
Abstract
Telephone counseling is an inexpensive method of providing counseling and crisis intervention in response to some of the mental health needs of the community. It can be provided at a counseling center or other unit with the purpose of providing mental health counseling for callers. The aim of this study was to investigate types of problems and interventions for callers at a telephone counseling service in Tehran, Iran. The data were collected using the records of 82 callers to the Telephone Counseling Center of the School of Behavioral Sciences and Mental Health-Tehran Institute of Psychiatry, affiliated with Iran University of Medical Sciences. The mean the number of calls made by callers was 1.53. The most common problems presented were marital and family conflicts (28.4%), mood disorders (24.3%), interpersonal and communication problems (17%), and behavioral problems of children (15.8%). Counselors offered psychosocial/educational advice (36.5%), recommendations for taking medications (26.8%), recommendations for in-person/individual counseling or family counseling (25.6%), and behavior therapy techniques (17%). Recommendations are made for the evaluation, structure, and process of telephone counseling services and for training telephone counselors in Iran.
Introduction
Using the telephone as a treatment modality and as a medium for crisis intervention has long been a major tactic for helping people in crisis and who are contemplating suicide. There has been a global growth of telephone counseling services and an increasing number of calls to these services, which is a clear indication of the importance and necessity of such services (Lester & Rogers, 2012). Telephone counseling was first used by suicide prevention services and crisis intervention in the 1960s as a way of proving immediate and cost-effective access to crisis intervention for those who are experiencing distress. Since then, the telephone has been used for a variety of services, such as teen hotlines for young people, those trying to quit smoking, and those addicted to drugs and alcohol (Lester, 1973, 1977a, 1977b, 1995, 2002; Lester & Brockopp, 1973).
Active listening is a key element in telephone counseling practice, combined with short-term crisis intervention (assessing resources and identifying solutions) focused on specific problems. The therapeutic alliance between the caller and the telephone counselor plays a major role in telephone crisis counseling. The early process in telephone crisis counseling requires empathy, warmth, and genuineness on the part of the counselor (Gould, Kalafat, Harrismunfakh, & Kleinman, 2007; Kalafat, Gould, Munfakh, & Kleinman, 2007; Ludman, Simon, Tutty, & Von Korff, 2007). The skills of the telephone counsellor, the characteristics of the caller, and the unique features of telephone counseling (such as caller anonymity and greater power for the caller, e.g., in terminating the contact) all impact on the effectiveness and outcomes of telephone counseling (Young, 2009).
Lester (1995) has listed several advantages of telephone counseling (see also Aguilera, Ramos, Sistiva, & Wang, 2018; Babac et al., 2018; Barnett & Scheetz, 2003; Downes, Mervin, Byrnes, & Scuffham, 2017; Grigorash et al., 2018; Lester & Rogers, 2012; Sundram, Corattur, Dong, & Zhong, 2018). First, the client does not have to travel to a specialized clinic, and this is especially important for people living in rural and sparsely populated regions. Telephone counseling permits the clients to remain anonymous, which can facilitate self-disclosure and openness. The counselor can also remain anonymous. Telephone counseling also gives the client more power. If they feel uncomfortable, it is much easier to end a telephone call than to stand up and walk out of a counselor’s office. Telephone counseling may be a good choice for people who have busy schedules, prefer the comfort of their home to a therapist’s office, and who are unable to leave home or travel (such as the disabled) but need to talk to a counselor (Dadfar & Lester, 2017). However, there are disadvantages. As the telephone is generally used for conversation, counselors have to avoid falling into a conversational mode with clients but remain focused on crisis intervention. In addition, some clients become too dependent on the service and become chronic callers.
The use of telephone counseling in primary care and also for health promotion behaviors of different types of clients or patients has been reported (e.g., Bombardier et al., 2008; Cava et al., 1999; Hunt et al., 2018; Levy et al., 2017; Lins et al., 2014; Lynch, Tamburrino, & Nagel, 1997; Pirkis et al., 2016; Simon, Ludman, Tutty, Operskalski, & Von Korff, 2004; Simon, Vankoff, Rutter, & Wagner, 2000; Stead, Hartmann-Boyce, Perera, & Lancaster, 2013; Tutty, Simon, & Ludman, 2000; Watzke et al., 2017). Applications of the telephone for behavioral health include crisis counseling, initial contact information, basic education about the problems facing callers, informing callers about available services, screening, appointment scheduling, assessment, counseling, support between face-to-face counseling sessions, case management, supervision, follow-up, and evaluation (Selvik & Stephenson, 2004). The telephone has also been used to check on attempted suicides after their release from the hospital and to monitor and motivate patients who are engaged in therapeutic tasks for their particular problems.
The Federal Occupational Health guidelines for counseling by telephone include assessing client appropriateness, conducting the initial assessment, documenting the counseling, evaluating the service, and counselor licensing. The Federal Occupational Health evaluation components for telephone counseling include the number of telephone cases, the length of counseling sessions, the rates of case assignment to affiliated counselors, client satisfaction ratings on access to care, client satisfaction ratings on the services received, outcomes ratings on productivity and absenteeism or the counselors, clinical outcomes, structured counselor feedback on their telephone cases, and anecdotal case information from counselors (Selvik & Stephenson, 2004).
In telephone counselling, the interaction between the counselor and the client is a complex, dynamic, and decision-making process (Bobevski & McLennan, 1998). Supervision plays an important role in the growth and development of counsellors and in the education of counsellors to help them understand and manage their interactions with clients (Kim, 1998; McNamara & Gillies, 2003; Sternitzke, Nixon, & Ponterotto, 1988).
Many telephone counseling lines have been provided by organizations and institutions in Iran, including Counselor’s Voice by State Welfare Organization of Iran in Tehran in 1992, increasing the number of lines and opening of telephone counseling in other centers of provinces of Iran in 1993, calls for counseling in education in 1997, direct communication line for children and adolescents in 1999, a telephone line for the Association for the Protection of Children’s Rights in 2000, assignment of 3-digit line of 148 for Counselor’s Voice throughout the country in 2001, a counseling police line support line in 2002, telephone counseling at the Tehran University in 2005, a 10-digit line of smart telecommunication for licensed persons from the Psychology and Counseling Organization of Iran in 2007, and the opening of the Telephone Counseling Center of the School of Behavioral Sciences and Mental Health-Tehran Institute of Psychiatry, which is affiliated with Iran University of Medical Sciences in 2015.
The Counseling Office in the office of the Cultural and Prevention Affairs vice-chancellor, which is affiliated with State Welfare Organization of Iran, monitors telephone counseling centers in Iran. There is a wide area network and a local area network. The data obtained from these centers in most of the provinces of Iran indicate that, despite cultural issues in the Iranian society, individuals have welcomed the opportunity to discuss their problems using the telephone, especially because of the anonymity involved. To organize and standardize the operation of telephone counseling centers, the Counseling Office has developed regulations for telephone counseling centers regarding counseling principles, cultural issues, and the specific features of telephone counseling. Supervision of telephone counseling centers is carried out in accordance with these regulations. Telephone counselors are licensed counselors or psychologists. An expert staff is responsible for the executive and supervisory activities of governmental and nongovernmental telephone counseling centers. Observers provide guidance when needed for telephone counselors regarding medical interventions and the use of appropriate counseling and psychological techniques as well as difficulties arising in particular cases. Telephone counseling is available in two shifts, day and night, anywhere in Iran. The telephone counseling process is monitored by a supervisor. The process of telephone counseling has seven stages: rapport, investigating the problem, clarification, finding appropriate solutions, applying the solution, termination, and follow-up after call. Telephone counseling does not provide long-term counseling for chronic disorders and problems but rather provides short-term guidance and advice or referral for specific cases to in-person counseling centers. The consultation time is limited to 30 minutes. Calls are assigned a code, and the counselor’s code is attached to the record of the call (Firouzi, 2007; Ghasemzadeh, 2007; Rezvanpour, 2001, 2007; State Welfare Organization of Iran, Prevention Development Center, 2011).
In a systematic review of crisis interventions in online psychological counseling, da Silva, Siegmund, and Bredemeier (2015) found three main issues: response to disasters, prevention of suicide, and trauma. In Iran, the usefulness of telephone counselling has been reported for the family caregivers of these breast cancer patients (Nasiriani, Motevasselian, Farnia, Shiryazdi, & Khodayarian, 2017), the quality of life in patients with coronary artery bypass graft (Bikmoradi, Masmouei, Ghomeisi, Roshanaei, & Masiello, 2017), the quality of life of patients with colostomies (Parchami Iraqi & Ahmadi, 2016), the perceived stress of caregivers of patients with Alzheimer’s disease (Bastani, Hosseini, & Javanbakhtian, 2012), quitting smoking (Heydari et al., 2011), and women’s quality of life postpartum (Khakbazan, Golyan Tehrani, Payghambardoost, & Kazemnejad, 2010).
Dehghani, Bolhari, Yaghubi, and Peyravi (2009) reported a high level of satisfaction in callers to the Tehran University telephone counseling service. For example, 76% scored the ease of contact as high, 92% scored whether the counselor listened well as high, 65% scored whether the counselor understood their problem as high, 88% felt comfortable talking to the counselor, 90% felt that the counselor was trying to help them, 39% said that they found a solution to their problems, 40% felt calmed down, and 82% felt satisfied overall with the telephone counseling. Clearly, follow-up with a sample of clients is needed to ascertain reasons for the lack of success with some clients.
The aim of this study was to investigate the types of calls and problems presented by callers to a telephone counseling service in Tehran, Iran.
Method
This was a descriptive cross-sectional study. The data were collected using the records of 82 callers to the Telephone Counseling Center of the School of Behavioral Sciences and Mental Health-Tehran Institute of Psychiatry, which is affiliated with Iran University of Medical Sciences. There were five counselors working in the Telephone Counseling Center. Their mean age was 44.8 years (standard deviation [SD] 23.9); 4 were female, 3 were married, and 4 had an MSc degree in clinical psychology.
The Center provides psychological and counseling services in the following areas: depression, anxiety, obsessive-compulsive disorders, suicide prevention, crisis intervention, sexual abuse, adolescent problems, couples’ communication problems, parenting, marriage counseling, divorce counseling, childhood hyperactivity, and addiction. The service is available through a designated telephone number on Saturday to Wednesday from 8.30 a.m. to 2 p.m. The Center is staffed by clinical psychologists.
Public information including announcements and posters are provided through the public relations section on the website (http://tip.iums.ac.ir) of the school. The Center does not rely only on the website, and staff at other organizations and institutes can refer people to the center. The data were analyzed using descriptive statistics, Pearson’s correlation coefficient, and tests of statistical significance (t tests) using SPSS version 24.
Results
The mean age of callers was 34.0 years (SD = 14.0). The modal caller was married (42.7%), had a high school education and a higher degree (34.1%), and was a housewife (26.8%). The mean number of calls made by callers (and, therefore, counseling sessions) was 1.53 (SD = 2.06; see Table 1).
Descriptive Data From 82 Callers.
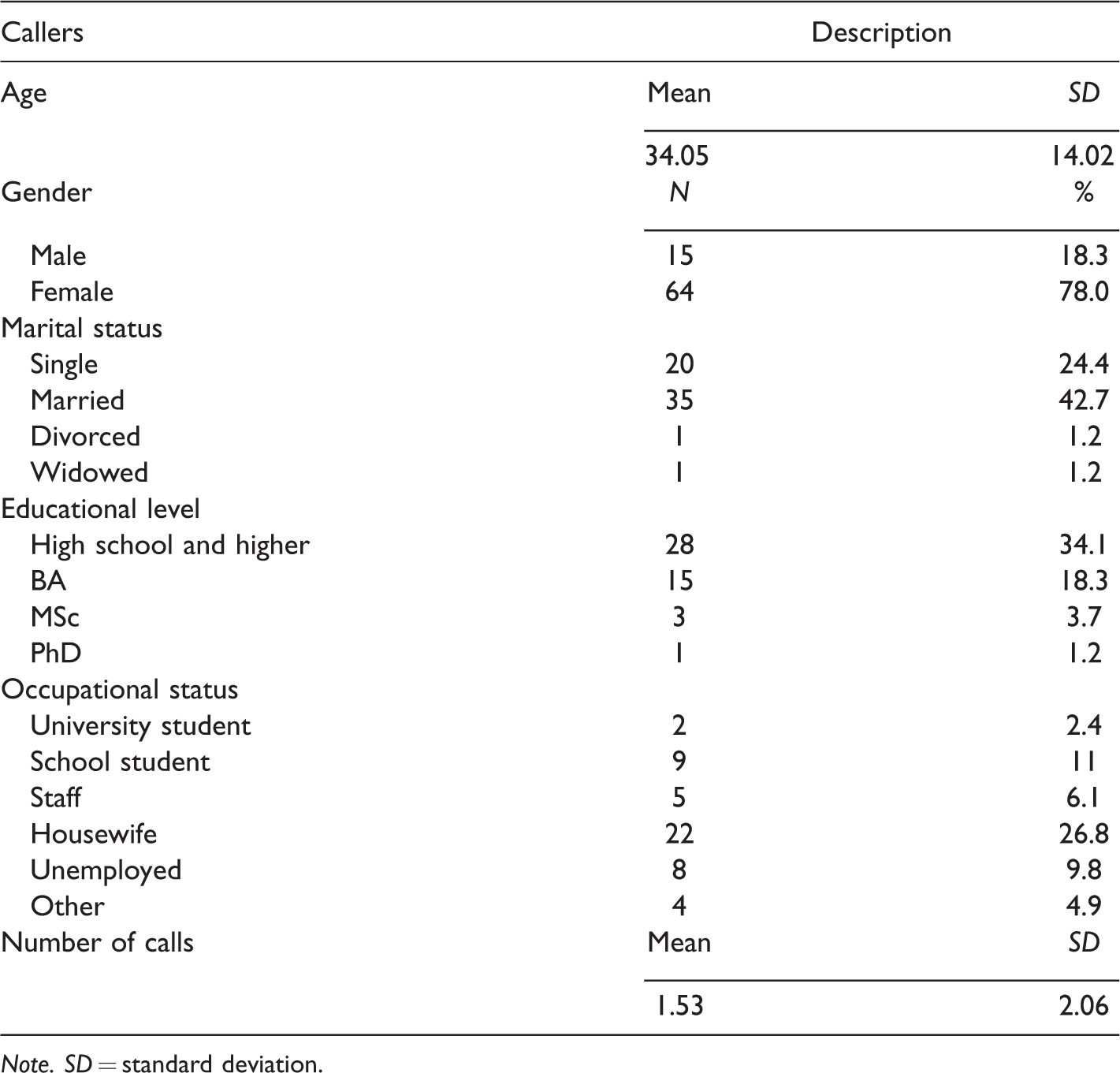
Note. SD = standard deviation.
The most common problems presented by the callers were marital and family conflicts (28.4%), mood disorders (24.3%), interpersonal and communication problems (17%), and behavioral problems of children (15.8%), respectively (see Table 2).
Problems of Callers (N = 82).

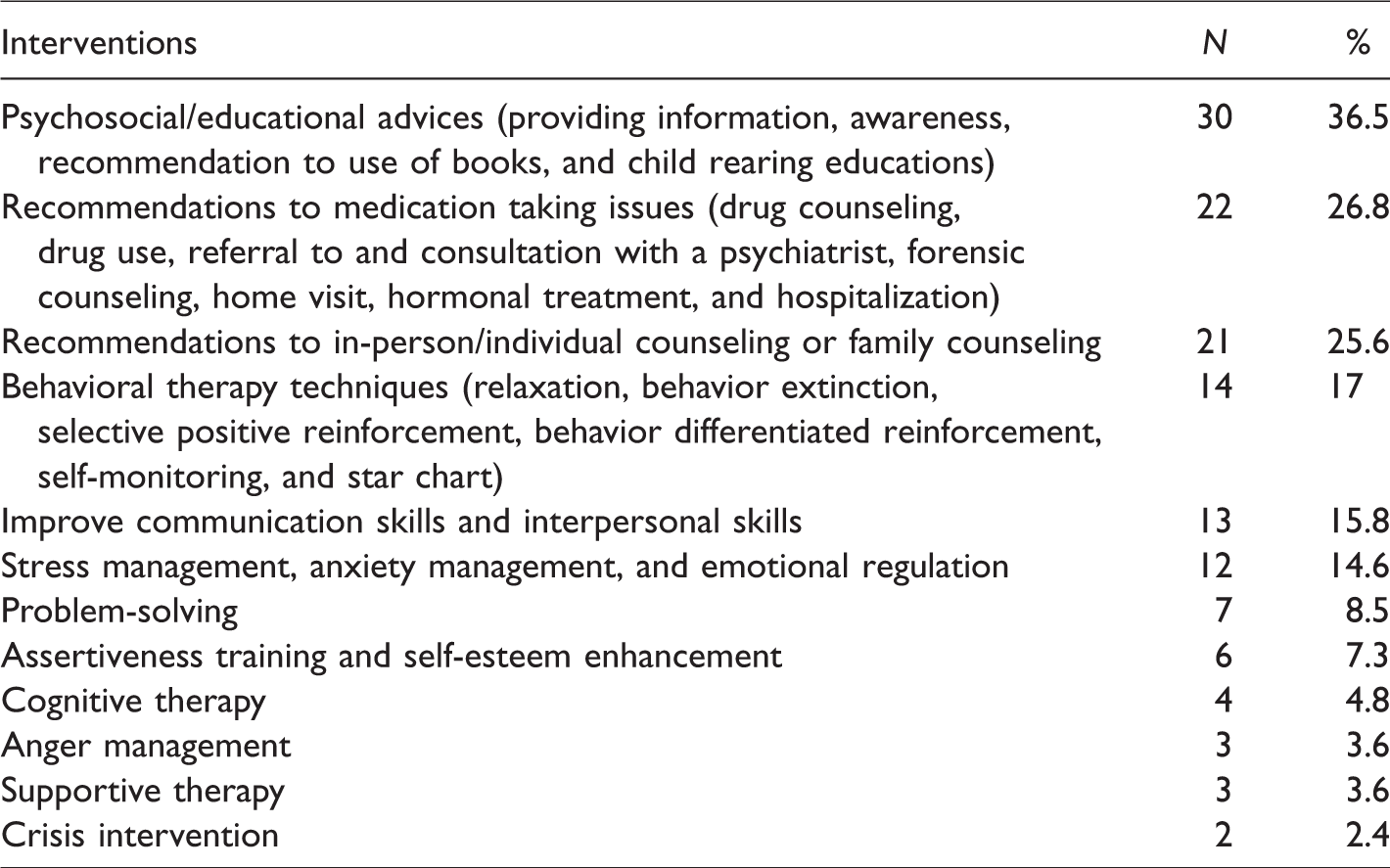
The most common interventions for callers were psychosocial/educational advice (36.5%), recommendations for issues with taking medication (26.8%), recommendations for in-person/individual counseling or family counseling (25.6%), and behavior therapy tactics (17%). Crisis intervention was required for two callers (2.4%; Table 3).
Interventions for Callers (N = 82).
There was no significant relationship between age and number of calls. There was a significant difference by sex for the number of calls. Male callers had a higher mean number of calls than female callers (Table 4).
Differences by Age and by Sex in the Number of Calls.
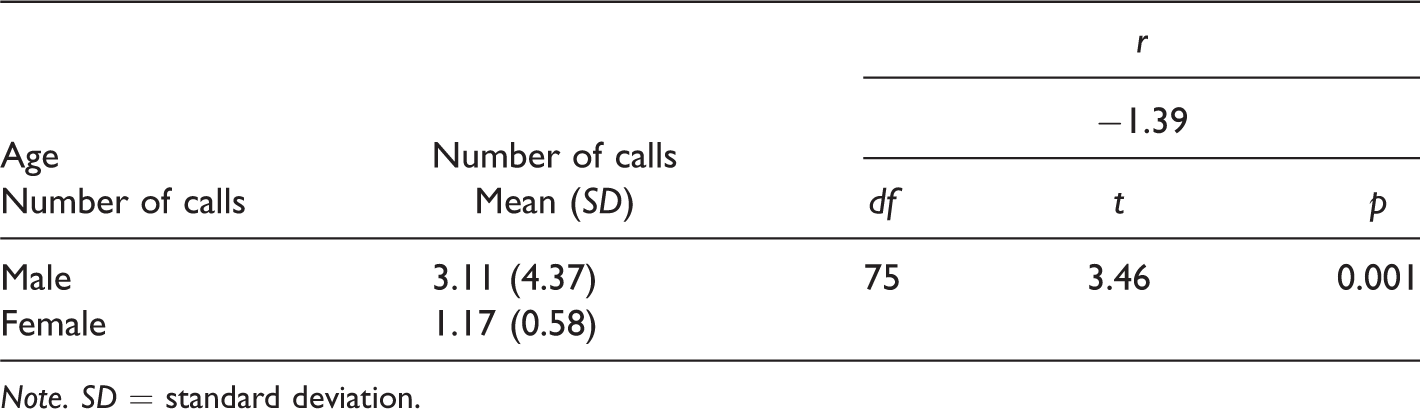
Note. SD = standard deviation.
Discussion
The mean number of calls made by clients to the telephone counseling service was 1.53, and the service does not seem to have created chronic callers. Most clients were helped with just one call. Ludman et al. (2007) reported that approximately 80% of their callers with depression completed eight or more sessions in telephone therapy group sessions.
Brockopp et al. (2002, cited in Lester, 2002) found that callers to their center were more often females, a feature found in our call center in Iran. Burgess, Christensen, Leach, Farrer, and Griffiths (2008) reported that the modal clinical profile of their callers was anxiety and depression, while Bassilios, Harris, Middleton, Gunn, and Pirkis (2015) found that callers had a higher risk of suicide and more often used other mental health services than noncallers.
Spittal et al. (2015; Middleton, Gunn, Bassilios, & Pirkis, 2016) found that predictors of repeat calls were being male or transgender, never having been married, but also suicidality, self-harm, and mental health problems. Pirkis et al. (2016) reported that frequent callers were more often isolated, in crisis, had major mental and physical health problems, and also used other services for their mental health issues. Middleton, Woodward, Gunn, Bassilios, and Pirkis (2017) found that frequent callers were more likely to call regularly to talk about their feelings than were other callers, while Bassilios et al. (2015) found that patients with anxiety disorders more often made repeat calls.
Initially, the counselors in Iran did not have experience with telephone counseling, and they may not have provided service with the same attention to quality and excellence as they would in face-to-face counseling. For example, it was unlikely that a counselor could help a caller in anger management or stress management in one session. It would seem that telephone counselors should be provided with training in what they can and cannot achieve in the course of one or two telephone calls. It may be that, for many problems, the telephone counselor should serve as a referral agent, knowing what resources exist in the community and helping callers make appointments with those services, as well as checking that the callers did go for treatment. It is possible for telephone counseling services to arrange with community services to give priority to clients that the telephone service refers to the service.
Telephone counseling should be staffed by trained and qualified counselors. The service offers two-way anonymity, which means that the identities of both counselor and caller can remain anonymous. The effectiveness of the counseling process depends on the trust that develops between the counselor and the caller. Any information about the caller must remain completely confidential, except when there is a risk of harm to themselves or to others.
For their employee assistance program (EAP), Selvik and Stephenson (2004) suggested that there were two areas (criteria and outcomes) for evaluating telephone counseling, and they also suggested using a multifaceted evaluation model. In a telephone counseling service, attention should be paid to whether the callers attracted to the service are appropriate clients and whether the counseling technique is appropriate for those callers. For their EAP, client satisfaction dimensions included service satisfaction (accessibility and convenience), productivity improvement (improved productivity at work, and improved work relationships), and client improvement (EAP’s effect on problem resolution, strengthening the client’s job effectiveness, and ability to cope with stress).
The counseling process entails an in-depth conversation between the client and a counselor who will take his or her time to fully understand the caller’s concern. Callers must be assured of continued support and care throughout the process. There should be no restrictions on the duration of calls or the number of times that a caller reaches out to the counselors for help. During the process, suggestions or assignments of tasks may be made in an effort to enable the caller to move toward a solution. The tasks may involve activities to help with introspection, reflection, prioritization, or goal setting, with the intention of moving toward achieving the identified goals. As the sessions progress, the counselors should keep a detailed account of how callers are progressing and make plans for future sessions. Once the desired goal is achieved, the process of counseling may end for the time being. However, it may be resumed at any point depending on caller’s need (Barnett & Scheetz, 2003; Car & Sheikh, 2003; Haas, Benedict, & Kobos, 1996; Mons et al., 2013; Dadfar, Seraji, & Dadfar, 2010; Reese, Conoley, & Brossart, 2002, 2006).
Telephone therapy can be useful for certain types of clients who prefer this modality for talking to a counselor and for many clients during their therapy when they need to talk to someone between formal face-to-face counseling sessions. Treatment by telephone has unique features that may be helpful and useful in improving the clients’ treatment such as the anonymity permitted and the immediacy of contact with a counselor. Therefore, therapists should consider how the telephone may be incorporated, as a regular and planned outreach program for some clients (Lester & Rogers, 2012).
Although, Dehghani et al. (2017) developed and validated a Supervision Scale in phone consultation in Iran with two therapeutic alliance and intervention dimensions for this scale, we recommend that telephone counseling services use a Technical Effectiveness Scale to measure the counselor’s performance after the call, including: (a) Can the caller be immediately re contacted? (b) Did the counselor ask for or obtain specific information regarding significant others? (c) Were specific problems identified? (d) Did the counselor communicate that he or she was willing to help? (e) Did the counselor develop a structured plan of action or help the caller develop one? (f) Did the caller agree to the action plan? (g) Was it determined whether or not this was a possible suicidal person? (h) If so, did the counselor ask about a suicide plan and previous suicidal behavior? The nature of telephone counseling with many anonymous callers prevents evaluating these services by asking clients their opinion of the counseling that they received.
To investigate the nature of telephone consultation, analysis of the actual dialogue should be made. The sequence of questions, and answers, demands/requests, and responses or evaluations are examples of these social actions in the approach of conversational analysis. In addition, the level of empathy of the counselors can be assessed, and this level can be related to the client’s satisfaction with the telephone contact.
Conclusions
Evaluating the effectiveness of telephone counseling is essential in many areas: quantity (the number of people who have used the telephone counseling service), quality (are there changes in the users’ mental state and behavior), and economic (is the service cost effective). Supervision of the telephone counselors is crucial as well as providing them with effective support systems. It is hoped that this study will stimulate further interest and discussion of the telephone as a mode of treatment and will prove useful for those setting up and operating telephone counseling services in Iran and for those training and supervising those on the front lines, the crisis interveners, and counselors.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.