
Abstract
Background
Although several studies have examined gait changes associated with continuous intrathecal baclofen (CITB) infusion for spasticity in ambulatory patients with acquired brain injury (ABI), none has included a control group.
Objective
To assess long-term changes in gait kinematics associated with CITB infusion for post-ABI spasticity.
Methods
Forty-three consecutive ABI patients underwent gait evaluations during an ITB bolus trial, with follow-up gait data available in 17 pump recipients (re-evaluated 24 ± 17 months after implantation, dose range 95–590 µg/day) and 8 non-recipients (re-evaluated 30 ± 19 months after screening). Temporospatial gait parameters and lower extremity joint range of motion (ROM) were analyzed.
Results
Changes in temporospatial gait parameters from baseline to follow-up did not differ significantly between pump recipients and non-recipients. Likewise, there were no significant between-group differences in changes in ROM over time except for a 7.5° increase in more-affected (MA) knee ROM during swing in pump recipients, compared with a 2.4° decrease in non-recipients (ANOVA group×time interaction, P = 0.027). Secondary analyses showed that baseline average Ashworth score in the MA leg correlated significantly with changes in MA stance time and less-affected initial double support time (r ≥ |0.56|, P ≤ 0.029) in pump recipients only.
Conclusions
The modest improvements in gait kinematics in pump recipients appeared to have limited clinical significance, considering no concurrent improvements in average gait speed and the study limitations. The overall results suggest that gait speed may be useful for goal setting, but it should not be considered the sole measure of CITB efficacy.
Introduction
Continuous intrathecal baclofen (CITB) infusion is an effective treatment option for reducing severe spasticity (Albright et al., 2003; Saulino et al., 2016). CITB exerts its therapeutic effect by delivering baclofen directly into the cerebrospinal fluid via an implanted pump-catheter system (Heetla et al., 2014; Saulino et al., 2011), thereby minimizing systemic side effects (Müller et al., 1988). CITB may also improve motor function, comfort, quality of life, and ease of caregiving (Creamer et al., 2018; Francisco et al., 2007; Masrour et al., 2024; Ordia et al., 2002).
While gait patterns may improve in patients within hours after an ITB screening bolus injection (Horn et al., 2005; Horn et al., 2010; Park & Song, 2024; Rémy-Néris et al., 2003), long-term outcomes with CITB infusion have been mixed across diverse neurological populations (Lee et al., 2023). Long-term follow-up gait studies after acquired brain injury (ABI) are particularly scarce. To date, the only ABI data come from two stroke cohorts evaluated at 4–25 months and 3–12 months post-implantation (Francisco & Boake, 2003; Schiess et al., 2011). Both studies demonstrated significant increases in gait speed, derived from 50-foot walk time or 6-min walk time.
Corresponding long-term CITB gait studies are limited in other neurological populations. Using the 25-foot or 10-meter walk time to assess walking speed, three multiple sclerosis studies reported non-significant changes in gait speed at 1-year post-implantation (Abbatemarco et al., 2021; Lee et al., 2018; Sammaraiee et al., 2020). In contrast, two case studies of hereditary spastic paraplegia found an increase in gait speed along with favorable kinematic changes such as increased knee flexion during stance and swing at 6 and 12 months post-implantation, respectively (Heetla et al., 2015; Molteni et al., 2005). In 19 children with cerebral palsy, CITB significantly improved knee flexion at initial contact without affecting gait speed at 2.8 ± 1.9 years post-implantation (Pruszczynski et al., 2018).
Studying gait beyond speed is warranted because gait speed may not be a sufficiently responsive measure for revealing changes in gait patterns (Cofré Lizama et al., 2019). Quantitative gait analysis provides a comprehensive assessment of movement biomechanics, allowing identification of gait deviations, development of treatment plans, and evaluation of outcomes (Wren et al., 2011). Previous studies have reported improvements in gait patterns in ABI subjects after ITB bolus injections. Along with an increase in gait speed, an increase in stride length, but not in cadence, was found after a bolus injection (Horn et al., 2005). A bilateral increase in ankle ROM (Horn et al., 2010) and increases in both minimal knee extension and maximal ankle dorsiflexion of the more-affected side when walking at maximum speed (Rémy-Néris et al., 2003) were reported in ABI post-ITB bolus injection. The stroke patient in a case report experienced an increase in maximum knee flexion during swing on the more affected side after 4 consecutive days of ITB bolus injections (Kim et al., 2024). Notably, no CITB study with ABI has comprehensively examined long-term changes in gait kinematics beyond gait speed. Furthermore, no prior study has included a control group, making it uncertain to what extent observed gait changes can be attributed specifically to CITB infusion.
Our longitudinal study of patients with ABI, whose clinical characteristics and responses to an ITB screening bolus trial suggested potential benefits of CITB infusion on dynamic spasticity and gait, provided a unique opportunity to compare treated and untreated patients. The treated cohort consisted of patients who underwent gait evaluation before and after the bolus trial, subsequently received a pump, and were re-evaluated months later while maintained on a stable CITB dose (pump recipients). The untreated (control) cohort included patients who completed gait evaluation during the bolus trial but did not receive a pump and were re-evaluated at a later time point (pump non-recipients). Accordingly, for the first time, longitudinal changes in temporospatial gait parameters and lower-extremity joint range of motion (ROM) were directly compared between the pump recipients and non-recipients.
Based on prior studies reporting improvements in gait patterns as a result of ITB bolus administration (Horn et al., 2005; Horn et al., 2010; Kim et al., 2024; Rémy-Néris et al., 2003) and CITB infusion (Francisco & Boake, 2003; Schiess et al., 2011) in patients with ABI, we hypothesized that CITB infusion would increase gait speed, stride length, and joint ROM during gait, resulting in significant differences between pump recipients and non-recipients. In the secondary analyses, we examined associations between baseline muscle hypertonia, CITB dose, and changes in gait outcomes.
Methods
Participants
From a pool of 43 consecutive ABI patients managed by the same clinical team, 17 pump recipients and 8 non-recipients were included in this retrospective cohort study (Table 1, Figure 1). Inclusion criteria for all participants were the ability to walk safely with or without assistive devices during an ITB screening trial, a positive clinical response to ITB bolus injection, and completion of a motion capture gait evaluation during the screening trial and at follow-up. The additional criteria for pump recipients were successful implantation of the drug delivery system (Medtronic Synchromed, Medtronic Inc, Minneapolis, MN) and no clinical evidence of the system malfunction at the time of follow-up. None of the authors was affiliated with the pump manufacturer. However, one of the investigators led a team that participated in dose titration and troubleshooting of the implanted system. The implantation took place 56 ± 40 months after ABI. The catheter tip was between T6 and T10 in 12 participants and between T4 and C7 in three participants (unknown in two). Pump recipients were initially titrated with a simple CITB mode, with flex dosing employed later in three. CITB dose was adjusted based on clinical assessment of tone, strength, and side effects. The study was approved by the institutional review board for human research, and all participants signed the informed consent.
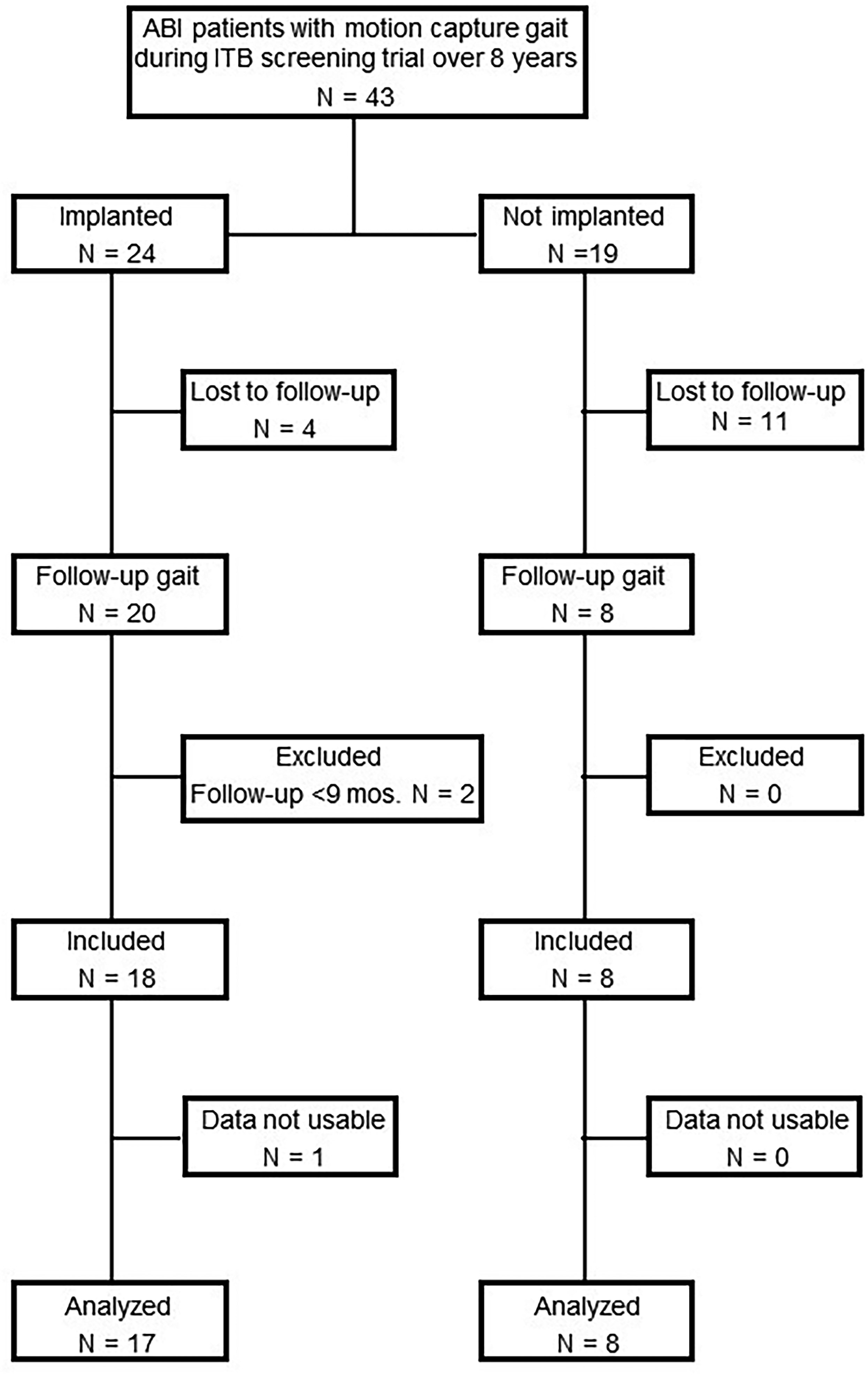
Flowchart describing the acquired brain injury (ABI) participants included and excluded in the current study.
Characteristics of Study Participants (Age at Baseline [BSL] in Years, All Other Times in Months).
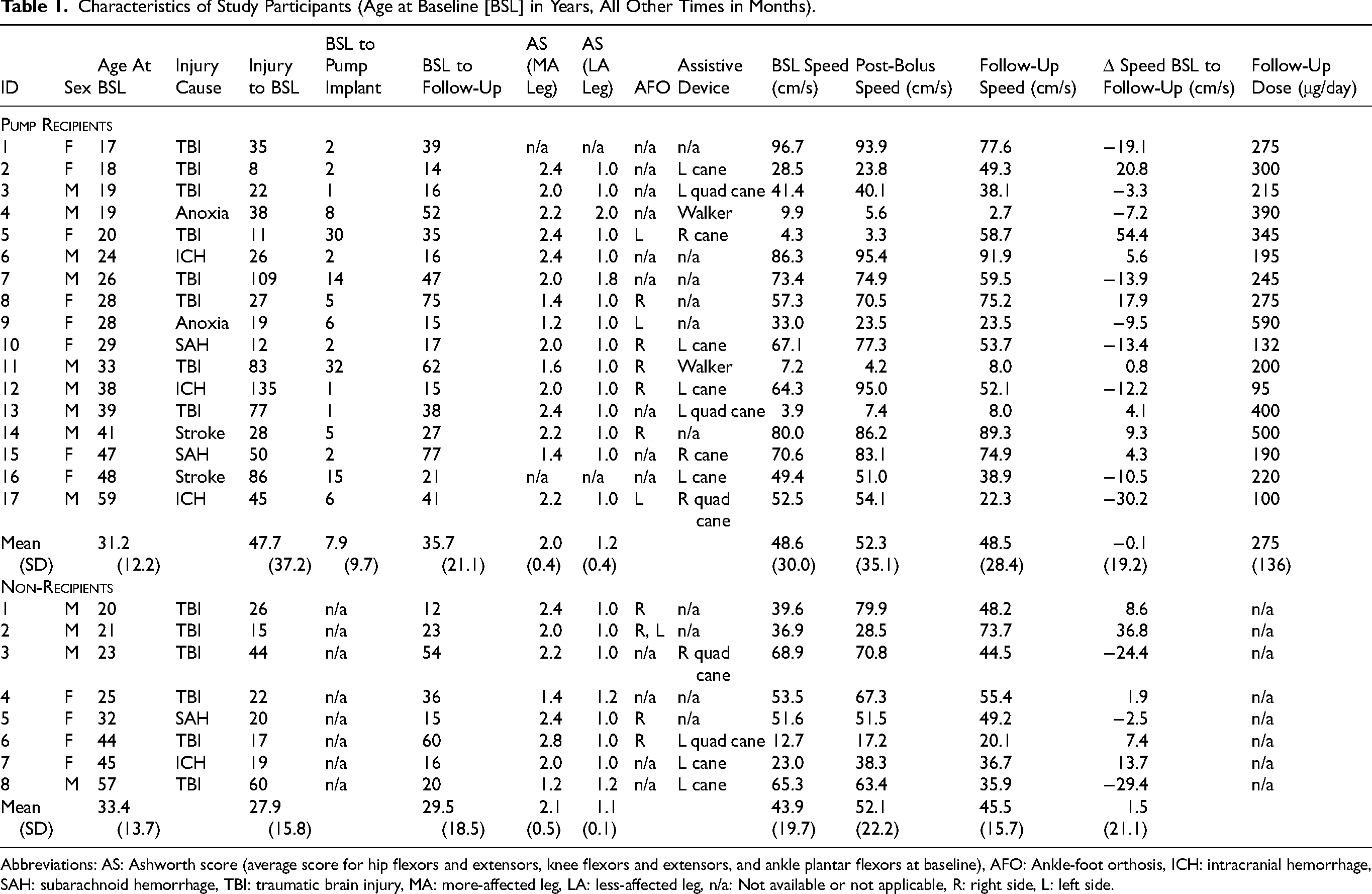
Abbreviations: AS: Ashworth score (average score for hip flexors and extensors, knee flexors and extensors, and ankle plantar flexors at baseline), AFO: Ankle-foot orthosis, ICH: intracranial hemorrhage, SAH: subarachnoid hemorrhage, TBI: traumatic brain injury, MA: more-affected leg, LA: less-affected leg, n/a: Not available or not applicable, R: right side, L: left side.
Gait Assessment
Kinematics data were collected using eight digital cameras (Motion Analysis Corp, Rohnert Park, CA) sampled at 60 Hz. Passive spherical reflective markers were affixed to body landmarks according to the Helen Hayes marker set (Kadaba et al., 1990). Five force plates (Type 4060; Bertec Corp, Columbus, OH) sampled at 1,200 Hz were utilized to determine critical gait instants.
The participants were instructed to walk at self-selected normal walking speed, beginning about 1 m outside a 7-m walkway and continuing without slowing down until they exited the walkway. They walked 4–5 times back and forth with short pauses after each pass using their own shoes and customary assistive devices or orthoses, if needed. From each data collection session, 10–25 gait cycles inside the walkway were analyzed in each participant.
Protocol
Gait was evaluated twice; first during the ITB bolus trial, with pre-injection data serving as the baseline, and again at follow-up. The interval between gait assessments did not differ significantly between the two groups (Table 1). During the ITB trial, gait and lower-limb hypertonia were assessed at baseline and 2, 4, and 6 h after the bolus injection. The baseline gait speed and the fastest post-injection speed were reported for descriptive purposes (Table 1). The average modified Ashworth score (Bohannon & Smith, 1987) in the hip flexors and extensors, knee flexors and extensors, and ankle plantar flexors at baseline was used to designate the more-affected (MA) and less-affected (LA) legs. When the Ashworth score was not collected (n = 2) or when differences were small (average difference ≤ 0.2, n = 5), MA and LA legs were determined from a combination of stance time (MA side has shorter stance time (Chow et al., 2010)) and gait video recordings (compensatory movements on the LA side). Hypertonia could not be assessed at follow-up due to the unavailability of therapists.
Data Reduction
OrthoTrak Gait Analysis software (Motion Analysis Corp) was used to process marker location and forceplate data. The OrthoTrak software utilized both ground reaction force and kinematic data to determine initial foot contact and toe-off, whereas marker locations were used to predict centers of the hip, knee, and ankle joints. The initial foot contact of the same foot defined a gait cycle. These data were used to determine gait speed, cadence, stride and step lengths, and time (percent of the gait cycle) spent in stance, initial double support, and single support. The ROM was computed as the difference between the largest and smallest joint angles during a specific phase of the gait cycle.
Statistical Analyses
To test the hypothesis that CITB infusion would increase gait speed, stride length, and joint ROM in pump recipients but not in non-recipients, a 2-group×2-time (baseline, follow-up) ANOVA with repeated measures on the time factor was conducted for each outcome measure. The group-by-time interaction was the primary focus, since our main interest was in the between-group differences over time.
To gain additional insights into the changes in gait speed over time, individual gait cycles were analyzed to determine the change in gait speed from baseline to follow-up for each participant. Because the number of gait cycles differed between sessions, data were evaluated with an independent t-test. The change in gait speed was categorized as increased (significantly faster, P ≤ 0.05), decreased (significantly slower, P ≤ 0.05), or unchanged (no statistical difference, P > 0.05). To determine whether receiving CITB was associated with a significant increase in gait speed, frequencies of speed increase vs. no increase (no change and decrease collapsed) were compared between the pump recipients and non-recipients using Fisher's exact test. The corresponding odds ratio was reported.
In the secondary analyses, Pearson product-moment coefficients of correlation were computed between changes in gait parameters and the mean baseline MA Ashworth score for each group separately, as well as with the CITB dose at the follow-up for pump recipients only. The correlation between the change in gait speed during the screening trial and the change in speed from baseline to post-CITB was also calculated.
Results were considered statistically significant at P ≤ 0.05. No adjustments were made for multiple comparisons due to the exploratory nature of this study.
Results
Mixed ANOVAs did not reveal any significant differences between pump recipients and non-recipients (i.e., no significant group effect) in any of the temporospatial and ROM measures (Tables 2 and 3). Significant main effects of time were found in the MA stance time (shorter at follow-up), LA single support time (longer at follow-up), MA ankle ROM during swing (larger at follow-up), and LA ankle ROM during single support (larger at follow-up). The only significant group×time interaction was detected in the MA knee ROM during swing (P = 0.027), with an increase for the pump recipients and a decrease for non-recipients from baseline to follow-up (Figure 2).
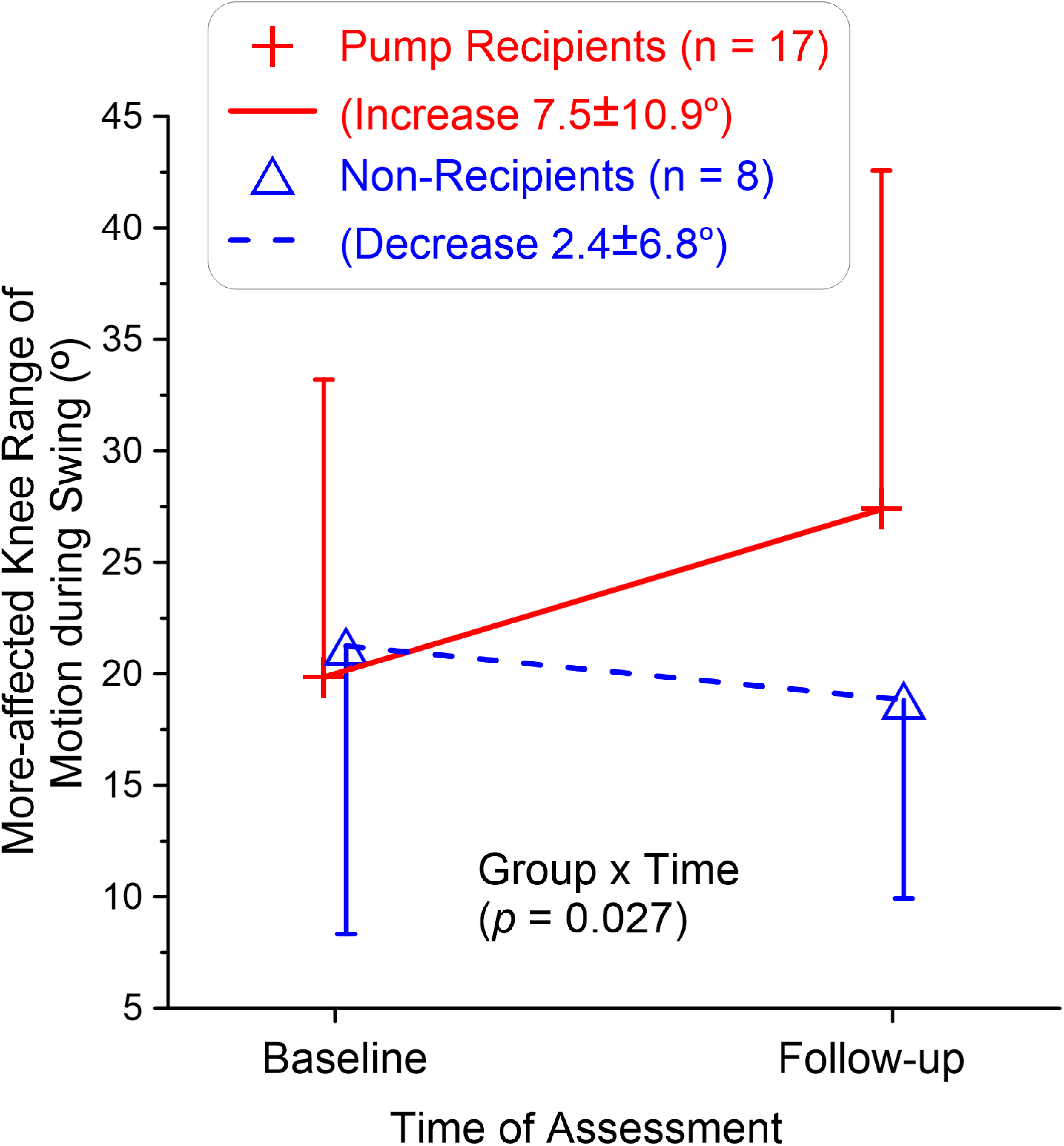
Significant interaction between group and time in the more-affected knee range of motion during swing. There was a trend of an increase from baseline to follow-up for the pump recipients and an opposite trend for the non-recipients.
Mean ± SD of Temporospatial Parameters for Pump Recipients and non-Recipients and p-Values of 2-way ANOVA Analysis for Each Parameter.
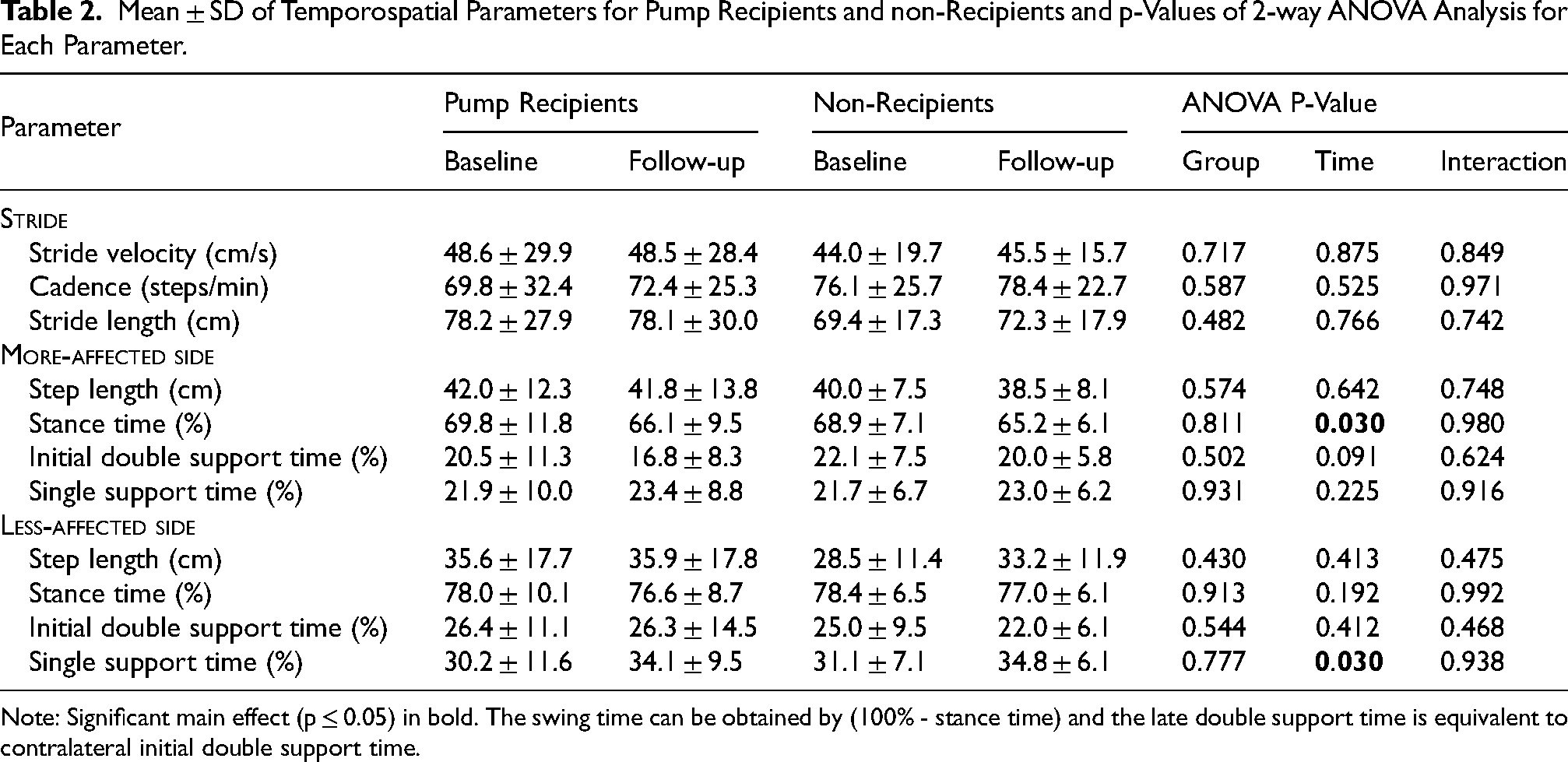
Note: Significant main effect (p ≤ 0.05) in bold. The swing time can be obtained by (100% - stance time) and the late double support time is equivalent to contralateral initial double support time.
Hip, Knee, and Ankle Range of Motion During Different Gait Phases for the More-Affected and Less-Affected Legs in Pump Recipients and non-Recipients (Mean ± SD) and p-Values of 2-way ANOVA Analysis for Each Parameter.
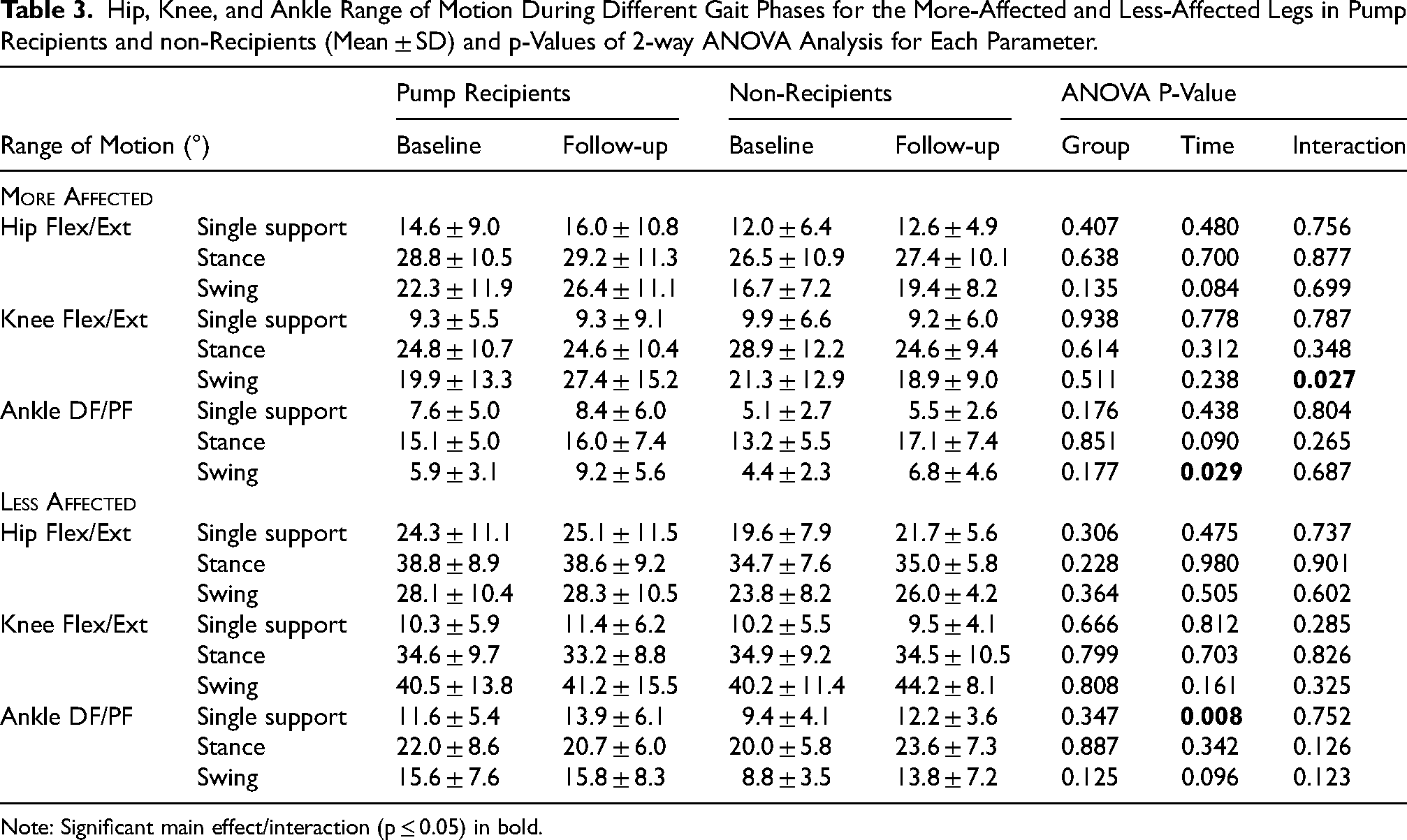
Note: Significant main effect/interaction (p ≤ 0.05) in bold.
Among the pump recipients, 6 (35%) participants significantly increased gait speed at the follow-up, 8 (47%) significantly decreased speed, and 3 (18%) did not significantly change speed. The respective frequencies in the non-recipients were 4 (50%), 2 (25%), and 2 (25%). The odds ratio for achieving an increase in gait speed with CITB administration was not significant (0.55, 95%CI 0.10 to 3.01, P = 0.667).
Secondary analyses revealed several moderate correlations that were only significant in pump recipients. The average baseline Ashworth score in the MA leg correlated negatively with the changes in MA stance time (r = −0.61, Figure 3a) and LA initial double support time (r = −0.56, Figure 3b). As for the ROM, the average baseline Ashworth score in the MA leg correlated negatively with the changes in MA knee ROM (r = −0.57, Figure 4a) and positively with the changes in MA ankle ROM (r = 0.57, Figure 4b) during single support. CITB dose at the follow-up correlated negatively with the changes in MA knee ROM during stance (r = −0.51, Figure 4c). The average baseline Ashworth score in the MA leg poorly correlated with the CITB dose at the follow-up (r = −0.06, P = 0.827). Similarly, the change in gait speed during the screening bolus trial poorly correlated with the change in speed from baseline to post-CITB (r = −0.05, P = 0.843).
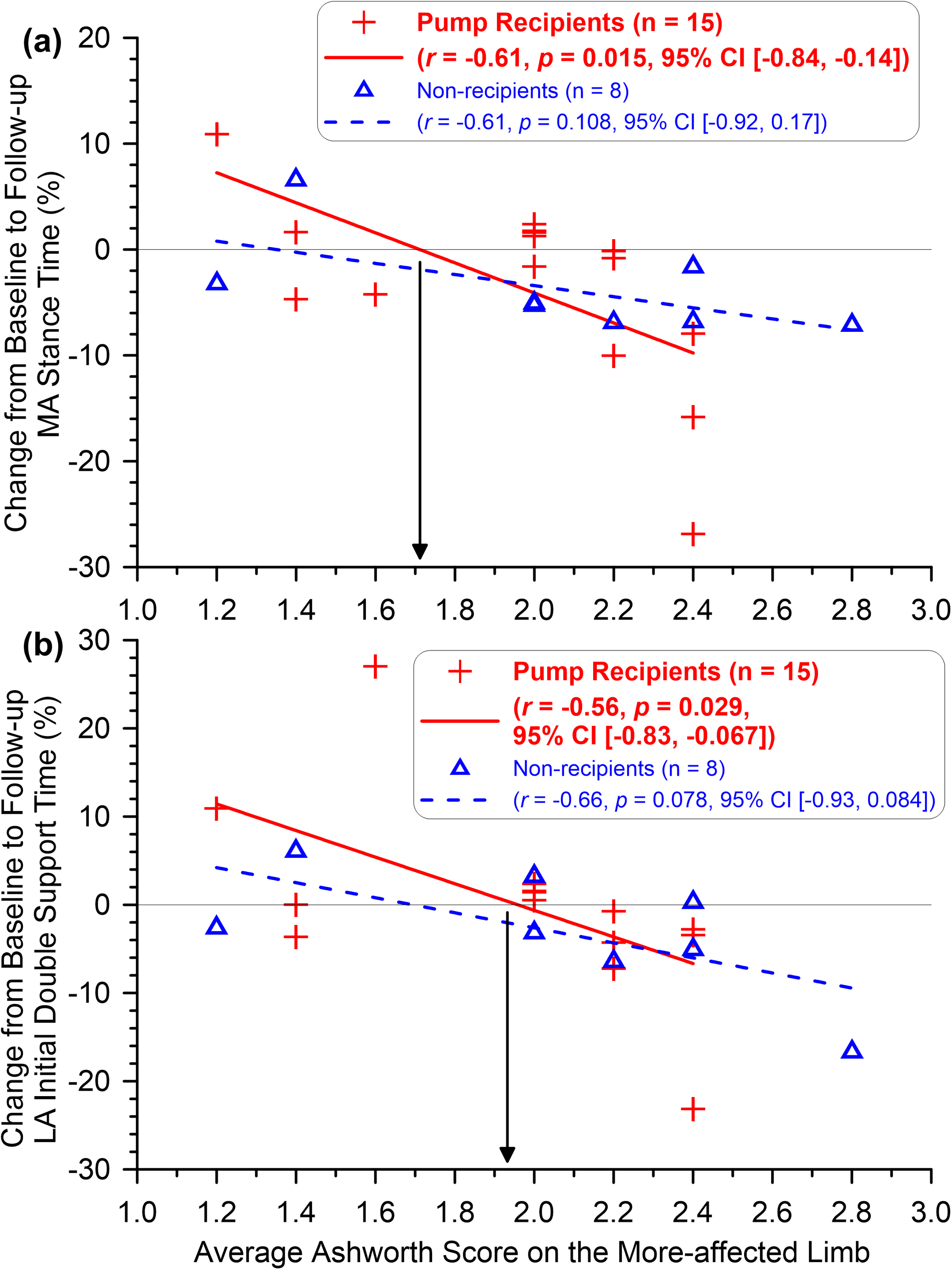
Relationships between the average baseline Ashworth score in the more-affected (MA) leg and baseline-to-follow-up changes in (a) MA stance time and (b) less-affected (LA) initial double support (equivalent to MA late double support) time. In pump recipients only, the MA baseline Ashworth score was inversely correlated with the changes in the MA stance and LA initial double support time from baseline to follow-up. The arrow line indicates the Ashworth score (around 1.7–1.9) that divides positive (an increase) and negative (a decrease) changes.
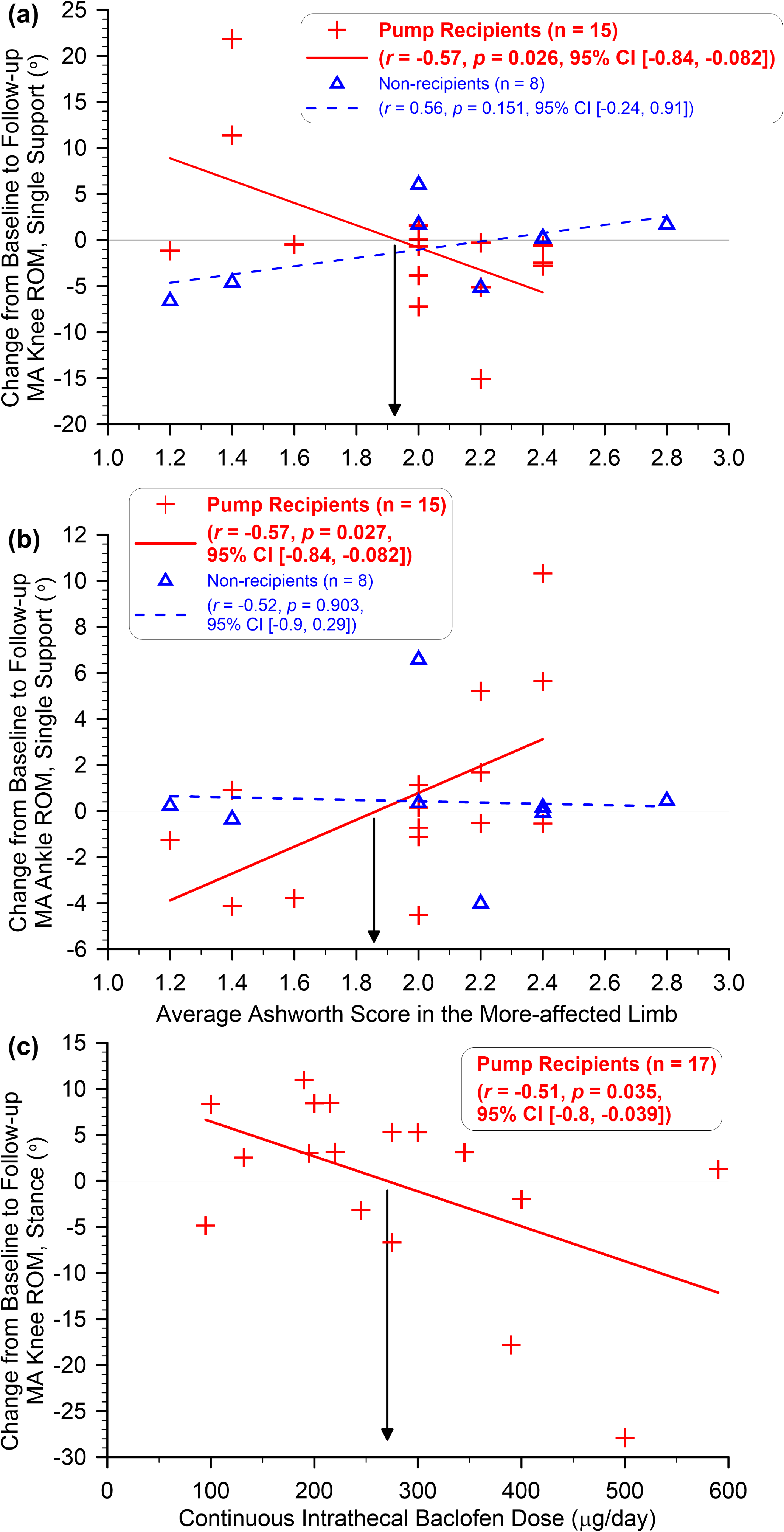
Relationships between the average baseline Ashworth score in the more-affected (MA) leg and baseline-to-follow-up changes in (a) MA knee range of motion (ROM) during single support, (b) MA ankle ROM during single support, and (c) between continuous intrathecal baclofen dose and baseline-to-follow-up changes in MA knee ROM during stance. The arrow line indicates the Ashworth score (∼1.8–1.9)/dose (∼275 µg) that divides positive (an increase) and negative (a decrease) changes.
During the study period, five pump recipients encountered system-related complications necessitating catheter revision. Two pump recipients had one surgical revision, and three recipients had two revisions for catheter-related complications. The time between the latest revision and follow-up gait evaluation ranged from 6 to 29 months. The change in gait speed from baseline to follow-up did not significantly differ between the five pump recipients with documented complications during the study period (3.1 ± 32.3 cm/s) and the 12 pump recipients without complications (−1.7 ± 13.5 cm/s, Mann-Whitney U test, P = 0.959, 2-tailed).
Discussion
This study aimed to explore changes in gait kinematics that can be ascribed to CITB infusion for problematic spasticity after ABI. Despite an improvement in one of the ROM measures found only in pump recipients, the overall results did not support the hypothesis that CITB would be associated with increases in gait speed, stride length, and joint ROM. Possible system malfunctions may have influenced the results of this study due to the disproportionate prevalence of these in this small sample. However, several months elapsed between the revisions and gait evaluations, and changes in gait speed were comparable between pump recipients who did and did not experience complications. The results of secondary analyses suggest that the diverse changes in gait kinematics among pump recipients may be related to the initial severity of muscle hypertonia and CITB dose at follow-up.
To the best of our knowledge, this is the first controlled study that examined the long-term effect of CITB administration in ambulatory ITB candidates. This makes a comparison to published case series difficult. Nonetheless, the finding of mixed individual results in temporospatial parameters with no significant overall difference between pump recipients and non-recipients agrees with the reports that CITB administration may not result in improved gait speed (Abbatemarco et al., 2021; Lee et al., 2018; Sammaraiee et al., 2020). Our results, however, differ from the two reports of significant improvements in gait speed in stroke patients at 4–25 months (Francisco & Boake, 2003) and 12-months post-implantation (Schiess et al., 2011). The reasons for these discrepancies are unclear. In the former study, CITB administration was combined with physical therapy, whereas no therapy was provided in the course of the latter study. Our sample received therapy of varied intensities and durations after pump implantation, but not at the time of follow-up gait evaluation. While clinical experience suggests that combining physical therapy with CITB improves ambulation to a greater extent than CITB alone, this study was not designed to evaluate the contribution of each specific treatment.
All study participants underwent a screening bolus trial via lumbar puncture, and 15 out of 25 increased gait speed at similar proportions (∼65%) between the two groups (Table 1). However, the decision to proceed with pump implantation was not based on post-bolus gait speed. Instead, it reflected a clinical judgement that CITB, alongside concurrent therapies, would achieve broader functional goals (e.g., improved comfort, walking endurance, gait appearance, or neurotoxin dose re-allocation for chemodenervation). Such tailored CITB dosing may have consequently exaggerated weakness and decreased gait speed. We suggest that gait speed may be useful for goal setting, but it should not be relied upon as the sole measure of CITB efficacy.
In contrast to traditional CITB administration, Schiess et al. (2011) reported a significantly increased gait speed in 20 of 26 stroke participants receiving periodic boluses over CITB at 12 months post-implantation, consistent with favorable bolus trial outcomes. This opens the possibility that periodic boluses may be a preferred mode of ITB delivery for patients who increase gait speed during the trial.
While significant main effects were not the primary focus of this investigation, it is worth noting that a decrease in the MA stance time coincided with an increase in the LA single support time from baseline to follow-up (Table 2). This pattern may reflect increased contralateral compensation over time in both groups. Specifically, patients may have shifted the weight-bearing role more towards the LA side to reduce loading on the MA side or to improve balance during walking by minimising the impact of MA-side weakness (Dorsch et al., 2016).
In both groups, the average ROM in the MA leg at baseline was within normal limits in the hip joint but decreased in the knee and ankle joints when compared to healthy adults walking at a very slow speed (Chow & Stokic, 2015). The significant group×time interaction for the MA knee ROM during swing depicts opposite trends in the changes over time for the two groups (Figure 2). In pump recipients, improvements in the MA knee ROM during swing over time were found in 11 out of 17 patients and exceeded 10° in six. This may be ascribed to lessening of the exaggerated quadriceps activity (Chow et al., 2017; Reinbolt et al., 2008), commonly inappropriate during pre- or initial swing (Kerrigan et al., 1991) and prolonged throughout swing (Lewek et al., 2007). It must be emphasized that, given the small sample size and other limitations, the clinical significance of a modest increase in the MA knee ROM during swing is limited, despite contrasting with the decrease observed in the non-recipients. Collectively, these findings may reflect a qualitative improvement in gait pattern despite no changes in speed. Objective gait assessment beyond gait speed may help optimize CITB therapy in ambulatory pump recipients, which deserves further study.
The moderate correlations revealed in the secondary analyses suggest that gait changes associated with CITB administration may be related to baseline muscle hypertonia in the MA leg at the time of a screening trial. For all significant correlations, the line of best fit intersected the X-axis (zero-change) at an average baseline Ashworth score of 1.7 to 1.9, indicating different changes from baseline to follow-up below and above these intersection points (see arrow lines in Figure 3). Specifically, if the average baseline Ashworth score in the MA leg was above 1.7–1.9, receiving CITB was associated with a relatively shorter stance time on the MA side, and shorter initial double support time on the LA side (equivalent to MA late double support time), and vice versa. Such changes correspond with faster walking speeds in patients with ABI (Chow et al., 2010), potentially signaling a positive outcome.
Furthermore, the secondary analysis indicated that the changes in the MA knee and ankle ROMs were also associated with the average baseline Ashworth score in the same leg. Specifically, pump recipients with baseline hypertonia above 1.9 points showed decreased knee ROM and increased ankle ROM during single support (Figure 4a-b). These preliminary results suggest that the link between baseline hypertonia and changes in gait kinematics with CITB therapy merits further investigation. Tentatively, the correlation findings reinforce the recommendation that clinicians should be cautious in recommending CITB to patients with less than severe hypertonia.
Improved ankle ROM in the MA leg may reflect reduced plantarflexor spasticity with CITB, permitting greater tibial translation over the stance foot, as observed within hours of ITB bolus injection (Chow et al., 2015). Our secondary analyses suggest that CITB dose may influence changes in joint ROM on the MA side, as CITB doses below ∼250 µg/day were associated with increased knee ROM during stance, whereas higher doses were associated with decreased ROM (Figure 4c). We speculate that higher CITB doses, although necessary to achieve specific functional goals, may lead to muscle weakness and negatively affect gait. These preliminary findings suggest that clinicians should remain vigilant to the potential increases in adverse effects associated with higher CITB doses.
Study Limitations
This study has several limitations because it was embedded in the clinical management of patients with muscle hypertonia at a single center. CITB dose was adjusted based on clinical judgment, with the overall motor function in mind, only one of which was gait. Thus, the selected CITB doses or mode of administration may have been suboptimal for improving gait. Also, pump recipients in this study experienced system malfunctions more frequently than in previous studies on CITB outcomes (Feller et al., 2021), raising the possibility of undiagnosed problems during the study period. However, all patients were routinely managed by the experienced team, and none reported unusual changes in muscle tone at the time of gait evaluation. Despite comparably fewer participants in the control group, drawn from a smaller pool of pump candidates who did not proceed with the pump implantation for various reasons (e.g., hesitancy, funding), the baseline characteristics of the two groups and the follow-up periods were similar. While the inclusion of controls is a strength of this study, the lack of randomization and the retrospective design likely introduced some selection bias. However, randomization in this clinical context is challenging from both practical and ethical perspectives, as intrathecal baclofen pump implantation is based on clinical indications, patient-specific factors, and shared clinical decision-making rather than experimental assignment alone.
Additional methodological limitations include the subjective determination of the MA leg in several participants and the absence of follow-up hypertonia assessment, which prevented exploring the relationship between changes in muscle tone and gait outcomes. The follow-up duration and rehabilitation exposure between baseline and follow-up were not controlled due to the retrospective nature of this study embedded in routine clinical practice, thus providing weaker evidence for causality compared to prospective studies. In addition, the lack of adjustment for multiple statistical comparisons likely inflated the Type I error rate (false positives). Given the above-mentioned limitations, caution is warranted in interpreting our findings. Further studies with larger cohorts are needed to validate the findings of the few studies addressing this issue, including this study.
Conclusions
In this cohort, we observed no overall group improvement in gait speed and ROM parameters. An improvement in the MA knee ROM during swing associated with CITB administration was observed, but its clinical significance is unclear. The results suggest that gait speed may be useful for goal setting, but it should not be the sole measure of CITB efficacy. Secondary analyses indicate that overall kinematic changes may vary depending on baseline hypertonia severity and CITB dose at follow-up. The individually varied outcomes highlight several factors that warrant further study, particularly the influence of baseline motor control, the dose and mode of ITB administration, and the role of concurrent therapy in achieving improved and durable mobility outcomes.
Footnotes
Abbreviations
Acknowledgments
We thank Terry S. Horn, PhD, and Mark Hemleben for contributing to data collection and processing and Kalisa K. Ramsey for her clinical services. Dr. Chow is the Gertrude C. Ford Director of Motion Analysis.
Ethical Considerations
This study was approved by the Institutional Review Board of the Methodist Rehabilitation.
Consent to Participate
IRB-approved consent forms have been collected from all participants.
Author Contributions
John W. Chow contributed to literature search, data collection, data analysis, manuscript preparation, and manuscript editing/review. Stuart A. Yablon contributed to design, data collection, and manuscript editing/review. Dobrivoje S. Stokic contributed to design, manuscript preparation, and manuscript editing/review.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Wilson Research Foundation,
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated during the current study are available from the corresponding author on reasonable request.