
Abstract
Background
Cervical stenosis is an important problem in patients with cervical pain, which may cause proprioception problems.
Objective
This study aims to evaluate the effect of the degree of cervical stenosis on cervical proprioception and cervical range of motion (ROM).
Method
A total of 111 patients presenting with cervical pain and undergoing cervical magnetic resonance imaging were included in the study. The ROM of the patients was measured with the Pa Cervical Range of Motion (CROM) device. Proprioception was evaluated with measurement of joint position error (JPE). JPE was assessed with neutral head position and target head position tests. The severity of stenosis was detected according to the Kang grading system. The Kruskal-Wallis test is used to compare joint position error in patients with different cervical stenosis stages.
Results
Twenty nine(%26) patients had no stenosis, 31 (28%) had mild stenosis, 31 (28%) had moderate stenosis, and 20 (18%) had severe stenosis. According to the neutral head positioning test, there was a significant difference in right lateral flexion between patients with different degrees of stenosis (grade 0: 1.67[0.67–4.67] vs. grade 2: 4.67[2.3–10.0], p = 0.009) and in flexion (grade 0: 8.0[2.67–10.0] vs. grade 3: 12.66[8.33–17.67], p = 0.011). There was also a significant difference in head-to-target JPEs in all motion planes(p < 0.05).
Conclusion
Degree of cervical stenosis significantly affects cervical proprioception and cervical ROM. The study's findings may guide clinicians in developing effective rehabilitation programs for proprioception in cervical stenosis and encourage further research on intervention effects at different stages of the disease.
Introduction
Neck pain is a common health issue that negatively impacts the quality of life across different age groups, with most individuals experiencing this condition at some point in their lives. 1 Epidemiological studies in the literature report varying prevalence rates of neck pain, with some studies indicating rates exceeding 80%. 2 One of the most important causes of neck pain is cervical disc disorders. Cervical spinal stenosis (CSS) can develop as a result of cervical disc disorders and spinal degeneration. CSS is characterized by the narrowing of the cervical spinal canal beyond normal limits, and this condition can lead to various symptoms such as pain, numbness, impaired fine motor skills in the hands, and gait disturbances, depending on the severity of the condition. 3
Direct radiography, computed tomography, and magnetic resonance imaging (MRI) can be employed in the assessment of CSS. MRI is presently the most commonly used imaging modality for the precise assessment of spinal canal stenosis. MRI not only measures the dimensions of the spinal canal but also provides detailed imagery of the spinal cord, intervertebral discs, osteophytes, and ligaments, all of which may contribute to spinal canal stenosis. 4 Cervical stenosis may result in findings such as myelopathy and radiculopathy. Studies have reported a decrease in sensitivity to light touch, pain, and proprioception during sensory examinations. 5 Patients with degenerative cervical myelopathy may exhibit functional impairments resulting from the loss of proprioception and tactile sensation, due to neurological deficits caused by spinal cord compression. Proprioception is the capacity of an individual to incorporate sensory signals from mechanoreceptors in order to ascertain the positions and movements of body segments in space. 6 Proprioception is crucial for joint stability and injury prevention. 7 Consequently, impaired proprioception may contribute to an increased risk of injuries and the development of pain.
The primary source of proprioceptive information is widely recognized to be muscle spindles, which are situated parallel to the extrafusal muscle fibers in all skeletal muscles.8,9 Muscle spindles are densely distributed in the neck region, as established by morphological and immunohistochemical studies. 10 The findings suggest that these muscles and muscle spindles may play a role in the accurate regulation of head and neck proprioception. This feedback aids in the maintenance of appropriate posture and and balance. Impairment in cervical proprioception can disrupt the coordination of neck muscles, resulting in disturbances in head posture. 11
A tight association is considered to exist between neck pain and proprioceptive dysfunction. 12 Inaccurate proprioceptive input can lead to increased and sustained reflex activation of neck muscles, potentially contributing to the development of neck pain over time. 13 Furthermore, neck discomfort may interfere with afferent signals from cervical proprioceptors, leading to distorted proprioceptive information and potentially intensifying the pain, thereby perpetuating a vicious cycle. 13 Despite the well-established critical role of proprioception in musculoskeletal pain, there is a paucity of studies specifically examining the relationship between proprioception and cervical pain.
Proprioception is also impacted in cervical disc disorders and thus in cervical stenosis. Although the clinical significance of proprioception in patients with neck pain is well-documented, there is a paucity of studies that evaluate the relationship between cervical stenosis and proprioception. In a study on patients with disc disorders requiring surgery, Freppel et al. noted that proprioceptive impairments may occur in individuals with advanced disc degeneration and stenosis, and that these impairments can be partially reversible through surgical intervention. 14 Furthermore, cervical stenosis may result in the development of cervical spondylotic myelopathy. The involvement of ascending and descending pathways in the spinal cord may result in the development of both cervical and extremity proprioception disorders in cervical spondylotic myelopathy. 15
Given the cervical stenosis has the potential to affect proprioceptive function, a detailed exploration of its severity and direct impact on proprioception is essential. Nevertheless, to our knowledge, no existing studies in the literature have explicitly investigated the correlation between the severity of cervical stenosis and its impact on proprioceptive function. To address this gap in the literature, the present study aims to evaluate the relationship between CSS severity—assessed using MRI—and proprioceptive function, measured through joint position error (JPE). By comparing quantitative proprioceptive measures across different degrees of imaging-based stenosis grading, this study aims to determine whether the severity of cervical stenosis is associated with impaired proprioception. This design directly addresses the current lack of evidence and provides a better understanding of the functional implications of cervical stenosis. We hypothesize that increased stenosis severity may correspond to reduced joint range of motion (ROM) and diminished proprioception. Clarifying this relationship may improve clinical assessment strategies and support the development of targeted rehabilitation approaches to mitigate functional deficits in patients with cervical spine pathology.
Methods
Study design
This cross-sectional study was approved by the Ethics Committee of The Buca Seyfi Demirsoy Training and Research Hospital Ethics Committee. The data for the study were collected at Buca Seyfi Demirsoy Training and Research Hospital between February 2024 and November 2024.
Evaluations and measurements other than the degree of stenosis were made by a different researcher to avoid bias. The classification of stenosis was performed by a physician. Proprioception measurements were conducted by a single physiotherapist, who was blinded to the stenosis classification, to prevent inter-rater and intra-rater bias.
Participants
The study included individuals who had previously applied to the Physical Medicine and Rehabilitation clinic of Izmir Democracy University Buca Seyfi Demirsoy Training and Research Hospital due to cervical pain and underwent cervical MRI.
Inclusion criteria; individuals aged 18 years and older, who had a previous cervical MRI and whose stenosis classification could be clearly determined on MRI. Exclusion criteria; patients who declined participation, had a history of cervical surgery, had vertigo, had neurological disorders that could potentially affect study outcomes, or had psychiatric and cognitive conditions
Patients who met the inclusion criteria were informed about the study, and voluntary consent was obtained from those who agreed to participate.
Outcome measures
Firstly, the degree of cervical stenosis of the patients was determined based on the previously requested magnetic resonance MRI images of the patients. The Kang grading system was used to assess the degree of spinal stenosis based on MRI evaluation. The Kang grading system has four degrees, ranging from 0 to 3, based on the extent of spinal cord compression. 16
Accordingly;
0: (no stenosis) no narrowing in the spinal canal 1: (mild stenosis) more than 50% of the subarachnoid space disappears without signs of cord deformity 2: (moderate stenosis) presence of deformity and stenosis in the spinal cord without spinal cord signal change 3: (severe stenosis) increase in T2 signal intensity of the spinal cord at the compression level.
The Kang grading system demonstrated almost perfect inter-observer agreement among radiologists (κ = 0.890) and substantial agreement among clinicians (κ = 0.691). 17
Demographic data of the patients such as gender, age, body mass index (BMI), education status, occupation, marital status, smoking status, exercise habits, and medical history were recorded. Subsequently, the patients’ pain, ROM, and cervical proprioceptive sensations were evaluated.
In our study, for both aforementioned tests, patients were instructed to maintain an upright seated position in a chair. The CROM device was affixed to the patient's head using a Velcro strap. For the assessment of JPE, an eye patch was placed over the patient's eye, and they were asked to keep their head in their usual position, which they perceive as their normal position. Deviations from the zero positions of the dials measuring in three planes on the CROM were recorded. For the head-to-target assessment, the target position was defined as half of the maximum measured active ROM value. With the patient's eyes covered by an eye patch, their head was first slowly positioned to the predetermined location, and they were asked to perceive this position while maintaining it. Then, the head was moved in the opposite direction, and the patient was asked to actively bring it back to the target position on their own. Each measurement was repeated 3 times and the average amount of deviation from the target position was recorded. Measurements were conducted separately for flexion, extension, right rotation, left rotation, right and left lateral flexion.
Sample size estimation
The sample size for the study was calculated using the GPower (G*Power 3.1.9.7 system, Franz Faul, Universität Kiel, Germany) program. Based on a sample size calculation with 90% statistical power, 95% confidence interval and 0.3 effect size, it was determined that at least 97 participants were required for the study. To account for potential dropouts, a total of 111 participants were planned to be included.
Statistical analysis
Statistical analyses were performed using SPSS 24.0 program. The normality of all variables was assessed using visual methods (histograms and probability plots) and analytical tests (Kolmogorov-Smirnov and Shapiro-Wilk tests Descriptive analyses were presented as frequencies and percentages (%) for categorical variables, median and interquartile range (IQR) for non-normally distributed variables, and mean and standard deviation (x ± ss) for normally distributed variables. To compare group differences according to the degree of cervical stenosis, one-way ANOVA was employed for normally distributed variables, the Kruskal-Wallis test was used for non-normally distributed variables, and the Chi-square test was applied for categorical variables. When the Kruskal-Wallis test indicated a statistically significant overall difference (p < 0.05), pairwise comparisons were conducted using the Independent-Samples Median Test to identify specific group differences while minimizing Type I error. This approach was selected to ensure appropriate follow-up testing that accounts for the ordinal structure of the stenosis grading and the non-parametric nature of the data. A p-value of less than 0.05 was considered statistically significant. Finally, Cohen's d was calculated to determine the effect size of significant differences, providing additional information on the magnitude of observed effects.
Results
The severity of CSS was assessed in a total of 111 patients presenting with cervical pain, and the patients were categorized into four groups based on the degree of stenosis for comparative analysis. The distribution of the cases was as follows: 29 (26%) had no stenosis, 31 (28%) had mild stenosis, 31 (28%) had moderate stenosis and 20 (18%) had severe stenosis. Gender, BMI, educational status, occupation, marital status, smoking habits, exercise routines, comorbid chronic diseases, and pain levels were assessed, with all descriptive data presented comparatively across the groups in Table 1.
Demographic characteristics of the patients who participated in the study.
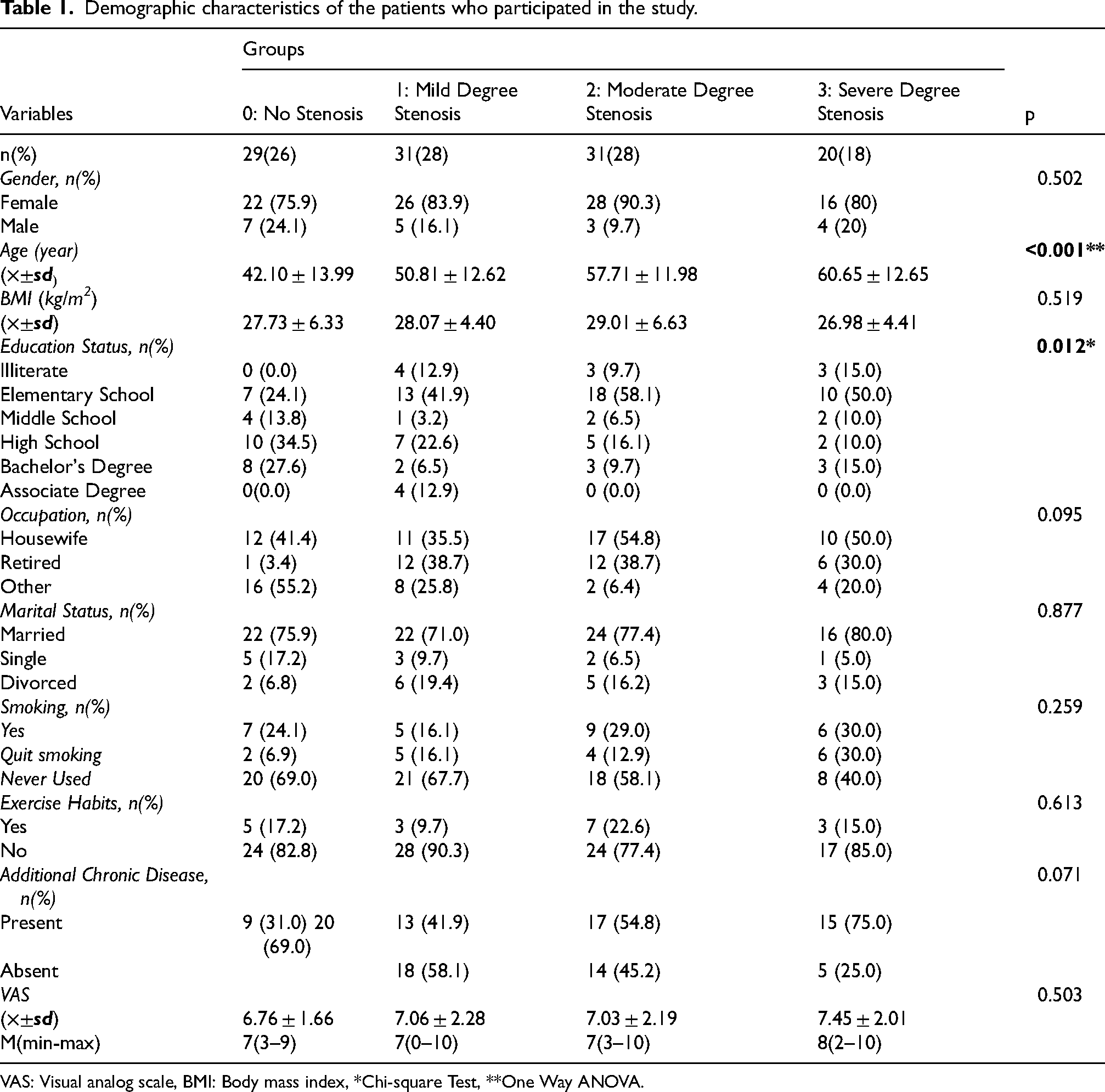
VAS: Visual analog scale, BMI: Body mass index, *Chi-square Test, **One Way ANOVA.
In our study, the ROM of patients with varying degrees of CSS was compared. Statistically significant differences were observed in flexion and right and left lateral flexion ROM among the groups, 0.007, 0.037, 0.038 respectively. (Table 2).
Cervical range of motion among patients in different degrees of stenosis.
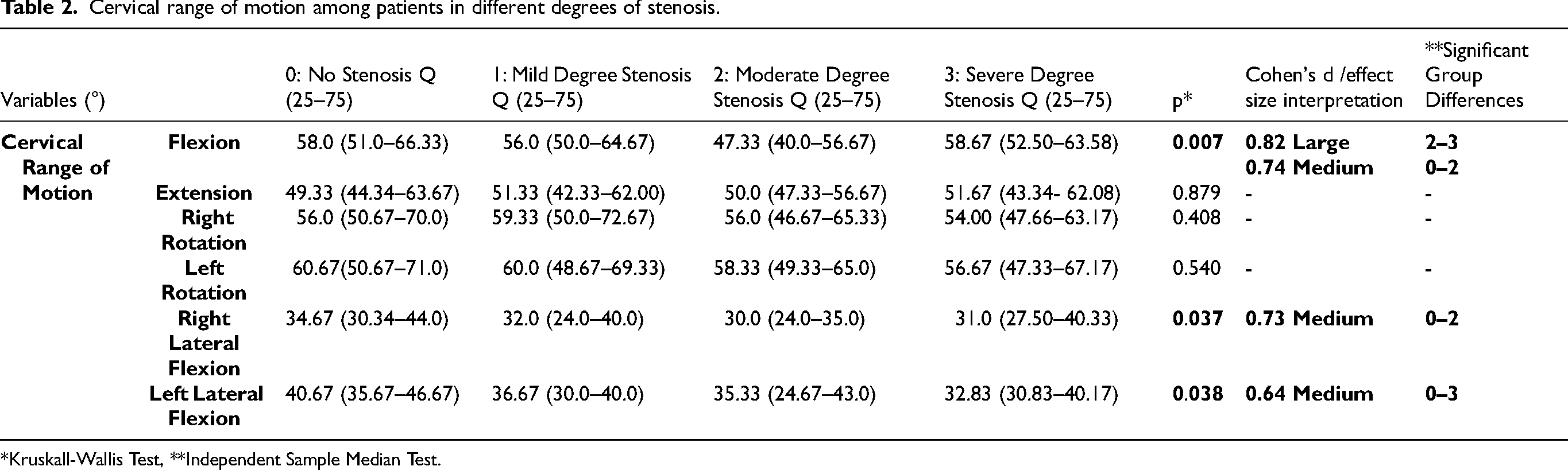
*Kruskall-Wallis Test, **Independent Sample Median Test.
When analyzing joint position sense, patients without stenosis demonstrated better proprioceptive ability during flexion(0.011) and right lateral flexion(0.009) while returning the head to the neutral position. Additionally, the target head position data revealed statistically significant differences across all cervical joint ROM between the groups(p < 0.05). In pairwise analysis patients with a greater degree had a higher JPE. The groups with significant differences are indicated in (Table 3). In the target head positioning (THP) test, a significant difference in total proprioceptive repositioning errors—calculated as the sum of JPEs across all motions—was detected among patients with varying degrees of cervical stenosis (p = 0.001) (Table 3).
Joint position error (JPE) according to the severity of cervical spinal stenosis.
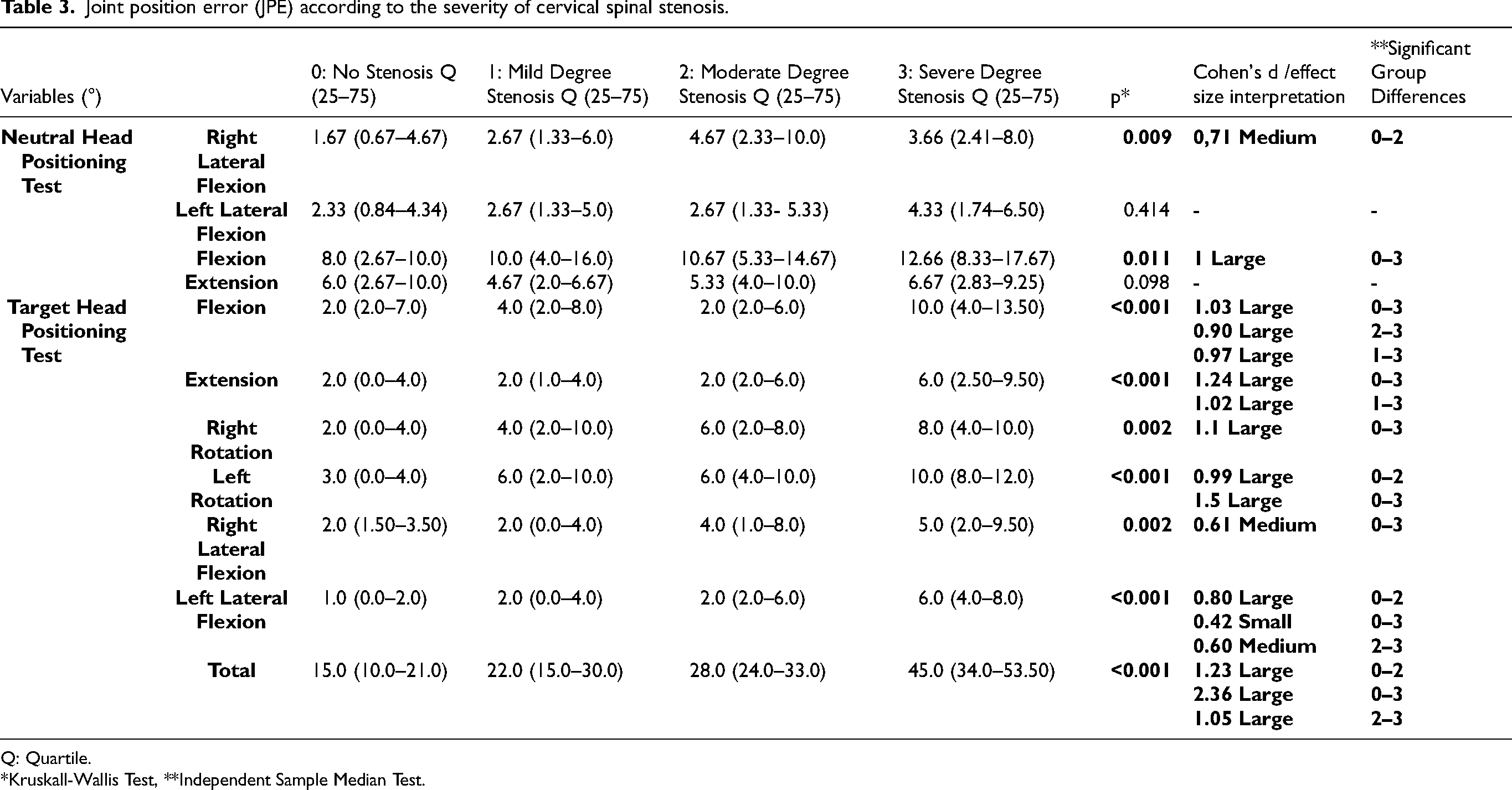
Q: Quartile.
*Kruskall-Wallis Test, **Independent Sample Median Test.
Discussion
In our study, we assessed the degree of cervical stenosis, joint ROM, and joint position sense in the cervical region. The findings revealed that patients with more severe stenosis exhibited greater restrictions in flexion and lateral flexion movements, demonstrating medium to large effect sizes. Furthermore, when proprioception was assessed using both the NHP and THP methods, patients with severe stenosis demonstrated greater impairment compared to those without stenosis. The majority of these measurements indicated medium to large effect size, underscoring the clinical significance of stenosis severity on proprioceptive function.
Presently, neck problems are among the most common musculoskeletal disorders. The increased use of certain technological devices and prolonged desk-based activities disrupts posture and causes an increase in neck problems. Research demonstrates that individuals with neck disorders exhibit changes in proprioceptive sense, which are attributable to functional alterations in muscle spindles and joint receptors. 29 These changes in muscle spindles affect the deep cervical flexor muscles, leading to postural disorders and increased pain. 30 Chronic neck discomfort is a health issue that profoundly impacts individuals’ quality of life, and the implications of this condition on proprioception are currently under investigation. Raizah et al. compared patients with chronic neck pain to asymptomatic persons and discovered that those with chronic cervical pain had more JPEs, and their functional balance tests were worse. 31 In another study, researchers compared patients over the age of 65 suffering from chronic neck pain with asymptomatic individuals. The findings revealed that neck extensor endurance was significantly reduced in individuals with chronic neck pain, and their cervical proprioception was notably impaired. 32 Current data indicate that chronic neck pain negatively affects proprioceptive sensitivity, and this may cause deterioration in balance and coordination skills in elderly individuals. It should be noted that impairment of proprioception can lead to difficulty in daily living tasks and a lower overall quality of life.33–35
One of the common reasons of neck pain is cervical disc degeneration and stenosis. Proprioceptive information is transmitted by specialized nerve endings known as proprioceptors, which are located in the joints, muscles, tendons, and skin. 36 Cervical proprioceptive afferents are mainly categorized into three types: joint receptors, muscle spindles, and Golgi tendon organs. These groups are crucial for maintaining posture and coordinating head and eye movements. 37 Cervical disc degeneration and cervical stenosis are associated with inflammation and abnormal mechanical stimulation. Inflammation and altered characteristics of mechanoreceptors lead to erroneous proprioceptive sensations in patients with cervical stenosis. 38
Proprioception is commonly evaluated by measuring JPE, which reflects an individual's ability to perceive and replicate specific head and neck positions. Several tools have been developed to measure JPE, including the CROM device, wearable inertial sensors, laser pointer systems, and optoelectronic motion analysis systems.25,39,40 Although these alternative methods have shown acceptable levels of reliability and validity, the CROM device was selected for the present study due to its widespread clinical use, ease of application, and cost-effectiveness. 41
Nevertheless, no study in the literature has been identified that assesses the correlation between the degree of stenosis and proprioception and joint ROM by researchers. Given that this is the first study on this topic, we believe our work holds significant importance.
Another group in which the proprioceptive sense is affected is patients with cervical spondylosis. Reddy et al. demonstrated that JPE is significantly higher in patients with cervical spondylosis compared to a healthy control group, indicating the impact of cervical spondylosis on proprioceptive function. 42 This study demonstrated that proprioceptive sensitivity is compromised in patients diagnosed with cervical spondylosis. Thus, the assessment of cervical proprioception is a critical component of the treatment process for individuals with cervical spondylosis and chronic neck pain. However, aforementioned study did not investigate the association between the severity of cervical stenosis, a secondary condition arising from cervical spondylosis, and proprioceptive function.
There are studies in the literature that investigate the efficacy of proprioception exercises in the treatment of cervical region pathologies. In a randomized controlled trial conducted by Izquierdo et al., training in proprioception targeting the cervical region was demonstrated to exert beneficial effects on the functionality of the deep cervical flexor muscles. 43 Likewise, a study examining the effect of proprioception training in patients with chronic neck pain showed that adding proprioceptive exercises to standard treatment was effective in reducing pain and disability. 44 These studies emphasize the importance of integrating proprioception training into treatment plans.
One significant effect of cervical stenosis is its impact on quality of life and activities of daily living. In a study investigating the effect of cervical spondylotic myelopathy on quality of life compared to other chronic diseases, it was revealed that cervical spondylotic myelopathy affects the quality of life of individuals more than cancer and diabetes. 45 This fact reveals the importance of taking the necessary precautions before cervical stenosis leads to myelopathy and emphasizes the significance of rehabilitation interventions once it has developed. In a study conducted on elderly individuals, Apaydın et al. showed that pain and quality of life were negatively affected as the severity of stenosis increase. 46 These findings indicate that cervical stenosis in elderly individuals may lead to difficulties in carrying out daily living activities. Nevertheless, unlike our study, proprioception and joint ROM were not evaluated in these studies.
Another factor that should be considered in patients with cervical stenosis and proprioceptive deficits is balance. Proprioceptive input is important for maintaining balance. A study revealed that cervical JPE correlates significantly with balance test scores, indicating that proprioceptive deficits contribute to balance impairments in patients with chronic neck pain. 31 Furthermore, Anwar et al. found that in patients with vestibular dysfunctions, such as benign paroxysmal positional vertigo and Ménière's disease, cervical proprioception deficits are significantly associated with balance impairments. 34
Another parameter evaluated in our study is the cervical ROM. Decreased ROM is a frequently observed finding in most etiologies of neck pain. Several studies have found that there is a substantial link between neck pain and ROM. 47 Stenneberg et al. indicated in their meta-analysis that individuals with neck pain experienced a more severe restriction in cervical ROM in all directions than those without. 48 In a study examining the upper and lower cervical regions separately, it was determined that extension was more affected. ROM is also affected in patients with cervical stenosis. Cervical stenosis is commonly associated with cervical degeneration, which leads to a reduction in ROM. Additionally, cervical stenosis worsens with certain movements, restricting these motions to minimize pain. 49 Harinathan et al. reported that cervical stenosis limits the ROM in cervical segments, thereby increasing the risk of whiplash injury. 50 However, the relationship between the degree of cervical stenosis and joint ROM was not examined in these studies.
In our study, we found that the ROM for cervical flexion and lateral flexion was significantly more restricted in patients with a greater degree of cervical stenosis. One probable explanation for the limitation in cervical flexion among these individuals is the reduced relaxation capacity of the cervical extensor muscles. The cervical flexion-relaxation ratio (FRR) provides a quantitative measure of the ability of the cervical extensor muscles to relax during full flexion of the cervical spine. In a study comparing the FRR in patients diagnosed with cervical lateral spinal stenosis to asymptomatic controls, researchers reported a significantly lower FRR in the patient group compared to the control group. 51 This finding suggests that cervical flexion may be more profoundly restricted in patients with a higher degree of stenosis. Moreover, the increased FRR observed in individuals with chronic neck pain further emphasizes the clinical significance of this metric. 52
Nevertheless, there are MRI studies in the literature indicating that cervical canal stenosis increases more markedly with extension compared to flexion. 49 The discrepancy between these findings can be attributed to the multifactorial nature of neck movements. Factors such as facet joint degeneration, muscles, and ligaments significantly influence these movements. Additionally, no differences were observed in pain severity among individuals with varying degrees of spinal canal stenosis. This observation suggests that elements beyond spinal canal stenosis contribute to pain in these patients, indicating that these same factors may also influence the restriction of extension observed in this population. Furthermore, it is important to note that the comparative study was MRI-based and focused on measuring spinal canal diameters, whereas our study utilized a goniometer to measure the individuals’ ROM. We believe that these differences are likely to explain the disparity observed between the two studies.
Additionally, lateral flexion is also affected more in patients with greater degree of cervical stenosis. Lateral bending is known to be affected in cervical disc diseases. This fact is commonly used in clinical practice. During assessment of cervical radiculopathy secondary to stenosis, one of the maneuvers that is made to compress foramina is lateral flexion, 53 Furthermore, it is documented that segmental contribution ratio in patients with herniated disc during cervical lateral bending is changed. 54 In contrast our results discovered that extension and cervical rotation are not affected by the degree of stenosis. This might be due to the fact that these movements rely more on the posterior elements and facet joints, which may not be as directly impacted by central canal narrowing.55,56
Daffner and colleagues conducted a study examining the relationship between disc disorders and cervical joint ROM, utilizing MRI imaging for assessment. 57 They found that although disc height, translational motion, and angular change were significantly affected at the level of disc herniation, no significant change was observed in adjacent segments. This study provides important insights into the segmental impact of disc herniation on movement at the affected level. However, it does not fully explore how disc disorders impact cervical mobility as a whole. While the aforementioned study assessed segmentally, our research encompassed all segments of the cervical region in a holistic manner.
The results of our study hold significant implications for the management of patients with cervical stenosis in clinical practice. Our findings indicate that patients with a higher degree of cervical stenosis may experience greater impairment in proprioception. This observation underscores the necessity of incorporating proprioceptive exercises into the rehabilitation programs for these individuals, highlighting the potential benefits of tailored therapeutic interventions. Furthermore, our findings highlight the importance of including ROM exercises in treatment plans for patients with cervical stenosis.
While previous research has demonstrated the benefits of proprioceptive exercises in managing chronic neck pain, there is a notable lack of studies that directly examine their effects on cervical stenosis. 58 Our results suggest that proprioceptive exercises could be a valuable addition to treatment plans for cervical stenosis. To confirm their efficacy, future research should prioritize randomized controlled trials designed to evaluate the long-term outcomes of proprioceptive training in this population.
Our study has some limitations. First of all, our study did not evaluate how these impairments in joint ROM and proprioception affect daily living activities and quality of life. Secondly, due to the lower frequency of advanced stenosis (stage 3), the number of patients identified in this group is comparatively smaller than in others. Studies that involve a greater number of patients with advanced cervical stenosis can yield more robust results. Significant differences may be detected across planes of motion—where our study found no significant difference between groups based on stenosis severity—with an increased sample of stage 3 patients. Another limitation of our study is the potential for interobserver variability in the MRI grading of cervical stenosis. To mitigate this issue, we utilized the Kang MRI grading system. Kang MRI grading system demonstrated high inter-observer agreement among radiologists and clinicians with variable experience. 17 Lastly, when categorized into four groups based on the degree of cervical stenosis, there was a significant difference in age among the groups. Given that cervical degeneration and stenosis are more prevalent in older individuals, these age differences are expected. However, this age variation may influence the outcomes, as proprioceptive abilities are known to decline with advancing age.
Conclusion
In conclusion, our study demonstrated that the severity of cervical stenosis significantly impacts cervical joint ROM and proprioceptive sense in the cervical region. These findings underscore the necessity of incorporating targeted proprioceptive training into rehabilitation strategies for patients with cervical stenosis. By integrating proprioception- specific exercises and therapeutic modalities that enhance proprioceptive feedback, clinicians can markedly improve functional outcomes and may even slow the progression of symptoms. Particularly, initiating proprioceptive training in patients with mild to moderate cervical stenosis may yield significant benefits by enhancing proprioceptive function before it becomes severely impaired. Future rehabilitation protocols should prioritize the improvement of proprioception, tailoring exercises to the individual needs and severity levels of cervical stenosis, to promote recovery and enhance quality of life.
Footnotes
Acknowledgements
We extend our gratitude to the Rector and the Scientific Research Projects Commission for their support of our project.
Ethical approval
The study was approved by Ethics Committee of Buca Seyfi Demirsoy Trainin and Research Hospital (Number: 2024/245, Date: 28.02.2024).
Author contributions
OE,BT,FT and ASKK participated in the conception and design of the study. OE, ASKK was responsible for data acquisition. OE, BT,FT and ASKK analyzed and interpreted the data. OE,BT,FT, ASKK drafted the manuscript and OE, BT and ASKK critically revised the manuscript for important intellectual content. All authors approved the final version of the manuscript.
Funding
The funding for purchasing the Pa CROM used in this project was provided by Izmir Democracy University Scientific Research Comission (HIZDEP-TIP2402).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available upon reasonable request.
Informed consent
Written informed consent was obtained from all participants.