
Abstract
Chronic health conditions are often accompanied by depression and a decrease in quality of life. This greatly complicates treatment and affects treatment outcomes. Thus, the purpose of this study was to analyze previously published stories of 10 survivors of chronic diseases and depression, using content analysis, to answer the following question: What can be learned from the experiences of the storytellers bereaved by the burden of chronic health conditions? A trajectory with four phases emerged from the analysis of theses survivors’ stories: (1) First Impressions, (2) Turning Point, (3) Resiliency … Limitation as an Opportunity, and (4) Paying It Forward. The explored trajectory represented the different stages of personalized experiences with chronic health conditions from initial diagnosis to completion of treatment. Persons diagnosed with chronic health conditions and co-occurring depression find happiness, joy, and freedom if they have adequate support systems, practice creatively unloading their trials, and make time for the opportunity to assist and be of service to others in similar situations. Implications of this study include that the trajectory identified will be a useful guide for professionals and paraprofessionals including those in health care and mental health care, as well as volunteers, friends, and family in working with persons who have co-occurring depression and chronic diseases.
Introduction
Researchers have found that among the top 10 leading causes of death in the United States, eight are health conditions including heart disease, cancer, strokes, and diabetes (Nichols, 2017). Chronic health conditions, although not leading killers, are found to be just as challenging for those diagnosed, including multiple sclerosis (MS), sickle cell disease (SCD), celiac disease (CD), and HIV/AIDS. For those with chronic health conditions, they disproportionately experience, and are at-risk for, depression (Adam et al., 2017; Feinstein, 2011; Gonzalez, Batchelder, Psaros, & Safren, 2011; Katon, 2011; Olver & Hopwood, 2013) as well as a decrease in overall quality of life (QOL; Rocha, Schuch, & Fleck, 2014).
Depressive symptoms and depression affect persons with chronic health conditions (e.g., MS, SCD, CD, and HIV/AIDS; National Institute of Mental Health [NIMH], 2018) at a much higher rate than those without. Depression causes complications for persons with chronic health conditions (Cheung & Sundram, 2017; NIMH, 2018; Walker et al., 2012). A few of these consequences and challenges include: adhering to a medical treatment plan, eating and sleeping, fatigue, decreased cognition, and feelings of worthlessness. These are worsened given depression that most often causes sadness, hopelessness, and decreased interest in activities (American Psychological Association, 2015).
Health-care providers, equipped to treat the presenting chronic health condition, may not be best to treat the accompanying or emerging depression experienced by the individual (Croghan & Brown, 2010). This lack of understanding and skill set in treating this depression can cause additional stress for the patient seeking hope, stability, and balance when facing these conditions. Moreover, the individuals’ QOL is greatly compromised due to various characteristics of the chronic health conditions, complications from the co-occurring depression, and side effects of the treatments associated with these chronic health issues (Colleoni et al., 2000; Walker et al., 2014).
The number of persons experiencing depression co-occurring with various health conditions is significant. To best understand the extent and gravity of the problem, here we present prevalence of depression co-occurring with various chronic health conditions. Depression among persons with heart disease has a prevalence of 31% to 45% (Huffman, Celano, Beach, Motiwala, & Januzzi, 2013). Next, cancer, which is the second leading cause of death, has varying depression prevalence depending on treatment phase, from “5% to 16% in outpatients, 4% to 14% in inpatients, 4% to 11% in mixed outpatient and inpatient samples and 7% to 49% in palliative care” (Walker et al., 2012, p. 898). Persons with diabetes are twice as likely to have depression as those in the general population (Moulton, Pickup, & Ismail, 2015). About 24% of those with MS (Marrie et al., 2015), 18% to 44% of people with SCD (Tartt, Appel, Mann-Jiles, Demonbreun, & John, 2015), 39% of those with CD (van Hees, Van der Does, & Giltay, 2013), and 19% to 43% of those with HIV/AIDS experience depression (Watkins & Treisman, 2015). In sum, these statistics highlight the presence of depression among persons with chronic health conditions.
This depression, or symptoms of depression, results in poorer physical health outcomes (e.g. Gonzalez et al., 2008; Huffman et al., 2013; NIMH, 2018; Tartt et al., 2015; Walker et al., 2012; Watkins & Treisman, 2015). Extant literature reports that long-term, people with chronic health conditions experience disease aspects that are persistent and depressing and contribute to hopelessness, decreased QOL, and reduced resiliency (e.g., Duggleby et al., 2012; Schattner, Shahar, & Abu-Shakra, 2008; Vann-Ward, Morse, & Charmaz, 2017). Duggleby et al. (2012), in a metasynthesis of qualitative literature, found that the concept of hope and suffering differs for older adults with chronic health conditions, as compared with younger adults with chronic health conditions. In another study, Megari (2013) found that disease symptoms permeate every aspect of life and have a great effect on QOL. Even more so, chronic health conditions were found to have a negative, debilitating impact on the person’s overall sense of self (Falvo & Holland, 2018). As persons affected with such chronic health conditions may construe chronic health conditions as a protagonist, they may allow these to control their behavior and affective states (Schattner et al., 2008).
To counteract this sense of hopelessness, decreased QOL, and symptoms of depression, resiliency building may be especially helpful for persons with chronic health conditions. Helping persons to develop and maintain an overall sense of hope is especially important to help individuals experiencing chronic health conditions (Duggleby et al., 2012). Resilience building especially can be used as an effective model to enable patients with chronic health conditions to protect their well-being from poor or adverse outcomes (Behel, Shamaskin, Guequierre, Emery, & Rybarczyk, 2012; Trivedi, Bosworth, & Jackson, 2011). A resilience framework can play an important role in exploring patients’ antecedents, such as personality traits, coping styles, and social support (Edward, 2013). Finding the individualized active or adaptable coping style and ability to elicit social support is essential to help persons with chronic health conditions to develop and maintain an overall sense of hope (Duggleby et al., 2012; Luyckx et al., 2008).
Given these patterns of co-occurring depression and chronic health conditions and resulting impact on outcomes, understanding how people successfully manage these co-occurring diagnoses from their own perspectives is important to guide treatment. Resources to address hope may be both internal and external, which means it is important for individuals across the lifespan to find meaning and identify strategies to help deal with chronic health conditions (Duggleby et al., 2012). The purpose of this study was to add to the emergent literature by analyzing already published, naturally occurring, stories of 10 survivors of chronic health conditions to answer the following question: What can be learned from the experiences of the storytellers bereaved by burden of chronic health conditions?
Method
Ten published stories from the chapter of the book The i'Mpossible Project (Volume 1 Reengaging with Life, Creating a New You; Rivedal, 2016) are used in this study.
Protection of Human Subjects
The stories analyzed are in the public domain and part of a published book series, The i'Mpossible Project. Those who agreed to tell their stories knew these accounts would be in the public domain. The first author consulted with her institution’s institutional review board for Human Subjects Protections; the institutional review board indicated that the project does not count as Research as the data are in the public domain.
Reflexivity: The Inspiration for The i'Mpossible Project
Key to the credibility of a qualitative research study is reflexivity: “A researcher’s background and position will affect what they choose to investigate, the angle of investigation, the methods judged most adequate for this purpose, the findings considered most appropriate, and the framing and communication of conclusions” (Malterud, 2001, pp. 483–484). Thus, for this study, it was important for the fourth author, who collected the data, to divulge his background and position.
Fourth author
Throughout my teenage years and into my mid-20s, life did not just give me lemons—it practically pelted them at me. Suicides, mental illness, frequent breakups, fights with family members, ignorant and bad decisions, and a lack of income and job opportunities were all commonplace. All around me I saw lemons but instead of seeing the possibility that I could make lemonade or even a few lemon popsicles I got angry, shut down, and the universe became all about me and a vendetta against god for forgetting to pass out a few strawberries and plums with all the lemons being thrown my way. It was only after experiencing a crisis at age of 27 years and learning about empathy and reframing that I was able to see that (a) the universe does not revolve around me or what I did or did not get and (b) that all those lemons could be made into lemonade that can be shared with others to keep them cool, hydrated, and healthy.
For over 6 years, I have been making lemonade—helping others through storytelling, seminars, and curriculum on mental health and suicide—but several years ago I wanted to learn how other people made lemonade. I needed to find new recipes and share them with the world. And so … I founded The i'Mpossible Project as a way to connect with lemonade amateurs and masters from around the world. In 2015 and in 2017, The i'Mpossible Project released two volumes of 50 true, short stories (Rivedal, 2016). The former included a diversity of topics, and the subjects of this study are derived from this edition.
Selecting Contributors for The i'Mpossible Project
Selecting contributors for this first volume of The i'Mpossible Project included inviting people through social media, at public speaking events, and asking friends, acquaintances, and colleagues if they would write a story (or invite someone else to write a story) of how they found hope in the face of an adverse event or experience of their choice. The stories in this book are powerful, inspirational, and proof that “impossible” is nothing more than a mindset, but so is possible—even in the face of harrowing odds.
Guidelines for the contributors in The i'Mpossible Project
Artistic work from professionals and amateurs alike cannot be presented with too many rules and restrictions or the creative process becomes burdensome and the finished product feels disjointed and inauthentic. The guidelines were that the piece had to (a) be 1,000 words or less; (b) be about the respective contributor; (c) be free of foul language and promotion of one’s own agenda (e.g., one’s career, religion); and (d) include what was learned, how the contributor’s life was changed, and what the reader can take away.
Data Analysis
The i'Mpossible Project's section on health has a total of 10 stories about chronic disease survivors’ experiences. The cofirst authors (two authors) read all the stories for a project in their qualitative research class and the following research question emerged from these 10 stories: What can be learned from the experiences of the storytellers with chronic health conditions? Both authors read all of the stories coded these using qualitative content analysis (Schreier, 2012), beginning with open coding (Elo & Kyngas, 2008). The authors coded independently in Atlas.ti using systematic steps with low-inference descriptors, which aim to record observations and include, “verbatim accounts of what people say … rather than researchers’ reconstructions of the general sense of what a person said” (Seale, 1999, p. 148), to increase the analytic rigor and explore the textual interpretation of the data. Examples of such low-inference descriptors included direct quotes such as, “The wound is the place where the Light enters you” and “A wrong turn in life isn’t always a bad thing.” Storytellers’ words verbatim were used to increase trustworthiness and avoid biased interpretation (Moustakas, 1994; Patton, 2002).
To increase credibility, the cofirst authors and second author met 6 times to discuss various interpretations of the coding process, review the emerging codes and phases, and capture the essence. Comparison, discussion, and selection of additional consensus made the coding and analysis process reflective. This reflective process enhanced interpretive and descriptive validity through the triangulation of investigators and sources and reliability through intercoder agreement (Creswell, 2007). The emerged phases of trajectory are the product of the collaborative coding and analysis of the data.
Results
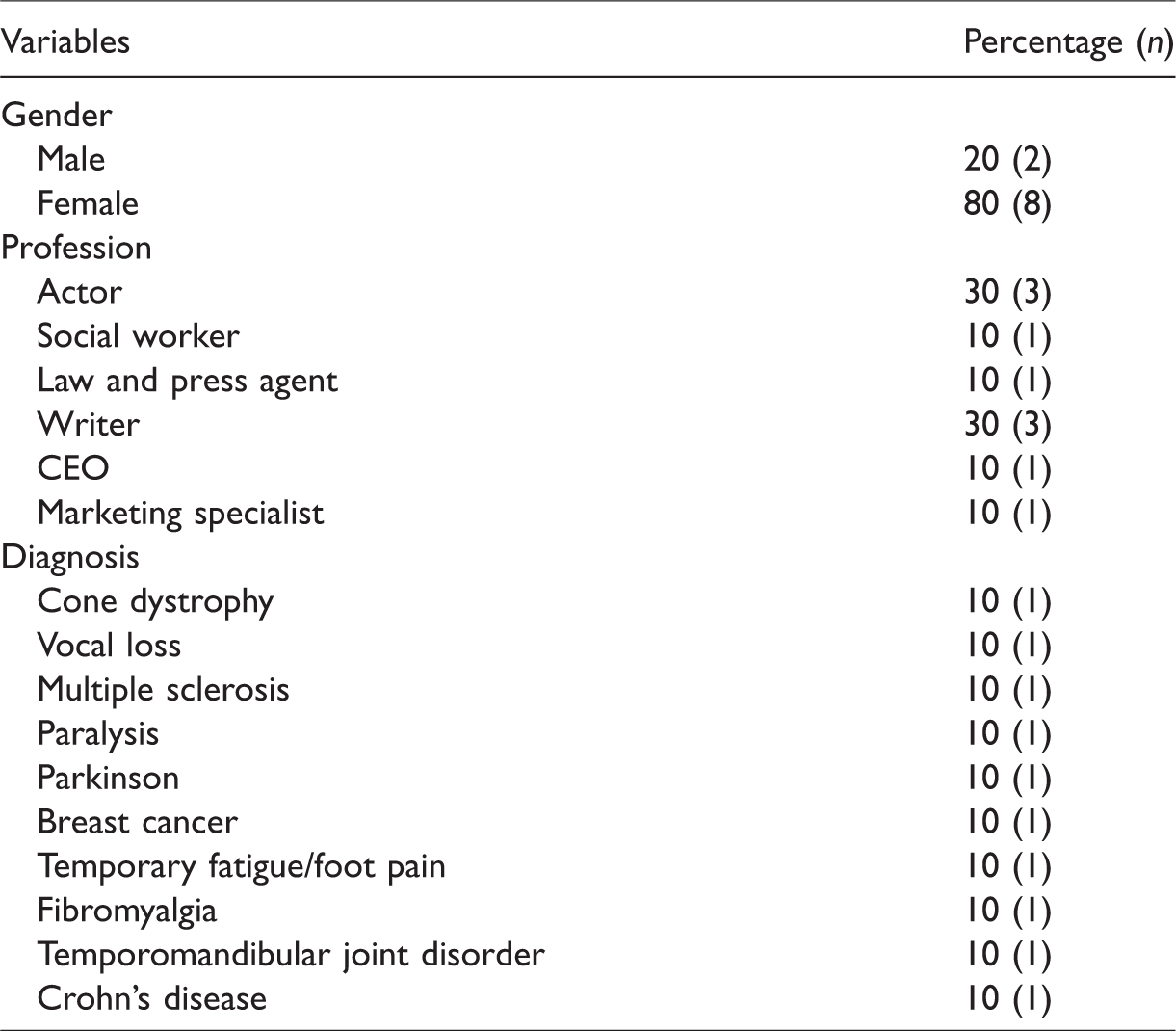
The sample of 10 storytellers was contributed by a majority of females (n = 8, 80%). Of professions, 30% of the storytellers were actors and writers. Each storyteller was diagnosed with differing conditions, for example, Cone Dystrophy, Cancer, and Fibromyalgia (Table 1).
Demographics.
Analysis of the storytellers’ accounts resulted in several phases and subphases of the trajectory of facing their respective chronic health conditions. Phases and subphases are (a) First Impressions: Identity crisis and Despair; (b) Turning Point: Self-realization, Support of family and friends, and Creative activity; (c) Resiliency … Limitation as an Opportunity; and (d) Paying It Forward.
Phase 1: First Impressions
Identity crisis
Each of the stories touch on the individual’s first impression after receiving a diagnosis or experiencing a symptom related to their disease. Among the first impressions are storytellers’ identity crises in which a symptom or the entire disease threatens their abilities to maintain their identities. One storyteller, Ms. N, who lost her voice stated, Though alarming—as I had never experienced this before in my entire career as an actor, singer, and teacher—I assumed after a day or two of rest, all would be well. Days later, when I was still unable to speak, I began to panic. (Rivedal, 2016, p. 37)
Despair
Another first impression experienced by storytellers was a sense of despair. Patients, generally, experienced an overall sense of hopelessness and distress following the initial identity crisis. Ms. MG, one storyteller, discussed challenges accepting, “I was in denial, depressed and hopeless. I started believing that I was a mistake in this world. I wanted to overcome my disability, but in truth, this wasn’t about overcoming a disease or mental illness” (Rivedal, 2016, p. 42). Similarly, Ms. M with MS stated, For the next few years, I slowly fell into a deep abyss of misery. I was emotionally, spiritually, mentally, physically, and financially vacant. One November evening in 2009, as I sat on my kitchen floor in my nighty, I decided I couldn’t live the way I was living. (Rivedal, 2016, p. 47)
Phase 2: Turning Point
From the first phase, each storyteller experienced a turning point in their story. This turning point changed the trajectory of their thought process as it related to their disease and physical health challenges. Spiritual mechanisms became a tool for many storytellers. For one storyteller, Ms. N came across spirituality and developed a belief in the greater good, stating, There is a beautiful quote from Rumi I recently stumbled across while I was sitting at home, starring at the walls, feeling sad and lost and sorry for myself: “The wound is the place where the Light enters you.” It’s amazing to me how life seems to hand us lessons on a silver platter, if only we are willing to slow down and be present to them—or in my case, when we are forced to. (Rivedal, 2016, p. 38)
Self-realization
Self-realization was a consequential phase for all storytellers. Their abilities, talents, and jobs were impacted by their lack of self-confidence. Following a diagnosis and then working through the initial crisis of identity and feelings of despair, storytellers have described coming out on the other side, realizing that their self-value is not based on their diagnosis. Rather they have realized that the physical challenges can be reduced with mental strength, self-confidence, and self-love. For example, Ms. N who is an actor expressed, It may seem dramatic that, less than a week after losing my voice, I would be sobbing uncontrollably at 3 a.m., scared, alone, and full of anxiety. But this breakdown was also my breakthrough. It really had nothing to do with my voice at all; it had to do with my self-value. It had to do with love. (Rivedal, 2016, p. 38) It takes trust to know that diving into the pain will allow the feeling of freedom to surface on the other side. From my own experience, I can say that each time I dove headfirst into feeling the pain that I faced, I came out on the other side more confident than ever … (Rivedal, 2016, p. 51)
Support of family and friends
Out of 10 storytellers, more than half of them acknowledged their family support. They have narrated how blessed and wealthy they were only for their family support. A male actor with Parkinson’s disease, Mr. J, described his family’s and friends’ support beautifully. He noted, “Love. I am blessed to have a wealth of great friends and a wonderful family. They are there for me whenever I need them” (Rivedal, 2016, p. 56). He also demonstrated a confident attitude about his wife’s support: “I’ll climb every hill and descend every valley, holding Charlene’s steady hand. Hopefully, I won’t become too big a burden to her. But I know that through it all, she will love me and I will love her” (Rivedal, 2016, p. 56). A female storyteller, Ms. MG, who had Cone Dystrophy mentioned that family, friends, and professionals are her great support system. She also mentioned “Help can come in many different forms, including simply talking about what I’m going through, writing, exercising, listening to music, meditating, traveling, and spending time with my dog, family, and friends” (Rivedal, 2016, p. 43). Similarly, a female blogger, Ms. H, who had breast cancer stated how supportive her fiancé and stepson were. She was informed about cancer when she was planning her wedding. Ms. H stated In those nine months between “Will you marry me?” and “I do,” I lost part of my breast to surgery and all of my hair to treatment. I was sick from chemo, I came into early menopause, and I developed a case of the walking farts. Nothing says “beautiful and sexy fiancée” like a sweaty, bald, lopsided woman with the walking farts. And yet, Carter and Stepson never left my side. (Rivedal, 2016, p. 58) When I was approached by Answers.com to write articles for their new Fatigue category, my first thought was that I couldn’t do it. No way! However, when I told my husband about the offer, he pushed me to give it a try. I did, and I loved it. (Rivedal, 2016, p. 67)
Creative activity
Different creative mechanisms were applied by most of the female storytellers to transform their physical pain and emotional stress into power. Their creative activity facilitated them to move through their struggle and be empowered. A storyteller who was paralyzed described how writing and singing help her to express her emotion and control her anger: “Finding a creative outlet allows you to not have to be solely reliant on another person and helps you move through your struggle. I have found that writing or putting on music and singing loudly helps me express myself” (Rivedal, 2016, p. 50). Ms. H described how she became a bestselling author applying her writing skill: “I started blogging as a way to communicate with friends and family during and after cancer treatment. I quickly learned how much I loved writing” (Rivedal, 2016, p. 59). Similarly, Ms. J’s story also provided evidence that writing helped her not only to handle her illness, but also it created an opportunity to share the information about fibromyalgia with others. She stated, Back in 2010—when I knew I had fibromyalgia, but before I had been formally diagnosed—I began a blog detailing my journey. The idea had been to share the information I found as I found it. I was new to this illness and I knew others were, as well. They might be less likely to engage in the kind of research that I was open to doing. The blog was a way for me to both document what I found and share it with others. Over the years, my activity levels varied with the blog, but it was always there. When I began to feel better, I also began to blog a lot more. (Rivedal, 2016, p. 67) I am actively involved in the Power of Pain Foundation, which helps low-income and underinsured patients with neuropathy pain. Through my advocacy work, I have had the pleasure of meeting thousands of patients and family members from around the country and online. Sharing my story and hearing their stories is what it’s all about. From the human connection and community we create, I get my drive to advocate for myself and others. (Rivedal, 2016, p. 71)
Phase 3: Resiliency … Limitation as an Opportunity
All of the storytellers expressed that their vulnerability and limitations inspired them to be powerful and courageous. They had gone through such adverse circumstances that made them resilient to face versatile challenges. At the beginning, although one storyteller, Ms. MG, felt “denial, depressed, and hopeless” (Rivedal, 2016, p. 42) because of ocular disorder, gradually she discovered that conquering fear and accepting the reality is everything in life. These skills of resiliency encouraged her to hike the mountain of physical challenge and enjoy a more buoyant spirit over time. Ms. MG described: Falling down and messing up has been a wonderful life lesson for me because it helps me to conquer my fears, and this has led me to become more resilient over time. I know things can be rough, but the trick to a better life is learning to be a good dancer. Life is all about rhythm and beat. You just have to learn how to dance to the different types of melodies. As I like to say, live life courageously. (Rivedal, 2016, p. 43) When I first heard my diagnosis, all those years ago, I would have never imagined my life to be as purposeful and fulfilling as it is today, and I definitely wouldn’t have thought colitis would be the reason for it all. (Rivedal, 2016, p. 76). Cancer hijacked my engagement, my wedding, and my life. At the time, it was easy to get swallowed by the “woe is me” feelings. But now, looking back at that year, I know that it was the biggest blessing I could have ever asked for. (Rivedal, 2016, p. 59) Chronic pain took my life away for several years, but it gave me something I never knew I had: a passion to write, and more importantly, a passion to help people through my writing. Chronic pain gave me a new life, as well as a new understanding of life, and a new appreciation for the small things and for the people in it. I would not be the person I am today if not for the pain I’ve learned to live with. (Rivedal, 2016, p. 67)
Phase 4: Paying It Forward
For all participants, a central tenant to overcoming the negative effects from the diagnosis of their chronic health condition, to acceptance, was paying it forward. Giving back to the community and supporting others, particularly those who have been affected by a similar diagnosis, has been a facet of the storytellers’ journeys. One participant, Ms. E, shared that this powerful experience has undoubtedly been the encouragement necessary to share her knowledge and resources to those with the same diagnosis, breast cancer. Ms. E mentioned that “The biggest blessing has been the lives I’ve been able to touch through all of my outreach—and not just my fellow breast cancer survivors, but all women” (Rivedal, 2016, p. 60). She also shared that her experience provided opportunities to support other cancer patients particularly through connection, advocacy, and awareness. Ms. E reported, The Coconut Head’s Survival Guide has become a forum for me to share home and family inspiration while still focusing on breast cancer advocacy and awareness. Some may brag about being a best-selling author, but after writing three books on cancer—including one for children—I can brag that I am a breast-selling author! (Rivedal, 2016, p. 59)
Discussion
People facing chronic health conditions are likely to develop depression and often struggle with maintaining their prediagnosis QOL (Rocha et al., 2014). Although treatment of the chronic health condition is primary, leaving the possible depression and other emotional consequences of chronic health conditions untreated is detrimental to the overall healing process as evidenced by research supporting that those with co-occurring chronic health conditions and depression have worse outcomes than those who have only the chronic health conditions. Thus, it is important to learn what those who thrive in the wake of chronic health conditions have done outside of treatment of the condition to move forward.
To do so, we analyzed stories from people who are thriving despite their diagnoses with chronic health conditions such as breast cancer, MS, and paralysis. Their stories highlight several key themes. First, initial diagnosis is met with identity crisis and despair. The identity crisis is strongly tied to the impact the change in their bodies has on their identities related to careers and personal relationships. These identity crises seem to be the gateway to the feelings of despair that are ultimately soothed at a turning point in their lives by a combination of supportive friends and family and creative activities. These creative activities such as writing paved the way along the journey for these storytellers to live life more resiliently and ultimately strive toward helping others in similar situations. In conclusion, as healers work with those facing chronic health conditions, not only should the usual activities be undertaken—for example, treatment of physical symptoms, medication for depression, engaging of support systems in treatment planning—but also there should be efforts to help those who are affected with chronic health conditions to move through reshaping their identities, creatively unloading their trials (e.g., through writing or other creative outlets), and focusing on helping others in similar situations.
Conclusion and Implications for Practice
This study highlights patterns of coping through co-occurring depression and chronic health conditions. Moreover, this study analyzes the lived experiences of persons facing various chronic health conditions and how they found hope amid diagnosis and treatment. The preceding quotations, which describe the lived experiences of persons facing chronic health conditions, demonstrate the effectiveness of both the power of community and the use of creative outlets to harness strength and hope. Every individual underwent four phases of development. Through these phases, from diagnosis to eventually sharing their story and help others, each individual’s outlook on life greatly transformed from a state of hopelessness and despair to an enthusiasm for life and passion for helping others. Although previous research has focused on how people cope with chronic health conditions diagnosis and treatment, a limitation of many of the studies is that the very act of inviting the participants to the study and consenting them creates the possibility of biases such as the researcher’s phrasing of the questions and social desirability. With this study, the storytellers wrote their stories for a collection aimed at helping others. The research came after the publication of the book, and thus the storytellers were free to express themselves without the focus on what they might have thought the researcher wanted (e.g., social desirability, guiding questions).
These findings may help professionals and paraprofessionals in health-care and other settings when working with people living with chronic health conditions. In using these lived experiences, practitioners, clinicians, friends, and family can share such stories with individuals affected with similar physical diagnoses and chronic physical diseases. The professional can involve the client in creative writing or other forms of creative expression to express feelings associated with a diagnosis. Similarly, health and mental health-care professionals can work with persons affected with a chronic health conditions to achieve their best QOL through treatment of any physical symptoms, engagement in support systems, in addition to working with others.
Every individual affected by a diagnosis of chronic health conditions and mental illness has a unique story to tell. Overall, it is important for health-care professionals to have an expansive range of resources and treatment options for persons affected with both chronic health conditions and mental illness. Through an established support system, storytelling, creative writing, and working with others, persons diagnosed with chronic health conditions and co-occurring depression can find happiness, joy, and freedom.
Footnotes
Authors’ Note
Vivian J. Miller, PhD, LMSW, is now affiliated with Bowling Green State University, OH, USA.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Correction (February 2024):
Article updated online to correct the issue publication year from 2021 to 2022. See https://doi.org/10.1177/10541373241230139
Author Biographies
![]()