
Abstract
Background
Treatment adherence is central to treatment success in rehabilitation for musculoskeletal conditions, including low back pain (LBP). Unfortunately, non-adherence to prescribed treatment is common and undermines treatment success.
Objective
To identify predictors of treatment adherence in physical therapy for patients with LBP.
Methods
209 cases of patients receiving physical therapy for a chief complaint of centralized LBP were retrospectively analyzed for predictors of treatment adherence. Symptom duration, pain intensity, level of disability, the presence of an opioid prescription, and patient cost were assessed as predictors of treatment adherence. Patients who completed their prescribed plan of care were classified as adherent.
Results
Logistic regression analysis revealed that individuals who had an opioid prescription were 2.56 (95% CI = 1.25–5.24, p = 0.010) times less likely to be adherent with treatment compared to individuals without an opioid prescription. Individuals who had symptoms for less than 1 month were 3.21 (95% CI = 1.12–9.24, p = 0.030) times less likely to be adherent with treatment compared to individuals who had experienced symptoms for 4 months to 1 year. Finally, individuals who paid greater than $40 per visit were 3.45 (95% CI = 1.31–9.09, p = 0.011) times less likely to be adherent with treatment compared to individuals who did not have to pay each visit.
Conclusion
The results of this study may help clinicians quickly identify and address risk factors for lower treatment adherence in patients with LBP to mitigate the impact of suboptimal treatment adherence on patient outcomes.
Introduction
Low back pain (LBP) is a significant health problem that has been ranked as the leading cause of global disability for three decades. 1 The 1-year incidence of LBP is estimated to be between 1.5%–36% with an estimated 24%–80% of individuals with a new episode of LBP experiencing a recurrent episode of symptoms within 1 year.2,3 The health-care costs of LBP have risen drastically with LBP estimated to lead to $300–600 billion in annual health care costs in the United States. 1 The high costs are related to both the high prevalence of the condition and high costs per episode of LBP. 4 In addition, an estimated 149 million workdays are lost each year due to LBP, 5 with two-thirds of the total annual costs associated with LBP related to decreased wages and productivity. 6 Considering the substantial impact of LBP on disability, health care expenditure, and workforce productivity, in 2019 the World Health Organization identified LBP as a major challenge to international health systems. 7
In response to the substantial burden associated with LBP, international guidelines have demonstrated a uniform movement towards non-medical approaches such as physical therapy for patients with LBP.8–11 Physical therapy is a cost-effective treatment for a variety of musculoskeletal conditions, including LBP.12,13 Physical therapy has been shown to reduce health care utilization and LBP related costs over a 1-year period when initiated in the first 3 days following onset. 14 In addition, a recent review of 14 distinct clinical practice guidelines for LBP recommend exercise therapy for patients with chronic non-specific LBP. 15 Unfortunately, up to 45% of patients receiving physical therapy for LBP do not experience significant improvement in pain or reduction in disability. 16 As a result, there is growing interest in identifying factors that predict whether a patient with LBP will experience improved pain and reduced disability from physical therapy treatment.
Treatment adherence is a factor that influences patient outcomes in physical therapy.17–19 Treatment adherence is defined as the extent to which a patient's treatment related behavior (e.g., taking medication, modifying habits, attending physical therapy) corresponds to a health care professional's advice. 20 Treatment adherence in physical therapy is multidimensional, including attendance at prescribed treatment sessions, following practitioner's advice, and compliance with prescribed exercises. 21 Though evidence for the relationship between treatment adherence and patient outcomes is limited regarding LBP, home exercise program (HEP) adherence in patients with LBP is associated with reduced pain and disability. 22 In addition, high levels of treatment adherence are related to better outcomes in individuals treated for osteoarthritis. 17 In community-dwelling, frail elderly individuals receiving multifactorial intervention that included physical therapy, high treatment adherence has been shown to relate to improved outcomes in frailty and mobility when compared to low treatment adherence. 18 Finally, cumulative levels of physical therapy treatment compliance are also associated with clinically significant improvements in pain and disability in patients with rotator cuff pathology. 23
While treatment adherence influences outcomes, poor adherence to treatment is common in health care, including physical therapy. Previous studies have shown that non-adherence to prescribed treatment can reach 70% across multiple conditions and patient populations. 24 Whereas more recent studies evaluating adherence in outpatient physical therapy for LBP have shown variable adherence rates to treatment attendance recommendations with rates of non-adherence ranging from 16.8%–57%.25,26 In addition, a recent systematic review found that patients were most likely to fail to show to physical therapy visits compared to other specialties. 27 Finally, in the literature on HEP compliance in LBP, estimates of the proportion of patients completing their exercises as prescribed vary between 68%–77%.21,22,28 Despite the relatively frequent occurrence of non-adherence in physical therapy, treatment adherence appears to be central to treatment success, which makes identifying factors that influence treatment adherence an important aim. Currently, there is a paucity of strong evidence that clearly identifies factors that influence treatment adherence in physical therapy. An improved understanding of factors that influence patient adherence could allow the identification of barriers and provide practitioners the opportunity to address modifiable factors to promote optimal adherence levels.
Among the factors that have been shown to contribute to reduced treatment adherence in physical therapy are low self-efficacy, depression, anxiety, helplessness, and pain. 19 In addition, a patient's level of education appears to impact treatment adherence in patients with LBP; however, the direction of this relationship is poorly understood due to conflicting study results.24,26,29 In patients with LBP, factors associated with increased treatment adherence include low-level function, higher levels of kinesiophobia, and more advanced age. 26 High disease severity has also been shown to positively influence treatment adherence in patients with spondyloarthropathies. 30 While the preceding evidence demonstrates there have been multiple variables shown to be associated with treatment adherence in a variety of patient populations, there remains a significant gap in the literature for factors that influence treatment adherence in patients with LBP. Therefore, there is further need to identify pre-treatment patient characteristics that predict adherence to physical therapy in patients with LBP. The significance of this study is that it could help identify relevant barriers and aid clinicians in developing strategies to reduce the impact of these barriers in patients at risk for non-adherence.
The purpose of this study was to assess whether common pre-treatment characteristics of subjects with LBP could predict whether patients would be adherent or non-adherent to treatment. It was hypothesized that symptom duration, pain intensity, level of disability, presence of an opioid prescription, and patient cost would be associated with treatment adherence in patients with LBP. More specifically, are these pre-treatment characteristics predictive of treatment adherence in patients with LBP.
Methods
Design
The study design was a retrospective observational analysis. Patient medical records from a rural, multi-site, private practice were reviewed for treatment episodes occurring between December 1, 2016, to December 31, 2018. Data for this retrospective cohort analysis was extracted from the clinic's electronic medical record system. This electronic medical record system contains demographic information, patient characteristics, and clinical documentation for each patient. Permission to conduct this retrospective analysis (Protocol #:20348) was provided on December 12, 2018, by the Texas Woman's University's Institutional Review Board in Dallas, Texas.
Patients
Patient records were entered into the study if they were evaluated for a primary complaint of centralized LBP and were between the ages of 18–85 years. Patient records were excluded if they presented with concomitant treatment diagnoses in addition to LBP (e.g., knee pain, shoulder pain, etc.) or if they experienced symptoms below the gluteal folds. Patient records were also excluded if they had surgery involving the lumbar spine in the past year. Finally, patients were excluded if they had been treated for LBP by a physical therapist in the past year.
Procedures
The retrospective dataset was retrieved from the electronic medical record including patients discharged between December 2016–December 2018. Initially, all cases from the two-year search period were screened by the primary investigator based on the ICD-9/ICD-10 diagnosis codes associated with the case and the patient-reported reason for seeking physical therapy. The primary investigator determined whether cases were appropriate for further analysis if their diagnosis code pertained to LBP (M54.5, S39.012, M54, etc.) or the patient's chief complaint at initial intake included LBP. After the initial screening process, the primary investigator analyzed the electronic medical record of each of the remaining cases utilizing the previously outlined inclusion/exclusion criteria.
If a patient record was appropriate for inclusion into the study, the primary investigator utilized the electronic medical record to extract patient demographic information, Numerical Pain Rating Scale (NPRS), history of symptom duration, Oswestry Disability Index (ODI), the presence of an opioid prescription, and patient cost per visit. The primary investigator excluded six cases that were missing one or more of the preceding variables. Following these procedures, 209 patient cases met all criteria to be included in the study.
Outcome variable
While adherence has been defined as the extent to which a person's behavior corresponds with the recommendations from a health care provider, 20 there is significant variation in how adherence and non-adherence are operationalized in existing literature 31 As previously mentioned, in physical therapy, adherence is multidimensional and includes attendance to prescribed appointments, following practitioner advice, and performance of prescribed interventions. 21 Due to the retrospective nature of this study, measurement of each dimension that makes up treatment adherence was not feasible. In this study, adherence was operationalized as whether a patient completed their prescribed physical therapy plan of care and was present for their final physical therapy visit or not, which was used as a construct for treatment adherence versus treatment non-adherence, respectively. Adherence was treated as a dichotomous variable (adherent or non-adherent) with subjects dichotomized as adherent considered the reference group.
Predictor variables
At the initial evaluation, patients reported their LBP symptom duration, which was recorded by the physical therapist in the patient's electronic medical record. While symptoms persisting greater than 3 months is commonly utilized as the definition of chronic pain,32,33 there was significant variability in how long the patients in this data set had been experiencing their symptoms. To gain a better understanding of the role of symptom duration on treatment adherence, symptom duration was categorized into four distinct categories: 0–4 weeks, 1–3 months, 4 months–1 year, and >1 year. Symptom duration was treated as a categorical variable due the limitations in participants being able to accurately recall when their symptoms began, particularly in participants with more persistent symptoms. Acute pain, defined as having symptoms for 0–4 weeks, was the reference category for this variable.
Patients were asked to rate their current pain using the NPRS during their initial evaluation, which was recorded by the physical therapist in the patient's electronic medical record. The NPRS is a commonly used outcome measure for patients with LBP. The NPRS is an 11-point scale with zero rated as no pain and 10 rated as worst pain imaginable. The NPRS exhibits adequate-to-excellent test/retest reliability in patients with chronic pain 34 and adequate responsiveness in patients with LBP. 35 The NPRS was utilized as a continuous predictor variable to determine whether the baseline level of pain intensity would be a predictor for treatment adherence.
Patient cost per visit, which was determined prior to the initiation of care for each patient, was retrieved from the patient's electronic medical record. The following patient cost categories were used: no cost ($0), low cost ($1–$19), moderate cost ($20–$39), and high cost (≥$40). Patient cost was treated as a categorical variable due to the distinct clusters of patient cost data that is related to the current trends in co-pay, co-insurance, and deductibles. No cost was the reference category for this variable.
The presence of an opioid prescription was considered another potential predictor of treatment adherence. To determine the influence of an opioid prescription on treatment adherence, the primary investigator reviewed the medication list in the patient's electronic medical record for the presence of an opioid prescription, which was treated as a dichotomous variable (opioid prescription or no opioid prescription). The absence of an opioid prescription was the reference category for this variable.
The ODI is a patient-reported questionnaire that gives a subjective percentage score of the level of disability a patient with LBP is experiencing. The ODI includes 10 items with each item consisting of six statements correlating to scores of zero (least disability) through five (greatest disability). Scores are calculated by dividing the total score of the 10 items by 50. The score is then multiplied by 100 to determine the percentage disability level of the patient. The ODI has been shown to have adequate-to-excellent validity,36,37 adequate-to-excellent test-retest reliability, 38 and adequate-to-excellent responsiveness. 37 The ODI was administered to patients at the date of their initial evaluation and recorded into the electronic medical record. The baseline ODI was utilized as a continuous predictor variable to determine whether the baseline level of disability would be a predictor for treatment adherence.
Data analysis
Statistical Package for Social Sciences (SPSS) Version 25 (IB Corporation, Armonk, NY) was used for all statistical analyses. Descriptive analysis, including means with standard deviations and frequency counts, were used to describe the patient sample. Binary logistical regression analysis with multiple predictors was used to determine the best set of predictors for treatment adherence. Regression results were expressed in odds ratios with 95% confidence intervals. A two-tailed significance level of .05 was set for all analyses. For predictor variables with odds ratios less than one, the inverse of the odds ratio (1/OR) was utilized to provide a simpler interpretation of the relationship between the predictor variable and the outcome variable, treatment adherence.
Results
For this study, 1073 patient cases were identified in the initial search. Of the 1073 patient cases, 184 cases were removed from data analysis prior to analysis utilizing the study's inclusion/exclusion criteria as the cases were not relevant to the focus of the current study or were inaccurate entries into the electronic medical record. Therefore, 889 cases were analyzed by the primary investigator utilizing the study's inclusion/exclusion criteria. 215 patient cases met the inclusion criteria for the study, but due to missing data in the patient's electronic medical record, only 209 cases were included in the final analysis. Figure 1 illustrates participant flow for the study.
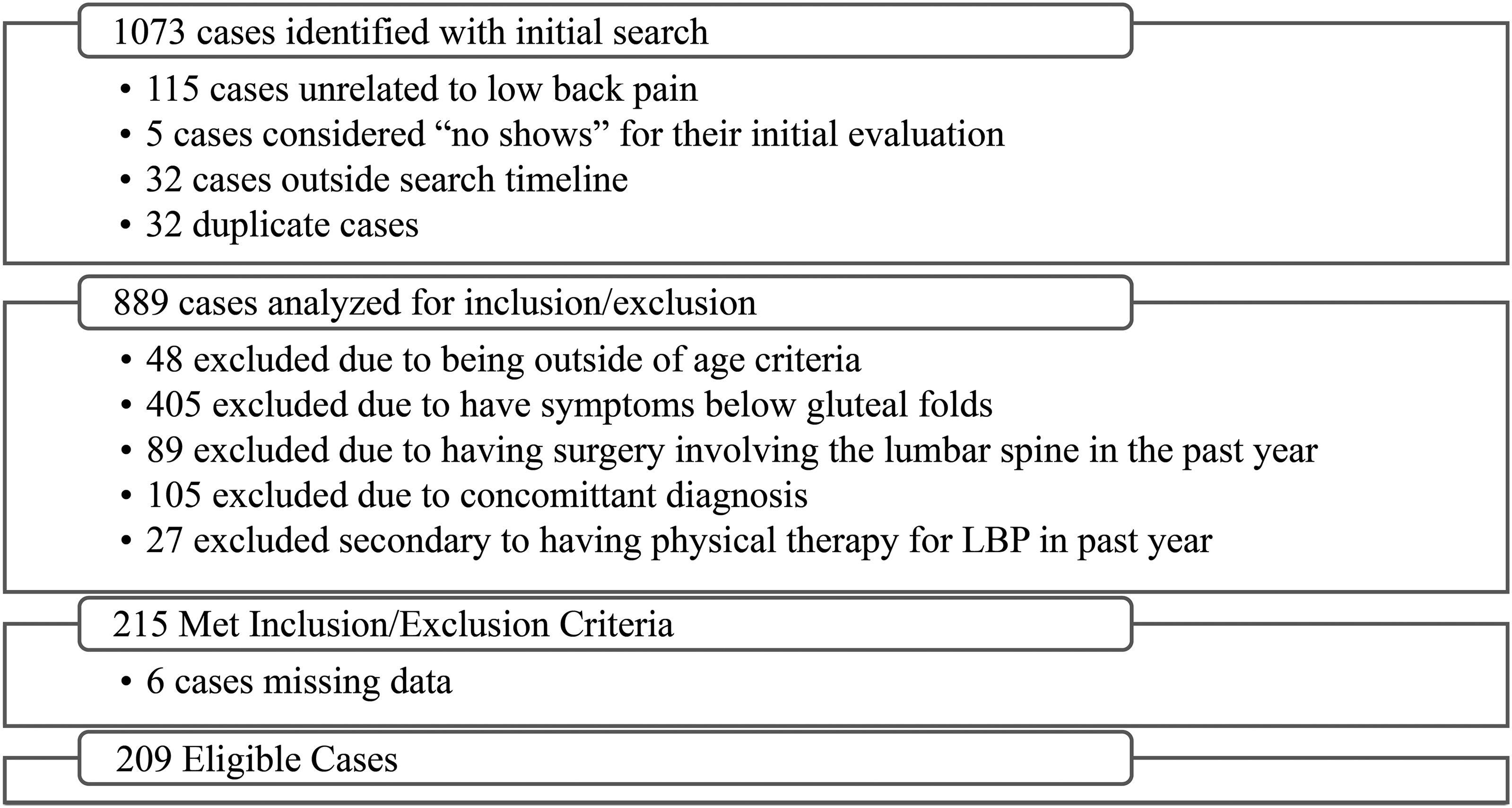
Flow of patient case inclusion/exclusion in the study.
Table 1 provides the baseline characteristics for the 209 subjects included in the study. Table 1 also includes a comparison of baseline characteristics between the 128 subjects (61.3%) dichotomized as adherent versus the 81 subjects (38.7%) who were dichotomized as non-adherent. The baseline characteristics of both groups were similar with the subjects dichotomized as adherent 7 years older and more likely to be male compared to the subjective dichotomized as non-adherent.
Baseline characteristics of patients included in the study.

Note. SD = standard deviation; NPRS = Numerical Pain Rating Scale; ODI = Oswestry Disability Index; Patient cost = patient cost/visit.
A summary of the logistic regression analysis is included in Table 2. The logistic regression model was statistically significant, X2(9) = 33.25, p = <0.001. The model explained 20.0% (Nagelkerke R2) of the variance in treatment attendance and correctly classified 66.0% of the cases. Of the five predictor variables, three were significant: the presence of an opioid prescription, symptom duration and patient cost. Individuals who had an opioid prescription were 2.56 (95% CI = 1.25–5.24, p = 0.010) times less likely to be adherent with treatment compared to individuals who did not have an opioid prescription. In addition, individuals who had symptoms for less than 1 month were 3.21 (95% CI = 1.12–9.24, p = 0.030) times less likely to be adherent with treatment compared to individuals who had experienced symptoms for 4 months to 1 year. Finally, individuals who paid greater than $40 per visit were 3.45 (95% CI = 1.31–9.09, p = 0.011) times less likely to be adherent with treatment compared to individuals who did not have to pay each visit. Baseline pain intensity and level of disability (ODI) were not significant predictors for treatment adherence in the logistic regression analysis.
Summary of logistic regression analysis of the associations between patient characteristics and treatment adherence.

Note. CI = confidence intervals; Opioid Prescription = the presence of an opioid prescription; NPRS = Numerical Pain Rating Scale. Categorical variables in the model had the following reference category: opioid prescription, participant without an opioid prescription; symptom duration, 0–4 weeks; Patient cost per visit, $0.
Indicates statistically significant values (p < .05).
Discussion
The purpose of this study was to assess if pre-treatment characteristics of patients with LBP could predict whether patients would be adherent or non-adherent to treatment. The results of this study revealed that high patient cost, the presence of an opioid prescription, and symptom duration less than 4 weeks have predictive value for lower treatment adherence in patients with LBP.
High patient costs as a predictor for lower treatment adherence is not a surprising finding considering the strong relationship between higher patient cost and lower medication adherence in the medical literature. 39 In addition, a recent investigation showed that patient costs of $30 or more per visit reduced the likelihood of a patient with LBP attending physical therapy by 29% compared to patients with no cost per visit. 40 The negative impact of higher patient cost on treatment adherence is particularly concerning when, in fact, physical therapy treatment for LBP has been shown to reduce overall healthcare and patient out-of-pocket costs by reducing the use of radiographic imaging, specialty physician visits, injections, emergency department visits, and surgery.13,41 With the results of the current study in mind, physical therapists should take patient cost into consideration when developing their plan of care recommendations. One way to reduce the burden of high costs for patients is reducing the frequency of in-clinic treatments. In addition, clinicians may be able to mitigate the impact of high cost on treatment adherence by improving a patient's personal cost-benefit analysis through providing patient-directed education that highlights the cost-effectiveness of physical therapy for LBP. While high patient cost presents a challenge for clinicians seeking to maximize treatment adherence and patient outcomes, early identification can provide the opportunity to minimize this burden's effect and improve treatment adherence to physical therapy.
Though physical therapy in the initial management of LBP has been shown to substantially decrease early and long-term use of opioids,41–43 the effect of an opioid prescription on treatment adherence has not been previously investigated. The findings of the current study demonstrate that the presence of an opioid prescription significantly increased the odds of a patient with LBP not adhering to their prescribed treatment. Understanding this complex relationship is challenging, and it is important to note that a study of this nature can only show an association between opioid use and treatment adherence, not a cause-and-effect relationship.
However, one potential reason for the finding that the presence of an opioid prescription influences treatment adherence is that patients who receive an opioid prescription for LBP demonstrate higher pain intensity and greater disability compared to individuals who do not receive an opioid prescription for LBP. 44 Higher symptoms at baseline could have led to patients to seek out other health care options prior to the completion of their physical therapy plan of care and may have contributed to poor treatment adherence. In addition, individuals who are prescribed opioids for LBP demonstrate lower self-efficacy, higher levels of movement-related fear, and higher levels of pain-catastrophizing, 44 which are variables that have been previously linked to lower treatment adherence. 19 Finally, prescription opioids have shown little to no positive effects in improving pain or disability long-term, 45 so individuals that had been taking these medications for an extended period may have experienced higher levels of helplessness, which has also been indicated as a deterrent to treatment adherence. 19 The findings of the current study highlight the importance of clinicians being aware of the presence of an opioid prescription and how it could impact a patient's treatment adherence. Future studies investigating this relationship should seek to better understand how daily opioid dosage, duration of opioid prescription, and medication adherence to an opioid prescription influence treatment adherence in this population.
Shorter symptom duration as a predictor of treatment nonadherence was an unexpected finding in this study. However, this may be related to the fact that patients with LBP who demonstrate symptoms of shorter duration recover faster compared to individuals with longer symptom duration. 46 In fact, most patients with an acute episode of LBP experience marked improvement in symptoms within 6 weeks following initial onset regardless of the type of treatment they receive. 47 The evidence surrounding acuity and its relationship with the rate of symptom improvement supports the notion that patients in the current study may not have completed their plan of care in its entirety due to the rapid resolution of their symptoms. These findings suggest that clinicians should consider shortening their plan of care duration recommendation for patients presenting with acute LBP. While the prognosis for an acute episode of LBP is favorable, one-to-two-thirds of individuals who recover from an initial onset of LBP experience recurrence of their symptoms in one year.48,49 Therefore, clinicians should also consider early patient education on self-management strategies that patients can utilize if they experience future symptom recurrence.
While the findings of the current study demonstrate that patients with symptoms less than 1 month are less likely to be adherent compared to patients with symptoms 4–12 months, there was not a significant difference between patients with symptoms less than 1 month and greater than 1 year. This may be related to the wide range of symptom duration in the patients categorized as having symptoms greater than 1 year. The symptom duration of patients in this category ranged from 13 months to 36 years. The variability in time since symptom onset in this group likely reflects other variations in this subset of participants, which is difficult to measure and understand due to the retrospective nature of this study.
The two predictor variables included in this study that did not significantly influence treatment adherence were pain intensity (NPRS) and the baseline disability (ODI). While the literature has not previously investigated this relationship, higher levels of disability at baseline have been associated with poorer outcomes in pain and disability in patients with LBP.50–52 Therefore, it was hypothesized that higher levels of symptom severity at baseline would influence treatment adherence. While subjects dichotomized as non-adherent did have higher levels of pain and disability at baseline, the influence of these measures on treatment adherence in this study was not significant.
Finally, while age was not a predictor variable of interest in this study, patients categorized in the adherent group (Mean age ± SD = 66.5 ± 15.0) were older than patients categorized in the non-adherent group (Mean age ± SD = 59.4 ± 16.8). A 2020 study by Dhondt et al. showed that higher age was associated with an increased likelihood that participants would complete a rehabilitation program for LBP. In the preceding study, there was a 5.1% increase in the odds that participants would be considered adherent for every one-year increase in age. While the study by Dhondt et al. (2020) demonstrated the association between age and treatment adherence, this is currently the only literature supporting this association. Therefore, the role of age in treatment adherence requires further investigation in future studies.
Strengths
The current study exhibits definite strengths. One strength of this study is the large sample of patients with LBP included. Though this study was retrospective, the adequate sample size allows for more precise estimates of predictive power. In a logistic regression analysis, appropriate sample size is determined by the minimum number of cases per predictor variable. Based on the two continuous predictor variables and number of categories in the three categorical predictor variables used in this study, a sample size of 90 cases would be appropriate. 53 In the current study, the sample size of 209 cases surpasses the suggested sample size for adequate power. In addition, the present study's findings provide clinicians with insight regarding the role of patient-specific factors on treatment adherence, which can be identified upon the onset of care in patients presenting with LBP. Identifying the presence of high patient out-of-pocket costs and shorter symptom duration at the onset of care will allow clinicians to address these factors by providing early patient education and modifying their plan of care recommendations. Another strength of this study is that the patients included were treated by physical therapists and physical therapist assistants with varying levels of education, years of clinical practice, treatment philosophies, and experience in treating patients with non-specific LBP. The diversity of clinicians involved in the treatment of patients in this study improves the generalizability of our findings and reflects the diversity of outpatient clinical practice in physical therapy.
Limitations and recommendations
This study, however, also has limitations. The primary limitation is the lack of control of potential confounding variables secondary to the retrospective nature of this study. This study does not assess the presence of psychosocial variables such as fear avoidance, anxiety, pain catastrophizing behaviors, depression, and self-efficacy. While these factors have been shown to influence treatment adherence, 19 pain, and disability in various populations,54–57 the influence of these variables on treatment adherence has not been thoroughly assessed in patients with LBP. Identification of psychological barriers for treatment adherence during the initial patient assessment may be important for clinicians to adopt appropriate management strategies to promote improved treatment adherence. Another limitation is that while this study shows that adherence is associated with multiple variables, this study cannot provide an understanding of why subjects were not adherent. In future prospective research, reasons for missed appointments or incomplete episodes of care should be assessed to provide a more thorough understanding of this important issue.
Conclusion
This study identified that patient cost, the presence of an opioid prescription, and shorter symptom duration are barriers to treatment adherence in individuals with centralized LBP. The results of this study may help clinicians quickly identify and address risk factors for lower treatment adherence in patients with LBP. Through improving treatment adherence, clinicians can potentially mitigate the negative influence that suboptimal treatment adherence can have on patient outcomes, which would further enhance the impact that physical therapists and physical therapist assistants have on the global burden of LBP.
Footnotes
Acknowledgements
The authors would like to acknowledge Krystal Rosario-Perez and Diana Huynh for their assistance in data collection.
Ethical considerations
Permission to conduct this retrospective analysis (Protocol #:20348) was provided on December 12, 2018, by the Texas Woman's University's Institutional Review Board in Dallas, Texas.
Informed consent
Not Applicable.
Author contributions/CRediT
Dr Seth Watson PT, PhD was the primary author and contributed to multiple roles including study design, data collection, data analysis, and manuscript writing.
Dr Mark Weber PT, PhD was a contributing author and contributed to multiple aspects of the study including data analysis, data interpretation, and manuscript review/editing. Dr Mark Weber also critically revised the manuscript for important intellectual content and approved the final version of the article for publication.
Dr Elaine Trudell-Jackson PT, PhD was a contributing author and contributed to multiple aspects of the study including study design, data analysis, and manuscript review and editing. Dr Elaine Trudell-Jackson also critically revised the manuscript for important intellectual content and approved the final version of the article for publication.
Dr Kelli Brizzolara PT, PhD was a contributing author and contributed to multiple aspects of the study including data analysis, data interpretation, and manuscript review/editing. Dr Kelli Brizzolara also critically revised the manuscript for important intellectual content and approved the final version of the article for publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that supports the findings of this study are available on request from the corresponding author, Dr Seth Watson, PT, PhD.