
Abstract
Objective
To map rehabilitation interventions and rehabilitation-relevant management reported for lateral medullary stroke (Wallenberg syndrome) and distinguish direct intervention evidence from management and assessment reports.
Data sources
PubMed/MEDLINE, Ichushi-Web, and Web of Science Core Collection were searched from inception to 12 March 2026. Cumulative Index to Nursing and Allied Health Literature was searched on 24 April 2026. Citation tracking was performed.
Review methods
Reports were eligible if they described rehabilitation, rehabilitation-relevant management, assessment, prognosis, or monitoring relevant to recovery or safety. Two reviewers screened records; charting and classification were verified by a second reviewer using operational definitions. Reports were grouped by clinical phase, target domain, safety management, outcome measures, and primary reporting function.
Results
The searches identified 741 records; 486 unique records were screened and 78 reports were included. Publication years ranged from 1997 to 2026; 60 reports were case reports or case series. Primary reporting functions were categorized as explicit intervention/program (n = 29), management/procedural pathway (n = 21), assessment/prognostic/monitoring (n = 18), and minimal-detail supportive/diagnostic (n = 10). Dysphagia was addressed in 63 reports, but only 22 were explicit intervention/program reports. No included report explicitly described sensory safety education.
Conclusion
The accessible literature is useful but mixed. Interpretation is limited by unretrieved full-text candidates, omitted databases/grey literature, no critical appraisal, and no independent agreement statistic for post hoc reporting-function classification. Future reports should separate therapeutic training from management pathways and describe dosage, safety management, reassessment timing, discharge function, sensory safety education, and daily-life precautions.
Keywords
Introduction
Lateral medullary stroke, classically described as Wallenberg syndrome or lateral medullary syndrome, is associated with ischemic involvement of the lateral medulla. It may present with dysphagia, truncal ataxia, gait disturbance, body lateropulsion, crossed or dissociated sensory symptoms, and autonomic manifestations. The distribution of sensory dysfunction is not always confined to a typical pattern, and it can influence safety precautions and daily-life guidance after stroke (Kim et al., 1997). Lateropulsion and gait disturbance also have immediate implications for fall prevention and mobilization in the acute phase, and recent physical therapy reports have begun to describe quantitative balance and vestibular assessments (Harayama et al., 2025; Matsuo et al., 2022).
Rehabilitation for this condition is not limited to direct therapeutic techniques such as swallowing exercises, physical therapy, occupational therapy, postural control training, gait practice, or activities of daily living training. Enteral feeding, airway and respiratory management, instrumental swallowing assessment, decisions about when to start, interrupt, or resume training, bladder management, and discharge planning can all shape whether rehabilitation is safe and feasible. Because several symptoms may evolve together over time, the clinical course is difficult to describe through a single discipline-specific intervention alone.
Existing reports are distributed across severe dysphagia, swallowing physiology, lateropulsion assessment, procedural management, and single-case intervention literature. Previous review-type articles and narrative summaries were useful for citation tracking, but our search did not identify a prior cross-domain scoping review or evidence map that separated direct rehabilitation intervention evidence from management, assessment, and prognostic literature for lateral medullary stroke/Wallenberg syndrome. A cross-domain map showing which problems are reported, at which clinical phase, and with what kind of reporting function remains limited. When intervention reports, assessment reports, prognostic reports, and management pathways are placed in the same table without distinction, the apparent amount of direct intervention evidence can be overestimated.
This scoping review and evidence map aimed to map rehabilitation interventions and rehabilitation-relevant management for lateral medullary stroke, Wallenberg syndrome, lateral medullary syndrome, or lateral medullary infarction across acute, subacute, and chronic phases. The review also aimed to distinguish direct training evidence from management and assessment literature, and to identify reporting items that should be prioritized in future case reports, case series, and intervention studies.
Methods
Review Design
This review was conducted as a scoping review using Joanna Briggs Institute guidance and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (Peters et al., 2020; Peters et al., 2022; Tricco et al., 2018). The protocol was registered in an online protocol repository before formal study selection. Protocol access details are provided in the title page/declarations file and Supplementary Methods. A completed Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews checklist is provided as a separate reporting-guideline checklist file. Because the purpose was to map the extent, nature, and gaps in the literature, formal critical appraisal was not conducted.
Eligibility Criteria
Participants
This review considered reports of patients diagnosed with Wallenberg syndrome, lateral medullary syndrome, lateral medullary infarction, or an equivalent diagnostic label. Closely related medullary-spectrum conditions were retained only when they could inform rehabilitation-relevant management in a lateral medullary or medullary-spectrum context.
Concept
The concept was rehabilitation or rehabilitation-relevant management directly related to functional recovery or safe clinical operation. At the charting and synthesis stage, each included report was assigned one mutually exclusive primary reporting function: explicit intervention/program, management/procedural pathway, assessment/prognostic/monitoring, or minimal-detail supportive/diagnostic. This categorization was an operational framework to separate direct training evidence from management and assessment reports; it did not treat management/procedural pathways as clinically unimportant or as non-interventions. Pure diagnostic, imaging, or neuroanatomical reports were excluded at full-text review when no connection to functional training, management decisions, safety management, or rehabilitation was identifiable.
Context
All clinical phases were eligible, including acute, subacute, chronic, mixed, and unclear phases. Settings included acute hospitals, inpatient rehabilitation, outpatient rehabilitation, and community-based follow-up. For international interpretability, acute hospital was defined as an inpatient setting for acute diagnosis, treatment, and early mobilization, whereas inpatient rehabilitation/rehabilitation setting was defined as an inpatient setting in which intensive multidisciplinary rehabilitation is provided after the acute phase. Country-specific terms, such as the Japanese convalescent rehabilitation ward, were treated as corresponding to a subacute or post-acute inpatient rehabilitation phase rather than as a separate setting category.
Types of sources. Case reports, case series, observational studies, randomized or quasi-randomized trials, feasibility studies, and practice-oriented clinical reports were considered when they met the population, concept, and context criteria. Reviews, editorials, and commentaries were excluded from inclusion but were used for citation tracking when relevant.
Information Sources, Search, and Source Selection
PubMed/MEDLINE, Ichushi-Web, and Web of Science Core Collection were searched from database inception to 12 March 2026. Ichushi-Web is a major Japanese bibliographic database for medical, nursing, and allied-health literature and was included to reduce language and regional bias in Japanese clinical reports. Cumulative Index to Nursing and Allied Health Literature, via EBSCOhost, was searched on 24 April 2026 before final synthesis to reduce under-ascertainment of nursing, allied-health, and practice-oriented rehabilitation-relevant reports. Cumulative Index to Nursing and Allied Health Literature records were merged with the existing search results and assessed using the same eligibility criteria and screening procedure.
No limits were applied for publication date or study design. No language filter was applied during database searching. After protocol finalization, language eligibility was expanded from Japanese and English to include one Korean-language report because full-text assessment and data charting were performed by a Korean-proficient reviewer. Backward citation searching of included reports and relevant reviews was conducted, and forward citation tracking was performed through Web of Science. A dedicated grey literature search of conference abstracts, theses, unpublished materials, clinical guidelines, institutional protocols, patents, and trial registries was not conducted. Embase, Scopus, the Physiotherapy Evidence Database (PEDro), and the Occupational Therapy Systematic Evaluation of Evidence (OTseeker) were also not searched. These omissions may have missed European, rehabilitation-database, physical therapy, occupational therapy, conference, thesis, protocol, or trial-registry records and are treated as limitations rather than as evidence that such literature does not exist. Complete final database-specific search strategies are provided in Supplementary Table S5.
Search results were imported into Zotero and deduplicated. Two reviewers independently screened titles and abstracts and then assessed full-text reports. At each stage, the reviewers compared decisions, rechecked discordant records against the Population, Concept, and Context eligibility criteria, and reached a consensus by discussion. A third reviewer adjudicated disagreements that could not be resolved by consensus. Before consensus, inter-rater agreement was calculated with Cohen's kappa for paired independent reviewer-decision logs for human title/abstract screening and full-text eligibility screening. Full texts were sought through institutional subscriptions, publicly available electronic full texts, EBSCOhost full-text availability, publisher websites, and bibliographic links. This review was scoped as a map of reports available through these retrieval routes; reports unavailable through these routes were coded as not retrieved, listed separately, and not assigned eligibility status.
Data Charting and Synthesis
Study selection and charting were conducted in a Microsoft Excel workbook, and an anonymized workbook aligned with the revised counts is provided as Supplementary Data 1. This workbook contains the final selection-flow summary, inter-rater agreement summary, included-report charting table, unretrieved-report list, protocol-amendment log, data charting form, search strategies, operational definitions, and audit summary used for the revised evidence map. One reviewer initially charted each included report, and a second reviewer checked all charted fields, target-domain labels, and primary reporting-function classifications. Discordant charting or classification entries were resolved by reviewer discussion, with third-reviewer adjudication if required. The initial charting form was based on the protocol and was refined during synthesis to include reporting function and diagnostic spectrum categories. Charted items included author, publication year, study design, setting, clinical phase, diagnostic label, diagnostic spectrum, target domain, discipline, intervention or management content, dosage, safety management, outcome measures, main rehabilitation-relevant findings, and primary reporting function. The charting form is provided in Supplementary Table S4, study-level characteristics are provided in Supplementary Table S1, operational definitions are provided in Supplementary Table S6, and screening agreement statistics are provided in Supplementary Table S7.
The synthesis first described all included reports by clinical phase, setting, primary discipline, target domain, diagnostic spectrum, and primary reporting function. Target domain labels were non-mutually exclusive, whereas primary reporting function was assigned as one mutually exclusive study-level category. The synthesis then cross-tabulated target domains by reporting function and presented an evidence map restricted to explicit intervention/program reports. To characterize potential retrieval bias, publication-year distributions were compared between reports unavailable through the specified retrieval routes and included reports. Analytic refinements, including the reporting-function framework, diagnostic spectrum grouping, retrieval-gap analysis, and explicit-intervention-only evidence map, were added during charting and synthesis without changing the population, concept, or context eligibility criteria; these refinements are summarized in Supplementary Table S3. Because the reporting-function and diagnostic-spectrum categories were introduced as analytic refinements during synthesis and finalized by consensus coding, percent agreement and Cohen's kappa were not calculated for those post hoc classification categories; this is reported as a limitation.
Results
Selection of Sources and Retrieval Gap
Figure 1 shows the study selection flow. The final database searches identified 741 records. After removal of 255 duplicates, 486 records were screened by title and abstract. Of these, 162 were excluded and 324 advanced to full-text review. Full text was retrieved for 165 reports, whereas 159 reports were not retrieved through the specified retrieval routes. Of the 165 full-text reports assessed, 78 were included and 87 were excluded. Reasons for full-text exclusion were no rehabilitation-relevant information (n = 72), diagnosis not consistent with Wallenberg syndrome (n = 13), and review, editorial, or commentary (n = 2). In the paired independent reviewer-decision logs, agreement was 90.3% for human title/abstract screening (Cohen's kappa = 0.82; n = 434) and 94.4% for full-text eligibility screening (Cohen's kappa = 0.89; n = 160).
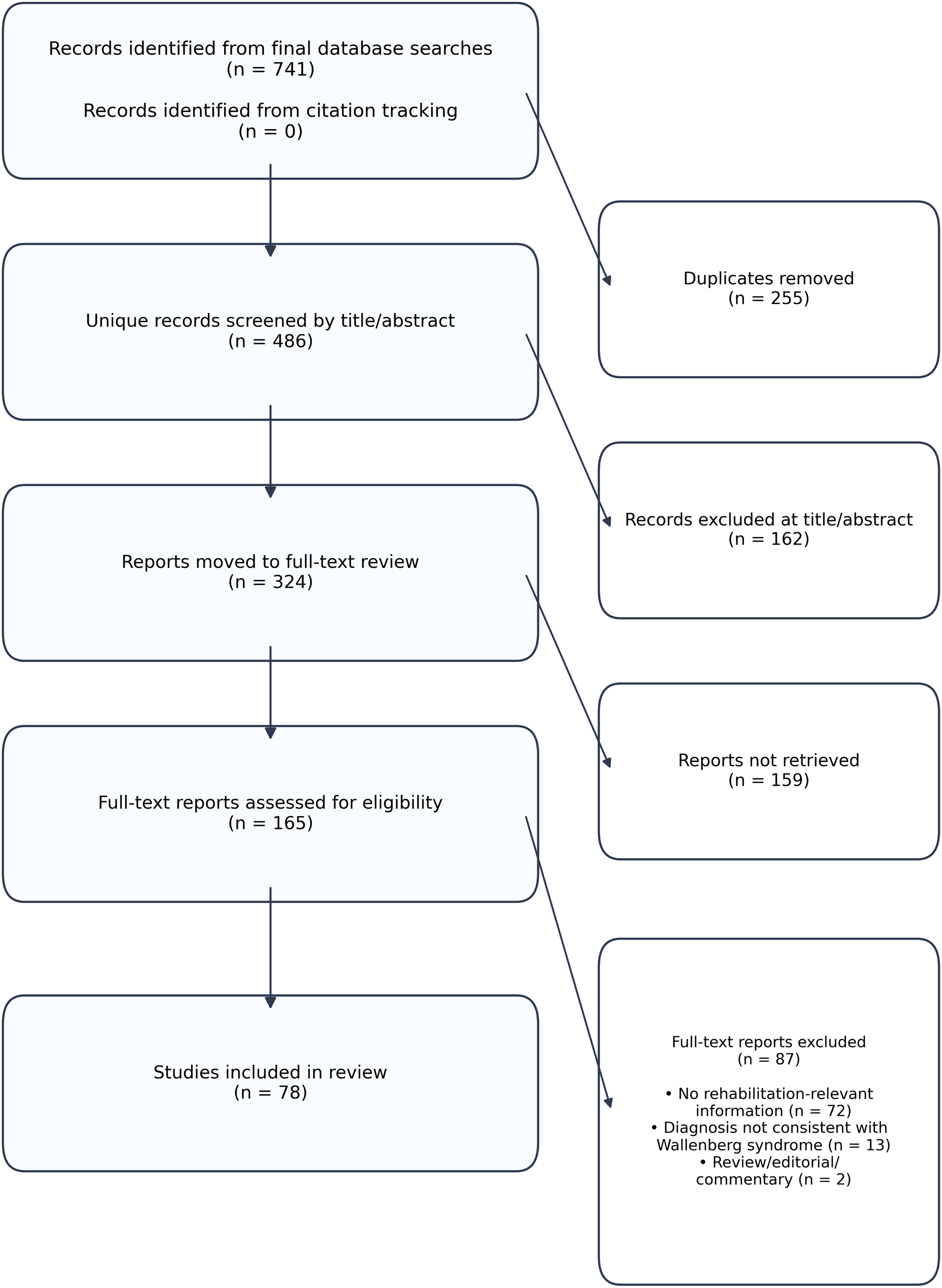
Source-selection flow diagram. Integrated counts include the Cumulative Index to Nursing and Allied Health Literature supplementary search; database-specific screening decisions are described in the Results and Supplementary Table S3.
The Cumulative Index to Nursing and Allied Health Literature search identified 63 records. Twenty-nine were duplicates of existing records or existing full-text candidates, 23 were excluded at title/abstract screening, and 11 were new full-text candidates. Of these 11 reports, three were newly included, one was excluded after full-text assessment, and seven were not retrieved. One previously unretrieved report was retrieved during this supplementary process and moved to the included set. Backward and forward citation tracking did not identify additional unique eligible records.
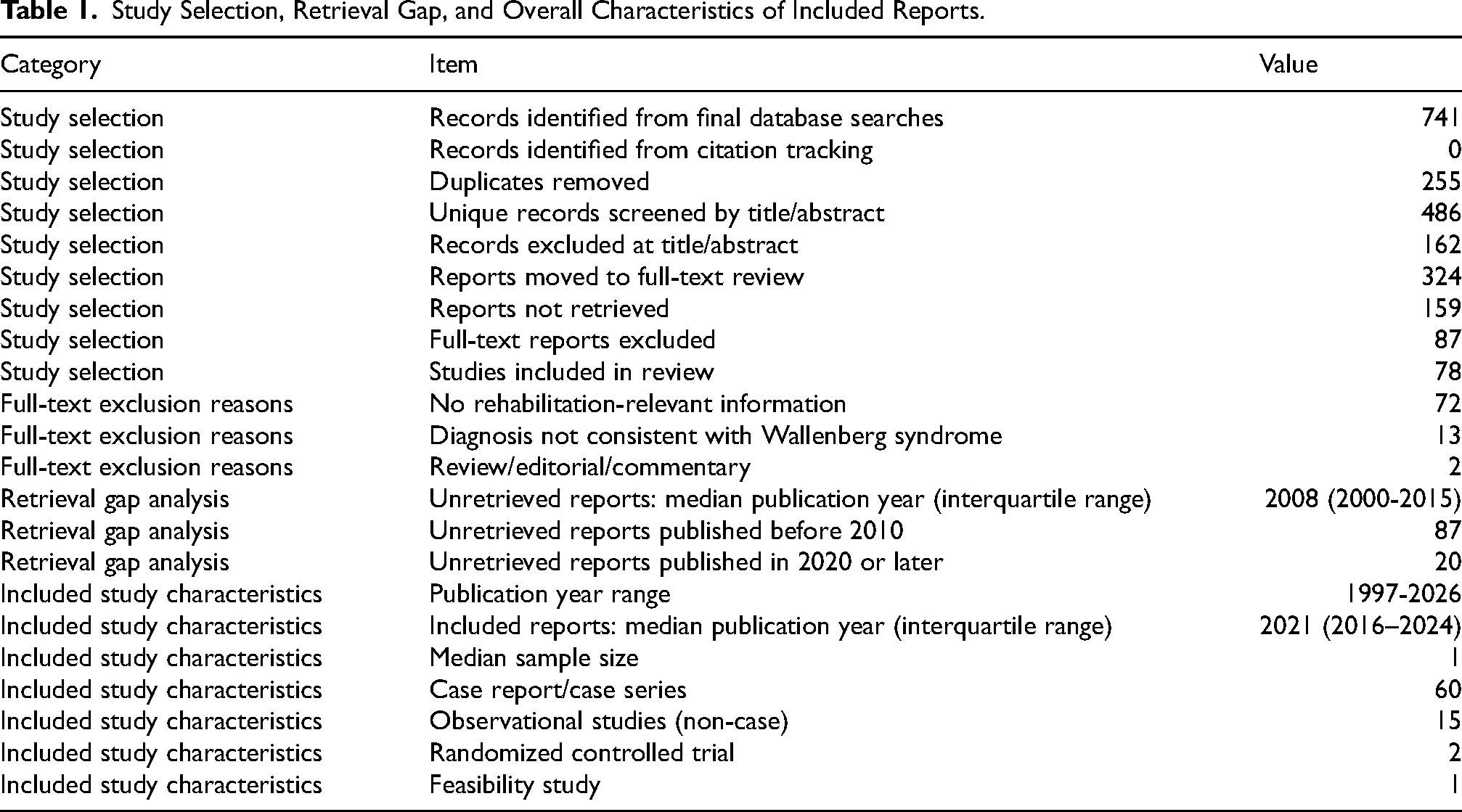
The 159 unretrieved reports were older than the included reports. The median publication year of unretrieved reports was 2008 (interquartile range, 2000–2015); 87 were published before 2010, and only 20 were published in 2020 or later. The median publication year of included reports was 2021 (interquartile range, 2016–2024). This pattern suggests that the retrieval gap mainly affects historical completeness. However, because retrieval status was determined before eligibility assessment, some unretrieved reports may have contained rehabilitation-relevant information, and less accessible non-English sources may have been underrepresented at full-text assessment and charting. The present map should therefore be interpreted as an accessible-literature map rather than a complete historical census. (Table 1)
Study Selection, Retrieval Gap, and Overall Characteristics of Included Reports.
Characteristics and Reporting Function
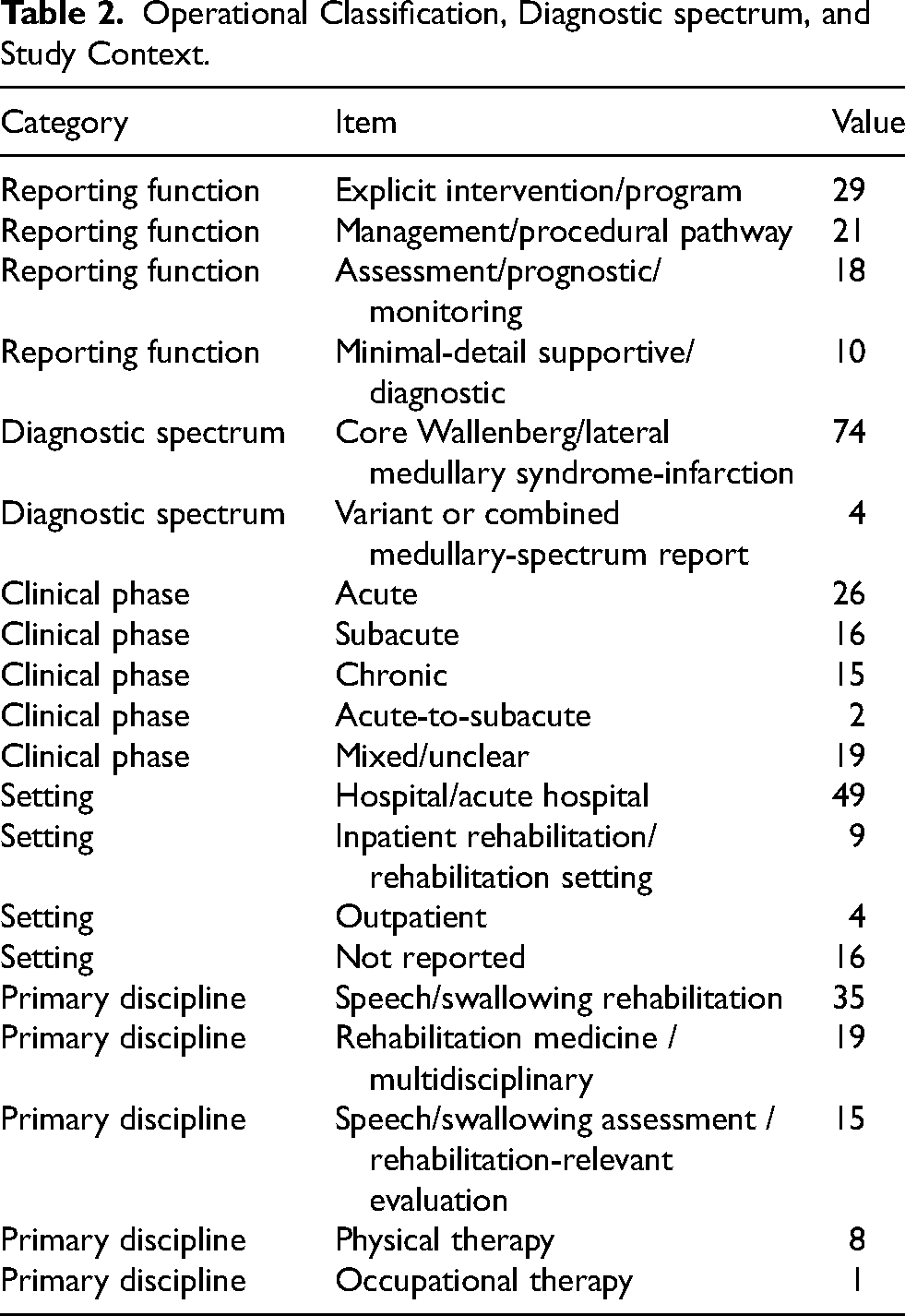
The 78 included reports were published from 1997 to 2026; 48 were published in 2020 or later. Sixty reports were case reports or case series, 15 were non-case observational studies, two were randomized controlled trials, and one was a feasibility study. Clinical phases were acute (n = 26), subacute (n = 16), chronic (n = 15), acute-to-subacute (n = 2), and mixed/unclear (n = 19). Settings were hospital/acute hospital (n = 49), inpatient rehabilitation/rehabilitation setting (n = 9), outpatient (n = 4), and not reported (n = 16).
By primary reporting function, 29 reports were explicit intervention/program reports, 21 were management/procedural pathway reports, 18 were assessment/prognostic/monitoring reports, and 10 were minimal-detail supportive/diagnostic reports. Thus, the 78 included reports should not be read as 78 direct intervention studies. Four reports were classified as variant or combined medullary-spectrum reports, including Opalski syndrome, atypical Avellis syndrome, dorsolateral medullary hemorrhage, and combined Millard-Gubler and Wallenberg syndromes (Khan et al., 2023; Nirlu et al., 2019; Yoshii et al., 2020; Zhu et al., 2022). (Table 2)
Operational Classification, Diagnostic spectrum, and Study Context.
Domain Distribution and Intervention Evidence
When non-mutually exclusive target domains were counted, dysphagia appeared in 63 reports, gait in 22, lateropulsion/balance in 16, autonomic or other rehabilitation-relevant management in eight, activities of daily living in six, and sensory dysfunction in three. However, only 22 of the 63 dysphagia reports were explicit intervention/program reports; the remainder were management/procedural pathway (n = 16), assessment/prognostic/monitoring (n = 16), or minimal-detail supportive/diagnostic (n = 9) reports. In the explicit-intervention-only evidence map, dysphagia reports were concentrated in the subacute and chronic phases (n = 9 and n = 10), whereas lateropulsion/balance and gait explicit-intervention reports were concentrated in the subacute phase (n = 5 and n = 6). No explicit intervention/program report addressed sensory dysfunction in any phase. This pattern supports the interpretation that dysphagia is the most frequently reported domain overall, but that the domain count should not be equated with direct intervention evidence. (Figures 2 and 3)
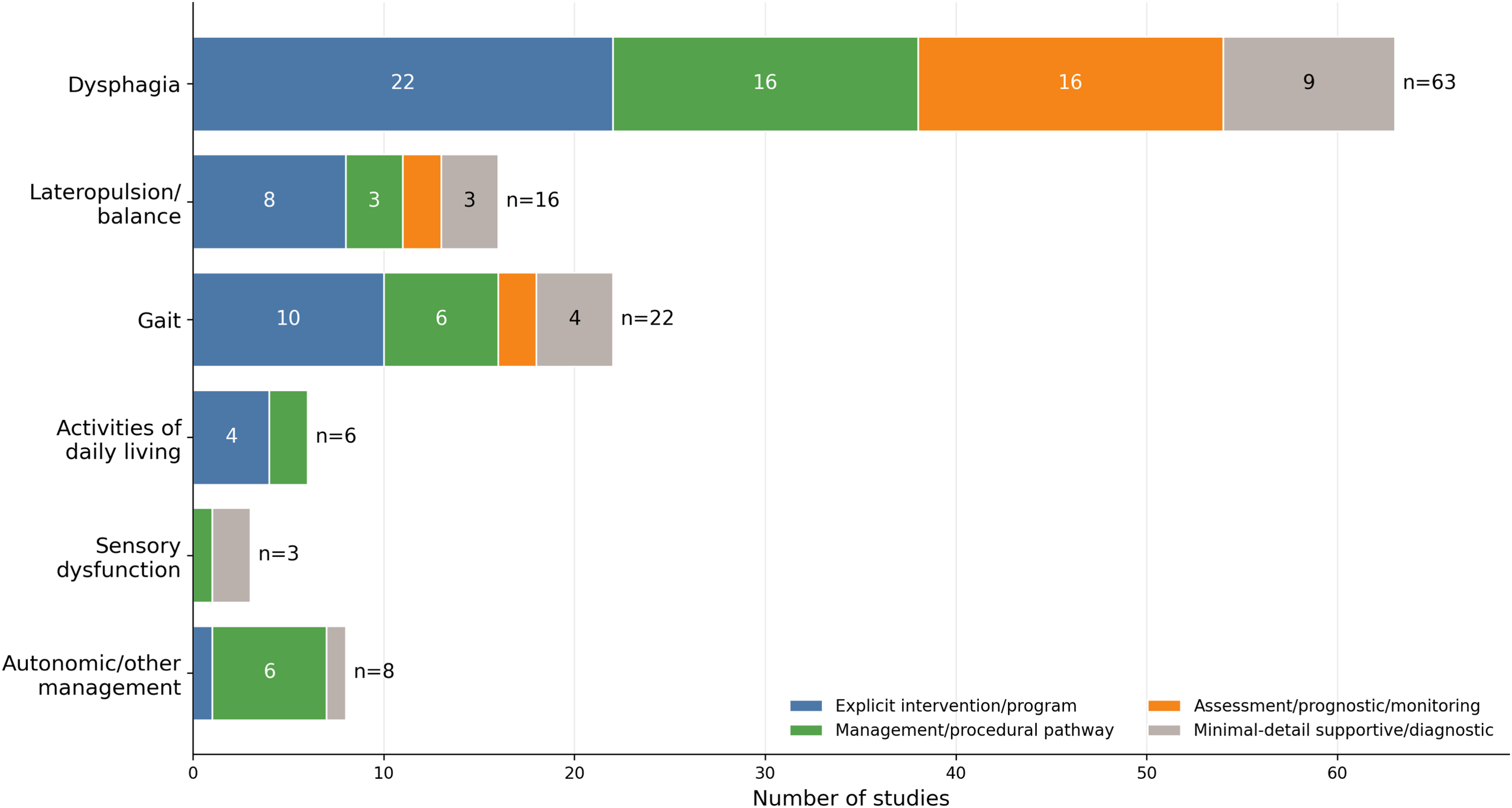
Reporting function within each target domain. Domain counts are non-mutually exclusive. Colors denote the operational categories: blue indicates explicit intervention/program, green indicates management/procedural pathway, orange indicates assessment/prognostic/monitoring, and gray indicates minimal-detail supportive/diagnostic. Small segments are shown without internal labels when needed to avoid crowding; exact counts are provided in Table 3.
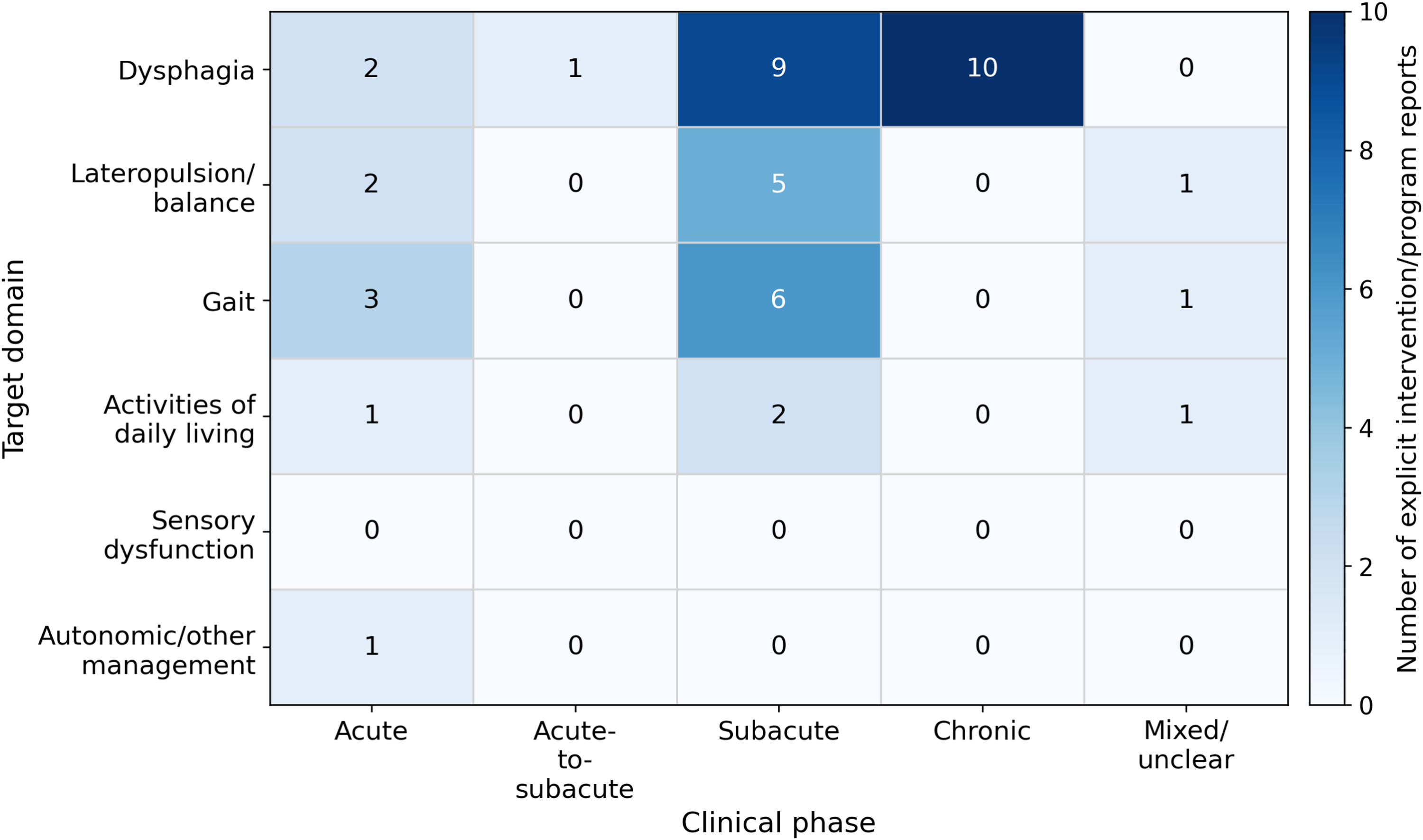
Evidence map of explicit intervention/program reports across clinical phase and target domain. Cell numbers and shading indicate the number of explicit intervention/program reports; darker blue indicates a larger count, and cells labelled 0 indicate no explicit intervention/program report. Counts are non-mutually exclusive across target domains.
Reporting Function Within Each Target Domain.
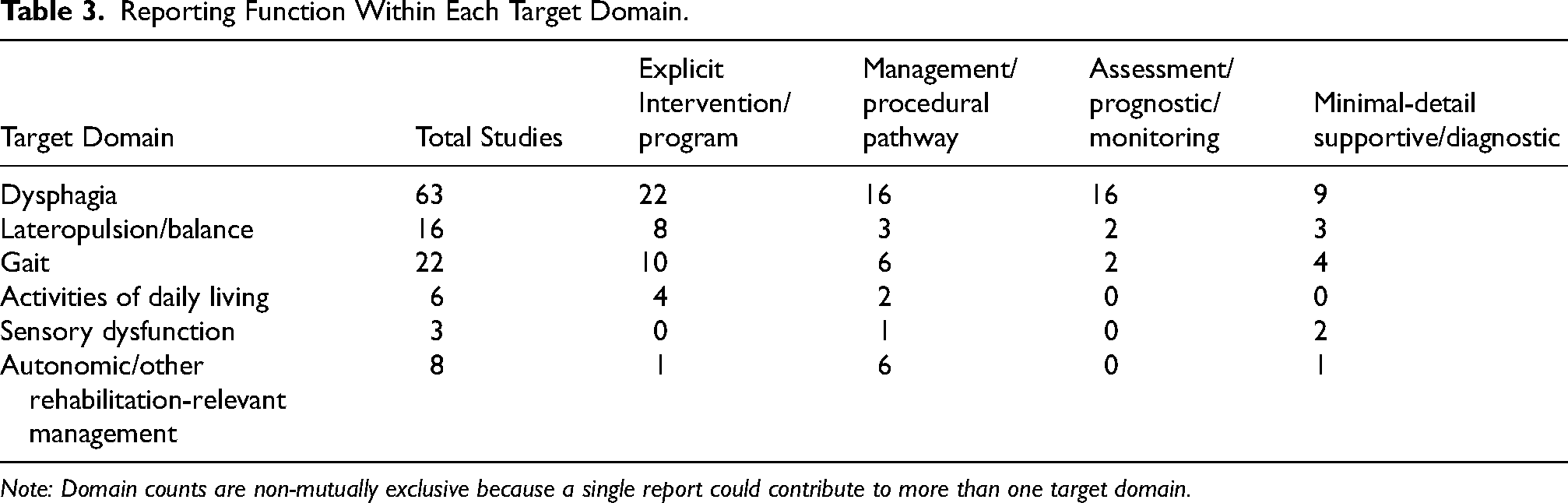
Note: Domain counts are non-mutually exclusive because a single report could contribute to more than one target domain.
Dysphagia-Related Literature
Dysphagia-related reports included a substantial assessment and prognostic literature. Studies addressed acute disconnection of premotor neuronal networks for swallowing, central control of swallowing, lesion-severity relationships, disruption of obligatory swallowing sequences, temporal characteristics of penetration and aspiration, diffusion tensor tractography, and cortical activation or connectivity during swallowing (Aydogdu et al., 2001; Cho et al., 2020; Dai et al., 2024; Jang et al., 2021; Kim et al., 2018; Kim et al., 2020; Li et al., 2025; Martino et al., 2001; Nakao et al., 2019; Oshima et al., 2013).
Explicit intervention/program reports included a randomized controlled trial of motor imagery based on action observation added to conventional dysphagia therapy, a brainstem infarction trial of repetitive transcranial magnetic stimulation that included a lateral medullary infarction subgroup (n = 11), biofeedback combined with functional electrical stimulation, oral motor facilitation technique with neuromuscular electrical stimulation, transcutaneous vagus nerve stimulation, vacuum swallowing, rehabilitation nutrition, and chronic-stage individualized rehabilitation (Gupta et al., 2025; Jakobsen et al., 2021; Khedr & Abo-Elfetoh, 2010; Kunieda et al., 2022; Son et al., 2022; Wakabayashi et al., 2021; Wang et al., 2024; Yuan et al., 2019). Management/procedural pathways included serial videofluoroscopic swallowing study or modified barium swallow guided feeding decisions, gastrojejunostomy or nasogastric feeding, pediatric multimodal intervention, early endoscopic intervention, balloon dilatation, cricopharyngeal botulinum toxin injection, cricopharyngeal myotomy, and swallowing surgery cohorts (Brooks et al., 2022; Chiti-Batelli & Delap, 2001; Finestone et al., 1999; Kang et al., 2019; Taniguchi et al., 2024). The boundary between conservative swallowing rehabilitation and procedure-led management was therefore not always sharp.
Lateropulsion, Gait, Daily Activities, and Safety Management
Explicit intervention/program reports for lateropulsion/balance and gait described physical therapy follow-up using center of pressure velocity, vestibular or postural control therapy, acute physiotherapy programs, lower-limb task-oriented exercise, interdisciplinary inpatient rehabilitation, task-oriented occupational therapy, Cawthorne-Cooksey exercises, and sensory stimulation with a hanger placed around the head (Chan, 2009; Dharmavel et al., 2024; Harayama et al., 2025; Herson et al., 2023; Kariya et al., 2024; Matsumura et al., 2025; Matsuo et al., 2022; Na et al., 2011; Song et al., 2026; Ye et al., 2024). Dosage reporting was incomplete. Among 10 explicit intervention/program reports that included lateropulsion/balance or gait, frequency was reported in seven, intensity in four, session duration in one, and total duration in three. Most reports were single cases or small case series, limiting dose-response interpretation.
Safety management was concentrated around dysphagia. Aspiration risk monitoring was described in 38 reports, enteral feeding support during severe dysphagia in 37, and instrumental swallowing monitoring in 31. Bladder management was reported in 13 reports, respiratory monitoring or management in eight, and compensatory posture for safer swallowing in seven. Reports describing lateropulsion with atonic bladder, urinary retention, central hypoventilation, central alveolar hypoventilation, and central sleep apnea indicate that rehabilitation-relevant management extends beyond swallowing care (Hayashi et al., 2024; Jeong et al., 2016; Maeda et al., 2025; Mishina et al., 2014; Tanaka et al., 2016). Outcome measures included videofluoroscopic swallowing study in 19 reports, Functional Oral Intake Scale in 10, Penetration-Aspiration Scale in nine, fiberoptic endoscopic evaluation of swallowing in five, and Functional Independence Measure in five. (Table 4)
Reported Outcome Measures and Safety Management among all Included Reports.
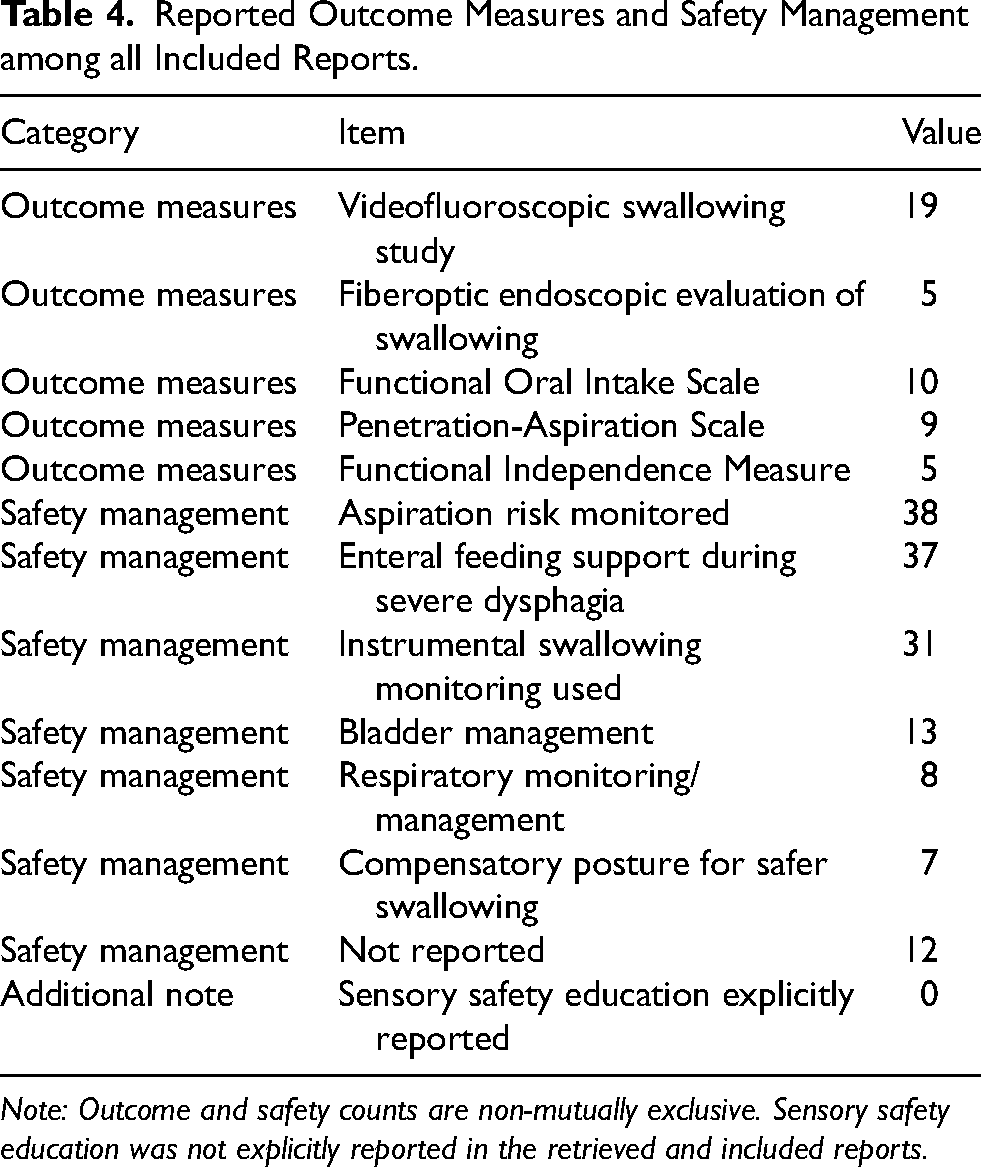
Note: Outcome and safety counts are non-mutually exclusive. Sensory safety education was not explicitly reported in the retrieved and included reports.
Discussion
This review shows that the accessible rehabilitation-relevant literature for lateral medullary stroke/Wallenberg syndrome is not merely small; it is functionally mixed. Among 78 included reports, only 29 were explicit intervention/program reports, and 60 were case reports or case series. The predominance of case reports and case series means that clinical decision-making cannot be based on comparative effectiveness or dose-response evidence for most domains. Therefore, the presence of 63 dysphagia-related reports should not be interpreted as 63 dysphagia intervention studies, and evidence density in these maps indicates where reports exist rather than which intervention should be preferred. Separating overall rehabilitation-relevant literature from direct intervention evidence makes the map more clinically interpretable.
The large size of the dysphagia literature is understandable because dysphagia in Wallenberg syndrome affects aspiration risk, nutrition route, pneumonia risk, oral-intake progression, and the indication for procedures. Dysphagia reports in this review frequently linked serial videofluoroscopic swallowing study or fiberoptic endoscopic evaluation of swallowing, tube feeding, postural compensation, botulinum toxin injection, myotomy, and swallowing surgery within the same care pathway. This pattern suggests that dysphagia rehabilitation for Wallenberg syndrome is often managed as a pathway that combines assessment, safety management, and intervention rather than as an isolated training technique. The two randomized trials should also be interpreted cautiously: one enrolled patients with Wallenberg syndrome, whereas the repetitive transcranial magnetic stimulation study was a mixed brainstem infarction trial that included a lateral medullary infarction subgroup (Khedr & Abo-Elfetoh, 2010; Wang et al., 2024).
Lateropulsion/balance and gait had fewer reports than dysphagia, but the available reports more often described explicit therapy content. The link between assessment and intervention was clearer in some physical therapy and occupational therapy reports using posturography, modified Clinical Test of Sensory Interaction and Balance, Berg Balance Scale, or functional mobility outcomes (Chan, 2009; Dharmavel et al., 2024; Harayama et al., 2025; Herson et al., 2023; Kariya et al., 2024; Matsumura et al., 2025; Matsuo et al., 2022; Na et al., 2011; Song et al., 2026; Ye et al., 2024). However, reproducible dosage information remained incomplete. Activities of daily living and participation were also under-reported, with only six reports including activities of daily living as a target domain and only five reports using the Functional Independence Measure. From the perspective of the International Classification of Functioning, Disability and Health, the literature remains weighted toward body function, with limited connection to activity and participation. Future physical and occupational therapy reports could use wearable inertial sensors, instrumented gait analysis, posturography, and activity monitoring to quantify lateropulsion, walking exposure, and participation, but these measures should be paired with clinically meaningful outcomes, adverse-event reporting, and discharge function.
The absence of explicit sensory safety education is clinically important. No included report described sensory safety education as a reproducible component. This does not prove that clinicians neglect sensory risk in practice; it more likely indicates that daily-life precautions for thermal injury, trauma, reduced temperature sensation, and impaired sensory input during gait are not being treated as reportable rehabilitation units. Autonomic and respiratory management reports also demonstrate why rehabilitation should not be defined only as hands-on training. Bladder management and respiratory monitoring can determine whether mobilization, swallowing progression, and discharge planning are safe.
For clinical reporting, the practical next step is not only to test new techniques but also to describe care pathways in a reproducible way. In a rare syndrome, well-described single cases can support later comparative work if they record lesion topography, clinical phase, baseline severity, intervention start and stop criteria, frequency, intensity, session duration, total duration, concurrent safety management, instrumental reassessment timing, adverse events, discharge function, and activities of daily living or participation outcomes. These reporting items should be treated as a minimum foundation for future comparative cohorts and randomized controlled trials: without standardized baseline severity, treatment dose, start/stop criteria, concurrent safety management, and follow-up outcomes, trial protocols cannot be replicated, pooled, or interpreted across sites. The reporting function framework used in this review may help future evidence maps separate direct interventions from management and assessment literature, but future reviews should predefine independent coding logs and report chance-corrected agreement statistics when similar operational categories are used.
Several limitations should be considered. First, 159 of 324 reports that advanced to full-text review were not retrieved through the specified retrieval routes. These reports were older than included reports, suggesting that the retrieval gap mainly affects historical completeness, but older reports may still contain clinically relevant information. Second, although no language limits were applied during database searching, full-text inclusion depended on languages that could be assessed by the review team; reports in other languages may therefore have been underrepresented at eligibility assessment and charting. Third, the Cumulative Index to Nursing and Allied Health Literature was added after protocol finalization and before final synthesis; the eligibility criteria were unchanged, but the title/abstract field strategy may still have missed practice-oriented reports. Fourth, a dedicated grey literature search was not conducted, and Embase, Scopus, PEDro, and OTseeker were not searched. Fifth, reporting-function and diagnostic-spectrum categories were introduced during charting and synthesis as operational refinements; final classification was consensus-based, and classification-specific percent agreement and Cohen's kappa were not calculated. Screening and full-text eligibility agreement statistics therefore should not be interpreted as reliability statistics for the post hoc reporting-function framework. Finally, charting depended on what each report described, and formal critical appraisal was not conducted. The absence of critical appraisal means that a dense cell in the evidence map should not be interpreted as high-quality evidence or low risk of bias. The review should therefore be interpreted as a map of accessible and contemporary rehabilitation-relevant literature rather than as a complete historical review or as evidence of intervention effectiveness. Within that scope, the findings show that future reports should distinguish direct intervention evidence from management and assessment literature and should describe dosage, safety management, reassessment timing, discharge function, sensory safety education, and daily-life precautions as reproducible reporting units.
Supplemental Material
sj-docx-1-nre-10.1177_10538135261459633 - Supplemental material for Rehabilitation and Management in Lateral Medullary Stroke (Wallenberg Syndrome): A Scoping Review and Evidence Map
Supplemental material, sj-docx-1-nre-10.1177_10538135261459633 for Rehabilitation and Management in Lateral Medullary Stroke (Wallenberg Syndrome): A Scoping Review and Evidence Map by Takafumi Izutsu, Nobuo Kutsuna, Syota Toyama, Kasumi Fujiwara, Kosei Goto and Takao Nakamura in NeuroRehabilitation
Supplemental Material
sj-xlsx-2-nre-10.1177_10538135261459633 - Supplemental material for Rehabilitation and Management in Lateral Medullary Stroke (Wallenberg Syndrome): A Scoping Review and Evidence Map
Supplemental material, sj-xlsx-2-nre-10.1177_10538135261459633 for Rehabilitation and Management in Lateral Medullary Stroke (Wallenberg Syndrome): A Scoping Review and Evidence Map by Takafumi Izutsu, Nobuo Kutsuna, Syota Toyama, Kasumi Fujiwara, Kosei Goto and Takao Nakamura in NeuroRehabilitation
Footnotes
Ethical Considerations
This scoping review used published literature only and did not involve new collection of individual participant data; ethics approval was not required.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
Takafumi Izutsu: Conceptualization, Investigation (title/abstract screening, full-text review, data charting), Data curation, Writing - original draft, Writing - review and editing.
Nobuo Kutsuna: Conceptualization, Methodology, Investigation (adjudication of screening and charting disagreements), Supervision, Project administration, Writing - review and editing.
Syota Toyama: Investigation (title/abstract screening, full-text review, data charting verification), Data curation, Writing - review and editing.
Kasumi Fujiwara: Investigation, Writing - review and editing.
Kosei Goto: Conceptualization, Writing - review and editing.
Takao Nakamura: Methodology, Writing - review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Study-level characteristics, the list of reports not retrieved through the specified retrieval routes, protocol amendments and analytic refinements, the data charting form, final search strategies, operational definitions, and source-selection inter-rater agreement statistics are provided in the supplementary material and in an anonymized review workbook submitted as ![]() . The workbook contains the final selection-flow summary, inter-rater agreement summary, included-report charting table, unretrieved-report list, protocol amendments, data charting form, search strategies, operational definitions, and audit summary. The completed Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews checklist is provided as a separate reporting-guideline checklist file. The protocol file and amendment log can be provided to the journal as confidential editor-only materials if required.
. The workbook contains the final selection-flow summary, inter-rater agreement summary, included-report charting table, unretrieved-report list, protocol amendments, data charting form, search strategies, operational definitions, and audit summary. The completed Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews checklist is provided as a separate reporting-guideline checklist file. The protocol file and amendment log can be provided to the journal as confidential editor-only materials if required.
Protocol Registration
The review protocol was registered in the Open Science Framework before formal study selection. Registration record: ![]() . If the public record remains under embargo at submission, the protocol file and amendment log should be uploaded as confidential editor-only materials to preserve double-anonymized peer review.
. If the public record remains under embargo at submission, the protocol file and amendment log should be uploaded as confidential editor-only materials to preserve double-anonymized peer review.
Use of Artificial Intelligence
A large language model-based generative artificial intelligence tool was used solely to translate the manuscript from Japanese into English and to correct grammar and phrasing in the translated text. The tool was not used in the design of the review, the development of the research questions or eligibility criteria, the search strategy, source selection, data charting, synthesis, or interpretation of findings. All conceptual and analytical work was performed by the authors. The translated text and all editorial suggestions were reviewed by the authors, who verified all data, references, and conclusions against the original source documents and charting records. The authors take full responsibility for the integrity and accuracy of the final manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.