
Abstract
Juvenile incarceration in the United States is declining; however, the rate of female youth incarceration is on the rise. Incarcerated female youth are more likely to have educational disabilities compared with female youth in public schools, as well as higher rates of mental health disorders and less consistent relationships with caregivers compared with incarcerated male youth. This article compares the characteristics of incarcerated female youth and the services available for incarcerated youth in the United States, Norway, and Mexico. Like the United States, Mexico is known for high rates of incarceration, whereas Norway is known for low rates of incarceration. All three countries have laws protecting the right of incarcerated youth to access education and mandating that juvenile facilities provide educational services. While this type of program is important, female offenders report that programs focused on close personal relationships were integral. Norway alone puts an emphasis on building positive relationships with facility staff and on involving community members in the programs for incarcerated youth. This may be a factor in Norway’s low incarceration rates and may how to help address the needs of incarcerated female youth in the United States and Mexico.
Keywords
The United States has the highest number of incarcerated youth in the industrialized world (McCarthy et al., 2016), and although the rates of juvenile incarceration have fallen drastically in the United States over the past 10 years, the rates of juvenile incarceration among female youth have increased in most offense categories when compared with male youth (Parrish, 2020). Female youth are incarcerated for less time than males, an average of 72 days, compared to the 94 days for male youth (Sedlak & Bruce, 2016). While shorter sentences may be considered a benefit rather than disadvantage, this means incarcerated female youth have less time to participate in education, treatment, and reentry programs compared with incarcerated male youth. Reentry programs refer to programs that are designed to help incarcerated individuals successfully reenter society. Sedlak and Bruce (2016) also reported that a larger percentage of incarcerated female youth, compared with male youth (i.e., 15% vs. 11%), name no parent as being a caretaker while they were growing up, and that 14% of female youth compared with 8% of male youth were raised in foster care, a group home, or other youth agency. This inconsistency in caretakers can disrupt educational services as these changes may require moves to different school districts or more secure settings, such as juvenile correctional facilities.
Nearly 40 years of research has recognized the low availability of services for incarcerated youth and that the available services have failed to factor in the needs of female offenders (Herrschaft et al., 2009). In essence, the incarceration of female youth appears to be on the rise in the United States; however, the program that is available for incarcerated female youth is not designed to meet their needs. To examine the unique needs of incarcerated female youth with disabilities, juvenile incarceration practices and available educational, treatment, and reentry services in the juvenile justice systems of the United States, Norway, and Mexico are discussed.
The United States incarcerates more youth than any other country and is ranked number one out of 233 countries for the highest prison population (World Prison Brief [WPB], 2021). Mexico also has a high rate of incarceration and is ranked ninth in the world (WPB, 2021). In contrast to the high prison populations of the United States and Mexico, Norway has comparatively low crime rates, incarceration rates, and recidivism rates (Labutta, 2017), and it is ranked 137th in the world (WPB, 2021). This article discusses practices in juvenile facilities in Norway that may contribute to the low rate of juvenile incarceration, compared with the practices in the United States and Mexico that may account for the high number of incarcerated youth, as well as the rising number of incarcerated female youth in the United States.
Synthesis of Content
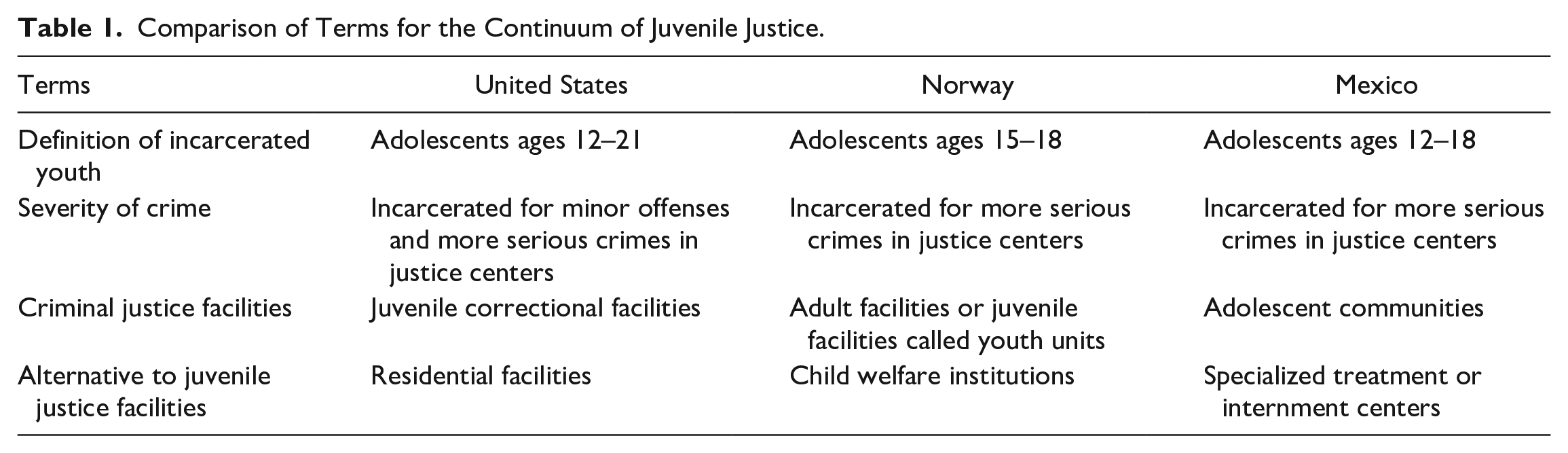
For the purposes of this article, the term “youth” refers to adolescents who have been convicted and confined to secure facilities. In the case of Norway, “youth” will also be used for adolescents who have been placed in child welfare institutions due to behavioral concerns. Youth (ages 12–21) in the United States who are convicted of violating the law may be placed in secure facilities, such as residential facilities or juvenile correctional facilities (Sickmund et al., 2021). These youth may be incarcerated for minor offenses such as underage drinking and truancy, as well as more serious violent crimes (Sawyer, 2019). In contrast, Norway has a larger continuum of placement options. Youth under the age of 18 who exhibit severe behavioral difficulties may be placed in child welfare institutions to receive treatment. Additionally, youth ages 15–18 may be incarcerated in juvenile correctional facilities called youth units or in adult facilities. Youth are only incarcerated for serious offenses such as violent crimes (Statistics Norway, n.d.). Similarly, in Mexico, only youth ages 12–18 who commit serious crimes are incarcerated in juvenile correctional facilities, referred to as adolescent communities (National Law of Integral Criminal Justice System for Adolescents, 2016). Across all three countries, the definition of “youth” and the juvenile justice continuum of care vary. In addition, the educational laws and definitions vary across countries (see Table 1).
Comparison of Terms for the Continuum of Juvenile Justice.
Incarcerated youth in the United States retain their rights to educational services through two federal statutes: the Individuals With Disabilities Education Improvement Act (IDEIA, 2004) and the No Child Left Behind Act (NCLB) of 2015 (Twomey, 2008). The NCLB (2002) was reauthorized in 2015 and renamed Every Student Succeeds Act (ESSA, 2015). In Norway, the right to education for every individual, including students with disabilities, is established in Article 109 of The Constitution (1814). In Mexico, the right to education is protected in the Third Constitutional Article, which states that every individual has the right to education, including incarcerated youth. While youth in juvenile facilities have the right to educational services in all three countries, the lack of available services, personnel, or training can hinder success (Azaola, 2015; Mulcahy & Leone, 2012; The Ombudsman for Children, 2020). Along with education, incarcerated youth may also be provided with mental health services and services that focus on reentry (see Table 2).
Comparison of Laws for Education in Confinement.
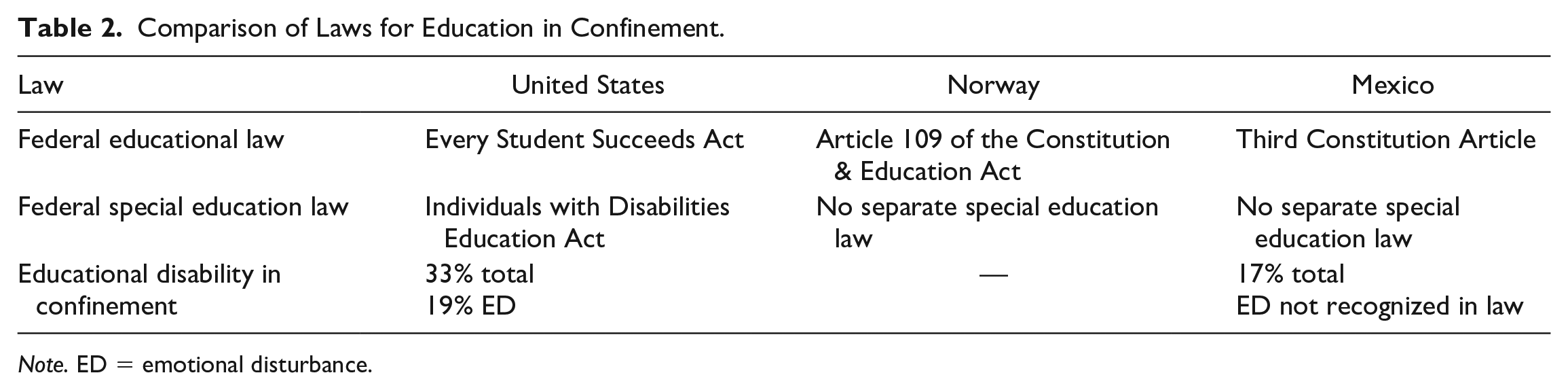
Note. ED = emotional disturbance.
Incarcerated youth in the United States are more likely to have mental health concerns, such as those categorized as emotional and behavioral disorders and educational disabilities, especially emotional disturbance (ED; Cavendish, 2014; Gagnon et al., 2009). Compared with incarcerated male youth, incarcerated female youth experience a significantly greater prevalence of mental health disorders, such as depressive disorders, anxiety, disruptive behavior disorders, and substance use disorders (Leve et al., 2016), which impact emotional and behavioral functioning across settings. Mental health disorders are also prevalent among youth in juvenile facilities in Norway (Fransson et al., 2019; Kayed et al., 2015). The most common disorders among the female youth were internalizing disorders, such as depression and anxiety disorders (Kayed et al., 2015). The term “emotional and behavioral disorders” is not consistently used as a category in the literature or reports on Norwegian youth in juvenile facilities. In Mexico, specific data on emotional and behavioral disorders among incarcerated youth are not available. However, mental health disorders are a common problem inside juvenile justice centers (Carroll et al., 2018), and 71.4% of incarcerated females ages 18 to 29 years were diagnosed with some mental health disorder (Document Analysis and Action for Social Justice [DAASJ], 2019). Given the prevalence of mental health disorders among incarcerated youth, especially female youth, in-facility education, health services, and reentry programs should include a focus on mental health.
Although there is a higher need for mental health services among incarcerated youth in the United States, especially among females, less than 15% receive treatment for mental health problems (Teplin et al., 2013). This results in youth with untreated mental illness being returned to their communities. In Norway, there are no specific statistics on the availability of services for incarecerated youth. However, only 38% of youth in child welfare institutions reported that they had received any help from the Specialist Health Services, which includes mental health services, in the previous 3 months (Kayed et al., 2015). While there are no specific statistics on the availability of services in Mexico, juvenile justice facilities do have a psychologist on staff. However, psychologists in Mexico are not required to have the same level of training and education as those in the United States and their recommendations are often ignored (Carroll et al., 2018). The availability of mental health services also impacts effective reentry programs. Reentry programs refer to those that are designed to help incarcerated youth reenter society and to reduce the risk of reincarceration. For many incarcerated youth, this includes educational programs designed to help youth graduate while incarcerated or reintegrate into public schools.
Reentry programs in the United States focus on what has worked historically for incarcerated males. These programs focus on practical aspects of transitioning back to community settings such as employment or vocation, education, and housing. Female offenders report that while these types of programs are important, relationship-related programs that focus on close personal relationships are integral to successful transition (Herrschaft et al., 2009). Like the United States, services for incarcerated youth in Mexico focus on education, employment, and vocation as priorities. The U.S. and Mexican facilities focus on the practical aspects of reentry; however, Norwegian facilities also place a great emphasis on building relationships between youth and facility staff (Fransson et al., 2019; The Ombudsman for Children, 2020). This is an extension of Norway’s philosophy of adhering to the “principle of normality” (Labutta, 2017, p. 351), that deprivation of liberty is the punishment, and that the punishment must not be more onerous than is necessary for security reasons (Labutta, 2017). Positive relationships between youth and caregivers are shown to increase engagement in educational settings (Martin & Collie, 2019). Engagement in this context is qualified as an increase in academic participation, academic enjoyment, and an increase in future aspirations.
Supporting Data
The Continuum of Juvenile Justice
Youth ages 12 to 18 years in the United States are incarcerated for varying reasons, from minor offenses such as status offenses (i.e., underage drinking and truancy) and substance use, to more serious crimes such as assault, robbery, and homicide. In 2019, approximately 36,500 youth ages 12 to 18 years were placed in secure facilities (Sickmund et al., 2021), with more than half of the youth (58%) incarcerated in juvenile correctional facilities. Although the justice system in the United States was built on the foundation of rehabilitation, over time the focus has shifted to punishment (Labutta, 2017). That is not to say that individual juvenile correctional facilities and state-mandated programs within the United States do not provide for more rehabilitative and preventative services. However, programs and philosophies are not consistent nationwide.
Norway has a very different standard for incarcerating youth and a broader continuum of care, compared with the United States. Labutta (2017) described the Norwegian model as one that applies the “principle of normality (p. 351),” which refers to the viewpoint that although individuals are physically removed from society by means of incarceration, they are not relationally removed. This is achieved by having members of the community provide services to those who are incarcerated. Only those youth ages 15–18 years who commit serious offenses are placed in either adult facilities or juvenile correctional facilities called youth units. Serious offenses may include violent crime, serious threats against a person, and sexual offenses (Statistics Norway, n.d.). Deloitte (2019) reported that 0.026 per 1,000 (0.0026%) youth were incarcerated in 2018, and approximately eight youth are incarcerated on any given day (Statistics Norway, n.d.). Information presented in this database is not interpretable in terms of discussing sex differences because of the low number of incarecreated females.
Youth under the age of 18 in Norway who exhibit severe behavioral difficulties, such as serious or repeated criminal offenses or persistent substance abuse, may be placed in child welfare institutions that are separate from the criminal justice system, to receive treatment (The Child Welfare Act, 1992, §4-24). In 2018, 390 youth were placed in such institutions (The Norwegian Directorate for Children, Youth and Family Affairs, 2019). Due to the recognition that the behavioral difficulties youth exhibit have a variety of causes and treatment needs, Norway has established different institutions aimed at three distinguished target groups: (a) youth who are at low risk of further development of behavioral difficulties, (b) youth who are at high risk for further development of behavioral difficulties, and (c) youth with persistent substance abuse (Deloitte, 2019). According to Deloitte (2019), as of 2018 only 19% of youth in the high-risk institutions were female and the percentage of female youth in high-risk institutions appears to be on the decline.
In Mexico, youth who commit serious crimes are placed in juvenile justice facilities, referred to as adolescent communities (National Law of Integral Criminal Justice System for Adolescents, 2016). Serious crimes may include homicide, sexual offenses, drug-related offenses, and possession of a firearm meant for exclusive use by the army. In a single year, 9,500 youth are confined to juvenile correctional facilities, and only 5.6% are females (National Security Commission, 2021). Placement decisions for youth in Mexico vary depending on their age and the crime committed. For example, youth from 12 to 13 years will not be placed in correctional facilities, even if they commit a serious crime. In these instances, the recommendation is to send the case to an Alternative Justice Center, where a mediation or restorative process can be carried out. Youth may also be placed in adolescent communities, called specialized treatment or internment centers, as an alternative to placement in a juvenile justice facility.
Education in Juvenile Facilities
A salient factor regarding the education of incarcerated youth is that they are more likely to have emotional and behavioral disorders, and educational disabilities, especially ED (Cavendish, 2014; Gagnon et al., 2009). Emotional and behavioral disorders include different mental health disorders, which may be included under the umbrella “emotional disturbance” (Dieterich et al., 2016) when there is adverse educational impact. Characteristics associated with ED include an inability to learn due to unsatisfactory interpersonal relationships, inappropriate behaviors or feelings under normal circumstances, a general pervasive mood of unhappiness and depression, a tendency to develop physical symptoms or fears associated with personal or school problems, or disorders of thought such as schizophrenia (IDEIA, 2004 § 300.8). Cavendish (2014) found that 33% of all incarcerated youth had a recognized educational disability, and 19% of all incarcerated youth were students with ED. This is compared to the 14% of students in public schools with a recognized disability and <1% of youth with ED in public schools (U.S. Department of Education, National Center for Education Statistics, 2021). However, not all youth with emotional and behavioral disorders or mental health disorders are identified with an ED.
In the United States, there are federal education and special education laws specifically designed to protect the right for incarcerated youth to access educational services. These are the IDEIA (2004) and NCLB (2002; Twomey, 2008). The NCLB was reauthorized in 2015 and renamed Every Student Succeeds Act. Although youth in juvenile correctional facilities retain the rights to educational services, the services provided often do not correspond to those in public school settings and fail to meet minimal standards based on evidence-based practices (Mulcahy & Leone, 2012). This includes the failure to provide appropriate special education support for students with disabilities.
Norway also has educational laws that protect the right to education for every individual, including incarcerated youth with disabilities. These rights are established in Article 109 of The Constitution (1814). Furthermore, the Education Act specifies that all students have a right to adaptive education, regardless of disability status. As such, youth in juvenile facilities keep their rights under the Education Act. The Education Act also establishes that special education services are reserved for students who need additional support to benefit from the adaptive measures implemented in general education (Gøranson et al., 2020). However, Gøranson et al. further explained that to receive special education services, students must go through an extensive evaluation process, resulting in a potential delay of access to appropriate services. Teachers from local schools come into the youth units to teach some of the incarcerated youth (The Civil Ombudsman, 2017), while others are permitted to attend local schools (The Prison and Probation Service, n.d.). Youth in child welfare institutions may attend local schools or institution schools (The Ombudsman for Children, 2020), but depending on the availability of resources, access to instruction and services may be delayed for extended periods of time (Rambøll, 2015). There are significantly fewer incarcerated youth in Norway, compared with the United States, and their needs are less well documented. As such, it is unclear if incarcerated youth in Norway are more likely to have educational disabilities.
Mexico’s Third Constitutional Article (Political Constitution of the United Mexican States, 2021, Art. 3) states that every individual has the right to education, including incarcerated youth. The Federal Law to Prevent and Eliminate Discrimination (2014) aims to prevent discrimination against any person and promotes equal treatment for all individuals. It is unclear what the educational performance is for incarcerated youth in Mexico. However, 17% of incarcerated youth were recognized as having disabilities (National Institute of Statistics and Geography, 2020). Moreover, there is no separate category for individuals with emotional and behavioral disorders (Sanchez et al., 2021). In a survey completed with incarcerated youth in Mexico, 67% reported participating in educational programs; however, in most institutions, there were no high-quality educational programs that would allow youth to continue their education while incarcerated (Azaola, 2015). Although all three countries have laws that recognize the educational rights and needs of youth in juvenile facilities, the United States, Norway, and Mexico reported a lack of available resources to support the needs of the youth.
Mental Health and Reentry Service
Although a large portion of incarcerated youth in the United States are screened for mental health concerns (i.e., 57%–91%) and receive more extensive follow-up assessments for mental health and substance abuse problems (i.e., 61%–78%), less than half (4%-41%) received formal services (Desai et al., 2006). Most receive informal counseling and support, but only a small proportion of facilities were formally accredited to meet the standards of care for juvenile facilities (Desai et al., 2006). Female youth are more likely to demonstrate internalizing disabilities, such as depression and anxiety (Barrett et al., 2015), as well as posttraumatic stress disorder (PTSD) and substance use disorders (Karlsson & Zielinski, 2020). While not all youth with mental health disorders receive special education services, elevated internalizing disabilities such as anxiety and depression are strongly related to poor academic achievement, which in turn cause negative emotions that further influence academic performance (Weidman et al., 2015). Providing mental health treatment that focuses on the mental health needs of incarcerated female youth could facilitate educational attainment, either in-facility or when returning to public schools.
Although it is unclear if incarcerated youth in Norway are more likely to have educational disabilities, one of the main characteristics of incarcerated youth is the presence of mental health disorders (Fransson et al., 2019). Additionally, a second main characteristic is prior placement in a child welfare institution (The Civil Ombudsman, 2015). Kayed et al. (2015) found that 76% of youth in child welfare institutions met the criteria for at least one mental health disorder the previous three months, while only 38% reported that they had received help from the Specialist Health Service during the same period. Moreover, female youth were nearly twice as likely to receive mental health services as male youth, even though they were equally likely to have at least one mental health disorder (Kayed et al., 2015).
The purpose of Norway’s child welfare law is to contribute to “children and young people (being) met with safety, love and understanding, and that all children and young people shall experience good and safe conditions when growing up” (The Child Welfare Act, 1992, 1-1). Although personnel in both the youth units and the child welfare institutions place emphasis on positive adult interactions and relationships, the implementation varies between institutions (Fransson et al., 2019; The Ombudsman for Children, 2020). Moreover, the success in developing such relationships in child welfare institutions is reported to be affected by factors such as staff turnover and the availability of resources (The Ombudsman for Children, 2020). The importance of building strong relationships is a priority in Norway; however, there is no reported standarized program or training on how to develop these relationships with youth that is shared across juvenile facilities.
There are no specific data about the mental health disorders present among incarcerated female youth in Mexico. However, among incarcerated adult women in Mexico, 71.4% were diagnosed with some mental health disorder (DAASJ, 2019). Mental health and reentry services are available for incarcerated youth in Mexico, but only 65% of incarcerated youth reported participating in workshops focused on employment or trade skills, and only 21% reported participating in therapy (Azaola, 2015). In a survey of incarcerated youth (Azaola, 2015), 28% reported that they had no plans or aspirations, and 45% felt their lives would remain the same or be worse than when they had entered incarceration. However, it is not clear if this was due to a low availability of services or a lack of engagement in available services. Although the law recognizes the importance of positive social ties between youth and the adults who work with them, Sanchez et al. (2021) reported a lack of properly trained personnel and educational programs that address social-emotional needs of students with mental health disorders.
Conclusion
While all three countries have specialized juvenile justice centers and alternative placement options, they differ in the way they function. Norway and Mexico incarcerate youth only for serious offenses, and Norway’s definition of youth is much narrower than in the United States and Mexico (see Table 1). The United States criminalizes minor infractions such as truancy from school and has the broadest definition of “youth” (i.e., 12–21 years). In addition, Labutta (2017) emphasized that the focus of the justice system in the United States is on punishment, compared with Norway’s justice system, which is focused on rehabilitation.
All three countries have educational laws that protect the right to education for all youth, regardless of placement, and the United States has educational laws that focus specifically on students with disabilities. Despite the laws in place, correctional facilities in the United States often failed to provide educational services to incarcerated youth that meet minimal standards (Mulcahy & Leone, 2012). In Mexico, Azaola (2015) reported a diminished quality of educational services for incarcerated youth. Norway The Ombudsman for Children, (2020) reported a potential delay in academic services for youth in child welfare institutions, based on the availability of staff and resources.
Incarcerated youth in the United States are more likely to have a special education disability compared with those in public school settings, especially ED (Cavendish, 2014; Gagnon et al., 2009), and incarcerated female youth are more likely to have mental health disorders compared with incarcerated male youth (Leve et al., 2016). While there are some services for incarcerated female youth that meet their education and mental health needs, the demand for services in the United States often outweighs the availability. No disability data were available for incarcerated youth in Norway; however, 76% of youth in child welfare institutions had at least one mental health disorder (Kayed et al., 2015), and most youth incarcerated in youth units have a history of placement in child welfare institutions (The Civil Ombudsman, 2015). While male youth in Norwegian child welfare instituions were just as likely to have a mental health disorder, female youth were twice as likely to receive mental health services (Kayed et al., 2015). In Mexico, a 2015 survery of incarcerated youth (Azaola, 2015) revealed 65% of incarcerated youth reported participating in reentry programs focused on employment or trade skills; however, only 21% of incarcerated youth reported participating in therapy .
The reentry programs available in the United States, Mexico, and Norway all focus on practical aspects such as education and employment. While programs that focus on the practical aspects of reentry are important, incarcerated females report a need for programs designed to promote close positive interpersonal relationships (Herrschaft et al., 2009). Norway is renowned for their low crime rates and recidivism rates (Labutta, 2017). In Norway, although there is no standardized programming shared across institutions, prioritizing positive relationships is an important part of the philosophy of working with incarcerated youth. In addition, Norway’s philosophy of adhering to the “principle of normality” (Labutta, 2017, p. 351) is evidenced in the educational programs in the youth units where teachers from local schools are brought in to teach or the youth are permitted to attend local schools.
Prevention, intervention, and rehabilitation programs such as those focused on practical needs (e.g., educational and vocational programs) have historically been generalized from research conducted on incarcerated males and are not satisfactory to meet the needs of incarcerated female youth in the United States. This is particularly concerning due to the rising rates of incarceration of female youth (Parrish, 2020). Incarcerated female youth are more likely to experience mental health disorders such as anxiety and depression (Leve et al., 2016), which are associated with poor academic outcomes (Weidman et al., 2015). Due to instability in housing and care resulting from transitioning between youth care facilities, incarcerated female youth have fewer consistent and secure relationships with adult caretakers, including teachers. As such, providing incarcerated female youth with positive relationship-based programs may be the basis for improving long-term outcomes, including educational outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.