
Abstract
Background
The objective of this study was to evaluate and compare the stability, functionality, balance, and muscular strength of the upper and lower extremities between CrossFit athletes with and without musculoskeletal pain.
Methods
The study included 65 individuals between the ages of 20–45 who did CrossFit training. The Extended Nordic Musculoskeletal System Questionnaire (NMQ-E) was used for musculoskeletal system problems, the Upper and Lower Extremity Y Balance Test (YBT) was used for lower and upper extremity balance assessments, respectively, the Single Leg Hop Test (SLHT) was used for functional performance assessments, the Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) and Closed Kinetic Chain Lower Extremity Stability Tests (CKCLEST) were used for stability assessment, and an isokinetic dynamometer was used for muscle strength assessment of the athletes included in the study. The study was registered on the Clinical Trials website by the number NCT05682534.
Results
The most frequently reported injury sites in CrossFit athletes were found to be shoulders (49.02%), waist (39.22%), knee (37.25%), and wrist (13.73%), respectively. While it was determined that there were statistically significant differences between the CKCLEST of athletes experiencing low back pain compared to those who did not (p < 0.05, p = 0.026), no differences were found between those with and without pain in any other measurement results (p > 0.05).
Conclusions
While it was observed that CrossFit athletes frequently had musculoskeletal system pain in the shoulder, waist, knee and wrist regions, balance, stability, strength, and functional performance were not affected despite the athletes’ pain.
Introduction
CrossFit was developed by Greg Glassman in 1995 and is an extreme exercise model that includes high-intensity sessions with a wide range of functional movements aimed at improving the physical capacities of athletes.1,2 CrossFit aims both to improve overall fitness and best prepare athletes for unforeseen physical challenges. 1 Initially developed for military training, this exercise training quickly spread among the civilian population as its popularity increased. 3
In CrossFit, trainings are high-intensity exercises called “Workout of the Day.” Rest periods are very short. In the workout of the day, different types of exercises are performed together, such as Olympic weightlifting, powerlifting, sprinting, plyometrics, calisthenics, gymnastics, and rope climbing. 1 Past studies show that CrossFit training improves endurance and increases VO2 max, 1 increases aerobic and anaerobic capacity, 1 and results in improvements in body composition, strength, flexibility, power, and balance. 4 However, there are studies reporting that CrossFit training is a risk factor for musculoskeletal injuries4,5 urinary incontinence6,7 and rhabdomyolysis8,9 and that it causes exercise dependence 1 It is stated that, in CrossFit athletes, the incidence of musculoskeletal injuries varies between 0.74 and 3.3 per 1000-h training session5,10 and injuries are frequently seen in the shoulder, waist, knee, and elbow regions.11–13 The injuries experienced are 41–45.3% strain14,15; 26.2% overload injuries 14 ; 24.7% joint injuries 16 ; 17.2% contusions 14 ; 13.0% tendinopathies, and 5.6% fractures and dislocations. 16 In the literature, CrossFit duration of more than 6 months, training duration, previous injuries, and gender have been reported as risk factors that may cause musculoskeletal injuries.1,10,17 It has also been reported that CrossFit athletes continue training despite injuries due to exercise addiction, which has been associated with injuries. 1 As the popularity of CrossFit sports increases daily, the prevention and management of musculoskeletal injuries are becoming increasingly important. When the existing literature is reviewed, it is seen that musculoskeletal injuries in CrossFit athletes are focused especially on the shoulder region, and this region is mostly evaluated in terms of functional performance. 18 However, CrossFit workouts consist of high-intensity and repetitive movements that intensively involve the upper and lower extremities. Therefore, training focusing only on the shoulder area may not fully reflect the athletes’ overall stability, balance, and functional performance.
The aim of this study was to determine and compare both upper and lower extremity stability, balance, lower extremity functionality, and muscular strength in CrossFit athletes with and without musculoskeletal pain. Thus, it was aimed to address the biomechanical and functional effects of pain in CrossFit athletes from a broader perspective and to contribute to strategies for injury prevention in the future.
Materials and methods
Subjects
In the study, assuming that the effect size would be large for pain in the knee region, the sample size required for 80% (1-β = 0.80) power at d = 0.8 and α = 0.05 level was calculated as 42 people, 21 from each group, using G*Power 3.1.9.2 software. Considering dropouts that may occur during the study, the number of samples increased by 50% and was determined as 31 for each group.
Those aged between 20 and 45 who had done CrossFit sports for at least 1 year and those who did CrossFit sports at least 2 days a week were included in the study, while those who were interested in a different branch of sports other than CrossFit, those with a neurological problem diagnosed by a doctor, and those who had received physiotherapy in the last 6 months were excluded from the study. There were 67 individuals who met the inclusion criteria. Since 2 people had health problems and left the study, the study was completed with 65 people. Both written and verbal information was given to all participants, and their written informed consent was requested. This study was approved by the Eastern Mediterranean University Ethics Committee on 14.10.2022 with the number ETK00-2022-0231. The consort diagram is shown in Figure 1.

Consort flow diagram.
Procedures
The Athletes included in the study were evaluated on two different, non-consecutive days, at least 48 h apart. On the first day, the sociodemographic information and training characteristics related to the sport of CrossFit athletes were questioned and recorded. The Extended Nordic Musculoskeletal System Questionnaire (NMQ-E) was performed to investigate musculoskeletal system problems, the Upper and Lower Extremity Y Balance Test (YBT) was performed for lower and upper extremity balance assessments, respectively, the Single Leg Hop Test (SLHT) was performed for functional performance assessments, and the Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) and Closed Kinetic Chain Lower Extremity Stability Test (CKCLEST) were performed for stability assessment. On the second day, quadriceps and hamstring muscle strength measurements were performed with an isokinetic dynamometer (60°/sec angular velocity).
This study was conducted in the Athlete's Health Unit of the Health Sciences Faculty of Eastern Mediterranean University. Verbal encouragement was given to the participants during the physical performance tests to ensure they were giving their best. All measurements were performed by the same physiotherapist.
Sociodemographic information
The personal information such as age, gender, profession, and dominant side of the athletes were recorded. Additionally, their number of weekly training sessions, daily training duration, and the movements they found most difficult were questioned. The causes, times, severity, types, and regions of musculoskeletal injuries experienced in the last year, as well as their interruption of training and methods of managing injuries, were recorded.
Evaluation of musculoskeletal system pain
The Extended Nordic Musculoskeletal System Questionnaire (NMQ-E) was used to evaluate the musculoskeletal pain conditions of the athletes. The Turkish translation and cultural adaptation of NMQ-E was conducted by Alaca et al.
NMQ-E is a visual questionnaire that can be completed in 10–15 min and questions feelings of pain in 9 areas of the body. If the answer is yes, the age of onset of pain, history of hospitalization, job change, last 12 months, last 1 month, current pain status, pain-related work interruption, seeking health services, medication use, and status of receiving a medical report are examined. Additionally, the frequency of pain, its variability on rest days, and its severity are questioned according to the region. 19
Evaluation of lower extremity functional performance
Single leg hop test (SLHT)
The Single Leg Hop Test (TBST) was used to evaluate the lower extremity functional performance of the athletes. In the validity and reliability study conducted by Sawle et al. in 2017, the internal consistency coefficient (ICC) of the test was found to be 0.85. Before the test, the athletes were given verbal information about how the test should be performed and were asked to perform two trials. For the test, the athletes were asked to stand on one leg and jump as far as possible. The test was repeated if the support leg was not landed on after the test and balance was lost. As a result of the measurement, the toe-heel distance was recorded in centimeters (cm) with a fixed tape measure. The test was performed 3 times for both legs and the best score was recorded as the test result. 20 The test is shown in Figure 2.
Single leg hop test (SLHT) practice.
Evaluation of upper and lower extremity stability
Closed kinetic chain upper extremity stability test (CKCUEST)
The Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) was used to evaluate the upper extremity stability of the athletes. This test evaluates upper extremity strength, endurance, and balance. The reliability study of the test (ICC: 0.92) was performed by Goldbeck and Davies, and its validity study was carried out by Don-Rour Lee and colleagues, and the validity coefficient was determined as 0.79 for the right hand and 0.78 for the left hand. 21 Before the test, the athletes were given verbal information about the test and were asked to try it twice. For the starting position, the athletes were asked to place their hands on the floor, marked with two yellow tapes, 36 inches (91.4 cm) apart, and were asked to touch the hand s/he started with to the other hand as quickly as possible for 15 s and then repeat this with the other hand. A 45-s break was given between each repetition. During the test, if the athletes’ backs were not straight, their knees touched the ground, and the weight-bearing extremity was not perpendicular to the ground, the time was stopped and the test was repeated, and the mean of the 3 tests was recorded as the test result.
Closed kinetic chain lower extremity stability test (CKCLEST)
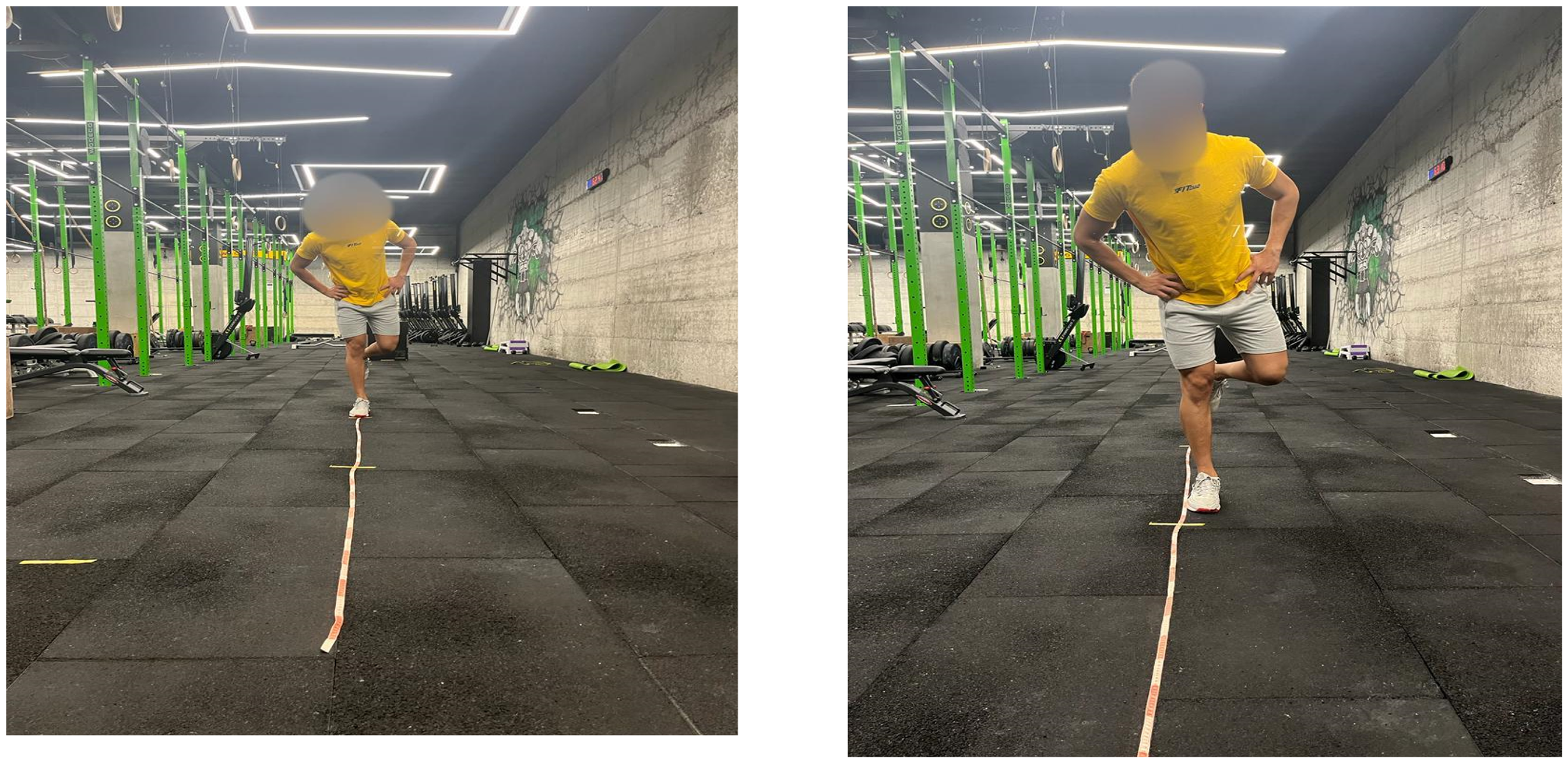
The Closed Kinetic Chain Lower Extremity Stability Test (CKCLEST), developed by Arikan and colleagues in 2021, was used to evaluate the lower extremity dynamic stability of the athletes. 22 Before the test, the athletes were verbally informed about the test and were allowed to try it 2 times. For the test, the athletes were asked to position themselves in a plank position on their forearms with their feet shoulder-width apart. The athletes were asked to touch one foot diagonally to the outside of their other foot while maintaining the starting position and then return to the starting position. They were then asked to perform the same movement with their other foot. The athletes were asked to repeat these movements with consecutive legs as fast as possible for 15 s. The test was repeated 3 times and the mean of the 3 tests was recorded as the test result. The test is shown in Figure 3.

Closed kinetic chain lower extremity stability test (CKCUEST) practice.
Evaluation of balance
Upper extremity Y balance test (UEYBT)
The Upper Extremity Y Balance Test (UEYBT) was used to evaluate the upper extremity balance of the athletes. The reliability studies of the test were supported by Gorman et al., and the validity test was performed by Westrick et al. 23 The test procedure was explained to the athletes before the measurements and they were given 3 trial opportunities, with a 5-s rest between each trial. The UEYBT kit was placed on the board with a 150 cm long tape measure and the position of the test was adjusted. The athletes were asked to reach in certain directions and 3 trials were performed in each direction. The reaching distances were recorded, and a composite score was calculated. The test was performed as shown in Figure 4.

Upper extremity Y balance test (UEYBT) practice.
Lower extremity Y balance test (LEYBT)
The Lower Extremity Y Balance Test (LEYBT) was used to evaluate the lower extremity balance of the athletes. In the study conducted by Plisky et al., the inter-rater reliability of the test was found to be (ICC: 0.85–0.91) and the inter-individual reliability was found to be (ICC: 0.99 −1.00). Before the test, the athletes were given detailed information about the test procedure and then the opportunity to try 2 times on the Y Balance Test Platform for adaptation. To do the test, the athletes were asked to stand with both hands on their waist and the big toe of one foot on the starting line in the center of the platform. The athletes were asked to reach in 3 directions (anterior [ANT], posterolateral [PL], and posteromedial [PM]) with the free side extremity and reach as far as they could with their fingertips while maintaining the lower extremity position placed in the center. During the measurement, if the participants transferred their body weight to the lying leg, separated the heel of the stance leg from the floor, or separated their hands from the hips, it was considered a fault, and the test was repeated. All reaching distances were recorded in centimeters. The test was repeated 3 times consecutively on both feet. 2-min breaks were given between the repetitions. For the composite score, lower extremity length measurement was also taken to be used in scoring (SIAS-Medial Malleolus). Mixed reaching distance was used in statistical analyses. The scores were normalized using the formula [(max anterior + max posteromedial + max posterolateral) / (3×Lower Extremity Length)] ×100. 24 The test was performed as shown in Figure 5.

Lower extremity Y balance test (LEYBT) practice.
Evaluation of muscle strength
Isokinetic muscle strength evaluation protocol
Muscle strength evaluation of athletes was performed using an isokinetic dynamometer (Cybex Humac Norm; Model: 502140, serial no: 2710, Computer Sports Medicine, Inc) at an angular velocity of 60 ˚/sec in the dominant and non-dominant lower extremities and peak torque values were recorded. The participants were asked to perform a 5-min light warm-up run before the test. Then, they were positioned on the isokinetic dynamometer seat with the body in an upright position and the hips and knees in 90° flexion, fixed with the help of a belt. The knee and ankle were fixed on the dynamometer with the help of a belt. First, the athletes were given preliminary information about the test to be performed and then the sample movement was performed, and the joint range of motion was determined by a dynamometer. After 3 trial repetitions, a 10-s (sec) break was given. After the break, the athletes were asked to perform 5 retests by applying maximum force and these values were recorded by the computer. 25 The test was performed as shown in Figure 6.

Isokinetic muscle strength evaluation practice.
Statistical analysis
The data obtained from CrossFit athletes in the study were analyzed using Statistical Package for Social Sciences (SPSS) 26.0 software. Sociodemographic characteristics of the athletes, some characteristics related to their CrossFit status, their pre-CrossFit sports status, CrossFit-related injuries, and NMQ-E findings were determined by frequency analyses. Descriptive statistics were given for anthropometric measurements, pain status, posture evaluations, balance evaluations, and strength evaluations of the athletes.
For the comparison of posture, balance, and strength evaluations of the athletes according to their pain status according to NMQ-E, the normal distribution of the data was examined and it was determined that the data did not show normal distribution. Mann-Whitney U test was used to compare the posture, balance, and strength evaluations of the athletes according to their pain status according to NMQ-E.
Results
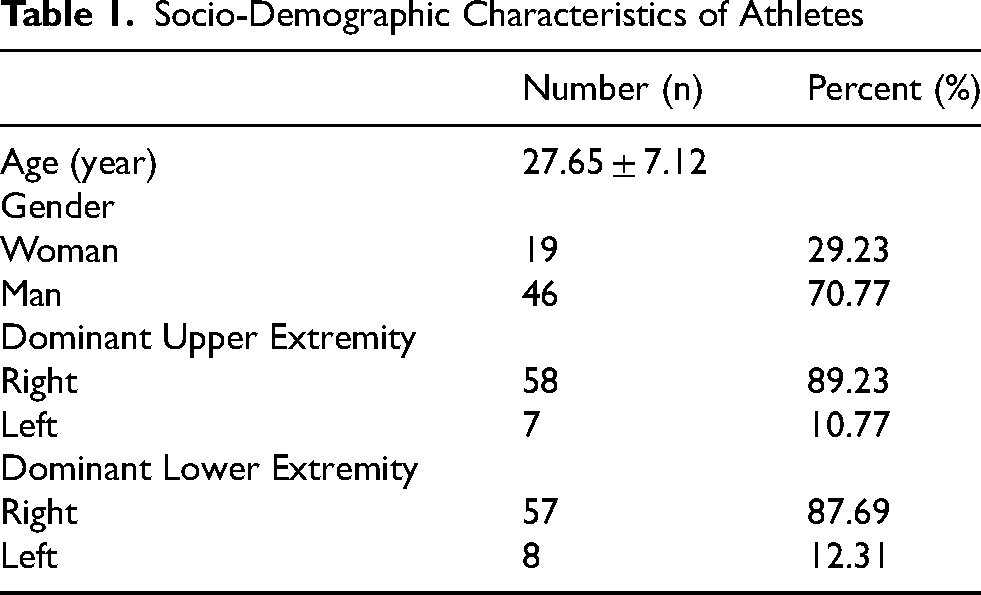
The socio-demographic information of the 65 athletes included in the study is given in Table 1. It was determined that the average age of the athletes participating in the study was 27.65 ± 7.12 years, of the participants, 29.23% were female 70.77% were male, and 72.31% had been doing sports before CrossFit. It was found that the athletes most frequently used the rest method to cope with CrossFit-related injuries and pain.
Socio-Demographic Characteristics of Athletes
The anthropometric measurement results of the athletes are given in Figure 7.

Anthropometric Measurements of Athletes. BMI: body mass index.
When Table 2 was examined, it was seen that 64.62% of the athletes have been doing CrossFit for 1–2 years and 35.38% for more than 2 years. It was found that 26.15% of the athletes had the most difficulty with snatches and 47.69% participated in CrossFit competitions.
Crossfit training information of athletes

Figures 8–11 show the CrossFit-related injury status of the athletes, and it was determined that 78.46% of the athletes had CrossFit-related injuries. It was found that 35.29% had strain/sprain, 23.53% had pain, 21.57% had spasm, 17.65% had meniscus degeneration, 15.69% had disc herniation, 13.73% had rotator cuff rupture, 11.76% had shoulder impingement type injuries, 56.86% had moderate severity, and the most frequently injured area was the shoulder with a rate of 49.02%.

Crossfit injuries.

Cause of crossFit injury.
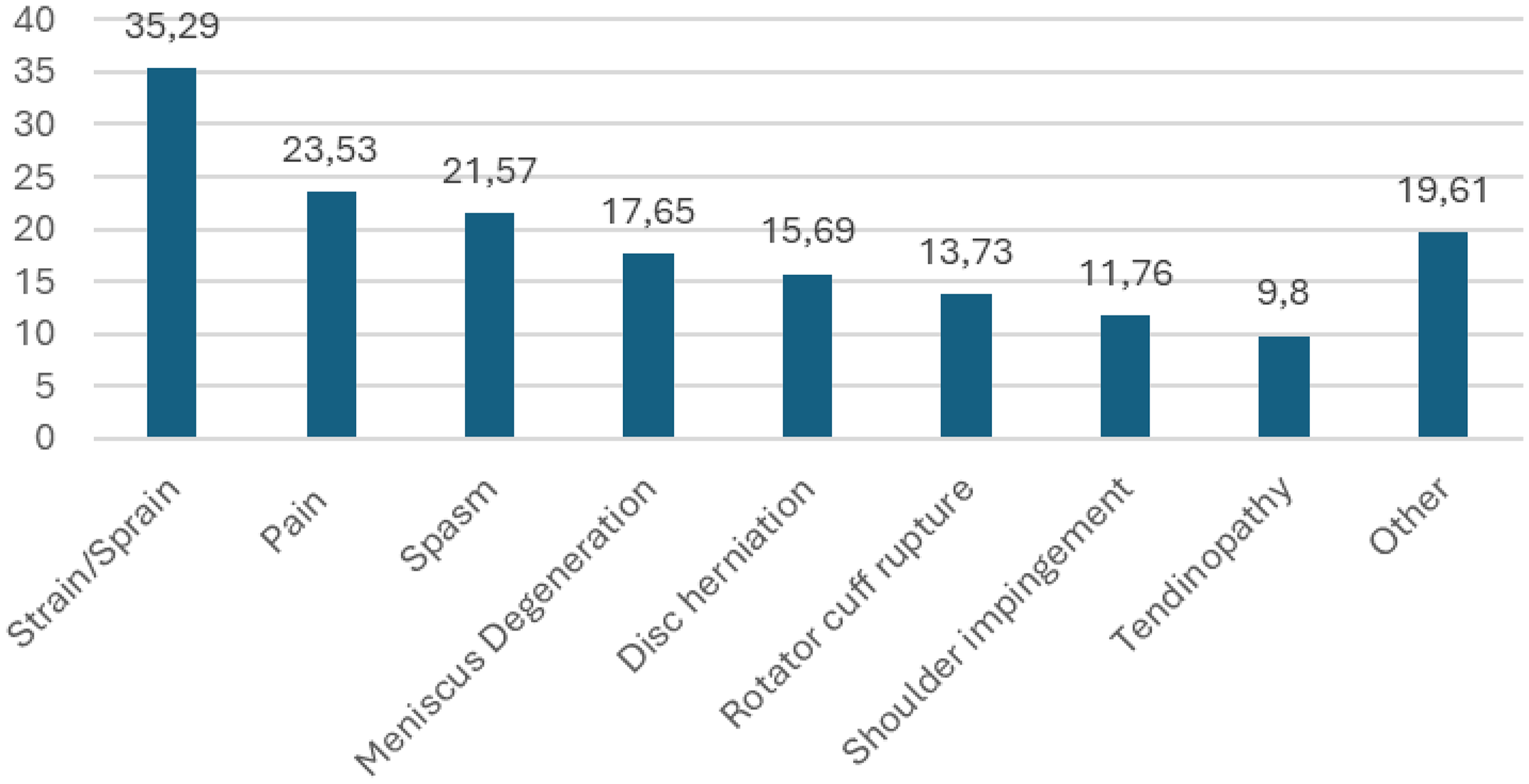
Crossfit injury type.
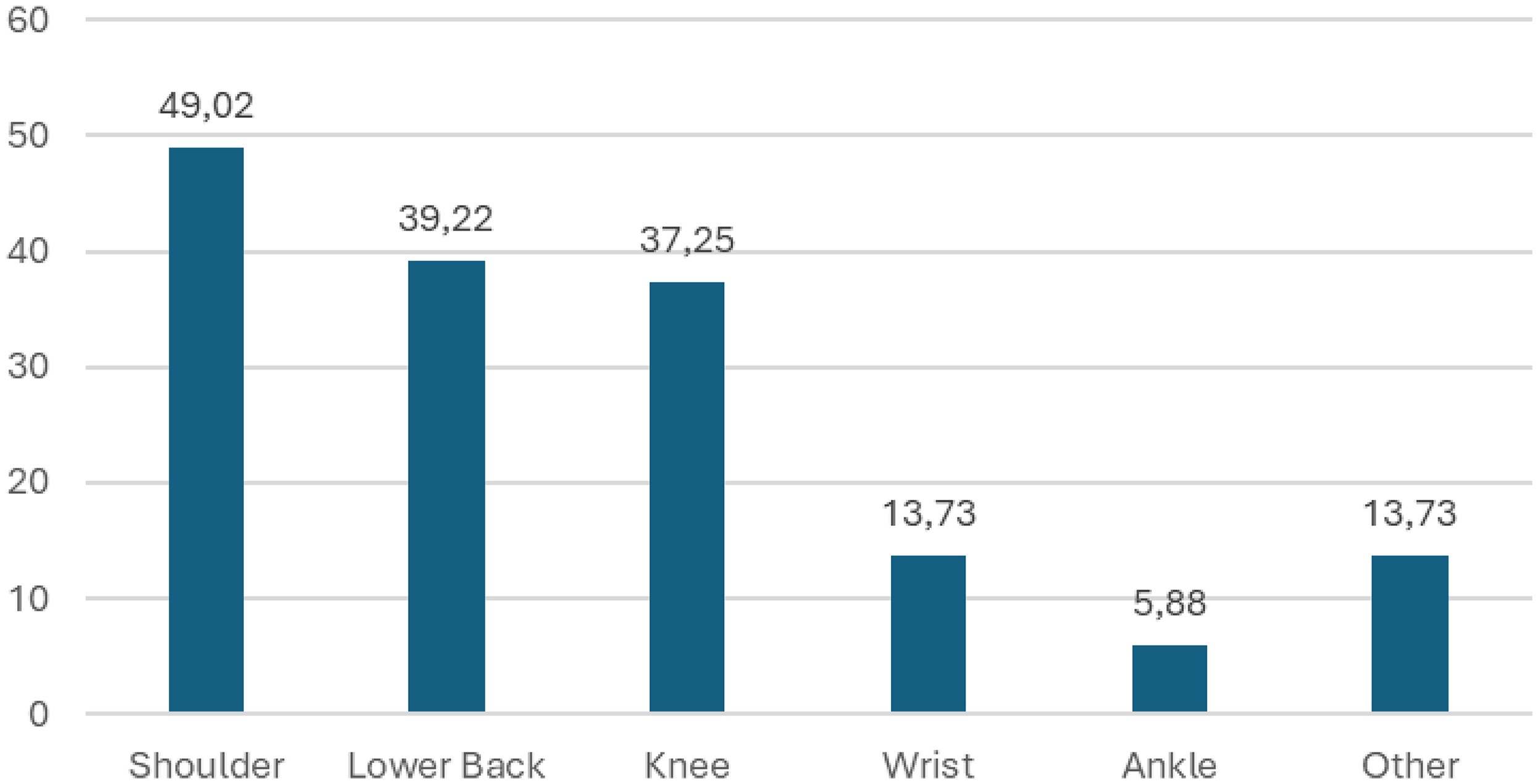
Injury regions caused by crossFit.
Figure 12 shows descriptive statistics for pain severity according to NMQ-E. It was found that the athletes’ neck pain mean severity was 4.43 ± 2.88, shoulder pain mean severity was 5.50 ± 1.75, back pain mean severity was 5.33 ± 1.51, elbow pain mean severity was 5.17 ± 0.98, hand-wrist pain mean severity was 4.78 ± 1.35, low back pain mean severity was 5.94 ± 1.61, hip pain mean severity was 5.50 ± 0.71, knee pain mean severity was 5.65 ± 1.66, and ankle pain mean severity was 6.27 ± 2.57.

Athletes’ pain severity according to the extended nordic musculoskeletal questionnaire.
Table 3 presents the findings obtained from the Mann-Whitney U test, which was used to compare the stability, balance, and functional performance evaluations of athletes according to their hand-wrist and shoulder pain status, and the stability, balance, and functional performance and strength evaluations according to their knee and low back pain status. No statistically significant differences were found between other stability, balance measurements, and functional performance measurements according to the hand-wrist pain status of the athletes (p > 0.05). The difference between CKCLEST measurements according to low back pain status was found to be statistically significant (p < 0.05). CKCLEST measurements of the athletes experiencing low back pain were found to be lower than those without pain. No statistically significant difference were found between other stability, balance, functional performance, and strength measurements according to the athletes’ back and knee pain status (p > 0.05).
Discussion
This study was conducted to determine and compare stability, functionality, balance, and muscular strength in CrossFit athletes with and without musculoskeletal system pain. The results of the analysis showed that the most frequently reported injury areas in CrossFit athletes were the shoulder, waist, knee, and wrist, respectively, and the pain intensity was highest in the shoulder, waist, knee, and wrist. While it was determined that the athletes with low back pain had low lower extremity stability, it was observed that none of the test results were affected in athletes with pain in other areas.
Participation in sports activities has positive effects on a healthy life, but it is also a known fact that it is a risk factor for injuries. 26 Different injuries occur in CrossFit, a high-intensity sport and the most common injuries are musculoskeletal system injuries.15,27 Studies show that CrossFit-related musculoskeletal system injury rates vary between 14.9% and 73.5%,6,11 and the most common injury types are: 17.2%–41% strain,27,28 30% general inflammation and pain, 27 30% general inflammation and pain, 29 17% contusion 29 and 5.6% fracture-dislocation 29 respectively. In this study, it was found that a high proportion of athletes (78.46%) had CrossFit-related musculoskeletal system injuries, and the most common types of musculoskeletal system injuries were strain, general pain, spasm, and disc herniation. Investigation of CrossFit injuries and risk factors has concluded that greater training duration,28,30,31 higher training frequency, 31 and sports experience (1 year and more) 32 are associated with a greater number of injuries. In addition, competitive CrossFit athletes are at higher risk of injury as they exert more effort while competing. 30 Also, athletes with more body weight and height may be subjected to more risk of injury due to the increased load they carry. 30 As far as movements are concerned, weightlifting, gymnastics, snatches, squats, Olympic weightlifting, and powerlifting movements like overhead presses are most involved in musculoskeletal injuries.13,27 The demand of the shoulder girdle for a greater range of motion and stability with overhead activities has been demonstrated to predispose to a higher incidence of shoulder injuries. 27 CrossFit's high repetition and speed emphasis can take relatively simple maneuvers and turn them into highly risky movements. The squats, specifically, require the thoracic and lumbar spine to remain in a neutral position. Since fatigue sets in with training, improper spinal alignment may result in greater intradiscal pressure, which can lead to injuries such as disc herniation. 33 For this study, we think that the fact that the athletes experienced a high rate of musculoskeletal system injuries may be due to their high training age, their frequency of training at least three or more times per week, and the fact that more than half of them were competitor athletes. The frequent use of exercises such as the overhead press and Olympic lifts in athletes’ training, which have been shown in previous studies to increase injury incidence, may have also contributed to an increase in muscle strain injuries. In addition, the high average height of the athletes may have created a biomechanical disadvantage during lifting movements, increasing the pressure on the spine and increasing the risk of musculoskeletal injuries.
Musculoskeletal system injuries are a general term including any trauma that damages muscles, bones, tendons, joints, ligaments, and other soft tissues. 30 Such injuries represent one of the most frequent health problems in athletes and negatively affect athletes causing decreased performance or withdrawal from competitions. as well as economic costs. They also negatively affect athletes in terms of economic costs. 30 It is reported that the most frequently injured body parts in CrossFit athletes are the “waist and shoulder regions”.27,31,32 Low back injuries are particularly common during weight-lifting movements, and shoulder injuries are common during gymnastic movements. 32 In addition to the waist and shoulder region, the rate of injuries to the knee and wrist region is also significantly higher. 34 In a study evaluating the distribution of injuries according to gender and age, it was reported that the most common spinal injuries in CrossFit athletes aged 19 and under were lumbar pain, spondylolisthesis, and sacroiliac joint injury. It was stated that these injuries developed as a result of lifting high weights and using inadequate technique during the squat and deadlift movements commonly used in CrossFit. The authors stated that insufficient core strength may also be a factor in injuries in these regions. 35 In a study used the Nordic Musculoskeletal System Questionnaire, it was determined that the most affected areas were the knees, wrists, hands, and lumbar spine. 36 Weight-bearing via the upper extremities, as in closed kinetic chain activities, increases the dynamic stability of the joint through joint approximation and co-contraction of the muscles around the joint. This process also allows for increased static stability through the stimulation of joint mechanoreceptors. It is also known that the anatomical structure of the glenohumeral joint contributes significantly to increasing overall stability during weight-bearing through the upper extremities. 21 In this study, both UEYBT and CKCUEST were used to evaluate the functionality, stability, and balance of the athletes. According to the study conducted by Silva et al., CKCUEST and UEYBT results were found to be similar in CrossFit athletes with and without shoulder pain. The authors stated that although the athletes had lower functional capacity and reported pain, they did not have difficulty performing various functional tests. The authors highlighted that the CKCUEST requires both shoulder and trunk stability due to the test's position, along with the need for power and speed. They also pointed out that because the test is bilateral, it is not possible to assess the extremities independently. 18 In another study comparing the physical performances of CrossFit athletes with and without subacromial pain, it was reported that there were no significant differences in CKCUEST, UEYBT, and other physical performance tests. 37 In another study, it was found that CrossFit athletes with poor shoulder medial rotation ROM (Range of Motion) values had good CKCUEST results. The researchers reported that although the shoulder was one of the most affected areas, it did not prevent receiving good results from the test. 34 In this study, the CKCUEST and UEYBT results of the athletes with and without shoulder pain or other upper extremity pain were similar. We believe that trunk stability played a role in influencing our results, as the athletes were positioned in a plank stance during the CKCUEST. Additionally, since the test could not be performed unilaterally, it is plausible that this played a role in similar results between athletes with and without shoulder pain.
In CrossFit, good core strength and a strong lower extremity help provide trunk stability when lifting weights and reduce the risk of injury. 35 There is no study in the literature measuring lower extremity stability in CrossFit athletes. According to our CKCLEST results, which we used to evaluate lower extremity strength and trunk stabilization, the stability test results of athletes with only low back pain were found to be statistically significantly lower than those without pain. As is known, core muscles are essential for postural control, stability, and mobility of the trunk. 3 Core stabilization achieved through core muscles ensures that the optimum possible energy is transferred from the trunk to the upper and lower extremities controlling the position and movements of the trunk during a sporting movement. 38 In the CrossFit exercise model, performance depends on the resistance of the muscles in the core region during athletic movements and the ability to maintain this resistance for a long time. 3 In this study, CKCLEST results were lower in CrossFit athletes with low back pain compared to those without low back pain. The inability to maintain trunk stability as a result of inhibition of core muscles due to low back pain may have negatively affected the results of CKCLEST performed in the plank position.
CrossFit is an exercise modality combining many physical fitness skills, including agility, flexibility, strength, cardiorespiratory endurance, coordination, and balance. 39 One of these skills, balance, is a critical component for continuity of movement in workouts and daily life, so achieving and maintaining good balance is imperative in CrossFit. 40 Dynamic balance, which plays an important role in determining athletic performance, is also an effective motor skill in preventing injuries. Deficiencies in lower extremity dynamic neuromuscular control may increase the risk of injury In this study, the widely used LEYBT was used to determine the lower extremity dynamic balance and injury risk of athletes. 40 In a study evaluating balance with LEYBT in male and female CrossFit athletes, it was reported that there was no significant difference according to gender, only men had weaker balance on their right sides than women. The researchers reported that the fact that the male athletes had poor balance on the right side indicated a higher likelihood of injury on that side. 40 A study examining the relationship of trunk strength and endurance to lower extremity performance in CrossFit participants found a correlation between the two. This correlation was explained by the need for adequate joint stability to manage distal movement, as outlined in the closed kinetic chain theory. 39 There is a limited amount of research on dynamic lower extremity balance in CrossFit athletes. However, a study among young athletes recorded similar Y balance test scores between individuals with and without low back pain. The authors suggest that visual, vestibular, and somatosensory systems involved in postural control may be affected by pain and sensory tissue damage. Despite this, they suggest that they will adapt and evolve new methods of postural control, such as alternative mechanisms of balancing, to deal with the challenges encountered due to pain. They also reported that participation in sports would lead to superior balance. 41 The inclusion of multifunctional exercises in CrossFit facilitates overall muscle strengthening of all the muscles in the body, especially the core muscles. Strong core muscles are more stable and may beneficially improve balance. Additionally, the highly trained subjects in the study may have developed new postural control strategies, which may have beneficially improved their balance.
CrossFit is a high-intensity, high-volume strength and conditioning exercise program that includes many motor skills. 39 Evaluating the skills required by sports branches is important to prevent injuries. SLHT is widely recommended for evaluating lower extremity horizontal explosive power and functional performance. 42 However, there are limited studies measuring horizontal explosive power in CrossFit athletes. In their study, Silva et al. evaluated the lower extremity explosive power in CrossFit athletes and sedentary individuals with lower extremity SLHT and stated that the explosive power of CrossFit athletes was better and that this was thanks to the muscular strength of the athletes. 39 In this study, no significant difference was found in the SLHT results between athletes with and without pain. In this sport branch, where both lower extremities are worked repeatedly in many exercises, it was expected that leg muscle strength would increase, considering the athletic experience and weekly training frequency of the athletes included in the study. Our study results showed that knee muscle strength production was similar in athletes with and without pain. We believe that the similarity of the athletes’ muscle strength indirectly affected their explosive power, resulting in similar results.
The strength produced by the muscles enables body movements and helps maintain joint stability and posture. Therefore, the strength capacity of skeletal muscles is essential for the regular functionality of the human body. Isokinetic dynamometers are the gold standard measurement methods used in the assessment of muscle strength. 43 In CrossFit, frequent repetition of exercises and the use of high weights increase muscle strength and endurance. 44 According to the results of the study conducted by Tibana et al., one of the limited number of studies evaluating knee region muscle strength in individuals doing CrossFit sports, in which they evaluated the relationship between performance and muscle strength using back and front squat tests at the CrossFit® Open 2020, it was reported that localized muscle strength had a strong relationship with performance. 44 There are also studies examining the effects of CrossFit training on athletes from different sports branches. 45 In a study conducted on volleyball players, it was determined that CrossFit training applied 3 days a week for 6 weeks statistically significantly improved leg strength and lower extremity explosive strength of the volleyball players. In another study, it was reported that 8 weeks of CrossFit training performed 3 times a week improved the lower extremity muscle strength, endurance, and speed of sedentary individuals. 46 This study, which is the first to evaluate knee extensor-flexor concentric muscle strength in individuals doing CrossFit sports with an isokinetic dynamometer, found that the muscle strengths of athletes with and without low back pain were similar. Moreover, it was observed that both quadriceps and hamstring muscle strength rates were higher in athletes without low back pain compared to athletes with low back pain. As is known, the use of waist belts by athletes during training contributes to the reduction of stress on the waist by optimizing the transfer of movements from the distal segment to the proximal segment. Reducing the load on the lumbar region can reduce the risk of injury and pain development in the lumbar region. 47 Additionally, the fact that athletes frequently perform movements with pressurized breathing causes increased intra-abdominal pressure. 4 Increased intra-abdominal pressure contributes to force production by stabilizing the muscles. 48 In this study, we think that using a waist belt and increasing intra-abdominal pressure during exercise helped all athletes maintain the stability of their lumbar spine and supported the strength production of the knee region muscles. It was observed that knee extensor-flexor concentric muscle strengths were similar in athletes with and without knee pain. According to the literature, individuals doing CrossFit appear to have higher knee muscle strength compared to athletes interested in sports such as football and handball, where lower extremity muscle strength is important. 49 Based on this information, we believe that mild pain does not affect knee peak torque muscle strength in CrossFit athletes.
Conclusions
The study results revealed that CrossFit athletes often experienced musculoskeletal pain in the waist, knee, and upper extremity regions. It was also observed that pain did not hinder the physical performance of athletes. Although the results may be anticipated given the generally high pain threshold observed in this athletic population, the current study provides an objective evaluation of functional performance through the use of standardized physical assessments. This approach enables a more detailed understanding of how musculoskeletal pain and physical capacity interact in well-trained individuals. As such, the study contributes meaningful clinical knowledge by linking subjective reports of pain with quantifiable performance outcomes an aspect that is frequently underrepresented in research on well-trained athletic populations.
Limitations
This study has some limitations. Competitive athletes may have a higher tolerance to pain due to their training history and physical capacity. The inclusion of competitive athletes in the study prevented the generalization of the study results to less-trained CrossFit athletes.
In future studies, the inclusion of athletes with different levels of training and the consideration of coaches’ level of education may increase the applicability of the results to a wider CrossFit community.
Supplemental Material
sj-docx-1-bmr-10.1177_10538127251341831 - Supplemental material for Stability, functionality, balance, and muscle strength in CrossFit athletes with and without pain
Supplemental material, sj-docx-1-bmr-10.1177_10538127251341831 for Stability, functionality, balance, and muscle strength in CrossFit athletes with and without pain by Merve Paksoy and Berkiye Kirmizigil in Journal of Back and Musculoskeletal Rehabilitation
Supplemental Material
sj-doc-2-bmr-10.1177_10538127251341831 - Supplemental material for Stability, functionality, balance, and muscle strength in CrossFit athletes with and without pain
Supplemental material, sj-doc-2-bmr-10.1177_10538127251341831 for Stability, functionality, balance, and muscle strength in CrossFit athletes with and without pain by Merve Paksoy and Berkiye Kirmizigil in Journal of Back and Musculoskeletal Rehabilitation
Footnotes
Acknowledgments
The authors have no acknowledgments.
Ethical considerations
This study was approved by the Eastern Mediterranean University Ethics Committee on 14.10.2022 with the number ETK00-2022-0231. All participants provided written informed consent prior to enrolment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Authors contributions
Author Merve Paksoy and author Berkiye Kirmizigil have given substantial contributions to the conception or the design of the manuscript, author Merve Paksoy to acquisition, analysis, and interpretation of the data. All authors have participated in drafting the manuscript, and author Berkiye Kirmizigil revised it critically. All authors read and approved the final version of the manuscript. All authors contributed equally to the manuscript and read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.