscale. Discriminant validity was established by comparing the mean shared variance (MSV) with the AVE, with AVE > MSV indicating satisfactory discriminant validity.37,38
Confirmatory factor analysis (CFA) was conducted using AMOS version 24.0 (IBM Corp.) to test the hypothesized factor structure. 23 Model fit was evaluated using multiple indices: Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), and Incremental Fit Index (IFI), with values >0.90 considered acceptable. Error indices, including the root mean square error of approximation (RMSEA), root mean square residual (RMR), and standardized root mean square residual (SRMR), were considered acceptable at values <0.08. A chi-square to degrees of freedom ratio (CMIN/df) of less than 5.0 was also used to indicate acceptable model fit.37,39
Results
Participants
In total, 200 nurses completed the questionnaires. The average time to complete the instruments was approximately 5 min. The majority of the participants were female (57%) and between 25 and 35 years old (51.5%). Table 1 shows the characteristics of the participants.
Basic socio-demographic and experience profiles of participants.
Item analysis
The item–subscale correlation coefficients for the Ar-Sh-ProQoL exceeded the recommended threshold of 0.30 (see supplementary file Table S1), indicating strong conceptual alignment between individual items and their corresponding subscales. Pearson correlations showed moderate and negative correlation between compassion satisfaction and burnout (r = −0.45, p < 0.01) and compassion fatigue (r = −0.35, p < 0.01), but burnout was positively associated with compassion fatigue (r = 0.42; p < 0.01). These findings support the scale's construct validity and its coherence as a measure of professional quality of life (see supplementary file Table S2).
Internal consistency
Subscale-level reliability coefficients ranged from 0.80 to 0.84, indicating acceptable to strong internal consistency (Table 2). McDonald's omega values for all subscales were ≥ 0.70, further supporting the reliability of the instrument. ICCs across two-time points were excellent for all three subscales, indicating good test-retest reliability of the instrument. No floor or ceiling effects were observed, indicating the scale's sensitivity in capturing a full range of responses (Table 2). Collectively, these results support the robustness of the Ar-Sh-ProQoL as a reliable tool for assessing professional quality of life among nurses.
Floor effect, ceiling effect, and reliability for the Ar-Sh-ProQoL.

Note: SD standard deviation, ω = McDonald's omega coefficient, ICC Infraclass correlation coefficient, a test-retest reliability for 30 participants.
Dimensionality
EFA revealed a three-factor solution (see supplementary file Table S3). The KMO value was 0.81, and Bartlett's test of sphericity was statistically significant (χ2 = 778.67, p < 0.01), indicating that the sample was appropriate for factor analysis. The extracted factors corresponded to the theoretical structure of the instrument: three items loaded on “Burnout,” 3 items on “compassion fatigue,” 3 items on “compassion satisfaction.’’ All factor loadings were acceptable, with the lowest value reported at 0.73, providing further support for the construct validity of the scale components.
Construct validity
CFA was conducted to compare the fit of one, two and three-factor models of the Ar-Sh-ProQoL. The one-factor model, in which all nine items were loaded onto a single latent construct, demonstrated poor fit, with fit indices falling below conventional thresholds (RMSEA = 0.12, CFI = 0.62, TLI = 0.50). The two-factor model also did not show adequate fit (RMSEA = 0.10, CFI = 0.81, TLI = 0.74).
In contrast, the hypothesized three-factor model, representing compassion satisfaction, compassion fatigue, and burnout, demonstrated a substantially better fit to the data. Model fit indices met or exceeded the accepted thresholds, supporting the multidimensional structure of the scale (RMSEA = 0.04, CFI = 0.98, TLI = 0.97). Fit statistics for both models are presented in Table 3, and structural diagrams are provided in Figure 1.
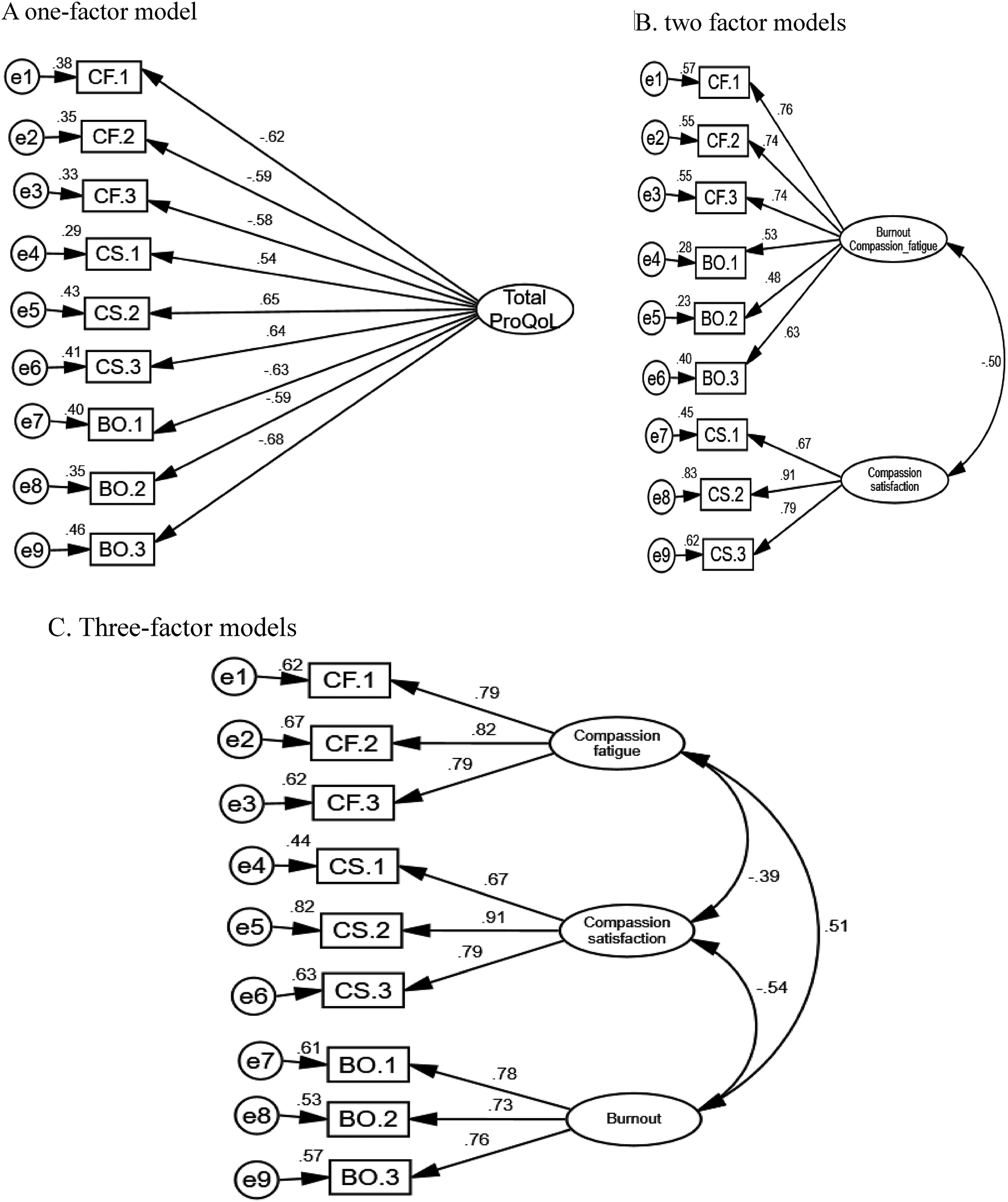
Graphical summary of one-factor and three-factor models.
Model fit statistics of confirmatory factor analysis for the Ar-Sh-ProQoL.

Note: CFI: comparative fit index; GFI: goodness of fit index; TLI: Tucker–Lewis Index; IFI: incremental fit index; RMSEA: The Root Mean Square Error of Approximation; CMIN: Chi-square Value; Df: degree of freedom.
Convergent and discriminant validity
The Ar-Sh-ProQoL demonstrated strong convergent validity. All subscales showed CR values above 0.70 (range: 0.84–0.88), and AVE values ranged from 0.75 to 0.80 (Table 4). As CR values exceeded AVE across all subscales, convergent validity was confirmed. Furthermore, significant correlations were observed between the Ar-Sh-ProQoL and related external constructs: job satisfaction (r = 0.51), perceived quality of care (r = 0.45), and intention to leave (r = 0.48), providing additional evidence of convergent validity.
Indicators of convergent validity and divergent validity of the Ar-Sh-ProQoL.

Note: AVE average variance extracted. CR Composite reliability, Bold diagonals are the squared root of AVE, and off-diagonals are correlations.
Discriminant validity was supported by comparisons of AVE, MSV and CR. In all cases, AVE values exceeded MSV values and CR values exceeded AVE for all subscale indicating that the subscales were more strongly related to their own constructs than to each other, and confirming good discriminant validity (Table 4).
Discussion
This study provides robust evidence supporting the psychometric soundness of the Arabic version of the Short Professional Quality of Life Scale (Ar-Sh-ProQoL) for use among Arab nurses. A key strength of this work lies in the rigorous cross-cultural adaptation process employed, which followed internationally recognized guidelines. The translation protocol included forward and backward translation, expert panel review, and pilot testing, ensuring both linguistic accuracy and cultural relevance. This comprehensive approach aligns with best practices in instrument adaptation and underscores the importance of cultural sensitivity in preserving content validity and construct integrity across diverse populations. 35
The Ar-Sh-ProQoL demonstrated strong reliability and validity for assessing CS, burnout (BO), and CF in Arabic-speaking clinical contexts. Internal consistency of the three subscales exceeded the recommended Cronbach's alpha threshold of 0.70, indicating acceptable to high reliability. These findings are consistent with those of prior validation studies conducted on the original English version 12 and other translated adaptations,40,41 reinforcing the scale's reliability within this population.
Construct validity was confirmed through both exploratory and confirmatory factor analyses. The EFA identified a three-factor solution corresponding to the original subscales—CS, BO, and CF—with all item loadings exceeding the acceptable threshold of 0.40. 28 This structural pattern mirrors findings from other international validations, 40 suggesting the scale's latent structure is both robust and culturally adaptable. CFA results further supported the proposed three-factor model, with fit indices surpassing conventional cutoffs, confirming the structural validity of the Arabic version and its alignment with the original theoretical framework.
Evidence of nomological validity was demonstrated through the expected pattern of correlations between the Ar-Sh-ProQoL and related constructs. The scale showed strong positive associations with JS and PQC, and a negative association with ITL, consistent with existing literature. 42 In particular, the inverse relationship between ProQoL scores and ITL supports the premise that higher professional quality of life is associated with lower intent to leave one's position—an association repeatedly documented in research on healthcare workforces.8,42,43
The importance of validating the Sh-ProQoL lies in its brevity, clinical feasibility, and theoretical alignment with the original instrument. Although originally developed by Stamm, the initial Sh-ProQoL lacked evidence regarding its factorial validity, as only reliability metrics such as Cronbach's alpha were reported. 44 This study addresses that gap by providing empirical support for the scale's latent structure and psychometric robustness. Given the relative lack of research focusing specifically on nurses—a vital but often understudied segment of the healthcare workforce—this study contributes valuable evidence for the application of the Sh-ProQoL in both research and practice. The validated scale offers a pragmatic and theoretically sound tool for healthcare administrators seeking to assess and enhance nurses’ well-being, workplace satisfaction, and retention through targeted interventions.
Conclusion
The findings of this study confirm that the Ar-Sh-ProQoL possesses strong psychometric properties, supporting its use as a reliable and valid instrument for assessing professional quality of life among Arabic-speaking nurses in Dubai hospitals. Its cultural relevance, brevity, and structural integrity make it well suited for both clinical and research applications in Dubai healthcare settings.
Practical implications for nursing practice
The Ar-Sh-ProQoL provides healthcare administrators and policymakers with a culturally adapted tool to assess and monitor nurses’ professional quality of life. Routine use of the instrument can help identify issues related to compassion satisfaction, burnout, and fatigue, enabling timely, targeted interventions to support nurses’ psychological well-being, reduce turnover, and improve patient outcomes. Its implementation may also guide strategies to enhance workplace satisfaction and organizational resilience within nursing teams.
Limitations and directions for future research
Despite its strengths, this study has several limitations. First, reliance on self-report data may introduce response biases and limit objectivity. Second, the sample was restricted to nurses working in a single geographical area, which may constrain the generalizability of the findings across broader Arabic-speaking populations. Third, although single-item measures were employed to reduce respondent burden in a clinical setting, prior research indicates that such indicators may be acceptable for assessing global constructs, such as job satisfaction. Nevertheless, future studies should consider the use of multi-item instruments to provide more comprehensive evidence of validity. Future studies should investigate the longitudinal stability of the Ar-Sh-ProQoL and validate its applicability in other Arab countries and diverse healthcare contexts. Such efforts will further establish the instrument's utility across settings and contribute to the development of culturally sensitive well-being measures in global nursing research.
Supplemental Material
sj-docx-1-wor-10.1177_10519815261445915 - Supplemental material for Psychometric properties of the Arabic version of the short professional quality of life scale in nurses
Supplemental material, sj-docx-1-wor-10.1177_10519815261445915 for Psychometric properties of the Arabic version of the short professional quality of life scale in nurses by Hasan Alelayan in WORK
Supplemental Material
sj-docx-2-wor-10.1177_10519815261445915 - Supplemental material for Psychometric properties of the Arabic version of the short professional quality of life scale in nurses
Supplemental material, sj-docx-2-wor-10.1177_10519815261445915 for Psychometric properties of the Arabic version of the short professional quality of life scale in nurses by Hasan Alelayan in WORK
Supplemental Material
sj-docx-3-wor-10.1177_10519815261445915 - Supplemental material for Psychometric properties of the Arabic version of the short professional quality of life scale in nurses
Supplemental material, sj-docx-3-wor-10.1177_10519815261445915 for Psychometric properties of the Arabic version of the short professional quality of life scale in nurses by Hasan Alelayan in WORK
Footnotes
Acknowledgments
The author would like to thank Mr Afif Mahmoud AlQadiry and Ms. Ebtisam Abdul Wahed Saleh Ali for their generous help in facilitating data collection. We appreciate all of the subjects for their participation. We also thank Phoebe Chi, MD, MPH, for editing the English text of a draft of this manuscript.
Ethical considerations
The study was approved by the Dubai Scientific Research Ethics Committee (DSREC-11/2024_43) and the Mohammed Bin Rashid University of Medicine and Health Sciences Medical Ethics Committee (MBRU; IRB-2024-555). All procedures were conducted in accordance with ethical guidelines, with particular attention to voluntary participation, informed consent, and participant anonymity.
Informed consent
Not applicable.
Funding
The author declares that no financial support was received for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.