
Abstract
Background
Subacromial pain syndrome (SAPS) is a common cause of shoulder pain and is frequently managed with exercise-based rehabilitation. In clinical practice, interventions such as dry needling (DN) and kinesiology taping (KT) are often used alongside exercise programs, although their short-term effectiveness remains unclear.
Objective
To compare the effectiveness of DN, KT, their combination and physical therapy modalities (PTM) when applied alongside exercise therapy in patients with SAPS.
Methods
Eighty adults with SAPS were included in this four-arm randomized controlled trial. Group 1 received KT plus exercise, Group 2 received DN plus exercise, Group 3 received combined DN and KT plus exercise, and Group 4 received PTM plus exercise. Interventions were applied over 3 weeks. Pain intensity and functional disability were assessed at baseline, week 1 and week 3, and kinesiophobia at baseline and week 3. Data were analyzed using Kruskal-Wallis, Friedman, and Wilcoxon signed-rank tests.
Results
Significant within-group improvements in pain, functional disability and kinesiophobia were observed in all groups (p < 0.01). At week 3, reductions in pain were greater in the combined DN and KT group than in the PTM group, while kinesiophobia showed a similar pattern, although improvement in the KT group was comparable to that of the combined group; functional disability improved similarly across groups.
Conclusion
All evaluated interventions were associated with improvement when used as adjuncts to exercise-based rehabilitation. The combination of DN and KT was associated with greater reductions in pain and kinesiophobia than PTM, whereas functional improvement was similar across groups.
Keywords
Introduction
Shoulder pain is a common musculoskeletal complaint, and subacromial pain syndrome (SAPS) is frequently used as an umbrella term for non-traumatic pain arising from the subacromial region. In routine clinical practice, this condition is usually identified according to the pattern of symptoms and findings on shoulder provocation tests rather than on the basis of a single structural diagnosis. Because these patients often present with overlapping clinical features related to rotator cuff–related pain, bursitis, or mechanical impingement, SAPS remains a practical and widely accepted term in rehabilitation research and clinical care.1–3 If no major structural damage is present, conservative multimodal treatment is usually the first-line approach. Conservative management includes exercise therapy (EX), physical therapy modalities (PTM), manual therapy, dry needling (DN), low dose laser therapy, taping methods and subacromial injections. 4
DN is a minimally invasive technique used to reduce pain and functional limitation, although its exact mechanisms remain incompletely understood. Previous evidence suggests that DN may provide short-term benefit in patients with shoulder pain and SAPS.5–9
Kinesiology taping (KT) has often been used in clinical practice as an additional therapeutic resource for treating shoulder pain. KT, also referred to as neuro-proprioceptive taping, is a popular clinical tool theorized to improve proprioception. KT has been proposed to provide a wide range of theoretical benefits, including mimicking the elasticity of skeletal muscle while allowing unrestricted range of motion, improving sensorimotor function, supporting joint alignment, and reducing pain through neurophysiological mechanisms. Despite the widespread application of elastic KT in clinical practice, its scientific effectiveness remains unclear, particularly in patients with shoulder pain. 10
Although KT and DN are both frequently used as adjunctive interventions in the rehabilitation of patients with SAPS, the available literature has mostly evaluated these approaches separately, and their relative short-term effectiveness remains unclear. To our knowledge, no randomized controlled trial has directly compared KT, DN, their combined use, and PTM within the same exercise-based rehabilitation design in patients with clinically diagnosed SAPS. This is clinically relevant because the use of a shared exercise framework allows the adjunctive effects of these interventions to be interpreted more consistently across groups. In addition, although fear of movement is increasingly recognized as a clinically meaningful outcome in musculoskeletal rehabilitation, kinesiophobia has not been evaluated as an outcome in previous interventional studies examining KT- and DN-based treatment strategies in SAPS. Therefore, this study was designed to compare the short-term clinical effects of DN, KT, their combined use, and PTM when applied alongside EX in patients with SAPS. We hypothesized that the combined use of KT and DN would be associated with greater short-term improvement than the other adjunctive interventions.
Material and methods
Design and setting
This study was designed as a prospective, single-blind, four-arm, parallel-group randomized controlled trial with an equal allocation ratio of 1:1:1:1. No changes to the trial design, methods, or outcomes were made after the trial started. The trial was conducted prospectively in a rehabilitation outpatient clinic between June 2021 and June 2022. All procedures were performed in accordance with the Helsinki Declaration. Written informed consent was obtained from all participants. The study was approved by a local institutional clinical research ethics committee (Approval No: 2021/9–4). The study protocol was prospectively registered in the ClinicalTrials.gov registry before the initiation of patient enrollment.
Participants
Patients were screened for eligibility by a physiatrist and invited to participate in the study. Eligible participants were adults with clinically diagnosed SAPS, defined as non-traumatic shoulder pain lasting longer than 6 weeks and localized predominantly to the anterolateral shoulder or upper arm during elevation, together with at least three positive clinical findings among the following: painful arc during flexion or abduction, positive Neer or Hawkins–Kennedy test, pain on resisted external rotation, and a positive Jobe's test.1–3 The term SAPS was preferred because the study population was defined clinically and likely included overlapping subacromial pain presentations rather than a single pathoanatomical impingement subtype. Both male and female patients were eligible for inclusion. In older participants with a possible risk of degenerative shoulder pathology, available prior shoulder radiographs were reviewed together with the clinical findings during screening, and patients with findings suggestive of glenohumeral osteoarthritis were excluded. MRI was performed only when additional diagnostic clarification was clinically required. Exclusion criteria were previous shoulder surgery, physical or injection therapy within the last 3 months, contracture, tendon rupture, cervical radiculopathy, systemic inflammatory disease, allergy, bleeding tendency, local infection or wound, cognitive impairment interfering with cooperation, malignancy, and clinical or imaging findings suggestive of glenohumeral osteoarthritis.
Randomization
The randomization sequence was generated using a computer-based random number generator with permuted block randomization to ensure balanced allocation across the four study groups. Randomly permuted block sizes of 4 and 8 were used. Allocation concealment was achieved using sequentially numbered, opaque, sealed envelopes prepared by an independent researcher not involved in participant recruitment or intervention. The same physiatrist enrolled participants and assigned them to the intervention groups. Participants were allocated in an equal 1:1:1:1 ratio. No stratification factors were used.
Interventions
A four-arm intervention design was used. In Group 1, KT was applied once per week across three sessions, Group 2 received DN twice per week for three weeks, and Group 3 received both interventions following the same schedules as Groups 1 and 2. Group 4 underwent conventional PTM combined with supervised exercise five times per week for three weeks (Figure 1).
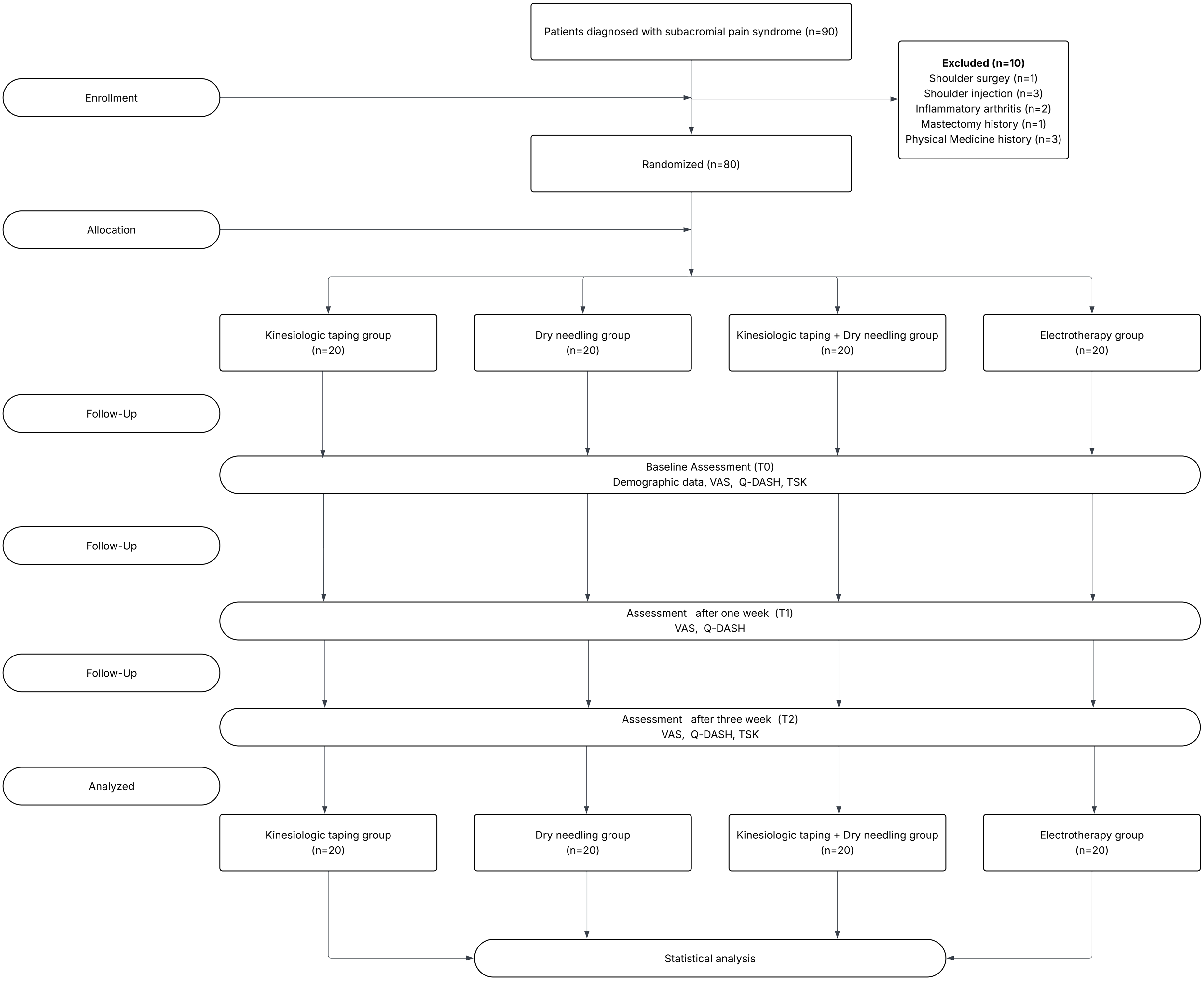
CONSORT flow diagram of participant recruitment, allocation, follow-up, and analysis.
Patients in Group 1 received KT after baseline assessment and skin allergy screening. A standard 5-cm Kinesio Tex tape was used. The taping protocol consisted of sequential application to the supraspinatus, deltoid and glenohumeral joint regions using Y- and I-strips with paper-off tension (approximately 20%–25% stretch), in line with commonly described shoulder taping applications. 11 The tape was intended to remain in place for approximately 3–5 days unless early detachment or skin irritation occurred, and it was reapplied weekly during the 3-week intervention period. The protocol used in the study is illustrated in Figure 2.
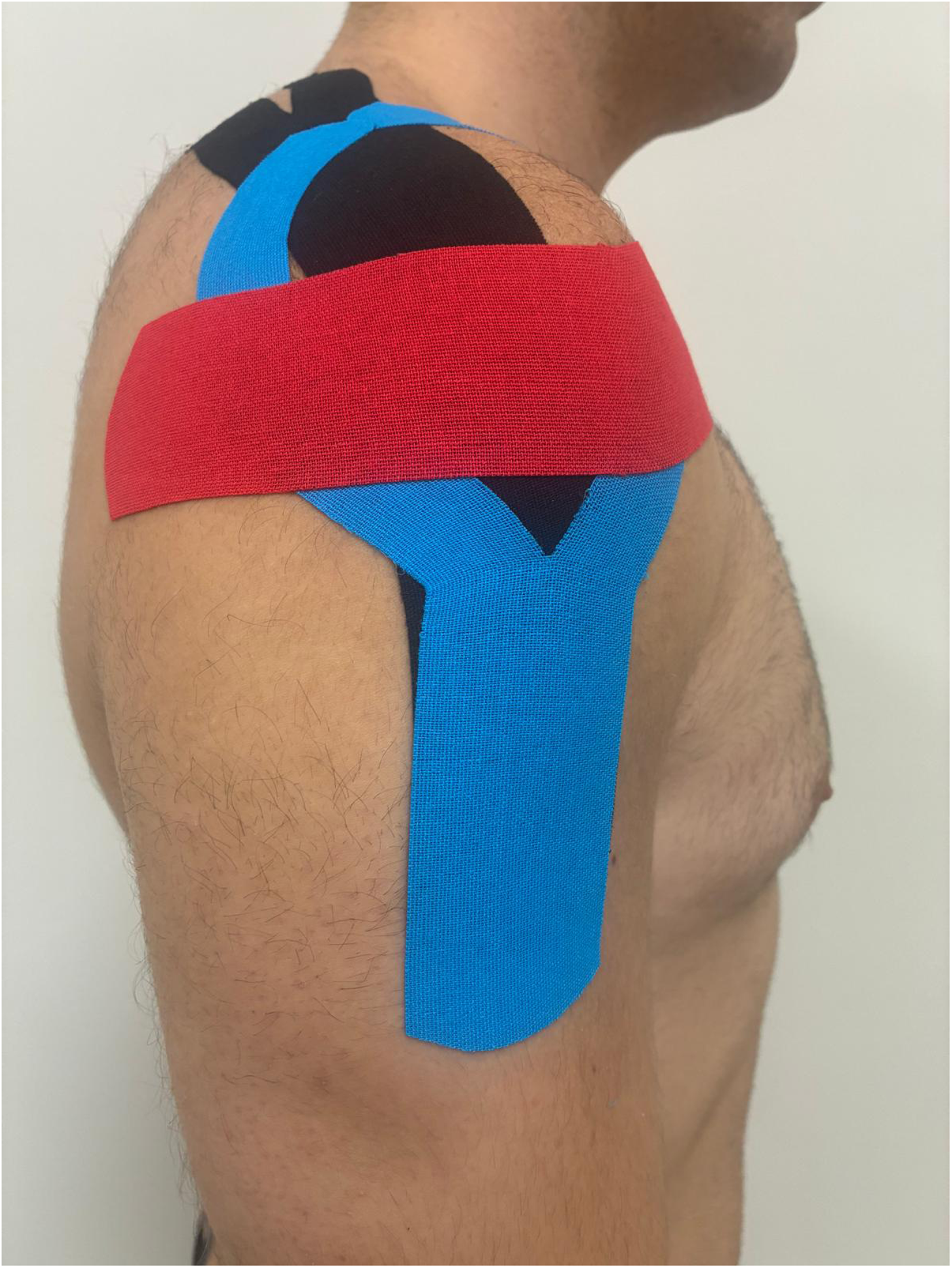
Application of the kinesiology taping technique used in the study. The taping protocol consisted of sequential application over the supraspinatus, deltoid, and glenohumeral joint regions using standard 5-cm Kinesio® Tex tape. (A) Supraspinatus: Y-strip applied from the insertion at the greater tubercle along the muscle belly toward its origin with approximately 20–25% stretch. (B) Deltoid: Y-strip placed from 3 cm below the deltoid insertion, with anterior and posterior tails applied along the corresponding muscle fibers. (C) Glenohumeral joint: I-strip applied from the coracoid process, extending laterally beneath the acromion and around the posterior deltoid edge to support joint alignment.
Patients in Group 2 received DN with disposable 0.25 mm × 25 mm stainless-steel needles that were inserted into the skin over taut bands of the upper trapezius, infraspinatus, supraspinatus and deltoid muscles. In the current study, the fast-in and fast-out technique described by Hong was applied.7,12 This technique consists of repeated short vertical needle movements within the muscle after insertion into the trigger point region and elicitation of a local twitch response. Once the most painful spot had been identified within a palpable taut band with pincer palpation within the upper trapezius or pectoralis major, or with flat palpation in the infraspinatus or subscapularis muscles. The needle was inserted, penetrating the skin to a depth of about 15–20 mm, until the first local twitch response (LTR) was obtained. Once the first LTR was obtained, the needle was then moved up and down (5 to 10 mm vertical motions with no rotation) in the muscle at approximately 1 Hz for 25–30 s. This procedure was done twice per week for three weeks. The DN procedure used in the study is illustrated in Figure 3.
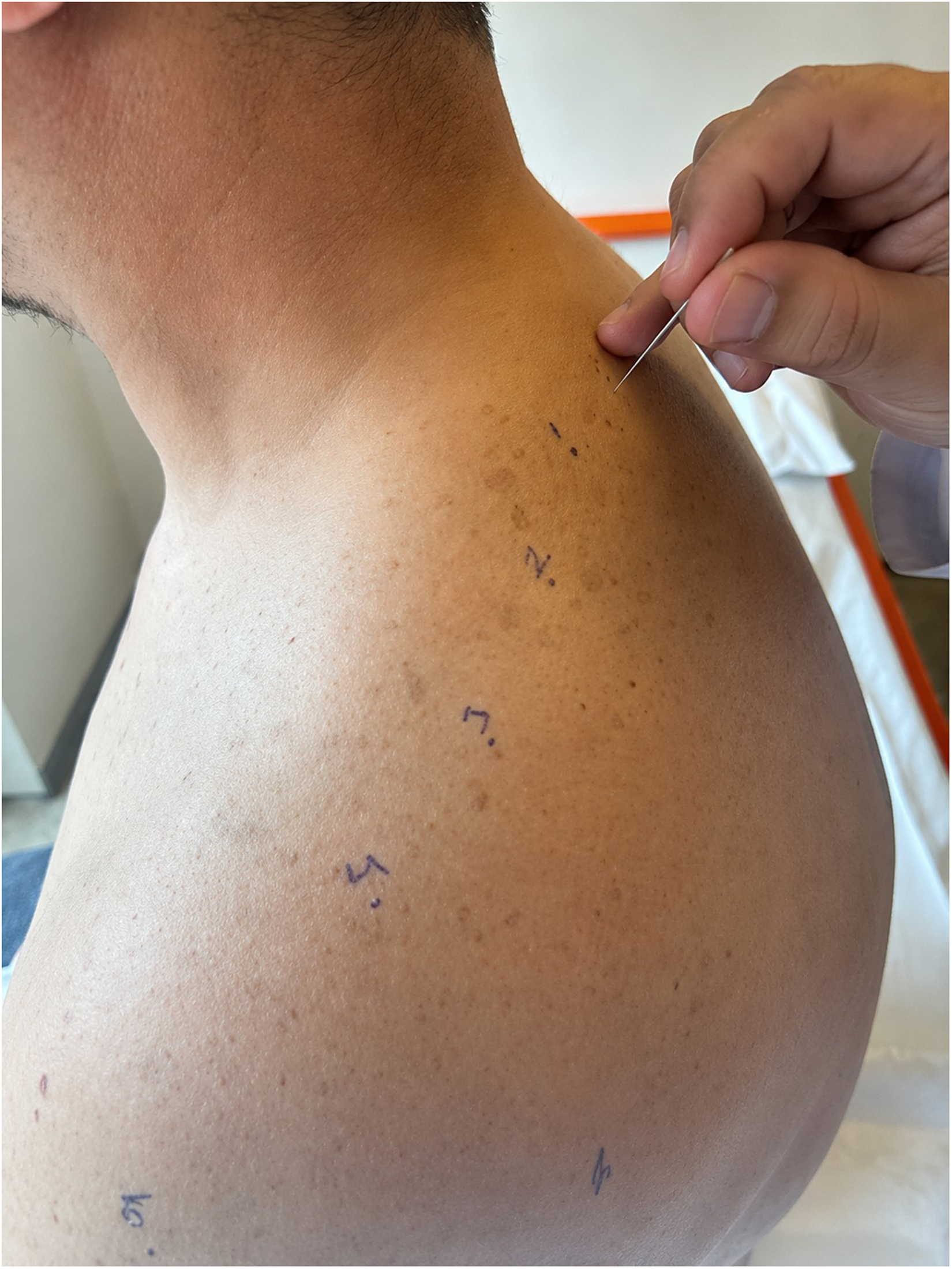
Dry needling procedure used in the study. Representative image showing dry needling applied to marked taut bands.
Combined intervention group: Patients in Group 3 received DN according to the same protocol as in Group 2. Immediately after completion of the DN procedure, KT was applied in the same treatment session according to the protocol used in Group 1. Accordingly, DN was not performed with the tape in situ.
Group 4 patients received conventional PTM consisting of transcutaneous electrical nerve stimulation (TENS), therapeutic ultrasound, and superficial heat therapy. TENS was applied to the painful shoulder region using a frequency of 80–100 Hz and a pulse width of 100–150 µs for 20 min. Therapeutic ultrasound was applied to the subacromial/anterior shoulder region at 1 MHz and 1.0–1.5 W/cm2 in continuous mode for 5–7 min. A hot pack was applied over the shoulder region for 15–20 min. In addition, passive mobilization toward end range and scapular stabilization training were provided. PTM was administered 5 days per week for 3 weeks.
Exercise program (all groups): All participants received a standardized home-based and therapist-supervised exercise program including pendulum exercises, active-assisted range-of-motion exercises, posterior capsule stretching, scapular stabilization, and rotator cuff strengthening. Exercises were performed daily with 10–15 repetitions per movement.
The 3-week intervention period was selected to reflect a short-term outpatient rehabilitation schedule commonly used in routine musculoskeletal practice and to evaluate early clinical response to adjunctive treatment in patients with shoulder pain.13,14 KT and DN were applied by two separate physiatrists with >5 years of clinical experience in managing shoulder disorders and certified training in DN and KT.
Outcome measurements
The primary endpoint of the trial was the change in pain intensity (VAS) from baseline to week 3. Secondary outcomes were upper-extremity functional disability evaluated with the short version of the Disabilities of the Arm, Shoulder and Hand Questionnaire (Q-DASH) and kinesiophobia measured with the Turkish version of the Tampa Scale of Kinesiophobia (TSK). Pain intensity and functional disability were assessed at baseline, week 1, and week 3 to evaluate early and short-term clinical response by the same blinded assessor, whereas kinesiophobia was assessed at baseline and week 3 because it was intended to reflect short-term change in fear of movement rather than immediate symptom response. No changes were made to the outcome measures after the trial started. Pain intensity was assessed using a visual analog scale (VAS), a widely used valid, and reliable measure of subjective pain intensity in clinical pain research. Participants rated their average shoulder pain during the preceding week on a 0–100 scale, with higher scores indicating greater pain. 15 Q-DASH was used to assess the patient's shoulder function. The questionnaire was applied face-to-face to all patients. The Q-DASH is a self-report questionnaire developed to evaluate upper extremity disability and symptoms. High scores on the Q-DASH indicate greater disability and disease severity. The maximum score on the test is 100 and represents the most severe level of disability. 16 The Turkish version of the Q-DASH has been shown to be valid, reliable, and culturally adapted for clinical use. 17 Kinesiophobia was measured with the TSK. This self-administered questionnaire consists of 17 items with a 4-point Likert scale. The score range is 17–68 (a higher score indicates a greater fear of re-injury from movement). The Turkish version of the TSK has been shown to be a reliable instrument for clinical assessment. 18 All questionnaires were administered face-to-face under assessor supervision, and outcome assessments were performed at the same predefined time points in all groups.
Blinding
The outcome assessor remained blinded throughout the trial. Allocation concealment was ensured using sequentially numbered, opaque, sealed envelopes prepared by an independent researcher who was not involved in participant recruitment, treatment administration, or outcome assessment. Because of the distinct appearance and procedural characteristics of the interventions, blinding of participants and treating clinicians was not feasible. To reduce potential performance bias, the interventions were delivered by experienced physiatrists with certified training in their respective techniques.
Statistical analysis
The sample size was determined before data collection using VAS pain intensity as the primary outcome. The assumed between-group difference was based on previously reported minimal clinically important differences for pain intensity in patients with rotator cuff–related shoulder disorders. Based on previous reports,19,20 a minimum clinically important difference of 3 points and a standard deviation of 4 points were assumed. With α = 0.05 and power at 80%, at least 20 participants were required in each group; allowing for an anticipated 10% dropout, the target sample size was set at 80. No interim analyses or stopping rules were planned.
All statistical analyses were performed using SPSS (version 22.0; IBM Corp., Armonk, NY, USA). The Shapiro-Wilk test was used to assess normality. Because most continuous variables were not normally distributed, continuous data were summarized as median (interquartile range [IQR]), and nonparametric tests were used for analysis. Categorical variables were presented as number (n), as appropriate. Because the sample size within each treatment arm was relatively small, a mixed-design ANOVA was not selected as the primary analytical approach. Instead, nonparametric methods were used to evaluate within-group changes over time and between-group differences at each assessment point. Between-group differences were analyzed using the Kruskal–Wallis test at each assessment point (and for change scores where applicable), whereas within-group changes over time were analyzed using the Friedman test. When the Friedman test was significant, post hoc pairwise comparisons were performed with the Wilcoxon signed-rank test using Bonferroni adjustment. Categorical data were compared using the chi-square test. Missing data were handled by complete-case analysis, and no imputation methods were applied. Because there were no missing data, per-protocol and intention-to-treat analyses were identical. No subgroup or adjusted analyses were performed. This analytical strategy did not directly evaluate the group × time interaction and should therefore be interpreted as a nonparametric assessment of within-group change and between-group differences at individual time points.
Results
Participant flow
A total of 90 patients with SAPS were assessed for eligibility. Ten patients were excluded for not meeting the inclusion criteria (shoulder surgery, n = 1; prior shoulder injection, n = 3; inflammatory arthritis, n = 2; history of mastectomy, n = 1; prior physical medicine treatment, n = 3). Remaining 80 cases were equally randomized into four groups (n = 20 per group): KT, DN, combined KT + DN, and PTM. All patients completed treatments and assessment sessions (T0, T1, and T2). There was no loss to follow-up, and all participants were included in the final analyses. The participant flow diagram is presented in Figure 1.
Baseline characteristics
Participants were recruited from the Physical Medicine and Rehabilitation outpatient clinic between 25 May 2021 and 25 May 2022. All follow-up assessments were completed in the same period. Analyses of the four groups revealed no statistically significant differences in baseline demographic or clinical characteristics, including age, sex distribution, body mass index, symptom duration, and baseline VAS, Q-DASH, and TSK scores (all p > 0.05). Table 1 summarizes the baseline demographic and clinical characteristics of the groups.
Baseline demographic and clinical characteristics of the study groups.
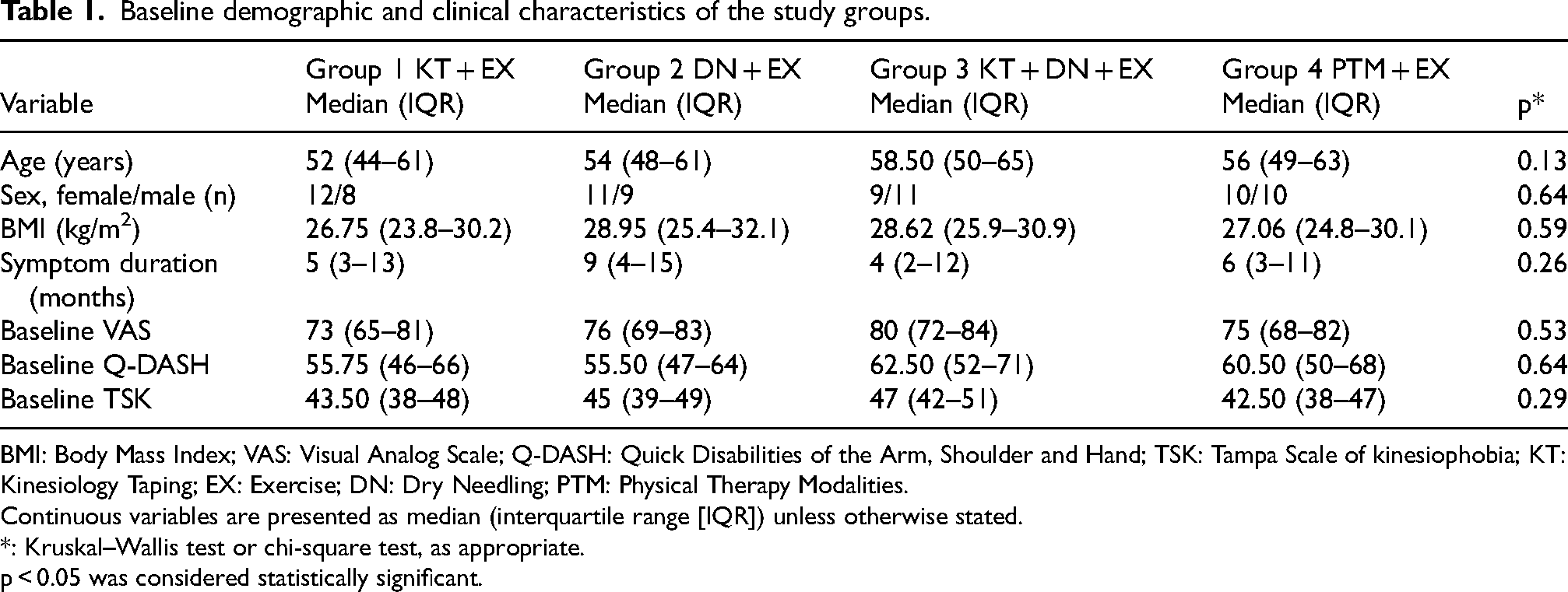
BMI: Body Mass Index; VAS: Visual Analog Scale; Q-DASH: Quick Disabilities of the Arm, Shoulder and Hand; TSK: Tampa Scale of kinesiophobia; KT: Kinesiology Taping; EX: Exercise; DN: Dry Needling; PTM: Physical Therapy Modalities.
Continuous variables are presented as median (interquartile range [IQR]) unless otherwise stated.
*: Kruskal–Wallis test or chi-square test, as appropriate.
p < 0.05 was considered statistically significant.
Clinical outcomes
Across all groups, pain, functional disability and kinesiophobia improved over time, indicating overall clinical improvement in all treatment arms. Pain, functional disability and kinesiophobia scores at baseline and during follow-up are presented in Table 2.
Pain, functional disability, and kinesiophobia scores across groups at baseline, week 1, and week 3.
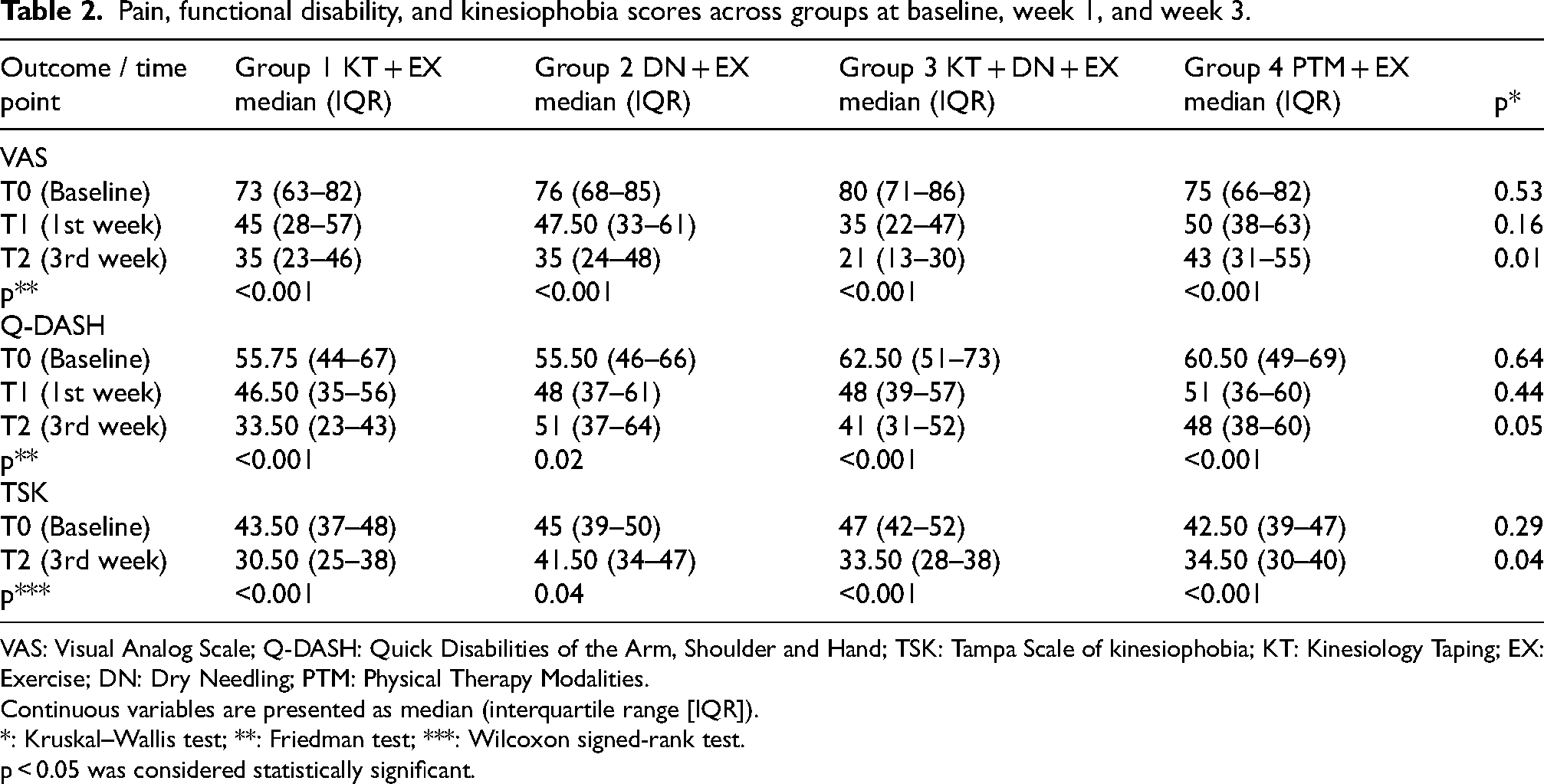
VAS: Visual Analog Scale; Q-DASH: Quick Disabilities of the Arm, Shoulder and Hand; TSK: Tampa Scale of kinesiophobia; KT: Kinesiology Taping; EX: Exercise; DN: Dry Needling; PTM: Physical Therapy Modalities.
Continuous variables are presented as median (interquartile range [IQR]).
*: Kruskal–Wallis test; **: Friedman test; ***: Wilcoxon signed-rank test.
p < 0.05 was considered statistically significant.
Statistically significant within-group changes over time were observed in pain intensity, functional disability, and kinesiophobia in all groups (Table 3). At week 1, no significant between-group differences were observed. At week 3, between-group differences were observed for pain intensity and kinesiophobia. In particular, greater reductions in pain intensity and kinesiophobia were observed in the combined KT + DN + EX group than in the PTM + EX group at the final assessment. However, for kinesiophobia, the improvement observed in the KT + EX group was similar to that in the combined group, suggesting that the advantage of the combined intervention was less clear for this outcome.
Changes in pain, functional disability, and kinesiophobia scores from baseline across treatment groups.
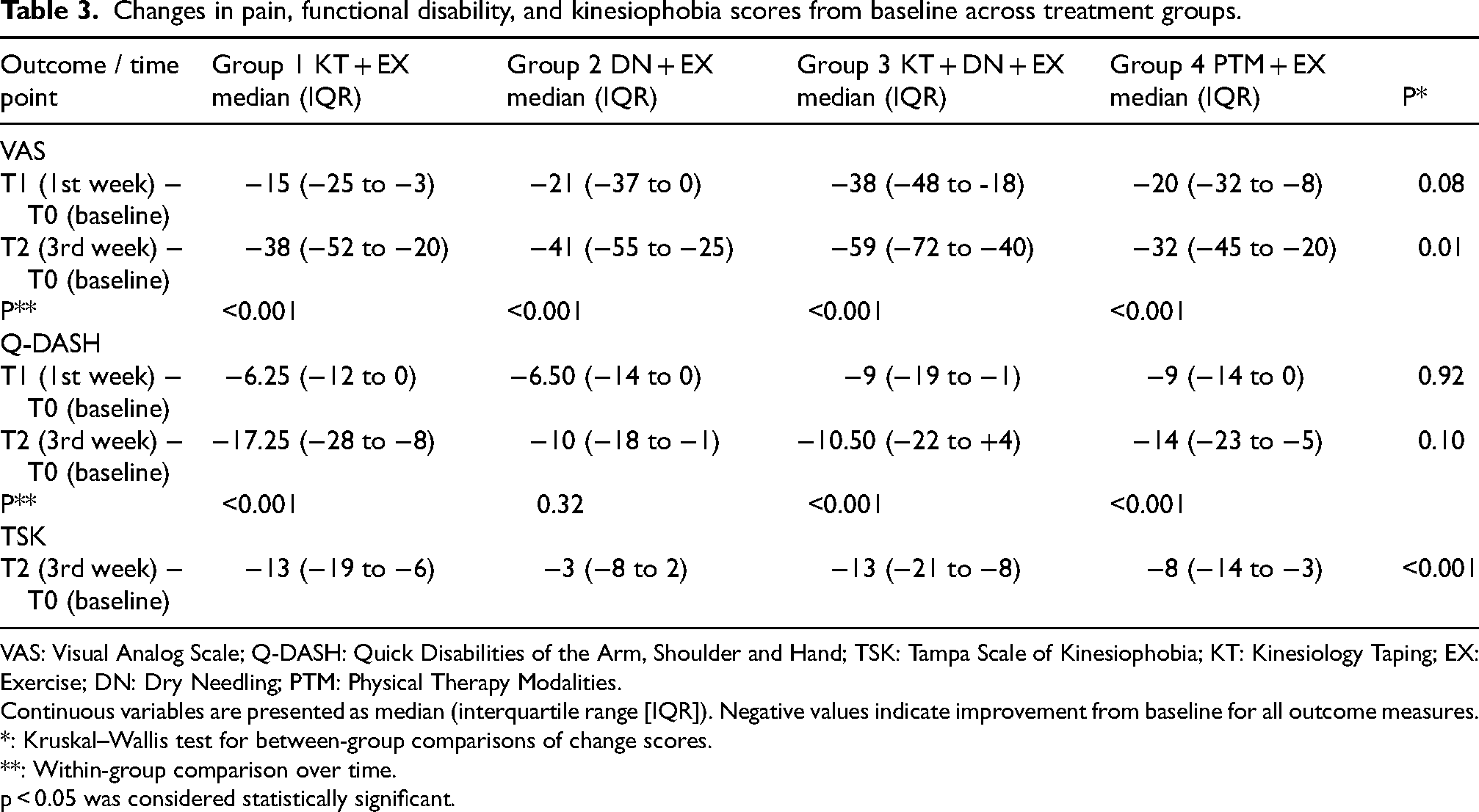
VAS: Visual Analog Scale; Q-DASH: Quick Disabilities of the Arm, Shoulder and Hand; TSK: Tampa Scale of Kinesiophobia; KT: Kinesiology Taping; EX: Exercise; DN: Dry Needling; PTM: Physical Therapy Modalities.
Continuous variables are presented as median (interquartile range [IQR]). Negative values indicate improvement from baseline for all outcome measures.
*: Kruskal–Wallis test for between-group comparisons of change scores.
**: Within-group comparison over time.
p < 0.05 was considered statistically significant.
Between-group differences in QuickDASH scores were not statistically significant at week 3. Functional disability improved over time in all groups. Overall, all groups showed improvement over time, while between-group differences at week 3 were observed for pain intensity and kinesiophobia.
No subgroup analyses, adjusted analyses or other exploratory analyses were performed. All findings presented in this study derive from the predefined primary and secondary outcome analyses. No adverse events, complications or treatment-related harms were reported in any of the intervention groups during the study period.
Discussion
This study was designed to compare the short-term clinical effects of KT, DN, their combined use, and PTM when applied alongside EX in patients with SAPS. The main findings were that all intervention groups showed short-term improvement. The combined KT + DN approach was associated with greater reductions in pain and kinesiophobia than PTM + EX at week 3, whereas functional disability improved in all groups without a significant between-group difference. Overall, these findings provide partial support for our hypothesis, particularly for pain and kinesiophobia, but not for functional disability.
In the present study, the short-term effects of KT, DN, and their combination, each applied alongside exercise therapy, were evaluated clinically. All interventions were associated with short-term clinical improvement when combined with exercise therapy. The comparative advantage of the combined intervention was more evident against PTM + EX than against KT + EX, particularly for kinesiophobia. In contrast, improvements in functional status were comparable across treatment groups. These findings should be interpreted as short-term comparative clinical observations within the context of the analytical approach used, rather than as definitive evidence of superiority of one intervention over another. This pattern was most evident for pain intensity, which showed the clearest short-term between-group difference in favor of the combined intervention. Importantly, the observed reductions in pain were consistent with changes generally considered clinically meaningful in patients with rotator cuff–related shoulder disorders.
In the physiotherapeutic management of shoulder disorders, treatment is commonly expected to begin with pain relief, followed by restoration of shoulder mobility and movement control. Subsequently, interventions aim to reestablish normal movement patterns and the scapulohumeral rhythm, ultimately progressing to a gradual increase in the range of active motion. 21 Exercises assisted by a physiotherapist have been identified as a critical component of treatment. 22 Nonetheless, the overall effectiveness of emerging adjunctive techniques continues to be investigated. In this study, two interventions were selected in accordance with these principles. Both were designed to provide rapid pain relief and promote neuromuscular reorganization, thereby enabling the initiation of therapeutic exercises at the outset of treatment. The first intervention was DN. A systematic review conducted by Blanco-Diaz et al. evaluated the effectiveness of DN combined with physiotherapy in the management of patients with SAPS. 9 However, this review did not include a meta-analysis. Accordingly, the present study was designed to extend the available evidence by directly comparing DN, KT, their combined use, and PTM within the same exercise-based rehabilitation framework in patients with SAPS.
Although DN is commonly associated with the management of myofascial pain, its use in SAPS may be justified by the frequent coexistence of myofascial trigger points and secondary muscle dysfunction in patients with rotator cuff–related shoulder disorders. The therapeutic effects of DN may also involve neurophysiological modulation and changes in the local tissue environment. The study was not designed to differentiate between nociceptive, myofascial or referred components of shoulder pain; therefore, the observed effects of DN should be interpreted within the context of multimodal pain mechanisms contributing to SAPS.7,8
KT was the second adjunctive intervention considered in relation to short-term pain relief, which differs from conventional athletic tapes because of its elastic material, capable of stretching up to 140% of its original length. It can remain on the skin for 4 to 5 days and demonstrates water resistance. In this study, the applied techniques likely provided support to the superficial fascia, facilitated glenohumeral joint alignment, and offered ligamentous support. Comparative studies have demonstrated that KT is more effective than sham taping in reducing activity-related pain in the short term.11,23 The findings from our study demonstrated significant short-term improvements in pain among patients receiving KT, consistent with previous reports comparing KT with conventional PTM. These results highlight KT as a promising intervention for short-term pain relief. Previous studies have also suggested that KT may contribute to pain relief through sensorimotor support and improved shoulder mechanics.11,24,25 Rundquist and Johnson showed that the application of KT led to significant changes in scapular kinematics during humerothoracic elevation and lowering. 26 Consequently, this form of shoulder support may have contributed to pain reduction in the participants.
With respect to functional outcomes, all treatment groups showed short-term improvement, but no significant between-group difference was observed. Similarly, no significant difference was found between the KT and DN groups in pain control. A study comparing KT and DN for myofascial pain reported no significant difference between the two treatments. 27 Additionally, Hayta and Umdu reported that both KT and DN were effective in improving pain and function for up to 12 weeks post-treatment, although DN demonstrated greater improvement in quality of life. 28 Conversely, another study found KT to be superior to DN in terms of pain reduction and functional improvement in patients with mechanical neck pain. 29 These findings suggest that the effectiveness of KT and DN may vary depending on the specific diagnosis. The differing mechanisms proposed for KT and DN may partly explain why their relative clinical effects appear to vary across pain conditions and diagnostic groups. 30
Functional disability improved in all groups, and Q-DASH outcomes were comparable across treatment arms. This suggests that reductions in pain may have supported participation in the exercise program, contributing to functional improvement regardless of the adjunctive intervention used. EX was provided to all participants as a shared component of treatment. The study was not designed to evaluate exercise in isolation but rather to examine the influence of additional interventions on short-term outcomes in the context of a standardized exercise program. Taken together, these findings highlight the central role of exercise in functional recovery.
Kinesiophobia, which affects between 51% and 72% of patients with chronic pain,31–33 promotes hypervigilance and exacerbates disability, consequently increasing pain perception. Since physical exercise plays a major role in rehabilitation, identifying and reducing kinesiophobia is important to prevent poor treatment adherence. Previous studies have highlighted the importance of reducing fear of movement in chronic pain rehabilitation through interventions such as exercise, pain education, and manual therapy.34–38
Kinesiophobia improved in all groups, supporting the clinical relevance of fear of movement as an outcome in shoulder rehabilitation. Among the evaluated approaches, the combined intervention was associated with a greater reduction in kinesiophobia at week 3 than PTM + EX. However, the improvement observed in the KT group was similar to that in the combined group, suggesting that the comparative advantage of the combined intervention for this outcome was less distinct. This pattern may suggest that the additional short-term pain relief associated with the combined intervention did not translate into a clearly greater reduction in fear of movement beyond that achieved with kinesiology taping plus exercise. These findings remain clinically meaningful because fear of movement may influence participation in rehabilitation and response to exercise-based treatment.
Further research is warranted to confirm and extend these findings. Future studies should incorporate longer follow-up periods, more detailed structural characterization of the shoulder, and analytical approaches that better account for repeated measurements over time. Future research should also consider factors such as cost-effectiveness, treatment accessibility, and patient preferences to provide a more comprehensive understanding of the practical role of DN and KT protocols in SAPS. Such considerations may help guide more individualized and evidence-informed clinical decision-making.
Limitations
This study has several limitations that should be considered when interpreting the findings. The follow-up period was relatively short and focused on early symptom changes during the initial phase of an exercise-based rehabilitation program, which limits conclusions about the persistence of treatment effects over time. Blinding of patients and physiatrists was not feasible because of the nature of the interventions and may have influenced treatment responses. The absence of an exercise-only control group means that the effects of the adjunctive interventions cannot be fully separated from those of exercise. This was a deliberate decision, as EX reflects routine clinical practice in patients with SAPS. Although MRI was used when clinically indicated, it was not performed systematically in all participants, which may have introduced some variability in diagnostic verification. Because the nonparametric analytical approach used in this study did not directly test the group × time interaction, differences in treatment response over time between interventions should be interpreted with caution. The differing treatment frequencies across groups should also be considered when interpreting the comparative effects of the interventions, as treatment burden and therapist contact may have contributed in part to the observed between-group differences. The relatively broad age distribution may also have increased clinical heterogeneity, including the possibility of unrecognized underlying structural shoulder pathology, despite predefined exclusion criteria, clinical screening, and selective use of imaging when additional diagnostic clarification was required. In addition, the single-center design and relatively homogeneous study population may limit the generalizability of the results. Despite these limitations, the findings offer relevant insight into short-term clinical effects during the early rehabilitation period.
Generalizability
Because the study was conducted at a single center and involved a relatively homogeneous patient population, generalizability to broader or more diverse clinical settings should be interpreted with some caution. Nevertheless, interventions such as KT, DN, and PTM are widely used in routine musculoskeletal rehabilitation, which supports the practical applicability of the results in comparable clinical environments.
Interpretation
Despite the short follow-up period and single-center design, the findings provide preliminary comparative evidence regarding the short-term effects of KT, DN, and their combined use when applied alongside EX in patients with SAPS. In particular, the findings support the potential role of these approaches as adjunctive components of multimodal rehabilitation rather than as alternatives to exercise-based treatment.
Conclusion
In patients with clinically diagnosed SAPS undergoing exercise-based rehabilitation, all adjunctive interventions were associated with short-term improvement. The combined DN + KT approach was associated with greater reductions in pain and kinesiophobia than PTM + EX, whereas functional improvement was comparable across groups. These findings suggest that DN and KT may be considered supportive adjuncts within multimodal rehabilitation rather than alternatives to exercise-based treatment. Further studies with longer follow-up are needed to determine whether these effects are maintained over time.
Footnotes
Ethical approval and ınformed consent
This study was approved by the Bursa City Hospital Clinical Research Ethics Committee (Approval No: 2021/9–4). All procedures were conducted in accordance with the Declaration of Helsinki, and written informed consent was obtained from all participants prior to inclusion.
Consent to participate
Written informed consent to participate was obtained from all participants prior to inclusion in the study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest related to this work.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.