
Abstract
Background
Mental health care users (MHCUs) have needs resulting from their participation in work-related-interventions. In long-term institutions, however, work interventions are neglected due to insufficient resources and knowledge needed to respond to these work needs.
Objective
To identify and describe the work needs of long-term MHCUs.
Method
A descriptive, qualitative inquiry study was conducted with 18 participants using semi-structured interviews.
Results
The need to improve quality of life and the need to fulfil contextual and societal demands emerged.
Conclusion
MHCUs not only appreciate work to earn a living, but also to achieve a sense of health and well-being, fulfil life-roles, and possibility for community reintegration.
Introduction
The Mental Health Care Act no 17 of 2002 stipulates that every mental health care user (MHCU) must be provided with treatment that facilitates their integration into the community (Parliament of South Africa, 2014). This includes seeking and finding employment in the open labour market. Nonetheless, there is an increasing occurrence of MHCUs who experience difficulties with achieving employment as a result of restricted opportunities for engagement in meaningful occupations within institutions (Kearns Murphy & Shiel, 2018).
Kearns Murphy & Shiel (2018) found that the MHCUs in institutions spend more time engaging in passive activities, such as sleeping, watching television, and sitting, despite their desire to engage in work. South Africa has been struggling to initiate a sustained response to mental health rehabilitation (Docrat & Lund, 2019), and as a result, MHCUs in long term care facilities experience ill-health and ill-being (Doble & Santha, 2008). Work is essential in meeting needs and is acknowledged to be a social determinant of health (Marmot et al., 2012).
In the context of mental health care facilities in South Africa, it is noteworthy that MHCUs in these facilities are predominantly from a low socio-economic status and often lack substantial social support. These individuals are admitted for extended periods, reflecting the ethical responsibility of the healthcare staff not to discharge them into an environment where they lack the necessary social support, leading to a higher risk of relapse and subsequent re-admission. Therefore, it becomes crucial in these facilities to equip MHCUs with adequate prevocational and vocational skills, enhancing their chances of successful reintegration into society upon discharge. Typically, users are released under the supervision of family or placed in appropriate facilities.
Although occupational therapists may also provide MHCUs with vocational rehabilitation within institutions, the complex work skills that the MHCUs learn may not be applicable (Castelejin, 2007). Despite the efforts, MHCUs stated that this does not provide the same meaning as open employment, as it is not equivalent to work with competitive wages, nor does it provide job satisfaction (Reker et al., 2000). In contrast, a South African study found that MHCUs were grateful for the opportunity to participate in work opportunities through vocational rehabilitation while residing in the hospital halfway house and attributed this to occupational therapy intervention (Tsatsi & Plastow, 2021).
Previous studies suggest that there is a correlation between engagement in purposeful work and improvement of mental health outcomes and quality of life (Crouch & Alers, 2014; Prior et al., 2013; Tomita et al., 2016). Similarly, a study by Koletsi et al. (2009) reported that work was a way to improve MHCUs’ health and self-esteem and decrease symptoms such as auditory hallucinations.
Furthermore, work is seen as a beacon of motivation (Provencher et al., 2002) and provides MHCUs with a means of coping with their psychiatric disability, as well as providing financial independence and stability (Koletsi et al., 2009). In addition, a study by Schnell et al. (2013) found that being able to work provided participants with the opportunity to feel part of society and attain a greater sense of belonging, thereby promoting community integration.
Incongruently, the lack of purposeful inclusion of MHCUs in work contributes to their experience of marginalisation and exclusion from society and results in negative financial, social and emotional outcomes (Chimara et al., 2021). Since mental illnesses generally develop at an age when people start their careers, they face many forms of marginalisation (Lindstrom Sol et al., 2021). As a result, this group experiences low levels of self-confidence and self-esteem, perceived stigma, and difficulties in achieving work goals. According to Zietsman and Castelejin (2014), occupational therapy aims to decrease occupational injustice and plays a crucial role in the delivery of care and treatment.
Although this is the case, Baker and Naidu (2021) identified that there is a paucity of resources and services for mental health in South Africa. Elwell-Sutton et al. (2017) acknowledge that the lack of resources in different communities is a result of inequalities that are deeply entrenched in the South African context. Although occupational therapists may also provide the MHCUs with vocational rehabilitation within long term institutions, the complex work skills that the MHCUs learn may not be translatable due to South Africa's challenges stemming from its rich cultural, political and socio-economic diversity (Castelejin, 2007).
This poses the question of whether occupational therapy work interventions within institutions are correctly directed towards addressing work needs that MHCUs have, to equip them with the necessary skills to obtain and sustain employment in their communities. As a result, this study asked what are the work needs of long-term MHCUs in a government-funded psychiatric institution? It aims to identify and describe the work needs of male long-term MHCUs in a psychiatric institution.
Methods
A descriptive qualitative study was used to describe the work needs of the male long-term MHCUs. The study was situated within a constructivist paradigm to explore findings from the subjective experiences of the MHCUs and construct knowledge therefrom.
The study was conducted at a government-funded psychiatric institution in Bloemfontein, South Africa. 15 research participants were recruited through purposive sampling. The inclusion criteria were that the MHCU must be older than 18 years, speak and understand English, Afrikaans, or Sesotho as these are languages of instruction at the hospital, and participate in the vocational rehabilitation programme. The MHCUs had to be stable without any positive symptoms at the time of data collection. The MHCUs needed a cognitive level of V and above of the Rancho Los Amigos Levels of Cognitive Functioning in order to understand questions asked and to adequately describe their experience.
The demographics of the MHCUs are listed in Table 1. It should be noted that all participants were male. This can be attributed to the predominantly male population at the institution, with very few females present in all the wards. Incidentally, no females met the inclusion criteria for participation in the study. The exclusion criteria was that MHCUs should not be scheduled for discharge within the period of the study's data collection. The study was approved by the University of the Free State Health Sciences Research Ethics Committee (ethics reference number: UFS-HSD2021/0137/2906). Permission to conduct the study at the hospital was obtained from the Free State Department of Health and later from the hospital's CEO. An information session was held with the MHCUs and only those who gave consent to participate in the study signed informed consent forms. No incentives were offered for participation in the study.
Demographics of participants.

*Work history was obtained through interviews with the MHCUs. Information obtained could not be confirmed through collateral information and may be unreliable.*
Participants will be referred to in abbreviated form for confidentiality: participant - P; interview number - 4 through 18. For example, P1.
Data was collected using face-to-face, semi-structured interviews utilising a self-compiled interview guide. The interview guide consisted of 13 main questions. These questions were derived from and designed using the Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES_Q) as well as work needs analysis surveys. Interviews were conducted in English, Afrikaans and Sesotho. Researchers were both English and Afrikaans speaking and conducted interviews with participants who preferred their interviews to be conducted in English and Afrikaans. For Sesotho speaking participants, an occupational therapy technician who is fluent in Sesotho assisted in translating the questions to Sesotho and conducting the interviews. The duration of each of the interviews ranged from between 30 to 45 min. Interviews were audiotaped in Sesotho, English and Afrikaans and transcribed verbatim and later translated into English for reporting purposes.
The 7 researchers and their supervisor (who understands Sesotho) reviewed all audio recordings and transcriptions for errors or exclusions of data and manually analysed the data using inductive thematic analysis. Braun and Clarke (2006) suggest that the familiarisation of data is the first step of data analysis. Braun and Clarke's (2006) method of thematic analysis was applied to translated transcripts. Following this step, the data was loaded onto Atlas Ti software for coding. Initial codes were generated based on the smallest units of meaning in the data. A total of 129 codes were identified. The codes were collated and resulted in 5 categories and later 2 themes. This was done repeatedly until data saturation was reached. The data was shared with the university supervisor to ensure triangulation and was stored securely with a password.
According to Botma et al. (2010) credibility of a research study is validated when the researcher reports the perspective of the participants as undoubtedly as possible. To ensure rigour in the study, the researchers made use of triangulation by involving the supervisor and co-coder from the hospital during data analysis and the interpretation of results. The researchers had prolonged engagement with the MHCUs through clinical training for their mental health placement at the hospital and thus were familiar with the culture and context surrounding the MHCUs. Researchers were reflexive in the data collection process of how their position of power as Caucasian females could potentially influence the responses gathered in the interviews.
It was also important to note that the occupational therapy technician who assisted with interpreting the questions was viewed in a position of power by the MHCUs. Dependability was ensured by the researchers making use of the semi-structured interviews informed by the Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES_Q), as well as work needs analysis surveys, making the study more consistent and repeatable. Confirmability was ensured through collective data analysis. Transferability was ensured by compiling a rich description of the population and context for readers to transfer information applicable to their setting and contexts.
Results
Two themes emerged from the research study which described the work needs that the MHCUs have: (1) The need to improve quality of life and (2) The need to fulfil contextual and societal demands. Figure 1 is a representation of the findings.
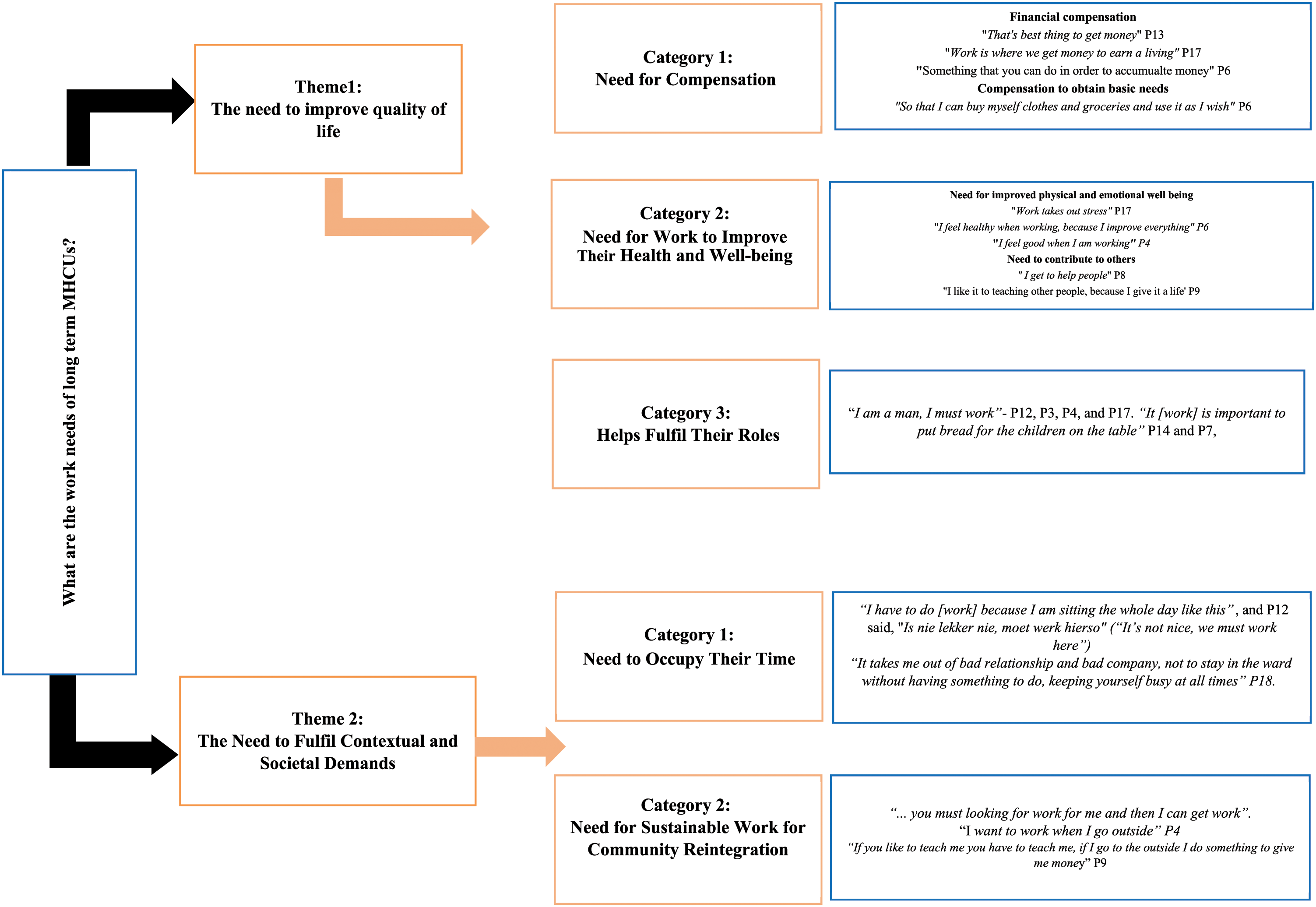
Findings.
Theme 1: the need to improve quality of life
The MHCUs’ need for work to improve their quality of life were evident in three categories: (1) Need for compensation, (2) Need to improve their health and well-being, and (3) Helps fulfil their roles.
Category 1: need for compensation
Most MHCUs noted compensation as the paramount element associated with work. Throughout the interviews, money was a recurring topic and surfaced as the participants’ greatest need and reward for the work they do. “That's the best thing, to get money” - P13. Several participants defined work as a means of obtaining an income; “Work is where we get money to earn a living” - P17, P2, P4, P8, P10. P6's definition of work was “something that you can do in order to accumulate money.”
According to the participants, financial compensation associated with work was more than just having money in their pockets; it was a necessity to address participants’ basic needs. This is evident in multiple responses from P6, P12, P8, and P9 that money as a reward for work they have done can be used to afford their basic needs. P12 noted, “I work so that I can buy myself clothes and groceries and use it as I wish”, and P17 expressed that “work is something that will make you to make income, so that you can put bread on the table”.
Category 2: need for work to improve their health and well-being
Numerous participants acknowledged that work has more meaning for them than the provision and meeting of basic needs. It is also about the need for work to contribute to their emotional well-being. Most of the participants expressed their emotions while engaging in work. P4, P17, P12, and P14 indicated that they “feel good when I am working” and P11, P3, and P6 said, “I feel happy when I work. I like it”.
Some of the satisfaction that contributed to their emotional well-being was being able to help other MHCUs. Participants were aware that despite work being a personal engagement, it also provided them with opportunities to help and teach other MHCUs a new skill. This experience was meaningful and provided motivation for work. P8 stated that he likes work because he “gets to help people”. Another participant stated that “I like it…to teach other people because I give it a life” - P9.
For other participants, work was also a stress relieving agent which contributed to their overall health and well-being. This is because engagement in work opportunities within the hospital was a rare occurrence. P17 stated that “work takes out stress”. Others were more aware of the physical benefits that came with engaging in work opportunities like gardening as supported by the following code: “I feel healthy [when working] because I improve everything” - P6.
Category 3: helps fulfil their roles
Work was recognised as a way of helping participants fulfil their life roles. Some of the participants had roles to fulfill outside the hospital setting; some were fathers, sons and partners. Work felt more meaningful for participants when it afforded them with the opportunity to provide for their families. Participants expressed this need by stating “I am a man, I must work”- P12, P3, P4, and P17. This need for fulfilment of roles was supported by P14 and P7, “It [work] is important to put bread for the children on the table”, relating to fulfilling both the roles of a father and breadwinner.
Theme 2: the need to fulfil contextual and societal demands
Although participants were aware that they were institutionalised without prospects of discharge, they still felt the need to fulfil contextual and societal demands. This was evident in two categories: (1) Need to occupy their time, and (2) Need for sustainable work for community reintegration.
Category 1: need to occupy their time
Participants expressed a deep need to occupy their time and the awareness that work provides the opportunity to do that. It was evident that participants have the need for constructive use of time. Due to the Covid-19 pandemic, opportunities to participate in work through vocational rehabilitation were limited. P9 stated that “I have to do [work] because I am sitting the whole day like this”, and P12 said, “Is nie lekker nie, moet werk hierso” (“It's not nice, we must work here”).
Other participants voiced the benefits of constructive use of time for them. They were aware that work spared them from maladaptive activities. P17 expressed that work prevents him from participating in destructive behaviours. P18 stated, “It takes me out of bad relationship and bad company, not to stay in the ward without having something to do, keeping yourself busy at all times”.
Category 2: need for sustainable work for community reintegration
It has been identified that participants have a need for sustainable work within the hospital setting that can be translated into the community. They expressed a desire to be able to find work outside the hospital setting. This is evident in the following codes: “If there is space for my working then I go, it's fine” - P11 and P6. P4 specifically stated that he wants the institution to assist him in finding opportunities for work; “… you must look for work for me and then I can get work”. The need for community reintegration through work was highlighted by P4 who stated, “I want to work when I go outside”.
Moreover, the participants have a need for this work to be representative of their skillset and the demands of the open labour market. P9 stated, “If you like to teach me you have to teach me, if I go to the outside I do something to give me money”. Likewise, P17 echoed the need to match the quality of the products produced in the leather work project to that of the open labour market.
Discussion
This study argues that among institutionalised MHCUs, there is a need to improve quality of life and fulfil contextual and societal demands. Provencher et al. (2002) found that work exposes MHCUs to new learning opportunities that can lead to improvement of their quality of life and their experience of well-being.
The need for financial compensation
The current study found that the participants had a prominent need to receive compensation for their work. The participants have all participated in vocational rehabilitation projects such as gardening, car washing, leatherwork, woodwork, and recycling projects, but they did not consider this equivalent to work. This supports the finding by Reker et al. (2000) that workshops that do not provide compensation are not considered ‘real work’. Throughout this study, participants understood work to be something one does to accumulate money in order to afford a better life and feel accomplished. Muñoz et al. (2006) state that an incentive is used to acknowledge participants who effectively demonstrate acceptable work habits and personal responsibility and can be motivation to participate in work.
In a study by Subramaniam et al. (2020) on young people with mental illness, 28 of 30 participants described the importance and benefits of work as primarily financial, enabling them to meet their day-to-day expenses. Similarly, a study identified that work provided MHCUs with financial independence, stability, and the choice of a better way of living (Koletsi et al., 2009). Although it is evident that there is a need for financial compensation, the practical execution thereof in context is challenging. Money can be a sensitive matter within mental health care facilities as some MHCUs have poor money management, specifically concerning substances.
Other means of compensation might be considered by implementing a token system. The code by P12 saying “I work so that I can buy myself clothes and groceries” aligns with Subramanium et al.'s (2020) study of young MHUCs’ need for money to meet their basic requirements such as food and shelter and also as a means of achieving economic stability, which gives them the ability to support themselves and their families.
The need to experience health and well-being
It was evident throughout the interviews that work for MHCUs was associated with positive feelings of “being happy” and “feeling good”. This aligns with a study conducted by Koletsi et al. (2009) which described work as a means to improve the mental health of MHCUs. Subramaniam et al. (2020) found that participants in their study also pointed out several benefits of work to their mental well-being. This included references to the positive impact of interactions with colleagues and the distraction provided by work which made them focus on getting the job done and allowed them to forget their symptoms or problems.
According to Abbas and Soeker (2021), MHCUs’ engagement in work led to an improved meaningful life, self-efficacy, and consequently improved well-being. This means that MHCUs’ engagement in work is about more than just compensation, but also about a way of maintaining health and well-being. The code: “I feel healthy when working because I improve everything” by P6 is evident of the MHCUs’ motivation to engage in work opportunities provided at the hospital despite the lack of financial compensation, as this improves other aspects of their lives. Ramukumba (2015) found that participation in work led to increased levels of happiness and contentment. In the same breath, a study by Blank et al. (2011) indicated that MHCUs’ reasons for working were not only money but also to garner appreciation, enjoyment, and satisfaction with life.
Similar to the findings in the study conducted by Saunders and Nedelec (2013), the current study found that the participants experienced increased social contact when working, which aided in the experience of emotional well-being. Additionally, they experience a need to work in order to contribute to society. This contribution can be in the form of teaching or helping others, which brings a sense of purpose and self-actualisation, thereby improving health and well-being. Tsatsi and Plastow (2021) suggest that the occupational need for interdependence is present among long term MHCUs residing in a halfway house who then find meaning and satisfaction in helping one another through collective occupations.
This contributed to MHCUs’ health and well-being. Characteristics of meaningful occupations according to Ikiugu et al. (2015) include connection with other people and self-transcendence. Both of these characteristics were identified by participants in the current study when considering work. Work thus enables MHCUs to consequently experience these characteristics.
The need to fulfil life roles
Participants in the current study have the need for work to contribute towards the attainment of various life roles. Some of the participants stated. “I am a man, I must work”- P12, P3, P4, and P17. Tsatsi and Plastow (2021) also found in their study that participants were expected to provide for their families in order to fulfil their roles as fathers and husbands, and work often contributed towards this fulfilment.
This need for MHCUs to fulfil life roles was reiterated by the participants in this study, saying that “It [work] is important to put bread for the children on the table”, relating to fulfilling both the roles of a father and breadwinner. Although financial compensation is connected to fulfilling this role, it speaks to a deeper sense of identity that comes with meeting expected life roles. A study by Netto et al. (2016) stated that engagement in meaningful work allowed MHCUs to establish and re-establish their identities and valued life roles.
Ikiugu et al. (2015) confirmed that returning to work restored the participants’ identities as providers of their families, while unemployment resulted in a loss of identity and a lack of purpose and structure in daily living (Macassa et al., 2021).
Fulfil contextual and societal demands: the need to occupy their time
Although participants were aware that they may not be reintegrated back into the community, they still felt the need to fulfil contextual and societal demands. This finding is similar to the one by Schnell et al. (2013) stating that work provides MHCUs with the opportunity to feel part of society, which in turn provides them with a greater sense of belonging according to Muñoz et al. (2006). MHCUs appreciated a programme that offered a variety of productive roles and engaged MHCUs in productive occupations that resonated with their role as workers in the community.
Apart from the stigma that associates MHCUs with not being able to work, Kearns Murphy and Shiel (2018) found that MCHUs in institutions spend more time engaging in passive activities despite their desire to work. The current study found that most of the participants had the desire to use their time constructively and identified the need for work to occupy their time.
Alexandratos et al. (2021) found that meaningful and purposeful use of free time improves quality of life. Participation in work helped MHCUs with structuring their day and creating routine. This structure is important in keeping MHCUs in touch with the world and maintaining their daily occupations (Sutton et al., 2012). The lack of constructive use of time upon discharge, be it participation in leisure or work, significantly contributes to readmission amongst MHCUs with schizophrenia (Smith et al., 2014).
Various factors may influence MHCUs’ participation in meaningful occupations. Lack of resources, shortage of occupational therapy personnel, and the COVID-19 global pandemic have all had a negative impact on MHCUs’ engagement in work related opportunities at the time of data collection. This resulted in a considerable increase in passive activities within their daily lives at the institution. Townsend and Wilcock (2004) suggest that MHCUs continuously face occupational imbalance and deprivation within institutions. Participation in work will not only assist, however, with improved quality of life but also assist in counteracting the negative effects of occupational imbalance and deprivation.
The need for sustainable work for community reintegration
Successful community reintegration needs to entail work skills that can help MHCUs generate an income. This is supported by Ramafikeng et al. (2020) who found that successful community reintegration requires MHCUs to have the skills and abilities necessary to live independently, which include the skill to generate an income. Participants expressed that the skills they are currently learning within the institution are not suitable for use in their communities post-discharge.
This is in contrast to the finding by Whatley et al. (2015) who found that skill transference was not a necessity in first world countries as disability grants were able to compensate for MHCUs’ cost of living. Although South Africa issues disability grants for MHCUs, it is not enough to sustain MHCUs’ cost of living, never mind their families. The minimum wage implemented in South Africa from March 2022 is R23,19 per hour (Mather, 2022) resulting in R3710,40 per month when working 8 hour a day for 20 days a month.
The maximum amount distributed for disability grants for an individual currently is R1980 per month (South African Government, 2022). Thus, despite the disability grant's purpose to substitute for an individual's inability to participate in competitive work, it is comparably lower than the minimum wage and thus impossible to cover basic needs.
Within the current study, P17 elaborated on the leatherwork skills they had obtained from one of the vocational rehabilitation projects: “I think people won’t like those belts. Maybe 90% will not buy but 10% will buy”. This is evidence of the disconnect between the skills acquired and the available resources and opportunities in their communities. This may reflect on the occupational therapy vocational rehabilitation programs as decontextualized from those required for successful community reintegration (Gamaldien et al., 2021).
According to Castelejin (2007), the complex work skills that occupational therapy provides through vocational rehabilitation may not be sustainable due to South Africa's challenges stemming from its rich cultural, political, and socio-economic diversity. Soeker et al. (2019) states that occupational therapists should consider the client's preferences and desired outcomes during vocational rehabilitation. Within the current study, participants stated that their desired outcome from work-related interventions is community reintegration.
Therefore, intervention should aim to meet these preferences and result in successful integration into the community upon discharge. In another study done by Monareng et al. (2006), 90% of the MHCUs wanted the facilitation of self-employment to be included in therapy to be able to meet South Africa's economic demands. Similar to the current study, these MHCUs want the work skills learned within the psychiatric institution to be carried over into the community.
Conclusion
In conclusion, this study argued that long term MHCUs have needs that are met by their participation in work. Like general society, MHCUs have the need to be compensated for their work. This is not surprising seeing that globally, work is viewed as a means through which to earn an income. MHCUs did not only appreciate work as a way to make a living, but also to achieve a sense of health and well-being. Work can elicit positive emotions and help MHCUs feel connected to others. This study identified work as an avenue for male MHCUs to meet their need to fulfil their roles as providers for their families and contribute to a positive self-identity.
Even though community reintegration may not always be possible, MHCUs participating in work would like to feel connected to the outside world by creating a routine through occupying their time with different work opportunities. At the same time, MHCUs see work as a means for community reintegration provided that the skills they learn through vocational rehabilitation are aligned with resources and opportunities available in their communities.
This study recommends that professionals in long-term mental health care should consider the work needs of MHCUs when providing therapeutic work or vocational interventions. Participation in work-related activities should be meaningful and help MHCUs meet their identified work needs. This will not only contribute to MHCUs’ experience of health and well-being while admitted to the hospital, but facilitate intervention that enables realistic community reintegration.
It is recommended for a similar study to be conducted with other participants diverse in age, culture, and background as work needs may differ from person to person. Occupational therapists can include the assessment of work needs in their work interventions to ensure that the interventions are well aligned with where MHCUs envision themselves. The findings of this study can be used to advocate for long term MHCUs in different institutions. Similarly, these findings can advocate for occupational therapy posts in public and private institutions as human and environmental resources remain a challenge in addressing MHCUs’ identified work needs. A follow-up study can help determine whether the identified work needs are met in psychiatric institutions across South Africa.
Footnotes
Ethics statement
The study was approved by the University of the Free State Health Sciences Research Ethics Committee (ethics reference number: UFS-HSD2021/0137/2906).
Funding
The authors did not receive funding for the publication of the article, authorship, or the research.
Informed consent
An information session was held with the MHCUs and only those who gave consent to participate in the study signed informed consent forms. No incentives were offered for participation in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgements
The authors would like to give thanks to Dr. T. Annandale for her contribution to the study and her position as the co-coder of this study, as well as the staff and mental health care users at the institution.