
Abstract
Background
Vocational rehabilitation counselors and policymakers need to better understand barriers to employment, not just related to the initial transition to employment, but to the length and quality of employment throughout the entire work lifecycle.
Objective
Our purpose was to identify the relationships of four types of barriers to employment with work life expectancy (WLE) among participants with spinal cord injury (SCI).
Method
Using self-report data, we applied a survival model to identify hazard of departure from the labor force, as a function of demographic, SCI, and socioeconomic characteristics, veteran status, and the four types of barriers to employment.
Results
Hazard of loss of employment and reduced WLE were associated with each of four types of barriers to employment, when considering one factor at a time. The four sets of barriers were: health considerations, poor job fit, low motivation/confidence, and lack of resources. When considering all factors simultaneously, all remained significant, except lack of resources. The findings identified relative importance of each type of barrier in relation to hazard of job loss and WLE.
Conclusion
Vocational rehabilitation counselors may utilize the findings to explore barriers to employment and diminished WLE among those with SCI.
Introduction
Spinal cord injury (SCI) is a neurologic disability that can significantly impact employment opportunities and time in the labor force. Persons with SCI typically experience lower employment rates than the general population (Post et al., 2020), despite the benefits of participation in employment (Meade et al., 2015). While return to work post-SCI is often achieved during rehabilitation, many individuals with SCI face challenges in retaining employment due to health and environmental barriers, and multiple factors contribute to the likelihood of sustaining post-injury employment (Karcz et al., 2022b).
Previous research has identified demographic and injury characteristics as related to employment after SCI, noting age, race, and physical function as predictors of the likelihood of employment. For instance, greater age at SCI and a greater injury severity have been found to associated with a diminished likelihood of post-injury employment after SCI (Karcz et al., 2022b; Nowrouzi-Kia et al., 2021; Ottomanelli & Lind, 2009). Similarly, nonwhite race/ethnicity has been associated with a diminished likelihood of employment (Karcz et al., 2022b; Nowrouzi-Kia et al., 2021). Although most research suggests that greater severity of SCI relates to a diminished likelihood of employment, it is not as strongly related to quality indicators, such as earnings, among those employed (Krause & Terza, 2006; Krause et al., 2008).
A more limited line of research has explored the barriers and facilitators to employment after SCI (Karcz et al., 2022a; Krause et al., 2021; Krause & Pickelsimer, 2008; Krause & Reed, 2011; Sturm et al., 2020). Krause et al. (2021) found the majority of participants were motivated to work based on the frequent endorsement of the importance of facilitators of employment, such as work being important and worth the effort. However, prominent barriers existed that kept them from working, including lack of assistance, training, and accessibility. Similarly, need for assistance and accommodations were identified as barriers in a cross-disability study sample (Dinelli et al., 2024). Among unemployed participants, health factors were found to be the most important barriers to future employment, even in comparison to health and financial disincentives (i.e., loss of health and financial benefits from earning too much money) (Krause & Pickelsimer, 2008). For instance, among those who reported being unemployed at baseline, all who reported pressure ulcers as a barrier to employment at baseline remained unemployed 5 years later.
A factor analysis of a set of 30 items indicated there were six factors underlying barriers and facilitators, although some factors were not adequately measured by sufficient items to form scales (Krause & Reed, 2011). More recently, a factor analysis of 32 barriers (Krause et al., under review) identified four themes: health, poor job fit, confidence and motivation, and resources. Despite the importance of barriers and facilitators to long-term employment outcomes, we can find no studies that investigated their relationship with employment throughout the work lifecycle.
One measure of long-term employment after SCI that may potentially be related to employment barriers is work life expectancy (WLE) or the predicted amount of time people will spend in the labor force throughout the time after SCI onset. It has been studied by generating predictive survival models of WLE estimating the probability of employment for each year after SCI onset (Pflaum et al., 2006) using a survival model, but not actual number of years employed. This early research used predicted life expectancy as the limit for WLE, using the logic that, as a group, the prediction for WLE should not exceed the life expectancy prediction. However, research has clearly indicated that those with greater education, earnings, and employment substantially exceed the life expectancy of those who do not have favorable economic characteristics (Krause et al., 2012), and these factors were not considered when capping WLE at the life expectancy estimates. They, therefore, underestimated WLE among those who were employed, particularly those with more severe SCI, because they did not account for the facilitative effect of being employed on life expectancy. More recent research on WLE identified the relationships of demographic and injury characteristics with employment trajectories (Krause et al., 2025) using the actual number of years employed since SCI onset and the hazard of job loss. The study found education level, race/ethnicity, age, and years post-injury to be significantly related to early exit from the labor force, and a trend of rapid early departure was seen for racial/ethnic minorities and those with lower educational attainment. These findings suggest the need for integrating additional covariates for a better understanding of factors related to WLE, including barriers to employment.
Our purpose was to apply a survival model to identify the relationships of four classes of self-reported barriers to employment, identified through the previous factor analysis, with hazard of job loss and WLE among participants with SCI. Multiple other covariates were assessed in the predictive equation, including demographic, SCI related, education, and veteran status. The findings shed light on the strength of the relationship of multiple types of barriers with hazard of job loss over time and WLE.
Method
Participants
Institutional review board approval was obtained prior to initiating data collection. Two existing longitudinal studies of SCI were used as the participant pool for recruitment, including the SCI Longitudinal Aging Study and the SCI Longitudinal Health Study. Details may be found elsewhere (Krause et al., 2025). The inclusion criteria were traumatic SCI, non-complete recovery, adult, and a minimum of one year post SCI onset. There was the added criterion of having been employed for at least one year since SCI onset, as our focus was only on those who had at least made an initial transition to employment.
There was a total of 2830 participants from an initial pool of 4516. After eliminating those who had not worked a minimum of 12 months after SCI onset, there was a final pool of 1335 cases. Those who were both over 65 and indicated they were retired did not complete the section on barriers, further reducing the sample to 1218. In the full Cox Proportional Hazards model, the sample size was further reduced to 959 by eliminating participants with missing data on any variable included in the statistical analysis.
Procedures
Data were collected through mailed and web self-report assessment (SRA) between December 2015 and October 2017. Nonrespondents were sent follow-up materials and those with current phone numbers were called to encourage participation. An additional set of materials was sent to those who agreed to participate but had misplaced or discarded materials. Participants were given $50 to compensate for their time and effort and as a way to promote optimal response.
Measures
The SRA measured multiple aspects of employment history. In the current analysis, we utilized the number of years having worked after SCI onset and current employment status as outcomes. Several covariates were measured including demographic, educational, and injury-related factors, as well as veteran status. These covariates were used as statistical controls to identify the relationships between four types of barriers to employment and WLE. Covariates included: geographic location of the United States (Midwest, Southeast), race/ethnicity (non-Hispanic White/other; Black, Hispanic, and American Indian), and educational milestones of less than a high school certificate (<12 years), high school certificate, vocational training, an associate's degree (12–15 years), and four-year degree or higher (16 years or more). SCI factors included age at SCI onset (less than 20 years old, 20–34 years, 35–49 years, and 50 years or older), years lived post-injury (9 years or less, 10–24 years, 25–39 years, and 40 or more), SCI severity (C1-C4, non-ambulatory; C5-C8, non-ambulatory; non-cervical, non-ambulatory; ambulatory, all levels).
The primary variables of interest were four factor scales derived from principal axis factoring with varimax rotation to 32 items (Krause et al., under review). This resulted in four factors, from which scales were developed, all of which were keyed in the direction of higher scores indicating greater barriers. These scales included: (1) health considerations, (2) poor job fit, (3) lack of motivation and confidence, and (4) lack of resources. The health considerations factor includes seven items that represent physical and mental limitations as barriers to employment, such as pain and memory problems. Job fit includes seven items and corresponds to beliefs about a lack of fit between what they are currently able to do and the jobs they would accept. The motivation/confidence factor contains four items that either address wanting to work or perception of their ability to maintain employment. The final factor is made up of three items relating to having adequate resources for employment, in terms of SCI injury support and educational attainment. Each of the four factors was grouped into high, moderate, and low scores to better interpret their relationships with hazard of job loss using the survival models.
Data Analysis
Stata version 16.1 was used to estimate adjusted Cox Proportional Hazards Survival Models of the association between four factor scales and WLE, controlling for demographic characteristics. A total of five models were fit, four of these models were the individual factor scales fit to WLE and controlling for demographic characteristics. The fifth comprehensive model considered all the factor scales together, along with demographic characteristics. The following demographics were used as controls in every model: education, age at diagnosis, time since diagnosis, sex, race/ethnicity, injury level, the region of the United States (Midwest, Southeast), and veteran status. With the inclusion of age at diagnosis and time since diagnosis, current age could not be included as age is perfectly predicted by the combination of these two other variables. For each factor scale, Kaplan-Meier plots were fitted to the data, using the non-parametric Kaplan-Meier estimator. These Kaplan-Meier plots estimate the proportion of people at a given time point who exited the work force. Statistical significance was determined by p ≤ 0.05, 95% confidence intervals that did not include the null hypothesis for a hazard ratio of 1, or by non-overlapping 95% confidence intervals where appropriate.
Results
Descriptive
The majority of the participants were male (72%) and non-Hispanic white (86%). The average age of the participants was 31 at the time of SCI onset and 49 at the time of the study (18 years had passed since onset). Forty-five percent were ambulatory (any neurologic level), with the remaining non-ambulatory participants including reporting C1-C4 (5%), C5-C8 (18%), and non–cervical injuries (32%). The average years of education was 15, with 3% having less than a high school education, 24% having a high school education, 24% having an associate's degree, 28% having a bachelor's degree, and 20% having a graduate degree based on self-reported years of education. Most were from the Southeastern United States (56%), and a relatively small portion were military veterans (6%).
Modeling
Preliminary – Individual Factor Scores
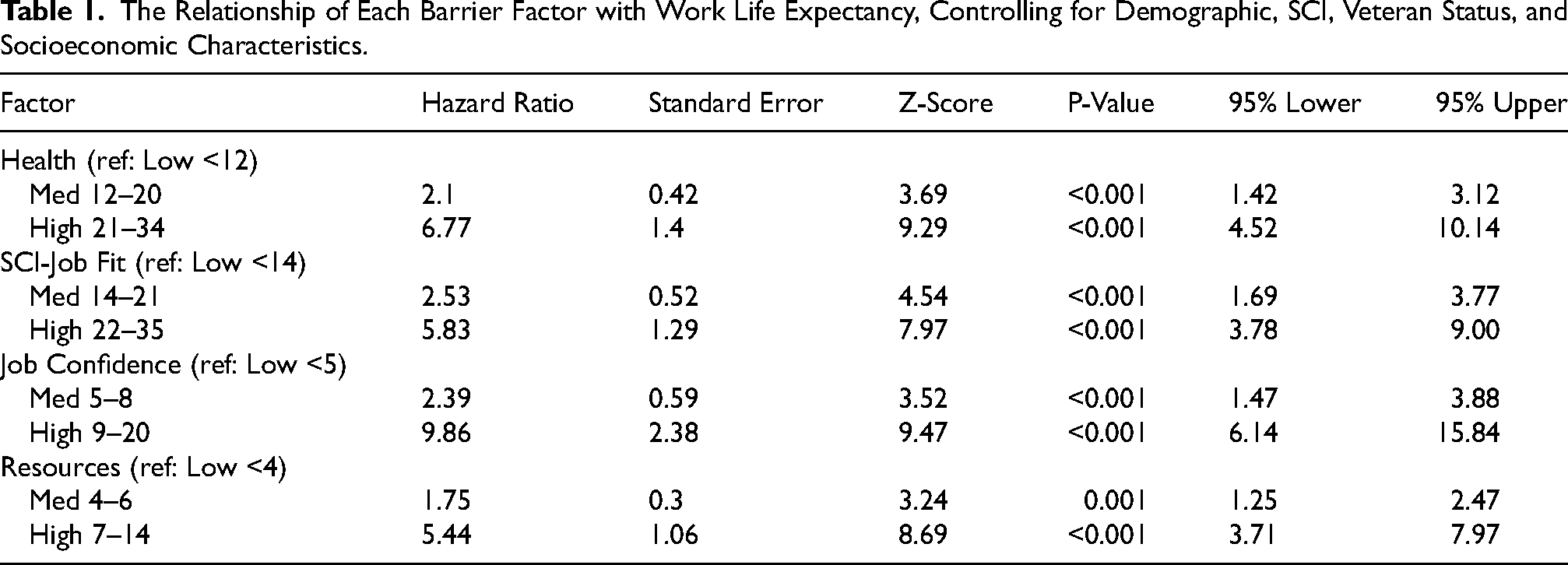
After controlling for multiple sets of demographic, SCI, socioeconomic, and veteran status predictors, each of the four barrier factors was statistically significantly related to a greater hazard of job loss and diminished WLE (Table 1). For each of these factors, when included in isolation after statistical controls, those with high scores on the barriers had the greatest hazard of job loss. The factor with the strongest relationship with the hazard of job loss was low motivation/confidence, and the factor with the weakest relationship was lack of resources.
The Relationship of Each Barrier Factor with Work Life Expectancy, Controlling for Demographic, SCI, Veteran Status, and Socioeconomic Characteristics.
Comprehensive Model
The results of the comprehensive model (Table 2) indicate that each of the four barriers factors were significantly related to WLE except resources, although the magnitude of the relationships differed between the types of barriers, with moderate barriers consistently being much less strongly related to WLE compared to high barriers. Job motivation and confidence were most strongly related to WLE, as those who reported a high number of barriers had 5.48 times greater hazard of job loss compared with those reporting the fewest barriers (95% CI = 3.14, 9.57), and those who scored moderate on this factor reported 1.72 times greater hazard of job loss (95% CI = 1.02, 2.89). This was the only factor where moderate scores were significant (Figure 1). The people who reported the lowest confidence in employment demonstrated 50% workforce attrition after 20 years.

Work lifeexpectancy as a function of job motivation/confidence.
The Relationship of all Factor Scales Considered Simultaneously, Controlling for Demographic, SCI, Veteran Status, and Socioeconomic Factors.
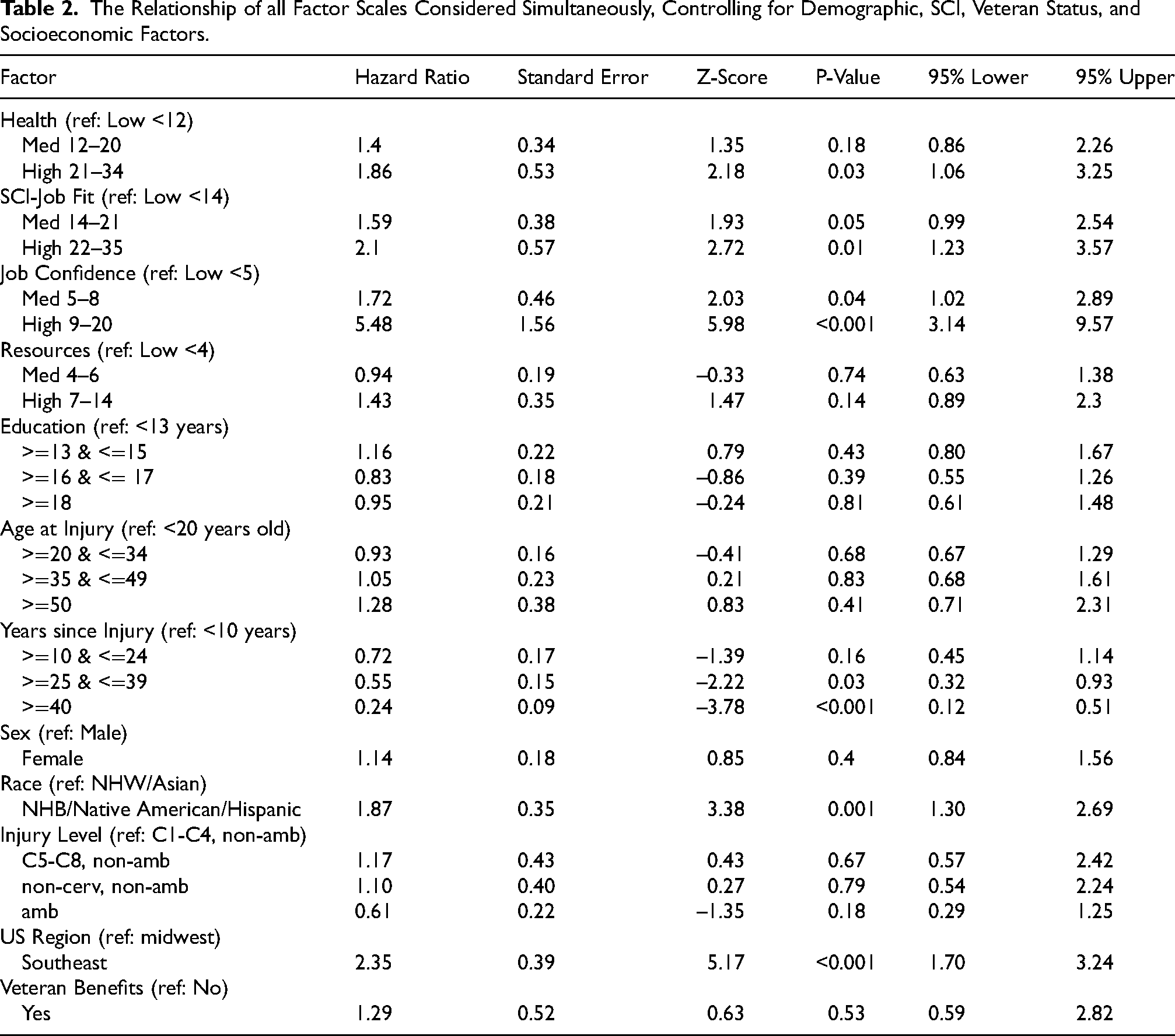
Both those with low and medium scores had less than 25% attrition after 30 years.
The factor of job fit with SCI had the next highest hazard ratio for those high in the factor compared with those lowest on the factor (OR = 2.1, 95% CI = 1.23, 3.57). Those with moderate scores on this factor just missed significance (OR = 1.59, 95% CI = 0.99, 2.54). Figure 2 demonstrates that people who feel a strong disconnect between jobs they are qualified for and jobs they are currently able to perform are more likely to exit the workforce sooner than low responders. Participants who expressed high job fit barriers demonstrated 50% attrition after 25 years, compared to medium and low responders, who each had 25% or less attrition for that same time period.

Work life expectancy as a function of SCI-job fit.
Those who were high on health considerations had a 1.86 (95% CI = 1.06, 3.25) greater hazard of job loss compared with those who were low on the factor. Those with moderate scores were not significantly different than those with low scores. As shown in Figure 3, individuals who report health-related barriers are a serious problem leave employment significantly sooner than people who report low health-related barriers to employment (i.e., low WLE). Fifty percent of those with high health-related barriers exited the workforce after 25 years, whereas those with medium and low barriers remained in the workforce much longer, with less than 25% attrition after 25 years.
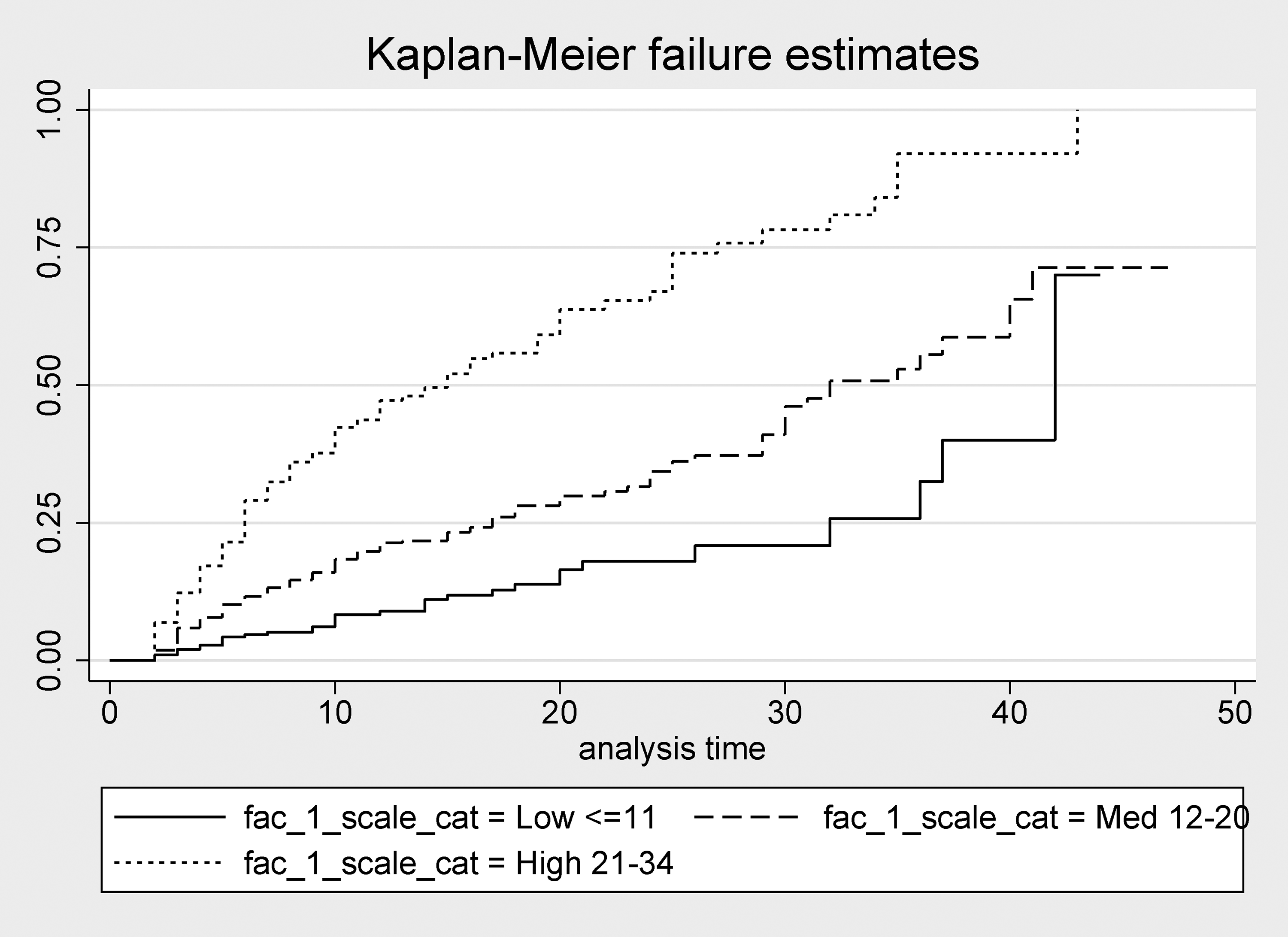
Work life expectancy as a function of participant health.
In the comprehensive model, access to resources was not a statistically significant predictor of WLE. Of the other covariates, only years post-injury, race, and geographic location were significant. Years post-injury reduced the likelihood of job loss for participants who had been injured for 40 or more years, 0.24 (95% CI = 0.12, 0.51), compared to participants who had been injured for less than 10 years. Non-Hispanic Blacks, Native Americans, and Hispanics had a higher probability of job loss (HR = 1.87, 95% CI = 1.30, 2.69), compared to the reference group of non-Hispanic Whites and Asians. Finally, participants living in the Southeast United States experienced higher job loss (HR = 2.35, 95% CI = 1.7, 3.24) than participants living in the Midwest.
Discussion
Our unique contribution was the identification of the relationships of four types of barriers to employment with WLE, as measured by the combination of the number of years worked post-SCI onset and the hazard of job loss. The findings are important in several respects. First, they identify the types of barriers that are most strongly related with WLE which is important because it measures work throughout the work lifecycle. Second, rather than simply identifying a cumbersome list of individual barriers, making it impractical to incorporate into vocational counseling, we built upon a previous factor analysis that reduced the number of covariates or considerations by grouping similar barriers and facilitators. Third, at the same time that we considered barriers, we additionally measured and controlled for multiple types of other covariates, including demographic factors, SCI severity, socioeconomic considerations, and veteran status. Taken together, this study summarizes new and important information that may be used by vocational counselors and policymakers to help individuals with SCI overcome the barriers that diminish their WLE.
Of the various sets of barriers, unfortunately, those related to motivation and confidence were most strongly related to WLE, as these may be the most challenging factors to change through intervention. The absence of motivation or confidence in work places vocational counselors in a difficult position, as they will always wish to facilitate employment opportunities, yet face this difficult barrier, and employment is not likely to be a realistic goal in these cases. It is important to point out that the findings, to some degree, may reflect the perspectives of those individuals who have worked after SCI onset, but have permanently left the labor force. In these cases, the findings are less of a concern as no vocational intervention would be necessary.
Job fit barriers, including the individual's perceptions that current jobs may be too difficult, do not use pre-SCI skills, or do not pay enough, also present significant challenges to the vocational counselor. From the perspective of economic theory, some of these perceptions may be accurate, as individuals build up healthy capital prior to disability through their work experiences, yet some of those skills may not apply after disability (Charles, 2003). For instance, someone with a cervical level SCI may no longer be able to do hands-on work which is problematic if their pre-SCI job was in a field that required significant upper body strength and dexterity (e.g., auto mechanic). Therefore, the vocational rehabilitation counselor may face a significant challenge in drawing out ways in which experiences and skills obtained prior to disability may translate to post-disability work within the same field.
The same economic theory (Charles, 2003) suggests that people with disabilities may use their unique experiences to develop skills that may be unique and particularly applicable after disability onset. Over time, they may build up disability capital. Using the same example, someone who is an auto mechanic may be able to translate some of those skills and knowledge to working with modified vehicles or other special considerations for people with disabilities, without having to do the same level of hands-on work. Many people with new disabilities obtain jobs that reflect some combination of pre-disability skills and focus on areas specific to people with special needs. Disability capital may be a way of opening doors for people with either limited motivation or those that see a poor job fit. Once they obtain post-disability employment, building disability capital may be a way of building long-term outcomes.
The third factor, health considerations, simply reflects the extent to which the individual has identified health issues related to SCI that limit the ability to work. Again, these may be difficult to work with within a counseling session. The health factor, in particular, suggests the need for an interdisciplinary focus that hopefully promotes better health and secondarily improves employment options. Furthermore, previous research has clearly indicated that when perceptions of poor health reflect chronic and debilitating issues, such as pressure ulcers, the likelihood of reemployment is minimal (Krause & Pickelsimer, 2008). Further, health interventions may be complicated and require a multidisciplinary approach to preparing the individual by addressing fundamental health needs as a prelude to return to and maintenance of employment.
The final factor, lack of resources, presents an outstanding opportunity to improve employment outcomes by adding resources. Despite finding that lack of resources was least strongly related to WLE, it was clearly related in the preliminary analysis that isolated its relationship with WLE. Introducing resources early on in the vocational rehabilitation process might be a starting point for helping the individual to see that there are possibilities beyond their current situation. As always, vocational counselors need to carefully consider adding resources that might tip the scales for the individual and lead to the first steps in establishing post-SCI employment.
Methodologic Considerations
There are several methodologic issues that must be considered when interpreting the results. First, all data are cross-sectional and represent the relationship of barriers at a single point in time with WLE, which included work throughout the work lifecycle. We differentiated those who were working at the time of the study from those who had worked postinjury but had since disengaged from employment. Therefore, although the relationships suggest barriers impacting future work, those relationships need to be evaluated using longitudinal data. Second, all data were self-report. Although it is unlikely there were reporting errors with basic characteristics like sex, race/ethnicity, age, and injury severity, it is possible there were errors in recall of number of years working or other employment parameters. Also, we measured perceived barriers rather than actual barriers, so the correspondence between actual barriers and perceived barriers may vary by person. Third, not all potential barriers were reflected in the measure. It is specifically noteworthy that those related to financial and medical disincentives did not comprise a factor and were eliminated in previous research (Krause et al., under review). Lastly, although WLE is an important cumulative index of work throughout the work lifecycle, it will also be important to demonstrate the relationships of barriers and facilitators to other employment outcomes as well.
Conclusion
Future Research
There are many needs for further research. First and foremost, there is a need to identify the relationship of each type of barrier with future outcomes using longitudinal research. Establishing the predictive validity of the barriers will help better predict future outcomes. Of course, the most important research will be the application of interventions that address the barriers to promote better research outcomes. The current research will help to guide those efforts. It is only through persistent research, with each study laying the foundation for the next approach, that we will see improved WLE among people with SCI.
Footnotes
Acknowledgements
n/a.
Ethics Statement
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. This study was approved by the Institutional Review Board (IRB) of the Medical University of South Carolina (Pro00114871).
Informed Consent
In accordance with the IRB approval, completion and return of the self-report assessment indicated implied consent under a waiver of written consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this publication were developed under grants from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant numbers 90DP0050 and 90DPEM0006). NIDILRR is a Center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this publication do not necessarily represent the policy of NIDILRR, ACL, HHS, and you should not assume endorsement by the Federal Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.