
Abstract
The MOM Program is a randomized, controlled trial of an intervention to promote mothers’ care for the health and development of their children, including accessing early intervention (EI) services. Study aims were to determine whether, relative to controls, this intervention increased receipt of and referral to EI services. Mothers (N = 302) living in high-poverty regions were recruited after having given birth to healthy infants and were randomized to the intervention (n = 152) or control (n = 150) group. Those in the intervention group received up to 11 home visits to promote well-child visits and referral to EI. Children in the intervention group were referred to and received EI services significantly more often than those in the control group. Maternal depression and age of the mother were significantly associated with referral to, and receipt of, EI.
Keywords
The impact of poverty on children’s health and development can be devastating. Children living in poverty are more likely to experience developmental problems (Simpson, Colpe, & Greenspan, 2003) and have unmet health care needs (Silver & Stein, 2001) than those not living in conditions of poverty. Timely screening for developmental problems and referral to appropriate early intervention (EI) services, if necessary, is particularly important for children living in poverty. Early identification of developmental delays and prompt referral to early childhood programs can have a positive impact on children’s cognition, school performance, behavior, and social well-being (Isaacs, 2008), thus helping to offset the deleterious effects of growing up in poverty.
Sociodemographic factors such as income, race, and maternal education have been found to relate directly to health care and EI service utilization and experiences. Mothers with low income and with less education have more difficulty entering their children into the EI system as compared with mothers with higher incomes and educational levels (Bailey, Hebbeler, Scarborough, Spiker, & Mallik, 2004). In addition, there is a discrepancy between the numbers of children identified with delays and those receiving services (Rosenberg, Zhang, & Robinson, 2008; Simpson et al., 2003). Rosenberg et al. (2008) found that 13% of children are identified as having developmental delays nationally, but only 10% of those children receive services for those delays by age 24 months. In a nationally representative sample of individuals receiving EI, Bailey et al. (2004) found an average gap of 5.2 months between diagnosis and referral. Increasing the numbers of children in low-income families who are referred to EI services and decreasing the wait time for service entry holds promise in promoting optimal developmental outcomes for children with early developmental delays.
Home-visiting programs have been shown to reduce the adverse effects of poverty and to promote optimal child development and family resilience. For example, in the Nurse–Family Partnership Program, home-visited mothers were found to have delayed and reduced subsequent pregnancies, decreased welfare dependence, and increased participation in the workplace (Olds et al., 1997; Olds et al., 1999; Olds et al., 2002; Olds et al., 2004). Positive child outcomes such as higher intellectual functioning and school achievement and fewer behavior problems have been demonstrated in both nurse and paraprofessional home-visiting programs (Isaacs, 2008; Olds et al., 1999; Olds et al., 2002; Olds et al., 2004; Olds, Sadler, & Kitzman, 2007; Sweet & Appelbaum, 2004). Maternal depression has been associated with decreased preventive health services for their children (Minkovitz et al., 2005). However, in a systematic review of the relationship between maternal depression and home-visiting programs, researchers found that, although rates of maternal depression range from 28% to 61% across programs, home-visiting programs do not typically change mothers’ depressive symptoms (Ammerman, Putnam, Bosse, Teeters, & Van Ginkel, 2010).
Home-visiting programs, although widely offered throughout the United States for families at risk of poor parenting, have not been used as a tool for improving participation, either in EI or early childhood programming. At the same time, by increasing mothers’ knowledge of existing opportunities and mothers’ ability to identify delays and seek appropriate services for their children, home-visiting programs hold great potential to address the gaps in referral and service utilization. Favorable outcomes of home-visiting programs in other areas related to school success and positive long-term outcomes have been described extensively (Gomby, 2005; Isaacs, 2008; Olds et al., 2007; Schonberg et al., 1998).
The MOM Program (Note: MOM is not an acronym) is an innovative home-visiting program designed to promote competence among mothers living in urban poverty. The goals of the program are to increase participation in child primary health care services and to promote participation in EI programs by prompting mothers to obtain services on behalf of their children. This report provides results from a randomized, controlled trial of The MOM Program on improving targeted outcomes. The study hypotheses are for children with developmental delays: (a) Children in the intervention group will be referred to EI services significantly more often than children in the control group, and (b) children in the intervention group will receive EI services significantly more often than children in the control group. Predictive factors associated with referral to, and receipt of, EI services are examined in an exploratory study aim.
Method
The Institutional Review Board of The Children’s Hospital of Philadelphia approved the plan and implementation of this study. Study staff, blinded to group assignment, evaluated the children and their mothers/caregivers in study offices near to each child’s third birthday (mean age = 33.6 months; standard deviation [SD] = 1.1) and conducted questionnaires over the telephone every 4 months. Families were given funds for transportation to the assessment visit and a small payment for food. Child participants were each given a book to recognize their participation in the study.
Participants
Between July 2001 and January 2002, we invited 650 mothers who met eligibility criteria to participate in the study. Mothers were recruited from the postpartum unit of an urban academic hospital. All mothers lived in Zip codes within the City of Philadelphia that had high rates of poverty, and each had singleton healthy infants weighing at least 2,500 grams with no identified genetic or developmental disorders.
Table 1 provides the number of eligible mothers invited to participate, randomized, and evaluated at the 33-month follow-up assessment. Outcomes for 89% of those initially recruited were evaluated. Of the 650 mothers who were initially eligible for the study, the study team missed contacting 32, largely due to their early discharge from the hospital. Of the remaining 618 potential participants, 302 mothers (46% of those invited to participate in the study) gave consent to participate. Reasons for nonparticipation were lack of interest (76%), disapproval by a family member (7%), moving (5%), and other (12%). Nonparticipating mothers were older (p < .001) and had more children (p < .01), but were not different in child’s gender or birth weight. We did not attempt to collect demographic information on nonparticipating mothers. Overall, 152 participants were randomized to receive the intervention and 150 to the control condition. Of the mothers enrolled in the study, 94% were African American, with a mean age of 23.1 years (SD = 5.6), with 54% female infants, and 44% first births. On average, the mothers reported 12.0 years (SD = 1.9) of education. Of the participants, 74% reported that they had 10 or more prenatal visits, 18% had 5 to 9 visits, 6% had 1 to 4 visits, and 2% had no visits.
Enrollment and Allocation of Participants

Measures
Denver Developmental Screening Test–II (DDST-II)
The DDST-II (Frankenburg, Dodds, Archer, Shapiro, & Bresnick, 1992; Frankenburg et al., 1996) is an updated version of the measure widely used by pediatric health care providers to measure developmental skill attainment for children from birth to 6 years of age. Each item on the DDST-II has been scaled to indicate at what ages 25%, 50%, 75%, and 90% of children pass that item, based on standardization data obtained on more than 2,000 children and oversampled for the younger ages to add precision to those age periods when development changes most rapidly. Reliability was found to be 90% agreement (interrater) and kappa 0.75 or higher (test–retest, same observer). Validity was established through developmental growth curves as well as the manner in which data were collected from the standardization sample. Based on parent report of the child’s skills in language, cognition, and motor development, the measure provides overall ratings of “normal,” “borderline,” or “abnormal” development, as determined by the patterns of items passed and failed in each area. Consistent with pediatric practice, if two or more areas were found to be “borderline” or “abnormal,” the child’s performance was described as “abnormal” for this study. This measure was administered to all participant mothers at the 16-month cohort telephone call by a caller who was blind to group assignment and who had been trained by a licensed psychologist to ask questions appropriately regarding children’s developmental skills. By design, this caller was not part of the intervention team, in an effort to gather accurate information from the mothers regarding children’s developmental status.
Ages and Stages Questionnaire (ASQ)
The ASQ (Bricker, Squires, Kaminski, & Mounts, 1988) is a series of developmental screening questionnaires for children ages 4 months to 48 months of age. Each of the 11 questionnaires is developed for a particular age range and contains 30 items examining development in the domains of communication, gross motor, fine motor, problem solving, and personal/social development. The questionnaires were standardized on 2,008 children from a wide geographic area within the United States, as well as from a variety of ethnic and socioeconomic backgrounds. Test–retest reliability has been established at 99% over 2 weeks and interrater reliability at 97%. Validity was established through comparing results with those of the Gesell classification; percentage agreement ranged from 79% at 4 months to 94% at 16 months. Also examined were sensitivity (38%-90% across the 11-age intervals) and specificity (81%-90%). The questionnaire is read to mothers by the evaluator, and the answers are recorded on the form. If the mother is not certain about achievement of milestones, the evaluator offers the child the appropriate developmental toy and observes the child’s activity. Each question is answered in “yes,” “sometimes,” and “not yet” format. Results of the ASQ ratings were categorized as “normal” or “at risk.”
The ASQ was completed during the 18-month home visits by home visitors who had been trained in its administration by a licensed psychologist experienced in its use for EI screening for service eligibility. As the mothers in the control cohort did not receive home visits, only children in the intervention home-visiting cohort were screened with the ASQ. The ASQ was included in the intervention protocol to help mothers become more aware of their child’s developmental status and of the possible need for EI services. Following the ASQ screening visit, mothers were called if there were concerns about their child’s development, and summary letters were sent to the mother and to the child’s health care provider (see Appendices B and C).
Wechsler Preschool and Primary Scale of Intelligence–Third Edition (WPPSI-III)
The WPPSI-III (Wechsler, 2002) is an individually administered scale of intelligence for preschool children, which includes tasks of language, nonverbal reasoning, concept development, and fine motor skills. Regarded as a “gold standard” measure for children this age (Sattler & Dumont, 2004), WPPSI-III scores have established reliability of .86 to .92 (test/retest) and .89 to .97 (internal consistency). Validity for WPPSI-III is based on test content as judged by comprehensive literature and expert reviews, as well as by response processes, as determined through theoretical and empirical evidence of response processes, results of factor analyses, and intercorrelation studies. Standardization procedures were extensive, with data collected on 200 children at the ages of those in the study and with appropriate distribution for race/ethnicity, maternal education, urban/rural status, and geographic region of the United States at the time of the 2000 Census. Standard scores for the verbal, performance, general language, and full scale IQ have a mean of 100 and a SD of 15. The WPPSI-III was used in this study to investigate possible group differences in children’s cognition as a result of study participation, and was administered when children were 33 months of age.
Beck Depression Inventory-II (BDI-II)
The BDI-II (Beck, Steer, & Brown, 1996) is a 21-item survey of symptoms of depression, using criteria of Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000). Reliability has been determined at .92 and .93 (internal consistency) and at .93 (test–retest). Validity of scores as compared with comparable measures ranges from r = .37 with the Scale for Suicidal Ideation to r = .68 with the Beck Hopelessness Scale. Items are rated along a 4-point scale from 0 to 3; higher scores are indicative of greater symptoms of depression. The total BDI-II score was used in analyses. Conceptualized as a possible moderating factor impacting EI referral and receipt of services, the BDI-II was completed by all mothers during the 33-month study visit.
Demographics were assessed through a series of questions regarding mothers’ age, race/ethnicity, level of education, employment status, receipt of public services, income, and other social indicators. Demographics were collected at study enrollment and at a study visit when children were 33 months of age.
Statistical Power and Assignment Ratios
For all power calculations, we set alpha = .05 and beta = .2, and specified two-tailed tests. These calculations led to a total target sample of 302, with an assumption of 20% attrition over time. Given the sample enrolled and retained at the 33-month follow-up assessment and assuming that, for normally distributed variables, 10% of the variance is accounted for by other terms in the model, we estimated the smallest detectable treatment main effects for key outcomes as follows: Based on population rates in Philadelphia, we estimated that 20% of children should be referred to EI services, with a detectable difference in rate of at least 25%.
Randomization
Once mothers gave consent to participate in the study in the presence of a trained staff member, a sealed envelope containing a card stating “Intervention” or “Control” was selected. The randomization envelopes were generated by a blinded staff member and were grouped in blocks of 20, to allow for relatively even distribution over the course of the recruitment/randomization process.
Treatment Conditions
Control
Mothers in the control condition (n = 150) received an information booklet on child/family services on enrollment and information on transportation for the 33-month follow-up evaluation. They were called every 4 months to maintain contact information.
Intervention —The MOM Program
Mothers in the treatment condition (n = 152) received all services of the control group. In addition, they received home visits and follow-up calls timed to well-child primary care appointments for the child’s first 3 years following American Academy of Pediatrics guidelines (American Academy of Pediatrics, 2000). The mothers received a mean of eight home visits (range = 0-11 visits) during the 3 years of the intervention. After receiving extensive training for each visit, the home visitors followed a manualized, detailed visit-by-visit protocol with the goals of (a) enhancing the mothers’ understanding of normal child development, (b) facilitating the child’s attendance at age-recommended well-child visits (and obtaining recommended immunizations at that time), and (c) supporting the process of identifying child-developmental delays and subsequent referral to and receipt of EI services. Visit protocols were developed from theories of human ecology (Bronfenbrenner, 1981) and self-efficacy (Bandura, 1977). The intent of the program design was to promote positive relationships with home-visited mothers by avoiding long or frequent home visits that might be seen as burdensome or intrusive. For this reason, the visits were intentionally short, but focused and protocol-driven to assure fidelity to the intervention.
Home visits were conducted by a member of the intervention team, consisting of two master’s level nurse practitioners (both Caucasian females in their late 30s) and two trained community workers (both African American high school graduates, one with some college coursework completed, in her mid-20s, and the other in her mid-50s). The four team members alternated study visits to allow participants the benefit of professional expertise and community wisdom. Each mother in the intervention was visited by at least three of the four home visitors.
Supervision for the home visitors was provided by a board-certified pediatrician, a PhD-level nurse practitioner, and two PhD-level psychologists in weekly 90-min team meetings. Training for each home visit was conducted initially in the supervision meeting, then in additional sessions after the weekly meetings. Didactic presentations, demonstration by a program leader, and staff role-plays were included into the trainings, with training provided by program leadership. Staff were observed individually in conducting the ASQ assessments, with additional training provided, if needed, until a criterion level had been attained. Videotapes illustrating the ideal conduct for each home visit were also reviewed with the home-visiting staff to illustrate the conduct of the home visits. An important part of the weekly supervisory meetings was a rigorous review of the progress of each intervention participant. Consistent with earlier findings that an assertive outreach policy resulted in higher program retention (Sullivan, Rumptz, Campbell, Eby, & Davidson, 1996), multiple attempts were made to contact mothers if home visits or well-child visits were missed. If a mother was persistently unresponsive to the efforts of one team member, another team member was asked to step in. Days and times of outreach efforts were also varied. Another key feature of the weekly supervision meeting was to emphasize the program model, which is one of supporting mothers to take action on behalf of their children. Study staff followed up with mothers as needed to prompt them to finish tasks such as completing immunizations or referral to EI. Consistent with the programmatic emphasis on developing mothers’ self-efficacy (Bandura, 1977), the home visitors did not complete tasks on mothers’ behalf.
A typical home visit was 15 min long. Mothers were informed of the content of the upcoming health visit for their child (e.g., which immunizations or screening tests were likely to be performed). Mothers were asked to describe any concerns about their child. They were shown checklists of child-developmental milestones for that age and asked whether their child met each of the milestones. Mothers were advised to bring concerns or questions to the child’s health care provider. Finally, mothers were informed of any early education services that might be appropriate for their child, such as Early Head Start. Families with other needs were referred to the child/family information booklet and supported via follow-up calls to obtain services needed. At child age 18 months, the visit began with a review of developmental expectations for children ages 18 to 24 months, with emphasis on emerging language skills. If the family had previously been referred to Early Head Start or to EI services, this was reinforced, such as by asking about referral progress, or by again providing contact information for service providers. The importance of immunizations and lead screening (and follow-up) was discussed. A photograph was taken of each child and given to the mother for inclusion in a program-provided personal organizer. Preparation for the upcoming child health visit was conducted by reviewing with the mother the importance of checking that the child was growing at expected rates, and by reviewing any questions for the health provider. Barriers for completing the child’s next health care visit were discussed, and possible solutions were developed with the mother. The mother was reminded of the importance of the annual gynecological visit and resources were shared, if necessary. Finally, contact information for the mother and the alternate contacts were reviewed, and any changes were noted. Finally, each family was offered a developmental screen by a home visitor using the ASQ (Bricker et al., 1988). If the screen suggested developmental delay, a letter was sent to the child’s pediatric care provider and the family was given information about the EI services. The full protocol for this 18-month home visit is available from the authors on request. To assure fidelity to the intervention, home visitors were asked to complete during each home visit a checklist of protocol-specific activities for that visit. Completed checklists were then reviewed administratively. Departures from the visit protocol were discussed in weekly staff meetings, and the correct visit protocol was reinforced. Problems that arose during home visits were discussed and solutions were developed. An example of a visit checklist is included in Appendix A, as well as sample letters sent to mothers and child health care providers informing them of the results of the developmental screenings (Appendices B and C).
Outcomes
Follow-up blinded assessments were scheduled for completion at a research office when the children reached a target age of 33 months; visits were completed at mean age of 33.6 months (SD = 1.1). At the 33-month visit, information was collected from mothers (n = 263), although rarely other family members, such as aunts or grandmothers, served as informants (n = 8). Mothers or caregivers were interviewed for a variety of demographic and social service use variables. Immunization data were collected from the health care providers of the children. Child-developmental measures were obtained at age 16 months through the DDST. Children in the intervention group were screened with the ASQ at the 18-month home visit. The ASQ was not administered to those in the control group because this was considered to be part of the intervention. Information on whether the children were referred to and received EI services was collected through phone calls to mothers made at 4-month intervals when children were 12 to 32 months of age. The phone calls were made to all participants by a research assistant who was blind to the randomized group status. Besides asking for up-to-date contact information, the caller asked whether the child had been referred to EI services and whether he or she had received EI services.
Statistical Models and Methods of Analysis
Data analyses were conducted for all cases randomized. Statisticians were blinded to the treatment group. The primary statistical model consisted of a two-level treatment factor (intervention vs. control group) and any covariates, to adjust for nonequivalence (p < .10) among treatment groups assessed at the baseline evaluation. All dependent variables were examined with respect to their distributional characteristics. Continuous dependent variables that did not violate the normality assumption were analyzed with the general linear model; dichotomous outcomes, such as receipt of EI services, were analyzed with the logistic-linear model (with the assumption of binomial distribution). Group differences in normal/abnormal performance ratings on the DDST were determined through Fisher’s exact test. Descriptive statistics were used to evaluate results of the ASQ screening. Log-linear test of equality over strata was used to evaluate group differences in the referral to, and receipt of, EI services. Cox best subset selection method for multiple regression was used to determine predictors of time to first EI referral and time to first receipt of EI services.
Results
Equivalence of Groups
As shown in Table 2, at baseline, the treatment groups were similar with respect to background characteristics. Table 3 illustrates maternal characteristics at the 33-month assessment. There were no significant group differences on any of the variables examined.
Comparisons of Participant Baseline Characteristics
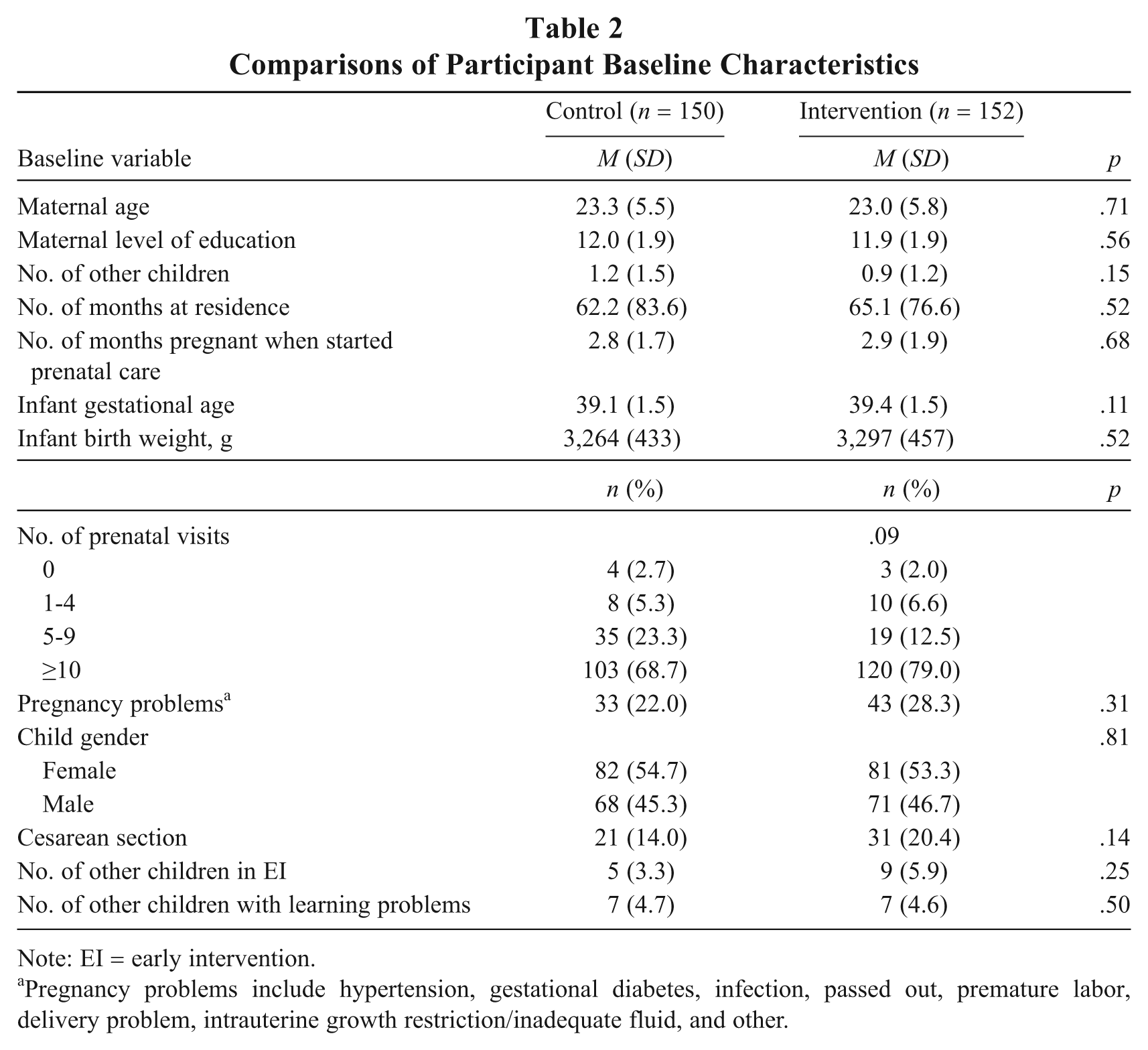
Note: EI = early intervention.
Pregnancy problems include hypertension, gestational diabetes, infection, passed out, premature labor, delivery problem, intrauterine growth restriction/inadequate fluid, and other.
Caregiver Characteristics at 33 Months

Note: BDI-II = Beck Depression Inventory-II.
BDI-II total scale is based on sample size, n = 134 for the control group and n = 135 for the intervention group.
Referral to and Receipt of EI Services
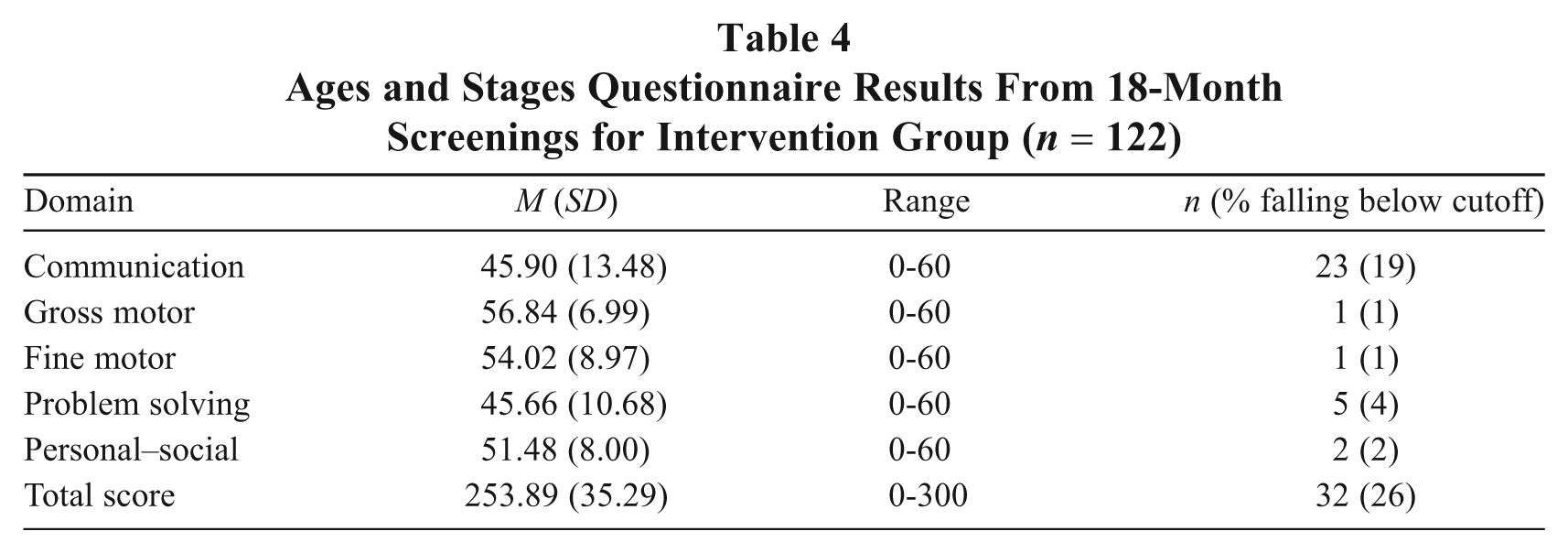
Of the 257 (85% of the 302 originally enrolled) children receiving the DDST at age 16 months, 61 (24% of the whole sample; 26 children in the intervention group, 35 in the control group) had scores indicating abnormal development, signifying that a referral to EI was warranted. There were no significant group differences in the number of children with abnormal findings, using Fisher’s exact test (two-sided) = 0.187, ns. At the 18-month home visit, 144 (95% of the 152 in the intervention group) children in the intervention group received the ASQ screening. Of those screened, 26 (18.1%) were found to be at risk developmentally (see Table 4). Group comparisons were not made because the children in the control condition did not receive the ASQ screening. Of the children in the intervention group who did not receive the ASQ at 18 months, all 8 had dropped out of the program by that time. Reasons for dropouts included 2 infant deaths, 3 mothers who were “too busy,” 2 mothers who experienced “too many calls,” and 1 mother who had moved out of the area.
Ages and Stages Questionnaire Results From 18-Month Screenings for Intervention Group (n = 122)
Although the 16-month developmental status of the children in the two groups was equivalent, group differences were identified in referral to, and receipt of, EI services. For the intervention group, 28 (20%) of 142 children were referred to EI, and for the control group, 10 (14.5%) of 145 children were referred to EI (confidence interval [CI] = 3.11 [1.92, 5.05], p < .001). With regard to receipt of EI services, 22 (15%) of 142 children in the intervention group received services, whereas 6 (4%) of 145 children in the control group received services (CI = 2.78 [1.62, 4.76], p = .0002). Figure 1 illustrates group outcomes in the referrals to EI services up to 33 months of age, with significantly more children in the intervention group referred to EI services, with log-rank χ2 = 10.27, p < .01. Figure 2 shows group outcomes in receipt of EI services, also displaying significant differences that favor the intervention group, with log-rank χ2= 10.56, p < .01. Multiple regression utilizing the Cox best subset selection method was used to identify maternal factors associated with time to first referral of EI services, including income, race, maternal education and other demographic data collected from the mothers. For the entire sample, beyond group assignment, the only factors identified were maternal depression (hazard ratio = 1.06; 95% CI = [1.03, 1.10]; p < .001), and age of the mother (hazard ratio = 1.10; 95% CI = [1.04, 1.16]; p < .01). Children with older mothers and mothers with more depressive symptoms were more likely to be referred to EI. Multiple regression using the Cox best subset selection method also identified factors associated with time of first receipt of EI services. In addition to group assignment, factors identified were maternal depression (hazard ratio = 1.06; 95% CI = [1.03, 1.10]; p < .001), and age of mother (hazard ratio = 1.09; 95% CI = [1.03, 1.15]; p < .01). Again, children were more likely to receive EI if their mothers were slightly older or had slightly more depressive symptoms. Post hoc comparisons were made of numbers of mothers in each group reporting clinical levels of depressive symptoms (17 or higher). For the control group, 29 of 134 mothers obtained scores higher than 17, whereas for the intervention group, 36 of 135 mothers obtained scores in this range (χ2 = .927, p = .34).
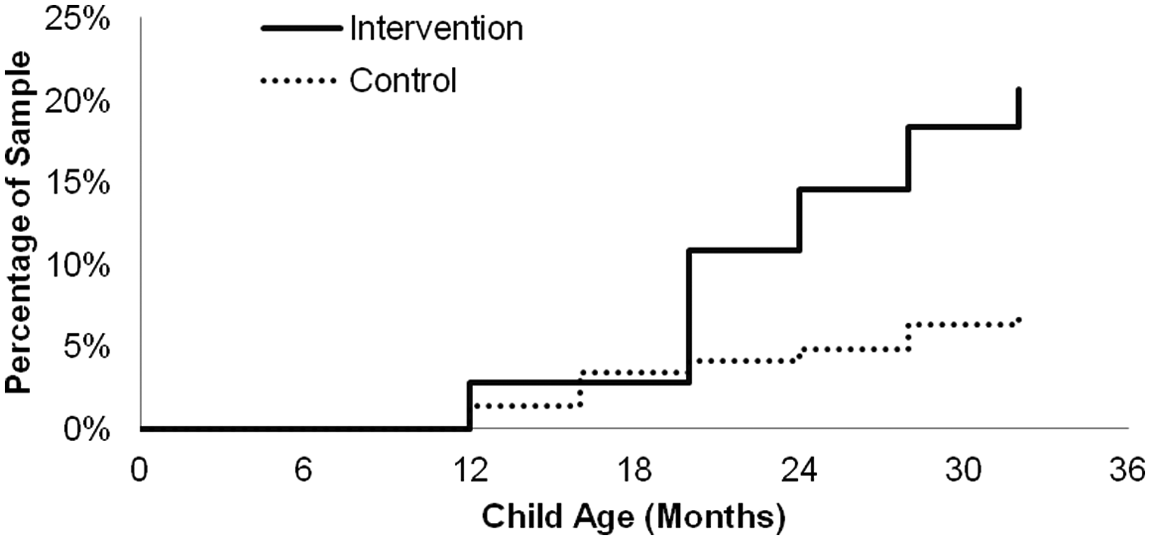
Time to First Referral for EI Services, p < .01
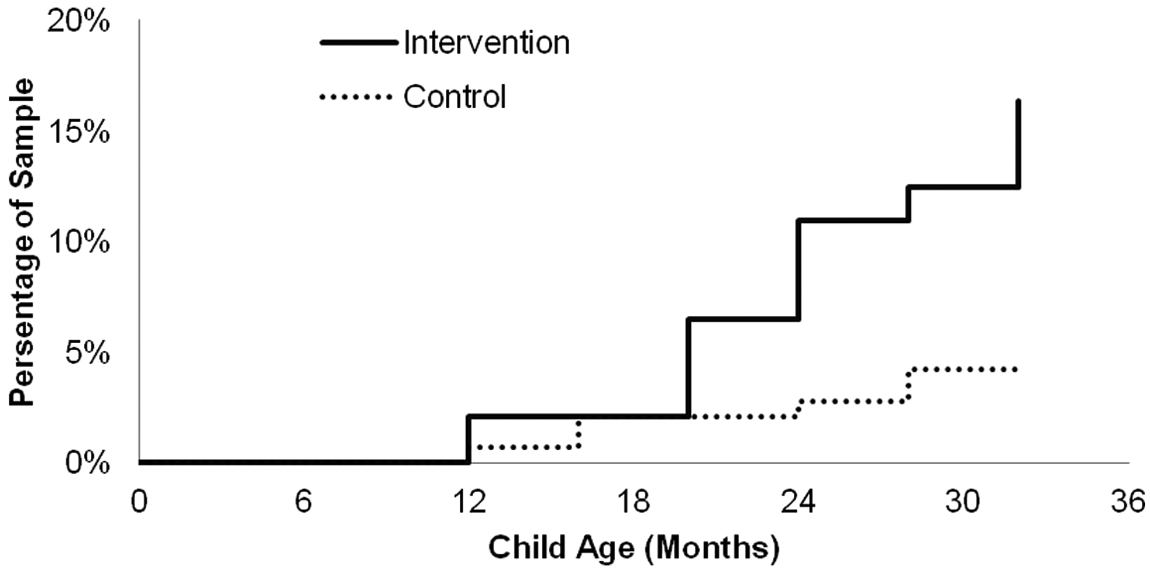
Time to First Receipt of EI Services, p < .01
Child Cognitive Outcomes
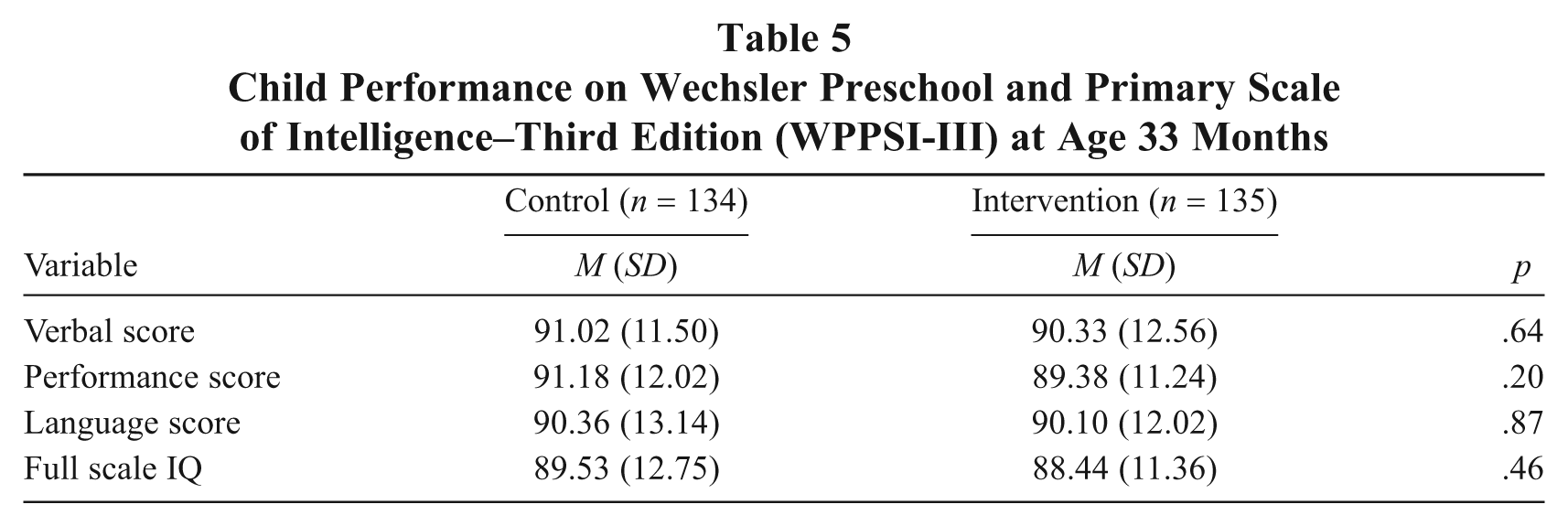
As shown in Table 5, there were no significant differences in cognitive outcomes at age 33 months for children in the intervention and control groups.
Child Performance on Wechsler Preschool and Primary Scale of Intelligence–Third Edition (WPPSI-III) at Age 33 Months
Discussion
Results from The MOM Program found developmental delays among 24% of the overall sample during developmental screenings at age 16 months. In addition, although there were comparable numbers of children in the intervention and control groups who showed developmental delays, children in the intervention group were more than three times as likely to receive EI services. Exploration of factors predicting referral to, and receipt of, EI services found that, across both groups, mothers who were slightly older (on average 23 instead of 21 years of age) and with slightly more symptoms of depression (on average 12 instead of 11) were more likely to have children referred to EI services and for those children to receive EI services.
As compared with other studies, our cohort showed higher rates of developmental delay. Rosenberg et al. (2008) found that 13% of children in a large national sample showed developmental delay, although national projections for children to show developmental delay were then at 2%. Although developmental delays are not uncommon among children living in poverty, not all children are screened as closely as the ones in our cohort, nor are mothers so systematically educated about child development. However, our cohort included only children who were singleton, full-term births without known medical or genetic conditions at birth; this would decrease the likelihood that there would be high rates of developmental delays (Marlow, 2004; Picard, Del Dotto, & Breslau, 2000). Our finding of relatively high rates of developmental delays within a presumably healthy cohort of children born to mothers living in poverty emphasizes the importance of providing maternal education about child development as well as early and repeated screenings for developmental delays for these families. This is particularly important in light of findings that show amelioration of early developmental delays through participation in EI programs (Bailey et al., 2004; Isaacs, 2008). In addition, extending the home-visiting program beyond the typical 2-year length allowed for screening and referral for EI services to occur more effectively. Because developmental delays are often not suspected until children show speech delays at 2 years of age (Glascoe, 2005), close monitoring of the children’s development, education on early child development milestones, and encouragement for mothers to follow up on developmental concerns were seen as essential in having children receive the necessary services. Interestingly, we found no group differences in child cognition at age 33 months. This may be indicative of further evidence of the general comparability of the intervention and control groups at 33 months, despite the group differences in referral to, and receipt of, EI services.
An intriguing finding is that, in addition to the effect of the intervention, slightly older mothers and mothers who showed slightly more depressive symptoms were more successful in referring their children to EI and more likely to have their children receive EI services. Maternal competence is known to increase with age (Mercer, 1985), which is why many home-visiting programs target teen mothers. Finding that slightly older mothers were more proficient at seeking services for their children is not, in itself, surprising. What is striking is that the mothers in the control group were, overall, less competent at obtaining EI services, although their ages were comparable with those of mothers in the intervention group.
Depression, with its characteristic reduced energy, pessimism, and disturbances in social relationships (APA, 2000), could presumably interfere with mothers’ ability to negotiate complex EI intake and service procedures. Interestingly, our study finds that higher rates of EI referral and service receipt were associated with increased maternal depression symptoms, though only in addition to the stronger effect of the intervention group. However, the level of depressive symptoms was relatively mild, subclinical, and similar in both the intervention and control groups. Our findings are not consistent with those of Minkovitz et al. (2005), whose large-scale study found that maternal depression was associated with decreased child health services. However, the relatively low level of depression among mothers in The MOM Program may have been such that mothers were less restricted in their ability to seek and obtain EI services. The focus of the program was not to ameliorate maternal depression but simply to empower mothers to seek and obtain necessary health services for their children.
Other factors that have been found to be barriers to accessing EI services, such as maternal income level, maternal education, and race/ethnicity, could not be examined due to the small and relatively homogeneous cohort, although other researchers have identified these as obstacles for obtaining EI services (Bailey et al., 2004; Bailey et al., 2005; Rosenberg et al., 2008). However, based on results from earlier studies, the largely African American, low-income sample in the current study might be expected to have difficulty accessing EI services (Rosenberg et al., 2008). Demonstrating significant differences in EI referral and enrollment in the intervention group is an important fulfillment of the program’s commitment to early developmental screening and follow-up when EI services were recommended.
Administration of the ASQ was used to evaluate child development status for the children in the intervention group in a more rigorous manner than the telephone-administered DDST, administered to all children in the study. Because the ASQ was the measure used by the City of Philadelphia for developmental screenings, we hoped to gather information that would be helpful to the mothers in advocating for their children’s EI participation. For this reason, results of the 18-month ASQ were shared with the mothers and with the child health care providers. The study design does not allow us to determine whether conducting the ASQ in this manner, and sharing the results with the mothers and child health care providers, was the “active” ingredient in the home-visiting program intervention, although it is certainly possible that this was a key element in the impact of the intervention.
Several limitations of the study must be noted. The initial high rate of refusal to participate in the study may affect the generalization of results, as the sample may have been biased toward those who perceived a need for services, or who were willing to participate in a service provision study. Those who refused study participation were slightly older than study participants but, in general, did not elaborate on their lack of interest in participating. The use of a telephone-administered DDST-II is a limitation for the collection of the 16-month developmental data, as this is not the method recommended by the authors. We adopted this method to be able to have comparable data on both groups of children, which would not otherwise have been possible. This study is also limited by the use of parent reports of EI service utilization. It would have been desirable to verify EI referral and access directly from the EI programs. In addition, independent verification of fidelity to the intervention offered by the home visitors was not obtained. The use of structured training, a detailed protocol, and a checklist for completing elements of each visit were designed to promote intervention fidelity. However, had we videotaped or audiotaped a sample of the home visits to determine intervention fidelity, we would have had greater assurance that the intervention had been delivered as planned, and we would have been able to report data on monitoring more precisely the fidelity of the intervention. Attempting to gather this type of data on the fidelity of the intervention would have been desirable and would have also allowed us to examine the participant acceptability of this procedure to monitor fidelity monitoring with our participants. In addition, although the study was designed to enhance maternal competence in providing for children’s health and development, these outcomes were assessed primarily by child outcomes. We did not gather systematic data regarding mothers’ perceptions of the home visits and the advice offered, which would have been helpful in informing future home-visiting practices aiming to target family-identified needs and preferences. Information on how maternal competence develops over the course of the intervention would have been helpful as well. Additional evaluations of maternal demographics at baseline, such as income and marital status, would have been useful to assess changes over the course of the intervention. Although the initial assessments of the mothers were planned to be brief, as mothers were being recruited in the postpartum unit of the hospital within 24 hr after having given birth, slightly expanding the scope of the initial assessment would have been fruitful for later analyses.
Although The MOM Program has the advantage of limited staff time involvement, and thus, lower costs, the focus of this home-visiting program is different from that of programs with more intensive interventions and that are geared toward mothers and children at higher risk. However, like those home-visiting programs with established empirical effectiveness (Duggan et al., 1999; Olds et al., 2002; Olds et al., 2004), The MOM Program uses a structured curriculum and goals for parents and children, and its design includes rigorous training and supervision of the home visitors. An innovative feature of The MOM Program is that of using a team of nurses and trained community home visitors, a method found in a recent meta-analysis to be equally effective in accomplishing home-visiting program goals (Nievar, 2010). Because 89% of program participants completed the 33-month intervention, we believe that some support is offered for the use of a “team” model of home visitors, rather than assigning a single home visitor to a family. Our program was not planned to be as intensive as some other home-visiting programs, in terms of number and length of home visits, so the “team” model of service provision was seen as appropriate for this model of service provision. A recent meta-analysis of results from home-visiting programs found that child outcomes were enhanced by increased numbers of home visits (Nievar, 2010). However, The MOM Program appears to have resulted in increased EI referrals and EI service receipt with relatively fewer and shorter home visits. More research is needed to determine whether fewer and shorter home visits might be sufficient to reach service referral and receipt goals.
In addition to recommending the use of a team approach to home visiting that includes nurses and community home visitors, The MOM Program offers other recommendations for practice. Having a weekly group supervision meeting was key to providing support to the home visitors in responding to the challenges that arose in the lives of the families and implementing the program. The weekly supervision meeting allowed not only for group problem solving but also for the provision of program support around the many frustrations that arose in the course of working with the families. Maintaining a positive attitude in the face of repeated telephone calls that were not returned, or attempted home visits at which no one was found to be home was challenging, but the weekly group meetings helped staff to “de-personalize” the difficulties, and also to work together to reach challenging families. The weekly supervision meeting was also important in that persistent and creative efforts to reach families were reinforced. A family that could not be reached during a typical workweek might be located in an unscheduled “drive-by” visit. Having a series of alternative contacts to draw on in reaching families helped maintain contact with those mothers who left the neighborhood, or who entered a shelter program. Because every family within the program was discussed each week, staff learned to clearly document their efforts. If new information became available, such as a new address or telephone number, this was recorded. The timing of all telephone calls was similarly noted, so that calls could be attempted at varying days and times during the week. Multiple staff members attempted family contacts, but in a well-coordinated manner. A key central element of the program was refusing to give up trying to reach the families served, which is applicable to various types of programs that serve families in their homes.
Although our program was developed within an academic children’s hospital, our children received health care services from a variety of providers in our city, including a number of public health clinics. Although providing regular developmental screenings for young children is part of the recommended guidelines for pediatric practice, we found that, in fact, many pediatric practitioners were conducting, at best, only brief developmental screenings. However, when provided with the results from the developmental screenings conducted through our program, the pediatric health care providers not only expressed appreciation but often worked with The MOM Program to facilitate EI program entry. Home-visiting programs not affiliated with a children’s health organization can work in tandem with child health care providers, with mothers’ permission, by requesting information on children’s health, such as immunization status, and by promoting regular child health care visits and sharing results of developmental screenings. In this way, home-visiting programs can create collaborative partnerships with child health care providers on behalf of vulnerable children and families.
We described results from our home-visiting program for children up to 36 months of age in this report, but our actual home-visiting program extended until the children reached 60 months of age. We thought it was important to extend the program beyond age 36 months because the problems facing mothers living in poverty around access to health care and educational services for their children do not diminish when children reach age of 3 years. A final report of the later outcomes from The MOM Program is in preparation, but we have reported preliminary evidence that children in the intervention group were significantly more likely to attend Head Start and to show reduced aggressive behavior (Schwarz et al., 2010).
In summary, The MOM Program provides initial notable and promising evidence for the utility of a brief, focused, home-visiting intervention to promote competence among low-income urban mothers in seeking and obtaining EI services for their children. Understanding how to promote low-income families’ access to EI is critical. The intervention appears to help mothers identify potential problems with their children and to access needed services. Public policy implications of this research include (a) the importance of developmental screenings in helping mothers understand children’s needs for services, (b) the importance of continuing home visits into the children’s 3rd year to identify delays and assist with accessing services, (c) initial support for a new model of home visiting that includes brief, focused interventions with multidisciplinary staffing, and (d) the importance of collaboration between pediatricians and early childhood interventionists in promoting early child development. The findings also support a need for more targeted services for younger mothers and raise questions about the relationship between maternal depression and service use.
Footnotes
Appendix A
Appendix B
Appendix C
Authors’ Note:
Donald F. Schwarz, Office of the Deputy Mayor of Health and Opportunity, City of Philadelphia, PA; Ann L. O’Sullivan, School of Nursing, University of Pennsylvania; Judith Guinn, Jennifer A. Mautone, and Elyse C. Carlson, The Children’s Hospital of Philadelphia, PA; Huaqing Zhao and Xuemei Zhang, Westat Biostatistics Data Management Core, The Children’s Hospital of Philadelphia, PA; Tara L. Esposito and Megan Askew, The Children’s Hospital of Philadelphia, PA; Jerilynn Radcliffe, The Children’s Hospital of Philadelphia, PA, and Perelman School of Medicine, University of Pennsylvania.
This work was supported by The William Penn Foundation (Grant 228-08). We wish to thank the following original staff members of The MOM Program for their contributions: Lori Romano, Wendy Mahoney, Kate Dillon, Suzette Harper, and LaVette Dibble.