
Abstract
Purpose
Upper limb dysfunction and inability to carry out everyday tasks are important consequences of disease process in breast cancer survivors. The aim of this study was to compare upper extremity functional exercise capacity and arm functionality between patients with breast cancer and healthy controls.
Methods
Ninety individuals participated in this analytical cross-sectional study. The study included 45 patients with breast cancer (mean age = 56.69 ± 9.37 years) and 45 healthy controls (mean age = 54.71 ± 6.54 years). The unsupported functional arm exercise capacity was evaluated using the 6-min Pegboard and Ring Test (6PBRT). The Quick Disabilities of the Arm, Shoulder, and Hand Questionnaire (Q-DASH) was used for arm functions.
Results
The 6PBRT score of patients with breast cancer was significantly lower than those of healthy controls with medium effect size (194.16 ± 34.91 rings and 218.87 ± 43.87 rings, respectively; p = 0.004, η2 = 0.065). The mean Q-DASH score of the patients was 22.12 ± 15.70. According to the Q-DASH score, 35.6% (n = 16) of the participants’ arm functions were classified as normal, 51.1% (n = 23) having problems but working, and 13.3% (n = 6) being unable to work. There was a significant moderate negative correlation between 6PBRT performance and Q-DASH score in patients’ with breast cancer (r = −0.453, p = 0.002).
Conclusion
Upper extremity exercise capacity and functionality are negatively affected in breast cancer survivors. Therefore, cardio-oncological rehabilitation approaches should incorporate arm aerobic exercise training to improve arm functionality during long-term follow-up after breast cancer medical treatments.
Introduction
According to recent statistics, the most prevalent malignancy in women is breast cancer, about 2.3 million new cases detected globally, accounting for approximately 23.8 percent of all new cancer cases. It is also reported to have the highest mortality rate among women, with about 670,000 deaths (15.4%). 1 While survival rates following breast cancer are steadily increasing due to advancements in treatment options, this improvement has also led to a rise in the prevalence of impairments and adverse long-term effects. 2 These persistent side effects and impairments can negatively impact physical, psychological, and social well-being and lead to an activity limitation and deterioration of quality of life. 3
The surgical and radiotherapy treatments that mainly target the breast, thorax, and axillary region negatively affect the musculoskeletal system, nerve tissues, and most importantly, the lymphatic system in these areas. 3 These treatments cause scarring and fibrosis in the breast, axilla and thorax, axillary web syndrome and tension in the pectoral muscles.3,4 These impairments can disrupt the kinematics of shoulder joint and cause a decrease in the range of motion (ROM), pain and discomfort in the shoulder and upper extremity. 5 Local treatments applied to these areas also cause damage to the nerve tissue in the region and cause neuropathies, neuropathic pain, loss of sensation, and impaired activation of the muscles. 6 At the same time, it has been reported that the most important treatment side-effect causing serious arm dysfunction is lymphedema. 7
Upper limb muscle weakness, upper extremity movement limitation, pain, and reduced quality of life are other common problems following surgery and radiotherapy for breast cancer. The prevalence and severity of these outcomes vary considerably from person to person. However, breast cancer survivors continue to be affected by physical problems even years after treatment, and these physical problems cause disruption in the activities of daily living (ADLs) and increase stress and anxiety for patients who are in remission and want to return to normal life. 8
Reduced upper limb function, or the inability to carry out everyday tasks because of upper limb dysfunction, is a typical side effect of breast cancer treatment. A prevalence of 60% one year following surgery has even been documented in studies. Upper limb dysfunction has a negative impact on quality of life, ability to participate in the community, and the perceived well-being of breast cancer survivors. Increased upper limb pain, decreased shoulder ROM and hand grip strength, and a higher number of comorbidities were the variables that were consistently linked to impaired upper limb function at the ICF function level in a systematic review of factors influencing ICF function level. 9 Results regarding the relationship between upper extremity function and variables in other ICF domains were reported to be conflicting. 9 The 6-min pegboard and ring test (6PBRT) is a simple, practical and feasible test that is frequently used in clinics and for patients with chronic disorders for evaluating upper extremity functional exercise capacity.10–12 The 6PBRT has good test-retest reliability in patients with breast cancer with an ICC1,2 value of 0.871 [95% confidence interval (CI) 0.769–0.928] and it is a valid functional test in breast cancer that presented significant correlations with peak oxygen consumption (r = 0.634, p < 0.001), and peak workload (r = 0.546, p < 0.001) during arm ergometer test. 10 The 6PBRT score was reported to be closely related to ADLs performance in different populations.13–15 Currently, there is a lack of studies in the literature investigating the 6PBRT performance of patients with breast cancer compared to healthy controls. Therefore, the primary aim of this study was to evaluate upper extremity exercise capacity and functionality in patients with breast cancer and to compare these findings with those of healthy individuals. The secondary aim of the study was to determine the relation of 6PBRT performance with arm functionality as an indicator for ADLs.
Materials and methods
Study design
This analytical cross-sectional study was performed at Hacettepe University, Faculty of Physical Therapy and Rehabilitation, Department of Cardiorespiratory Physiotherapy and Rehabilitation between March and May 2025. The patients with breast cancer were recruited from Hacettepe University, Faculty of Medicine, Department of Medical Oncology. The study was approved by the Hacettepe University Faculty of Physical Therapy and Rehabilitation Ethics Board (February 20, 2025, with FTREK 25/01 approval number), and written informed consent was provided for each participant. The study was registered at ClinicalTrials.gov (NCT06859593).
Participants
The study included breast cancer survivors and age- and sex-matched healthy adults without any chronic disease. The inclusion criteria for breast cancer survivors were individuals aged 18–65 years with stage I-III breast cancer who were willing to participate in the study, who were at least 15 months post-surgery and active treatment (e.g., surgery/chemotherapy), who had no problems in reading and/or understanding the scales, and who were able to cooperate with the tests. The presence of active infection that may affect exercise performance, such as neurological or musculoskeletal problems, symptomatic heart disease, or any disease that may affect cognitive status was an exclusion criterion for breast cancer survivors. Healthy individuals between the ages of 18–65 years volunteered to participate in the study, had no problems in reading or understanding the scales, and could perform the tests with cooperation. The following are the requirements for healthy controls to be included: Be willing to engage in the study, be between the ages of 18 and 65 years, who could cooperate during the examinations and had no barriers for reading or comprehending the scales. Healthy adults were excluded if they had any neuromuscular or orthopaedic conditions that would affect their ability to walk or do exercises, any chronic illnesses, or rheumatic or mental illnesses that could affect their ability to comply or cooperate with exercise tests.
Sample size calculation
The results of the study conducted by Oncu et al. the reliability and validity of upper extremity functional tests in breast cancer patients were used to determine the sample size of our study. 10 According to this study, to achieve a power of 90% and an effect size of 1.28, at least 14 people should be included separately for the two groups. Considering that there may be a 10% patient loss, a required sample size of at least 16 participants was planned in both groups. On the other hand, we tried to include as many as participants for increasing effect size of primary outcome and expected variability according to stage of cancer, type of surgery, and type of adjuvant therapy. The analysis was performed using the G*Power analysis system (G*Power Software version 3.1.9.3, Heinrich Heine University, Düsseldorf, Germany).
Assessments
Participants’ age, body weight, height, body mass index (BMI), affected extremity, family history, and smoking history were recorded. The patients with breast cancer were questioned and their lymphedema status was recorded as either “present” or “absent”. Arm length, arm circumference, and forearm circumference were measured. Functional arm exercise capacity and upper extremity functionality were evaluated.
Measurement of arm length, arm and forearm circumference
Arm circumference and length were measured using a tape measure. With the participants’ arms in the anatomical position, the distance from the acromion process to the lateral border of the radial styloid process was measured and recorded as arm length. Arm circumference was measured from the midpoint between the acromion and olecranon, and forearm circumference was measured from the side of the olecranon where the forearm reached the largest diameter when the arm was in a relaxed position next to the body. 16 Arm length, arm circumference, and forearm circumference of the dominant side of healthy individuals were compared to the affected side of patients with breast cancer.
Unsupported functional arm exercise capacity
Functional upper extremity exercise capacity was assessed using the 6-Minute Pegboard and Ring Test (6PBRT). The reliability and validity of 6PBRT was demonstrated in patients with breast cancer. 10 During the test, participants were seated in front of a pegboard and instructed to simultaneously move rings from the lower to the upper pegs using both hands as quickly as possible. The total number of rings moved was recorded as the 6PBRT score. Before and after the test, systolic blood pressure (SBP), diastolic blood pressure (DBP) with aneroid sphygmomanometer (Erka, Bad Tölz, Germany), heart rate (HR) and oxygen saturation (SpO2) with pulse oximeter (Nonin pulse oximeter palmsat® 2500 series, Plymouth, MN, USA) were measured and perceptions of dyspnea, general fatigue and arm fatigue according to modified Borg scale (mBS/0-10) were recorded. 10
Upper extremity functionality
Participants’ upper extremity functionality was assessed using the 11-item Disabilities of the Arm, Shoulder, and Hand Quick Questionnaire (Q-DASH). 17 The overall Q-DASH score is between 0 and 100, with 0 denoting no functional impairment and 100 denoting severe upper limb dysfunction. The following are the cut-off positions for functional interpretation: 0–15: Upper extremity function is normal; 16–40: having problems but working; and >40: being unable to work. 18
Statistical analysis
IBM SPSS Statistics version 23.0 (IBM Corp., Newark, NY, USA) was used for all statistical analyses. Histograms and probability plots, as well as analytical tests like the Kolmogorov-Smirnov test, were used to assess the data distribution's normality. Depending on the data distribution, either the independent samples t-test or the Mann-Whitney U test was used to compare the outcomes of breast cancer patients with healthy controls. Categorical variables were analyzed using either Fisher's exact test or the Chi-square test. The Pearson correlation coefficients were calculated to investigate the relationship between the 6PBRT score and Q-DASH score, arm length, arm circumference, and forearm circumference variables. Statistical significance was defined as a p-value <0.05. 19 The correlation levels were interpreted as follows: 0–0.25: Negligible, 0.26–0.49: Weak, 0.50–0.69: Moderate, 0.70–0.89: Strong, 0.90–1.00: Very strong correlation. 20 The one-way analysis of variance (ANOVA) was used to compare 6PBRT and Q-DASH scores among breast cancer survivors according to cancer stage and type of adjuvant therapy. When overall significance was observed, pairwise post-hoc tests were performed using Tukey's test, and Bonferroni correction was applied to control for type I error for multiple comparisons of 6PBRT and Q-DASH scores. A multiple regression analysis was done to determine the effects of BMI, comorbidities and smoking history on 6PBRT score. Analysis of covariance (ANCOVA) was performed to control confounding factors, including BMI, comorbidities and smoking history on 6PBRT score as primary outcome. The partial η2 values were classified as small effect (η2 = 0.01), medium effect (η2 = 0.06), and large effect (η2 = 0.14). 21
Results
The flowchart of the study was presented in Figure 1. Fifty-five patients with breast cancer were directed by a medical oncology physician. The two patients with breast cancer did not meet the inclusion criteria, and eight patients refused to participate in the study. Forty-eight healthy adults were interviewed for the study. Three healthy adults did not agree to participate in the study. Therefore, 45 patients with breast cancer and 45 healthy controls were included in the study (Figure 1).
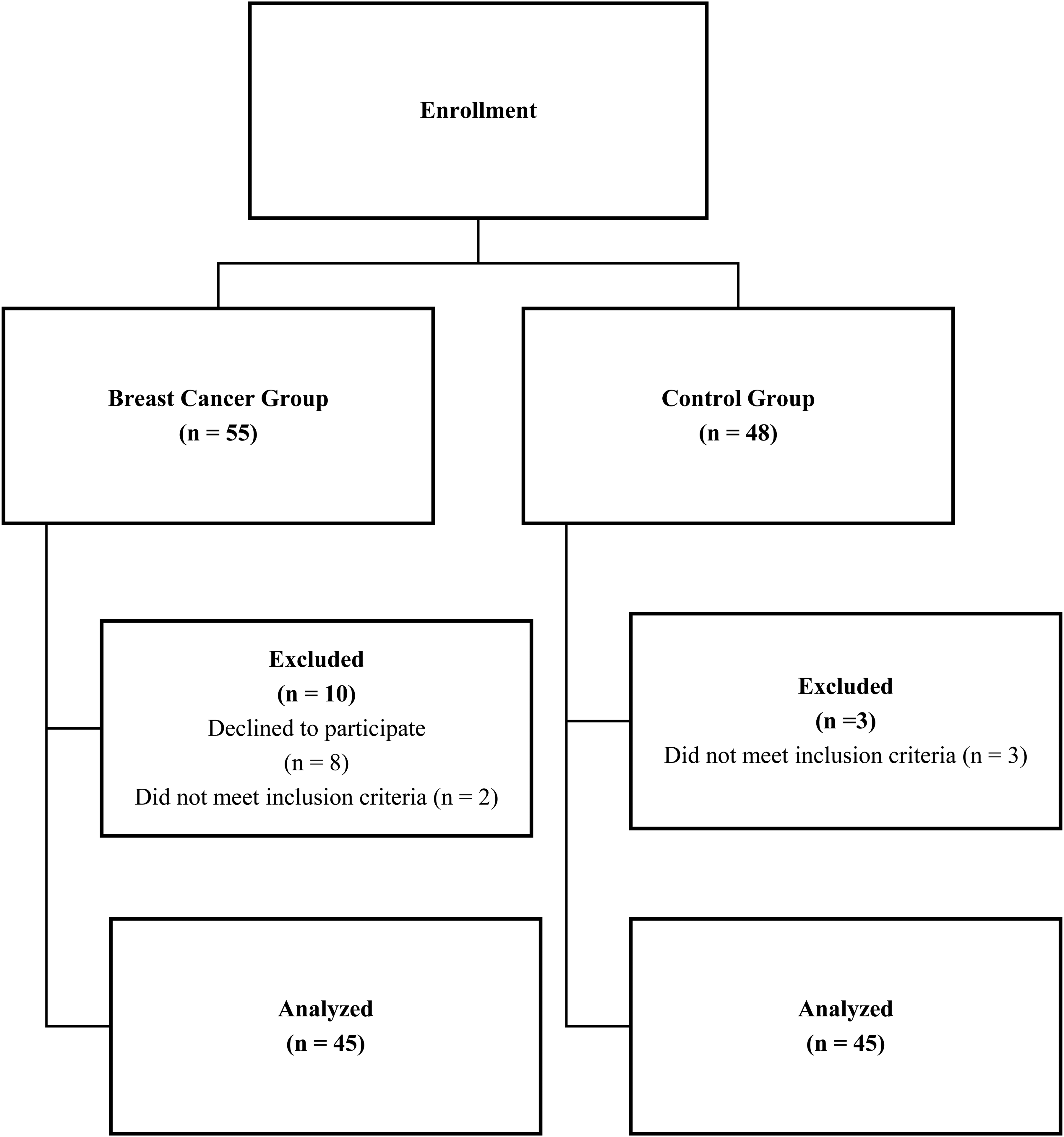
Flow diagram of the study.
The demographic and clinical characteristics of all participants are presented in Table 1.The mean age was 56.69 ± 9.37 years in the breast cancer group and 54.71 ± 6.54 years in the control group. The groups were comparable for age, gender and BMI (p > 0.05, Table 1). The distribution of comorbidities were as follows in patients with breast cancer: 11.1% (n = 5) had hypercholesterolemia, 31.1% (n = 14) had hypertension (HTN), 6.7% (n = 3) had thyroid dysfunction, and 11.1% (n = 5) diabetes mellitus (DM) (Table 1).
Demographic and clinical information of all participants.
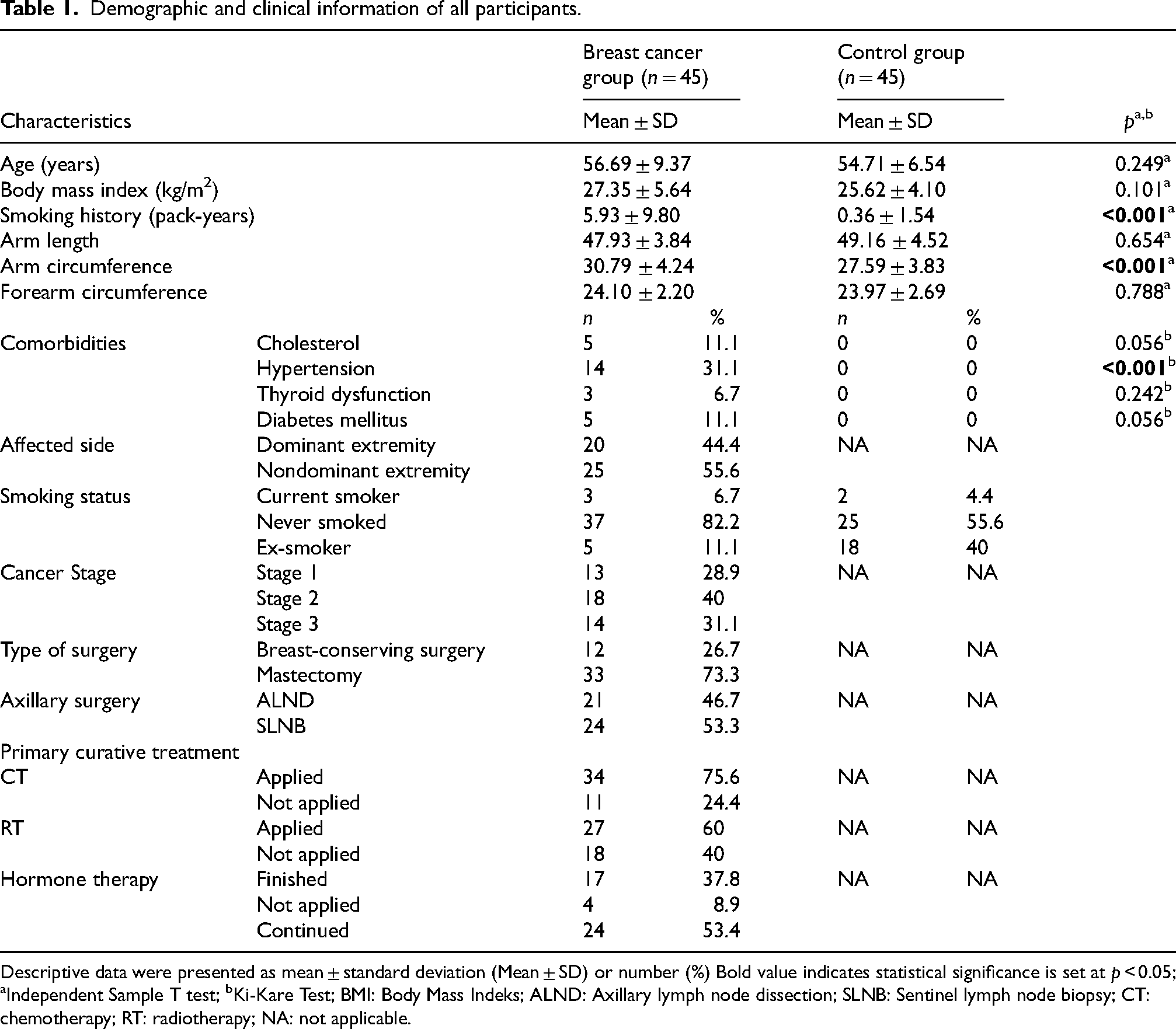
Descriptive data were presented as mean ± standard deviation (Mean ± SD) or number (%) Bold value indicates statistical significance is set at p < 0.05; aIndependent Sample T test; bKi-Kare Test; BMI: Body Mass Indeks; ALND: Axillary lymph node dissection; SLNB: Sentinel lymph node biopsy; CT: chemotherapy; RT: radiotherapy; NA: not applicable.
According to clinical status, 28.9% of patients (n = 13) had stage 1, 40% (n = 18) had stage 2, and 31.1% (n = 14) had stage 3 breast cancer. 26.7% (n = 12) of patients with breast cancer had breast-conserving surgery and 73.3% (n = 33) had a mastectomy. Axillary lymph node dissection (ALND) was performed in 46.7% (n = 21), and sentinel lymph node biopsy (SLNB) in 53.3% (n = 24), of the patients with breast cancer. There was no breast cancer related lymphedema (BCRL) in breast cancer patients who participated in the study.
The 6PBRT score was 194.16 ± 34.91 rings in patients with breast cancer and 218.87 ± 43.87 rings in the healthy controls. There was a statistically significant difference between two groups in terms of 6PBRT score. (p = 0.004, Table 2, Figure 2). The 6PBRT score of 27 (60%) patients with breast cancer was lower than the 95% confidence interval (CI) of the healthy controls (205.69–232.05 rings). According to ANCOVA analysis, there was significant difference with medium effect in 6PBRT score between breast cancer and healthy groups after controlled for BMI (F = 6.074, p = 0.016, η2 = 0.065), smoking history (F = 9.351, p = 0.003, η2 = 0.097), hypercholesterolemia (F = 7.927, p = 0.006, η2 = 0.084), thyroid dysfunction (F = 8.320, p = 0.005, η2 = 0.087), HTN (F = 6.703, p = 0.011, η2 = 0.072) and DM (F = 7.437, p = 0.008, η2 = 0.079). The BMI, comorbidities and smoking history significantly predicted 6PBRT score in breast cancer survivors based on multiple regression analysis [F(6, 38) = 3.925, p = 0.004, R2 = 0.383]. The BMI and presence of DM from variables added statistically significantly to the prediction (p < 0.05). There were no effect of BMI and smoking history on 6PBRT score in healthy controls [F(2, 42) = 1.422, p = 0.253, R2 = 0.063].
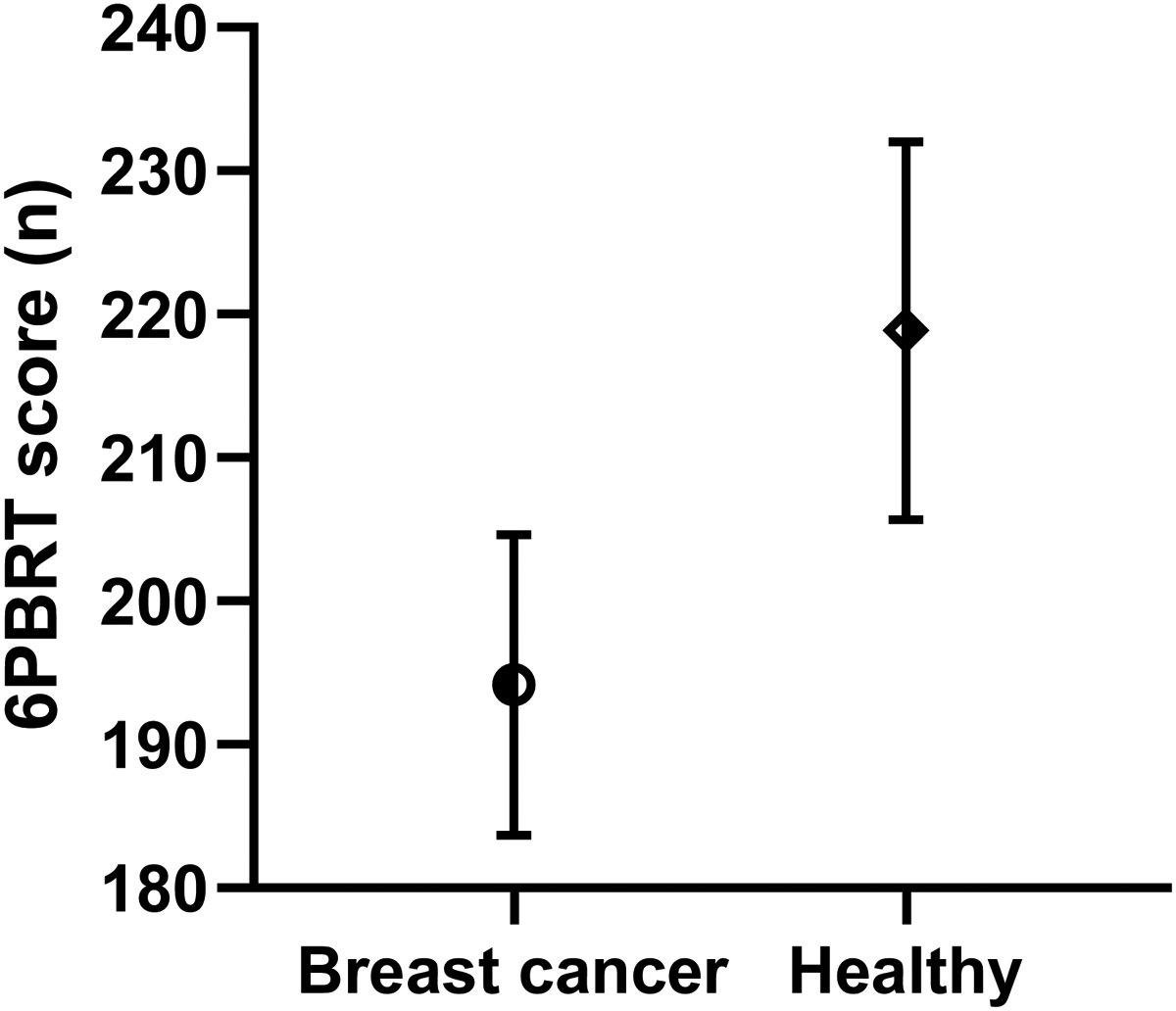
The 6PBRT score between the patients with breast cancer and healthy controls (p = 0.004). Figure was presented as mean with 95% confidence interval.
Comparison of pre and post test results of 6PBRT score, Q-DASH score and 6PBRT, Q-DASH parameters of the participants.
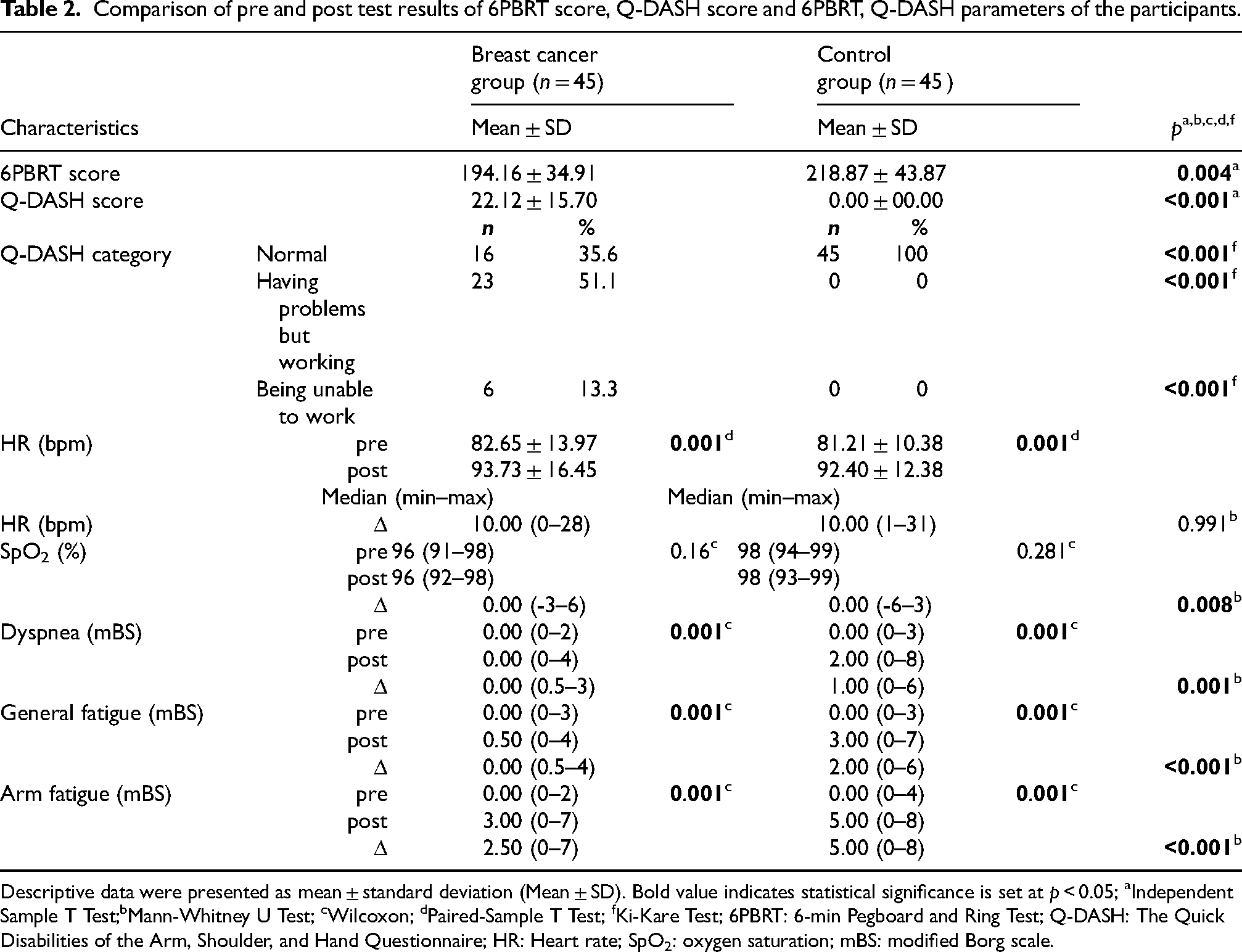
Descriptive data were presented as mean ± standard deviation (Mean ± SD). Bold value indicates statistical significance is set at p < 0.05; aIndependent Sample T Test;bMann-Whitney U Test; cWilcoxon; dPaired-Sample T Test; fKi-Kare Test; 6PBRT: 6-min Pegboard and Ring Test; Q-DASH: The Quick Disabilities of the Arm, Shoulder, and Hand Questionnaire; HR: Heart rate; SpO2: oxygen saturation; mBS: modified Borg scale.
The difference between the baseline and endpoint values of HR, dyspnea, arm fatigue and general fatigue parameters of 6PBRT was statistically significant in both groups (p < 0.05, Table 2). The changes in SpO2, dyspnea, arm fatigue and general fatigue during 6PBRT were significantly higher in healthy controls than patients with breast cancer (p < 0.05, Table 2).
The mean Q-DASH score of the breast cancer and healthy groups were 22.12 ± 15.70 and 00.00 ± 00.00, respectively (Table 2). There was a statistically significant difference in Q-DASH score between the groups participating in the study (p < 0.001, Table 2). According to the Q-DASH score, 35.6% (n = 16) were classified as normal arm functions, 51.1% (n = 23) having arm function problems but working, and 13.3% (n = 6) being unable to work due to arm functions in breast cancer.
There were significant differences in 6PBRT and Q-DASH scores between the groups based on cancer stages (p < 0.05, Table 3) but there was no significant difference after Bonferroni correction for multiple comparisons (p > 0.05). The 6PBRT score and Q-DASH score did not differ according to type of surgery, chemotherapy, radiotherapy, and hormone therapy in patients with breast cancer (p > 0.05, Table 3). The 6PBRT score was 181.23 ± 33.20 rings for patients who underwent ALND, while it was 205.45 ± 32.97 rings for patients who underwent SLNB in the group with breast cancer. The 6PBRT score of the ALND group was lower than that of the SLNB group (p = 0.018, Figure 3). In the group with breast cancer, the Q-DASH score of patients who underwent ALND was 28.24 ± 15.91, while the 6PBRT score of patients who underwent SLNB was 16.76 ± 13.68. The Q-DASH score of the ALND group was also lower than that of the SLNB group (p = 0.013).
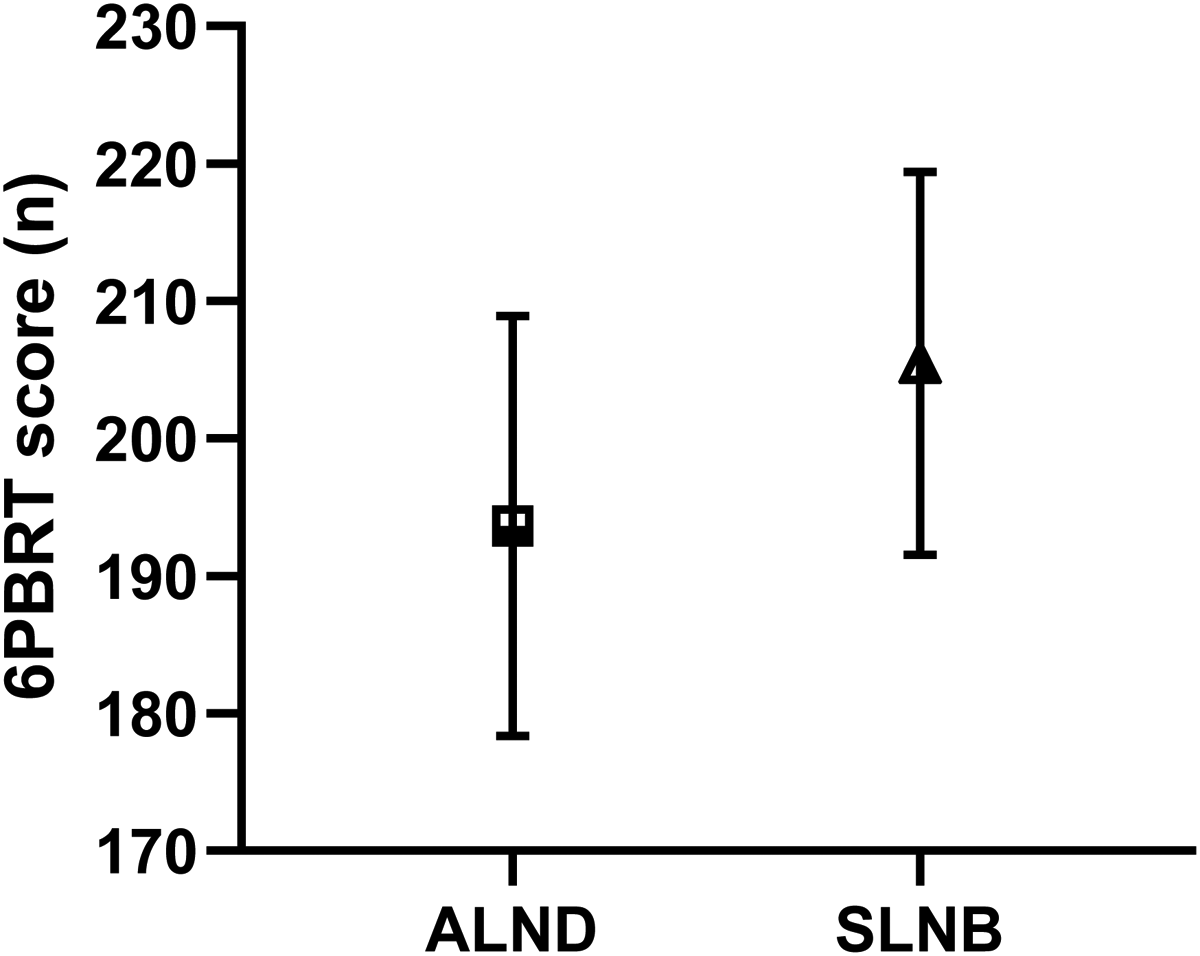
The comparison of the 6PBRT score in patients with breast cancer underwent axillary lymph node dissection versus sentinel lymph node biopsy (p = 0.018). Figure was presented as mean with 95% confidence interval.
6PBRT score of breast cancer patients according to cancer stage and type of adjuvant therapies
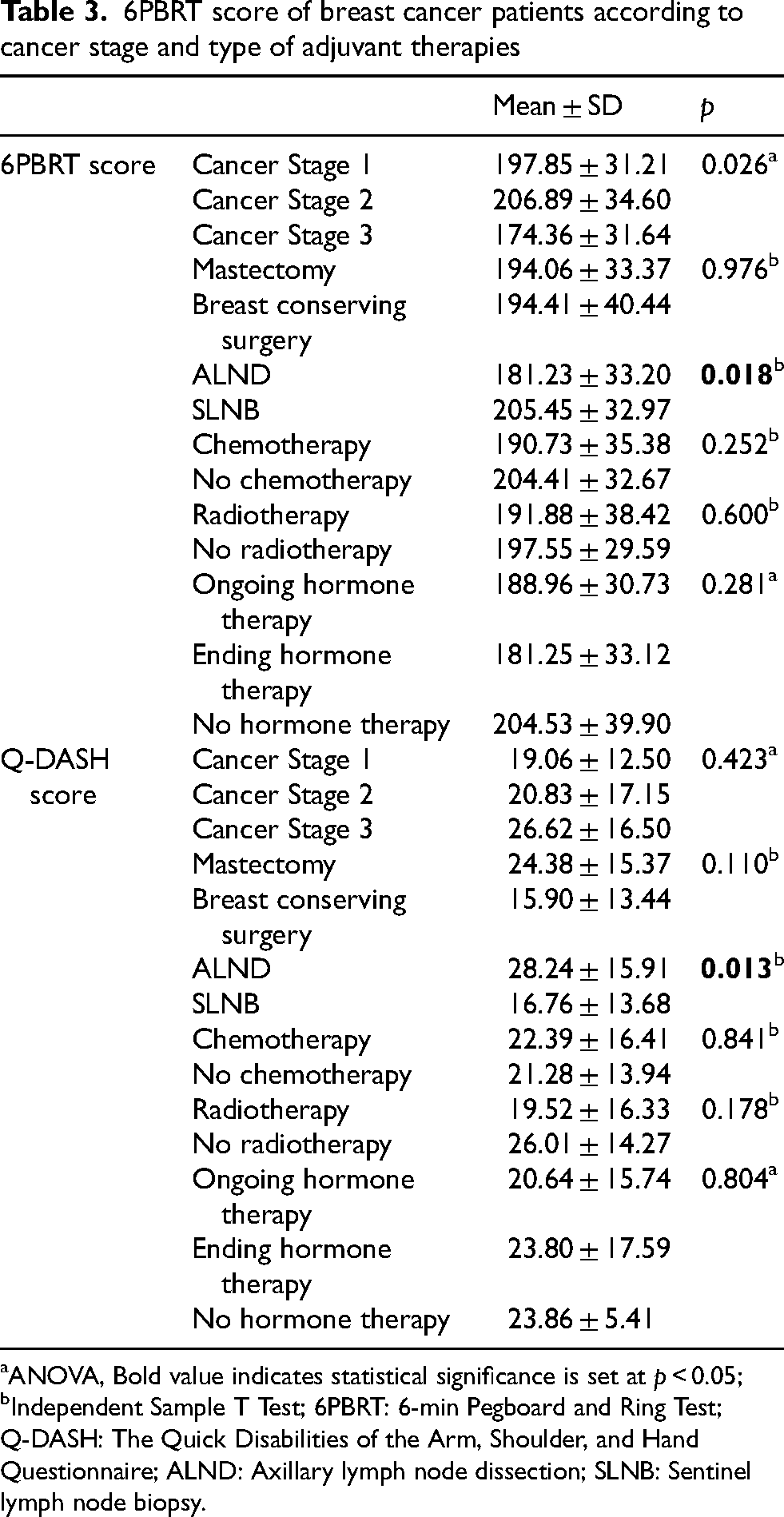
ANOVA, Bold value indicates statistical significance is set at p < 0.05; bIndependent Sample T Test; 6PBRT: 6-min Pegboard and Ring Test; Q-DASH: The Quick Disabilities of the Arm, Shoulder, and Hand Questionnaire; ALND: Axillary lymph node dissection; SLNB: Sentinel lymph node biopsy.
There was also a statistically significant negative correlation between the 6PBRT performance and Q-DASH score in breast cancer survivors (r = −0.453, p = 0.002). There was no statistically significant correlation between 6PBRT performance and Q-DASH score in healthy individuals (p = 0.411). Otherwise, there was no significant correlation between 6PBRT score and upper arm length, arm circumference, and forearm circumference in both groups (p > 0.05).
Post hoc power analysis was carried out on our mean 6PBRT scores in breast cancer and healthy groups data (d = 0.623, α = 0.05 [two-tailed]). Power (1−β) of this study was 83%.
Discussion
According to main findings of this study, patients with breast cancer have worse 6PBRT performance than healthy controls, which is a measure of functional arm exercise capacity. The majority of breast cancer patients experience arm dysfunction, which is linked to functional limitations in ADLs. The functional arm exercise capacity of breast cancer survivors isn’t affected by the type of surgery, chemotherapy, radiotherapy, and hormone therapy. Otherwise, functional arm performance of patients underwent ALND is poorer and arm dysfunction during daily life is greater than those who underwent SLNB.
Our previous study showed that the 6PBRT is a useful, easy, feasible, applicable, and reliable field test with good test-retest reliability that assesses both arm function and endurance. Peak oxygen consumption and maximal workload obtained on arm ergometry are significantly associated with the 6PBRT score and this test was determined to be valid for assessing functional arm exercise capacity in breast cancer patients. 10 To the best of our knowledge, this was the first study to compare 6PBRT performance of patients with breast cancer compared to healthy controls.
Sufficient ROM, strength, and muscular endurance of arms are required for successful functional performance of the upper limb. Decline in upper limb function following surgical and radiation treatments, is frequently seen in the first year after treatment and persists in subsequent years in breast cancer. Decreased upper limb function compared to pre-cancer levels has been self-reported in 21% to 35% of women treated for breast cancer up to 6 years after diagnosis. 22 Long-term decline in upper extremity mobility has been reported in women treated for breast cancer. One study reported a > 10% decrease in shoulder joint flexion >5 years after breast cancer treatment, while another study stated that ≥20 degrees of motion loss was present 7 years after surgical treatment. 23 At the same time, a 10% to 15% decrease in upper extremity strength has been reported within 1 to 5 years after breast cancer treatment. 24 There are conflicting results in the literature regarding muscular endurance in breast cancer survivors. While some studies reported no deficiency in muscular endurance, others reported a 20% loss in breast cancer. 22 Oncu et al. reported that higher 6PBRT scores were associated with higher upper extremity arm endurance in breast cancer survivors. 10 In this study, it was shown that upper extremity functional exercise capacity and endurance of individuals with breast cancer were lower than that of healthy individuals, in accordance with the previous findings. We determined this activity restriction with performance-based functional arm exercise test compared to healthy controls for the first time. The 6PBRT test leads a moderate cardiorespiratory and metabolic demand when compared with maximal arm cycle ergometer test in healthy individuals. 25 Hemodynamic variables (HR, SpO2, SBP, and DBP) and dyspnea, arm fatigue, and general fatigue perceptions were recorded before and after 6PBRT to evaluate the effect of 6PBRT on these variables in both group. There were clinically significant increases in the above-mentioned variables after the test in both groups. This situation can be attributed to increased metabolic demands due to various changes in the respiratory and circulatory systems during the 6PBRT test. These changes indicate that 6PBRT provides the necessary load and can be used as an exercise test in this population. 16 Otherwise, higher change in dyspnea, arm and general fatigue perceptions in healthy individuals could be related with higher effort and performance during 6PBRT in this group.
LeBlanc et al. reported that the Q-DASH score was valid and reliable for assessing upper extremity function in patients with breast cancer. In addition, the mean Q-DASH score was 19 ± 19, and the median score was 11 (0–80) in their study and they showed functional impairments in arms. 26 In our study, the mean Q-DASH score of individuals with breast cancer was 22.12 ± 15.70. According to the Q-DASH score, approximately 65% of breast cancer patients participating in our study experienced problems with upper extremity function. The 6PBRT was mostly shown to reflects limitations in ADLs in chronic respiratory or cardiac disorders.15,27 Our study also showed that there was a moderately negative correlation between the Q-DASH score and 6PBRT score in patients with breast cancer. This supports the idea that the 6PBRT is a test that accurately reflects arm function in daily life in breast cancer patients, as reported in the literature.15,27
A wide range of issues affecting the breast, shoulder area, and/or upper limb can arise from several treatment techniques for breast cancer, such as hormone therapy, immunotherapy, chemotherapy, radiotherapy, and axillary and breast surgery. The most commonly reported morbidities associated with these interventions include BCRL, sensory disturbances such as numbness, and axillary web syndrome. These complications can significantly impair upper extremity function and negatively impact overall quality of life in breast cancer survivors. 28 Studies have reported incidences of 20% for lymphoedema, 78% for numbness, and 86% for axillary web syndrome in breast cancer survivors. In addition, loss of shoulder ROM is frequently described after breast cancer surgery and radiotherapy, and has been reported to occur between 0% and 84%, particularly in relation to axillary surgical management. 9 Patients treated with ALND are more likely than those with SLNB to have decreased shoulder ROM, muscle weakness, pain, lymphedema, and limited ADLs. 29 The patients with breast cancer who underwent SLNB had significantly more abduction, flexion, and adduction ROM than patients who underwent ALND 9–12 months after axillary surgery. 8 Barranger et al. reported that the probability of shoulder restriction was 1.27 times more likely for the ALND group than for the SLNB group. 30 As a result of our study, the Q-DASH score and 6PBRT score of the ALND group were lower than the SLNB group as an expected finding. In our study, it was found that the 6PBRT score of the breast cancer group did not change according to breast cancer stage. In addition, there was no difference on both the 6PBRT and Q-DASH scores according to type of surgery and adjuvant therapy in patients with breast cancer. BCRL is one of the most important factors with negative effect on the upper extremity functionality of individuals after breast cancer. In the light of this information, the advanced stage of cancer may cause a larger surgical operation and higher prevalance of BCRL in breast cancer.10,28 Otherwise, De Groef et al. reported that arm dysfunction isn’t related with treatment-related factors in these population. 9 We think that absence of BCRL in breast cancer survivors with different disease stages and other factors related with arm functional performance could led to comparable 6PBRT scores depending on cancer stage, type of surgery and adjuvant therapy.
Studies have reported that there were no relations between arm length and circumferences of arm and forearm and 6PBRT score in healthy adults.16,31 Oncu et al. reported that there was a moderately negative correlation between arm and forearm circumferences and 6PBRT score in breast cancer survivors. The reason for this finding was reported to be that 18.7% of the individuals participating in the study had BCRL that may have a negative association with functional arm performance. 10 In our study, we didn’t show any correlation between arm and forearm circumferences and 6PBRT scores in both groups. One reason for this finding was due to the absence of BCRL in the patients with breast cancer. We also think that there is no relationship between arm length and 6PBRT score because all participants were kept at arm length distance from the pegboard during 6PBRT. Fonseca et al. reported that the 6PBRT score is negatively correlated with BMI, body fat and fat mass in their study. 25 Ozsoy et al. showed that the 6PBRT score was significantly lower in older COPD with higher smoking exposure compared to healthy controls. 32 According to ANCOVA analysis, the significant difference in 6PBRT score between breast cancer vs healthy controls is still present after adjusting for BMI, smoking history and comorbidities. Despite these variables (BMI, smoking history and comorbidities) explain 6PBRT score in breast cancer survivors based on multiple regression analysis, BMI and DM are significant contributor to the prediction. These shows us that higher BMI and presence of DM comorbidity have negative effect on functional arm performance in breast cancer. We think that these could be associated with change in muscle quality and performance with negative changes in body composition and DM pathological process.
The main limitation of this study was the heterogeneous distribution of the disease stage of breast cancer patients. This could have limited the generalizability of our results. As the adjuvant therapy of breast cancer becomes more individualized, several treatment techniques are combined based on the cancer's stage. Despite there is some data regarding any association between arm function and treatment-related factors in breast cancer, variability in disease stages might lead inconsistent associations with 6PBRT performance. Therefore, more research about the effects of disease stage on arm functional performance is needed. The second limitation of this study was inclusion of wide age range (18–65 years). The third limitation of our study is that the participants’ physical activity levels were not assessed. Otherwise, the strength of our study lies in being the first study to compare the upper extremity exercise capacity of individuals with breast cancer and healthy individuals by using functional arm exercise test.
Conclusion
In conclusion, breast cancer survivors have lower functional arm exercise capacity, as shown by the 6PBRT score and decreased arm functionality compared to healthy individuals. The 6PBRT performance is closely with upper extremity functionality in breast cancer. Future studies are needed to study the effects of disease on arm functional exercise capacity based on the disease duration and in a limited range of age and should consider also body composition and comorbidity level of patients. At the same time, the effectiveness of different arm training programs or rehabilitation protocols on functional arm exercise capacity should be investigated in future studies. Our study will serve as a guide for future research and clinical interventions in the cardio-oncologic rehabilitation field.
Footnotes
Ethics approval
The Hacettepe University Faculty of Physical Therapy and Rehabilitation Ethics Board approved this study (20.02.2025, FTREK25/01).
Consent to participate
Yes.
Consent for publication
Yes.
Author contributions
HO: concept, design, data collection and or processing, data analysis and or interpretation, literature search, writing manuscript
EC: concept, design, supervision, data collection and or processing, data analysis and or interpretation, literature search, writing manuscript, critical review
NVY: concept, design, supervision, data collection and or processing, data analysis and or interpretation, literature search, writing manuscript, critical review
MS: supervision, data analysis and or interpretation, writing manuscript, critical review
SA: data collection and or processing, writing manuscript
Declaration of conflicting interests
The authors declare that they have no conflict of interest.
Data availability statement
Not applicable.