
Abstract
Background
Pain is the most common symptom in Thoracic Outlet Syndrome (TOS).
Objective
This study was conducted to determine the characteristics of pain in patients with TOS.
Methods
66 patients (59 female, 7 male) participated in this cross-sectional study. Pressure pain thresholds (PPT) and pain intensity were evaluated. Central Sensitization Inventory (CSI), Tampa Kinesiophobia Scale (TSK), Toronto Alexithymia Scale (TAS) and Pain Catastrophizing Scale (PCS) were used. Mann-Whitney U and Spearman tests were used for statistical analyzes.
Results
A significant positive correlation was observed between symptom duration (6.42 ± 5.33 years) and both CSI (r = 0.261,p = 0.034) and TSK (r = 0.271,p = 0.028). Centrally sensitized patients were found to have significantly worse kinesiophobia (p = 0.005), catastrophizing (p = 0.031) and alexithymia (p = 0.049). Patients with pain catastrophizing had higher kinesiophobia (p = 0.003). There was no difference in PPT in trapezius (p = 0.507) and infraspinatus (p = 0.690) muscles but there was a difference in the extensor carpi radialis (p = 0.009) and extensor indicis proprius (p = 0.002). Pain values were similar between patients who had undergone surgery and those who had not.
Conclusions
The findings of this investigation indicate that symptoms related to central sensitization in TOS are linked to chronic pain indicators, while catastrophizing is associated with kinesiophobia. Additionally, it was observed that a prolonged duration of symptoms in TOS intensifies the severity of central sensitization and kinesiophobia. The similarity in pain parameters between the surgical and non-surgical groups may reflect the effects of chronic pain due to prolonged symptom duration. These results suggest that TOS should not be perceived solely as a musculoskeletal issue.
Keywords
Introduction
Thoracic Outlet Syndrome (TOS) is a multifaceted condition caused by the compression of the brachial plexus, subclavian vein, or subclavian artery at the thoracic outlet. 1 The etiology of TOS includes congenital bone and soft tissue anomalies, post-traumatic changes, and repetitive upper extremity use. 2 Although national data are unavailable, globally collected prospective data estimate the annual incidence of neurogenic thoracic outlet syndrome to be 2–3 cases per 100,000 people, venous 0.5–1 per 100,000, and arterial TOS 0.2–0.7 per 100,000, confirming that TOS is a rare disease. 3 TOS is characterized by diffuse compression symptoms, the most common sign of which is pain. Pain is not limited to the upper extremities but may radiate to the neck, upper back, chest and occipital regions. 4 Unlike pain, paresthesia, grip weakness, impaired fine motor skills, muscle atrophy, pallor, and color changes in the extremity are other pathophysiological findings observed in TOS. 5 Additionally, in a prospective study including 66 patients undergoing surgical treatment for neurogenic TOS, depression and anxiety were found to be highly prevalent, with 43% of patients screening positive for depression and 35% for anxiety. 6
The diagnosis of TOS may be delayed because of problems in differential diagnosis and because many diseases show similar symptoms. TOS may be confused with diseases such as carpal tunnel syndrome, cervical disc pathologies, complex regional pain syndrome, cubital tunnel syndrome and shoulder tendinopathies due to similar symptoms.7–10 In addition to the wide-ranging aetiology, the lack of standardized diagnostic criteria leads to delayed diagnosis and delayed initiation of effective treatment.10,11 Consequently, patients often present with chronic pain. 12
Chronic pain induces morphological and histological changes in the pain neuromatrix, contributing to psychosocial responses such as depression, anxiety, pain catastrophizing, kinesiophobia, alexithymia, and central sensitization.13,14 These factors, which are fundamental components of chronic pain, contribute to an increase in the intensity and duration of pain. 15 The effect of chronic pain on emotional and behavioral factors, and consequently on quality of life, has been studied in various musculoskeletal disorders. Yücel et al. found that high central sensitization inventory scores in patients with chronic musculoskeletal pain were associated with more severe pain, longer symptom duration, and increased disability. 16 Additionally, Feng et al. identified anxiety as the primary determinant of central sensitivity in patients with carpal tunnel syndrome. 17 In a large cross-sectional study published in 2025 by Skúladóttir et al. chronic pain was identified in 59% of individuals with a history of whiplash, and this group reported significantly more severe pain, higher pain interference, lower health-related quality of life, and higher disability compared to chronic pain patients without a history of whiplash. 18 Asiri et al. reported that in patients with chronic neck pain, kinesiophobia showed a strong positive correlation with pain intensity, suggesting that individuals with greater fear of movement experience higher levels of perceived pain. 19 This relationship highlights the role of psychological factors, particularly fear-avoidance beliefs, in amplifying pain perception through mechanisms such as hypervigilance, increased muscle tension, and altered pain modulation. Aaron et al. conducted a meta-analysis examining the relationship between alexithymia and pain-related outcomes, revealing that individuals with chronic pain exhibited significantly higher alexithymia scores compared to both the non-clinical and the non-pain clinical control group. Additionally, alexithymia showed a positive correlation with pain intensity, physical intervention, depression, and anxiety. 20 All of the factors mentioned may promote behavioral patterns associated with intractable pain and ultimately reduce the effectiveness of treatment interventions.21,22
Although the presence of long-term pain symptoms in TOS is known, the characteristics of chronic pain are unknown. Chronic pain and functional impairments associated with TOS may also affect cognitive and behavioral processes such as pain-related anxiety, focusing on the pain, and avoidance behaviors. Therefore, it is crucial to evaluate both the physiological and cognitive-behavioral aspects of TOS to understand its multifactorial impact on patients.
Therefore, this study aimed to evaluate the central components of pain in TOS patients and to explore their relationship with established pain parameters. We hypothesized that symptom duration in TOS patients affects all pain characteristics. Additionally, there was relationship between pain intensity, central sensitization, kinesiophobia, pain catastrophizing, and alexithymia in TOS patients.
Methods
This cross-sectional study included 66 patients (59 women, 7 men) diagnosed with TOS who were evaluated at the Faculty of Physical Therapy and Rehabilitation Hand Surgery Rehabilitation Unit at Hacettepe University. Data for this study were collected between January 2019 and February 2020. Clinical evaluation, computed tomography angiography, brachial plexus magnetic resonance imaging and nerve conduction EMG were routinely performed. Roos test was performed in clinical evaluation. 23 All patients experienced pain, paresthesia, numbness and weakness in the arms during the Roos test. With these results, the Roos test was recorded as positive. In computed tomography angiography, subclavian artery and vein compression were examined. None of the patients had a positive EMG result. According to the literature, EMG gives conflicting results in patients with TOS. 24 Therefore, EMG results were not taken into consideration in the diagnosis. 25 All evaluations were performed and diagnosed by a thoracic surgeon with 28 years of experience (AKC). As a result of physical examination and imaging, all patients were diagnosed as mixed type.
Inclusion and exclusion criteria
Body Mass Index (BMI) between 18.5 and 29.9 who exhibited typical TOS symptoms such as numbness, tingling, and upper arm weakness, particularly aggravated by overhead movements or continuous arm use, were included in the study. In addition, participants had to be literate in Turkish and capable of understanding and completing the questionnaires without assistance.
Participants with a BMI outside the 18.5–29.9 range were excluded to reduce potential confounding effects of obesity or underweight status on pain thresholds, nerve compression, and musculoskeletal function. The patients with cervical disc herniation, fibromyalgia, rotator cuff disorders, carpal tunnel syndrome, cubital tunnel syndrome, ankylosing spondylitis, neoplastic process and those who did not provide consent were not included in the study.
Outcome measures
Age (year), gender, height (cm), weight (kg), affected side, pain location and symptom duration (year) were recorded. Symptom duration was calculated as the time elapsed from the onset of the pain to the initial assessment. A body diagram was used to determine the location of pain and the percentage of specific pain sites. People were asked to mark the painful areas on the body diagram. The study team identified the anatomical regions on the body diagram. The percentage of patients’ pain sites was calculated by dividing the number of patients who marked each site by the total number of patients.
Also, central sensitization, pain catastrophizing, kinesiophobia and alexithymia, which are the psychological and the central components of chronic pain were assessed.
1.Pain Catastrophizing Scale (PCS): Assesses the frequency of catastrophic thoughts related to pain, with scores ≥30 indicating significant catastrophizing. A maximum score of 52 points can be obtained from the scale and a high score indicates a high level of pain catastrophizing. The Turkish version of the scale was used to assess pain catastrophizing (Cronbach's Alpha = 0.90).26,27
2.Central Sensitization Inventory (CSI): Evaluates central sensitization, with scores ≥40 indicating central sensitization. 28 The Turkish version of the scale, which has very high validity (Cronbach's alpha = 0.92), was used. 29
3.Tampa Scale of Kinesiophobia (TSK): Measures fear of movement and re-injury, with higher scores reflecting greater kinesiophobia. The Turkish version of the scale, which has high validity, was used in the present study (ICC = 0.806). 30
4.Toronto Alexithymia Scale (TAS): Alexithymia is inadequacy in emotional control and cognitive functioning. Alexithymia was assessed with The Toronto Alexithymia Scale (TAS). A higher score reflects severe alexithymia. A score of ≤51 points indicates the absence of alexithymia, and a score of ≥61 points indicates a high level of alexithymia. 31 The Turkish version of the scale, which had high validity, was used (Cronbach's Alpha = 0.78). 32
5.Visual Analogue Scale (VAS) is a widely used clinical tool for assessing the subjective intensity of pain. It consists of a 10-centimeter horizontal line, where the left endpoint (0) represents “no pain” and the right endpoint (10) indicates “worst pain imaginable”. 33 Participants were asked to mark a point on the line corresponding to the intensity of pain they experienced. The distance from the left endpoint to the marked point was then measured with a ruler and recorded in centimeters (cm). The VAS was administered to evaluate pain intensity during rest, activity, and nighttime conditions.
Pressure pain threshold (PPT) assessment:
The pressure pain threshold was measured in terms of kilogram force (KgF) with the Chatillon-100 LBF AMETEK device. PPT is a sufficiently reliable measurement for clinical use. 34 Measurements were made bilaterally in the trapezius, infraspinatus and extensor carpi radialis muscles. The researcher placed the device in the relevant site and the device was applied in a vertical direction and at a constant rate while increasing the force at a constant rate of 1 kg/cm2. The patients were asked to give a verbal response such as ‘ok/sufficient’ when they felt only a slight pain. The measurements were made from the midpoint of the upper trapezius for the trapezius muscle, 2–3 fingers below the scapular spine for the infraspinatus muscle, and 2–3 fingers below the lateral epicondyle for the extensor carpi radialis muscle, from the medial side of the radius 4–5 fingers above the lateral styloid process for the extensor indicis proprius muscle 35 (Figure 1). The pain tolerance level was recorded. After all 8 muscles were investigated, the subjects were allowed to rest for 5 min. This procedure was repeated a total of 3 times.

Pressure pain threshold measuring points.
Statistical analysis
Data obtained in the study were analyzed statistically using SPSS Version 20 software. Conformity of the variables to normal distribution was assessed using visual (histogram and probability graphs) and analytical methods (Kolmogorov-Smirnov, Shapiro-Wilk tests). Descriptive analyses were stated as mean ± standard deviation values for numerical data. In the examinations of the relationships between data, Spearman analysis was used for non-normally distributed data and Pearson analysis for normally distributed data. In the interpretations of the correlation analyses, values between 0.00 and 0.10 were evaluated as ‘negligible’, 0.10–0.39 as ‘weak’, 0.40–0.69 as ‘moderate’, 0.70–0.89 as ‘strong’, and 0.90–1.00 as ‘very strong’. 36 A positive correlation coefficient indicated a linear relationship between the variables, and a negative correlation showed an inverse relationship. Comparisons of pain characteristics between patients with and without central sensitization, pain catastrophizing and non-catastrophizing, operated and non-operated were performed with independent t-tests when data were parametric, and with Mann-Whitney U-tests when data were non-parametric. Type 1 error level was taken as 5% for statistical significance.
Results
The demographic characteristics and pain-related scores of the patients are summarized in Table 1. The mean age of the participants was 36.97 ± 9.73 years, with a mean symptom duration of 6.42 ± 5.33 years. TOS was observed on the right side in 19 patients, on the left side in 26 patients, and bilaterally in 21 patients.
Demographic characteristics of patients.
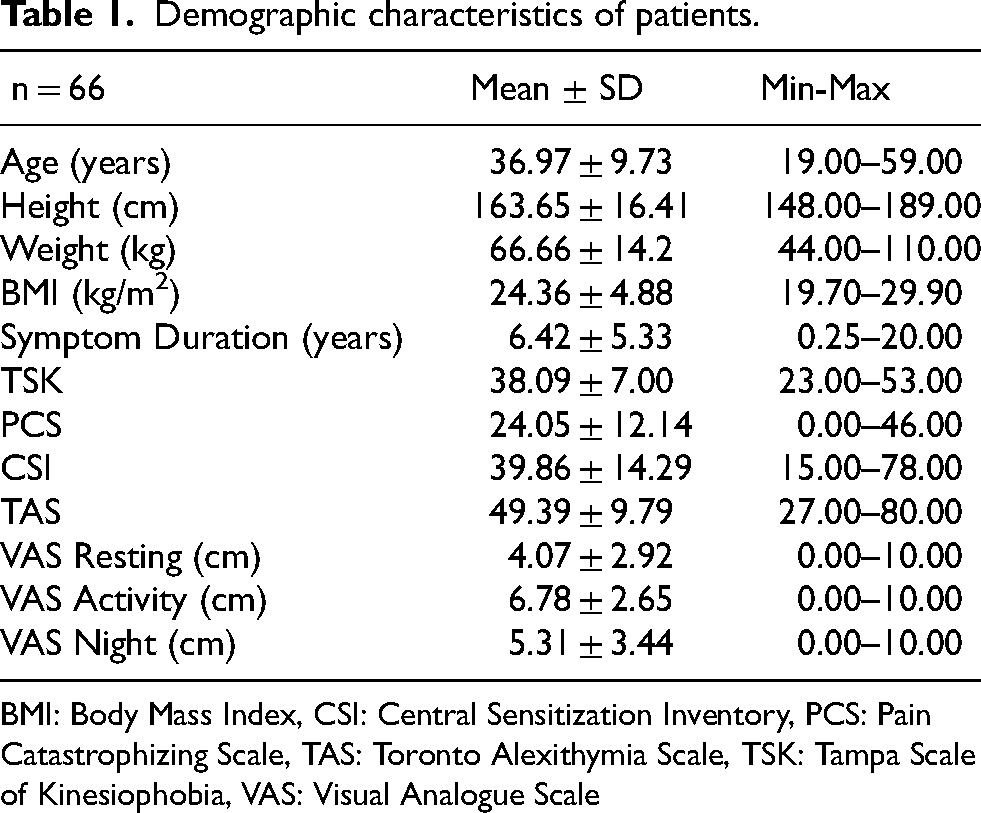
BMI: Body Mass Index, CSI: Central Sensitization Inventory, PCS: Pain Catastrophizing Scale, TAS: Toronto Alexithymia Scale, TSK: Tampa Scale of Kinesiophobia, VAS: Visual Analogue Scale
The distribution of pain locations showed that the hand (67%) and thoracic region (67%) were the most affected areas. This was followed by the elbow (64%), shoulder (57%), and forearm (55%). Pain was also frequently reported in the supraspinous fossa (40%), axillary region (37%), and infraspinous fossa (37%). The upper trapezius (35%) demonstrated a moderate prevalence of pain, whereas the occipital region (11%), face (11%), and lumbar region (9%) were the least frequently affected areas. The pain locations are presented in Table 2.
Pain locations of patients.

Pressure pain thresholds (PPT)
This analysis aimed to compare the pressure pain thresholds in the affected and unaffected extremities of TOS patients. Since it was not possible to make a comparison between sides in patients with bilateral TOS, these patients were excluded from this analysis. Therefore, the data from 21 patients with bilateral TOS were excluded. Pressure pain threshold comparisons were performed for the trapezius, infraspinatus, extensor carpi radialis, and extensor indicis proprius muscles using data from 45 patients with unilateral TOS.
PPT values of the trapezius (p = 0.507) and infraspinatus (p = 0.690) muscles were similar in patients with and without TOS. PTT values of the extensor carpi radialis (p = 0.009) and extensor indicis proprius (p = 0.002) muscles were similar. Detailed PPT findings are presented in Table 3.
Patients’ pressure pain threshold values.
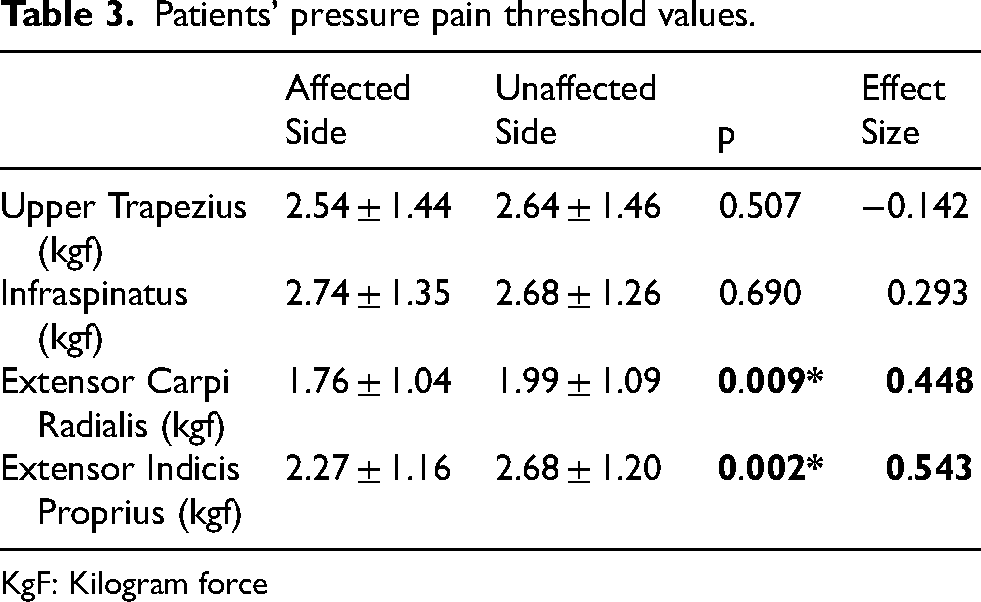
KgF: Kilogram force
Correlation analysis
Symptom duration showed statistically positive correlations with CSI (r = 0.261, p = 0.034) and TSK (r = 0.271, p = 0.028) (Table 4). A weakly positive correlation was observed between PCS and CSI (r = 0.271, p = 0.027), and a moderate correlation was found between PCS and TSK (r = 0.567, p < 0.001). Additionally, CSI was positively correlated with TSK (r = 0.323, p = 0.008) and VAS-resting pain intensity (r = 0.261, p = 0.034) (Supplementary File 1).
Correlations between symptom duration and pain parameters.
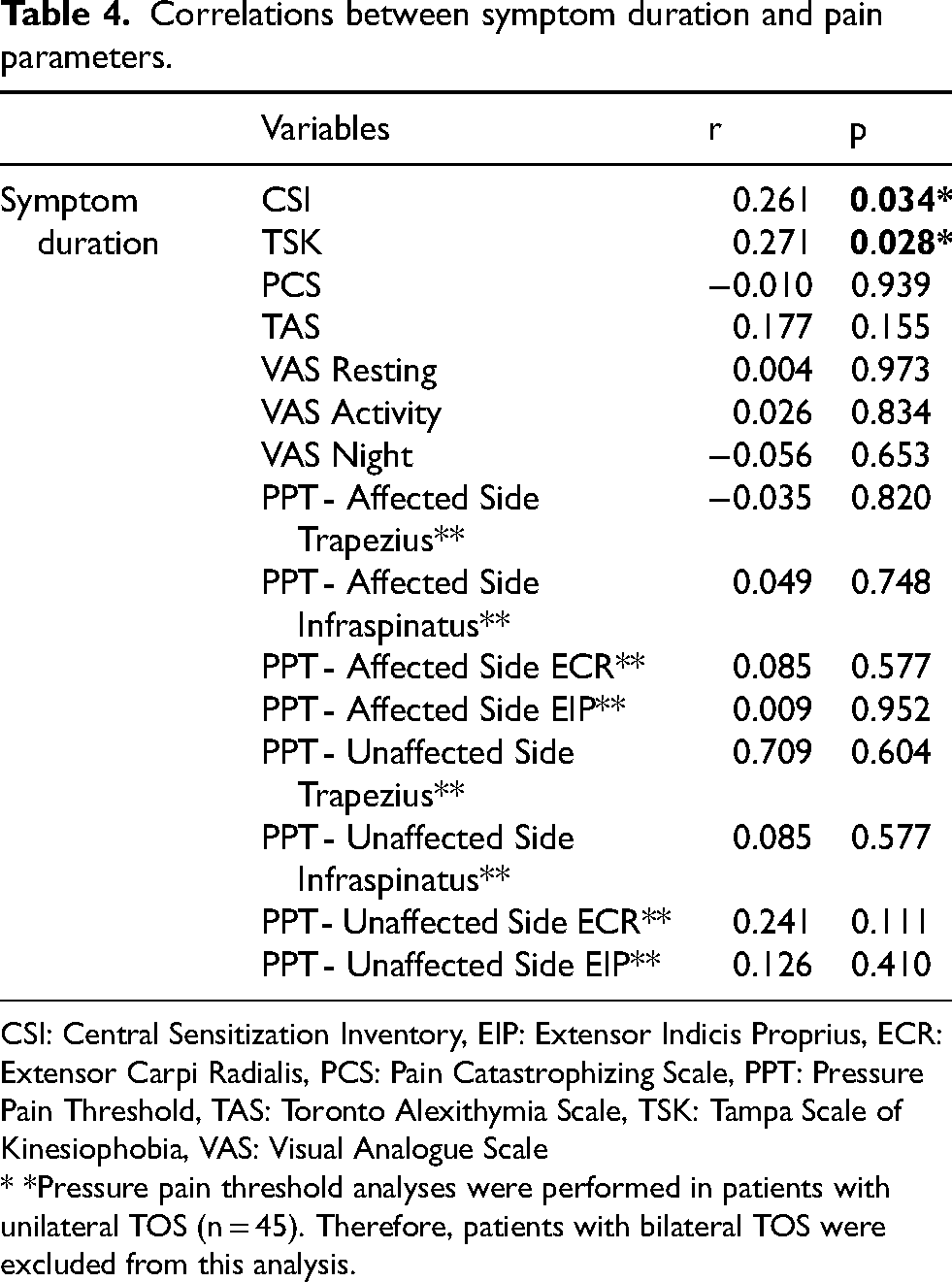
CSI: Central Sensitization Inventory, EIP: Extensor Indicis Proprius, ECR: Extensor Carpi Radialis, PCS: Pain Catastrophizing Scale, PPT: Pressure Pain Threshold, TAS: Toronto Alexithymia Scale, TSK: Tampa Scale of Kinesiophobia, VAS: Visual Analogue Scale
* *Pressure pain threshold analyses were performed in patients with unilateral TOS (n = 45). Therefore, patients with bilateral TOS were excluded from this analysis.
Comparison of groups
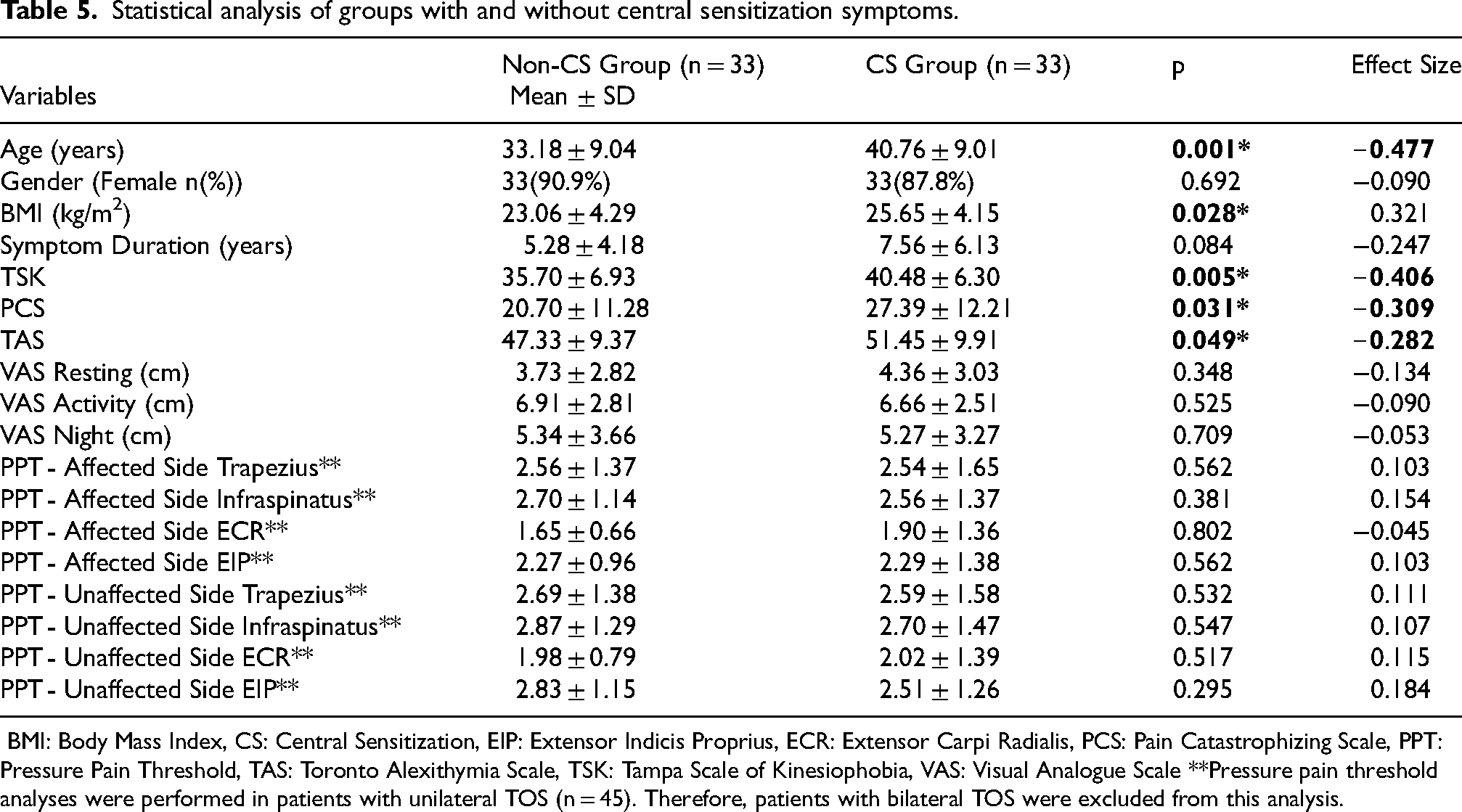
When comparing participants with and without central sensitization, significant differences emerged in several variables. The CS group was older than the non-CS group (p = 0.001, d = −0.48) and had a higher body mass index (p = 0.028, d = 0.32). Although symptom duration was longer in the CS group (7.56 ± 6.13 years) compared to the non-CS group (5.28 ± 4.18 years), this difference did not reach statistical significance (p = 0.084).
Psychological measures showed that the CS group reported significantly higher scores on the Tampa Scale of Kinesiophobia (p = 0.005, d = −0.41), Pain Catastrophizing Scale (p = 0.031, d = −0.31), and Toronto Alexithymia Scale (p = 0.049, d = −0.28). Pain intensity at rest, during activity, and at night did not differ significantly between the groups. The analysis was conducted only in patients with unilateral TOS. Based on data obtained from 45 participants, there was no difference in PPT values between the affected and unaffected extremities (Table 5).
Statistical analysis of groups with and without central sensitization symptoms.
When participants were grouped according to their PCS scores, no significant differences were found in age, gender distribution, BMI, symptom duration, pain intensity and alexithymia. A significant difference was observed for kinesiophobia: participants in the high-PCS group had higher TSK scores compared to those in the low-PCS group (p = 0.003, d = –0.44), indicating that greater pain catastrophizing was associated with higher levels of movement-related fear. Although central sensitization scores tended to be higher in the high-PCS group (44.00 ± 15.21) compared to the low-PCS group (37.50 ± 13.35), the difference approached but did not reach statistical significance (p = 0.057). The analysis was conducted only in patients with unilateral TOS. No significant group differences were found for any pressure pain threshold measurements on either the TOS or non-TOS sides across the trapezius, infraspinatus, extensor carpi radialis, or extensor indicis proprius muscles (Supplement File 2).
Surgical vs. Non-Surgical Groups
No significant differences were found between the operative and non-operative TOS groups in demographic, clinical, or psychosocial variables. Both groups showed comparable levels of central sensitization, kinesiophobia, pain catastrophizing, alexithymia, pain intensity, and pressure pain thresholds, indicating that surgical status was not associated with differences in pain sensitivity or psychological factors (Table 6).
Statistical analysis of the operated and non-operated patients.
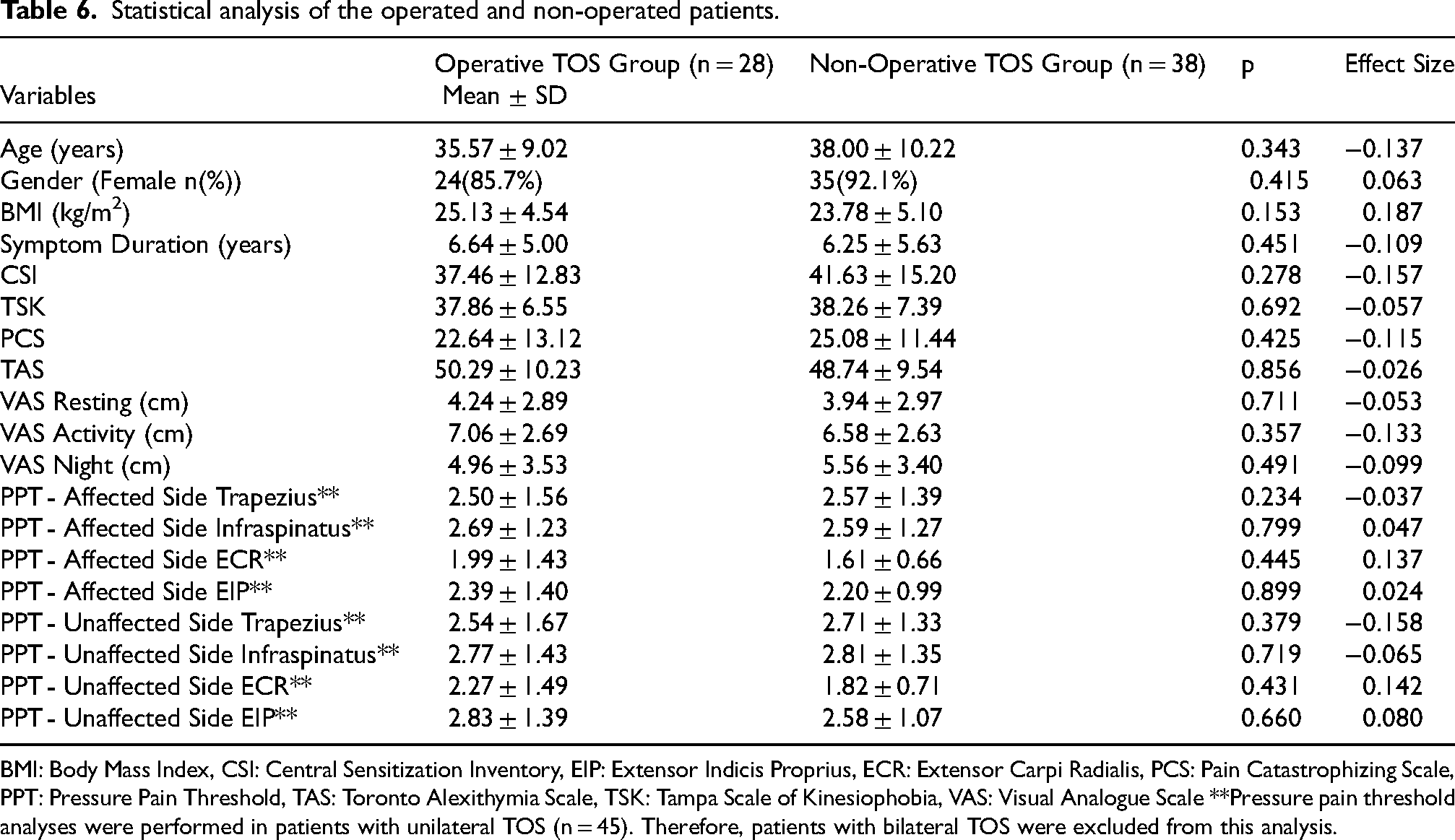
BMI: Body Mass Index, CSI: Central Sensitization Inventory, EIP: Extensor Indicis Proprius, ECR: Extensor Carpi Radialis, PCS: Pain Catastrophizing Scale, PPT: Pressure Pain Threshold, TAS: Toronto Alexithymia Scale, TSK: Tampa Scale of Kinesiophobia, VAS: Visual Analogue Scale **Pressure pain threshold analyses were performed in patients with unilateral TOS (n = 45). Therefore, patients with bilateral TOS were excluded from this analysis.
Discussion
This study explored the pain characteristics of TOS patients, revealing that longer symptom duration correlates with increased central sensitization and kinesiophobia. Chronic pain indicators such as pain catastrophizing, kinesiophobia and alexithymia were higher in the patients who have higher central sensitization. Patients with a high pain catastrophizing level were seen to be significantly affected by the fear of movement. In the patients who had undergone surgery and those who had not, pain component results were found to be similar. Additionally, distal part of the upper extremity showed lower PPT levels than proximal parts.
The International Association for the Study of Pain (IASP) defines central sensitization (CS) as an “increased responsiveness of nociceptive neurons in the central nervous system to normal or subthreshold afferent input.” Based on this definition, CS may offer a neurobiological explanation for chronic pain, even when there is no evident macroscopic tissue damage and peripheral nociceptors function normally. 37 The sensitization of the central nervous system, similar to inflammation, is necessary as a homeostatic mechanism in the body. It plays an adaptive and protective role in the short term by preventing further tissue damage and promoting healing in the days following an acute injury. However, when this mechanism persists over time, it becomes maladaptive, leading to pain that loses its protective function and continues even in the absence of ongoing tissue injury. This maladaptive transition helps explain why some patients experience long-term pain despite successful tissue healing. 38 This paradigm shift highlights the importance of addressing central mechanisms in the assessment and management of chronic pain. Previous studies have observed activation changes in limbic-cortical regions involved in the pain neuromatrix, such as the insula, anterior cingulate cortex, prefrontal cortex, dorsolateral frontal cortex, and somatosensory cortex, in individuals with central sensitization.39–42 Such structural and functional alterations in these regions may lead to maladaptive behavioral changes related to pain. 43
The key finding of this study was that longer pain duration was associated with greater central sensitization and kinesiophobia. We believe that longer symptom duration led to higher CS levels in our patients with TOS. The pain-related emotional and cognitive effect is more severe in patients experiencing pain for a long time. 44
In our study, the higher prevalence of kinesiophobia, pain catastrophizing, and alexithymia in the group with high CS may be due to the maladaptive effects of prolonged symptom duration. As the duration of symptoms increases, patients may avoid movement and experience associated behavioral changes. We have found that 36% of patients exhibited severe pain catastrophizing. Also, it was found correlated with kinesiophobia. We have shown that some studies have reached the same conclusions as us. Rogers et al. reported that a positive, moderate-strong correlation between kinesiophobia, pain catastrophizing, pain awareness, and pain-related negative cognitive/emotional parameters and disability in a large-scale meta-analysis of patients with pain symptoms. 45 Similarly, Uritani et al. showed that higher pain catastrophizing levels decreased physical activity in patients with knee osteoarthritis. 46 Dahmani et al. showed a strong relationship between CS scores and pain catastrophizing in a sample of 296 patients with knee osteoarthritis and chronic low back pain. 47 Bilika et al. showed that there was strong pain and kinesiophobia effect in those with central sensitization in patients with chronic shoulder pain. 48 Walankar et al., reported that patients with central sensitization had significantly higher levels of pain catastrophizing, kinesiophobia, and functional disability, while both the physical and mental components of quality of life were markedly reduced. These findings indicate that central sensitization not only amplifies pain perception but also negatively affects individuals’ psychological well-being and daily functioning. 49 All these findings may suggest that chronic pain is not merely a peripheral phenomenon but may also be associated with learned fear and negative pain-related beliefs. However, given the cross-sectional nature of our study, the directionality of the observed associations between chronic pain and central sensitization remains uncertain. Therefore, although the current findings support the relationship between chronic pain and TOS, causality cannot be inferred from this study. Longitudinal and interventional studies are needed to clarify whether mechanisms such as central sensitization, kinesiophobia, pain catastrophizing, and alexithymia can alter the process of pain chronification in TOS.
Another important finding of our study was the similarity of all the pain characteristics of patients who had undergone surgery and those who had not. The similarity in pain-related, psychological, and sensory parameters between the surgical and non-surgical TOS groups suggests that surgical decompression alone may not be sufficient to reverse central sensitization–related changes or maladaptive pain processing. This finding from our study may draw attention to the need to re-evaluate the factors influencing recovery after TOS surgery, as the literature has primarily focused on the possibility that the likelihood of recurrence may depend on the surgical approach used. 50 Although there are no studies investigating how baseline central sensitization or maladaptive behavioral changes affect postoperative recovery in TOS, this relationship has been examined in other disease populations in the literature. Abrishami et al. reported that heightened preoperative pain sensitivity, particularly to suprathreshold heat stimuli, predicted greater postoperative pain, suggesting that central sensitization mechanisms may influence recovery after surgery. 51 Suer et al. demonstrated that patients undergoing shoulder surgery who exhibited higher baseline kinesiophobia and pain catastrophizing scores experienced significantly greater postoperative pain intensity. 52 Similarly, Tokgöz et al. investigated the impact of pain catastrophizing and kinesiophobia on clinical outcomes in patients undergoing shoulder arthroscopy and found that 37% of patients exhibited significant levels of catastrophizing. The study reported that individuals with higher pain catastrophizing also demonstrated greater kinesiophobia and poorer postoperative functional recovery. 53 For these reasons, altered behavioral patterns and ineffective coping strategies may limit the effectiveness of conventional and surgical treatment methods. Future studies should investigate the contribution of baseline behavioral, emotional, and cognitive factors to postoperative recovery in TOS patients.
Notably, while the proximal muscles (trapezius and infraspinatus) exhibited comparable pressure pain thresholds between the affected and unaffected sides, the distal muscles (ECR and EIP) presented significantly reduced PPT values on the affected extremity. Additionally, when examining pain localizations, we found that among patients with unilateral TOS, 55% reported forearm pain and 64% reported elbow pain on the affected side. In contrast, 35% of these patients experienced pain in the upper trapezius region and 37% in the infraspinous fossa.
The presence of lower pain thresholds and wider pain distribution in the distal regions may represent a characteristic feature of TOS. These findings should be kept in mind during differential diagnosis and treatment planning, as they may indicate distal compression lesions rather than proximal pathologies.
This study has several limitations. The relatively small sample size represents the primary limitation of this study. It is possible that with a larger cohort, the outcomes of the correlation analyses would have yielded different results. Another limitation is that a more comprehensive evaluation of chronic pain could have been achieved by assessing additional parameters such as motivation, memory, anxiety, and depression. However, including all these parameters might have extended the assessment process considerably; thus, a consensus through the Delphi method may help determine the most appropriate evaluation tools in future studies. Furthermore, the use of self-reported, patient-based questionnaires carries the inherent risk that results may be influenced by factors such as participant motivation, recall bias, or the accuracy of self-reported information.
Conclusion
The findings of this study highlight the association between long symptom duration and chronic pain characteristics in patients with thoracic outlet syndrome, as well as the relationship between high central sensitization and more maladaptive cognitive-behavioral characteristics. These results emphasize that TOS is not merely a musculoskeletal condition but also exhibits features of chronic pain. In this context, early screening of psychological risk factors such as central sensitization, pain catastrophizing, and kinesiophobia in TOS assessment may help identify high-risk individuals who could benefit from personalized and multidisciplinary interventions. Furthermore, integrating a biopsychosocial framework into clinical practice may necessitate redefining rehabilitation strategies for TOS. Cognitive-behavioral interventions targeting maladaptive pain beliefs, catastrophic thinking, and emotional dysregulation may enhance rehabilitation outcomes. Clinical approaches such as pain neuroscience education and motivational interviewing could also be incorporated into TOS management.
Overall, these findings support a transition toward a multimodal and interdisciplinary rehabilitation model that combines physical therapy, pain education, and psychological support. Such a model addresses not only the peripheral musculoskeletal pathology but also the central and cognitive-emotional mechanisms contributing to chronic pain, thereby improving treatment efficacy, supporting functional recovery, and reducing symptom recurrence or postoperative complications.
Future research should employ longitudinal, interventional, or prospective cohort designs to determine the directionality of these associations and to evaluate whether targeting central sensitization or maladaptive pain beliefs can improve clinical outcomes. Interdisciplinary rehabilitation strategies integrating physiotherapy, pain neuroscience education, cognitive-behavioral therapy, and psychological counseling should be systematically tested in controlled studies.
Supplemental Material
sj-docx-1-bmr-10.1177_10538127251411107 - Supplemental material for An evaluation of the pain characteristics of patients with thoracic outlet syndrome
Supplemental material, sj-docx-1-bmr-10.1177_10538127251411107 for An evaluation of the pain characteristics of patients with thoracic outlet syndrome by Şule Tüzen Tek, Tüzün Fırat and Ayten Kayı Cangır in Journal of Back and Musculoskeletal Rehabilitation
Supplemental Material
sj-docx-2-bmr-10.1177_10538127251411107 - Supplemental material for An evaluation of the pain characteristics of patients with thoracic outlet syndrome
Supplemental material, sj-docx-2-bmr-10.1177_10538127251411107 for An evaluation of the pain characteristics of patients with thoracic outlet syndrome by Şule Tüzen Tek, Tüzün Fırat and Ayten Kayı Cangır in Journal of Back and Musculoskeletal Rehabilitation
Supplemental Material
sj-docx-3-bmr-10.1177_10538127251411107 - Supplemental material for An evaluation of the pain characteristics of patients with thoracic outlet syndrome
Supplemental material, sj-docx-3-bmr-10.1177_10538127251411107 for An evaluation of the pain characteristics of patients with thoracic outlet syndrome by Şule Tüzen Tek, Tüzün Fırat and Ayten Kayı Cangır in Journal of Back and Musculoskeletal Rehabilitation
Footnotes
Acknowledgment
The authors thank all respondents for participating in the study.
Ethical approval and informed consent statements
The study was approved by the relevant Institutional Review Board of the Hacettepe University (Decision No: 2020/05-47). Written informed consent was obtained from all participants prior to data collection.
Informed consent
All participants provided informed consent prior to their involvement in the study.
Author contributions
Şule Tüzen Tek and Tüzün Fırat contributed to the planning of the study, data collection, data analysis, data interpretation, drafting and publication of the manuscript. Şule Tüzen Tek is also responsible for the study as a whole. Ayten Kayı Cangır contributed to the interpretation of the data and the intellectual content of the manuscript. Finally, all authors gave final approval of the version of the article to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.