
Abstract
Background
Fine motor impairment is common in Huntington's disease (HD). Neurologic Music Therapy (NMT) is the therapeutic application of music for neurorehabilitation. Measured by magnetoencephalography (MEG), the modulation of motor-related oscillations via NMT is associated with restorative motor training. In HD, the impact of NMT on fine motor function and associated neurophysiology have yet to be explored.
Objective
Conduct a proof-of-concept study to determine the feasibility of NMT and MEG evaluation in people with HD.
Methods
Three participants with HD and impaired fine motor skills underwent a five-week NMT intervention. Pre- and post-intervention assessments included the Unified HD Rating Scale, the Grooved Pegboard Test, and MEG recording during a cued finger-tapping task.
Results
There was 100% adherence to the pre and post visit assessments and MEG, and 93% adherence to the NMT intervention. A visual increase in evoked beta/gamma power at cue onset along with an earlier evoked beta response at 500–800 msec post cue were observed in the neuromagnetic data after NMT.
Conclusion
NMT-based fine motor rehabilitation, and its evaluation with neurophysiological studies, are feasible in HD. More work is needed to determine if this intervention holds potential to influence functional change or spectral patterns of motor cortical activity.
Introduction
Huntington's disease (HD) is an inherited and autosomal dominant disorder caused by an expansion in CAG repeats in the HTT gene, leading to a relentlessly progressive neurodegenerative disorder characterized by motor dysfunction, cognitive impairment, and neuropsychiatric disturbances (Bates et al., 2015). Motor symptoms occur on a spectrum from hyperkinetic chorea to hypokinetic parkinsonism, both of which affect fine motor skills (Bates et al., 2015). Fine motor impairments can be associated with bradykinesia, rigidity, incoordination, chorea, or dystonia. Currently, there are no disease modifying treatments for HD (Bachoud-Lévi et al. 2019; Ross & Tabrizi, 2011). As a result, individuals with HD often experience difficulties with fine motor tasks due to the disease itself and potentially from symptomatic treatments aimed at decreasing chorea.
Neurologic Music Therapy (NMT) is an evidence-based clinical approach that has proven benefit for motor rehabilitation in patients with a spectrum of neurologic disorders (Thaut & Hoemberg, 2014), however in HD most studies yielded limited data regarding the impact on fine motor function (Schwartz et al., 2019). Furthermore, the neural mechanism by which NMT exerts any effect on fine motor networks is not well understood. In Parkinson's disease (PD), neuroimaging studies suggest music-based interventions are safe and affect distinct sensory and cerebellar regions to compensate for damaged basal ganglia pathways (de Bruin et al., 2010; Machado Sotomayor et al., 2021; Nombela et al., 2013; Nozaradan et al., 2017). We and others have previously shown that NMT-based fine motor interventions specifically modulate neural oscillations in the beta and gamma frequency bands in PD- the same frequencies known to be affected in HD (Blumenstock & Dudanova, 2020; Buard et al., 2019b; Painold et al., 2010, 2011; Rothe et al., 2015). Thus, NMT interventions are promising rehabilitation therapies for basal ganglia diseases such as PD and HD. Captured via magnetoencephalography (MEG), cortical activity in the beta and gamma bands reflects the relevant motor responses targeted by NMT.
In this proof-of-concept study we explore the feasibility of using an NMT based intervention for fine motor rehabilitation in HD, and determining neurophysiologic changes using MEG.
Methods
Participants were recruited from the University of Colorado Hospital Huntington's Disease Center of Excellence, based on a diagnosis of HD by a movement disorders neurologist, age 30–85 years, and on stable medications for at least 30 days prior to initial evaluation. Exclusion criteria included inability to move hands or fingers, ferrous metal implants interfering with MEG acquisition, or a diagnosis of dementia. The study was approved by the Institutional Review Board (IRB #16-2308, approved 4, November, 2019) and all participants signed written, informed consent.
Three right-handed participants underwent a 5-week NMT intervention using the somatosensory and motor rehabilitation NMT techniques to specifically focus on fine motor training (see intervention protocol developed by Buard et al., 2021). A board-certified music therapist conducted 15 NMT sessions, three times per week for five consecutive weeks, utilizing both in-person and online formats. The sessions included fine and gross motor warm-ups with range of motion exercises accompanied by music/rhythm. Then, finger scale exercises were played on a weighted keyboard in order to provide auditory feedback and resistance training and further improve fine motor strength and dexterity. Castanets were also used to strengthen the pincer grasp. Last, auditory rhythmic cues from a metronome were added to deliver the critical feedforward information that creates anticipation, repetition, periodic stability and continuous timing. Each participant completed a baseline visit within one week prior to starting the NMT intervention and a post intervention assessment within one week of NMT completion. Clinical and dexterity changes were captured using, respectively, the Unified Huntington's Disease Rating Scale (UHDRS), and the Grooved Pegboard Test (GPT) (Reuben et al., 2013). Additionally, subjects completed the Huntington's disease Quality of Life survey (HD-QoL) and the Hospital Anxiety and Depression Scale (HADS). Lastly, participants underwent MEG imaging while performing an auditory-motor task, as described in Buard et al. (2019b). The task consisted on tapping using the right index finger in timing with an acoustic burst stimuli (2000 Hz, intensity of 70 dB above subjective threshold). A quick practice session was performed prior to the MEG recording session. A total of 6 sequences of 30 s separated by a 5 s rest period were presented. Mean distance to cue (MDC) was measured during the auditory-motor task to assess entrainment of motor behavior to the rhythm (Buard et al., 2019a). Negative MDC values indicate most taps per participant occurred before the beat and positive MDC values indicate most taps per participant followed the beat. Preprocessing, co-registration with structural MRI and source analyses were identical to those described in Buard et al. (2019a), except that stimulus-locked spectral analysis was instead performed over a 0–800 msec time period in order to fully capture the temporal activation of neural responses to an external cue. In addition, we measured the inter-trial phase locking value: a measure of phase consistency of neuronal responses with external stimuli, and calculated the mean phase locking factor (MPLF) across trials per participant. MPLF computation is described in our previous investigation of the neurophysiological mechanisms of NMT in PD (Buard et al., 2019a).
Results
Participants had 100% adherence to the pre and post visit assessments and MEG scan while adherence to the NMT intervention was 93%. There was no change in the number of tapping responses before and after NMT. Two of the three participants exhibited negative MDC averaged values suggesting entrainment, while the third participant mostly produced positive values (ie. tapped after the beat), suggesting that participant may not be entrained. However, no difference was found for any participant from before to after the NMT intervention in MDC values.
Spectral analysis in the motor cortex during a cued finger tapping task exhibited a visual, but non-significant, increase in evoked power in the beta and low gamma band at tone onset (Figure 1A, time 0 – white arrow), suggesting an increase in neuronal mobilization during movement preparation after a course of NMT (Figure 1A). Interestingly, a later component (500–800 msec post tone – black arrow) of evoked beta motor activity was shifted earlier in time post- NMT compared to pre-NMT intervention. Therefore, we further investigated whether this could be due to a phase reset of the oscillations and measured the associated MPLF. Time frequency MPLF indicated NMT generated an increase at tone onset as well as a shift in time for the later component (Figure 1B), similar to our evoked power results.
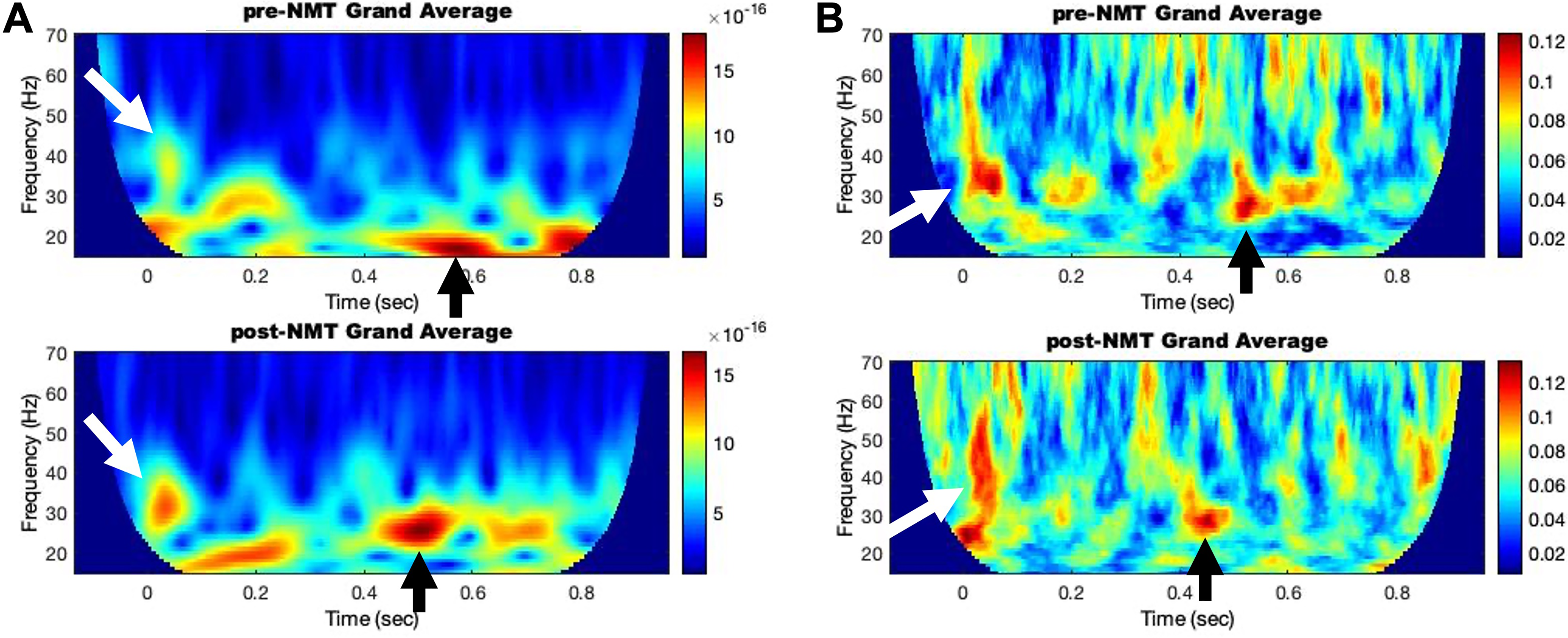
Composite Data of Time-Frequency Representation of the Neuromagnetic Changes (pre NMT -top- and post NMT -Bottom-) of Evoked (A - Left) and Mean Phase-Locking Factor (B - Right) in the Left Primary Motor Area During a Cued Right-Hand Finger Tapping. 0 Indicates Tone Onset.
Pre- and post- intervention data for the motor assessments are exhibited in Table 1. Two participants improved by ≥10 points on the UHDRS, while one participant worsened by one point. Assessments for non-motor symptoms are shown in the supplementary data. No statistically significant findings were noted, likely attributable to small sample size. Assessments specific for fine motor function, including finger taps, hand pronation/supination, and GPT demonstrated variable improvements.
Motor-Related Assessment Performed Before (pre) and After the NMT Intervention (post). Higher Scores Indicate Increased Impairment.
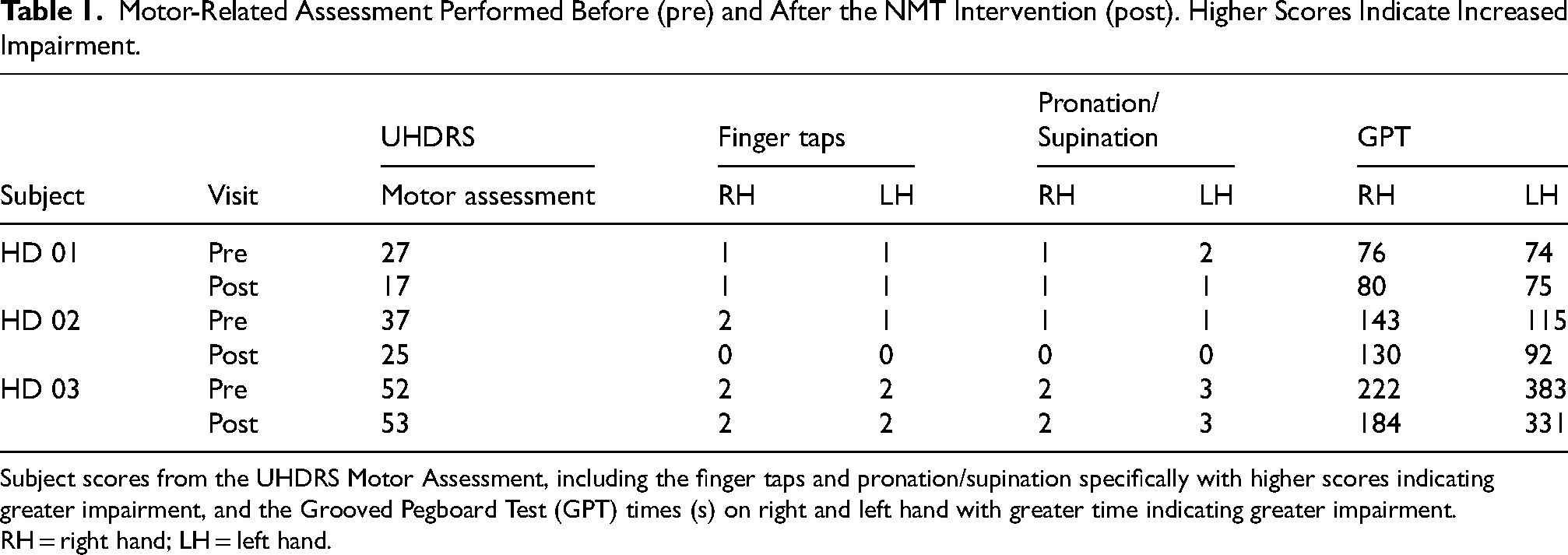
Subject scores from the UHDRS Motor Assessment, including the finger taps and pronation/supination specifically with higher scores indicating greater impairment, and the Grooved Pegboard Test (GPT) times (s) on right and left hand with greater time indicating greater impairment. RH = right hand; LH = left hand.
Discussion
Our study suggests NMT is a feasible and tolerable intervention which may impact fine motor neurophysiology in the context of rehabilitation. While this proof-of-concept study was not powered to detect statistically significant changes, it does demonstrate feasibility and provides a theoretical framework of the mechanisms underlying potential therapeutic effects.
The use of MEG is innovative and suggests NMT may increase the mobilization efficiency of neuronal populations involved in motor activities in patients with HD. The increased evoked response at tone onset may indicate an activity coupling between the auditory and motor regions, as previously found in a pilot study with patients with PD (Buard et al., 2019b). Temporal rhythmic entrainment of motor responses has become one of the major neurological mechanisms linking music and rhythm to brain rehabilitation, and has provided a scientific basis for the development of NMT techniques. The time shift in evoked response may be a consequence of auditory-motor coupling, leading to increased motor activity efficiency, possibly due to bypassing or compensating for deficient basal ganglia-thalamo-cortical loops (Damm et al., 2020; Nombela et al., 2013).
Motor impairments in HD have been associated with worsened quality of life, and increased caregiver burden (Banaszkiewicz et al., 2012; Helder et al., 2001; Ho et al., 2004). In this study, two of the three participants had improvement in the motor section of the UHDRS. The UHDRS is a scale of motor impairment ranging from 0–124, with no established minimal clinically significant change. Previous studies on music therapy in HD suggests that certain NMT techniques such as Rhythmic Auditory Stimulation (RAS) may allow patients to successfully modulate their gait velocity given metronome provided rhythmic cues (Devlin et al., 2019; Thaut et al., 1999). Schwartz and colleagues (2019) conducted a systematic review of literature investigating the effect of music, dance, and rhythmic auditory cueing on HD symptoms reported five research articles which specifically assessed motor outcomes (Delval et al., 2008; Johnson et al., 2000; Kloos et al., 2013; Thaut et al., 1999; Trinkler et al., 2019). However fine motor movements were evaluated only by one small (n = 5) pilot study (Hyson et al., 2005), which showed a non-significant trend toward improvement with fine motor tasks on the UHDRS. Interestingly, our three participants improved in different domains, which raises the possibility that patients may have differential responses dependent on symptom burden. Given the variability in response to each assessment, responders may be symptom-specific. A future direction should consider exploring factors related to responders and non-responders and whether neurophysiological markers such as MEG can predict responses.
Strengths of this study include the use of MEG in addition to clinical measures to explore the mechanisms underlying the influence of NMT on fine motor function in HD. The standardized clinical assessments using the UHDRS in addition to the HADS allow for a comprehensive understanding of the effects of NMT. This is particularly important as individuals with HD have a high burden of neuropsychiatric symptoms (Paoli et al., 2017), and NMT has been shown to have a positive effect on mood symptoms in those with neurologic conditions (Raglio et al., 2015). Lastly, use of the GPT in addition to the fine motor section of the UHDRS provides thorough evaluation for a functionally meaningful change in fine motor function. Limitations include the small sample size without a control group and lack of blinded assessments by the rater. Additionally, the finger tapping task during MEG was completed pre- and post- intervention, and thus there may have been a learning effect resulting from re-exposure of this task.
Conclusion
NMT-based fine motor rehabilitation is a feasible intervention in people with HD. Whether it has an effect, and if so whether that effect is driven by neuronal oscillatory modulation, will need to be defined in larger studies.
Supplemental Material
sj-docx-1-nre-10.1177_10538135251330979 - Supplemental material for Neurologic Music Therapy for Fine Motor Recovery in Huntington’s disease: A Proof-Of-Concept Magnetoencephalography Evaluation
Supplemental material, sj-docx-1-nre-10.1177_10538135251330979 for Neurologic Music Therapy for Fine Motor Recovery in Huntington’s disease: A Proof-Of-Concept Magnetoencephalography Evaluation by Emily Forbes, Lucas Lattanzio, Karrie Hardin, Leah Quiller, Amy W Amara, Lauren C Seeberger and Isabelle Buard in NeuroRehabilitation
Footnotes
Acknowledgements
We would like to thank the participants who contributed their time to this study, as well as the music therapists who worked to develop the original protocol, Sarah Thompson and Rebekah Stewart. We would also like to thank Benzi Kluger for his continuous support of this line of research, as well as members of the University of Colorado Huntington's Disease Center of Excellence.
Ethical Considerations
The study was approved by the Institutional Review Board (IRB #16-2308, approved 4, November, 2019).
Consent to Participate
All participants signed written, informed consent.
Consent for Publication
Informed consent for publication was provided by the participants.
Author Contributions/CRediT
Emily Forbes, DO,MS; Investigation, Project Administration, Resources, Visualization, Writing- original draft.
Lucas Lattanzio, BA; Data curation, Investigation, Project Administration, Visualization, Writing- review and editing.
Karrie Hardin, MT-BC, NMT; Investigation.
Leah Quiller, MM, MT-BC, NMT; Investigation.
Amy W Amara MD, PhD; Writing- review and editing.
Lauren C. Seeberger, MD; Investigation, Resources.
Isabelle Buard, PhD: Conceptualization, Investigation, Methodology, Project Administration, Supervision, Visualization, Writing- review and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflicting Interests
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: E.F has served as a site investigator for studies sponsored by Neurocrine, Biogen, BIAL, and Biohaven, and the Michael J Fox Foundation for Parkinson's Research. L.S has performed advisory work for Neurocrine and Biohaven. A.A reports she has served as a site investigator for studies sponsored by Michael J Fox Foundation for Parkinson's Research, Parkinson Study Group, Aligning Science Across Parkinson's (ASAP) Initiative, Biogen, Idec and the NIH NINDS. She receives grant funding from NIH NICHD. She is a consultant for PhotoPharmics, Inc, and Grey Matter Technologies, LLC. None of these affiliations represent a conflict of interest with the current work. The remaining authors confirm this research was conducted in the absence of any commercial or financial conflict of interest related to this study.
Data Availability
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.