
Abstract
Background
In recent years, the effect of low level laser therapy (LLLT) on pain in tendinopathy has been increasingly evaluated in clinical trials. However, conflicting evidence regarding its use persists.
Objective
The aim of this review is to evaluate the effect of LLLT on pain in the management of tendinopathy, and investigate the influence of LLLT parameters on the effect size of pain score.
Methods
Searches of eight databases were conducted from inception to Jan 2025. Meta-analyses were conducted where possible, using either a fixed- or random-effects model, standardized mean differences (SMDs), and tests of heterogeneity. Multivariable meta-regression was performed to identify significant predictors of the effect size in pain score.
Results
Thirty-five clinical controlled trials were identified and included in the meta-analyses. Compared to minimal intervention, LLLT provided superior pain relief in chronic tendinopathy, with pooled SMD −0.57(95% confidence interval [CI] −0.93 to −0.20, P = 0.002) after sensitivity analysis (15 RCTs, 299 participants in the experimental group and 282 participants in the control group). Additionally, the total number of sessions was a significant predictor of the effect size of pain relief (P < 0.05), after adjusting for age.
Conclusions
LLLT is more effective than minimal intervention for pain relief in chronic tendinopathy. Greater total number of treatment sessions may be associated with a greater extent of pain relief.
Other
No funding was received for this review. PROSPERO registration number (CRD42021256567)
Introduction
Tendinopathy poses a substantial socioeconomic burden on society, 1 and it affects the mobility and quality of life among the individuals. 2 To date, a plethora of treatment options, that is, therapeutic modalities, exercise protocols and surgical interventions have been evaluated.3,4 In particular, low lever laser therapy (LLLT) has been increasingly scrutinized in clinical trials over the past decade, 5 plausibly due to the publication of World Association for Laser Therapy (WALT)'s guidelines. 6
Despite it has been more than a decade since the works of Tumilty et al. (2010) have been published, the clinical effectiveness of LLLT remains uncertain. The conflicting evidence regarding the use of LLLT remains apparent in the varying conclusions drawn from the numerous reviews published in recent years. For example, some reviews have reported that LLLT is effective in the management of tendinopathy,7,8 but not others.9–12 As a result, the clinical effects of LLLT on tendinopathies are still not clearly expressed, 4 and the progress in understanding the clinical effectiveness of LLLT in tendinopathy remains limited.
There is also an lack of understanding of the relationship between parameters of LLLT, and the extent of pain- relief in tendinopathy, despite the previous works in the literature.13,14 In a previous review, the optimal parameters were determined by vote counting. 15 For example, Tumilty et al. (2010) reported two-third of the studies (i.e., 4 out of 6) which showed positive results used parameters that met the WALT guidelines. To date, the relationship between irradiation parameters such as frequency of LLLT and pulse duration, and outcome measures such as pain has also been investigated. 16 However, other parameters which are often adjusted or determined clinically by practitioners, such as wavelength, energy density, frequency of treatment sessions per week and total number of sessions have not been studied.
Therefore, we conducted a systematic review of randomized controlled trials to compare the effect of LLLT (intervention) against minimal intervention or other forms of treatments (comparison) on pain relief (outcome) in individuals with tendinopathy (participants). We included trials involving individuals with tendinopathic pain, defined as pain associated with tendon injury. As a secondary objective, we examined the impact of LLLT parameters, such as wavelength (nm), energy density (J/cm2), frequency of sessions per week, and total number of treatment sessions of LLLT on the effect size of pain score.
Methods
The study protocol was registered on PROSPERO (http://www.crd.york.ac.uk/PROSPERO/; registration number CRD42021256567). This review was also conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 17
Search strategy
We conducted a comprehensive literature search across multiple databases, including MEDLINE (1966-present), CINAHL (1966-present), Embase (all years), Cochrane Central Register of Controlled Trials, Physiotherapy Evidence Database (PEDro), ProQuest Dissertations and Theses databases, Scopus, and OTseeker, to identify studies on the use of LLLT for pain management in tendinopathy. The most recent search was conducted on Jan 6, 2025, using the following search terms: low power laser therapy; low power therapeutic laser; low power light therapy; low level therapeutic laser; low level light therapy; low level laser therapy; low intensity therapeutic laser; low intensity light therapy; near infrared laser therapy; photobiomodulation; pain; tendino*; tendonitis (Supplementary 1). The reviewers adhered to a pre-defined selection process established before the start of the review, which included a checklist for inclusion criteria. Articles were considered eligible for inclusion if they were randomized controlled human trials and included individuals with acute (less than 6 months) 18 or chronic pain (greater than 3 months) 19 associated with tendon disorders, assigned the experimental group to receive treatment that included LLLT, assigned the comparison group to receive alternative interventions excluding LLLT, and lastly, included pain score as a short-term outcome measure. Two reviewers (B.W.D.Y and E.C.W.L) independently assessed study eligibility. Any disagreements were resolved by consensus.
Data extraction and quality of trials assessment
The methodological quality of the trials was assessed using the PEDro scale, 20 evaluating, key domains such as population, treatment allocation, blinding, prognostic comparability, and analysis. Data extraction included trial participants characteristics (age, gender, and duration of condition), intervention details (type of laser, wavelength in nm, frequency in Hz, pulse duration in nsec, average power output in mW, energy density in J/cm2, number of sessions per week, study duration in weeks, and/or total number of sessions), and pre-intervention and post-intervention pain scores. A standardized extraction form was used for consistency.
Risk of bias was assessed using the Cochrane risk-of-bias tool, which examines five distinct bias domains: selection bias, performance bias, detection bias, attrition bias, and reporting bias. If pain scores were reported for multiple activities or time points, the pre- and post-intervention pain scores reflecting the worst mean difference were extracted. 21 Pain scores were approximated using available median value and interquartile range, whenever they were not presented in mean and/or standard deviation.22,23 Correspondences with the authors via emails were attempted when there was insufficient information about the outcomes to permit data analysis. 24
Quantitative data synthesis and analysis
Inter-rater reliability analyses were conducted using IBM SPSS Statistics 21.0 for Windows (IBM Corp, Armonk, NY). Agreement on the total quality score was assessed using Kappa statistics, 25 and was classified as poor (<0.00), slight (0.00–0.20), fair (0.21–0.40), moderate (0.41–0.60), substantial (0.61–0.80), or almost perfect (0.81–1.0). 21
Where feasible, results were pooled using formal meta-analytical techniques with Review Manager (RevMan) for Windows (Version 5.4, The Cochrane Collaboration, 2020). To account for variations in outcome scales across studies, standardized mean differences (SMDs) for pain score, along with their 95% confidence intervals (Cis), and tests of heterogeneity (χ2) were calculated. 21 SMD, an indicator of effect size, was interpreted as small (0.2), moderate (0.5) and large (equal or greater than 0.8). 26 The I2 statistic was used to determine the degree of between-trial heterogeneity. 21 The I2 value was interpreted as low (25%), moderate (50%), and high (75%) level of heterogeneity, respectively. 27 Fixed-effect or random-effects models were applied as appropriate, based on the assumed commonality of effect size. 28 For instance, data were amalgamated using a random-effects model, if trials exhibited differences in ways that might potentially influence the pooled outcome. 28
Subgroup analyses were performed based on the intervention (control arm) strata. The use of this method has been previously reported, and it renders the control arm more comparable to the intervention arm. 21 For instance, trials in which participants received no LLLT or sham LLLT when assigned to the control groups were categorized as ‘LLLT versus minimal intervention’. This grouping also included trials which utilizes other methods of ensuring minimal intervention in the control arm by providing both groups with exercise or treatment modalities such as ultrasound or hotpack. Conversely, trials in which participants received treatment (other than LLLT) when assigned to the control groups were categorized as ‘LLLT versus other forms of intervention’. The differences in pre- and post-intervention pain score were computed such that negative differences showed that the results supported LLLT, whilst positive differences showed that the results supported either minimal intervention or other forms of intervention. 29
To examine the impact of energy density, treatment frequency per week, total number of LLLT sessions and wavelength on the effect size of pain score, we performed multivariable regression analyses if there were at least 10 available studies. 30 Statistical significance was set at P < 0.05 for all analyses. To assess the risk of publication bias, particularly the non-publication of small trials with negative results, we plotted SMD against SE and visually inspected the symmetry of this ‘funnel’ plot.
Quality of evidence assessment
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) system was used to determine the quality of evidence for pain score included in the meta-analyses.31,32 GRADE evaluate evidence across five domains (risk of bias, publication bias, imprecision, inconsistency and indirectness), classifying the quality of evidence as high, moderate, low or very low. Under this system of evaluation, randomized controlled trials are initially considered as high-quality evidence, while observational studies start as low-quality evidence corroborating estimates of intervention effects. Two independent reviewers (B.W.D.Y and E.C.W.L) assessed the quality across these domains, adjusting ratings as necessary, and the overall quality of evidence was determined for pain outcome.
Results
Study selection
The initial electronic database search yielded a total of 227 articles. Figure 1 illustrates the review process detailing the inclusion and exclusion of articles.

Selection process for studies included in analysis.
Methodological quality
There was substantial agreement between the two reviewers (κ = 0.881, P < 0.001), with agreement rates ranging from 91.1% to 100% across the individual items. Based on the PEDro scale, the trials had a mean methodological quality score of 5.84 (range = 2–9) out of a possible 10 points (Table 1). Commonly unmet criteria included the concealment of allocation, blinding of treating therapists, and blinding of patients.
Details of the included randomized controlled trials.

Mean and/or SD not reported.
Values which gave worst outcome (mean difference) were extracted; when pain measures were reported in more than 1 activity, outcome, or condition.
Gender not reported.
FFI, Foot Function Index (score out of 230); modified MPQ, McGill Pain Questionnaire (score out of 300); RCT, Randomised controlled trial; SF-36 Bodily Pain, Short-Form-36 Bodily Pain subscale (score out of 100); SF-MPQ TPS, Short-form McGill Pain Questionnaire Total Pain Score (score out of 45); SPADI Pain, Shoulder Pain and Disability Index Pain subscale (score out of 50); VAS, Visual Analog Scale (score out of 10-cm or 100-mm).
Study characteristics
Thirty-five trials (762 patients in the experimental group and 789 patients in the control group), which had data for measures of pain, were available for pooling (Figure 2). Fifteen trials evaluated the effects of LLLT on tendinopathic pain over the shoulder,33–47 12 trials over the elbow,48–59 4 trials over the foot/ankle,60–63 3 trials over the hand/wrist,64–66 and 1 trial over the knee. 67 About one-third of the trials were found to have low risk of bias. Evidence of asymmetry and considerable symmetry were visually confirmed in the funnel plots, that is, Figure 3(a) and (b) respectively. The studies were symmetrically distributed around the combined effect size, with a relatively balanced concentration on either side of the SMD, as shown in Figure 3(b). However, this was not observed in Figure 3(a).

Forest plot (effect size and 95% CI) of pain which compared (a) laser versus minimal intervention, and (b) laser versus other forms of intervention in randomized controlled trials. The pooled estimates of standardised mean difference in pain and its confidence interval are shown in shoulder tendinopathy (solid triangles), elbow tendinopathy (solid diamonds), wrist tendinopathy (solid squares), knee tendinopathy (vertical line) and foot/ankle tendinopathy (solid circles). Pooled estimates of subgroup clinical conditions are indicated by empty symbols, whilst pooled estimate of all clinical condition is indicated by the cross.
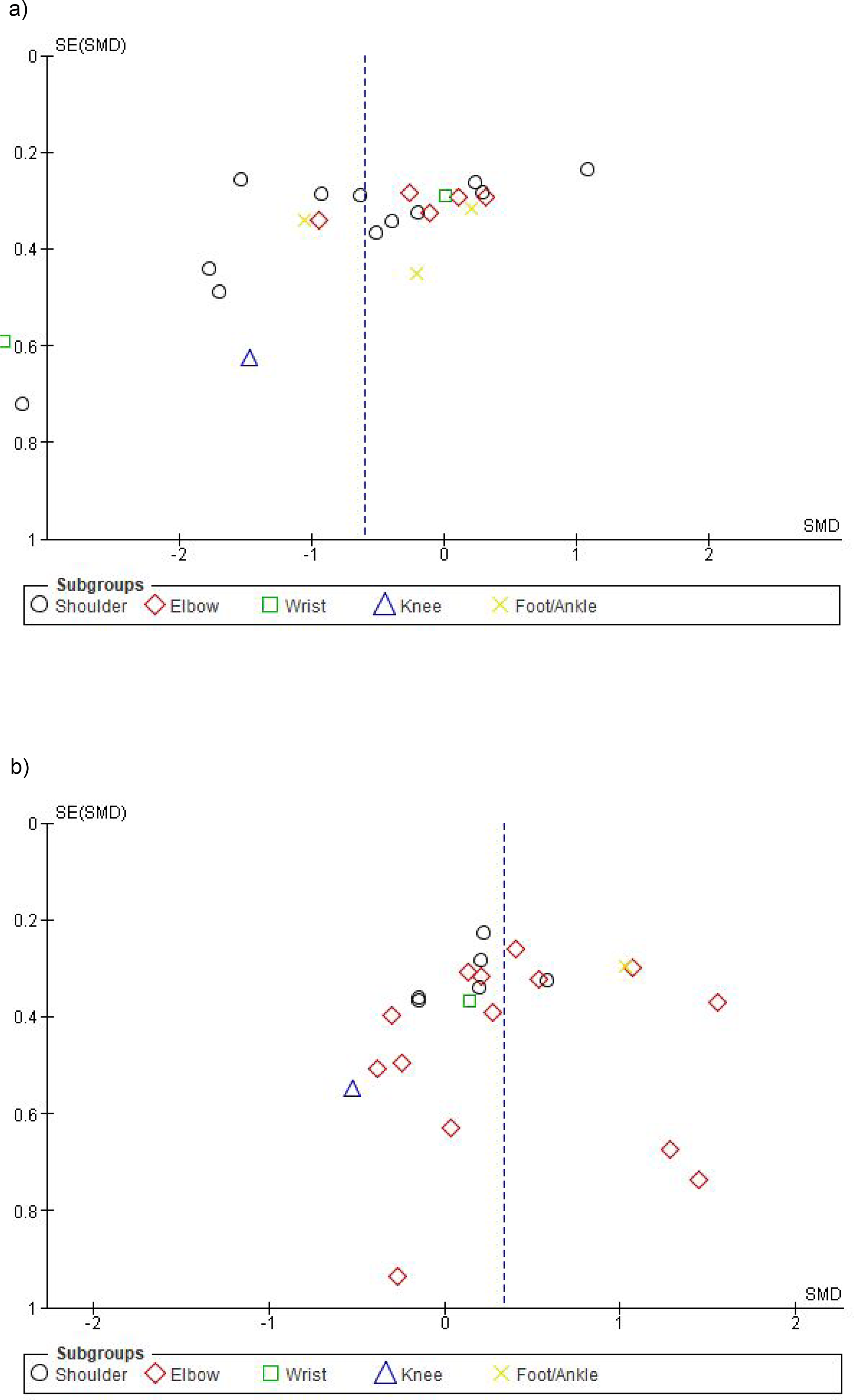
Funnel plot of standardised mean difference (SMD) against standard error of SMD in pain score which compared (a) laser versus minimal intervention, and (b) laser versus other forms of intervention in randomized controlled trials.
LLLT versus minimal intervention
Data were pooled using a random-effects model, revealing a significant pooled standardized mean difference in pain (−0.59, 95% CI −0.96 to −0.23, P = 0.001) between LLLT and minimal intervention. However, high level of heterogeneity was observed (I2 = 86%, τ2 = 0.66, χ2 = 157.22, df = 22, P < 0.001) (Figure 2(a)). Given the high level of heterogeneity, two post-hoc sensitivity analyses we conducted. First, we removed two outlier studies,38,64 yet the pooled standardized mean difference in pain between LLLT and minimal intervention remained significant (−0.40, 95% CI −0.73 to −0.07, P = 0.02). Despite this adjustment, heterogeneity remained high (I2 = 83%, τ2 = 0.47, χ2 = 114.99, df = 20, P < 0.001). Secondly, we included only trials which studied chronic tendinopathy,35–38,41–43,47–49,51,52,60–62 that is, by excluding one trial with acute tendinopathy, 50 one trial with a mix of acute and chronic tendinopathy, 39 and six other trials which did not report chronicity of tendinopathic condition.33,34,40,64,65,67 The pooled standardized mean difference in pain between LLLT and minimal intervention in chronic tendinopathy remained persistently significant (−0.57, 95% CI −0.93 to −0.20, P = 0.002) with a high level of heterogeneity (I2 = 77%, τ2 = 0.39, χ2 = 61.42, df = 14, P < 0.001).
LLLT versus other forms of intervention
When comparing SMD in pain between LLLT and other forms of treatment, the pooled SMD in pain between the groups was significant (0.33, 95% CI 0.12 to 0.55, P = 0.002) (Figure 2(b)) with a moderate level of heterogeneity (I2 = 47%, τ2 = 0.12, χ2 = 41.73, df = 22, P = 0.007). Similarly, we followed up with another two post-hoc sensitivity analyses. After removing an outlier, 49 the pooled SMD in pain between the groups remained significant (0.28, 95% CI 0.10 to 0.47, P = 0.003) with a low level of heterogeneity (I2 = 32%, τ2 = 0.06, χ2 = 30.78, df = 21, P = 0.08). Conversely, after the removal of trials which studied acute tendinopathy45,55,58 and those which did not report chronicity of tendinopathy,44,63 the pooled standardized mean difference in pain between LLLT and other forms of intervention in chronic tendinopathy was not significant (0.25, 95% CI −0.03 to 0.54, P = 0.08) with a moderate level of heterogeneity (I2 = 54%, τ2 = 0.18, χ2 = 34.50, df = 16, P = 0.005).
Predictors of LLLT pain-relieving effect
The most commonly used parameters of LLLT were 904 nm,36,38,43,49,51,65 3 sessions/week34,35,38–41,47,48,51,61,62,64 for 12 sessions 35,47,48,52,61,62,64 (Table 2). The energy density of LLLT (J/cm2) was commonly not reported.38,43,49,60,65,67 After adjusting for age, the multivariable meta-regression analysis identified total number of session (n) (Beta = 0.296, P = 0.037) as an independent predictor of the effect size in pain score among participants with tendinopathy (Table 3). In other words, the greater total number of sessions was associated with greater effect size in pain score after adjusting for covariates such as age. The model correctly predicted 70.2% of the variability in the effect size of pain score.
The parameters of low lever laser used by the various studies (n = 23).

Predictors for low lever Laser treatment effect size in tendinopathy (via multi-variable linear regression analysis).

B, regression coefficient; SE, standard error of B ; Beta, Beta coefficient ; t, t-statistics ; 95% CI, 95% confidence interval for regression coefficient.
GRADE
Supplementary Material 2 summarizes the strength of evidence based to the GRADE criteria, with overall certainty of evidence ranging from very low to moderate.
Discussion
LLLT is superior to minimal intervention
This systematic review has synthesized the evidence for the effectiveness of LLLT as a modality for pain relief (SMD =−0.59, P = 0.001) when compared to minimal intervention in patients with tendinopathy. This is borne out to be a reduction of 2.47 points in pain score, and it concurs with a recent review which reported a similar reduction, albeit smaller, of 1.06 points in pain score (Figure 3(b), p.9 therein). 68 Another review which investigated shoulder tendinopathy reported pain reduction of approximately 1.6 to 2 points (Figure 2, p.116 therein). 8 Taken together, the extent of pain relief when comparing LLLT and minimal intervention in the management of tendinopathy is considered clinically meaningful within the context of musculoskeletal conditions. 69
LLLT is not superior to other forms of intervention
Our review has shown that LLLT is not superior to other forms of intervention for pain relief in chronic tendinopathy as evident with our post-hoc sensitivity analysis result. This findingis consistent with that of Tripodi et al. (2021), who similarly reported that LLLT was equally as effective as other forms of intervention in reducing pain during the management of tendinopathy (Figure 3(a), p.9 therein). 68 Our finding suggests that LLLT should not be used as a standalone, but rather as an adjuvant therapy during the management of tendinopathy. This assertion is supported by trials which reported significantly and clinically meaningful moderate to large effect size in pain score when using LLLT as an adjunct to exercise therapy in our review.33,51,60,64,67 This is not surprising as exercise has been reported to garner good evidence of effectiveness as a standalone70,71 or adjunctive treatment 72 for tendinopathy. Synthesizing all these findings, it is clear that LLLT when used alongside conventional treatments can effectively reduce pain in tendinopathy and should be considered as part of a comprehensive treatment approach.
Mechanism of action
There are a number of postulated mechanisms underlying pain attenuation by LLLT. Essentially, the mechanisms of LLLT in the management of tendon injury are primarily mediated by photobiological stimulation. 73 By inference of previous studies which demonstrated LLLT-mediated effects such as increased conduction latency 74 and increased pressure pain threshold, 75 it is tempting to speculate that LLLT may exert its effect by activating the descending inhibitory system in tendinopathy. This is based on the premise of central sensitization76,77 and reduced conditioned pain modulation78,79 which have been consistently reported in tendinopathy. The application of LLLT has also been purported to effect pain modulation through the stimulation of peripheral nerve fibers and the release of endogenous opioids. 80 This in turn suppresses synaptic activity that leads to approximately 30% of neural blockade. 80 However, this mechanism merits further investigation. The other mechanisms include the suppression of inflammation as evident with a reduction in the anti-inflammatory cytokines,5,75 and the activation of cytochrome C oxidase to promote tendon healing 81 from human trials, whilst evidence from animal studies suggest the activation of vascular endothelial growth factor to promote angiogenesis, 82 and the increase in collagen type to promote proliferation of fibroblasts.83,84 The multifaceted pain attenuation mechanism triggered by the exposure to LLLT lends strong physiological plausibility and warrants further research to fully elucidate this clinical implication.
Parameters for LLLT
Our review of the literature revealed variability in the technical and temporal parameters of LLLT, and that it is uncertain how LLLT can be administered with a greater pain-relieving effect. Nonetheless, we have identified herein that the total number of sessions was a significant predictor of the effect size in pain score, after adjusting for age. However, this predictor was not significant when univariable regression analysis was performed. Furthermore, Kate et al. (2018) reported that the pain-relieving effect of LLLT were not attributed to the frequency of treatment and number of treatment sessions in a myriad of orthopaedic conditions such as rotator cuff tendinopathy, carpal tunnel syndrome, radiculopathy, joint arthralgia, dental pain and fibromyalgia. 13 Nevertheless, WALT has recommended daily LLLT over a span of two weeks or LLLT on alternate days over a period of 3 to 4 weeks for optimal benefit. 85 The wavelength was not identified as a significant predictor in our review. Nevertheless, about half of the included studies used wavelength of 810 to 890 nm (Table 2), and these concur with one of the absorption bands by the cytochrome c oxidase within the mitochrondria, that is, about 800 nm in the near infrared spectrum.14,86 Interestingly, a review finding from Zein and colleagues 14 suggested that the tendon, which has a lower number of mitochondria when compared to the muscle, may respond better to higher dosage (J/cm2) of LLLT. 14 It is also important to appreciate the biphasic dose response when applying LLLT to for optimal dosing within the therapeutic window.14,86 We believe that more transparent reporting on the technical parameters, and important prognostic factors such as the gender proportion and duration of condition in future studies would allow the elucidation of further insights on the optimal LLLT parameters for pain relief.
Limitations
One of the challenges encountered during this review included the lack of reporting on the duration of condition in almost a quarter of all the included trials (8 out of 34) in the meta-analysis,33,34,40,44,63–65,67 rendering difficulty with performing subgroup analyses according to chronicity of condition. However, based on the available information and data on duration of tendinopathy from the remaining included trials in the meta-analysis, it became apparent that the external validity of the findings from this review are limited mainly to chronic tendinopathy. Secondly, one of the funnel plots which displayed asymmetry suggests a variety of possible reasons. For example, it is plausible that trials with smaller sample size and negative results may have been underreported in the literature. Alternatively, smaller studies with positive results may have influenced the results of the meta-analysis. Nonetheless, the use of various databases checking reference lists and inclusion of non-English language studies has been undertaken to locate trials thoroughly, and it is conceivable that the ‘missing studies’ would not have made a substantial difference to this review. In addition, sensitivity analyses have been performed to obtain a more robust conclusion from the meta-analysis. Lastly, different pain outcome measures were used across the studies, but this has been circumvented by expressing the treatment effects in SMD since the pooled standard deviation would have adjusted the between-study differences in terms of the different pain measurement scales used. 87
Conclusion
In conclusion, this review highlights that LLLT is superior to minimal intervention for pain relief in chronic tendinopathy. However, it should be used as an adjunct, rather than in isolation. The total number of treatment sessions may influence the magnitude of pain relief provided by LLLT.
Supplemental Material
sj-docx-1-bmr-10.1177_10538127251339104 - Supplemental material for Shedding more light on the short-term effect of low-level laser therapy on pain in tendinopathy: A systematic review with meta-analysis
Supplemental material, sj-docx-1-bmr-10.1177_10538127251339104 for Shedding more light on the short-term effect of low-level laser therapy on pain in tendinopathy: A systematic review with meta-analysis by Benjamin Wei Da Yap and Edwin Choon Wyn Lim in Journal of Back and Musculoskeletal Rehabilitation
Supplemental Material
sj-docx-2-bmr-10.1177_10538127251339104 - Supplemental material for Shedding more light on the short-term effect of low-level laser therapy on pain in tendinopathy: A systematic review with meta-analysis
Supplemental material, sj-docx-2-bmr-10.1177_10538127251339104 for Shedding more light on the short-term effect of low-level laser therapy on pain in tendinopathy: A systematic review with meta-analysis by Benjamin Wei Da Yap and Edwin Choon Wyn Lim in Journal of Back and Musculoskeletal Rehabilitation
Supplemental Material
sj-docx-3-bmr-10.1177_10538127251339104 - Supplemental material for Shedding more light on the short-term effect of low-level laser therapy on pain in tendinopathy: A systematic review with meta-analysis
Supplemental material, sj-docx-3-bmr-10.1177_10538127251339104 for Shedding more light on the short-term effect of low-level laser therapy on pain in tendinopathy: A systematic review with meta-analysis by Benjamin Wei Da Yap and Edwin Choon Wyn Lim in Journal of Back and Musculoskeletal Rehabilitation
Supplemental Material
sj-docx-4-bmr-10.1177_10538127251339104 - Supplemental material for Shedding more light on the short-term effect of low-level laser therapy on pain in tendinopathy: A systematic review with meta-analysis
Supplemental material, sj-docx-4-bmr-10.1177_10538127251339104 for Shedding more light on the short-term effect of low-level laser therapy on pain in tendinopathy: A systematic review with meta-analysis by Benjamin Wei Da Yap and Edwin Choon Wyn Lim in Journal of Back and Musculoskeletal Rehabilitation
Footnotes
Author contributions
Both BWDY and ECWL contributed to the study conception and design, data extraction, analysis and interpretation of results, and manuscript preparation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has received funding from the Active Global Health Sciences Education Group Pte Ltd.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Guarantor
ECWL.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.