
Abstract
Applied behavior analysis (ABA) services can improve the quality of life for individuals with autism spectrum disorder (ASD). However, not all children receive services based in ABA. The disconnect between available services and accessing services may be the result of families experiencing barriers. Online parent training addresses many of these barriers by connecting families with service providers that they otherwise would not have access to. Furthermore, this approach allows for a family centered approach that empowers parents. A combination of parent training modules and video conferencing sessions allow parents to learn techniques and try them out with the support of a service provider. This article provides service providers with guidelines and suggestions for developing and providing services online.
Researchers have identified early intervention services as an important factor in the development of children with autism spectrum disorder (ASD; Wong et al., 2015). Services based in applied behavior analysis (ABA) are the most widely used evidence-based practice for children with ASD (Peters-Scheffer, Didden, Korzilius, & Sturmey, 2011). Unfortunately, families face barriers in accessing evidence-based services due to knowledge of services, location, availability of service providers, and cost (Cason, Behl, & Ringwalt, 2012; Cole et al., 2016; DeMoss, Clem, & Wilson, 2012; Heitzman-Powell, Buzhardt, Rusinko, & Miller, 2014; H. Meadan & Daczewitz, 2014; J. Meadan et al., 2016). The utilization of file sharing and video conferencing platforms provide service providers with the opportunity to disseminate parent training and increase access to services. File sharing platforms allow service providers to share training modules and documents with families through secure email platforms. Video conferencing platforms allow service providers and families to communicate via a web camera from remote locations.
Current Model
Services based in ABA facilitate positive behavior change through systematic application of behavioral principles, discrete trial training, reinforcement, prompting, shaping, antecedent-based interventions, and modeling (Baer, Wolf, & Risley, 1968; Cooper, Heron, & Heward, 2007; Wong et al., 2015). Services are typically provided by professionals, and funding resources (e.g., insurance, Medicaid) may set specific requirements of who must provide those services in order for reimbursement to be provided (Leaf et al., 2017). Depending on the individual barriers that a family may face, such as location, transportation, and availability of service providers, it may be difficult for families to access services even when they have insurance or Medicaid coverage. Teachers, paraprofessionals, parents, and other family members can learn to implement techniques and interventions based in ABA (Sarokoff & Sturmey, 2008). In fact, they are most likely already implementing strategies without knowing the names of the strategies (Cooper, 1982). Therefore, one potential solution to increase access to services is to increase parent training. Research has demonstrated that parents can learn and implement interventions with their children (Kasari, Gulsrud, Paparella, Hellemann, & Berry, 2015; Wainer & Ingersoll, 2012). This article provides suggestions and guidelines for providing parent training online.
Parent Involvement
Decades of research have provided support for the importance of empowering and training parents to implement interventions (Dunst, 1985; Dunst, Hamby, Trivette, Raab, & Bruder, 2000). Furthermore, research has demonstrated that techniques based in ABA can be learned and implemented by parents (Heitzman-Powell et al., 2014; Subramaniam et al., 2016; Wainer & Ingersoll, 2012). In addition, when parents are taught to implement interventions, they are more likely to continue interventions after services end (Hanft & Pilkington, 2000; Woods, Wilcox, Friedman, & Murch, 2011). Typically, parent interventions are conducted in person, making it difficult for families experiencing barriers to participate (Kasari et al., 2015; H. Meadan & Daczewitz, 2014). Researchers have addressed this issue by providing parent training through distance education models (Heitzman-Powell et al., 2014; H. Meadan & Daczewitz, 2014; J. Meadan et al., 2016; Pickard, Wainer, Bailey, & Ingersoll, 2016; Subramaniam et al., 2016; Vismara, McCormick, Young, Nadhan, & Monlux, 2013).
Distance Education Models
Online training disseminated via file-sharing platforms can alleviate the constraints of attending in-person trainings. Training videos, presentation software such as PowerPoint, interactive activities, specific parent training curriculum, and learning modules can be shared with parents remotely (Heitzman-Powell et al., 2014; H. Meadan & Daczewitz, 2014). Parents can access training materials at their convenience using tablets, smartphones, or computers with Internet or cellular access. One limitation to providing training through file sharing platforms instead of in person is the loss of real-time interaction between parents and trainers (Pickard et al., 2016; Wainer & Ingersoll, 2012). However, the addition of video conferencing allows for service providers to provide feedback and have parents try interventions in real time (Cole et al., 2016; Vismara et al., 2013). The following guide was created service providers to use when considering and developing parent training programs.
Recommended Components
Effective parent training disseminated remotely should include opportunities for feedback, specific training related to needs of the child and family, and follow-up (Ingersoll, Shannon, Berger, Pickard, & Holtz, 2017; Vismara et al., 2013). Instead of being a linear progression, parent training should be a continuous cycle of training, feedback, and implementation. Furthermore, service providers should consider the child’s natural environment, incorporate opportunities for collaboration, and follow guidelines of adult learning principles (Knowles, Holton, & Swanson, 2014; Woods & Lindeman, 2008). For a checklist of components to consider when developing online parent training, refer to Figure 1. In addition to recommended components, service providers should consider technical and legal requirements to providing parent training online.
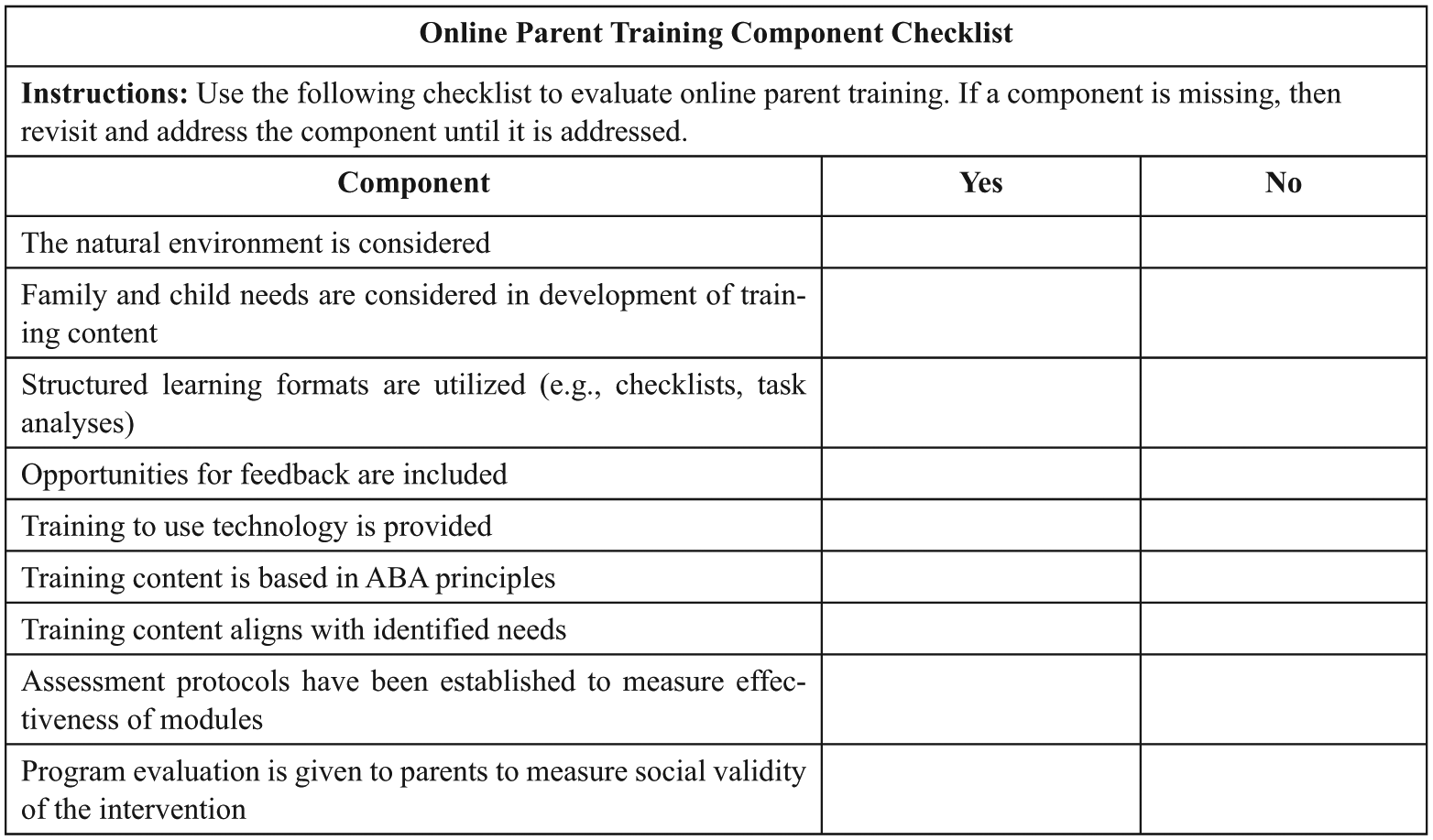
Recommended components for parent training provided online.
Special Considerations
Delivering parent training via video conferencing services requires internet or cellular access and an electronic device with video recording capabilities. Furthermore, accessing and utilizing video conferencing and online training requires technological skills that may need to be addressed before parent training can start. For example, parents may need to be trained how to login to video conferencing platforms. Therefore, consideration of family familiarity with technology is an important step in providing parent training online.
In addition to training parents to use the technology, service providers need to be aware of security precautions to take when personal information is shared online. File sharing and video conferencing platforms should use security measures that are in compliance with the Health Insurance Portability and Accountability Act (HIPAA, 1996). Service providers can check HIPAA requirements and submit compliance questions by accessing the U.S. Department of Health and Human Services website (U.S. Department of Health and Human Services, n.d.). In addition, it is important that professionals are cautious when recommending parent training and e-coaching. For example, some children may engage in self-injurious behaviors (e.g., head banging, skin picking) that require immediate, in-person intervention. This column provides suggestions to providing ABA-based training to families remotely that can be useful to service providers, including board-certified behavior analysts (BCBA) and university professionals.
Material Development
Providing online parent training may require the development of content; however, the development of training material can be alleviated by utilizing resources already in existence. For example, service providers can use internet modules such as Autism Focused Intervention Resources and Modules (AFIRM; https://afirm.fpg.unc.edu/afirm-modules). Furthermore, service providers can access and share training videos available on video-sharing websites (e.g., YouTube). In addition to sharing training modules and videos, service providers should incorporate try-and-apply activities that allow parents to implement interventions techniques with their child. A try-and-apply activity can involve the parent collecting data, incorporating environmental supports into the home, or running discrete trials.
Initial Intake
Before the family begins online parent training, an intake session should occur to access the needs of the family and the child. If possible, intake sessions should occur in person. By conducting the intake session in person, the service provider has the opportunity to interact with the family in the natural environment. However, if this is not feasible, the intake session could be conducted through video conferencing. Whether in person or via video conference, service providers should establish rapport with the family and ask questions to understand the routines, customs, and culture of the family (Knowles et al., 2014; Woods & Lindeman, 2008). This allows the service provider to provide the family with supports that are culturally relevant and realistic. During the initial intake session, service providers should conduct a functional behavior assessment by collecting direct and indirect data (Gresham, Watson, & Skinner, 2001). Direct data refer to data collected in real time, in the child’s natural environment (Cooper, 1981). Indirect data consist of data collected through interviews and behavior rating scales (Cooper et al., 2007). To further illustrate the process, the following scenario is described.
A family living in a rural area contacted a service provider. The service provider sent a survey with questions about the family’s routines, concerns about the child’s behavior, and possible areas that the family would like to focus (see Figure 2). The service provider reviewed the responses before the intake session. During the intake session, the service provider was able to gain more insight on the family’s needs by clarifying responses from the questionnaire and asking additional questions. Furthermore, the service provider provided the parents with behavior rating scales and checklists such as the Vineland Adaptive Behavior Scales (Sparrow, Cicchetti, & Saulnier, 2016).
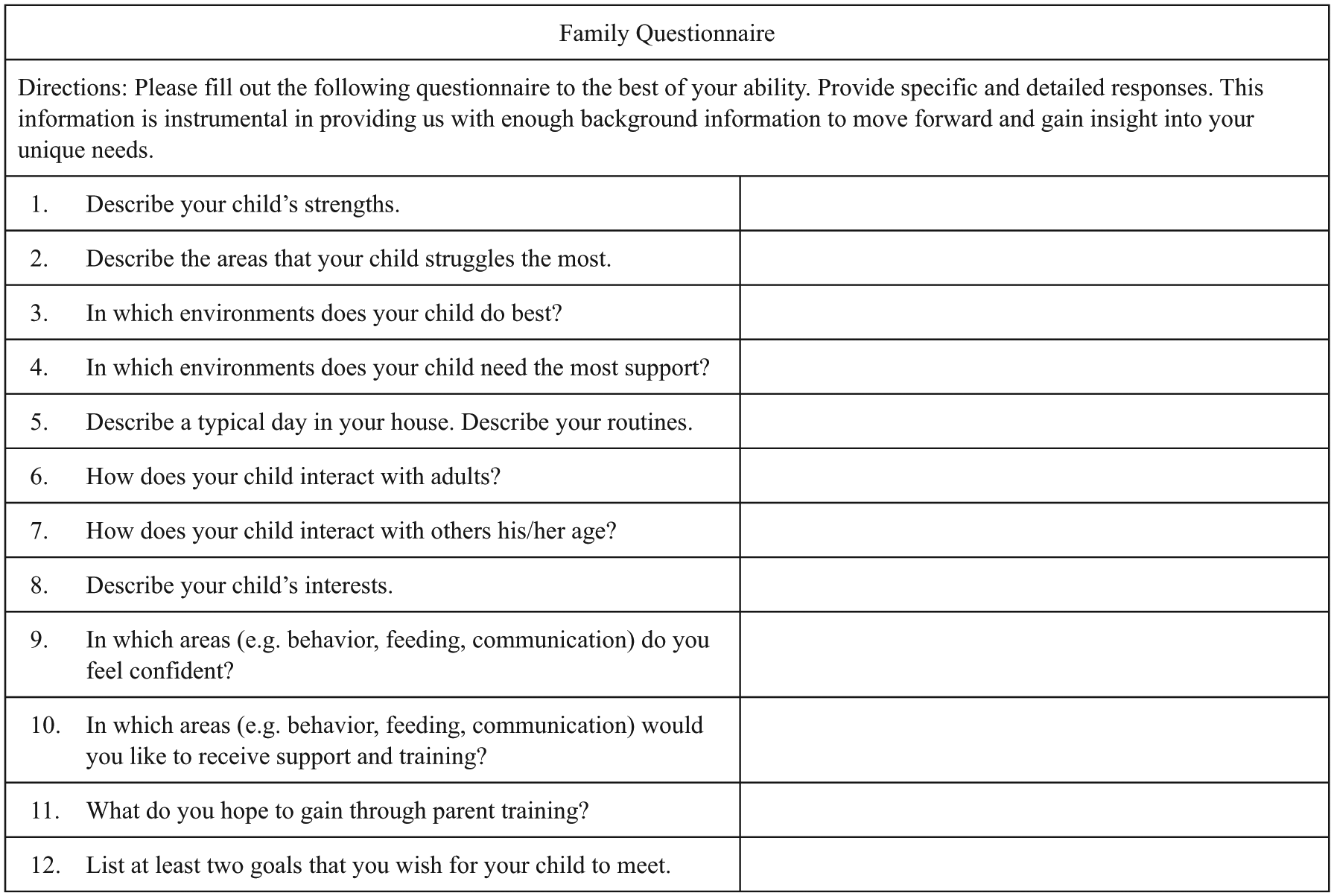
Sample questionnaire to provide parents during intake process. Questionnaires are an opportunity to ask questions that provide additional insight to formal assessments.
After completing the interview, rating scales, and checklists, the family interacted with their child as they normally would for 15 minutes of play. While observing the family and child interact, the service provider was able to take notes of how the parents and child interacted. During the observation, the child engaged in tantrum behavior several times. After discussing the interaction, the service provider and family determined that decreasing tantrum behavior and teaching a more appropriate replacement skill was the top priority. The service provider helped the family create an operational definition by using measurable terms to describe the tantrum behavior. Furthermore, the service provider and family determined what would and would not count as tantrum behavior. For example, crying without dropping to the floor was not counted as tantrum behavior. The parents were then provided with a learning module on how to record antecedent, behavior, consequence (A-B-C) data (Cooper et al., 2007). The parents recorded data over a week, then sent the data to the service provider.
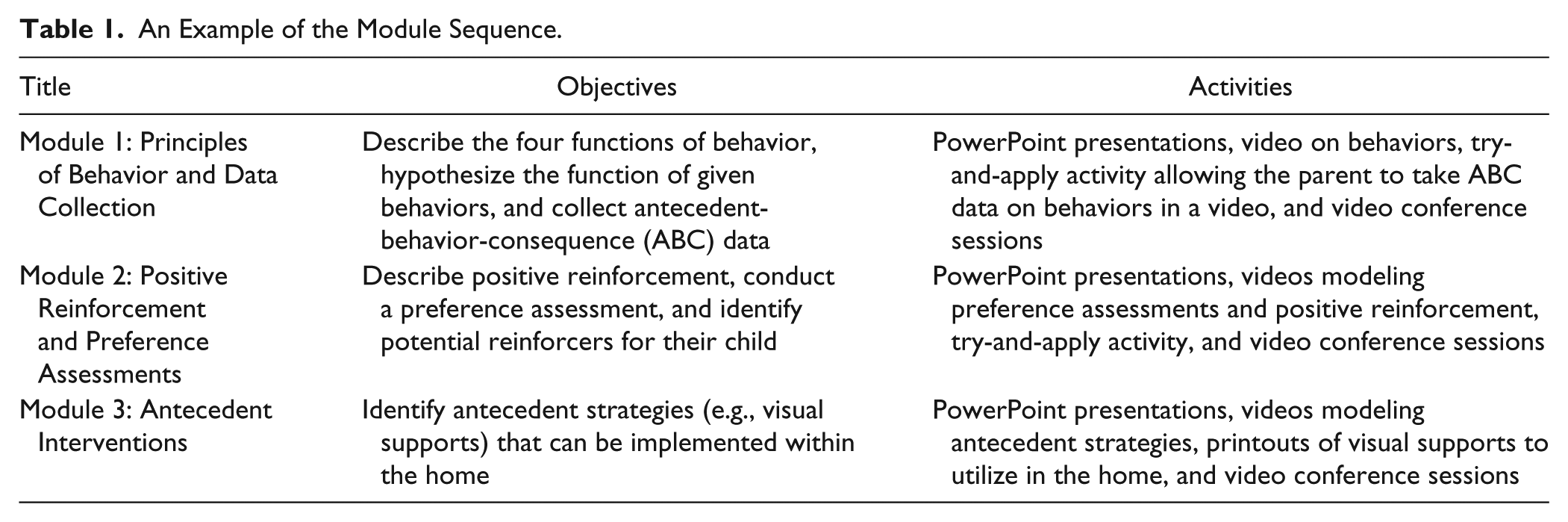
The service provider used the questionnaire, information gathered from the intake session, behavior scales, and anecdotal data to hypothesize the function of the behavior. Through this process, the service provider and parent developed a behavior intervention plan to decrease the tantrum behavior and increase more appropriate replacement behavior. By developing the behavior plan with the parents, the service provider was able to develop a plan that would be realistically implemented within the home. In addition to developing a behavior plan, the service provider shared a series of training modules on functions of behaviors, antecedent interventions, and reinforcement. An example of the module sequence is provided in Table 1.
An Example of the Module Sequence.
E-Coaching and Customized Didactic Sessions
After the intake session and dissemination of online training modules, service providers could use e-coaching sessions to model strategies. Furthermore, e-coaching sessions allow the families to implement techniques and strategies with the immediate feedback, guidance, and support of the service provider. In order to provide the family with opportunities to request support, e-coaching sessions should occur at least once a week (Vismara et al., 2013). This allows service providers to identify subsequent parent training to target.
Pretests and posttests can be utilized to determine learning of module content. Specifics of mastery criteria to move onto new modules should be established prior to parents starting modules. For example, 100% mastery may be more crucial for content involving foundational skills required for future modules. In addition to setting mastery criteria for modules, service providers can utilize data of a target behavior to measure effectiveness of the parent training intervention. For example, in the provided scenario, the service provider could use frequency and duration data of tantrum behavior to determine program effectiveness.
Feedback
Throughout parent training, it is essential that service providers give positive, constructive feedback to facilitate learning (Feil et al., 2008; Pickard et al., 2016; Wainer & Ingersoll, 2012). During video conferences, service providers should designate time to answer questions or concerns that parents may have, provide feedback, and problem solve any issues that arise. After watching submitted videos or engaging in video conferences with families, service providers could also submit written feedback. Feedback should be positive, acknowledge parent strengths, and provide suggestions. For a sample feedback template, refer to Figure 3. As new concerns and topics are addressed, the cycle would continue.
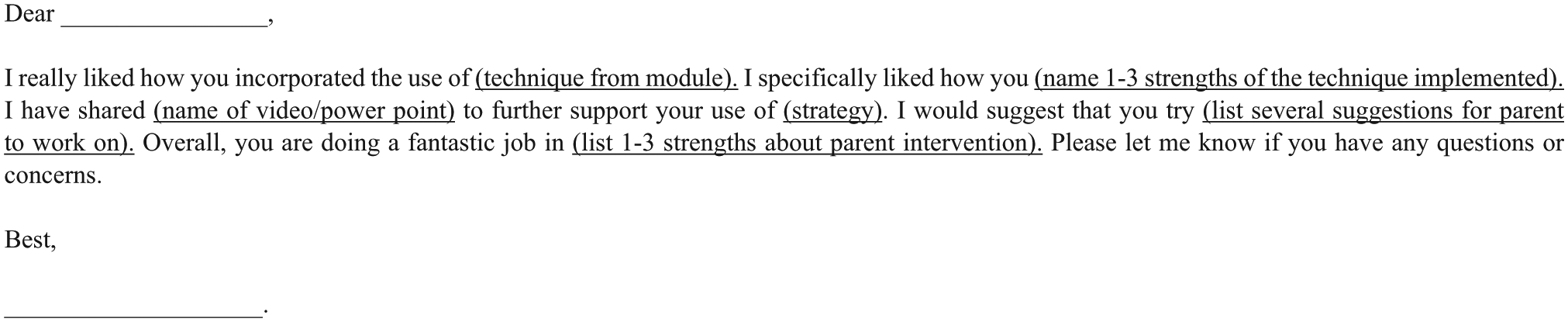
Email template for written feedback.
Social Validity
Social validity is an important component of online parent training. Service providers should utilize a measure of social validity to assess if parents find the training to be worthwhile, feasible to implement, meaningful, and effective. An example of a survey to measure social validity is provided in Figure 4.
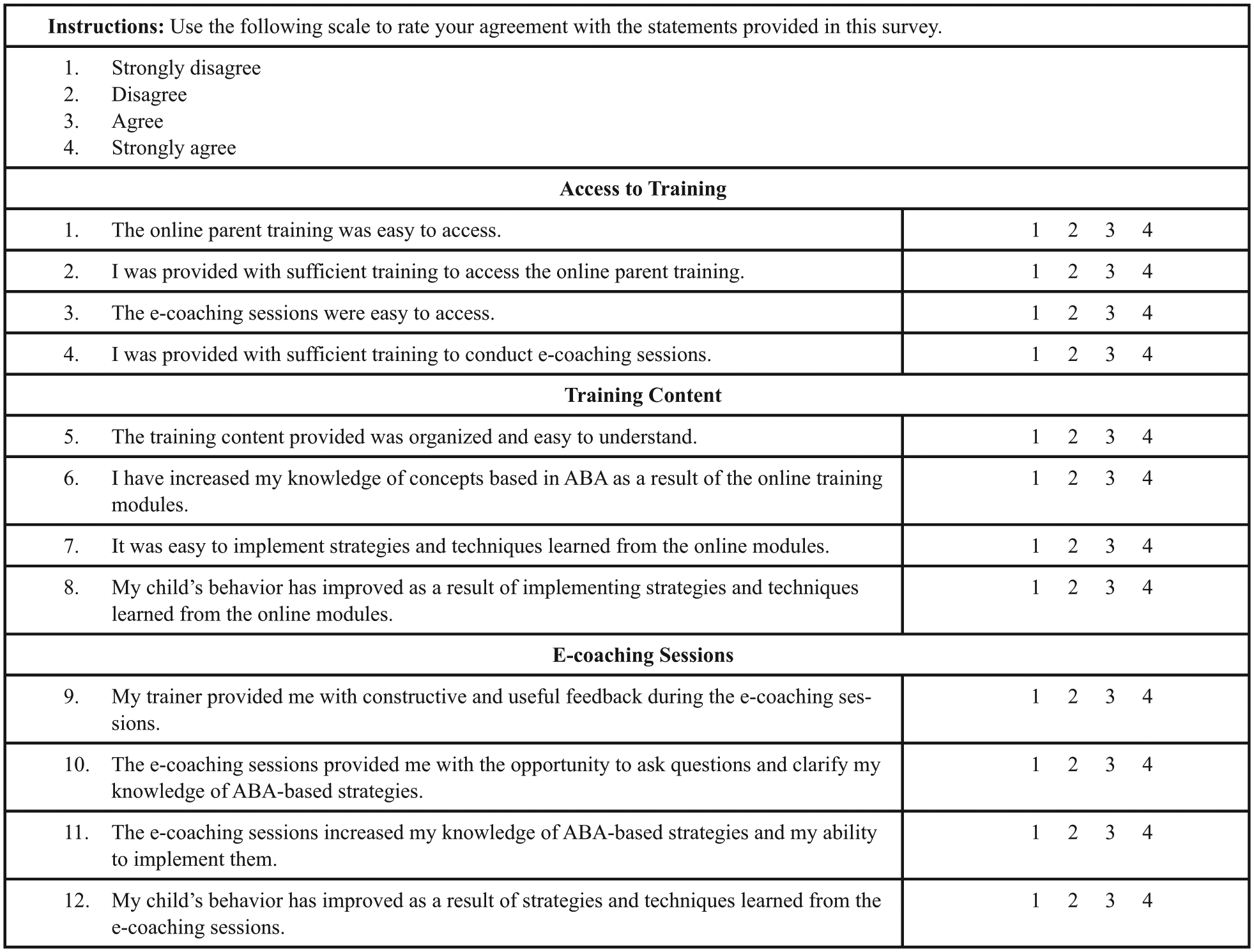
Sample survey to measure social validity of online parent training.
Conclusion
There are several limitations to providing parent training online. First, online parent training may not be appropriate for all children and families. Second, parent training delivered remotely is not yet accepted by insurance companies as a billable service (Bearss et al., 2018). However, despite limited insurance funding, parent training delivered online can potentially be a cost-effective supplement or alternative for children who receive limited or no services due to financial constraints (Dunst et al., 2000; Heitzman-Powell et al., 2014).
Providing training to parents of children with ASD through file sharing platforms and e-coaching via platforms in compliance with HIPPA allows parents to learn strategies and techniques leading to empowerment. Parent training can be useful not only for families of children with ASD, but for families of children without ASD who engage in behavior that interferes with their daily functioning. By providing training and coaching remotely, access to families with transportation issues, irregular work schedules, or to families in rural areas can be increased. In addition, because parents are a constant in their child’s life, parents can continue providing interventions long after services typically occur (Woods et al., 2011).
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.