
Abstract
Coaching caregivers of young children on the autism spectrum is a critical component of parent-mediated interventions. Little information is available about how providers implement parent coaching for children on the autism spectrum in publicly funded early intervention systems. This study evaluated providers’ use of parent coaching in an early intervention system. Twenty-five early intervention sessions were coded for fidelity to established caregiver coaching techniques. We found low use of coaching techniques overall, with significant variability in use of coaching across providers. When providers did coach caregivers, they used only a few coaching strategies (e.g., collaboration and in vivo feedback). Results indicate that targeted training and implementation strategies focused on individual coaching components, instead of coaching more broadly, may be needed to improve the use of individual coaching strategies. A focus on strengthening the use of collaboration and in vivo feedback may be key to improving coaching fidelity overall.
Leaders in early intervention increasingly recognize that coaching caregivers to use evidence-based interventions with their children enhances caregivers’ self-efficacy and ability to improve their child’s participation in daily routines (Hanft et al., 2004). Providing early interventions that include the entire family, not just the child, aligns with the family-centered practices that the Division for Early Childhood recommends for Part C early intervention (DEC, 2017) and guidelines for Part C services set forth in the Individuals with Disabilities Education Act (IDEA, 2004). The Program for Infants and Toddlers with Disabilities (Part C of IDEA) is a federal grant program that assists states in operating a comprehensive statewide program of early intervention services for infants and toddlers with disabilities, ages from birth through 2 years, and their families. Early intervention for young children on the autism spectrum 1 is typically provided through Part C–funded early intervention service providers. Caregiver coaching in early intervention is an interactive process between a practitioner and a caregiver intended to promote the caregiver’s ability to support the child’s participation in family and community settings (Hanft et al., 2004). High-quality caregiver coaching leads to improved parent responsiveness and use of interventions to promote their child’s communication and participation in daily activities (McDuffie et al., 2013; Moore et al., 2014). Including caregivers as partners in intervention delivery also leads to improved self-efficacy and engagement, and reduced caregiver stress (Estes et al., 2014; Siller et al., 2018). Recent reviews have also found that parent-mediated interventions lead to improvements in children’s language and communication skills (Heidlage et al., 2020; Trembath et al., 2019).
Most effective coaching models are largely based on adult learning theory, which posits that adults benefit from specific strategies other than didactic instruction to motivate and teach them (Knowles et al., 2020). Effective caregiver coaching should be provided in the family’s home or community and include a repertoire of strategies to increase caregivers’ skills, motivation, and self-efficacy (Dunst et al., 2010; Rush et al., 2003). Five core elements of effective coaching include (a) the use of authentic learning experiences: taking advantage of learning opportunities that occur as part of real-life challenges or usual daily routines, (b) collaborative decision-making: actively involving the caregiver in selecting learning goals and intervention techniques, (c) demonstration: modeling the use of techniques through role-plays or actual application, (d) in vivo feedback: observing the caregiver’s use of intervention techniques and providing immediate feedback, and (e) reflection: engaging the caregiver in self-evaluation or assessment of their performance.
There have been increasing efforts to train early intervention providers in using caregiver coaching strategies (Dunst, 2015; Dunst et al., 2015). However, most related studies find that providers infrequently use coaching strategies during sessions (Campbell & Coletti, 2013; Douglas et al., 2020). Instead, they are more likely to work directly with the child than to coach caregivers (Salisbury et al., 2012). Caregivers often observe rather than interact with their child during intervention sessions (Campbell & Sawyer, 2007). When providers do use coaching strategies, they are more likely to use an expert teaching model, such as sharing information with caregivers, rather than providing direct feedback about the parents’ use of intervention techniques.
While almost all caregivers of children with disabilities can benefit from coaching, this may be especially true for parents of children on the autism spectrum, in large part due to the rise in evidence supporting parent-mediated interventions for autism spectrum disorder (ASD; Green et al., 2015; Oono et al., 2013). Growing evidence suggests that coaching caregivers of young children on the autism spectrum to implement intervention strategies leads to children’s improved cognitive ability, social functioning, functional behavior, and daily living skills (Green et al., 2010; Kasari et al., 2014; Rogers et al., 2012; Stahmer et al., 2020). There is little information, however, about how these parent-mediated interventions are translated into practice in Part C early intervention service systems. It is likely that the same poor implementation of caregiver coaching in early intervention more broadly is present for families of children on the autism spectrum receiving early intervention services. A clear understanding of how Part C early intervention providers coach caregivers of young children on the autism spectrum is lacking and would offer an important first step toward developing strategies to support the widespread implementation of evidence-based, parent-mediated interventions.
The goal of this descriptive observational study was to understand how early intervention providers are using parent coaching within usual care through observations of usual practice for children on the autism spectrum. We aimed to evaluate whether early intervention providers use parent coaching strategies during their usual early intervention sessions and the extent to which coaching strategies are implemented with fidelity to best practices in caregiver coaching. We hypothesized that early intervention providers would demonstrate low fidelity to evidence-based caregiver coaching strategies when working with families of young children on the autism spectrum during their usual sessions. We also explored differences in use of coaching strategies during in vivo sessions and telehealth sessions during the shift to telehealth observed during the pandemic.
Method
Setting
This study was conducted in the early intervention system in a large city in the United States. In this system, ASD likelihood and service eligibility are determined using the Modified Checklist for Autism in Toddlers (Robins et al., 2013), which is a clinical observation and parent interview measure. Each year, this early intervention system serves approximately 850 children with, or at increased likelihood for, ASD through service contracts with 13 provider agencies. Providers from these agencies provide services in the families’ homes, using an interdisciplinary family-centered approach. In April 2020, service delivery pivoted from home-based to a telehealth model in response to the coronavirus disease 2019 (COVID-19) pandemic.
Participants
Providers
We enrolled 25 Part C early intervention providers. Inclusion criteria for providers were as follows: (a) employed by a Part C early intervention agency, and (b) have at least three children in the ASD service classification on their caseload. Agency leaders distributed information about the study to providers. Interested providers contacted the study team and were then screened for eligibility.
Parents and children
Families were selected from participating providers’ caseloads and invited to participate in the study. Inclusion criteria for families were as follows: (a) child less than 36 months of age, (b) child has a classification of ASD or is considered high autism likelihood as determined by the early intervention system, (c) family receives early intervention services through the Part C early intervention system, and (d) parent speaks English or Spanish.
Observations
We recorded one early intervention session with each participating family. Sessions averaged 50 min with a range from 24 to 96 min. We started data collection for the study prior to the COVID-19 pandemic and continued during the pandemic, requiring a shift in data collection procedures. Prior to the pandemic, observations occurred in the family’s home, the usual setting for Part C early intervention services. A research team member traveled to the family’s home and video-recorded one early intervention session with the family and provider. During the pandemic, the early intervention system pivoted to providing early intervention services through tele-intervention. We obtained video recordings through a secure teleconference platform for these sessions. We observed 10 in-person sessions before the pandemic, and 15 tele-intervention sessions during the pandemic. The content and focus of early intervention sessions during the pandemic continued to focus on administration of the child’s Individualized Family Service Plan as much as possible, as mandated by the early intervention system.
Coaching Fidelity Measure
We adapted a coaching fidelity tool to assess providers’ use of evidence-based coaching strategies during observations. The coaching fidelity tool combined elements from the Triadic Intervention and Evaluation Rating Scale (TIERS; Basu et al., 2010) and a parent coaching fidelity form from a commonly used parent-implemented ASD intervention, the Project ImPACT Fidelity of Implementation for Coaching Form (Ingersoll & Dvorstak, 2010). The TIERS is a validated observational tool designed to measure the use of parent-focused and collaborative coaching techniques in early intervention. The Fidelity of Implementation for Coaching Form was developed for the Project ImPACT curriculum and has been used to assess parent coaching of parents of young children with autism and developmental delays (Stadnick et al., 2015; Stahmer et al., 2020). We combined the TIERS and Project ImPACT: Fidelity of Implementation for Coaching Forms to ensure that we captured generally agreed-upon parent coaching activities and those that are used in autism-specific interventions. The combined set of items was reviewed to remove duplicate items. We categorized the remaining items under the five elements of parent coaching: collaboration (actively involving the caregiver in selecting intervention techniques), daily routines (practicing or discussing the use of intervention strategies within usual daily activities), demonstration (modeling and explaining how to use intervention strategies), in vivo feedback (delivering feedback about the caregivers’ use of intervention strategies), and reflection/problem-solving (engaging the caregiver in self-evaluation or assessment of their performance). We then added new items to ensure that the form captured provider’s fidelity to all five parent coaching elements. Items that did not fit in one of the five parent coaching strategies were excluded. The coaching strategies measured on the coaching fidelity checklist are derived from evidence-based practices in caregiver coaching and adult learning theory and are considered best practice in caregiver coaching, regardless of provider discipline. Finally, we consulted four experts in parent coaching, parent-mediated intervention, and early intervention to assess the content validity of the adapted tool and made modifications based on their expert feedback. All of the experts rated the final tool as valid for measuring the essential elements of parent coaching. The adapted coaching fidelity form consisted of 25 items (see Table 1 for items). Fidelity was rated on a 5-point scale ranging from 1 (never observed) to 5 (almost always observed), with a rating of 4 or 5 indicating acceptable fidelity. We calculated a summary score for each coaching domain by averaging the ratings for each item in the domain (e.g., a fidelity score for collaboration comprised the mean of the four items in the collaboration domain for each provider) and an overall fidelity score was calculated as the mean for all of the scored items.
Items Included in the Adapted Coaching Fidelity Scale.
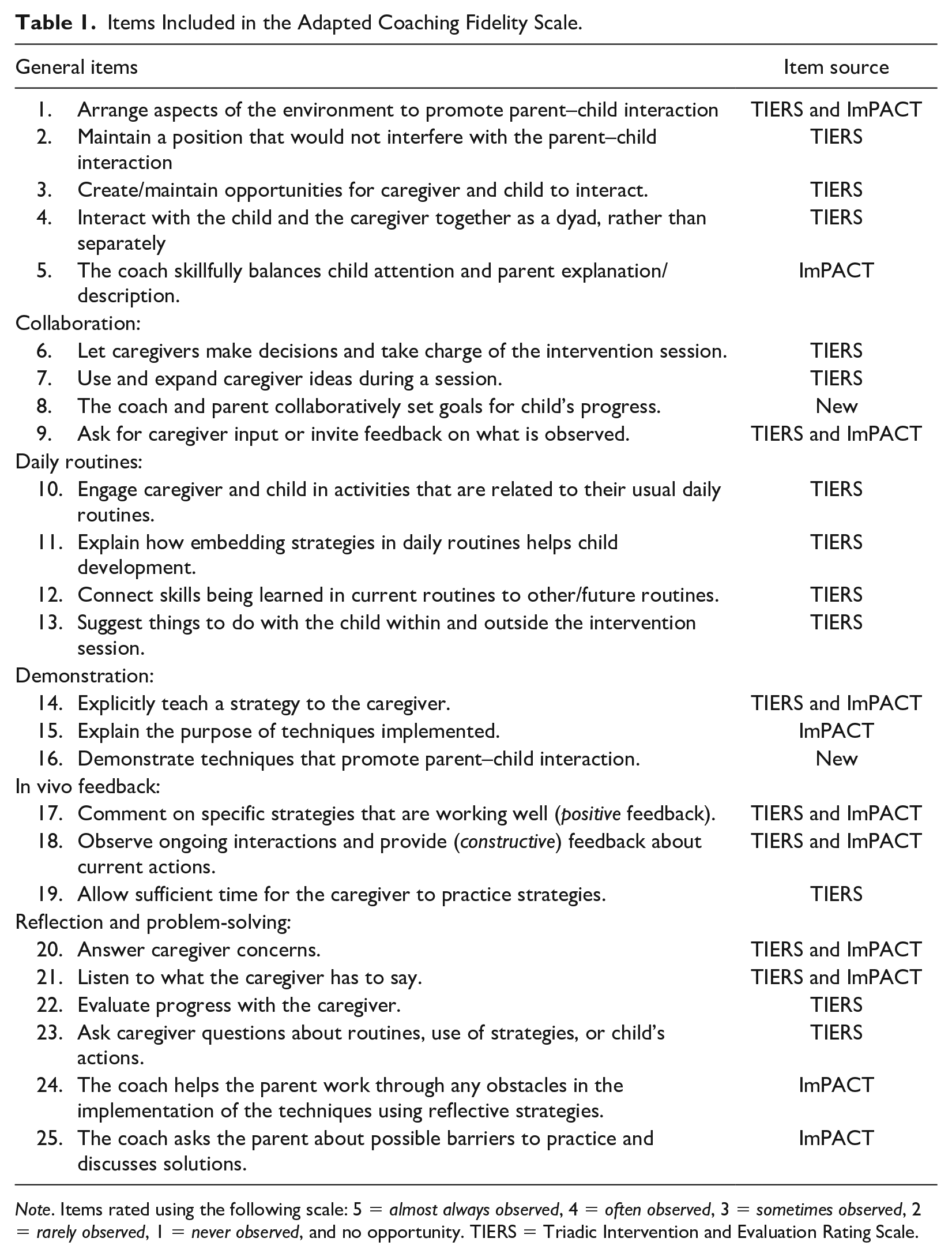
Note. Items rated using the following scale: 5 = almost always observed, 4 = often observed, 3 = sometimes observed, 2 = rarely observed, 1 = never observed, and no opportunity. TIERS = Triadic Intervention and Evaluation Rating Scale.
Video Coding
Trained research assistants coded video recordings of each session using the adapted coaching fidelity form. Research assistants were trained to manage inter-rater agreement at the item level of at least 90% interobserver agreement within 1 point on each item prior to coding any videos. Twenty percent of the videos were double-coded to ensure agreement. Interobserver agreement was strong (M = 95%, range = 86%–100%) and discrepancies were discussed and resolved through consensus.
Data Analysis
We calculated descriptive and summary statistics for each observation and across observations. We calculated mean fidelity for each coaching strategy and overall coaching fidelity for each observation. Summary means, standard deviations, and ranges for each coaching strategy and overall fidelity were calculated across providers. We were also interested in whether the use of particular coaching strategies was correlated with use of other coaching strategies. We therefore computed correlation coefficients for each pair of coaching strategies. An independent samples t test was used to compare coaching fidelity for sessions conducted in person and through tele-intervention.
Results
Demographic characteristics for providers and families are presented in Table 2. Consistent with the interdisciplinary approach of Part C early intervention systems, providers varied in their disciplinary backgrounds: 79% were special instructors (instructors who provided services in families’ homes), 11% were occupational therapists, 5% were speech and language pathologists, and 5% were physical therapists. Providers had an average of 8.5 years of experience working in early intervention (range = 1–30 years), 78% reported receiving specialized training in autism interventions, and 68% reported receiving training in parent coaching. The providers were all female of whom 63% were White, 16% were Black, 11% were Hispanic, 11% were Asian, and 5% identified as multiracial. The demographic characteristics and training experience of these 25 providers were consistent with those of providers in the early intervention system overall.
Demographic Characteristics of Study Participants.

Twenty-five caregivers of young children receiving Part C early intervention services participated. Caregivers were from diverse ethnic backgrounds: 28% were Black, 28% were Hispanic, 24% were White, 12% were multiracial, and 8% were Asian. Caregivers’ ages ranged from 25 to 50 years, with a mean age of 31 years. There was a wide socioeconomic diversity among participating families: 42% of families reported an annual household income of less than US$20,000, 17% reported annual incomes between US$20,000% and US$40,000, 13% reported incomes between US$40,000 and US$60,000, and 28% reported an annual income >US$60,000. Children were, on average, 21.5 months of age (SD = 7.78, range = 12–35 months). Twenty-two families spoke English as their primary language and received services in English. Three families spoke Spanish as their primary language and received early intervention services in Spanish.
Providers demonstrated considerable variability in their use of coaching strategies (Figure 1). Providers had the overall lowest fidelity ratings for working within Daily Routines (M = 2.22, SD = .71) followed by Collaboration (M = 2.58, SD = .95). The mean fidelity score for Demonstration was 3.49, with greater variability in use of this strategy across providers (SD = 1.21). Mean fidelity for Reflection and Problem-Solving was 3.70, with less variability across providers (SD = .67), and mean fidelity for In Vivo Feedback was 3.80 (SD = 1.07). Mean overall coaching fidelity was 3.27 (SD = .60).
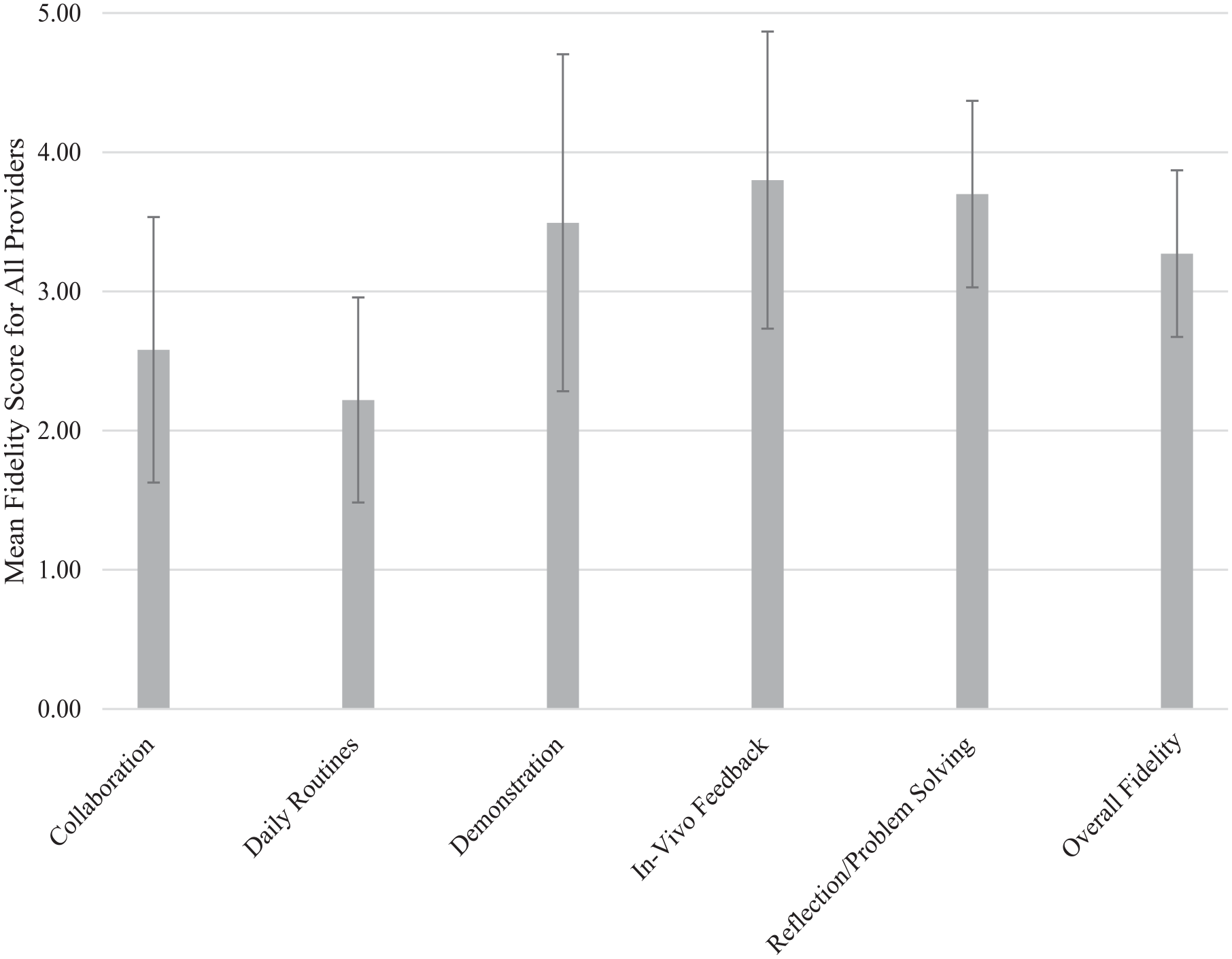
Observed coaching fidelity during usual early intervention sessions.
Correlations between each pair of coaching components are presented in Table 3. A strong correlation was observed between Collaboration fidelity and In Vivo Feedback Fidelity (r = .68, p = .0001). A moderate correlation was also observed between the use of Collaboration and Daily Routines (r = .44, p = .027) and In Vivo Feedback and Daily Routines (r = .43, p = .038).
Correlations Among Fidelity of Use of the Coaching Strategies.
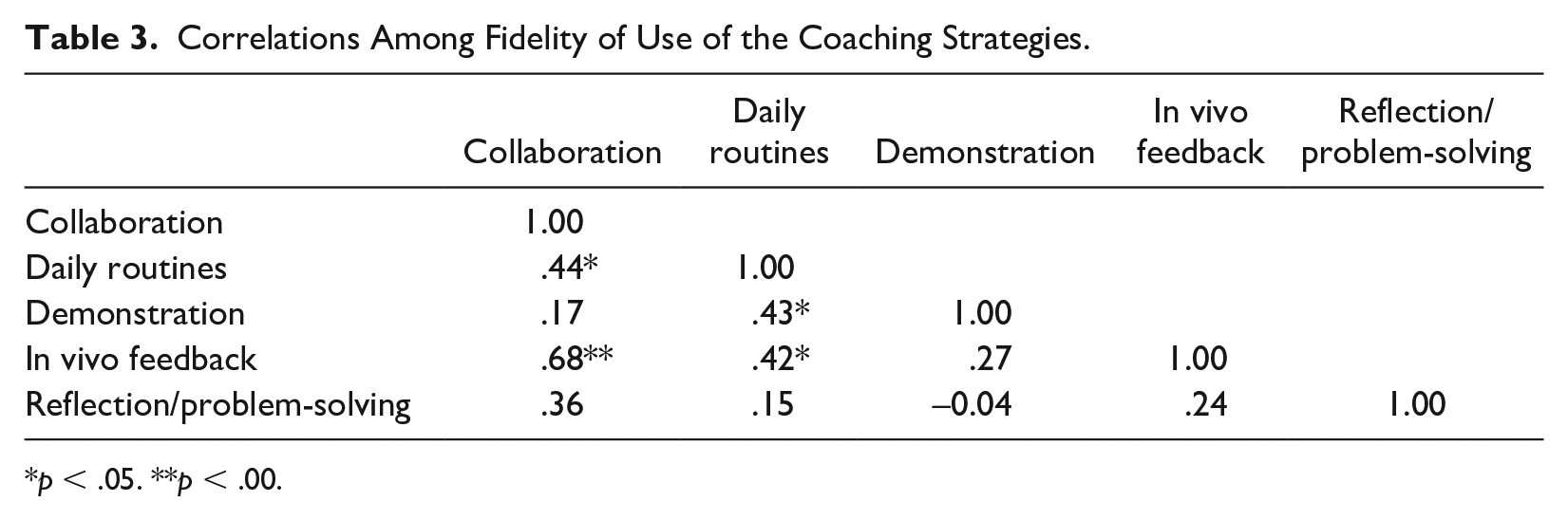
p < .05. **p < .00.
We found no statistically significant differences in coaching fidelity between in-person and tele-intervention sessions for any of the coaching strategies, namely, collaboration: t(19) = –.21, p = .83; daily routines: t(10) = –.70, p = .49; demonstration: t(16) = –.74, p = .47; in vivo feedback: t(19) = –.46, p = .65; reflection/problem-solving: t(14) = .58, p = .57; or for overall coaching fidelity, t(14) = –.62, p = .54.
Discussion
We assessed providers’ use of parent coaching during their usual early intervention sessions with families of young children on the autism spectrum in the Part C early intervention system of one large city. We hypothesized that providers would demonstrate low fidelity to evidence-based caregiver coaching strategies during their usual sessions. Our observations supported this hypothesis. Providers’ use of parent coaching strategies was generally low and they used some strategies more than others. Some providers used specific coaching strategies consistently but other providers rarely used them and providers’ use of a given strategy was only partially associated with their use of other strategies.
Previous research has found that autism support teachers’ attitudes and beliefs about interventions, and their self-efficacy related to implementing an intervention are associated with their use of specific evidence-based practices in schools (Locke et al., 2019). Similarly, early intervention providers’ attitudes and beliefs about caregiver coaching, and their self-efficacy with using caregiver coaching with families of young children on the autism spectrum, likely influenced their use of these strategies. Future research evaluating early intervention providers’ attitudes, beliefs, and self-efficacy with caregiver coaching is needed to inform the development of targeted implementation strategies to improve the use of coaching in early intervention for these families.
We found that providers who used collaborative coaching strategies were more likely to use in vivo feedback during sessions. Collaborating with caregivers about their child’s treatment has been associated with increased caregiver empowerment and buy-in with their child’s treatment (Dempsey & Dunst, 2004; Thompson et al., 1997). Similarly, in vivo feedback is a core component of coaching linked to improvements in caregivers’ use of intervention strategies and subsequent gains in children’s communication and behavior skills (Caron et al., 2016; Shanley & Niec, 2010). Although our findings are preliminary, they signal a relationship between these two coaching strategies. We hypothesize that feedback and collaboration occurred together because taking the time to collaborate with caregivers and empower them to become active partners in their child’s intervention strengthens the therapeutic alliance and makes it easier to deliver constructive feedback. This interpretation is consistent with previous findings demonstrating the additive value of combining several adult learning practices, such as collaboration and in vivo feedback, on improving adult learner outcomes (Dunst & Trivette, 2012).
Of all the coaching strategies, providers had the lowest fidelity to implementing intervention practices within daily routines. Providers rarely coached families to practice intervention skills during usual daily activities. Instead, providers were more likely to work with families during a contrived play session. Intervention goals for young children on the autism spectrum are often focused on improving social communication skills and using a child’s motivation and interests to guide the intervention. These approaches are often implemented during play-based activities. However, guidance for coaching caregivers of young children emphasizes the importance of learning skills within daily routines to facilitate sustained practice (Romano & Schnurr, 2020; Santana, 2020). Coaching caregivers to use intervention strategies within daily routines can also improve the generalization and usefulness of the skills they learn. It can also reduce caregiver burden by providing them with tools to support their child within already occurring routines, instead of adding additional time for intervention into their family schedule (Stahmer & Pellecchia, 2015). Approaches to embedding ASD intervention strategies within naturally occurring routines are well established (Wetherby & Woods, 2006), but our data suggest that they are not being implemented in community-based early intervention.
Training and supervision for providers working with young children usually emphasizes child-directed intervention strategies (Dunst et al., 2019). Although many intervention manuals mention training parents of children on the autism spectrum, they largely focus on how to work directly with the child instead of how to coach parents. The early intervention system, partnering on this project, recognized the need for targeted training in caregiver coaching and implemented a countywide didactic training series focused on caregiver coaching. Most providers we observed reported receiving training in caregiver coaching; however, we found that most of these providers did not use caregiver coaching during their sessions. This is consistent with previous research indicating that training alone is not sufficient to change provider behavior (Beidas et al., 2012). Targeted implementation supports that move beyond training are needed to improve the use of caregiver coaching within early intervention for families of young children on the autism spectrum.
We were surprised that there was no difference in the use of coaching between sessions delivered in person and through tele-intervention. Recent reports of the use of telehealth for ASD treatment report that caregivers are more involved during telehealth sessions (White et al., 2021; Yi & Dixon, 2021). Our results, however, found no significant difference in use of evidence-based coaching strategies for sessions occurring in person versus through tele-intervention. Caregivers who were involved during tele-intervention sessions were typically involved in lengthy conversations about the child’s goals, updating on the family’s activities since the previous sessions, and talking through suggestions for practice instead of using direct coaching strategies to actively engage the caregiver in learning intervention strategies. Involving caregivers during early intervention sessions is necessary but not sufficient to promote caregiver use of intervention strategies. This is an interesting preliminary finding that warrants further exploration in larger samples, given the continued use of telehealth to deliver intervention.
An important area for future research is to better understand parents’ and caregivers’ perspectives toward participating in caregiver coaching sessions. Providers may not have coached caregivers because the caregivers preferred a more child-directed approach to early intervention. Understanding caregivers’ attitudes toward coaching and their expectations for involvement in their child’s sessions can lead to a more collaborative and family-centered approach to early intervention. Developing strategies to support early intervention providers in building rapport with caregivers and gaining buy-in from caregivers related to coaching may improve the implementation of caregiver coaching within early intervention for young children on the autism spectrum. Similarly, future research should explore providers’ perspectives toward coaching caregivers of young children on the autism spectrum. Given the low use of caregiver coaching we observed, further inquiry into perceived barriers and facilitators to coaching within early intervention are needed, so as to inform the development of strategies to improve its implementation in Part C early intervention.
Several study limitations are worth noting. The small sample size limits the generalizability of the findings. However, our findings are consistent with previous evaluations of caregiver coaching in early intervention, showing limited use of caregiver coaching with families of young children more broadly (Douglas et al., 2020; Romano & Schnurr, 2020). In addition, the providers we observed responded to our recruitment flyer and were interested in participating in the study. These providers may have been more engaged and motivated than other providers in the early intervention system. If that is the case, then our findings regarding use of evidence-based coaching may represent an overestimate of the use of coaching in Part C early intervention more broadly, which would amplify the need for additional implementation supports to improve the use of parent coaching for young children on the autism spectrum. Although the sample is limited, the study offers the first examination of the use of caregiver coaching for families of young children on the autism spectrum served in publicly funded early intervention programs. Given the growing support for the use of caregiver coaching and parent-mediated interventions for young children on the autism spectrum, an examination of how providers working in publicly funded early intervention use coaching is an important tool for developing implementation targets and strategies to improve the use of caregiver coaching in early intervention.
Conclusion
Parent-mediated interventions for young children on the autism spectrum are gaining increasing support as effective and feasible models of intervention delivery. Parent coaching is a critical aspect of all parent-mediated intervention models. Our observations of early intervention sessions for young children with ASD found infrequent use of evidence-based coaching strategies, highlighting an important and understudied implementation gap. Future research should elucidate the reasons for this implementation gap and develop implementation strategies to improve the use of evidence-based caregiver coaching with families of young children on the autism spectrum. We also found that providers used some individual coaching strategies but did not use others, suggesting the need for targeted training and implementation strategies focused on individual coaching components, instead of coaching more broadly.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported here was supported by the Institute of Education Sciences, U.S. Department of Education, through Grant R324B180017 to the University of Pennsylvania. The opinions expressed are those of the authors and do not represent views of the Institute or the U.S. Department of Education.