
Abstract
Background
Occupational therapy practitioners (OTPs) are increasingly using artificial intelligence (AI) in various settings to enhance evaluation, intervention, documentation, and decision-making. Challenges such as limited training, high costs, and ethical concerns contribute to under-utilization. Understanding current use, future potential, and adoption factors is essential for advancing AI use in the field.
Objective
This study investigates OTPs’ current AI use, anticipated future applications, and correlations between AI usage, experience, and practice settings.
Method
A descriptive, quantitative survey collected data on participants’ years of practice, practice settings, AI exposure, and current and future AI use.
Results
A total of 43 OTPs (39 occupational therapists and 4 occupational therapy assistants) completed the survey, with 63% having 1–5 years of experience. Most participants worked in acute care hospitals, outpatient settings, or schools. Over 60% were familiar with AI, though only 17% had formal training. Common AI usage includes documentation software, wearables, and large language models. Future applications were expected to involve real-time feedback via wearables, intervention development, and documentation. Familiarity with AI was linked to a belief in its positive impact. Younger clinicians anticipated “weekly” AI use, while older clinicians expected “monthly” use in the future.
Conclusion
Growing AI familiarity among OTPs shows promise for advancing practice. However, limited training and generational differences highlight the need for targeted education to maximize AI integration.
Introduction
The American Occupational Therapy Association (AOTA) defines artificial intelligence (AI) as “a computer program's ability to perform reasoning, learning, sensory interaction, and adaptation tasks that are most frequently attributed to human intelligence”. 1 Within occupational therapy (OT), AI has the potential to support the entire occupational therapy process as outlined in the Occupational Therapy Practice Framework: Domain and Process (OTPF–4), including evaluation, intervention, and outcomes. Specifically, AI may enhance occupational profiles, assessments of occupational performance, intervention planning and implementation, and documentation across a wide range of practice settings.2–6 AI tools may also enhance professional reasoning, facilitate interprofessional collaboration, and promote client autonomy and shared decision-making during goal development and intervention planning. 1
Advances in artificial intelligence (AI) are beginning to influence how occupational therapy practitioners support occupational performance, participation, and outcomes. AI-enabled tools such as wearables and virtual reality systems can collect real-time data related to movement quality, safety, and adherence to home programs. 4 In addition, AI technologies support clinical workflows by improving documentation efficiency through voice-to-text dictation, virtual scribes, and large language models that assist with clear, reimbursement-ready clinical notes.2–3 Collectively, these applications offer opportunities to enhance monitoring and documentation while reducing administrative burden, allowing practitioners to devote more time to client engagement and therapeutic use of self.
Outside of occupational therapy literature, there is a growing interest in the application of AI across rehabilitation and clinical decision-making, that can have implications on OT practice. A high-impact systematic review by Sumner et al. identified expanding use of AI-supported technologies in physical rehabilitation, which includes wearables, robotic systems, and application-based platforms, however the authors also identified inconsistent clinical outcomes. 7 JAMA provides a recent systematic review that explored large language models (LLM's) within healthcare utilized for documentation, administrative tasks and evaluations, highlighting the need for increased clinician-reported outcomes to guide effective adoption. 8 Advances in AI-driven clinical decision support systems have shown promise in rehabilitation contexts, as machine-learning models demonstrate improved outcome prediction and clinical decision supports. 9 Together, these studies highlight both the promise and limitations of AI application and support of clinical decisions within rehabilitation.
Despite these potential advantages, several barriers influence the integration of AI into OT practice. Resistance to AI persists, and is often rooted in concerns related to transparency, professional autonomy, and ethical practice. Therapists frequently report limited knowledge and training related to AI, which can negatively affect confidence and competence in selecting and implementing AI-supported tools within occupation-centered practice.1 The complexity of AI systems may also limit understanding of how decisions and responses are generated, contributing to mistrust.5 Within occupational therapy, ethical concerns include uncertainty regarding the risk-to-benefit ratio of AI-supported interventions and data privacy concerns, as AI development relies on sensitive personal and occupational data that may be vulnerable to breaches or misuse.1,5
Concerns regarding workforce displacement also remain prevalent. Daniyal et al. 10 reported that 50% of healthcare professionals expressed fears related to unemployment associated with future AI implementation. Despite these concerns, there is limited quantitative research examining OTPs’ experiences, perceptions, and clinical reasoning related to AI use in practice.11–12 This lack of evidence represents a significant barrier to integration and should be considered when examining relationships between practitioner characteristics and AI adoption. 13
The integration of AI into healthcare can also be examined through the Unified Theory of Acceptance and Use of Technology (UTAUT). This framework proposes that technology adoption is influenced by performance expectancy, effort expectancy, social influence, and facilitating conditions, with these relationships moderated by factors such as age, experience, and willingness to use. 14 Applied to occupational therapy, performance expectancy may be viewed in OTP's beliefs that AI can improve clinical efficiency, accuracy of documentation, or effectiveness of interventions. Effort expectancy may be reflected through the frequency of AI usage, as higher use implies a wider impact on the OT process. The impact of social influence can be viewed with AI within formal and informal professional settings, plus access to training, and personal AI usage.
Through the lens of UTAUT, OTP factors such as age, years of experience and exposure to AI may impact current and future AI use. Examining these factors within the constructs of UTAUT, allows a theoretically grounded approach to better understanding the adoption of AI in OT practice, plus highlights potential areas for targeted education and profession wide trends.
Given therapists’ limited knowledge of AI and the emerging nature of evidence supporting its efficacy, AI has not yet been widely integrated into occupational therapy practice. This gap raises important questions regarding how OTPs are currently using AI to support occupational performance and how they anticipate incorporating AI into future practice. Accordingly, the aims of this study were to: (1) examine occupational therapy practitioners’ current use of AI within clinical settings; (2) explore practitioners anticipated future integration of AI across the OT process; and (3) investigate relationships between practitioner demographics and AI use in occupational therapy practice.
Methods
Design
This study employed a descriptive, quantitative design using a peer-reviewed survey to explore how occupational therapists (OTs) and occupational therapy assistants (OTAs) incorporate artificial intelligence (AI) into their clinical practice. 15 The focus was on capturing a broad range of perspectives regarding AI utilization in occupational therapy. Institutional Review Board (IRB) approval was obtained from Messiah University (2024-011). Informed consent was provided electronically by participants at the start of the survey. The survey link remained active for three weeks.
Participants
Participants were recruited through convenience and snowball sampling methods. Convenience sampling involved electronically contacting university alumni and hospital employees, while social media postings further promoted participation. The survey link was posted in occupational therapy Facebook groups, including AI4OT (370 members), OT4OT (34,000 members), and Occupational Therapy Treatment Ideas & Information (68,000 members). Researchers also encouraged sharing the survey link outside of the initial groups to support snowball sampling. Group administrators facilitated the survey's distribution, and participants’ anonymity was preserved. Inclusion criteria required participants to be OTs or OTAs aged 18 or older who had practiced within the past year in any clinical setting. Exclusion criteria included individuals who had not practiced within the past year or who were occupational therapy students.
Instrument
The survey instrument was a 22-item, researcher-created questionnaire administered via Qualtrics, an online survey platform and consisted of two sub scales; current AI use and future AI use. The survey assessed use of AI throughout the occupational therapy process, challenges related to AI use and anticipated future use of AI (See Appendix A, Table 1). Although the survey was developed by the researchers, content and face validity were prioritized through peer review by two experts in occupational therapy and artificial intelligence. The survey was provided to the experts in advance, and adjustments were made based on expert feedback to enhance clarity and relevance. Item development was informed by the Occupational Therapy Practice Framework, 4th edition (OTPF-4), which provided structure for aligning questions with the evaluation, intervention, and outcomes phases of OT practice, to enable the use of discipline-specific terminology.14,16 Due to the use of AI in OT being an emerging area with limited frameworks, the survey is intentionally exploratory in nature to capture early trends in practitioner experiences and perspectives. Response options for current and anticipated AI use were categorized as “frequently” (daily), “occasionally” (weekly), “rarely” (monthly), or “never” (zero).
Internal consistency reliability was evaluated for the survey items assessing occupational therapy practitioners’ current and anticipated future use of artificial intelligence in clinical practice. Based on the survey structure, two subscales were examined separately: Current AI Use (8 items) and Anticipated Future AI Use (8 items). Cronbach's alpha and McDonald's omega were calculated for each subscale, and corrected item–total correlations and alpha-if-item-deleted statistics were examined to assess whether any items weakened scale performance.
Although the survey was exploratory in nature, item development ws conceptually informed by the Unified Theory of Acceptance and Use of Technology (UTAUT). 14 Performance expectancy was operationalized within the survey through items assessing OTP's perceived usefulness throughout the OT process, including evaluation, intervention planning, intervention implementation, educational material development and documentation. Effort expectancy was indirectly surveyed to report current and future frequency of AI use. Facilitation conditions were surveyed through respondents’ years of experience, plus items requesting prior exposure to AI and formal or informal AI training, while social influence was explored by surveying familiarity with AI and reported use within clinical contexts.
Data analysis
Data were analyzed using IBM SPSS Statistics for Windows, Version 28.0. Descriptive statistics, including frequencies, percentages, and means were calculated to summarize participant demographics and survey responses related to AI familiarity, current use, and anticipated future use. Inferential analyses were conducted to examine group differences and relationships among variables. One-way analyses of variance (ANOVA) were performed to assess differences in current and anticipated AI use across different clinical setting types. Independent sample t-tests were conducted to evaluate differences between age groups (25–34 years vs. 35–64 years) in anticipated AI use, specifically for intervention implementation.
Pearson product-moment correlation coefficients were computed to examine the strength and direction of relationships between variables, including familiarity with AI and current use of AI across occupational therapy process stages (evaluation, intervention planning, intervention implementation, educational material development, and documentation). Correlations were also assessed between current AI use and anticipated future use within each domain. Correlation strength was interpreted using standard thresholds: values greater than 0.75 were considered good to excellent, values between 0.50 and 0.74 were considered moderate to good, and values between 0.25 and 0.49 were considered fair.16,17 All tests were two-tailed, and statistical significance was set at p < .05.
Results
Demographics
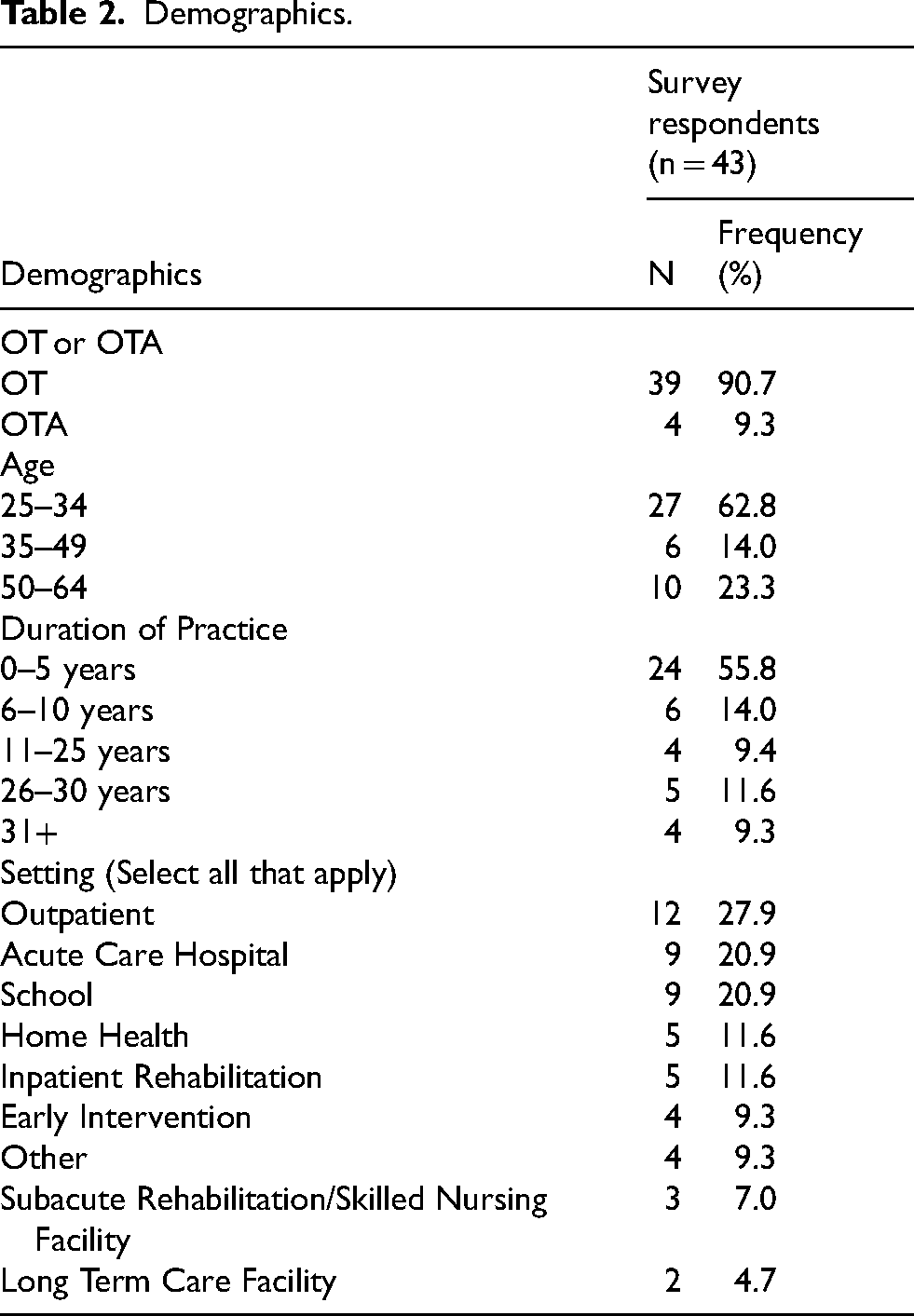
A total of 43 practitioners from across the United States participated in the survey, the majority of whom were occupational therapists (90.7%), with a smaller proportion identifying as occupational therapy assistants (9.3%). Most respondents (62.8%) were between the ages of 25 and 34, and nearly 56% had five years or less of practice experience, indicating a sample largely composed of early career professionals. Participants represented a range of practice settings, with outpatient care (27.9%), acute care hospitals (20.9%), and school-based therapy (20.9%) being reported (see Table 2 in Appendix B for further demographic information).
Familiarity and training with AI
When asked about their familiarity with AI, 38% of respondents reported being not familiar, 43% were somewhat familiar, and 19% identified as familiar with AI technologies. Over 83% of participants indicated they did not receive formal training on AI use through webinars, workshops, or continuing education. In terms of current use, participants most commonly reported using AI tools such as Spellcheck (67%), Apple Watch (42%), ChatGPT (37%), Siri (28%), and Alexa (26%) within their occupational therapy practice. Less frequently used tools included Grammarly (16%), Fitbit (9%), Oculus VR (9%), Microsoft Copilot (5%), and Oura Ring (5%). Notably, 20% of respondents reported that they do not currently use any AI tools in their practice.
Current and future use of AI
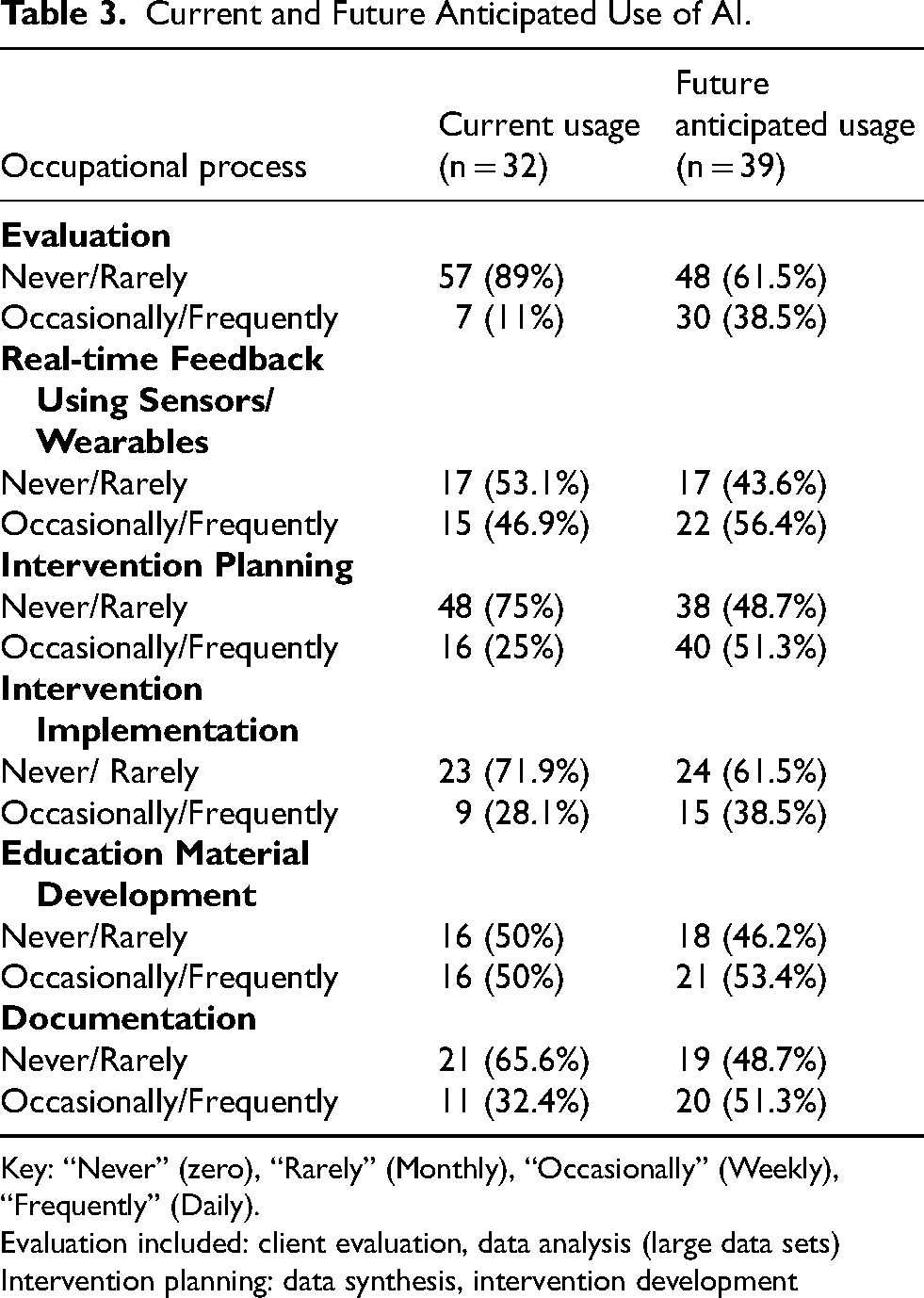
Of the 43 respondents, nine reported not using artificial intelligence (AI) tools in their occupational therapy (OT) roles. The remaining participants who had experience with AI were asked to rate both their current and anticipated future use of AI throughout the OT process. A summary of these findings is presented in Table 3 (Appendix C). Overall, participants reported low current use of AI across all phases of the OT process. Most indicated they used AI either infrequently (monthly) or not at all. However, there was a consistent trend toward increased anticipated future use of AI in OT practice.
The evaluation phase, which includes the occupational profile, analysis of occupational performance, and data interpretation, had the lowest reported current use of AI. Only 11% of participants reported using AI occasionally (weekly) or frequently (daily), while 89% indicated no use or rare use (monthly). Notably, anticipated future use increased, with the percentage of respondents reporting no or rare use decreasing by 27.5%, suggesting growing openness to AI integration in evaluation. Regarding the use of AI for real-time feedback (e.g., through sensors or wearable technology), 46.9% of participants reported current occasional or frequent use, with 56.4% anticipating this level of use in the future.
In the intervention planning phase, comprising data synthesis and the development of intervention strategies, 75% of participants reported rarely or never using AI. However, 51.3% anticipated occasional or frequent use in the future. Similarly, during the intervention implementation phase, 71.9% reported no or current monthly use of AI, yet 38.5% expected to use it weekly or daily in the future. The highest reported current use of AI was in the development of educational materials, with 50% of respondents indicating occasional (weekly) or frequent (daily) use. This trend is expected to continue, with 53% anticipating future use at the same level. For documentation tasks, 25.5% of participants currently use AI occasionally (weekly) or frequently (daily). This number is projected to rise, with nearly 42% expecting to use AI more regularly for documentation in the future.
Benefits and challenges of integrating AI
Results highlighted both the benefits and challenges of integrating AI in OT practice. Challenges included a lack of knowledge (60.5%) and training (62.8%) on AI tool use while respondents also identified concerns about patient privacy (34.9%), and data security (25.6%). However, respondents identified significant benefits including improved documentation (46.5%), increased efficiency in treatment planning (44.2%), and creativity in intervention formulation (39.5%). Support among supervisors varied with 79% of respondents identifying their supervisors as “extremely” or “moderately” supportive of their AI use.
Relationships
There were several significant relationships found in this study. First, those who were more familiar with AI were more likely to utilize AI currently in their jobs for data synthesis (r = .544, p < 0.01), intervention planning (r = .522, p < 0.01), implementation (r = .467, p < 0.01), and education material development (r = .383, p < 0.05). Generally, practitioners who currently use AI more frequently in the evaluation (r = 0.597, p < 0.01), data synthesis for intervention planning (r = .449, p < 0.05), intervention implementation (r = 0.422, p < 0.05), education material development (p = .653, p < 0.01) and documentation (r = 0.461, p < 0.05), were also more likely to anticipate using it during those same stages of the OT process in the future.
There was no statistically significant difference between the frequency of current or anticipated AI use across various settings (p = 0.647). There was also no correlation or statistically significant difference between participants’ length of practice and current or future AI use. There was a statistically significant difference among those ages 25–34 (M = 2.48, SD 1.005) and 35–64 (M = 1.71, SD, 0.914) regarding the amount of anticipated use of AI for intervention implementation (t = 2.355(37), p = 0.024).
Lastly, most respondents (67%) believed that AI would “positively impact” OT practice over the next five years, with 13% anticipating a “very positive” impact. A small amount (8%) foresaw a “negative” or “very negative” impact, while 13% expect “no impact” at all. Practitioners who were more familiar with AI had greater positive perceptions of AI's potential future impact on occupational therapy (r = 0.485, p < 0.002). These findings suggest a strong optimism among OT practitioners regarding AI's potential to enhance clinical practice and outcomes in the near future.
Reliability of AI scale
Internal consistency analyses supported the reliability of the AI use subscales. The 8-item Current AI Use subscale demonstrated acceptable internal consistency, Cronbach's α = .76, McDonald's ω = .75, based on 30 complete cases. The 8-item Anticipated Future AI Use subscale demonstrated excellent internal consistency, Cronbach's α = .92, McDonald's ω = .93, based on 39 complete cases. Corrected item–total correlations for the Current AI Use subscale ranged from .35 to .53, and corrected item–total correlations for the Anticipated Future AI Use subscale ranged from .48 to .86. Examination of alpha-if-item-deleted statistics indicated that no item removal meaningfully improved the Current AI Use subscale, and although deletion of the documentation item in the Future AI Use subscale produced a slight increase in alpha, the improvement was minimal and did not justify item removal. These findings support the internal consistency of the survey's current and future-use AI subscales.
Discussion
This study explored occupational therapy (OT) practitioners’ familiarity with artificial intelligence (AI), its current and anticipated use across the OT process, and perceptions of its benefits and challenges. The findings highlight the emergent integration of AI in OT practice, the potential for future adoption, and the barriers that must be addressed to realize its full benefits. In addition, our results underscore the need for support and training via their institution or setting to adopt and advance AI usage effectively. Bridging gaps between knowledge/training and supportive environments could foster broader acceptance and implementation of AI in OT.
Demographics and familiarity and training with AI
Participant demographics provide important context for these findings. Most respondents were early-career practitioners (ages 25–34 with 1–5 years of experience) working primarily in acute care, school-based, and outpatient settings, reflecting national employment trends, personal technology usage and practice areas where efficiency and documentation demands are high.17,18 Although most participants reported some familiarity with AI, few had received formal training, indicating a clear gap between exposure and competency. Many practitioners routinely used AI-enabled tools such as Spellcheck and voice assistants without recognizing them as AI, suggesting that everyday use of these tools, does not necessarily translate into confidence with more advanced applications. These findings may highlight the need for accessible OT-specific education to support effective and confident AI integration across practice settings.
Current and future use of AI
AI use within the occupational therapy process currently remains limited, with most practitioners reporting monthly or no use of AI for evaluation and intervention planning. This pattern aligns with prior research showing that clinicians often struggle to integrate AI into daily workflows despite general awareness.18,19 However, respondents anticipated increased future use of AI across evaluation, intervention planning, and educational material development, reflecting recognition of its potential to support efficiency and clinical decision-making. Anticipated growth in documentation use was more modest, likely reflecting ongoing concerns related to privacy and data security that continue to influence healthcare AI adoption.20,21
Practitioners with greater AI familiarity were more likely to use it for clinical tasks such as data synthesis, intervention planning, and educational material development. Greater familiarity also correlated with optimism about AI's future impact on OT practice. These findings possibly suggest that exposure to and experience with AI may drive both immediate and future adoption, highlighting the importance of formal education and training initiatives. 22 No significant differences in AI use were observed across practice settings or length of practice, indicating that AI adoption is not confined to specific environments or experience levels. However, younger practitioners (ages 25–34) reported greater anticipated use of AI for intervention implementation than older colleagues, suggesting generational differences in comfort with emerging technologies.
Findings suggest that OTPs may benefit from incorporating low-risk, task specific AI tools, such as educational material development, documentation support and data synthesis, to improve efficiency, while preserving professional judgement. Continuing education, plus entry-level training at college and university levels, should incorporate OT-specific AI training that can focus on topics such as; ethical use, data privacy, and meaningful AI use throughout the OT process. At the organizational and policy level, institutions and professional bodies should develop guidelines, training supports and competency standards to promote ethical and safe adoption of AI across various settings and populations.
These findings also highlight several possible barriers to AI adoption in occupational therapy, particularly gaps in training and concerns related to privacy and data security. Such challenges may limit clinicians’ willingness or ability to integrate AI tools into practice. Challenges related to AI-based documentation are not unique to occupational therapy. Nursing literature suggests that early limitations in AI-generated documentation may improve as systems are refined to better identify key disease elements and integrate relevant data into electronic medical records, underscoring the importance of ongoing system development and validation. 23
Overall, AI use among occupational therapy practitioners remains limited, particularly in evaluation and intervention planning, despite respondents being predominantly early-career clinicians working in settings where efficiency demands are high. 24 Although most participants reported some familiarity with AI, few had received formal training, reflecting a gap between exposure and competency that reflects trends across healthcare.22,25 Practitioners frequently used basic AI-enabled tools such as Spellcheck and voice assistants without recognizing them as AI, suggesting that everyday exposure may not translate into confidence with more advanced clinical applications. While respondents anticipated increased future AI use across the OT process, concerns about privacy and data security continue to limit adoption, underscoring the need for OT-specific education to support effective and responsible integration of AI into practice.26,27
Several limitations should be considered when interpreting the findings of this study. First, the study was limited by a relatively small sample size (n = 43) and a largely homogeneous participant pool. Recruitment challenges contributed to low enrollment despite multiple outreach strategies, including email and social media dissemination. The small sample size restricted the use of more rigorous statistical analyses and limited the strength of inferences that could be drawn from the data.
Participants were primarily recruited through technology-focused social media groups, which may have resulted in overrepresentation of occupational therapy practitioners with preexisting interest or engagement in technology and AI. This recruitment approach introduces potential self-selection bias and may contribute to more favorable perceptions of current and anticipated AI use than would be observed in a more broadly representative sample.
Geographic representation also presents a limitation. All respondents practiced within the United States, with the majority located on the East Coast, limiting representation of practitioners in other regions or international contexts where AI adoption and regulation may differ. Similarly, the sample was skewed toward occupational therapists (OTs) rather than occupational therapy assistants (OTAs), potentially underrepresenting OTA perspectives. Given the collaborative nature of occupational therapy service delivery, these factors may limit understanding of how AI is perceived and utilized across roles and practice contexts.
Additionally, most participants were younger than 34 years of age, resulting in limited representation of practitioners with longer clinical experience. Because years of practice may influence professional reasoning, comfort with emerging technologies, and adoption of innovation, this demographic skew may affect the interpretation of findings.
This study utilized a researcher-developed survey, which was informed by existing literature, expert review, and alignment with the OTPF4. The survey was intended to be exploratory given the emerging nature of AI and OT and has limited strength of inferences and generalizability of findings. The findings should be interpreted as preliminary, and future research should focus on developing and validating standardized instruments which can support a more rigorous assessment of AI integration within OT and related rehabilitation disciplines. Additionally, the modest sample size, limited geographic concentration of respondents, and a younger demographic representation limits external validity and transferability of results.
Conclusion
AI is currently being used by occupational therapy practitioners (OTPs) across a range of ages, practice settings, and levels of clinical experience. Common applications in current practice include educational material development, documentation, and real-time feedback using sensors. However, disparities in use exist due to varying levels of familiarity, which also influences anticipated future adoption. Practitioners anticipate increased use of wearables, data synthesis, and educational tools in clinical practice. These findings highlight the need for continued research on AI applications within healthcare, particularly to evaluate their relevance, efficacy, and accuracy within the OT process. Future studies should also assess changes in knowledge, confidence, and skill in using AI before and after continuing education or training programs to evaluate their effectiveness.
The study's findings also carry important implications for workplace functioning in OT settings. By streamlining documentation, supporting clinical decision making, and reducing cognitive load, AI aligns with core themes of occupational performance and workplace efficiency. Meaningful integration of AI has the potential to improve productivity and better support OTPs in managing the demands inherent in daily clinical practice, ultimately enhancing both practitioner workflow and patient care.
Footnotes
Acknowledgements
The authors extend thanks and gratitude to the participants for their time and valuable perceptions, contributing towards the study. Additional gratitude is given to the peer reviewers of the survey, Angela Bernard, and Josette Merkel. Further thanks to Laura Miller and Greg Privitera for the statistical analysis of the data collected from the survey.
Ethical approval
Ethical approval was obtained and granted from the Institutional Review Board through Messiah University, IRB #2024-011, prior to the administration of this study. The board conducted an Exempt review and deemed this study to be ethical and safe for the participants.
Informed consent
Informed consent was obtained prior to administration of the questionnaire for all participants of the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Appendix A
How often do you
Appendix B
Demographics.
| Survey respondents (n = 43) | ||
|---|---|---|
| Demographics | N | Frequency (%) |
| OT or OTA | ||
| OT | 39 | 90.7 |
| OTA | 4 | 9.3 |
| Age | ||
| 25–34 | 27 | 62.8 |
| 35–49 | 6 | 14.0 |
| 50–64 | 10 | 23.3 |
| Duration of Practice | ||
| 0–5 years | 24 | 55.8 |
| 6–10 years | 6 | 14.0 |
| 11–25 years | 4 | 9.4 |
| 26–30 years | 5 | 11.6 |
| 31+ | 4 | 9.3 |
| Setting (Select all that apply) | ||
| Outpatient | 12 | 27.9 |
| Acute Care Hospital | 9 | 20.9 |
| School | 9 | 20.9 |
| Home Health | 5 | 11.6 |
| Inpatient Rehabilitation | 5 | 11.6 |
| Early Intervention | 4 | 9.3 |
| Other | 4 | 9.3 |
| Subacute Rehabilitation/Skilled Nursing Facility | 3 | 7.0 |
| Long Term Care Facility | 2 | 4.7 |
Appendix C
Current and Future Anticipated Use of AI.
| Occupational process | Current usage (n = 32) | Future anticipated usage (n = 39) |
|---|---|---|
|
|
||
| Never/Rarely | 57 (89%) | 48 (61.5%) |
| Occasionally/Frequently | 7 (11%) | 30 (38.5%) |
|
|
||
| Never/Rarely | 17 (53.1%) | 17 (43.6%) |
| Occasionally/Frequently | 15 (46.9%) | 22 (56.4%) |
|
|
||
| Never/Rarely | 48 (75%) | 38 (48.7%) |
| Occasionally/Frequently | 16 (25%) | 40 (51.3%) |
|
|
||
| Never/ Rarely | 23 (71.9%) | 24 (61.5%) |
| Occasionally/Frequently | 9 (28.1%) | 15 (38.5%) |
|
|
||
| Never/Rarely | 16 (50%) | 18 (46.2%) |
| Occasionally/Frequently | 16 (50%) | 21 (53.4%) |
|
|
||
| Never/Rarely | 21 (65.6%) | 19 (48.7%) |
| Occasionally/Frequently | 11 (32.4%) | 20 (51.3%) |
Key: “Never” (zero), “Rarely” (Monthly), “Occasionally” (Weekly), “Frequently” (Daily).
Evaluation included: client evaluation, data analysis (large data sets)
Intervention planning: data synthesis, intervention development