
Abstract
Background
Hand edema is a common post-stroke complication that negatively affects function and quality of life. However, interventions for hand edema remain limited.
Objective
In this study, we investigated whether contralateral resistance handgrip exercises performed with the non-paretic hand could immediately and sustainably reduce hand edema in patients with stroke.
Methods
This study used a B–A–B single-case design to explore the effects of the intervention in inpatients more than 3 months post-stroke. During the two 8-day intervention phases, the participants performed rhythmic handgrip exercises at 30% of the maximum voluntary contraction for 5 min daily as part of their occupational therapy sessions. A baseline phase without intervention was interposed. The hand volume was measured by using water displacement before and after exercise sessions to assess immediate and sustained effects.
Results
Four inpatients with paretic hand edema (93–110 days poststroke) participated in this study. Contralateral handgrip exercise resulted in immediate reduction in paretic hand edema in three of the four patients; however, only one patient showed a sustained effect. The intervention was simple and feasible, with responses varying across individuals.
Conclusions
This small single-case study suggests that contralateral handgrip exercise may contribute to reducing hand edema in some patients; however, its sustained benefits remain uncertain. This low-cost approach may serve as a candidate adjunct intervention in rehabilitation, particularly when paretic limb movements are limited. However, given the exploratory nature of this small single-case study, further investigation with larger samples and more rigorous designs is warranted.
Introduction
Stroke represents a major global health challenge, with nearly 94 million prevalent and 12 million incident cases worldwide, according to 2021 estimates (Feigin et al., 2025). After a stroke, many patients exhibit swelling and edema of the paretic hand, with reported prevalence rates as high as 73% for swelling and approximately 33% for clinical edema (Boomkamp-Koppen et al., 2005). This persistent edema not only causes discomfort and fibrotic changes in affected tissues but also contributes to the decline of hand function and limits daily activities, thereby reducing quality of life (Boomkamp-Koppen et al., 2005; Gustafsson et al., 2016).
Hand edema after stroke is often under-recognized; however, patients may report heaviness and concern over cosmetic appearance. Furthermore, edema promotes contracture, making its management essential. Interventions such as the use of Lycra garments with glove splints, upper limb range of motion exercises, and laser therapy may be effective in reducing poststroke hand edema. However, these approaches have limited clinical applicability due to short intervention periods and the restriction of study populations to patients in the early phase after stroke onset. By contrast, conventional interventions, such as bandaging, intermittent pneumatic compression, Kinesio taping, and orthoses, have yielded inconclusive results, suggesting that study conditions and participant characteristics may have influenced these findings (Giang et al., 2016). These limitations highlight the need for further research to establish clinically applicable and generalizable evidence for the management of post-stroke hand edema. In addition, demand has recently increased for simpler approaches, such as compressive wrapping and wrist–hand orthoses, rather than treatments like fluidotherapy, which have limited application owing to cost and equipment constraints (Pelak et al., 2026). Therefore, new approaches should be explored to improve the management of hand edema after stroke. Although its pathogenesis remains unclear, reduced venous return likely contributes to post-stroke hand edema (Hayashi et al., 2025). Resistive grip exercise using the non-paretic hand increases venous flow volume in the paretic hand in patients with stroke (Hayashi & Abe, 2020). Furthermore, previous studies have suggested that unilateral upper limb exercise can influence blood flow in the contralateral arm via central command (Ishii et al., 2017) and a consensual effect (Kiss et al., 2019). Taken together, these findings suggest that exercise of the non-paretic upper limb may induce changes in venous return in the contralateral paretic limb, thereby potentially contributing to the reduction in hand edema. Therefore, incorporating this handgrip exercise into rehabilitation for patients with stroke may immediately reduce contralateral hand edema. Even if the edema-reducing effect of this intervention is transient after a single session, repeated daily applications may allow small session-by-session reductions in hand volume to accumulate over time, thereby gradually decreasing the baseline level of hand edema. Previous studies (Hayashi & Abe, 2020; Hayashi et al., 2025) have primarily focused on physiological changes, such as enhanced venous return, and it remains unclear whether this improvement in venous circulation translates into a reduction in hand edema. As post-stroke hand edema is influenced not only by reduced venous return but also by other multiple factors, including autonomic and sympathetic vasomotor dysfunction as well as stroke-related vascular changes affecting capillary filtration and reabsorption, enhanced venous return should be regarded as only one of several contributors rather than a mechanism that necessarily results in edema reduction (Giang et al., 2016). Rehabilitation staff are widely involved in the management of post-stroke hand edema in hospital settings. However, the effective management of hand edema following stroke remains challenging (Giang et al., 2016). If effective, this simple intervention may offer a safe, low-cost adjunct to existing approaches for mitigating hand edema, particularly in early inpatient rehabilitation settings where more complex modalities may not be feasible. In this study, we aimed to explore whether contralateral resistance handgrip exercise immediately and/or sustainably reduces hand edema in inpatients with subacute stroke more than 3 months after onset.
Methods
Study Design
This study employed a B–A–B single-case experimental design as a pilot to explore the immediate and sustained effects of the intervention. In this study, we adopted a B–A–B design rather than implementing a prolonged pre-intervention baseline. In single-case experimental research, phase structures are often adapted to accommodate clinical constraints while preserving the essential experimental features of the design (Smith, 2012). This decision was made to balance methodological considerations with clinical feasibility in a subacute inpatient rehabilitation setting. For inpatients with post-stroke hand edema, extending the preintervention baseline or adding an additional withdrawal phase would have substantially increased participant burden and prolonged the period without an active intervention component, which was considered impractical and ethically undesirable in routine clinical practice. The study design comprised three consecutive phases: an initial intervention phase (B1, 8 days), a withdrawal/baseline phase (A, 8 days), and a second intervention phase (B2, 8 days).
All participants provided written informed consent before participation, and the study protocol was approved by the Institutional Ethics Committee (Institution name removed for blinding] (Approval No. [XXXX]). The study was conducted in accordance with the TREND statement guidelines for nonrandomized intervention studies.
Participants
Eligible participants were aged 20 to 85 years; were more than 3 months post-stroke; exhibited motor paralysis; and had visibly greater edema of the paretic hand compared with the contralateral side. Individuals with a history of cardiovascular disease, cardiac surgery, a pacemaker, previous pulmonary embolism, respiratory disease, any restriction or prohibition of exercise by their attending physician, or difficulty understanding or following instructions related to bed rest or exercise were excluded. Given that this was an exploratory, single-case experimental study conducted in a single inpatient rehabilitation ward, the sample size was intentionally limited, and no formal a priori sample size calculation was performed. In line with the recommendation that single-case experimental designs should include at least three participants (Smith, 2012), we selected a convenience sample of four inpatients with post-stroke hand edema.
Intervention
The intervention was delivered as a component of occupational therapy. Each case comprised an initial intervention phase (8 days), an 8-day withdrawal period (baseline phase), and a second intervention phase (8 days). During the intervention phases, participants performed rhythmic handgrip exercises using the non-paretic hand at 30% of their maximum voluntary contraction (MVC), which has been shown in previous studies to effectively promote venous return in the paretic upper limb (Hayashi & Abe, 2020), for 5 min, once daily. The grip strength was measured using a digital handgrip dynamometer (Takei Scientific Instruments, Niigata, Japan), and the 30% MVC was determined as the average of two maximal-effort trials. All handgrip exercise sessions were conducted under the supervision of an occupational therapist, maintaining a rhythm of 1 s of contraction and 1 s of relaxation using a metronome. No handgrip exercise was performed during the baseline phase.
Upper limb positioning during sleep and other non-exercise periods was not specifically controlled in this study. Occupational and physical therapy were not restricted across phases and were delivered as standard care. However, no direct interventions targeting upper limb edema (e.g., compression techniques and prolonged upper limb elevation) were provided during the study period.
Outcome Measures
To measure the hand volume, the participant's hand was gently immersed in a water-filled volumeter until the stop pin was positioned either between the middle and ring fingers or between the index and middle fingers. The position of the stop pin was consistently set at the same location for each participant. The hand was submerged so that the proximal part of the forearm was immersed in water. The displaced water was collected and transferred to a graduated cylinder to determine the hand volume by weight (Boomkamp-Koppen et al., 2005). Measurements were taken before and immediately after each exercise session during the intervention phases, as well as once daily before routine occupational therapy sessions during the baseline phase. All measurements were conducted at approximately the same time each day with participants in a seated position. The volumeter was positioned at a height such that, when the upper limb was immersed in water, the shoulder and elbow joints were approximately at 0° flexion and 0° extension, respectively. All edema measurements were performed by two occupational therapists, who collaborated and cross-checked each assessment to ensure accuracy. However, inter-rater reliability for the volumetric assessments was not evaluated. For the intervention, the same two occupational therapists were involved, with each participant assigned to one therapist who was responsible for delivering the intervention. Consequently, the therapist who conducted the edema assessment was also responsible for the intervention for each participant, and blinding was not feasible.
Statistical Analysis
All statistical analyses were performed using R (version 4.2.2). The Wilcoxon signed-rank test was used to compare the paretic hand volume immediately before and after each handgrip exercise session during the intervention phases to assess the immediate effects of the intervention. Phase-level (sustained) changes across the first intervention (B1), baseline (A), and second intervention (B2) phases were evaluated using the Tau-U statistic, calculated with R. Tau-U was used as a nonparametric effect size, summarizing the non-overlap between phases. Because a decrease in hand volume indicated improvement, Tau-U > 0 reflected improvement, and Tau-U < 0 reflected worsening. P-values were obtained via randomization tests, and 95% confidence intervals (CIs) were estimated using bootstrap resampling. No baseline trend adjustments were made because the baseline phase was short. For the Wilcoxon signed-rank tests and Tau-U statistics, two-sided p-values were calculated, with a significance level set at 0.05.
Results
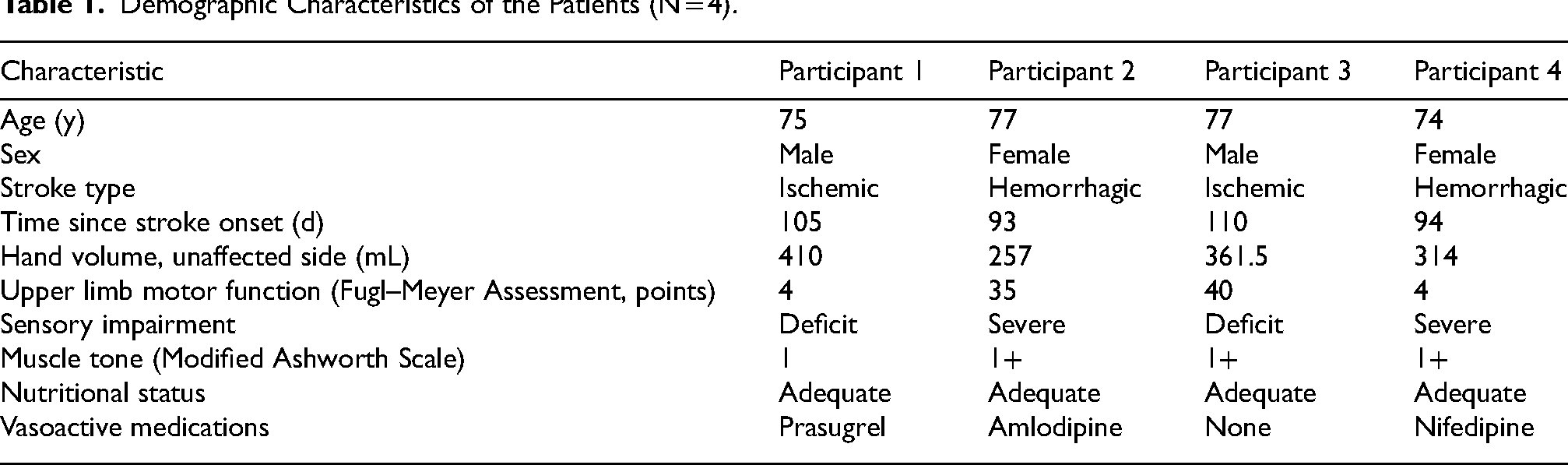
Four inpatients with paretic hand edema after stroke (mean age, 76.3 years; 93–110 days post-stroke) at a single hospital met the eligibility criteria and provided informed consent to participate in this study. At the beginning of the study, the affected hand was more swollen than the unaffected hand in all the participants. All patients exhibited severe or deficit sensory impairment. Muscle tone, as assessed using the Modified Ashworth Scale, ranged from 1 to 1 + . All patients maintained an adequate nutritional status. Some patients were receiving medications with vasodilatory or vascular effects, including the calcium-channel blockers amlodipine and nifedipine and the antiplatelet agent prasugrel, but none were treated with diuretics, systemic corticosteroids, or potent direct vasodilators (e.g., organic nitrates, such as nitroglycerin or isosorbide dinitrate) during the study period (Table 1). All intervention sessions were successfully completed according to the planned schedule.
Demographic Characteristics of the Patients (N = 4).
Immediate Effect
The paretic hand volumes (pre–post) during each phase (B1, A, and B2) are shown in Figure 1.
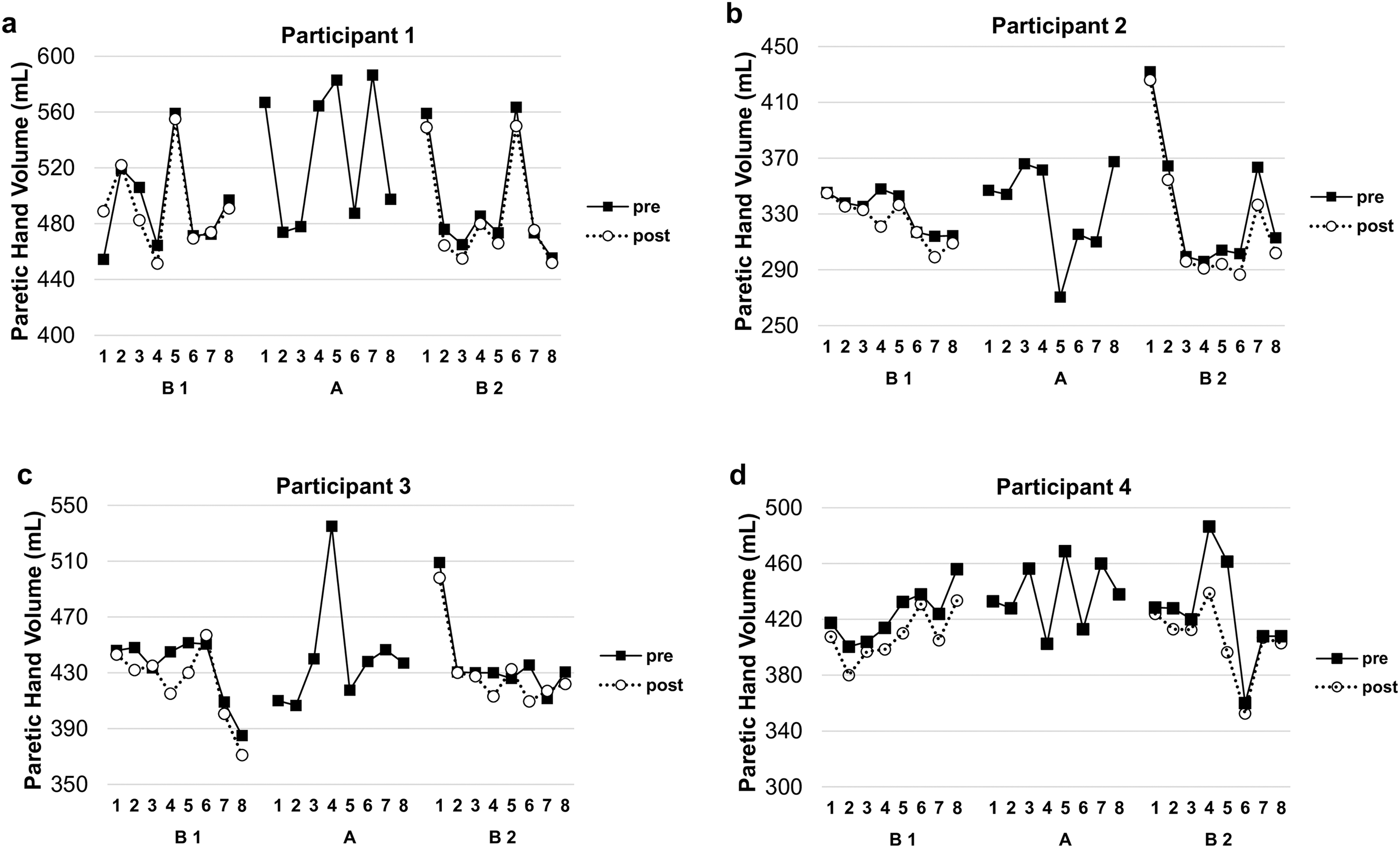
Changes in the paretic hand volume before and after contralateral handgrip exercise in four participants. (a–d) Each panel displays daily hand volume (mL) measurements for an individual participant across the three study phases: first intervention (B1), baseline (A), and second intervention (B2). Solid squares and lines indicate pre-intervention measurements; open circles and dashed lines indicate post-intervention measurements.
For Participant 1, no significant change was observed in the first intervention phase (B1: median difference, −3.0 mL; p = 0.44), whereas a significant reduction in hand volume was observed in the second intervention phase (B2: median difference, −8.8 mL; p = 0.02).
Participant 2 exhibited a significant reduction in hand volume during both intervention phases (B1: median difference, −4.0 mL; p = 0.02; B2: median difference, −10.0 mL; p = 0.01). Moreover, Participant 3 exhibited a non-significant reduction during the initial phase (B1: median difference, −11.2 mL; p = 0.06) and no significant change in the second phase (B2: median difference, −5.5 mL; p = 0.14). Participant 4 exhibited a significant reduction in hand volume during both intervention phases (B1: median difference, −17.2 mL; p = 0.01; B2: median difference, −7.5 mL; p = 0.01). Additionally, during the handgrip exercise with the non-paretic hand, slight contractions of the finger flexor muscles, consistent with associated reactions, were observed in Participants 2 and 3 (Table 2).
Immediate Effects of the Intervention on the Paretic Hand Volume.
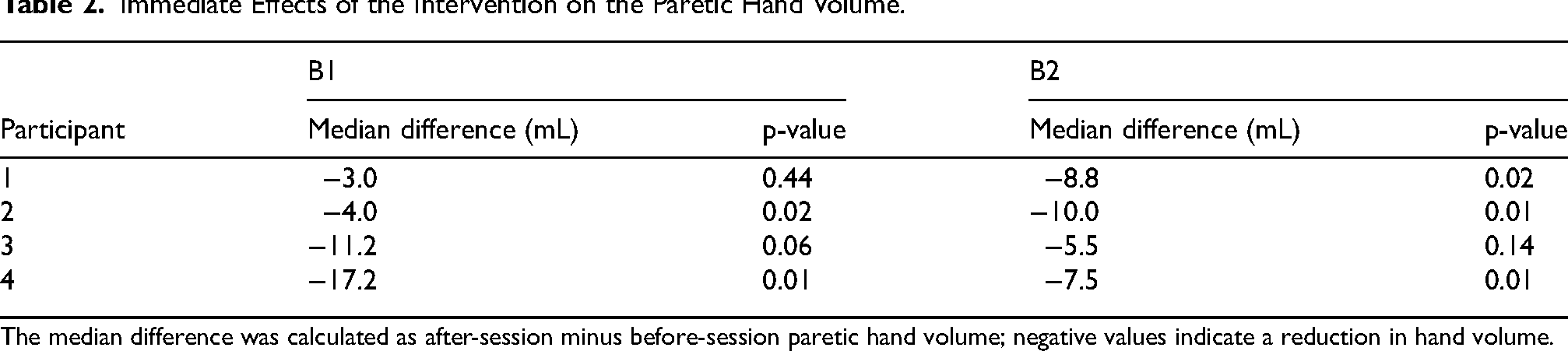
The median difference was calculated as after-session minus before-session paretic hand volume; negative values indicate a reduction in hand volume.
Sustained Effect
For Participant 1, A and B1 resulted in a Tau-U value of 0.53 (95% CI: −0.06, 0.91; p = 0.08) (Table 3). The contrast between A and B2 produced a Tau-U value of 0.66 (95% CI: 0.19, 0.97; p = 0.03). For Participant 2, the A versus (vs.) B1 comparison resulted in a Tau-U value of 0.22 (95% CI: −0.41, 0.75; p = 0.51), and the A vs. B2 comparison showed a Tau-U of 0.19 (95% CIs: −0.44, 0.78; p = 0.56). Moreover, for Participant 3, the A vs. B1 comparison resulted in a Tau-U value of −0.16 (95% CIs: −0.75, 0.44; p = 0.65), and the A vs. B2 comparison showed a Tau-U of 0.16 (95% CIs: −0.50, 0.78; p = 0.64). For Participant 4, the A vs. B1 comparison resulted in a Tau-U value of 0.39 (95% CIs: −0.17, 0.88; p = 0.22), and the A vs. B2 comparison showed a Tau-U of 0.23 (95% CIs: −0.34, 0.80; p = 0.46).
Sustained Effects of the Intervention on the Paretic Hand Volume.
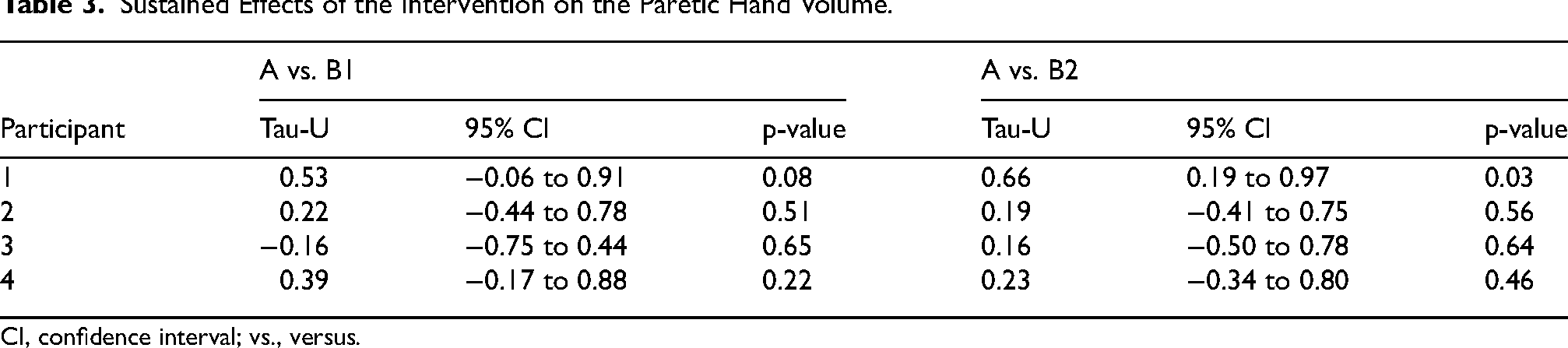
CI, confidence interval; vs., versus.
Discussion
In this B–A–B single-case study, we examined whether contralateral handgrip exercises could reduce paretic hand edema. Three of the four participants showed immediate within-session reductions in hand volume, whereas a sustained phase-level improvement was observed only in Participant 1, and this effect was limited to the period between A and B2.
Although using the affected hand may stimulate the muscle pump and help reduce edema, this is often not feasible in patients with severe paralysis. Moreover, a previous study found no clear association between upper limb activity and hand edema in patients with stroke (Gebruers et al., 2011), suggesting that increased use alone may not be sufficient for effective edema management in this population. Therefore, supplemental therapeutic interventions beyond promoting hand use are needed to manage post-stroke hand edema in severely affected patients.
Although contralateral exercise is hypothesized to promote venous return in the paretic limb, the precise underlying mechanisms remain to be fully elucidated. Potential contributing factors include central command-mediated sympathetic cholinergic vasodilation, which may increase the velocity of venous blood flow to the affected extremities (Ishii et al., 2017). Additionally, previous studies have reported that active movement of the non-paretic limb in patients with hemiplegia can increase blood flow in the paretic limb (consensual effect) (Kiss et al., 2019). As another mechanism, the edema reduction observed in this study may, at least in part, have resulted from unintended local muscle pump activity induced by slight involuntary contractions in the paretic upper limb, although these contractions were not quantified using electromyography. This limitation means that the improvements cannot be solely attributed to centrally mediated mechanisms; rather, they may reflect the combined influence of both central and peripheral factors. However, even in Participant 1, who exhibited the lowest level of muscle tone and no involuntary movement of the paretic upper limb during the handgrip exercise, an immediate effect was observed. Therefore, the interpretation of the results requires caution. The immediate within-session findings suggest that exercise likely facilitated an immediate enhancement of venous return, which may account for the transient reduction in edema observed immediately following the exercise session. However, the limited sustained phase-level effects suggest that this improvement in venous return was likely transient. Previous studies (Gustafsson et al., 2014; Roper et al., 1999) have also suggested that hand edema decreases immediately after an intervention, but such effects are not long-lasting. Rebound frequently occurs; thus, more comprehensive and longer-lasting management strategies are needed. This finding suggests that immediate physiological benefits (e.g., enhanced venous return) are not sustainable. Mechanisms such as sympathetic cholinergic vasodilation are typically short-lived and may not be sufficient to induce the long-term structural changes in fluid dynamics required for sustained edema reduction. It should be noted that these mechanisms were not directly measured or verified in this study; therefore, they remain hypothetical explanations for the observed edema reduction, warranting further investigation in future research. However, this simple, equipment-free intervention can be performed independently by patients, and a higher frequency may increase the sustained effects.
Notably, responses to the intervention varied among the participants. The specific pattern of responses among the participants suggests that while motor and sensory functions were similar across the four participants, other unmeasured physiological factors may have played a crucial role in mediating the effect of the intervention. In this study, the autonomic nervous system function was not evaluated. However, previous studies have shown that some patients with stroke exhibit autonomic dysfunction (Damkjær et al., 2023), which may be a possible contributing factor to edema (Wang et al., 2021). This may have contributed to individual differences in the degree of hand edema reduction observed in response to the intervention.
In this study, three of the participants showed large daily fluctuations in hand edema volume, with changes of approximately 100 mL. Two examiners measured the hand edema volume using the water displacement method to ensure measurement accuracy; therefore, the observed 100-mL fluctuations are unlikely to reflect measurement error. Severe or deficit sensory impairment and immobility of the paretic limb, especially while remaining below the level of the heart during sleep, may have contributed to the increased edema.
The main limitations of this study are the small sample size and short intervention period, which restrict the generalizability of the findings. In addition, the statistical interpretation of the findings is challenging because the number of data points per phase was very limited, and multiple comparisons were conducted; therefore, the present results should be interpreted with caution. Another limitation is that we did not employ a standard A–B or A–B–A–B sequence and instead began with the intervention phase (B) in a B–A–B design. Starting with the B phase may constrain comparisons with the pre-intervention phase. Furthermore, autonomic nervous system function, which may influence the development of hand edema and individual responsiveness to the intervention, was not assessed using standardized testing methods. Additionally, because the same occupational therapist performed both the assessments and the interventions, the outcome assessors were not blinded. This lack of blinding represents a major potential source of measurement bias and may have contributed to an overestimation of the immediate effects observed in this study. The positioning of the paretic upper limb during periods outside the intervention or rehabilitation sessions, including sleep posture, was also not standardized across participants and may have acted as an uncontrolled confounding factor. In addition, overall daily activity levels were not systematically monitored, which may have further influenced the development and fluctuation of hand edema. Muscle contractions observed in the paretic upper limb during contralateral handgrip exercises were not quantitatively evaluated using electromyography. Future research should employ larger samples and longer protocols, explore the optimal exercise frequency and intensity, and incorporate physiological assessments to better define the role of contralateral handgrip exercises in edema management.
Conclusion
The present findings provide preliminary evidence that contralateral handgrip exercise may help reduce paretic hand edema in some patients, particularly in the immediate phase following exercise. However, because the sustained effects and broader applicability of this intervention are still unclear, further research with larger samples and more rigorous designs is needed. Further studies should investigate whether increasing the intervention frequency or duration enhances efficacy. This simple and feasible protocol may be a potential adjunct for the management of post-stroke hand edema.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to the rehabilitation staff at Tokai Memorial Hospital for their invaluable contributions to this study.
Ethical Approval
This study was approved by the Ethics Committee of Seijoh University, Japan (Approval Number: 2021C0009). All participants provided written informed consent prior to participation.
Consent to Participate
Written informed consent was obtained from all participants involved in the study.
Consent for Publication
Not applicable.
Author Contributions
Conceptualization: Hiroyuki Hayashi, Ayana Kato, Naoki Tomiyama
Methodology: Hiroyuki Hayashi, Ayana Kato, Naoki Tomiyama
Data Collection: Hiroyuki Hayashi, Ayana Kato, Naoki Tomiyama, Hibiki Ogihara
Data Analysis: Hiroyuki Hayashi, Ayana Kato, Naoki Tomiyama
Writing–Original Draft: Hiroyuki Hayashi
Writing–Review & Editing: Ayana Kato, Naoki Tomiyama, Hibiki Ogihara
Supervision: Hiroyuki Hayashi
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Japan Society for the Promotion of Science (Grant Number: 19K19623).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available within the article.