
Abstract
Background
Upper extremity (UE) recovery in individuals with subacute stroke often plateaus despite conventional physical therapy (CPT). Smartphone-based virtual reality (VR) represents a low-cost, semi-immersive approach that may enhance task-specific training and neuroplasticity.
Objective
To determine whether CPT augmented with smartphone-based VR improves UE function more than CPT alone.
Methods
Fifty-seven participants (28 in the experimental group and 29 in the control group) with stroke in the subacute stage (6 weeks–6 months post-stroke) and moderate UE impairment (Fugl-Meyer Assessment–Upper Extremity [FMA-UE] score 20–50) were randomized to receive either CPT plus smartphone-based VR or CPT alone, five sessions per week for six weeks. Outcomes included motor impairment (FMA-UE), activity-level dexterity (Purdue Pegboard Test), and muscle strength (grip strength).
Results
Both groups demonstrated significant improvements (p < 0.001). The experimental group showed significantly greater improvements across all outcomes, with large effect sizes.
Conclusion
Smartphone-based VR providing semi-immersive, gaze-driven interaction with virtual tasks significantly enhances UE recovery and represents a scalable adjunct to rehabilitation.
Keywords
Introduction
Stroke is a leading cause of long-term disability worldwide, with upper extremity (UE) impairment affecting approximately 70–75% of survivors and significantly limiting independence in activities of daily living (ADLs) (Feigin et al., 2021; Langhorne et al., 2009). Although some spontaneous recovery occurs, many individuals with moderate impairment experience incomplete functional restoration, particularly after the early subacute phase, despite intensive rehabilitation (Kwakkel et al., 2003; Veerbeek et al., 2011).
Conventional physical therapy remains the cornerstone of post-stroke rehabilitation, focusing on task-specific training and repetitive practice. However, limitations such as reduced training intensity, low patient engagement, and declining motivation may restrict its effectiveness in promoting optimal neuroplastic changes (Pollock et al., 2014;Winstein et al., 2016). These challenges have driven increasing interest in technology-assisted rehabilitation approaches.
Virtual reality (VR) has emerged as a promising adjunct in neurorehabilitation by enabling repetitive, task-oriented, and interactive training within enriched environments that enhance motor learning and neuroplasticity (Laver et al., 2025; Levin et al., 2015; Maier et al., 2019). Systematic reviews and meta-analyses have established that VR training is a highly effective intervention for improving motor outcomes when compared to traditional rehabilitation methods (Aminov et al., 2018). Previous evidence suggests that VR-based interventions can improve upper limb motor recovery after stroke; however, many systems are costly and require specialized equipment, limiting their use in routine clinical practice (Corbetta et al., 2015).
In contrast, smartphone-based VR systems offer a low-cost, portable, and widely accessible alternative that can deliver engaging rehabilitation through commercially available devices. Recent feasibility studies indicate that smartphone-based VR platforms are well-accepted by both clinicians and patients, offering a viable solution for increasing therapy accessibility (Chua & Liew, 2019). Despite these advantages, there is still limited high-quality evidence examining their effectiveness, particularly in individuals with moderate upper limb impairment during the subacute stage, a critical window for neuroplastic recovery. Unlike most previous VR stroke rehabilitation systems that rely on dedicated hardware or high-cost immersive setups, the present study investigates a smartphone-based semi-immersive VR system as a low-cost and widely scalable alternative for subacute stroke rehabilitation.
Therefore, this randomized controlled trial aimed to investigate whether adding smartphone-based semi-immersive VR to conventional physical therapy leads to greater improvements in upper extremity motor function, dexterity, and strength compared with conventional therapy alone. It was hypothesized that the VR-augmented intervention would produce superior functional outcomes.
Methods
Study Design
This study was designed as an assessor-blinded, parallel-group randomized controlled trial conducted in accordance with the CONSORT guidelines. The study aimed to evaluate the effectiveness of smartphone-based semi-immersive VR as an adjunct to conventional physical therapy (CPT) for improving UE function after stroke. Blinded outcome assessment was implemented to minimize measurement bias, and standardized intervention protocols were used to ensure consistency and reproducibility.
Ethical Approval and Compliance
The study adhered to the Declaration of Helsinki and Good Clinical Practice (GCP) guidelines. Ethical approval was obtained from the Institutional Review Board, Faculty of Physical Therapy, Badr University (IRB00014233-23), and the trial was prospectively registered in the Pan African Clinical Trial Registry (PACTR202504595052372).
All participants provided written informed consent after receiving detailed verbal and written information about the study, including objectives, procedures, potential risks and benefits, and their right to withdraw at any time without affecting clinical care. Confidentiality was strictly maintained, and all procedures were designed to minimize risk and discomfort, with continuous monitoring throughout the trial.
Participants
Participants were recruited from outpatient rehabilitation clinics between May and November 2025. Eligible individuals were aged 40–65 years and had experienced a first-ever ischemic or hemorrhagic stroke.
Participants were included if they were within the subacute phase of stroke recovery, defined as 6 weeks to 6 months post-stroke at the time of enrollment.
Eligibility screening and verification procedures were conducted prior to randomization in accordance with the predefined study protocol. Final dataset review was additionally performed to ensure methodological consistency of the sample analyzed.
Inclusion criteria were:
Moderate upper extremity (UE) motor impairment, defined as a Fugl-Meyer Assessment Upper Extremity (FMA-UE) score of 20–50. Adequate cognitive function to follow study instructions, defined as a Mini-Mental State Examination (MMSE) score ≥24. Sufficient functional ability to hold and manipulate a smartphone using the affected upper limb
Smartphone handling ability was operationally defined using both strength and functional criteria. Participants were required to demonstrate a hand grip strength >5 kg and the ability to grasp a standard smartphone (6.1-inch display, ∼180 g), maintain a stable grip for at least 10 s, and perform simple controlled movements (e.g., reaching and wrist rotation) under therapist supervision during screening. All VR training tasks were subsequently performed using the affected upper limb.
The requirement for smartphone handling ability was included to ensure safe and effective participation in VR sessions, as participants were required to maintain stable head–device alignment and perform coordinated upper limb movements during task execution. Prior to enrollment, all participants had completed a course of standard post-stroke rehabilitation delivered during the early recovery phase in their respective clinical settings. This rehabilitation typically included conventional physiotherapy focused on mobility and basic upper limb exercises.
The duration of prior rehabilitation ranged from 2 to 4 weeks, depending on individual clinical progression and discharge planning. All participants were enrolled after completion of their routine rehabilitation program, and there was a minimum interval of 1–4 weeks between the end of prior rehabilitation and baseline assessment to minimize potential carryover effects.
Exclusion criteria included:
Severe upper limb spasticity (Modified Ashworth Scale score >3) Uncorrected visual or vestibular impairments. History of significant motion sickness Concurrent participation in other upper limb rehabilitation trials Any additional neurological or orthopedic condition, other than stroke, that could affect upper limb function
Randomization and Blinding
Participants were randomly assigned (1:1) to experimental or control groups using a computer-generated randomization sequence prepared by an independent researcher. Allocation concealment was ensured using sequentially numbered, opaque, sealed envelopes.
Outcome assessors were blinded to group allocation. Due to the nature of the intervention, participant and therapist blinding was not feasible; however, participants were instructed not to disclose their group assignment during outcome assessments to reduce detection bias.
Interventions
Both groups received five 60-min sessions per week for six weeks. The control group received 60 min of CPT per session, while the experimental group received 30 min of VR training followed by 30 min of CPT.
CPT program (both groups): Task-specific reach–grasp–release exercises, progressive resistance for shoulder/elbow stabilization, and bilateral coordination tasks. Therapists followed a structured manual and adjusted intensity according to tolerance while maintaining dosage equivalence (Table 1).
Intervention Training Protocols.
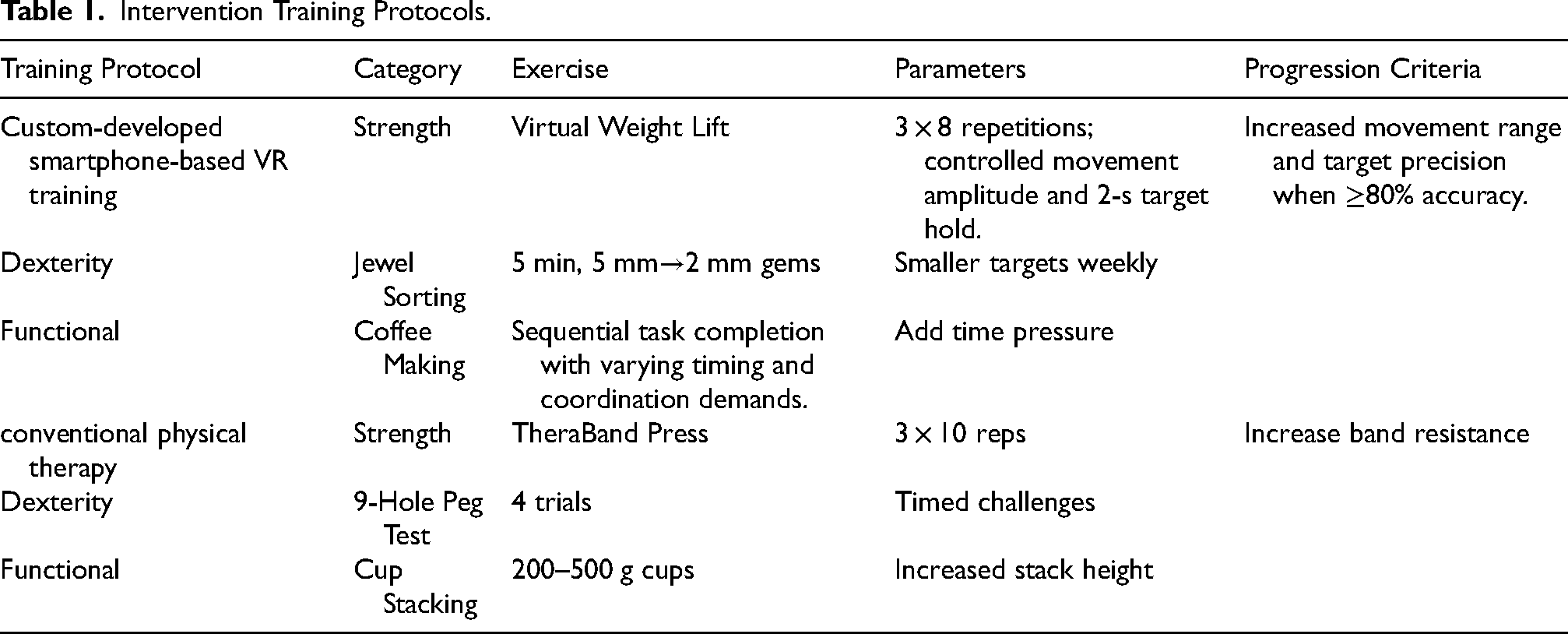
Experimental group: The VR system consisted of a smartphone inserted into a head-mounted display (Google Cardboard), providing a semi-immersive, first-person visual environment.
Interaction within the virtual environment was achieved using head-orientation tracking via the smartphone's inertial sensors (gyroscope and accelerometer), enabling gaze-based control.
Participants performed task-oriented upper limb movements synchronized with virtual tasks; however, upper limb kinematics were not directly tracked. Task performance was determined by successful interaction with virtual targets using gaze-directed control. The VR program was custom-developed using the Godot Engine (v4.x) and included task categories for strength, dexterity, and functional simulation (detailed task environments and technical parameters are provided in Supplementary Table 1).”
Strength-oriented tasks: simulated lifting tasks requiring controlled movement amplitude and sustained positioning Dexterity tasks: fine motor activities such as jewel sorting with progressively smaller targets Functional simulations: activities of daily living (e.g., virtual coffee preparation) requiring coordinated sequential movements
Progression and Accuracy
Task difficulty was automatically adjusted based on performance. Accuracy was defined as the percentage of successfully completed task attempts relative to total attempts, calculated using predefined spatial and temporal criteria (e.g., correct trajectory and completion within time limits).
Task difficulty was adapted based on accuracy by reducing target size, shortening allowable time windows, or increasing the number of sequential steps. No mechanical resistance or haptic feedback was applied.
Fidelity and reproducibility: Sessions were delivered by licensed physical therapists with ≥5 years of neurorehabilitation experience. Adherence was monitored using structured CPT checklists and automated VR logs.
Data were analyzed using a per-protocol approach, including participants who completed at least 80% of the intervention sessions.
Outcome Measures
Assessments were conducted at baseline and immediately after the 6-week intervention by blinded evaluators. Outcome measures were selected according to the WHO International Classification of Functioning, Disability and Health (ICF) framework:
Motor Impairment: FMA-UE was used as the primary measure due to its high sensitivity in detecting motor changes in subacute stroke (Page et al., 2012). Activity level: Manual dexterity was assessed using the Purdue Pegboard Test (number of pegs placed in 30 s) (Tiffin & Asher, 1948). Grip strength: Measured using a calibrated handheld dynamometer (Jamar-type), with participants seated, shoulder adducted, elbow flexed at 90°, and forearm in neutral position. Three trials were performed with the affected hand, and the mean value (kg) was recorded.
The Simulator Sickness Questionnaire (SSQ) was administered during VR sessions for safety monitoring purposes only and was not included in outcome analysis (see Supplementary Table 1 for safety monitoring details).
Sample Size Calculation
Sample size was calculated using G*Power (version 3.1) for repeated-measures ANOVA (within–between interaction). Based on an anticipated effect size of 0.8 (derived from pilot data), α = 0.05, and statistical power of 80%, a minimum of 52 participants (26 per group) was required. To account for potential dropout, 60 participants were recruited.
Statistical Analysis
All analyses were performed using IBM SPSS Statistics (version 25; IBM Corp., Armonk, NY, USA). Normality and homogeneity of variance were assessed using the Shapiro–Wilk and Levene's tests, respectively.
A mixed-design multivariate analysis of variance (MANOVA) was used to examine the effects of group (VR vs control) and time (pre- vs post-intervention) on outcome measures. When significant interaction effects were detected, Bonferroni-adjusted post-hoc analyses were conducted. In addition, independent samples t-tests were used to compare baseline characteristics between groups to confirm group equivalence prior to intervention.
Results
Participant Flow
A total of 74 individuals were screened for eligibility. Fourteen participants were excluded (9 did not meet inclusion criteria and 5 declined participation). The remaining 60 participants were enrolled and initially randomized to the experimental group (n = 30) and the control group (n = 30).
During final dataset review and consistency checking, two participants from the experimental group and one participant from the control group were excluded from the final analysis because their intervention initiation timing was found to be inconsistent with the predefined temporal eligibility criteria. These exclusions occurred prior to final statistical analysis and were unrelated to treatment adherence, intervention tolerability, or loss to follow-up.
Therefore, the final analyzed sample consisted of 57 participants: experimental group (n = 28) and control group (n = 29). All analyzed participants completed the intervention and post-treatment assessments. Participant flow is summarized in Figure 1 (CONSORT Flow Diagram).
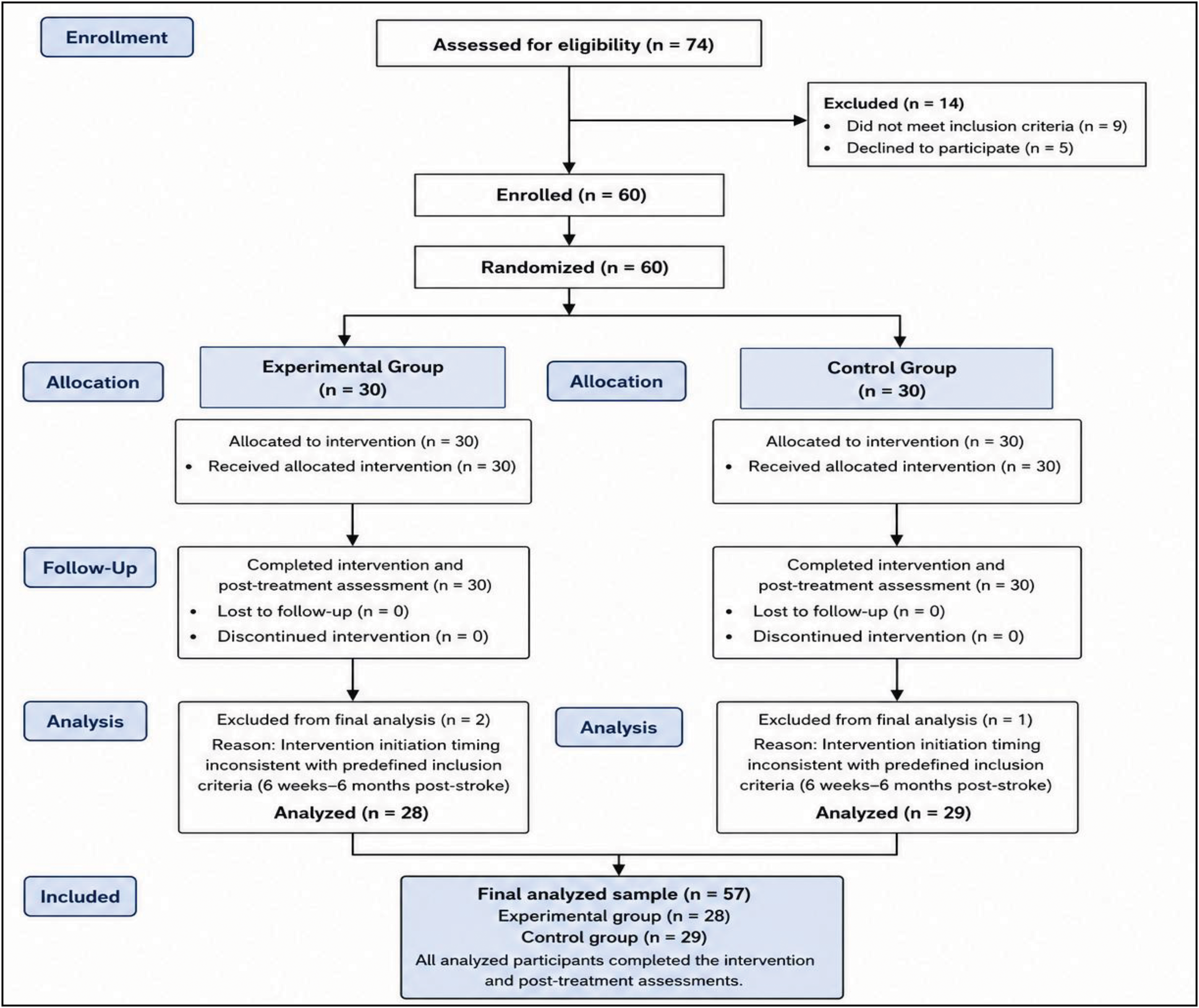
Consort flow diagram illustrating flow of participants through the trial including enrollment, allocation, follow-up, and analysis.
Baseline Characteristics
Baseline demographic and clinical characteristics are summarized in Table 2. There were no statistically significant differences between the experimental and control groups in age, sex distribution, anthropometric measures, duration of illness, affected side, or baseline outcome measures (all p > 0.05), indicating successful randomization and baseline comparability.
Participant Demographics and Baseline Characteristics.
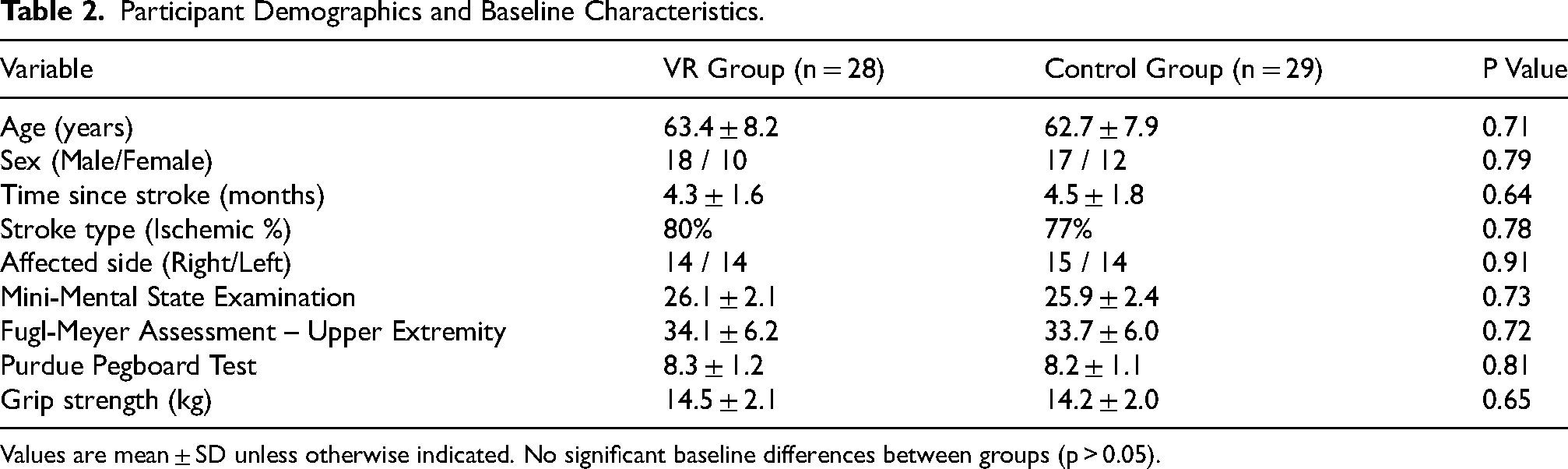
Values are mean ± SD unless otherwise indicated. No significant baseline differences between groups (p > 0.05).
Intervention Adherence
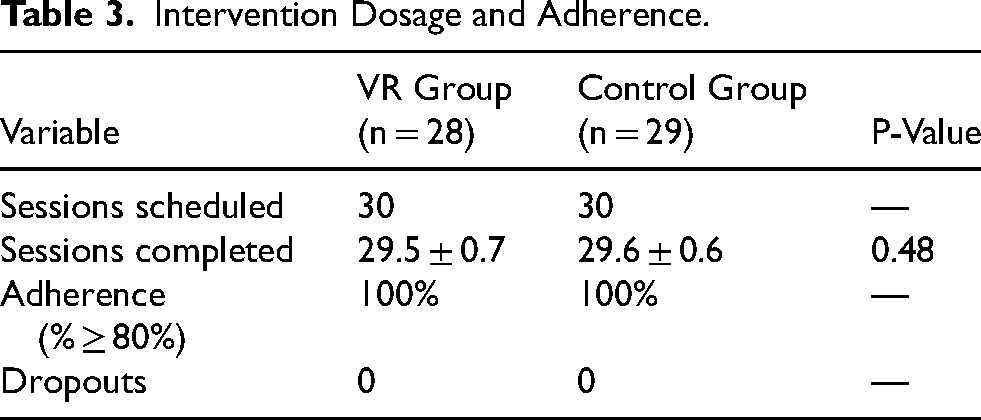
All participants completed the prescribed intervention sessions. The mean number of completed sessions was comparable between groups, with the VR group completing 29.5 ± 0.7 sessions and the control group completing 29.6 ± 0.6 sessions (p = 0.48). These figures indicate that both groups received a nearly identical “dose” of therapy, ensuring that the observed differences in motor recovery were likely due to the specific nature of the intervention rather than variations in total training time.
Adherence and Dropouts
Among the final analyzed sample, adherence was 100% in both groups, defined as completion of at least 80% of the scheduled sessions (Table 3). No participants in the analyzed sample were lost to follow-up or discontinued the intervention during the six-week study period, reflecting high participant engagement and the feasibility of the smartphone-based VR protocol.
Intervention Dosage and Adherence.
Safety and Tolerability
The intervention was well-tolerated. As monitored by the SSQ, no participants reported significant symptoms that required session termination or modification. In accordance with the study protocol, these data were recorded for safety monitoring purposes and were not subjected to formal statistical analysis. This supports the safety profile of the semi-immersive VR configuration used in this study.
Effects of Intervention on Outcome Measures
Multivariate Analysis
The mixed multivariate analysis of variance (MANOVA) revealed a significant time × group interaction effect across the dependent variables (Wilks’ λ = 0.02, F = 1112.22, p < 0.001, η2 = 0.98), indicating differential treatment effects over time between groups. Significant main effects of time (Wilks’ λ = 0.005, F = 3785.01, p < 0.001, η2 = 0.99) and group (Wilks’ λ = 0.42, F = 25.39, p < 0.001, η2 = 0.57) were also observed.
Within-Group Comparisons
Both groups demonstrated significant improvements from baseline to post-intervention across all outcome measures (p < 0.001 for all). However, the experimental group exhibited a greater magnitude of improvement compared with the control group across all variables, suggesting that while conventional therapy is effective, the addition of VR provides a substantial additive benefit (Table 4 & Figure 2).
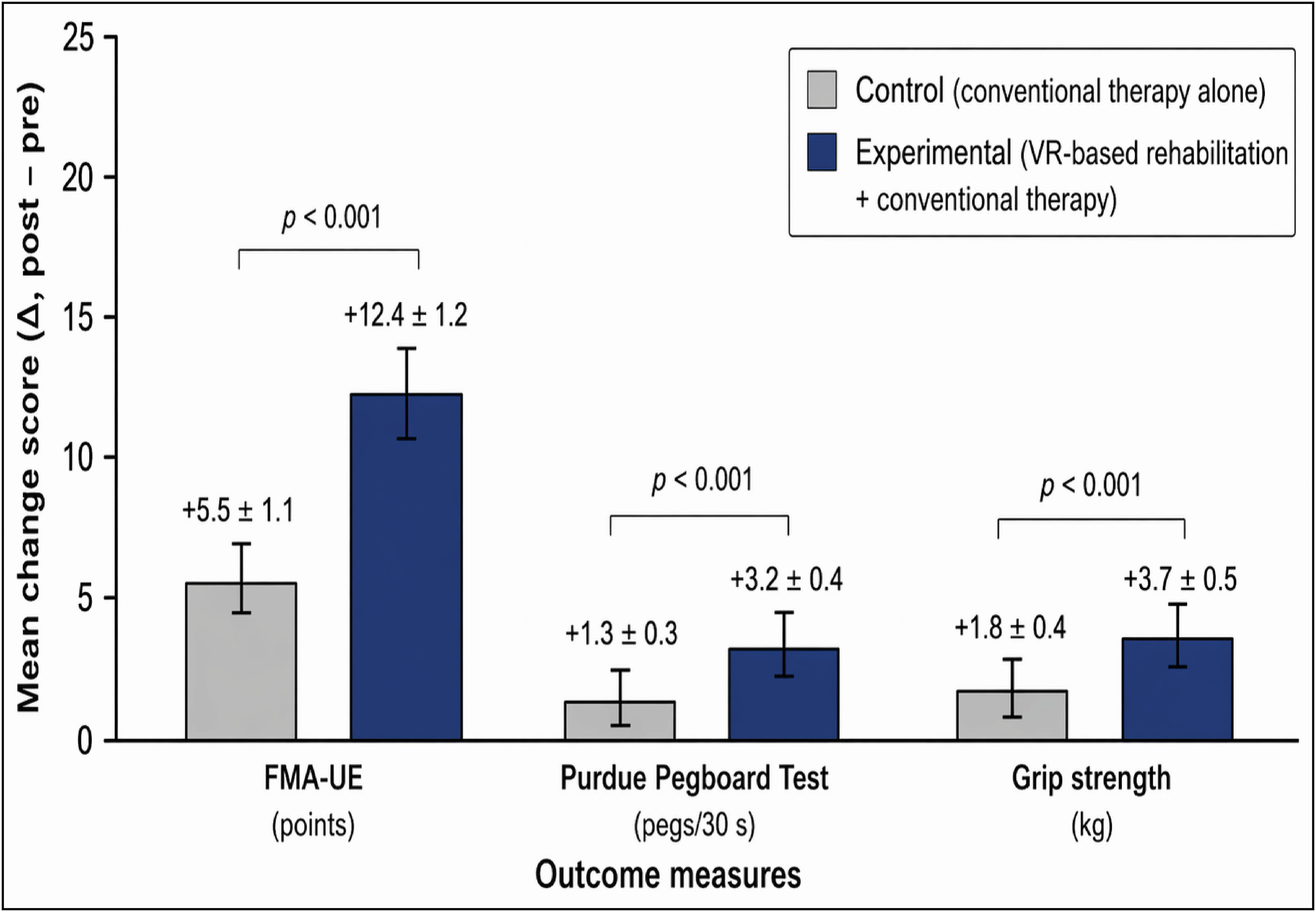
Change scores (Δ post–pre) for upper extremity outcomes in the experimental (VR + CPT) and control (CPT) groups. Bars represent mean ± standard deviation. The Y-axis displays change scores, with outcome-specific units (FMA-UE: points; Purdue Pegboard: number of pegs; grip strength: kg). Effect sizes (Cohen's d) reflect between-group differences and are presented above each outcome. Statistically significant differences between groups are indicated (*p < 0.001).
Pre- and Post-Intervention Outcomes.
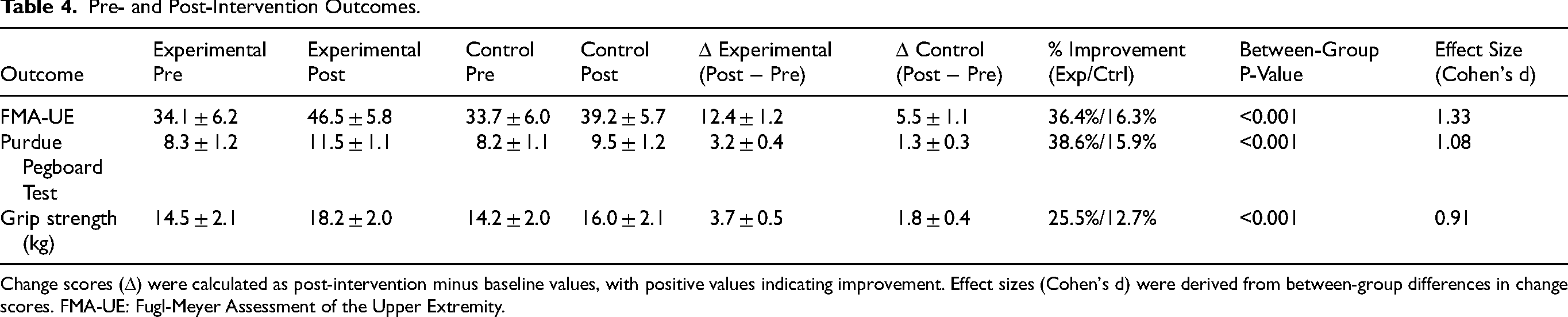
Change scores (Δ) were calculated as post-intervention minus baseline values, with positive values indicating improvement. Effect sizes (Cohen's d) were derived from between-group differences in change scores. FMA-UE: Fugl-Meyer Assessment of the Upper Extremity.
Between Group Comparisons
Baseline equivalence was confirmed, as there were no statistically significant differences between groups at baseline (p > 0.05 for all outcomes). Following the six-week intervention, the experimental group demonstrated significantly greater improvements than the control group in upper extremity motor function (FMA-UE), manual dexterity (Purdue Pegboard Test), and muscle strength (p < 0.001 for all). These findings indicate a superior treatment effect for the VR-augmented intervention compared to conventional physical therapy alone (Table 4 & Figure 2).
Change Scores and Percentage Improvement
The experimental group demonstrated greater gains than the control group in FMA-UE (Δ = 12.4 vs 5.5), Purdue Pegboard Test (Δ = 3.2 vs 1.3), and grip strength (Δ = 3.7 vs 1.8). All between-group differences in change scores were statistically significant (p < 0.001), indicating a robust treatment effect.
These findings were supported by large effect sizes across all outcomes, including FMA-UE (d = 1.33), Purdue Pegboard Test (d = 1.08), and grip strength (d = 0.91), confirming the clinical relevance of the intervention.
Percentage improvement from baseline was greater in the experimental group across all outcomes (FMA-UE: 36.4% vs 16.3%; Purdue Pegboard: 38.6% vs 15.9%; grip strength: 25.5% vs 12.7%).
Discussion
This randomized controlled trial demonstrates that augmenting CPT with smartphone-based semi-immersive VR significantly enhances UE recovery in subacute stroke patients with moderate impairment. The experimental group achieved superior improvements in motor function, manual dexterity, and muscle strength compared with CPT alone, with large effect sizes across all outcomes. These findings provide robust evidence that low-cost, mobile VR technology can serve as an effective adjunct to standard neurorehabilitation.
The present results are consistent with and extend the current evidence base on VR for stroke rehabilitation. The most recent Cochrane review by Laver et al. (2025), which included 190 trials and 7,188 participants, concluded that VR may be beneficial in improving upper limb function and activity, with more promising effects observed when VR was added to usual care rather than substituted for it. The findings align closely with this conclusion: the VR-augmented group received additional therapy time through the VR component while maintaining the full CPT dose, supporting the notion that VR's benefit is partly mediated through increased total therapy duration. As Laver and colleagues noted, spending more time in therapy is known to improve outcomes after stroke, and VR can offer an engaging way to increase therapy time without constant clinician supervision.
A contemporaneous frontier review by Cardile et al. (2025) provides important context for interpreting these results. Their systematic review of 46 studies found that VR interventions yielded positive motor outcomes in 76.3% of cases, with semi-immersive VR achieving the highest proportion of significant improvements (88.24%). The use of a semi-immersive smartphone-based system in the present study aligns with the modality showing the most consistent motor benefits. Furthermore, the absence of a statistically significant association between VR typology and stroke phase suggests that VR can be beneficially applied across various recovery stages. Early foundational work by Cameirão et al. (2010) established the effectiveness of VR-based training for enhancing motor recovery; these new results extend that evidence to a low-cost, smartphone-based semi-immersive platform.
The findings also resonate with a recent meta-analysis by Lu et al. (2025). Although their primary focus was on lower limb mobility, they established that VR therapy significantly improved functional outcomes when applied with frequencies of ≥20 sessions. The intervention protocol of 30 sessions over six weeks used here comfortably exceeds this threshold, reinforcing the dose-response relationship seen across stroke recovery domains. In addition, Wankhede et al. (2025) provided a comprehensive neuroscientific framework for understanding VR's effects, highlighting its role in modulating neuroplasticity through enhanced neuronal connectivity, sensory feedback mechanisms, and motor learning processes. These mechanisms likely underpin the functional gains observed in our participants.
Clinical Significance
A key strength of the study is that the observed improvements exceeded established thresholds for clinically meaningful change. For the FMA-UE, the experimental group's mean improvement of 12.4 points reaches the minimal clinically important difference (MCID) of 12.4 points identified by Hiragami et al. (2019) for convalescent patients with moderate to severe hemiparesis. This gain also comfortably exceeds the MCID of 9–10 points typically reported for broader subacute stroke populations. Furthermore, a meta-analysis by Kolmos et al. (2025) confirms that FMA-UE improvements during usual care in subacute stroke average 10–12 points; the VR group exceeded this benchmark, whereas the control group's improvement of 5.5 points was more modest.
For grip strength, the experimental group's 25.5% improvement translates to a gain of 3.7 kg, approaching or exceeding the commonly cited MCID of ≥5 kg or ≥10–15% improvement (Winstein et al., 2016), a meaningful functional change given that grip strength is strongly associated with independence in activities of daily living.
Mechanisms Underlying Treatment Effects
The superior outcomes observed in the VR group likely reflect the convergence of several key therapeutic mechanisms. Task-specific, repetitive practice within an enriched environment is a well-established driver of experience-dependent neuroplasticity (Kleim & Jones, 2008; Maier et al., 2019). The VR task spanning strength, dexterity, and functional domains—provided diverse motor challenges that complemented the CPT curriculum. The integration of real-time visual and auditory feedback, coupled with gamification elements, may have enhanced motivation and adherence (Burke et al., 2009; Choi et al., 2016). A qualitative meta-synthesis by Ding et al. (2025) confirmed that VR rehabilitation enhances perceived self-benefits, including physical and psychological improvements, and that user engagement and supportive environments are key facilitators of positive outcomes. The high adherence rates (100%) and absence of dropouts in our trial support the motivational value of this approach.
The dynamic difficulty adjustment (DDA) embedded in our VR system ensured that task demands remained optimally challenging throughout the intervention period. Recent work by Chen et al. (2024) supports this concept, demonstrating that difficulty adaptation driven by attention levels can improve task engagement and training outcomes. Furthermore, research by Patel et al. (2025) highlights the critical importance of timing and dosage of VR training in the subacute period, noting that dose-timing interactions can significantly influence motor recovery trajectories. The combination of early subacute timing and adaptive difficulty likely created conditions favorable for maximizing recovery.
The semi-immersive, first-person perspective employed in our system warrants particular consideration. Cardile et al. (2025) noted that semi-immersive VR may strike an optimal balance between providing sufficient sensory engagement to drive motor learning while minimizing the cybersickness and cognitive overload sometimes associated with fully immersive systems. This is consistent with the recorded safety data, which showed no significant simulator sickness.
Accessibility and Real-World Applicability
A distinguishing feature of our intervention is its reliance on widely available smartphone technology combined with low-cost head-mounted displays. This addresses a critical gap in global rehabilitation. The World Health Organization (2019) and recent literature emphasize the urgent need for affordable interventions, particularly in low-resource settings (Dias et al., 2020). The recent development of culturally adapted systems, such as AdaptRehab VR for Ethiopian populations (Gemechu et al., 2025), underscores the global demand for such scalable solutions.
The potential for home-based deployment is especially promising. A systematic review by Huang et al. (2025) of eight randomized controlled trials concluded that home-based VR training positively affects upper extremity function recovery in patients with stroke, particularly motor control improvement, with customized VR systems being more effective than commercial systems with moderate to severe disorders. Similarly, a feasibility trial by Sheehy et al. (2025) demonstrated that non-immersive home-based VR training is safe and feasible for continuing rehabilitation after discharge from inpatient or outpatient therapy, with participants completing an average of 26 sessions and reporting high enjoyment. These findings suggest that smartphone-based VR systems like ours may be particularly well-suited for bridging the gap between supervised clinical rehabilitation and independent home practice.
However, it should be noted that evidence on home-based digital technology interventions is not uniformly positive. A systematic review and meta-analysis by Gooch et al. (2025) found no evidence of effect for virtual reality compared with time-matched conventional exercise on upper limb motor impairment or activity limitation when delivered at home during the acute and subacute phases, though the certainty of evidence was low. This discrepancy underscores the need for further research comparing supervised versus unsupervised delivery models and highlights the importance of the structured, therapist-supervised context in which our intervention was delivered.
Strengths and Limitations
This study has several strengths, including its randomized, assessor-blinded design, standardized intervention protocols, and high adherence rates (>80%), which support internal validity and feasibility. The use of validated outcome measures aligned with the ICF framework enhance clinical relevance. Importantly, the implementation of a low-cost, portable smartphone-based VR system demonstrates the potential for scalable and accessible neurorehabilitation without compromising effectiveness.
However, several limitations should be acknowledged. The six-week intervention period limits conclusions regarding long-term retention of gains. Upper limb kinematics were not directly assessed, restricting insight into movement quality and recovery mechanisms. The absence of the Action Research Arm Test (ARAT) may limit comparability with other studies. Participant and therapist blinding was not feasible, although assessor blinding mitigated this risk. The lack of a sham VR condition prevents isolation of VR-specific effects from increased therapy exposure. Additionally, the sample was limited to subacute stroke patients with moderate impairment, which may affect generalizability to other populations.
Future Directions
Future research should include longer follow-up periods (6–12 months) to assess durability of outcomes and the role of booster sessions. Comparative studies evaluating supervised versus home-based VR interventions are needed, particularly given mixed evidence for remote rehabilitation (Gooch et al., 2025; Huang et al., 2025). Incorporating neuroimaging and neurophysiological measures could further elucidate mechanisms of recovery (Wankhede et al., 2025).
Dose–response studies are warranted to determine optimal training parameters, building on recent work on dose–timing effects (Patel et al., 2025). Economic evaluations will also be essential to support large-scale implementation, especially in resource-limited settings. Future systems may benefit from integrating approaches such as action observation training (Errante et al., 2026) and myoelectric pattern recognition (Munoz-Novoa et al., 2025). Finally, qualitative research exploring user experience may help identify barriers to adoption and inform real-world application.
Conclusion
Smartphone-based VR is a viable, effective adjunct to conventional therapy for subacute stroke patients with moderate UE impairment. The intervention produced significant, clinically meaningful improvements in motor function, dexterity, and strength while remaining accessible and scalable. These findings support the potential for low-cost mobile VR to transform stroke rehabilitation, particularly in resource-limited contexts. Future studies should focus on long-term efficacy, home-based delivery, and neural mechanisms, guiding the development of scalable, evidence-based VR rehabilitation protocols.
Supplemental Material
sj-doc-1-nre-10.1177_10538135261456309 - Supplemental material for Smartphone-Based Semi-Immersive Virtual Reality Enhances Upper Extremity Function in Subacute Stroke: A Randomized Controlled Trial
Supplemental material, sj-doc-1-nre-10.1177_10538135261456309 for Smartphone-Based Semi-Immersive Virtual Reality Enhances Upper Extremity Function in Subacute Stroke: A Randomized Controlled Trial by Abd El-Hamied Ibrahim El-Sayed Mohammad El-Sherbini, Shreen Ibrahim Taha, Dany Alphonse Anwar Habib, Hanaa Mohsen Abd-Elfattah and Hager Rasmy Elserougy in NeuroRehabilitation
Footnotes
Acknowledgments
Special thanks to all our patients who participated in the research for their patience and dedication.
ORCID iDs
Institutional Review Board Statement
The study was reviewed and approved by the local ethical committee of the Faculty of Physical Therapy, Badr University (Approval No: IRB00014233-23).
Informed Consent
All the authors reviewed and approved of the final manuscript and consented to its publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data are available at reasonable requests from the corresponding author.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process’
Generative AI tools were used solely for language editing and improvement of clarity. No AI tools were used for data analysis, interpretation, or generation of scientific content. The authors take full responsibility for the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.