
Abstract
Premature, untimely, or traumatic death of a family member has been shown to be related to later substance use issues among some surviving family members. However, research on these deaths has been limited in that no studies to date have explored associations between these deaths and other mental health disorders co-occurring with substance use. Therefore, this study examined the relationships between premature, untimely, and traumatic deaths of family members (parents, grand- and great grandparents, other family members, and pets) and comorbid psychopathology among a convenience sample of 104 individuals attending treatment for substance use issues. Results indicated that these kinds of death are commonly found within the families of the respondents. In addition, it showed that these deaths were significantly related to higher levels of comorbid anxiety, mood, and personality disorder symptoms. Of particular interest was the finding that these symptoms were significantly related to death among respondents’ grand- and great grandparents rather than among their nuclear families. Further research is needed to assess what kinds of family dysfunction related to death are present in this population and what kinds of interventions may be effective in treating them.
Substance use disorders (SUD) are a perplexing and persistent problem that impacts not just the individual who abuses alcohol and drugs but also affects the community at large. The abuse and misuse of substances costs the United States more than $410 billion per year through the criminal justice and health-care systems as well as through lost work productivity (National Institute on Drug Abuse, 2015). In addition, another $600 billion goes to the cost of treating SUD. The presence of mental health disorders comorbid with SUD tends to complicate treatment (Cacciola, Alterman, McKay, & Rutherford, 2001; Myrick & Brady, 2003). Therefore, it is important to identify risk factors associated with comorbid disorders commonly found among individuals in treatment for SUD.
One such risk factor is death of a family member. Even under the very best of circumstances, the loss of a family member to death is very difficult for the surviving family members to manage. Walsh and McGoldrick (2004) have discussed how death of a family member can have long-term negative effects stemming from the need to accommodate major changes in the family system and realignment of its emotional field. Walsh and McGoldrick point out that although the response to the death will be influenced by the family's existing belief system, that belief system will itself be modified by the death (as well as by other experiences of loss). Thus, in the current study, we explore the possibility that experiencing premature, untimely, and traumatic death (PUT) in the family system may have long-term effects on the surviving family members’ relationships and mental health status. For the purposes of this study, premature death refers to the death of any family members who died at a young age (i.e., at an age that death would not generally be expected, such as in childhood, or early adulthood). Untimely death refers to dying at a particularly difficult time such as on Christmas Eve, at a wedding, or just after someone else important to the family died. Finally, traumatic death refers to any particularly traumatic way of dying including, but not limited to, murdered, extreme pain or humiliation, auto accident, fire or explosion.
In regard to untimely death, McGoldrick and Walsh (2004) also explained that the timing of a given loss within a family's life cycle can influence the level of impact the death will have. That is, if a loss occurs “off-time” (p. 29) for the family, such as when a child loses his or her mother at an early age, when parents lose a child or a spouse dies early in life, acceptance of the death may be more difficult for the family. In addition, McGoldrick and Walsh suggested that multiple losses, or a loss co-occurring with the stress of other major life cycle or developmental changes, can influence the family's ability to adjust. In addition, these authors suggested other factors that may complicate grief and mourning in a family: a family history of traumatic loss and of unresolved mourning, the nature of the death, and the significance and function of the person who has died to the family.
Although the vast majority of the research concerning death of family members is focused on the death of a parent as discussed earlier, a small amount of research has considered other family members. For example, Crehan (2004) noted that the death of a sibling during childhood may result in later death anxiety or distorted thinking concerning illness, the most harmful effects on the surviving sibling are related to the emotional unavailability of the parents due to their own grief. In addition to individuals who are traditionally considered to be family members (e.g., mother, father, sister, brother, grandparents, etc.), some literature suggests that pets may be considered by many individuals to be family members and may be mourned as such in the event of their death (Durkin, 2009; Field, Orsini, Gavish, & Packman, 2009; Morley & Fook, 2005). Cordaro (2012) has suggested that since many people do not understand the level of grief, an individual may suffer at the loss of a pet, the person who has suffered the loss may experience disenfranchised grief, complicating the grieving process and possibly resulting in clinical levels of depression.
For decades, a considerable body of research has explored the relationships between family death and substance use issues (Bowser, Word, Stanton, & Coleman, 2003; Coleman, 1978; Coleman, Kaplan, & Downing, 1986; Furr, Johnson & Goodall, 2015; Hawks, Mitcherson, Ogborne, & Edwards, 1969; Risser, Bonsch, & Schneider, 1996). For example, clinical studies in the 1960s noted relationships between premature, unexpected, or traumatic family loss, and opiate and cocaine addiction (Ellinwood, Smith, & Vaillant, 1966; Hawks et al., 1969). In an early study of death among family members of heroin addicts, Coleman (1978) reported that among a sample of individuals in treatment for heroin addiction, 72% of their families had experienced the premature, untimely, or traumatic death of at least one family member. Coleman also pointed out that individuals with heroin dependency reported unexpectedly high rates of deaths among their grandfathers occurring during their fathers’ childhoods. In a later study, Coleman et al. (1986) compared a group of individuals with heroin dependency attending a methadone maintenance program with a normal group consisting of students enrolled in college, and a psychiatric group attending outpatient treatment. They found that the heroin-dependent individuals reported a significantly greater number of premature and unexpected deaths in their families than the other two groups.
Researchers have interviewed relatives of deceased individuals who had SUD issues, finding that 80% of these individuals had experienced at least one trauma during childhood, the most common trauma being the divorce or death of their parents (Risser et al., 1996). In addition, unresolved grief has been shown to be a common experience among substance abusing women (Raskin, 1992). In more recent research, Nickerson, Bryant, Aderka, Hinton, and Hofman (2013), utilizing a sample of 9,292 adults from the National Comorbidity Survey-Replication study, reported that about 25% of those with alcohol abuse or dependence and about 12% of those with drug abuse or dependence reported having lost a parent. Unfortunately, Nickerson et al. provided no information concerning whether these losses were PUT deaths or not. Another recent study that identified losses experienced before and while abusing substances and while in treatment found that 72% of their sample of 68 individuals had experienced the death of someone special (though unspecified) at some point before becoming substance dependent (Furr et al., 2015). Research on intravenous drug users has also found robust relationships between the extent of HIV risk-taking behaviors during adulthood and the number of deaths of close family members experienced during childhood, the effectiveness of the mourning process, the closeness of the relationship with the deceased, and attendance at the funeral (Bowser et al., 2003).
Although the studies discussed earlier brought the issue of family death to the attention of the substance abuse research and practice communities as being a relatively common occurrence, they tended either to focus on a particular substance (e.g., heroin) or on problems associated with the death of a parent. Therefore, it is not yet known if these kinds of death are related to the broad range of SUD problems normally seen in treatment or if the death of other family members may also be problematic. In addition, these studies have failed to examine how these deaths may be related to the comorbid mental health issues commonly seen in individuals in treatment for SUD issues. Instead, studies that have explored death and mental health disorders have involved individuals without comorbid SUD issues. Below is a brief review of the literature concerning family death experiences and mental health disorders other than SUD.
Family Death, Depressive, and Anxiety Disorders
Research has shown that the early death of a parent is linked to major depressive disorder (MDD; Jacobs & Bovasso, 2009; Kunugi et al., 1995; Tyrka, Wier, Price, Ross, & Carpenter, 2008) as well as to phobia and alcohol dependence (Otowa, York, Gardner, Kendler, & Hettema, 2014) later in life. Nickerson et al. (2013) found that most of the anxiety and mood disorders (as well as intermittent explosive disorder) were significantly associated with the loss of a parent earlier in life and suggested that the early death of a parent acts as a “non-specific risk factor” (p. 123) for the development of psychopathology in adulthood. Their findings also showed that the earlier the age of the loss of a parent, the more at risk the individual was for psychopathology when they reached adulthood, suggesting the possibility that disrupted attachment might be a predisposing factor in its development. Furthermore, Nickerson et al. suggested that the loss of one parent might affect the ability of the surviving parent to provide adequate care to the child. This deficiency could then compromise the ability of the child to manage distress and regulate emotions through childhood and adolescence, thus contributing to the development of later psychopathology. Although these studies have shown connections between parental death and later psychopathology, they have not explored how the death of other family members may be related to these disorders. Miyabayashi and Yasuda (2007) found that people who had suffered the loss of a loved one to some form of sudden death (suicide, accident, and acute illness) reported clinical levels of both physical health problems and depression. Unfortunately, they did not specify the relationship of the loved ones and so it is not known if they were family members.
Complicated grief may also be associated with depressive disorders (Zisook, Shuchter, Sledge, Paulus, & Judd, 1994) as well as with anxiety disorders (Jacobs et al., 1990) and posttraumatic stress disorder (PTSD; Murphy et al., 1999). In more recent research, it was reported that levels of MDD, PTSD, and prolonged grief failed to decrease over a 6-year period among one third of a sample of individuals who had lost family members in a sudden natural disaster (Kristensen, Weisaeth, Hussain, & Heir, 2015). There was no attempt, however, to relate grief and psychopathology to SUD disorders in these studies.
These results as well as other research on bereavement due to sudden, unexpected loss (Prigerson et al., 2009; Simon et al., 2011) suggest that for some individuals a chronic grieving state may last for many years. However, the effects of grief are not limited just to those who have directly suffered the loss of a loved one. Walsh and McGoldrick (2004) suggested that the pathological mourning of a family member's death can result in anxiety and depression that may become part of “the chain of influences that reverberate throughout the family network of relationships, including partners, parents, children, siblings, and extended kin” (p. 6). Gajdos (2002) also noted a “cascade of anxiety” (p. 306) after the death of an important grandparent that can flow down the generations through the Bowenian concept of emotional triangulation. Gajdos suggested that this triangulation may result in problem behaviors in a grandchild who may have had little or no direct emotional relationship with the grandparent. Similar to the studies mentioned in previous paragraphs, none of these investigations explored the relationships between pathological grief and addiction. However, Brave Heart (2003) has noted the impact of historical trauma on rates of PTSD and other anxiety disorders, depression, and addiction in Native American communities.
Family Death and Personality Disorders
Very few studies have been conducted to explore possible relationships between bereavement and the development of personality disorders. Reich (1986) found significantly higher rates of antisocial personality disorder among individuals in outpatient treatment for psychiatric issues who had suffered the early death of a parent. Other researchers who compared women diagnosed with borderline personality disorder with women with other personality disorders found that there was significantly more loss of a parent among the women with borderline (LaPorte & Guttman, 1996). More recently, a group of researchers (Liotti, Pasquini, & the Italian Group for the Study of Dissociation, 2000) compared psychiatric clients diagnosed with and without borderline personality disorder for differences in distribution of clients’ early traumatic experiences and perinatal losses experienced by clients’ mothers. Liotta et al. found that a client whose mother had experienced serious loss of an attachment figure within 2 years of the client's birth was 2.5 times more likely to develop borderline personality later in life than a client whose mother had not experienced such a loss. Similar to the research on death and depressive or anxiety disorders discussed earlier, these studies failed to examine the relationships between family death and personality disorders among individuals with co-occurring SUD.
Study Rationale
One limitation of early studies of premature, untimely, and traumatic (PUT) death is that they have focused on individuals with opiate or cocaine addiction (Coleman, 1978; Coleman et al., 1986; Ellinwood et al., 1966; Hawks et al., 1969). In addition, they have failed to examine the potential impact of the PUT deaths of other family members other than parents on individuals’ mental health symptomatology. Finally, they have not explored the relationships between these deaths and other comorbid mental health disorder commonly found in individuals in treatment for SUDs. The goals of the current study were to address these gaps and determine the prevalence of PUT death experiences among the families of individuals receiving treatment in a residential SUD facility. Family members included parents, siblings, grandparents, great grandparents, other family members, and pets. Grandparents and great grandparents were included in the questionnaire to explore the possibility of intergenerational transmission of dysfunction associated with PUT death. In addition, we aimed to examine the impact that these losses among their families had on the psychopathology of these individuals including anxiety disorder, MDD, and personality disorders.
Method
Participants
After approval from the university internal review board was granted, a sample of 104 individuals consecutively enrolled into treatment in a for-profit residential substance abuse treatment center located in southeastern Florida was recruited. Services provided by the agency included detoxification services as well as residential, partial hospitalization, intensive outpatient, and outpatient services; most of the services are paid by third party reimbursement. All of the clients who participated in the study were part of the residential treatment program, having stepped down from the detox unit after having achieved medical and psychiatric stability sufficient for the lower level of care. Within 72 hours of entry into the residential unit, clients underwent a psychosocial assessment as a normal part of the agency's intake procedure. At the time of the assessment, clients were recruited by clinical staff at the agency to participate in the study. After signing a consent form, clients were given a brief check-off list containing three questions about their experiences of premature, untimely, or traumatic death of family members (see Appendix A) which they completed and returned during the assessment process. Clients who refused to sign the consent form were not given the questionnaire and were not included in the study. The mean age of the sample was 35.1 years and approximately 61% were male. The sample was almost exclusively White non-Hispanic, with only 9.6% of respondents reporting any other race or ethnicity.
Measurement
Millon Clinical Multiaxial Inventory (MCMI-III)
Mental health and substance use characteristics of the sample were assessed using the MCMI-III (Millon, Millon, Davis, & Grossman, 2009). This instrument that has been utilized frequently in the psychological assessment of drug users (Calsyn, Wells, Fleming, & Saxon, 2000; Teplin, O’Connell, Daiter, & Varenbut, 2004). It is a self-report questionnaire containing 175-items in 28 scales, with demonstrated psychometric properties (Craig & Olson, 2001; Millon, 1997). Fourteen of the scales measure personality disorder traits, while 10 measure clinical syndromes. The remaining four scales measure validity and response style. For the purposes of the current study, scales for anxiety, PTSD, major depressive, bipolar, dysthymia, somatoform, thought, delusional, and alcohol and drug disorders were used. In addition, for personality disorder analyses, the scales for the nine personality disorders contained in the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013; paranoid, schizoid, schizotypal, antisocial, borderline, histrionic, narcissistic, avoidant, and depressive) were used.
To enhance maximum diagnostic efficiency of the MCMI-III, the developers employed base rate transformations score for raw score conversion to account for the prevalence rate (Gibertini, Branderberg, & Retzlaff, 1986). Base rate scores under 75 indicate that there are few or no traits or symptoms indicating a diagnosable mental disorder. Scores between 75 and 85 suggest that there are traits and symptoms of mental disorder present, but that they do not reach clinical levels. Scores over 85 indicate that the individual has all of the traits and symptoms for diagnosable mental disorder.
Family grief questionnaire
Appendix A presents the questions asked in the Family Grief Questionnaire. The three questions asked on this one-page questionnaire were developed by the researchers specifically for this study. The questionnaire asked participants to indicate by checking a box whether any member of their family had died young, had died at a time that was particularly difficult for the survivors, or had died in a traumatic way. Possible family members included the nuclear family (parents and siblings), and the older generation family grandparents (maternal and paternal) and great grandparents. The older generation category was included because of the literature discussed earlier concerning the intergenerational transmission of trauma and its possible connection with addiction in the current generation. Other family members and pets were also included in each of the death categories.
Data Analysis
Utilizing SPSS statistical software, frequency analyses were conducted to determine how many PUTs had been experienced by individuals in the sample in each of the death categories. Because of the detailed nature of the questions asked in the Family Death Questionnaire (see Appendix A), the number of deaths in many of the categories was either zero or very low and so several of the variables were merged to create new variables. For example, the two parent variables (mother and father) for all three types of death were combined into one variable (PAR). Computing a single parent variable alowed us to compare our results with other studies that have examined parental death. Because there were very few deaths among siblings, the two sibling variables (sister and brother) were combined with the single other family member variable and the single pet variable for each type of death into one variable (OTH). Finally, the four grandparent variables (maternal and paternal categories) and the two great grandparent variables (including great grandmother and great grandfather) in each of the types of death were combined into a single variable (GRAND) allowing us to explore the possibility of intergenerational transmission of problems associated with a death in those earlier generations.
Bivariate correlation analyses were then conducted with all of the MCMI-III mental health disorder profiles and the PAR, GRAND, and OTH variables to determine if there were any significant relationships between them. The PAR, GRAND, and OTH variables were dichotomized into No Death (0) versus Death (1) categories and means of the significantly correlated mental health variables were compared using independent samples t-test analyses.
Results
Frequencies
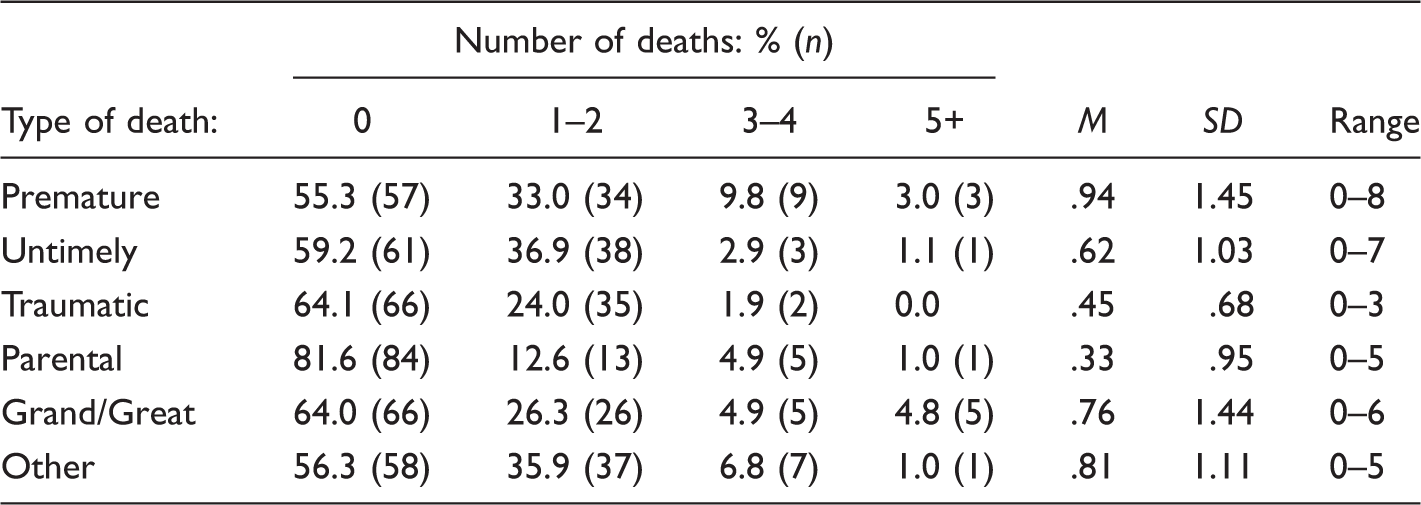
Percentages and Frequencies of Premature, Untimely, and Traumatic Death and These Deaths Among the Three Family Groupings (n = 103).
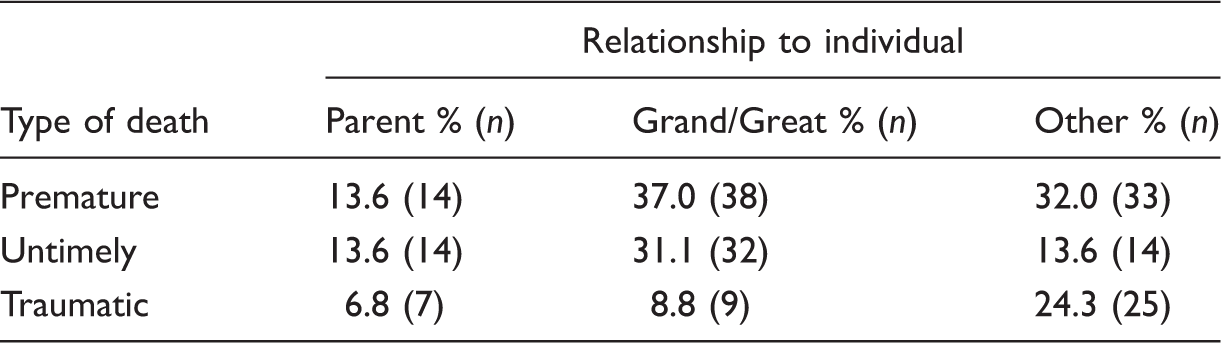
Percentages and Frequencies of Premature, Untimely, and Traumatic Death Among Respondents’ Relationship With the Deceased (n = 103).
Bivariate correlations
None of mental health disorder profiles was significantly related to either the death of the parents or others. However, among the GRAND was significantly correlated with anxiety (r = .2323, p < .05), somatoform (r = .203, p < .05), bipolar (r = .253, p < .01), PTSD (r = .253, p < .01), thought (r = .270, p < .01), MDD (r = .270, p < .01), and delusional (r = .204, p < .05). Among the personality disorder profiles, GRAND was significantly correlated with avoidant (r = .238, p < .05), dependent (r = .315, p < .01), schizotypal, (r = .272, p < .01), borderline (r = .203, p < .05), and paranoid (r = .248, p < .05).
Independent samples t tests
Results of Independent Samples t Tests comparing the Means of Respondents With Death Versus No Death in Their Grandparents’ Generation for Significantly Correlated Mental Health Disorders.
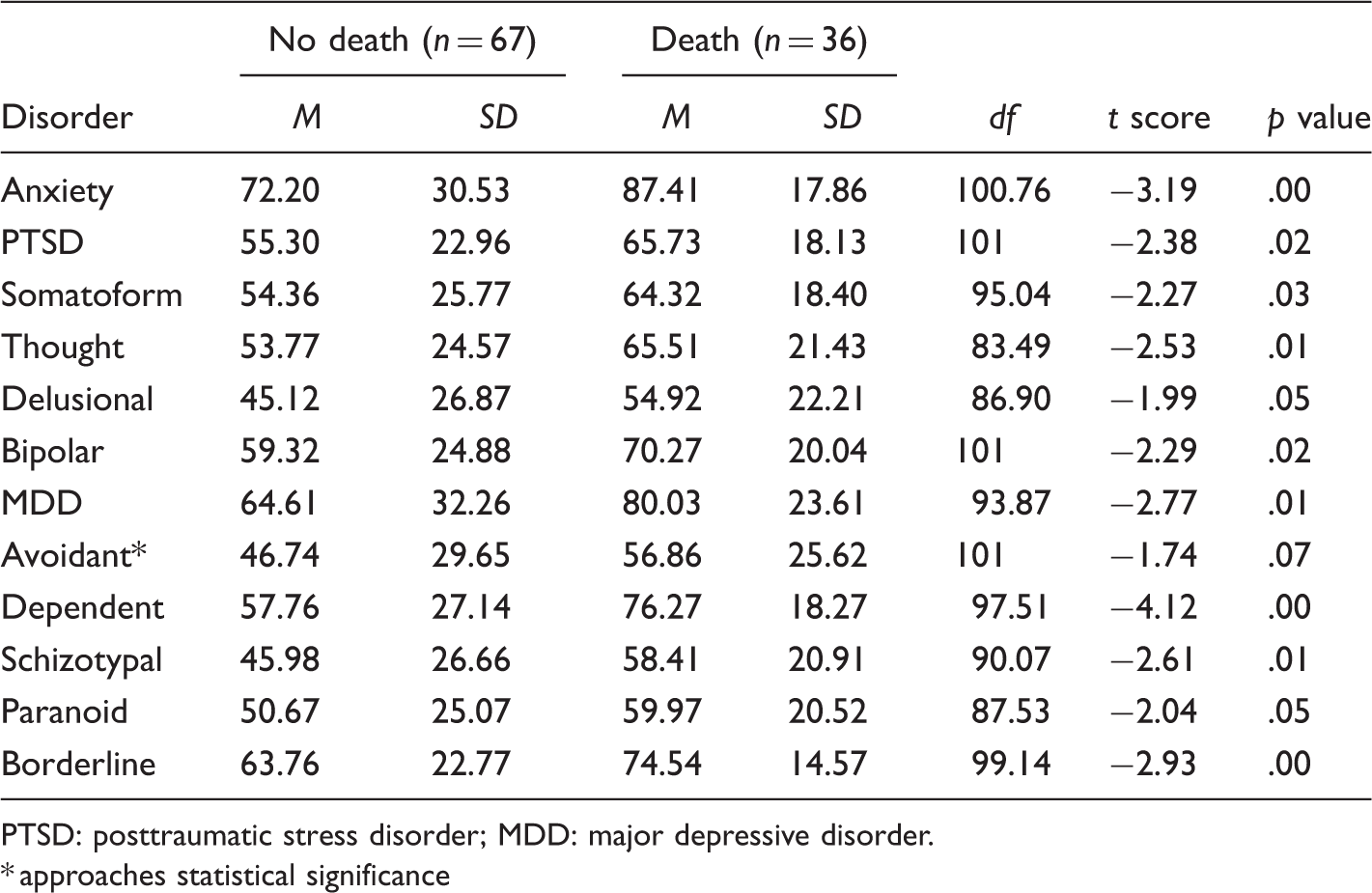
PTSD: posttraumatic stress disorder; MDD: major depressive disorder. * approaches statistical significance
Discussion
There is a considerable body of research that has explored the relationships between death of family members and substance use issues, much of which has focused on parental death to the exclusion of other important family members (Bowlby, 1961, 1980; Clarkin, Lenzenweger, Yeomans, Levy, & Kernberg, 2013; Nickerson et al., 2013). In addition, the studies examining relationships between family death and mental health disorders currently in the literature do not explore this issue among individuals with comorbid substance abuse issues (Jacobs & Bovasso, 2009; Kunugi et al., 1995; LaPorte & Guttman, 1996; Liotti et al., 2000; Miyabayashi & Yasuda, 2007; Reich, 1986; Tyrka et al., 2008; Zisook et al., 1994). The purpose of this study, therefore, was to determine to what extent individuals in treatment for SUD issues had experienced the PUT of family members (including members of the nuclear family, pets, grand- and great grandparents, and other family members). In addition, we explored possible relationships between the death of family members and the presence of traits and symptoms associated with multiple mental health disorders. This is the first study to examine PUT of family members, as it is related to comorbid traits associated with mental health disorders among individuals with substance use issues.
Our results showed that these types of death were relatively common among our inpatient sample, with about two thirds of our respondents reporting between one and eight of these losses. Interestingly, the most commonly experienced death was the premature death of a grandparent or great grandparent, with 37% of clients reporting this loss in their family. The second highest percentage was again among the untimely death of grandparents and great grandparents, with about 31% of clients reporting this experience. In addition, almost 32% reported the premature death of a sibling, some other family member, or a pet and 24% reported a traumatic death in this group.
Our bivariate analyses provided some surprising results. Research has shown significant relationships between parental death and anxiety (Nickerson et al., 2013), depressive symptoms (Jacobs & Bovasso, 2009; Nickerson et al., 2013; Kunugi et al., 1995; Tyrka et al., 2008), and borderline personality disorder (LaPorte & Guttman, 1996; Liotti et al., 2000). In addition, it has been suggested that the death of a sibling (Crehan, 2004) or of a pet (Cordaro, 2012) could also have harmful mental health effects. However, our results indicated that neither the death of a parent nor the death of a sibling, pet, or other family member was significantly related to any mental health symptomatology.
In contrast, the death of a grand- or great grandparent was significantly positively correlated with symptom levels of seven mental health disorders, (anxiety, PTSD, somatoform, thought, delusional, bipolar and MDD), in addition to five personality disorder profiles (avoidant, dependent, schizotypal, paranoid, and borderline). Between-group means were significantly higher in the Death group for all of the mental health symptoms except avoidant (which approached significance). These results are congruent with Coleman et al.’s (1986) research in which she found higher rates of death among the grandfathers of individuals with heroin dependency (on methadone maintenance) compared with college students (with no history of substance use or mental health disorders) and to individuals with a diagnosis of neurosis or personality disorder (in outpatient treatment).
This finding concerning grand- or great grandparents is particularly interesting, as it may suggest that disturbances caused by their PUT could be transmitted down the generations to their children's children and grandchildren. Possible mechanisms for the intergenerational transmission of family disturbances that contribute to these disorders could be either direct or indirect. An example of direct transmission would be when a grandparent died and the grandchild then coped with the death by using substances. Alternatively, disturbance could come down the generations through Gajdos’ (2002) idea of a “cascade of anxiety” (p. 306) that could affect the grandchild indirectly through their parent's dysfunctional communication patterns related to complicated grief. Furthermore, Walsh and McGoldrick (2004) have suggested that families who experience the loss of a loved one must not only grieve the loss but reorganize their family structures to accommodate it. Perhaps, the families of individuals who present in treatment with mental health symptoms such as those reported in our sample have had a particularly difficult time processing their grief and reorganizing their structure, with consequent anxiety, depression, somatic complaint, and dysfunction in both thinking and personality among their descendants. Research has clearly shown that there is a high probability that insecure attachment styles, such as those caused by the inadequate parenting suggested by Nickerson et al. (2013), could be passed down to later generations (Verhage et al., 2015). Since a high proportion of clients in treatment for SUD report insecure attachment styles (Horton, Diaz, Weiner, & Malloy, 2012), it is possible that some of that insecurity has been passed down because of dysfunction associated with the grand- and great grandparents’ death.
Clinical Implications
Our results suggest that the intergenerational transmission of dysfunction after the death of a grand-or great grandparent may be an issue underlying numerous mental health disorder symptoms that are common among individuals in treatment for SUDs. Consideration must, therefore, be given to possible interventions at the micro, mezzo, and macro levels. At the micro level, it may be important to conduct a thorough assessment of the death of family members and an exploration of how the client's substance use problems may be related to these losses and possible traumas. For example, determining if the death had a direct effect on the development of addiction and comorbid psychopathology (i.e., if the individual's method of coping with the death by using substances became his or her habitual way of coping with adversity or painful feelings), treatment planning could target the development of new coping mechanisms. Discussion of emotions and behaviors related to loss could be the emphasis of individual therapy sessions. In addition, since dysfunction due to deaths of individuals in the far past may travel down the generations as attachment problems, it seems extremely important to address any attachment issues exhibited by clients not only to help them overcome their addictions but also to prevent further transmission of attachment problems to their children and grandchildren.
At the mezzo level, if it was determined that the death affected the development of the individual's mental health issues indirectly through his or her parents’ unresolved grief or dysfunctional communication patterns, family therapy could perhaps become a focus of treatment. Coleman (1978) has described individuals with drug dependency issues whose families have suffered a PUT death as having enmeshment, blurred generational boundaries, and “terror” (p. 81) concerning separation from or loss of a family member. Coleman reports that these individuals often have intensely intimate and overly dependent relationships with one parent (usually the mother) who, because she is terrified she will be rejected by and will lose her child, will not discipline her child and will enable his or her drug use. In these cases, then, individual family members could be referred to therapy for their own unresolved grief or attachment-related issues with an aim toward reducing their enabling behaviors.
At the macro levels, it is important that health care, law enforcement, and social service agencies gain an understanding of the possible intergenerational effects of PUT and develop programs to help surviving family members. For example, it might be helpful for hospitals to institute policies and procedures that address the possibility of mental health issues that target the family members who have lost someone to these kinds of death. Police officers could be trained to provide information on available community services and resources to the survivors when they respond to an event in which one of these kinds of death has occurred. Social service organizations could link with hospitals and law enforcement agencies to identify families at risk of problematic grief responses and offer in-home or community-based bereavement groups and concrete support for those family members having difficulty coping with these deaths.
Limitations and Future Research
This study is the first to explore possible relationships between three specific kinds of death (PUT) across multiple generations among a sample of individuals attending inpatient SUD treatment. Because of its exploratory and cross-sectional nature, no causation can be established. In addition, the Family Grief Questionnaire was a self-report instrument constructed by the researchers asking about a large number of possible relationships in which the three types of deaths could have occurred. Including a large number of family members in the questionnaire and having a sample of size of 104 individuals forced us to combine several of the relationship categories (i.e., other family members were combined with pets) in order to have an adequate number that allowed us to conduct statistical analyses. However, since we did obtain results that have statistical significance from this sample, we feel that future researchers may want to consider replicating this study with a larger sample.
The use of a self-report instrument also did not allow for the researchers to obtain information directly from earlier generations and instead relied on the respondents’ memory and knowledge of family deaths. Future studies should be designed to gather information from earlier generations if at all possible and to conduct face-to-face interviews to gather qualitative data concerning the effects of deaths of family members on family functioning and survivor parenting capabilities. It is also important that future studies assess what kinds of family dysfunction related to death, especially those deaths occurring in the grand- and great grandparent generations, are present in this population and how these issues might best be treated in a clinical setting. Since our study suggested the possibility of attachment issues coming down the generations, future research might also include an attachment instrument for the client being treated as well as for his or her parents when possible.
There are also limitations to generalizability related to the lack of racial diversity in our sample. That is, our sample was almost exclusively White non-Hispanic, and results could differ if other racial or ethnic groups experience death in different ways. In addition, the agency in which data were gathered was a private, for-profit agency that tends to attract relatively high SES clients with access to insurance further limiting the generalizability of the study findings.
Conclusion
Research has shown that the PUT of a family member is related to later substance use issues among some surviving family members (Bowser et al., 2003; Coleman, 1978; Coleman et al., 1986; Ellinwood et al., 1966; Nickerson et al., 2013). However, research on these deaths has been limited in that no studies to date have explored associations between these deaths and other mental health disorders co-occurring with substance use. Therefore, this study examined the relationships between PUTs of family members (parents, grand- and great grandparents, other family members, and pets) and comorbid psychopathology among a convenience sample of 104 individuals attending treatment for substance use issues. Results indicated that these kinds of death were commonly found within the families of the respondents. In addition, it showed that these deaths were significantly correlated with higher levels of comorbid anxiety, mood, and personality disorder symptoms. Of particular interest was the finding that these symptoms were significantly correlated with death among respondents’ grand- and great grandparents rather than among their nuclear families. Further research is needed to assess what kinds of family dysfunction correlated with death may be present in this population and what kinds of interventions may be effective in treating them.
Footnotes
Appendix A
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.