
Abstract
Background
Healthcare workers faced immense challenges during the early COVID-19 pandemic, contributing to their psychological distress. Female workers have been shown to be at higher risk, but most studies only measured birth-assigned sex, thereby overlooking sociocultural (gender) differences.
Objective
To examine the respective roles of sex and gender in the association between COVID-19–related occupational stressors and psychological distress among healthcare workers over time during the early phase of the pandemic.
Methods
This longitudinal study examined 382 Canadian healthcare workers (12.8% male, 87.2% female; 92.9% white) monitored weekly over 8 weeks during the first two waves of the pandemic. Using sociodemographic and work data, we developed a composite gender index and investigated how sex, gender, and COVID-19-related stressors related to psychological distress (anxiety, depression, posttraumatic stress) using linear mixed models.
Results
COVID-19-related stressors were associated with higher distress. A more feminine gender score, but not female sex, predicted higher distress. A modest interaction was observed based on a small subgroup, suggesting lower anxiety and posttraumatic stress among medically vulnerable workers with higher feminine gender scores. Overall distress decreased modestly over time, although models explained a limited proportion of variance.
Conclusion
These findings underscore the need to go beyond birth-assigned sex in mental health assessments of healthcare workers during public health crises.
Keywords
Introduction
Owing to the nature of their work, healthcare workers faced emergent work-related challenges during the COVID-19 pandemic.1,2 Greater need for healthcare required network-wide reorganization of care and rapid learning of new protocols3–5 while facing personal protective equipment (PPE) shortages.6,7 Challenges already present in the healthcare sector were also exacerbated, such as the amount of overtime and contagion risks at work. 8 It also increased exposure to critical events such as the death of patients or colleagues. 9
This situation has been described through the lens of workplace stress (e.g., Barello et al. 10 ). According to the Job Demands-Resources (JD-R) theory, workplace stress is the result of a transaction in which job demands, or stressors, are perceived by a worker as greater than the available resources to meet them. 11 The previously mentioned aspects of healthcare work during the pandemic, including PPE shortages, can therefore be considered in the job demands category, as they add workload and mental burden.6–7 Studies have, however, highlighted that stressors outside of work have a great impact on the psychological distress of workers, which can lead to overestimation of the effects of work-related factors when they are not taken into account. 12 During a pandemic, the health of both relatives and individuals is a frequent subject of fear, especially in the case of preexisting health conditions.13–14 Significant upheavals caused by being quarantined 15 and losing income 16 also negatively impact mental health.
Numerous studies have linked stressors encountered at work during the pandemic by healthcare workers6,17,18 to significant negative psychological consequences.19,20 These workers are at high risk of experiencing psychological distress, characterized by symptoms such as depression, anxiety, and posttraumatic stress.21,22 While resources are integral to the JD-R model, some studies suggest that job demands, but not resources, predict the psychological distress of workers during the early stage of the pandemic.6,23
Systematic reviews and meta-analyses of studies conducted during the first wave of infection among healthcare workers reported prevalence rates ranging from 20–55% for anxiety symptoms, 19–60% for depressive symptoms, and 2–57% for posttraumatic stress symptoms.20,24 These results are comparable to those observed during other pandemics among these same workers.19,25 At the occupational level, psychological distress among workers has consequences for the effectiveness of the healthcare network considering its relationship with absenteeism, 26 turnover intentions, 27 and decreased performance.28,29
While a momentary increase in psychological distress is a normal response to challenging events, its chronicity and magnitude are of greater concern for the wellbeing of workers. 30 Lasting and elevated psychological distress increase, for example, the risk of developing a psychiatric disorder31,32 and health conditions. 33 Longitudinal studies conducted during the early pandemic noted an overall decrease in psychological distress levels over this period.34,35 These levels have been reported to increase or remain elevated in a minority of Canadian healthcare workers. 36 While COVID-19-related occupational stressors have been associated with psychological distress in the healthcare sector, it is important to assess precisely the conditions that might lead some healthcare workers to experience more important and lasting psychological distress. However, it remains difficult to describe how such factors influence the trajectory of psychological distress, as the majority of studies evaluating factors related to the mental health of healthcare workers during the pandemic have used cross-sectional designs (e.g., Busch et al. 19 ).
Sex and gender among workers
Notably, working conditions are not experienced the same way by every worker. Personal characteristics can affect the way work conditions are evaluated by workers and their consequences. 37 Consistent with previous studies on mental health,38–40 female healthcare workers were more at risk during the pandemic for experiencing anxiety, depression, and posttraumatic stress symptoms than their male peers were.41,42 However, while studies on the subject tended to use both terms interchangeably, they solely analysed data according to birth-assigned sex groups (i.e., sex) and not gender. Sex refers to biological attributes such as chromosomal sex, hormonal profiles, and reproductive anatomy. It is distinct from gender, the characteristics associated socioculturally with sex. 43 Gender socialization occurs in response to birth-assigned sex and shapes the development of one's identity. 44 It contributes to forms of gender expression that are broadly organized along a continuum between femininity and masculinity.44,45
The conflation of gender with sex makes it difficult to clarify which factors are propounded to be responsible for observed differences. 46 It can also lead to an overestimation of the homogeneity of both sexes in terms of lived experiences and characteristics. 47 As gender socialization is a complex and dynamic process, individuals of the same sex can indeed exhibit traits and behaviors that each reflect or defy gendered expectations to different degrees 44 To address this nuance, a data-driven diagnostic approach to gender can be used. 48 This approach operates on the premise that psychosocial differences observed between sexes can serve as proxies for gendered experiences. 49 As it is descriptive, it allows gendered markers to emerge organically from the specific study population, ensuring the measure is contextually sensitive.48,49
An individual's sex and gender play significant roles in both the type and frequency of stressors to which they are exposed and in how those stressors are assessed and managed. 37 For this reason, both are presumed to contribute to observed sex differences in the prevalence of psychological distress. 50 Studies have indeed revealed that some COVID-19-related stressors and fears are strongly related to symptoms of psychological distress in female healthcare workers.51,52 The factors driving these sex differences remain unclear. Proposed explanations include biological mechanisms, such as differences in the stress response system, 39 and psychosocial mechanisms, such as differences in socialization regarding the expression of negative emotions.50,53
Healthcare is a female-dominated field in Western societies such as Canada.54,55 For this reason, identifying the main occupational determinants of psychological distress during a pandemic could provide valuable insights for preventive actions in the case of future pandemics. These results could also help identify specific between- and within-sex vulnerabilities in this female-dominated field to reduce mental health inequalities among workers.
For these reasons, the objective of this study is to describe how sex and gender influence the relationship between exposure to COVID-19-related job stressors and psychological distress over time among healthcare workers during the early stage of the pandemic.
Methods
Participants
This prospective cohort study collected self-reported data through a mobile application during the first and second waves of COVID-19, between May 8, 2020, and January 24, 2021, in the province of Quebec, Canada. The design used methodological aspects of the Ecological Momentary Assessment (EMA) methodology, 56 as participants were asked to use a mobile application weekly to complete several questionnaires. Data collection was anonymous, confidential, and voluntary. The research ethics board of the University of Montreal Hospital Research Centre approved the research project. We obtained written consent from every participant before their participation.
Recruitment
Eight healthcare institutions in the province of Quebec participated in our study. The research team began by contacting research coordinators from each institution. Promotional materials were distributed through various platforms to reach all employees. Workers interested in the study transmitted their consent through a web form or by directly emailing the research coordinator. Following the receipt of the consent form, as well as sociodemographic and professional information from participants, instructions for installing the mobile application Ethica were sent to them to start data collection. Eight hundred and seventy-two health care workers were enrolled in the study. A total of 410 participants who did not answer the three distress questionnaires at least six times over the monitored period and 80 who did not answer the posttest retrospective questionnaire were excluded. Analyses were performed on the remaining 382 participants.
Protocols
Two collection strategies were employed to collect the data. First, the participants were asked to use the mobile application for a period of 12 weeks. During this time period, participants completed weekly questionnaires assessing psychological distress indicators. Due to participation attrition, only 8 weeks of data were retained for analyses. Second, at the end of the monitoring period, all registered participant received a link to an online survey on the SurveyMonkey platform. The online survey contained retrospective items about the COVID-19-related stressors that participants had experienced during the same period.
During this study, participants whose psychological distress scores exceeded the clinical threshold received a message at the end of the questionnaires to encourage them to contact help resources. The participants who reported thoughts of death or self-harm were given a list of resources to contact. They were also contacted first by email by a member of the research team and then by phone if they did not answer in the following days.
Measures
Psychological distress was assessed weekly via three indicators: symptoms of (i) anxiety, (ii) depression, and (iii) posttraumatic stress. The lookback period for symptoms was changed from the commonly used two weeks (GAD-7 and PHQ-9) or one month (PCL5–8) to a single week. Weekly global scores were calculated for each instrument.
Anxiety
The French version of the General Anxiety Disorder-7 (GAD-7) assesses symptoms of anxiety. The GAD-7 is a self-reported standardized questionnaire composed of seven items that assess how frequently in the last seven days the respondents experienced stated anxiety symptoms via a four-point frequency scale ranging from 0 = not at all to 3 = nearly every day. 57 The clinical cut-off score for moderate to severe symptoms is 10. Its internal consistency was good for both sexes (Cronbach's alpha: male = .91, female = .89).
Depression
The French version of the Patient Health Questionnaire (PHQ-9) was used to assess symptoms of depression. The PHQ-9 is a self-reported standardized questionnaire composed of nine items that assess how frequently in the last seven days the respondents experienced stated depressive symptoms using an identical scale to the GAD-7. 58 The clinical cut-off score for moderate to severe symptoms is 11. Its internal consistency was also good for both sexes (Cronbach's alpha: male = .86, female = .87).
Posttraumatic stress
The French translation of the short version of the Posttraumatic Stress Disorder Checklist for Diagnostic and Statistical Manual of Mental Disorders, fifth edition (PCL5–8), was used to assess posttraumatic stress. The PCL5–8 is a self-reported standardized questionnaire composed of eight items measuring how much the respondents were bothered by posttraumatic stress symptoms during the past seven days via a five-point scale ranging from 0 = not at all to 4 = extremely. 59 The clinical cut-off score for moderate to severe symptoms is 13. The internal consistency of the resulting scale was also good for both sexes (Cronbach's alpha: male = .92, female = .89).
COVID-19-related stressors
COVID-19-related stressors were evaluated in the online survey via retrospective questions covering the monitoring period. The participants were asked to indicate whether they had encountered each situation individually during the monitored period. The information was recorded with 0 = no and 1 = yes. Assessed job stressors included PPE shortages; a lack of personnel; constraints affecting propagation risk reduction, such as confusing safety protocols; COVID-19 outbreaks at the unit; and COVID-19-related deaths of colleagues or patients. Assessed personal stressors included being quarantined, having lost income related to the COVID-19 pandemic, having COVID-19-related deaths of relatives, being positive on the COVID-19 test, and being vulnerable to COVID-19 for any medical reasons.
Sex
Birth-assigned sex was assessed as part of the sociodemographic information provided by the participants. The information was recorded as 0 = male and 1 = female.
Gender
On the basis of the validated methodological approach of Pelletier et al., 60 we produced a composite gender index based on sociodemographic and professional information previously reported to differ significantly across birth-assigned sex groups.61–64 The variables that were selected for the initial screening and selection process, all self-reported, intended to capture the multidimensional nature of gender by integrating sex-related components as they manifest specifically within this cohort. 60 Using a composite index provides several methodological advantages: it reduces model complexity, increases statistical power, and allows for the retrospective analysis of gender in datasets where it was not directly measured. 48
Specifically, the variables were 1) history of having consulted a professional or taken work leaves for mental health reasons (recorded with 0 = no, 1 = yes); a history of having been exposed to situations such as 2) fire, 3) physical aggression, 4) armed aggression, 5) unwanted or uncomfortable sexual behaviors, or 6) violent death (recorded each with 0 = no, 1 = yes); 7) employment in high-risk environments for contamination, such as COVID-19 wards, elderly care, emergency care, and intensive care units (recorded with 0 = no, 1 = yes); 8) taking care of another family member (elderly or person with disabilities); 9) having sought support from colleagues (recorded with 0 = no, 1 = yes), or 10) supervisors (recorded with 0 = no, 1 = yes) during the monitored period; 11) average level of fear experienced in the workplace during the monitored period (assessed using a scale of 1 to 5).
Following Pelletier et al., 60 our gender index was produced by first conducting a principal component analysis followed by a scree test with these sex-related variables. This was done to reduce their number. Logistic regressions were then conducted with the retained variables using sex as the dependent variable, removing nonsignificant variables one at a time in descending order on the basis of their p value. A propensity score was calculated using the remaining variables to produce the gender index. The resulting gender index is a continuous variable ranging from 0 to 1 expressing the degree to which an individual's psychosocial profile aligns with the one associated with female participants in the sample. A higher gender score therefore indicates a more “feminine” profile, whereas a lower score corresponds to a more “masculine” one.
Confounding Variable
Among the provided information, age was also accounted for as a confounding variable, as reviewed literature suggests that older individuals tend to experience less psychological distress than younger individuals do. 65
Data analyses
We performed the analyses in R version 4.3.2. Significance was set at α = 0.05 for all analyses. Missing psychological distress observations accounted for less than one percent of the data and were imputed via the last observation carried forward (LOCF) method. 66 T tests were performed to compare baseline scores between workers who completed the psychological distress questionnaires 5 times or less and those who completed them 6 times or more. There were no significant differences between the groups in terms of anxiety, depression, or posttraumatic stress (P > 0.05). Pearson and point-biserial correlations were used to screen for multicollinearity. No variable pair added to a single model had correlation score above .50.
We then performed linear mixed model analyses to assess the effects of age, sex, gender, and COVID-19-related stressors on psychological distress over time via the lmer package (version 1.1–35.1). Models were compared on the basis of their Akaike information criterion (AIC) values. Anxiety, depression, and posttraumatic stress were each individually used as the dependent variables in different models. We followed a step-up model-building strategy for each dependent variable, as described by West et al. (p.40) 67 : we first identified an unconditional model, with the fixed effect intercept as the only fixed effect parameter.
To test for both linear and nonlinear growth trajectories of psychological distress across time, random intercepts for linear, quadratic, and cubic slopes were added one at a time. This additionally accounted for individual differences in baseline psychological distress in our models. The fit of each unconditional model was then compared. The intraclass correlation coefficients (ICCs) for the anxiety, depression, and posttraumatic stress unconditional models were .69, .76, and .71, respectively. Fixed effects for age, sex, gender, time, and COVID-19-related stressors, as well as interactions between sex, gender, and stressors, were added sequentially to the models. Effects were retained on the basis of improved fit. Following Cohen's criteria, 68 marginal R2 values of .02, .13, and .26 were interpreted as representing small, medium, and large effect sizes, respectively. Figures were created using the ggplot2 package (vers. 3.5.1), and a table was created using the sjPlot package (vers. 2.8.16).
Results
A total of 382 healthcare workers aged 18 to 64 years (mean = 41.0, SD = 9.2) were retained for the study. The sample was predominantly female (female: n = 333, 87.2%; male: n = 49, 12.8%). A large majority identified as White (n = 355, 92.9%), whereas 6 identified as Hispanic (1.6%), 6 as Asian (1.6%), 3 as Arab or Western Asian (0.8%), 4 as Black (1.1%), and 8 identified as other groups (ex. : Indigenous; 2.1%). Figure 1 shows the distribution of gender scores according to sex. The mean (SD) gender score for the sample was .87 (.16), with a mean (SD) of .90 (.006) for females and .66 (.04) for males. A third (n = 192; 31.2%) worked in at least one of the following settings: the COVID ward (n = 63, 16.5%), the elderly care unit (n = 43, 11.3%), the emergency care unit (n = 27, 7.1%), or the intensive care unit (n = 23.6%). Over the monitored period, the mean (SD) anxiety, depression, and posttraumatic stress scores were 5.02 (3.24), 5.57 (3.83), and 5.79 (4.28), respectively. Almost two-thirds (59.4%) did not once reach a clinical cut-off score over the monitored period, whereas approximately one tenth (12.6%) reached at least one of any clinical cut-off scores for at least 4 weeks.
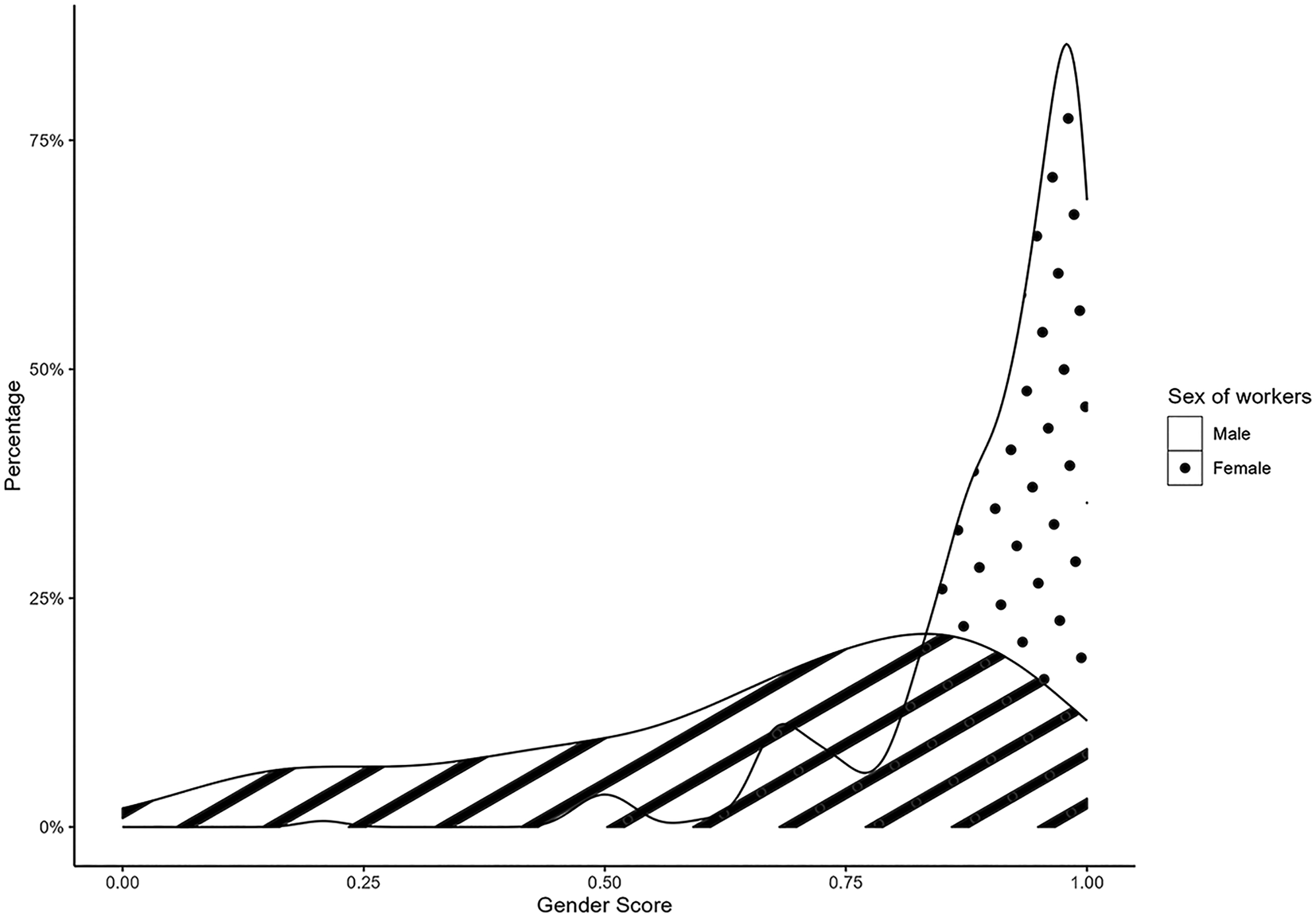
Distribution of gender scores according to sex among healthcare workers (n = 382)
Preliminary analyses
Six variables were retained for our gender index. A more feminine gender score was positively related to a history of having consulted a mental health professional (B = 0.88, p = .02), having been exposed to unwanted or uncomfortable sexual behaviors (B = 2.70, p < .001), employment in a unit at higher risk for contamination (B = 0,94, p = .01), having sought support from colleagues during the monitored period (B = 0.92, p = .01), and average level of fear experienced at work (B = 0.24, p = .008). It was negatively associated with having been exposed to armed aggression (B = −2.02, p < .001). The accuracy of the propensity score was 0.82 on the basis of its c value. The resulting gender score was moderately correlated with sex (0.50).
Linear mixed models
Table 1 shows the parameter estimates and the model fit for the final linear mixed models. Age, sex, loss of income, and interactions between gender, time, and stressors other than being vulnerable to COVID-19 did not improve fitness for the models and were not retained.
Linear mixed models of the predictors of psychological distress (n = 382).
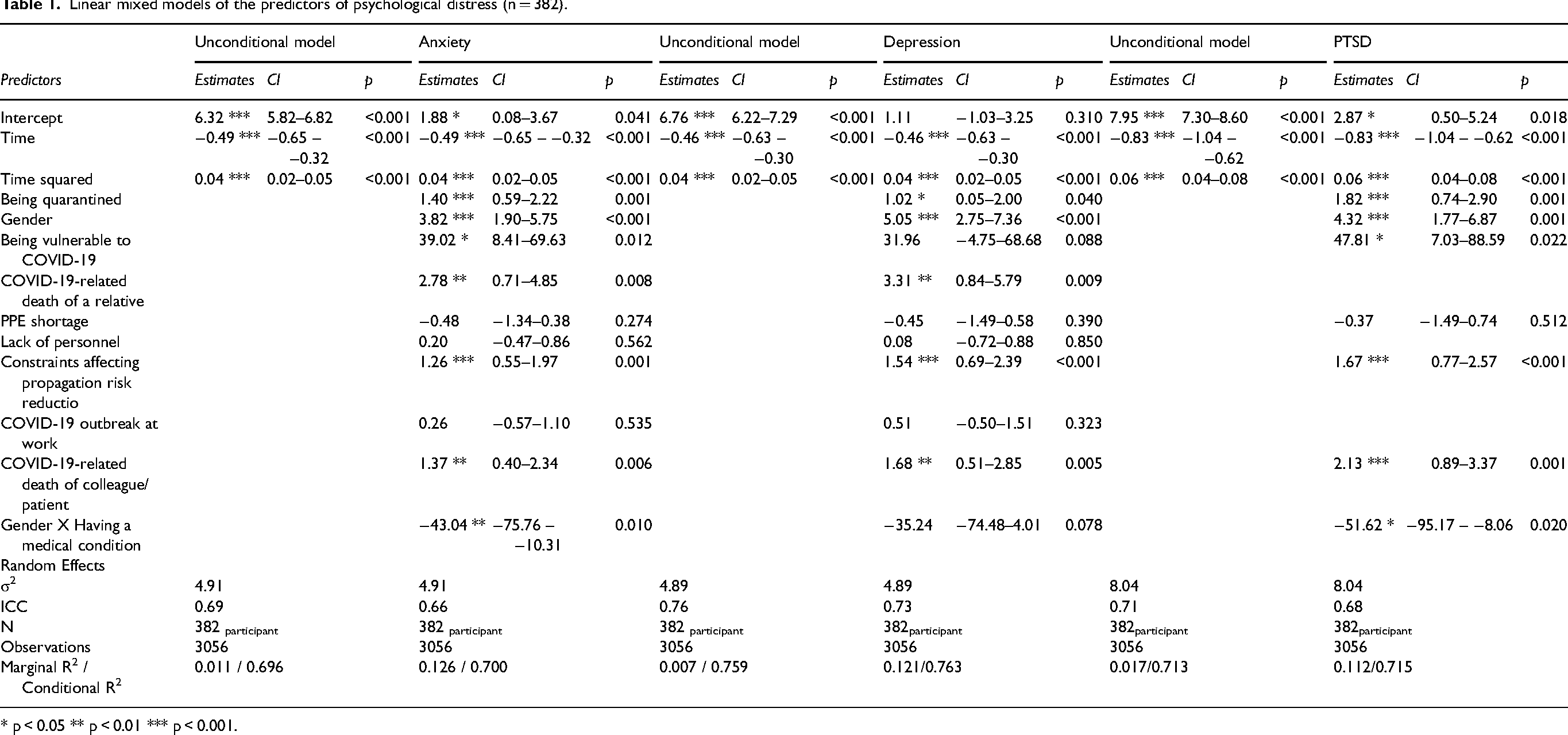
* p < 0.05 ** p < 0.01 *** p < 0.001.
Anxiety (B = 0.04, CI = 0.02–0.05, p < .001) gradually decreased over time (Figure 2(a)). There were significant positive associations with being quarantined (B = 1.40, CI = 0.59–2.22, p < .001), COVID-19-related death of a relative (B = 2.78, CI = 0.71–4.85, p = .009), constraints affecting propagation risk reduction (B = 1.26, CI = 0.55–1.97, p < .001), and COVID-19-related death of a colleague or patient (B = 1.37, CI = 0.40–2.34, p = .006). There was also a positive interaction effect between gender and being vulnerable to COVID-19 on anxiety (B = −43.04, CI = −75.76−10.31, p = .01). While anxiety was positively associated with a feminine gender score for participants who were not vulnerable to COVID-19, there was a negative association for those who were vulnerable (Figure 3(a)). The retained predictors predicted 12.6% of the variance in anxiety (Marginal R2=.126), an additional 11.5% compared with the unconditional model, with an ICC of .66.
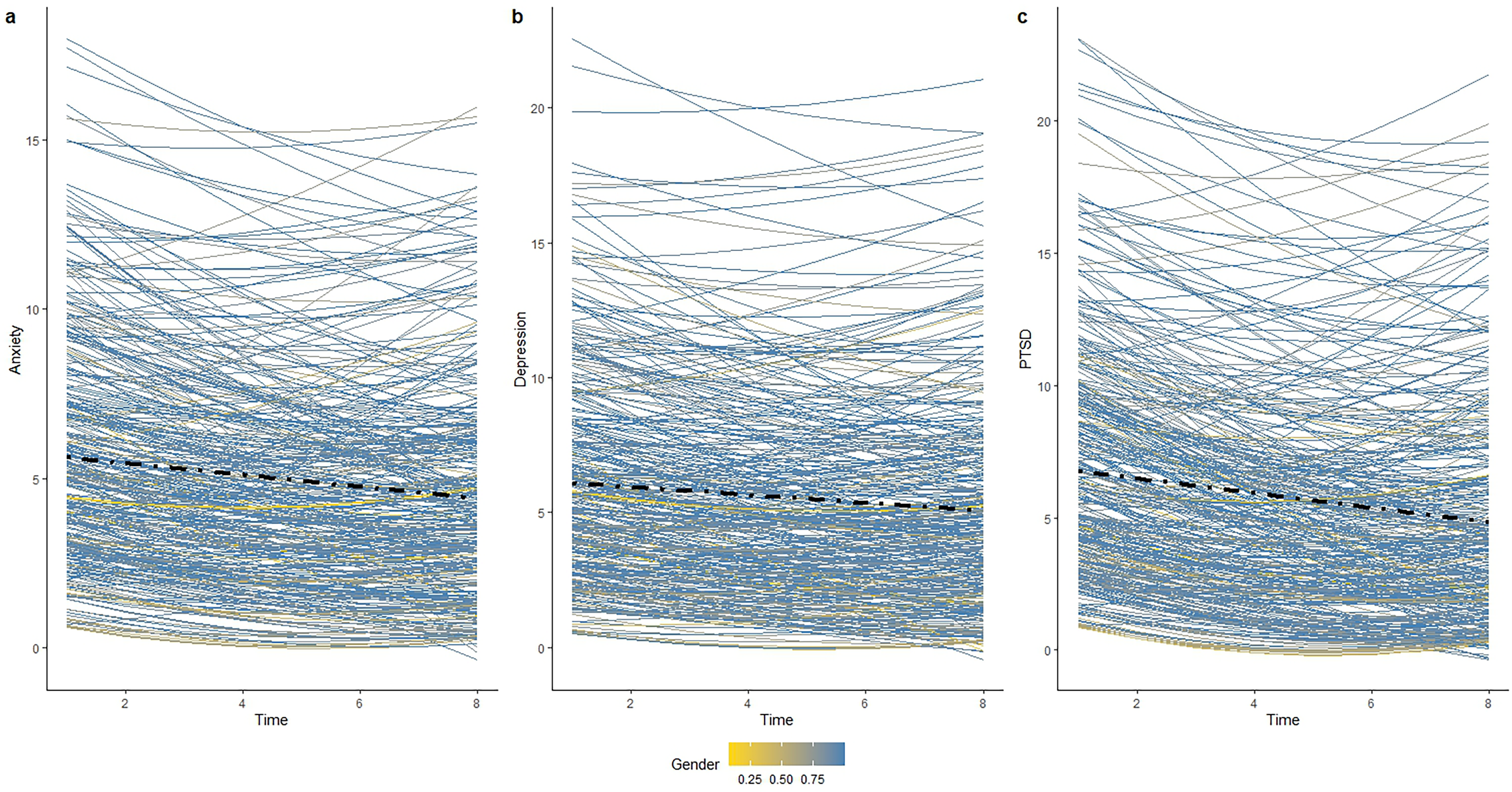
Psychological distress over time according to COVID-19-related stressors and gender (n = 382)

Effects of interactions between gender and vulnerability to COVID-19 on psychological distress (n = 382).
Depression (B = 0.04, CI = 0.02–0.05, p < .001) gradually decreased over time (Figure 2(b)). There were significant positive associations with the feminine gender score (estimate = 5.05, CI = 2.75–7.36, p < .001), being quarantined (B = 1.02, CI = 0.05–2.00, p = .04), COVID-19-related death of a relative (B = 3.31, CI = 0.84–5.79, p = .009), constraints affecting propagation risk reduction (B = 1.54, CI = 0.69–2.39, p < .001), and COVID-19-related death of a colleague or patient (B = 1.68, CI = 0.51–2.85, p = .005). The retained predictors predicted 12.1% of the variance in depression (Marginal R2 =.121), an additional 11.4% compared with the unconditional model, with an ICC of .73.
Posttraumatic stress (B = 0.06, CI = 0.04–0.08, p < 0.001) gradually decreased over time (Figure 2(c)). There were significant positive associations with being quarantined (estimate = 1.82, CI = 0.74–2.90, p < .001), constraints affecting propagation risk reduction (B = 1.67, CI = 0.77–2.57, p < .001), and COVID-19-related death of a colleague or patient (estimate = 2.13, CI = 0.89–3.37, p < .001). There was also a positive interaction effect between gender and being vulnerable to COVID-19 (B = −51.67, CI = −95.17−8.06, p = .02). While posttraumatic stress was positively associated with a feminine gender score for participants who were not vulnerable to COVID-19, there was a negative association for those who were vulnerable (Figure 3(b)). The retained predictors predicted 11.2% of the variance in posttraumatic stress (Marginal R2=.112), an additional 9.5% compared with the unconditional model, with an ICC of .68.
Discussion
This study examined how birth-assigned sex and psychosocial gender influenced the association between exposure to COVID-19-related stressors and psychological distress over time among healthcare workers during the early stage of the pandemic. First, COVID-19-related stressors contribute to greater psychological distress. Additionally, a feminine gender score was associated with greater psychological distress among our selected healthcare workers, independent of sex. Interactions between gender and being vulnerable to COVID-19 also influenced anxiety and posttraumatic stress symptoms.
Relationship between COVID-19-related stressors and psychological distress
As hypothesized, some COVID-19-related stressors contributed to psychological distress among healthcare workers during the early stages of the pandemic, although the effects were modest. Consistent with previous longitudinal studies (e.g., López Steinmetz et al., 35 symptoms of anxiety, depression, and PTSD decreased gradually. This pattern suggests adaptation to the pandemic's evolving challenges. They also remained below the clinical cut-off scores for moderate to severe psychological distress for the majority of workers. Interestingly, while similar groups of stressors influenced anxiety and depression, the COVID-19-related death of a relative did not appear to contribute to symptoms of PTSD among workers. Posttraumatic stress symptoms tend to manifest in relation to serious threats to health and security. 69 Because most COVID-19-related deaths involved older adults with preexisting medical conditions, 70 these events may not have been perceived as particularly threatening by healthcare workers’ relatives, even if they were distressing. Comparatively, the death of patients under their care or of colleagues who shared that responsibility might have been perceived as generally more traumatic to them.
In contrast to the findings of several previous studies (e.g., Britt et al., 6 PPE shortages, a lack of personnel, and the COVID-19 outbreak in the workplace did not appear to have contributed significantly to the psychological distress of workers. In terms of personal stressors, being positive for COVID-19 and having lost income did not. It is possible that differences in results across studies reflect different methodologies and time frames. Continuing our longitudinal study as the pandemic further unfolded might have captured the slowly increasing effects of specific stressors that could be further gendered. This also does not necessarily mean that these COVID-19-related stressors did not broadly lead to personal negative consequences for healthcare workers. For example, work dissatisfaction and symptoms of burnout might constitute more direct consequences of some of these stressors than symptoms of anxiety, depression, and posttraumatic stress.12,71 It is also worth noting that the sample included different healthcare professions, which introduces variations in work environments, responsibilities, and exposure profiles. Because the analyses did not adjust for these profession-specific working conditions, it is possible that some COVID-19-related stressors were not experienced with the same frequency, intensity, or relevance across the professional groups. This heterogeneity could have weakened associations between specific stressors and psychological distress. This may partly explain why some stressors did not emerge as significant predictors. It may also explain why the combined effect of the retained stressors on psychological distress appeared modest during the monitored period.
Overall, COVID-19-related stressors were associated with higher psychological distress among healthcare workers. However, distress levels remained low during the early phase of the pandemic. Our results could however suggest the importance of rapidly assessing and offering support to workers, who, for example, are more specifically exposed to grave situations such as work-related fatalities.
Sex and gender differences in psychological distress
We found differences in psychological distress among workers according to gender score but not by sex. These results are surprising given the well-documented sex differences in mental health,42,53 as well as the previously identified higher prevalence of psychological distress among female healthcare workers. 72 Fixed effects were added to the models in a stepwise fashion and retained based on model fit. Sex was also excluded before gender was introduced. These results therefore do not reflect a suppression effect.
However, the gender distribution of our sample, which was skewed toward femininity in both sexes, may help explain these findings. This distribution does not reflect highly distinct sociocultural groups but can be expected in an occupational setting such as healthcare. Indeed, healthcare is a female-dominated field, 54 which is at least in part related to the traditional relationship between caregiving and femininity. 73 Our gender distribution suggests that the experiences, roles and values that lead male individuals to work in this setting can be more similar to their female peers than they are in a less gendered environment. It is important to emphasize that the terms ‘masculine’ and ‘feminine’ used in this study for gender scores do not represent prescriptive gender categories. Rather, they serve as descriptive labels for sample-specific, statistically derived psychosocial profiles. These profiles reflect how sex-related components manifested within this cohort of healthcare workers.
Notably, the province of Quebec, where we conducted our study, ranks highly internationally in terms of gender equality. 74 Compared with results from other countries, sex differences in psychological distress can be small among Quebec workers.12,75 Limited statistical power among male participants may also explain the absence of significant sex effects. The absence of adjustments for profession-specific working conditions may also have influenced the results regarding sex and gender. Male and female are unevenly represented across healthcare professions. 76 Since these professions can also differ in working conditions, it is possible that some sex- or gender-related associations were influenced by these underlying differences. More specifically, Unmeasured occupational differences may have affected certain associations, making it more difficult to isolate the unique contributions of sex and gender to psychological distress. Larger samples would be needed to clarify factors that may have reduced sex differences in this population. Nonetheless, it remains important to emphasize that only measuring birth-assigned sex in our sample would have greatly limited our analyses.
As hypothesized, a more feminine gender score, regardless of sex, was associated with greater psychological distress. However, it did not influence the effects of the majority of COVID-19-related stressors. In our study, a feminine gender score was linked to a greater likelihood of working in wards, such as elderly wards, which are more severely affected by the pandemic. 77 While healthcare work is female dominated, greater gender segregation can be found in high-contact care roles such as nursing, which experienced greater challenges during the pandemic. 63 As defined by our composite index, a feminine gender score also captured a history of previous distressing events, greater daily apprehensions, and help in seeking personal problems. In this sense, regardless of sex, femininity appears to influence psychological distress modestly through personal and professional dynamics beyond the stressors examined in this study.
We observed an interaction between gender score and vulnerability to COVID-19 due to a medical condition. Although vulnerability to COVID-19 was generally associated with greater distress, a more feminine gender score was modestly associated with lower anxiety and posttraumatic stress symptoms among at-risk workers. This finding was contrary to our third hypothesis. However, only nine participants in our sample were considered medically vulnerable. Given the very small size of this subgroup, this interaction should be interpreted with considerable caution and viewed as exploratory. One possible explanation is that femininity has been associated with heightened health risk perception and greater engagement in preventive behaviors, 78 which may facilitate help-seeking or resource utilization. It is therefore conceivable that more feminine at-risk workers received or mobilized additional forms of support, potentially buffering distress. Alternatively, help and considerations provided to all at-risk workers during the early pandemic might also have been better received by more feminine individuals, with similar consequences. Replication in larger samples is necessary before drawing firm conclusions. If supported, such findings could inform strategies to reduce distress among medically vulnerable workers during public health crises.
Limitations and strengths
This study has several limitations that should be taken into account. Since exposure to COVID-19-related stressors was measured via dichotomized retrospective items, differences in the frequency and duration of exposure, as well as qualitative differences in experience, were not accounted for. This could also have led to recall bias. A large number of participants were excluded because the retrospective survey was not completed, which reduced the statistical power of this study. As the survey was sent through a different modality than other measurements did, loss of convenience, compounded with a heavy workload due to the pandemic, might have lessened the motivation of workers to complete it. Future studies could thus add additional measurements of exposure to stressors during the monitoring period, which could help clarify psychological distress trajectories related to specific stressors.
The vast majority of participants (92.9%) identified as White. However, in 2021, 16% of Quebec's population was a racialized minority. 79 This demographic was underrepresented in this study. Additionally, racialized minorities tend to be overrepresented in some healthcare professions: while Black and Filipino workers each account for 3% of workers in other occupations, they represent 12% and 11% of nurse aides, orderlies and patient service associates, respectively. 80 Our results might not, as such, describe the experience of particularly vulnerable workers in terms of risk and exposure. In addition, while it reflects sex ratios in the healthcare sector, a small sample of 49 male workers might have diminished the statistical power of sex-related analyses. Future studies should consider aspects of our recruitment methodology, which might have led to this underrepresentation, and specific recruitment efforts for these demographics should be put into place to ensure a representative sample.
Nevertheless, our study used sociodemographic and professional information to gain a deeper understanding of the effects of sex and gender on the experiences of healthcare workers at the beginning of the pandemic. It also went beyond the cross-sectional design usually found in similar studies by using an EMA methodology to gather information on psychological distress. As it included a change in distress over time, its results help clarify the extent to which the pandemic resulted in significant increases in psychological distress among healthcare workers. Three different validated questionnaires were also used to measure psychological distress, leading to a better overview of relevant symptoms during the assessment period. Future research could include more refined measurements of gender constructs that could include gender identity, gender roles, gender relations, and institutionalized gender to provide a more comprehensive picture.
Conclusion
The present study suggested that gender had a small but significant influence on levels of psychological distress among healthcare workers during the early stage of the pandemic, independent of sex. While COVID-19-related stressors increased psychological distress, only vulnerability to COVID-19 showed a direct interaction with gender, although this finding was based on a small subgroup. Our findings could suggest that organizational responses to out-of-work events, including proactive support for workers during and after quarantine, may help address psychological distress. Accounting for these experiences may help clarify how pandemic-related pressures interact with gendered dynamics in shaping mental health. These findings also highlight the need to go beyond measuring birth-assigned sex to understand the sociocultural gendered dynamics that influence mental health in the workplace. This could lead to additional efforts to measure gender-based dynamics in specific workplaces in order to offer more individualized interventions and resources to workers. Taken together, teasing apart gendered profiles could help efforts to better understand gender inequalities in health and reduce distress in the healthcare sector during public health crises as well as other challenging contexts.
Footnotes
Acknowledgments
The authors have no acknowledgments
Ethical considerations and disclosures
The research ethics board of the University of Montreal Hospital Research Centre approved the research project (No. MP-02-2021-8963).
Informed consent
All participants provided written informed consent prior to participating.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by the Fonds de Recherche du Québec—Ministère de l’Économie et Innovation under grant #2020–2023-COVID19-PSOv2a-51476; the Fonds de Recherche du Québec - Société et Culture under grant #325839; the Fonds de Recherche du Québec— Santé under grant #332085; and the Canadian Institutes of Health Research under grant #0682004759.
Fonds de Recherche du Québec - Santé, Institute of Gender and Health, Fonds de Recherche du Québec—Ministère de l’Économie et Innovation, Fonds de Recherche du Québec-Société et Culture, (grant number 332085, 0682004759, 2020-2023-COVID19-PSOv2a-51476, 325839).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
For reasons pertaining to confidentiality, the authors are not allowed to submit primary data.