
Abstract
Background
Adolescent idiopathic scoliosis (AIS) is frequently accompanied by spinal pain, but the underlying mechanisms remain unclear. Psychological factors such as kinesiophobia may play a key role in shaping pain perception and limiting physical activity in this population.
Objective
To compare kinesiophobia levels between adolescent idiopathic scoliosis and age-matched healthy controls, and to examine the associations among kinesiophobia, pain, and quality of life.
Methods
This cross-sectional controlled study included 128 participants (72 with AIS and 56 healthy controls), all of whom had experienced spinal pain at some point in their lives. Pain intensity was evaluated using the Visual Analogue Scale (VAS), kinesiophobia with the Tampa Scale for Kinesiophobia (TSK-17), and quality of life with the refined Scoliosis Research Society-22 (SRS-22r). Cobb measurements were used to assess deformity severity. Statistical analyses were performed to determine intergroup differences and correlations between variables.
Results
Kinesiophobia scores were similar between groups but showed a significant positive correlation with pain intensity both in the AIS group (r = 0.34, p = 0.003) and in controls (r = 0.27, p = 0.044). In AIS patients, those reporting pain had significantly lower SRS-22r pain and function scores (p < 0.05). No correlation was observed between Cobb angle and either pain or TSK scores.
Conclusion
Adolescents with idiopathic scoliosis experience kinesiophobia primarily as a response to pain rather than as a function of deformity severity. Early pain management, reassurance, and motivational strategies to reduce movement-related fear may enhance adherence to exercise therapy and improve rehabilitation outcomes.
Keywords
Introduction
Adolescent idiopathic scoliosis (AIS) is a complex three-dimensional deformity of the spine that occurs between the ages of 10 and 18 years. 1 According to current diagnostic criteria, a Cobb angle of ≥10° on a standing posteroanterior (PA) radiograph is sufficient for the diagnosis of scoliosis. 2 The prevalence of back pain in patients with AIS has been reported to range between 27.5% and 72%. Interestingly, no consistent relationship has been demonstrated between pain and curve magnitude, deformity pattern, or structural abnormalities detected by magnetic resonance imaging. 3 These findings suggest that pain in AIS cannot be explained solely by biomechanical factors but is also influenced by psychological and social determinants.4,5
The biopsychosocial model has recently gained prominence as a framework for understanding the multidimensional nature of pain in adolescents with AIS. This model posits that pain arises not only from biological processes but also from the interaction of psychological status, social environment, sleep quality, stress levels, and coping skills. Studies in adolescents with AIS have demonstrated that depression, anxiety, and sleep disturbances are significantly associated with pain severity. Moreover, functional impairment and reduced quality of life are not solely related to the physical consequences of scoliosis but are closely linked to psychosocial components. 4 Therefore, assessing pain in AIS solely based on curve magnitude is insufficient; a multidimensional approach that incorporates psychosocial aspects is required.
Within this psychosocial framework, one of the most prominent concepts highlighted in recent literature is kinesiophobia. Defined by Kori et al. in 1990, kinesiophobia refers to an excessive, irrational, and debilitating fear of movement, based on the belief that activity may cause pain or re-injury. The theoretical foundation of this concept lies in the fear-avoidance model proposed by Lethem et al. in 1983, which suggests that fear and catastrophizing tendencies regarding pain trigger avoidance behaviors, leading to functional decline and the development of chronic pain.4,6 Thus, kinesiophobia is not merely a symptom but a psychological mechanism that facilitates the chronification of pain.
A more recent perspective proposed by Kochan et al., conceptualizes kinesiophobia not only as a behavioral reaction but also as an intrinsic psychological barrier that limits participation in physical activity. 7 Fear has been identified as a prognostic indicator in physiotherapy, often reducing adherence to exercise interventions. Consequently, kinesiophobia emerges as a critical factor that may negatively affect rehabilitation outcomes, particularly among adolescents.4,8,9
Recent studies have reported a notable prevalence of kinesiophobia among individuals with AIS. Ye et al., demonstrated the validity of the Tampa Scale for Kinesiophobia (TSK) in this population, 10 while Figueras et al., found a significant association between pain intensity and kinesiophobia in both adolescent and young adult scoliosis patients. 11 Their findings revealed that patients with higher pain levels exhibited increased kinesiophobia, anxiety, and depressive symptoms, along with school or work absenteeism and social dysfunction.10–12 However, the absence of healthy control groups in these studies has limited the generalizability of results and prevented a clear understanding of the role of kinesiophobia in AIS.
Therefore, the present study aims to evaluate kinesiophobia levels in AIS patients in comparison with healthy controls, examine its relationship with pain and quality of life, and contribute to the development of effective rehabilitation strategies based on these findings.
Materials and methods
Study design
This study was a prospective, single center, controlled, cross-sectional study approved by the Ethics Committee of Başakşehir Çam and Sakura City Hospital (approval no: 2023–654). An a priori power analysis was performed using G*Power software (version 3.1.9.7) to determine the minimum sample size required to detect a difference in kinesiophobia levels between adolescents with idiopathic scoliosis and healthy controls. The effect size (Cohen's d = 0.53) was calculated based on previously published mean and standard deviation values of Tampa Scale for Kinesiophobia scores reported in adolescents with idiopathic scoliosis by Figueras et al. 11 and in healthy control participants by Tissot et al. 13 Specifically, the pooled standard deviation was derived from these values, and the mean difference between groups was divided by the pooled standard deviation to obtain Cohen's d. Assuming a two-tailed significance level of α = 0.05 and a statistical power of 0.85, the required total sample size was calculated as 128 participants. This sample size was considered sufficient to detect a moderate effect size in kinesiophobia between groups and to ensure adequate statistical power for the primary analyses.
Patients were consecutively recruited from those who presented to the scoliosis outpatient clinic between 2023 and 2024. Inclusion criteria were as follows: a diagnosis of idiopathic scoliosis, a major curve in the coronal plane with a Cobb angle ≥10°, no history of previous exercise therapy, bracing, or surgical intervention, age between 10 and 18 years, and the presence of current spinal pain or a previous history of spinal pain. Patients with congenital, neuromuscular, or syndromic scoliosis were excluded from the study. The control group consisted of age- and sex-matched individuals who were evaluated in the same outpatient setting but did not meet the diagnostic criteria for scoliosis based on clinical examination and standing radiographs. The same criterion regarding current or experience of spinal pain was also applied to the control participants.
Adolescents and their parents who agreed to participate were informed about the study and provided written consent. Demographic characteristics, leg length discrepancy, and the presence of foot deformities were recorded. All participants underwent a physical and neurological examination, and their history of spinal pain was documented in detail. For patients diagnosed with scoliosis, Cobb angles were measured electronically by the same investigator, and curve location and type were classified and recorded in the patient files. As outcome measures, the Visual Analogue Scale (VAS), refined Scoliosis Research Society-22 questionnaire (SRS-22r), and Tampa Scale of Kinesiophobia-17 (TSK-17) were administered to the scoliosis group. In the control group, VAS and TSK assessments were performed.
Outcome measurements
Pain intensity was evaluated using the
There is also evidence supporting the use of the TSK in non-clinical populations. Houben et al. examined the factorial structure and psychometric properties of the scale in a general population sample and concluded that it is applicable to healthy individuals as well. 16 Although direct validation of the TSK in a non-clinical healthy population is limited, the scale has been used in control or comparison groups that included healthy individuals. 13 In line with this evidence, the questionnaire was administered to healthy control participants who had previously experienced pain but were not experiencing clinically relevant pain at the time of assessment.
Statistical analysis
All statistical analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY, USA). Descriptive statistics were presented as mean ± standard deviation (SD), median (min–max), and frequency (n, %), as appropriate. The normality of continuous variables was assessed using the Shapiro–Wilk test. Between-group comparisons (scoliosis vs. control; pain vs. no pain) were conducted using the independent samples t-test or Mann–Whitney U test for continuous variables, depending on the distribution, and the chi-square test or Fisher's exact test for categorical variables. Correlations between continuous variables were evaluated using Pearson or Spearman correlation coefficients. Pearson's or Spearman's correlation coefficients were interpreted as weak (r = 0.10–0.29), moderate (r = 0.30–0.49), or strong (r ≥ 0.50).
In addition to p-values, effect sizes were calculated to improve the interpretability of statistical findings. Cohen's d was used for between-group comparisons, with values of 0.2, 0.5, and 0.8 interpreted as small, moderate, and large effects, respectively. For correlation analyses, multiple comparisons were addressed by adopting a hypothesis-driven analytical strategy focused on predefined clinical relationships between pain, kinesiophobia, and functional outcomes. As secondary analyses were exploratory, no formal adjustment for multiple testing was applied; instead, effect sizes and consistency of associations were emphasized to reduce overinterpretation of isolated statistically significant findings. A p-value of < 0.05 was considered statistically significant.
Results
A total of 255 adolescents presenting to the scoliosis outpatient clinic between 2023 and 2024 were screened for eligibility. During screening, 96 participants were excluded because they did not meet the diagnostic criteria for scoliosis (Cobb angle <10°). Among the remaining adolescents diagnosed with scoliosis (Cobb angle ≥10°), additional exclusions were made due to neuromuscular/congenital scoliosis (n = 6), previous spinal surgery and/or a history of bracing/exercise therapy (n = 28), sagittal plane deformities (e.g., Scheuermann kyphosis) (n = 16), absence of current or previous spinal pain (n = 28), incomplete questionnaires/missing data (n = 4), and declined to participate (n = 5). Ultimately, 72 adolescents with AIS were included in the analysis. The control group consisted of age- and sex-matched individuals evaluated in the same outpatient setting who did not meet the diagnostic criteria for scoliosis on clinical examination and standing radiographs, and the same pain criterion (current or previous spinal pain) was applied; 56 healthy controls were included in the analyses.
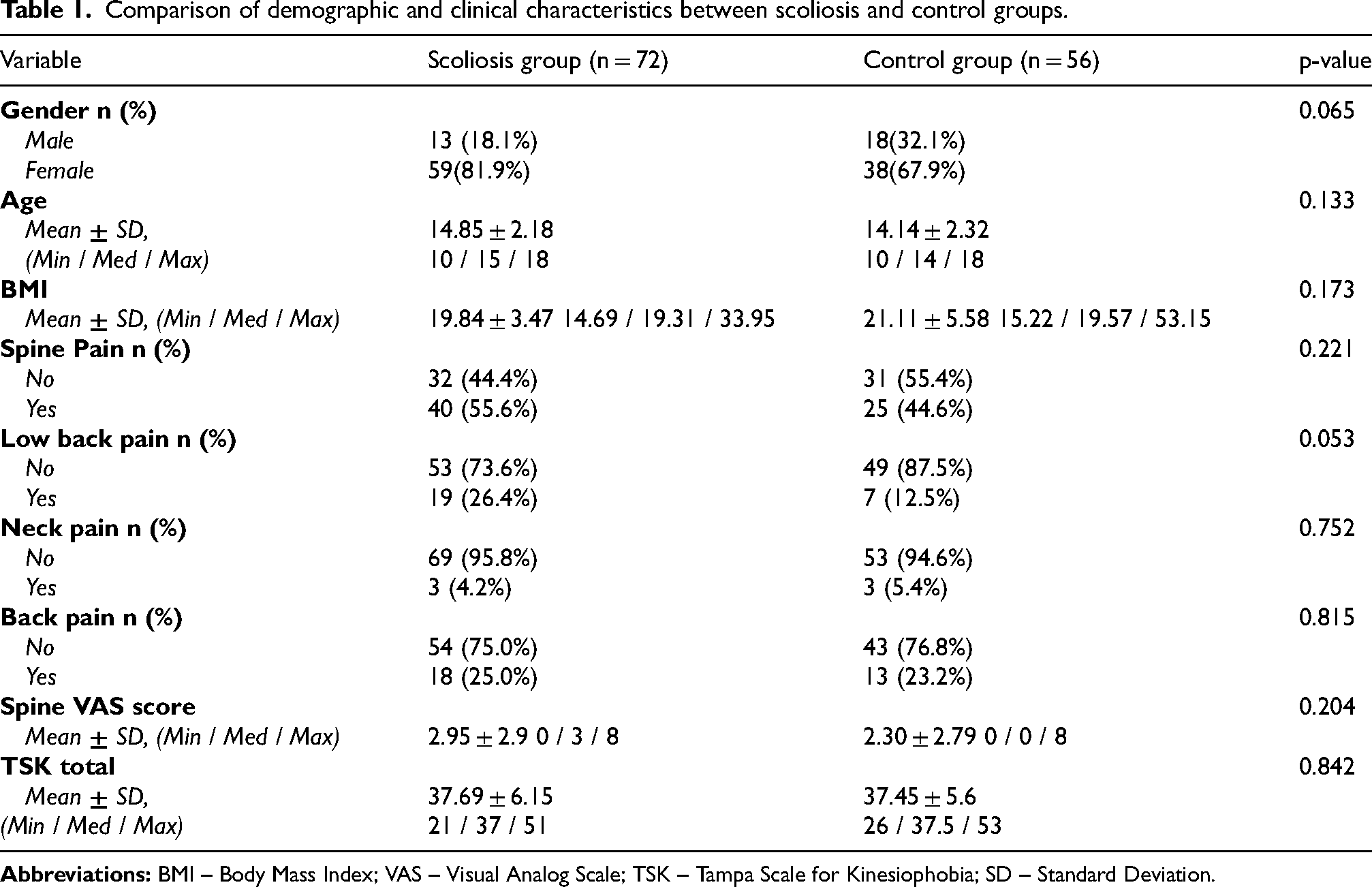
The mean age was 14.85 ± 2.18 years (10–18) in the scoliosis group and 14.14 ± 2.32 years (10–18) in the control group (p = 0.133). No significant difference was observed in BMI values (19.84 ± 3.47 vs. 21.11 ± 5.58; p = 0.173). Regarding pain distribution, spinal pain was reported in 55.6% of the scoliosis group and 44.6% of the control group (p = 0.221). The mean spinal VAS scores were 2.95 ± 2.9 (0–8) in the scoliosis group and 2.30 ± 2.79 (0–8) in the control group, with no significant difference between the groups (p = 0.204). Similarly, TSK total scores were comparable (scoliosis: 37.69 ± 6.15; control: 37.45 ± 5.6; p = 0.842) (Table 1).
Comparison of demographic and clinical characteristics between scoliosis and control groups.
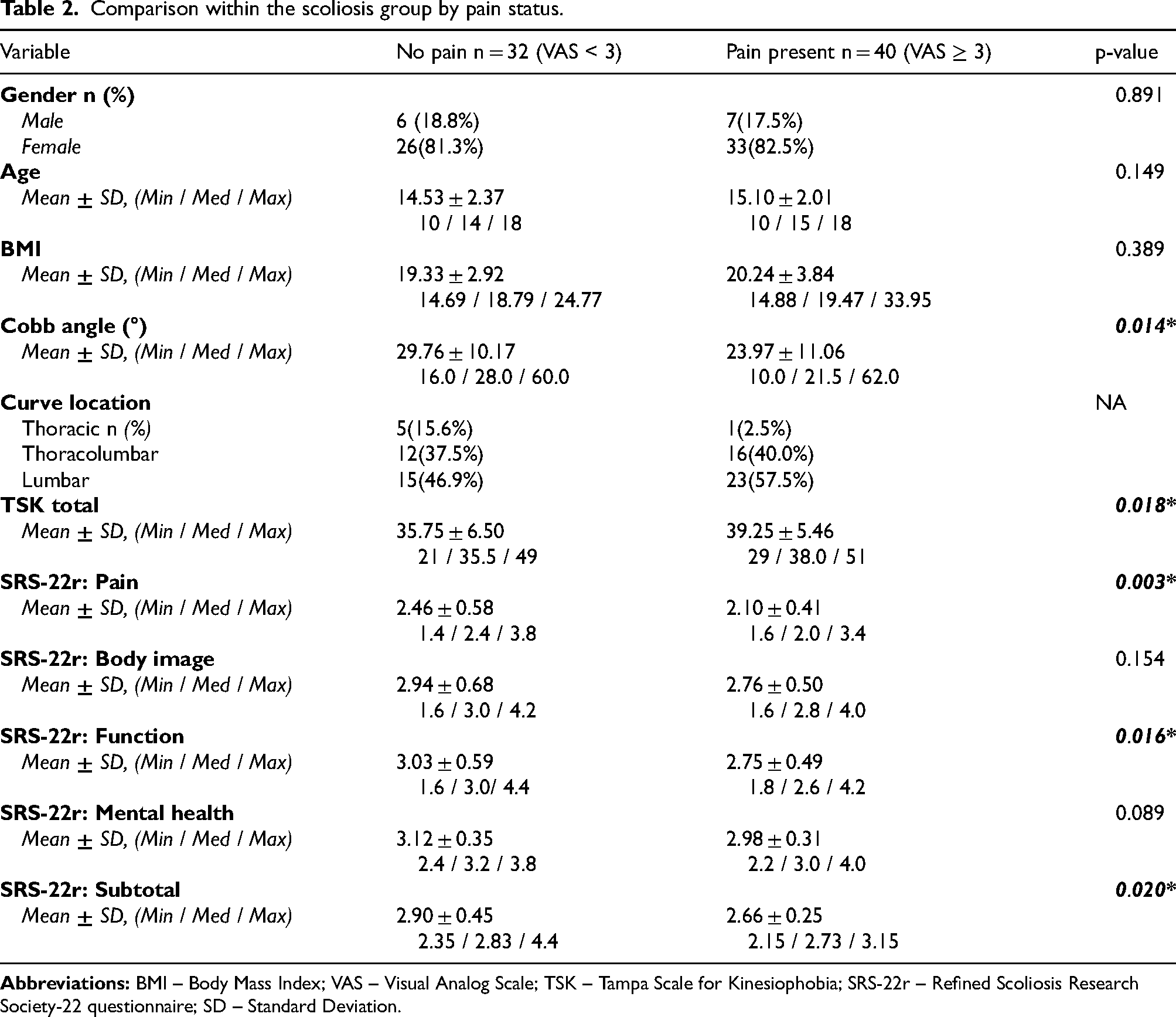
In the scoliosis group, subgroups with pain (VAS ≥ 3, n = 40) and without pain (VAS < 3, n = 32) were compared. No significant differences were found between the groups in terms of gender, age, or BMI (p > 0.05). However, the Cobb angle was significantly higher in the painless group (29.76 ± 10.17° vs. 23.97 ± 11.06°; p = 0.014). The TSK total score was significantly higher in the pain group (39.25 ± 5.46 vs. 35.75 ± 6.50; p = 0.018). Similarly, the SRS-22r pain (2.10 ± 0.41 vs. 2.46 ± 0.58; p = 0.003), function (2.75 ± 0.49 vs. 3.03 ± 0.59; p = 0.016), and subtotal scores (2.66 ± 0.25 vs. 2.90 ± 0.45; p = 0.020) were significantly lower in the pain group. No significant differences were observed in the body image and mental health subscales (p > 0.05) (Table 2). Within the scoliosis group, effect size analysis revealed moderate differences between participants with and without pain. The difference in Cobb angle demonstrated a moderate effect size (Cohen's d = 0.55). Kinesiophobia levels were higher in the pain group, with a moderate effect size for TSK total score (d = 0.58). Regarding health-related quality of life, the SRS-22r pain domain showed a moderate-to-large effect size (d = 0.72), while the function domain (d = 0.51) and subtotal score (d = 0.65) demonstrated moderate effect sizes.
Comparison within the scoliosis group by pain status.
Correlation analyses demonstrated weak-to-moderate positive associations between pain intensity and kinesiophobia. Specifically, VAS scores were weak-to-moderately correlated with TSK total scores in the total sample (r = 0.312, p < 0.001), the scoliosis group (r = 0.340, p = 0.003), and the control group (r = 0.270, p = 0.044) (Figure 1). In the total sample (n = 128), age was positively correlated with VAS (r = 0.310; p < 0.001) and VAS low back score (r = 0.187; p = 0.034). In addition, BMI showed significant correlations with VAS neck (r = 0.243; p = 0.006) and TSK total score (r = 0.214; p = 0.015).
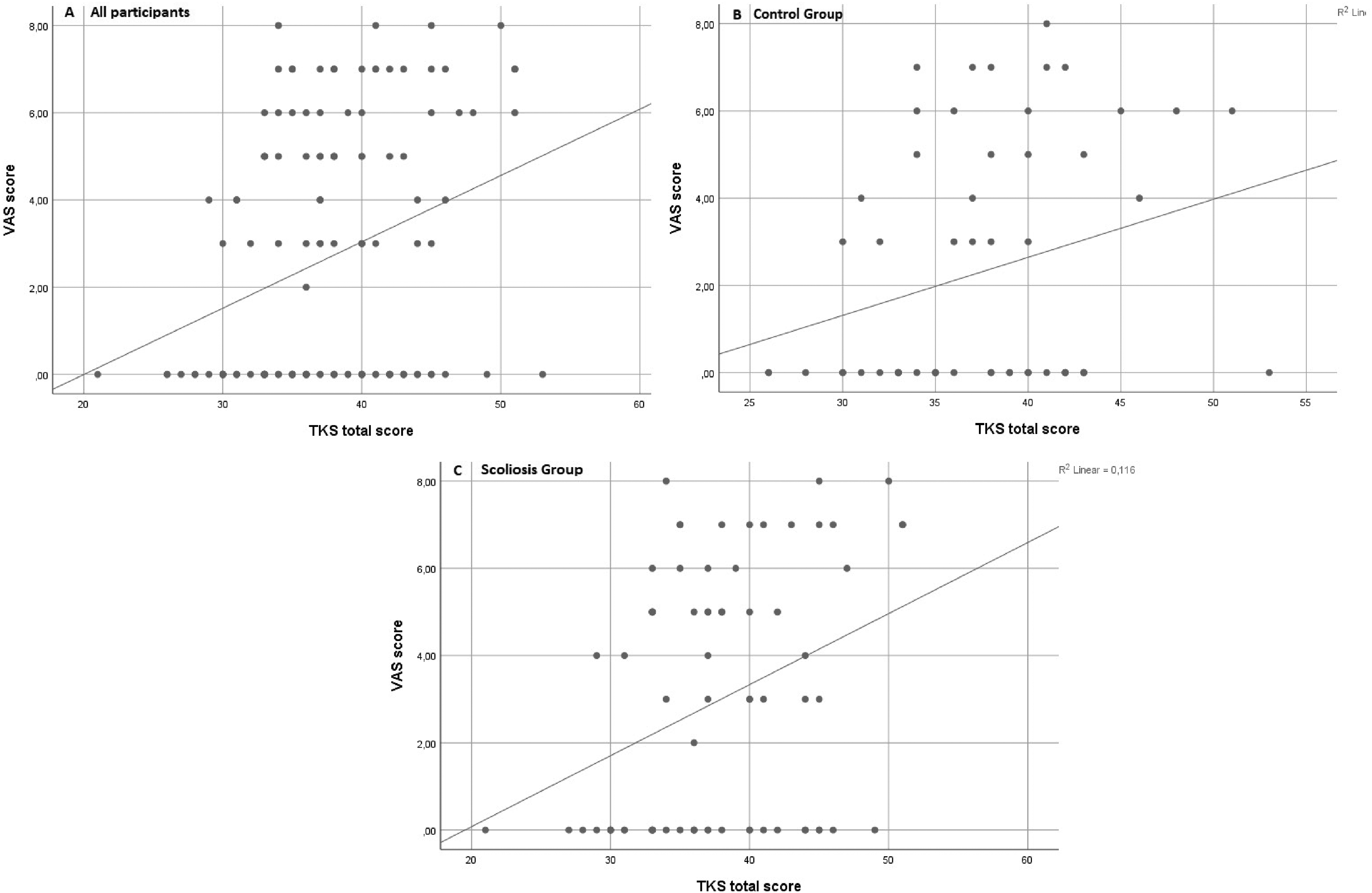
Association between VAS and TSK total scores: (A) all participants, (B) control group, (C) scoliosis group.
In the scoliosis group, age was positively correlated with TSK total score (r = 0.258; p = 0.029), and BMI was associated with VAS neck (r = 0.350; p = 0.003). Furthermore, VAS showed significant positive correlations with VAS score (r = 0.633; p < 0.001), VAS back (r = 0.504; p < 0.001), and TSK total score (r = 0.341; p = 0.003).
In this group, VAS was also negatively correlated with SRS pain (r = –0.426; p < 0.001), function (r = 0.355; p = 0.002), mental health (r = –0.260; p = 0.028), and subtotal score (r = -0.444; p < 0.001). VAS low back score was negatively associated with SRS pain (r = –0.482; p < 0.001), function (r = –0.234; p = 0.048), mental health (r = –0.303; p = 0.010), and subtotal score (r = –0.413; p < 0.001). TSK total score was also significantly negative correlated with SRS pain (r = –0.423; p < 0.001), body image (r = –0.374; p = 0.001), function (r = –0.304; p = 0.009), mental health (r = –0.271; p = 0.021), and subtotal score (r = –0.529; p < 0.001).
In the control group (n = 56), age showed positive correlations with VAS (r = 0.392; p = 0.003), VAS score (r = 0.282; p = 0.035), and VAS neck (r = 0.265; p = 0.049). BMI was positively correlated with TSK total score (r = 0.342; p = 0.010). Moreover, VAS total score was significantly correlated with VAS score (r = 0.388; p = 0.003), VAS neck (r = 0.336; p = 0.011), VAS back (r = 0.597; p < 0.001), and TSK total score (r = 0.270; p = 0.044).
Discussion
In this study, we examined the relationship between pain, kinesiophobia, and functional outcomes in AIS patients. Our results demonstrated that pain was a common finding among adolescents, yet its intensity was not correlated with the degree of spinal deformity (Cobb angle). Instead, both pain and fear of movement appeared to reflect multifactorial interactions involving psychosocial, behavioral, and perceptual components rather than purely structural determinants. The presence of kinesiophobia in this population—independent of curve severity—suggests that psychological responses to pain or the anticipation of pain may play a critical role in shaping activity avoidance and perceived disability. This observation aligns with recent evidence indicating that radiographic parameters poorly explain the intensity of back pain in AIS, and that cognitive-emotional factors such as fear-avoidance beliefs are stronger predictors of physical.5,19–21 These findings highlight the importance of integrating a biopsychosocial framework into the assessment and rehabilitation of adolescents with scoliosis, as addressing kinesiophobia may be as critical as managing the deformity itself.
In our study, the mean Cobb angle was significantly lower in participants who reported spinal pain, which contrasts with some previous findings suggesting that greater spinal deformity is associated with higher pain intensity.3,5 However, other recent reports have shown results consistent with ours. Balagué et al., stated that spinal curvature alone does not reliably explain the occurrence or severity of back pain in AIS population. 22 Similarly, Sarkovich et al., reported that approximately 48% of newly diagnosed AIS patients experienced low back pain, yet no significant correlation was found between pain severity and Cobb angle. 23 These findings, in line with our results, indicate that pain in AIS is not primarily determined by curve magnitude, particularly in mild-to-moderate deformities (mean Cobb angle < 30°), and may instead be influenced by psychosocial and behavioral factors.
In our cohort, age showed a significant positive correlation with TSK scores, suggesting that fear of movement tends to increase with age. This finding is consistent with the results of Figueras et al., who demonstrated that adults with idiopathic scoliosis exhibited higher kinesiophobia scores (mean = 24.2 ± 6.6) compared to adolescents (mean = 21.5 ± 5.9), and that TSK was significantly correlated with pain intensity and depressive symptoms only in the adult group. 11 These results indicate that while kinesiophobia may be weakly expressed during adolescence, it progressively strengthens with increasing age and pain chronicity. Importantly, unlike the study by Figueras et al., which lacked a healthy control group and used an earlier version of the TSK, our study included age-matched healthy participants and applied the validated TSK-17 form. This methodological advantage allowed us to demonstrate more clearly that kinesiophobia is associated with pain experience rather than with the degree of deformity. Moreover, consistent with our findings, Wlazło et al. reported in their umbrella review that higher pain severity was strongly correlated with kinesiophobia across various musculoskeletal disorders, regardless of anatomical localization, emphasizing the central role of pain perception and psychological conditioning in the development of fear of movement. 6
In contrast to our findings, Yagci et al. reported significantly higher kinesiophobia levels in AIS patients compared to healthy controls. However, this discrepancy may primarily stem from methodological differences in the selection of control participants. In their study, the control group consisted exclusively of completely pain-free adolescents with no prior experience of musculoskeletal pain or spinal symptoms. As acknowledged by the authors, their low TSK scores may have reflected a lack of exposure to movement-related fear rather than a genuine absence of kinesiophobia. 24 This issue has also been highlighted in previous psychometric research by Houben et al., who noted that pain experience is essential for meaningful interpretation of TSK responses, since the scale is inherently pain dependent. 16 In contrast, our study included healthy, age-matched individuals who had previously experienced pain but were pain-free at the time of assessment. This methodological approach likely provided a more ecologically valid comparison and a more accurate reflection of kinesiophobia independent of structural deformity.
In the previously mentioned study, untreated AIS exhibited the highest kinesiophobia scores among all subgroups, which the authors attributed to the absence of an active therapeutic process. 24 However, it may also be speculated that fear of movement itself could act as a barrier to initiating treatment, particularly exercise-based interventions. Moreover, since pain intensity was not assessed in their study, it remains unclear whether the presence of pain drove kinesiophobia, the lack of therapy, or psychological avoidance tendencies.
Reduced physical activity is a well-documented phenomenon among adolescents, and this tendency appears to be even more pronounced in those with idiopathic scoliosis. Previous studies have shown that adolescents with scoliosis engage less frequently in sports and recreational activities compared to their healthy peers, largely due to fear of pain, low self-efficacy, and perceived physical limitations.25,26 However, Diarbakerli et al., found comparable overall physical activity levels between patients and healthy controls, suggesting that inactivity in this population may not result solely from structural limitations but could also be influenced by psychological or behavioral factors. 27 In this context, kinesiophobia may represent a key psychological factor contributing to physical inactivity in this population.
Considering that physiotherapeutic scoliosis-specific exercises (PSSE), increasingly recognized as the cornerstone of non-surgical AIS rehabilitation, fear of movement could limit adherence to such therapeutic interventions. Previous studies have shown that kinesiophobia negatively affects participation in exercise-based scoliosis rehabilitation and may lead to poor adherence to PSSE programs. 24 Similarly, a recent scoping review by Fazalbhoy et al. highlighted that adherence to PSSE remains a major challenge in AIS management, influenced by factors such as motivation, self-efficacy, and fear of pain. 28 Recent bibliometric evidence also supports the central role of exercise therapy in AIS rehabilitation, emphasizing that PSSE contribute not only to curve stabilization but also to psychological well-being and quality of life.26–28 Therefore, strategies that address movement-related fear and promote self-confidence in physical activity should be emphasized as part of comprehensive scoliosis rehabilitation, particularly during adolescence—a critical period for behavioral development and body image formation.
In our study, adolescents with scoliosis who reported pain had significantly lower scores on SRS-22r in the pain, function, and subtotal domains, while mental health and body image scores remained comparable between groups. This finding indicates that the negative impact of pain is primarily reflected in functional capacity and daily activity rather than in psychosocial or self-perception domains. Kaya et al., similarly demonstrated that pain intensity was the strongest predictor of reduced SRS-22r function and pain scores, independent of curve magnitude. 19 Consistent with this, Balagué et al., emphasized that pain in AIS is often multifactorial and not directly proportional to Cobb angle severity. 22 The absence of significant differences in mental health and self-image domains in our study may be explained by the relatively mild deformities (mean Cobb < 30°) and shorter symptom duration, suggesting that psychological adaptation mechanisms may still be active during adolescence.
Recent evidence also shows that pain management in AIS remains inconsistent. Théroux et al., reported that although 47% of AIS patients experienced back pain, only about 20% received any structured pain management intervention. 29 Similarly, de Leeuw et al., found that 26% of patients continued to experience pain one year after surgery, often of neuropathic character. 30 These findings highlight the need for more systematic assessment and treatment of pain in this population. Importantly, pain-related functional limitations may further discourage participation in physical activity during this critical developmental period. Previous studies have shown that adolescents with scoliosis tend to engage less in sports and recreational activities, partly due to pain-related fear and reduced self-efficacy.25,26 Therefore, early identification and multidisciplinary management of pain and movement-related fear could help preserve functional well-being and promote healthier activity behaviors.
This study has several limitations. First, the cross-sectional design precludes establishing a causal relationship between kinesiophobia, pain, and functional outcomes. Longitudinal studies are needed to clarify how these variables interact over time. Second, although our sample size was determined through a priori power analysis, all participants were recruited from a single center, which may limit the generalizability of the findings. Third, psychological factors such as anxiety, depression, and coping style were not independently assessed, which could provide a more comprehensive understanding of the biopsychosocial mechanisms underlying pain and fear of movement. Finally, pain was self-reported rather than objectively measured, introducing the possibility of recall bias.
Conclusion
The findings of this study indicate that in AIS population, fear of movement (kinesiophobia) is associated with the experience of pain rather than with the degree of spinal deformity. During adolescence, changes in body image and psychosocial dynamics may increase susceptibility to kinesiophobia, which can negatively influence participation in physical activity, adherence to treatment, and long-term functional outcomes.
AIS management should not focus solely on the magnitude of curvature but should also prioritize early pain control, motivational support, and psychoeducational strategies to reduce fear of movement and support confident participation in exercise from the early phases of treatment, thereby improving overall rehabilitation success.
Footnotes
Acknowledgments
Not applicable.
Ethical considerations
This study was approved by the Ethics Committee of Başakşehir Çam and Sakura City Hospital (Approval number: 2023–654). All procedures involving human participants complied with institutional and national research committee ethical standards.
Consent to participate
Written informed consent to participate was obtained from all adolescents and their parents.
Consent for publication
Not applicable. The manuscript does not contain any identifiable personal data.
Author contributions
Concept: D.F., T.Ş., Design: D.Z.E., D.F., Data collection or processing: D.F., A.A., G.Y.S., Analysis or interpretation: T.Ş., D.Z.E., Literature search: D.F., A.A, G.Y.S., Writing: D.F., T.Ş.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.