
Abstract
For understanding the role of culture in coping in different cultural settings, we have conducted studies among cancer patients in 10 countries, within the framework of an international study on meaning-making coping. This article reports on part of the results we obtained from a study in Portugal; specifically, the reported findings are restricted to nonreligious/spiritual coping methods, methods we call secular existential meaning-making coping. The main aim is to identify the diversity of coping methods using a cultural lens. Thirty-one participants with various kinds of cancer were interviewed. Six different kinds of coping methods related to secular existential coping emerged from thematic analyses of the interviews: discourse of the self, positive solitude, nature, positive transformational orientation, body–mind relationship, and working. Findings revealed that these six methods facilitated patients’ psychological adaptation to the oncological disease. The findings suggest the importance of considering cultural and social context when exploring coping strategies among cancer patients.
Cancer presents a considerable challenge to the individual’s psychological balance and may cause discontinuity in how people relate to themselves and to the world. Psychological adaptation involves the development of cognitive–emotional approaches to regulating and giving meaning to the emotional experience of facing cancer. There are significant differences in the ways in which patients adapt to the disease, and these differences are related to sociodemographic, disease-related, and psychosocial factors (Brandão, Schulz, & Matos, 2017). Cultural factors can also influence assessment of the stressor event, how people react to the situation, and the coping strategies used (Kayser et al., 2014; Kuo, 2011). Marsella and Yamada (2000) defined culture as: Shared learned meanings and behaviors that are transmitted from within a social activity context for purposes of promoting individual/societal adjustment, growth, and development. Culture has both external (i.e., artifacts, roles, activity contexts, institutions) and internal (i.e., values, beliefs, attitudes, activity contexts, patterns of consciousness, personality styles, epistemology) representations. (p. 4)
The main aim of this study is to identify the diverse meaning-making coping methods cancer patients in Portugal use and to discuss these methods from a cultural perspective. The results presented here are restricted to secular existential coping methods. We have discussed the findings on religious and spiritual coping methods in another article (Ahmadi, Matos,Tavares,Tomás and Ahmadi (2018)). Moreover, given the important role of family and personal relationships in Portuguese society, the meaning-making coping related to these relationships will be discussed separately in another paper.
Meaning-Making
Meaning-making is described as “an important self-regulatory process within the individual, and a process of mutual regulation in relationships” (Davis, 2015, p. 431). There is no clear definition of an individual’s sense of meaning in life and meaning-making processes are not easily recognized (Park, 2010; Schnell, 2009). The current definitions are based on ambiguous and simple models that fail to take into account the complexity of the construct 'meaning of life' (Martela & Steger, 2016). Despite the problem of exactly defining meaning-making, according to a psychological approach, there is some consensus on the importance of coherence, purpose, and significance (Lloyd, 2018).
Reker and Wong (2012) added that, to achieve an enduring sense of personal meaning, there is a need to integrate meaning-filled daily experiences (i.e., situational meaning) with a larger, higher purpose (i.e., global meaning). A sense of belonging, significance, and meaning in the everyday life of individuals is achieved not in a vacuum but in an enhanced and broader context. Therefore, we expect the cultural environment to influence the meaning-making coping methods used by cancer patients (Banerjee et al., 2011). When patients with cancer are able to attribute a positive global meaning to life and their cancer experience, they typically display better psychological adjustment (e.g., better quality of life; Lee, Cohen, Edgar, Laizner, & Gagnon, 2006a, 2006b; Vickberg et al., 2001). During the process of meaning-making, while people are faced with a stressor event, they may attribute new meanings to the situation through problem-solving and positive reassessment (Ching, Martinson, & Wong, 2012; Skaggs & Barron, 2006).
Secular Existential Meaning-Making Coping
In many studies in the field of coping, the terms religious and spiritual have been used to address meaning-making coping methods that are essentially based on existential issues. Nevertheless, a number of studies (Ahmadi, 2006; Ahmadi & Ahmadi, 2015; Ahmadi, 2018; Ahmadi, Ahmadi, Erbil, & Cetrez, 2016) have demonstrated use of other coping strategies that cannot reasonably be regarded as religious or spiritual. Coping strategies of this kind can be defined as existential in nature, which refers to a search for meaning that is not connected in any way to religion or religious symbols or that has no clear connection to a sacred religious/spiritual source. Here, we use the term existential coping because these strategies concern individuals’ efforts to locate an inwardly source—in themselves, others or the world—that can assist them in coping with their problems. Their problems have created an existential vacuum that requires the old order be elaborated into a new order—a new order that can help them fill this vacuum. Figure 1, taken from Ahmadi & Ahmadi (2018), shows the relation between religious, spiritual, and secular existential coping as it appears in our project.
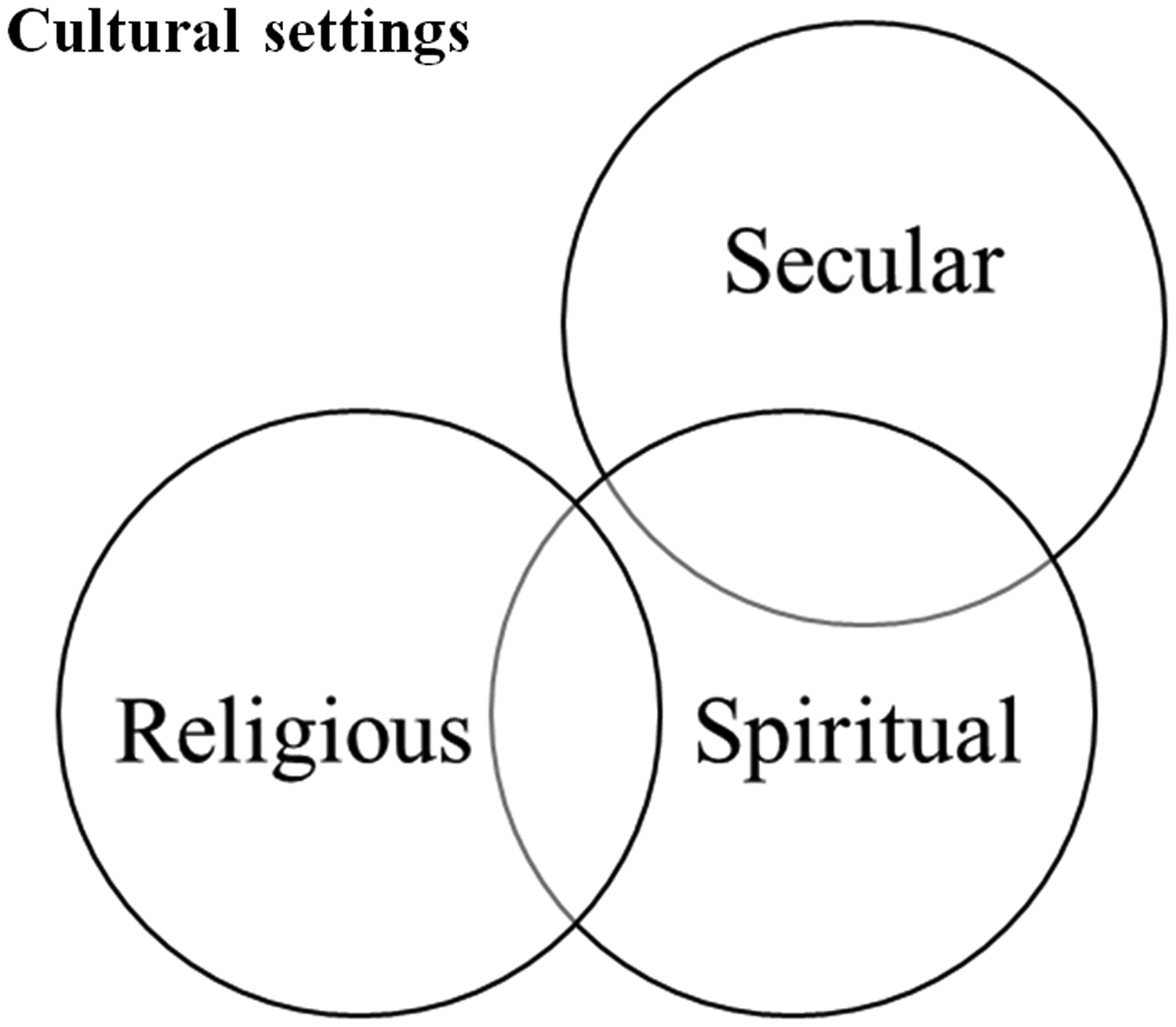
Relation of existential meaning-making domains (Anonymous & Anonymous, 2018).
According to this model (see Figure 1), the concepts and topics that are part of the religious and spiritual domains overlap to some extent. The concepts and topics of spiritual and secular meaning-making coping also show some overlap, but note the lack of overlap between secular and religious concepts and topics (Ahmadi & Ahmadi, 2018, p. 136). This occurs because our definition of religion is “a search for significance that unfolds within a traditional sacred context” (Ahmadi, 2006, p. 72). Moreover, we define spirituality as “a search for connectedness with a sacred source that is related or not related to God or any religious holy sources” (Ahmadi, 2006, pp. 72–73). Thus, secular meaning-making coping has almost no connection with a traditional sacred context, but it can intersect with people’s endeavors to connect with a sacred source, absent any reference to God or traditional religious contexts. As mentioned, according to our definition, the sacred is not necessarily related to a religious context but instead to an inwardly context of sanctification.
It should be mentioned that the term existential meaning-making has been used in a broader way by Lloyd (2018). According to her: “Existential meaning making encompasses lived experiences leading to a fundamental sense of belonging, significance, and meaning in everyday life, as well as in relation to critical events and ultimate concerns as life and death” (p. 31). Secular existential meaning-making is confined to those experiences that are, as explained above, outside the realm of religiosity and spirituality but reflect a sense of belonging, significance, and meaning in individuals’ everyday lives.
In this article, we discuss the secular meaning-making coping of individuals who faced cancer in their developmental trajectory and who used a culturally sensitive approach. Standards for Reporting Qualitative Research (O’Brien, Harris, Beckman, Reed, & Cook, 2014)—have been followed.
Method
Data-Gathering Method
To understand and explore the strategies used by Portuguese oncological patients, we conducted semistructured interviews. The interview guide was constructed based on the Swedish interview study that is part of the larger project (Ahmadi, 2015). However, new open-ended questions were added, and some questions and phrases were modified to make them more suitable to the Portuguese culture and context. Participants also provided sociodemographic (e.g., age, occupation, religion orientation) and clinical (e.g., type of cancer, oncological treatments) information.
Participants
Thirty-one participants (24 women) have been recruited using the snowball method. The participants lived in three different districts of Portugal: Faro (South), Aveiro (Center), and Porto (North). Inclusion criteria of this study were being an adult (female and male) who had received, in the past, a cancer diagnosis or a patient who was still undergoing oncology treatment (e.g., hormone therapy). Religious orientation was not a criterion for participation. Participants’ age ranged between 20 and 73 years. Table 1 presents the sample’s sociodemographic and clinical characteristics.
Sample Characteristics.
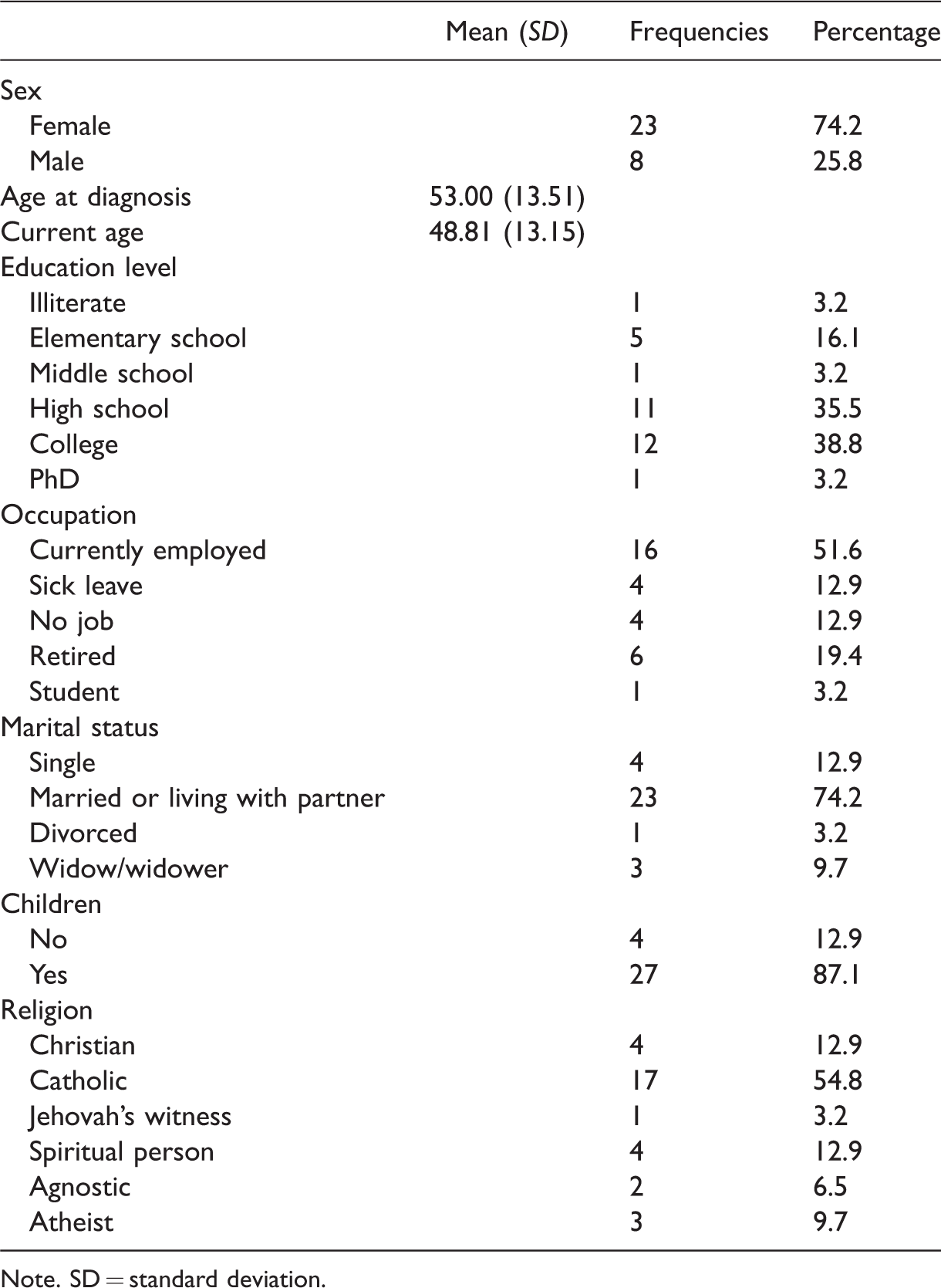
Note. SD = standard deviation.
Ethical Considerations and Procedure
This study was approved by the Ethical Committee of Comissão de Ética da Faculdade de Psicologia e de Ciências da Educação da Universidade do Porto [Ethics Committee of the Faculty of Psychology and Education Science of the University of Porto] (ref. no. 2017/10-1). Before the interview started, the interviewer stressed that participation was voluntary and that the participant could end the interview at any time without consequences to him/her. Moreover, participants were informed that their identity would be preserved, that is, that their names and personal data would be coded to guaranty their anonymity and confidentiality. They were asked permission to be audiotaped. All participants signed an informed consent form.
Two female interviewers (R. T. and C. T.) conducted the individual, face-to-face interviews (October 2017–June 2018). Participants could choose the place where the interviews were conducted (e.g., participant’s home, medical clinic), and the data were audiotaped. The duration of the interviews ranged from 15 to 162 minutes (M = 55 minutes). Some participants had extreme difficulties talking about the disease period. In these cases, the interviewer asked whether the participant wished to finish the interview. None of the participants chose to interrupt the interviews.
Data Analysis
Supported by QSR NVivo10 software, the interviews were transcribed in full and analyzed. The participants’ discourses were coded according to emerging themes using a thematic analysis method (Braun & Clarke, 2006). Given that the aim of the larger project was to investigate diverse meaning-making coping methods (religious, spiritual, and secular existential coping), we started from and extended a modified version of Pargament’s Religious Coping (RCOPE) (Meaning, Control, Comfort/Spirituality, Intimacy/Spirituality, Life Transformation) that has been used in previous qualitative and quantitative Swedish studies (Ahmadi, 2006, 2015). These five fundamental religious functions constitute the basis of RCOPE (Pargament, Koenig, & Perez, 2000). The emerging categories and subcategories were linked to relevant codes in the material. Therefore, the researchers (R. T., P. M. M., and C. T.) read the transcribed interview protocols independently and translated into English a large pool of interview excerpts. The second step was to compare the meaning units that emerged. To achieve conformability, that is, to minimize the authors’ influence on the coding process and ensure their objectivity, they discussed their previous knowledge in the area. In cases where there was no initial agreement on emerging categories, all of the researchers debated the data and identified, by means of consensus, the final themes. In several cases, there was a need to return to the original interview transcripts to guarantee that the identified meaning units corresponded to the participants’ discourse. Following the coding process, the fundamental characteristics of the various methods of coping with cancer observed among the participants were established.
Results and Discussion
In this article, we present the results on secular existential meaning-making coping. The results on religious and spiritual meaning-making coping were presented in another article (Ahmadi et al., 2018). Moreover, findings on the role of family and personal relationships will be discussed in a separate paper. Figure 2 shows the secular existential meaning-making coping methods that emerged from the interviews.
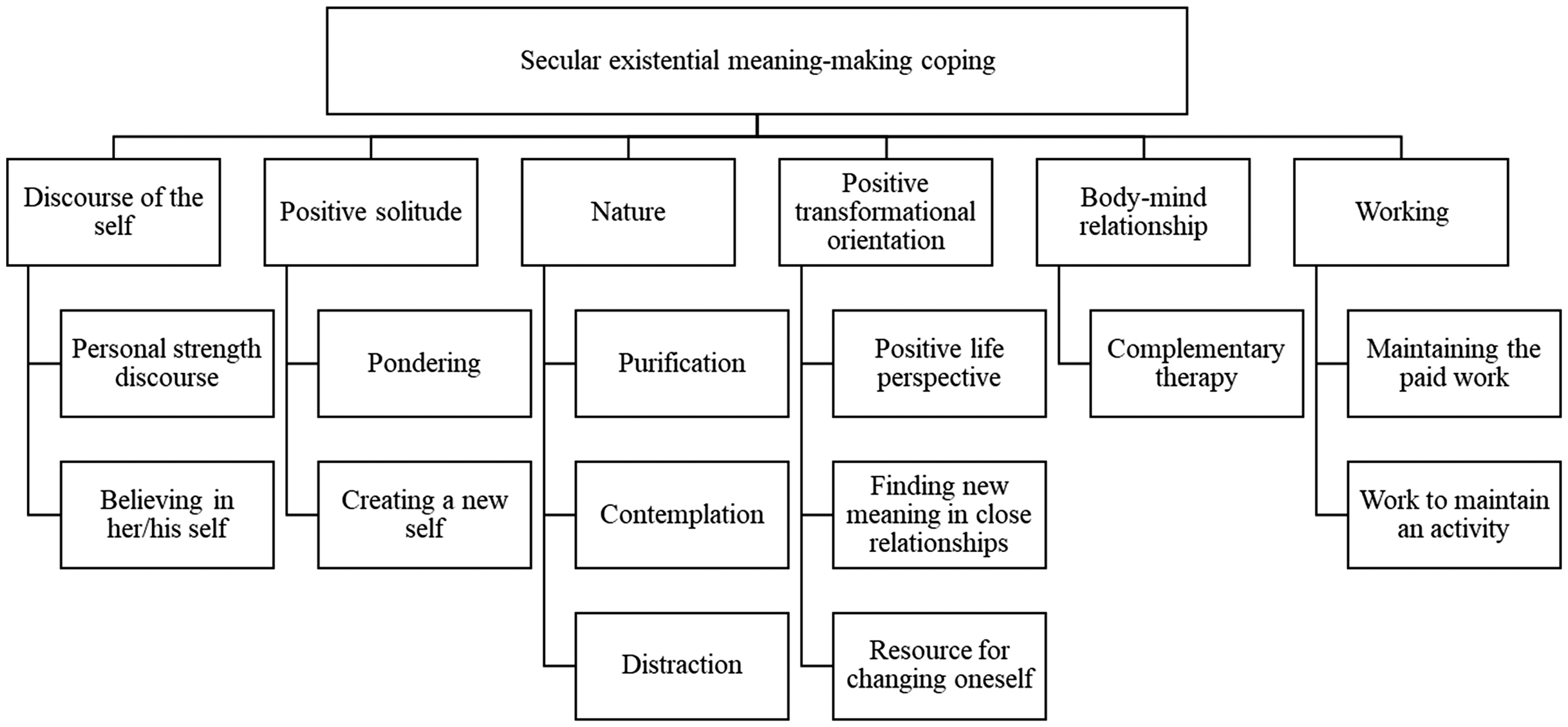
Themes and patterns of secular existential meaning-making coping.
Discourse of the Self
Discourse of the self as a secular existential meaning-making coping was found in this study. We identified two patterns concerning the discourse of the self as a form of secular existential meaning-making coping: Personal strength discourse and Believing in oneself.
The first pattern found was a personal strength discourse that served as a self-protection mechanism. In some cases, to cope with cancer participants used an internal protective mechanism and adopted a positive discourse regarding how they dealt with the disease, although this discourse presented internal contradictions across different parts of the interview. I handle [the disease] well. (…) I’m not a pessimistic person. I play around with this situation [diagnosis of cancer]. (…) I don’t allow other people to make me feel bad. (…) Some days are easy, others are more difficult, but I need to go forward because some people are worse off than I am. (…) I’m not a person who cries. (…) Sometimes, I’ve cried and thought “What are you crying for? There are children [also with cancer] who have never hurt anyone, and you an adult are crying for what?” (…) Now, it’s time to forget [the cancer diagnosis]. (Female, 56 years old) When I was sure of my diagnosis, I felt a deep shock. The story about the heroes of cancer, it is all shit. (…) In the family, nobody talks about my disease. (…) the family environment is not one of disgrace or of bad destiny. (…) My personality and my personal competencies have helped me handle and overcome cancer. (Male, 72 years old) I’m a I’m a curious person, because all this amuses me. My strongest feature is my temper and my strength, it’s too big. (Female, 58 years old) The doctors told me: Lady, you healed yourself with your willpower. Because they said I was going to die. [But] I’ve never been down. That’s why I say, that one’s way of being is the cure for diseases. (Female, 73 years old)
One of the RCOPE methods used by Portuguese oncological patients was the spiritual connection (Ahmadi et al., 2018). In using this method, the patients look for a stronger connection with God or a spiritual person. However, when using the coping method personal strength discourse, one does not seek spiritual connection with God or some other outworldly spiritual source but looks for a source of strength in oneself. This entails a search for an inner power, which may help the patient cope with the stress associated with illness. However, in the personal strength discourse, participants appear to use intellectualization as a defense mechanism, that is, participants talked about their cancer experiences using general statements, avoiding commenting on particular personal reactions and emotions (Di Giuseppe et al., 2018). This mechanism was a way to maintain a self-image of a healthy and strong person who was not affected by a cancer diagnosis.
When men/women face a severe disease, like cancer, they are forced to adopt a new role: a sick role (Parsons, 1991). Parson perceived health as a normal condition and as a person’s optimal ability. Disease, on the other hand, was seen as a deviant condition that makes the person concerned dependent on others. However, Parson’s analysis of the sick role is not based on a medical discourse but on a social, political perspective. Disease is seen as a threat to the social order. The sick role changes how the patient views herself/himself and how others view her/him; this, in turn, affects the individual’s way of facing her/his cancer and coping with it. Believing in oneself challenges the sick role and makes the individual believe she/he can defeat the illness and be cured. This challenge gives the patient the strength to cope with the psychological effects of cancer.
Positive Solitude
Positive solitude is another secular meaning-making coping method; our participants have used in coping with their illness. In this study, preferring to be alone and having the chance to contemplate was recognized as one of the methods used by the Portuguese participants to cope with the anxiety and stress caused by cancer. Several reported having enjoyed being by themselves during this difficult time. We have chosen the term positive solitude for this attitude, which implies an appreciation of being alone. In this secular meaning-making coping strategy, two patterns were recognized: Pondering and Creating a new self.
In some cases, participants felt that being alone allowed them to think about their experience of having cancer. This strategy represents the Pondering pattern. For example, a 66-year-old woman described her situation: Being alone is good. Everyone has her moments and needs to be alone. And needs to think, speak to herself and all these things. That was true in my case. I’ve always had many moments alone, some helped, others didn’t, but these moments made me the person that I am today. I can’t say that all the moments that I was alone were bad, but also not all have been good, they’ve made me who I am today.
Nature
Another secular meaning-making method used by our participants was nature. We found three patterns in this coping method: Purification, Contemplation, and Distraction.
In relation to the Purification pattern, participants mentioned that being in nature was a way of experiencing positive feelings, like emotional relief. For one 37-year-old woman, this method was a way to “clean her soul.” As we can see in the following excerpt, Purification is not merely a way of cleaning the soul but also a way of stilling one’s anger: [Being in nature] a good feeling, a relief … Because in such moments, a person can cry. Everything comes to mind, but we cry and let it go … and this makes us feel some relief. (Female, 46 years old) An important thing to me (…) before surgery was to schedule a weekend with family in Gerês, because I love Gerês (…) I got there in the forest, I took off my sandals, sat on a rock, my bare feet on the ground and I was there talking about, maybe with God and myself. The contact with nature was very important. (Female, 54 years old) And in fact, the birds are real therapists for us, from the point of view of being distracted, they help us pass the time and it was something that helped me in my recovery after liver surgery. (…) One thing, that served me very well was observing the birds and the way they feed.
In both cases, whether a secular or a religious coping method, the issue at stake is that informants perceived a “sacred” value in nature. Concerning the sanctification of nature, it should be mentioned that, in their search for significance, people sanctify different aspects of life. The importance of such a search is magnified when people face a serious life crisis. As Pargament (Zinnbauer, Pargament, & Scott, 2003) pointed out, almost any object can be considered divine in nature. The sacred qualities include attributes of transcendence (e.g., holy, heavenly), ultimate value and purpose (e.g., blessed, inspiring), as well as timelessness (e.g., everlasting, miraculous). The timeliness and immensity of nature—the fact that whatever happens in the world, nature will go on at the same pace—have had a calming and consoling effect on the informants in this study. Nature grants a feeling of security when everything else is chaotic. By sanctifying nature, a person facing a crisis like cancer can experience a spiritual feeling that functions like therapy.
Positive Transformational Orientation
The painful journey that some cancer patients had undergone made them feel more grateful in their present life and brought about “a turning point” in life, a positive transformation caused either by interpreting the situation and their relation with others from a positive perspective or by strengthening their feeling of self. In this study, we found three patterns in relation to positive transformational orientation: Positive life perspective, Finding new meaning in close relationships, and Resource for changing oneself.
Regarding the Positive life perspective pattern, some participants mentioned being able to identify positive aspects of having cancer. Thus, during the disease period, participants used the Positive life perspective coping method, meaning they interpreted their situation from a positive perspective. The main reasons were that their painful journey had taught them to be more grateful for their current life. That is, after cancer, participants adopted new attitudes and started to live their life differently. Several interviewees used this method, as we can see in following excerpts: I think after all, I became more perceptive; I became another person after the disease, I now value the small things in life more. (Female, 62 years old) Sometimes, I look at my illness as an opportunity, a moment of happiness, because my friends have suffered so much, they are gone because of complicated treatments. (…) I can only say that I was very lucky and very happy to go through this. (…) I realized that maybe it was a stage I had to overcome that would make me stronger. (Male, 54 years old) So, it was a rebirth. I’m being reborn at every level. (…) It took me dying once, to be reborn, once again. Now we’re building a new relationship.
The third pattern found was cancer as a Resource for changing oneself, concerning the coping method positive transformational orientation. One of the benefits of overcoming cancer was that the disease had taught patients lessons about themselves and their relationship to life. According to our participants, cancer had helped them become less anxious and rethink their priorities. Several interviewees explained how such a view has helped them cope with their illness: Our spiritual [feeling] tells us “This [cancer] is a challenge. Nothing’s going to happen [i.e., not going to die]. This is just for you to learn some new things, learning that you have to make changes in your life (. . . ).” (Female, 40 years old) Things happen for a reason. Maybe it’s to make us better people. (Female, 50 years old) I think that all these stages of life [had cancer and a cancer recurrence after 10 years] made me a different woman. (…) I used to be anxious, very nervous, I used to go to battle [for everything]. I was always running and [describes herself as a hurricane]. Today I confront life in a totally different way. I tell my daughter: Don’t rush. Breathe. You don’t need to be perfect, because this destroys you slowly, slowly. (Female, 52 years old)
Use of a personal transformation strategy to handle stressful and painful events, such as cancer, decreases the threat of the situation, thus making it more bearable (Wong, Lawrence, Struthers, Mclntyre, & Friedland, 2006). Personal changes can occur along different dimensions, such as lifestyles, personality, values, among other things (Wong et al., 2006). This pattern appears to be associated with posttraumatic growth, this is, the perception of positive changes owing to the experience of traumatic or stressful life events (Tedeschi & Calhoun, 2004). Thus, the pattern positive transformational orientation could emerge in patients experiencing posttraumatic growth (Chan, Ho, Tedeschi, & Leung, 2011; Danhauer et al., 2013). According to Calhoun, Tedeschi, Cann, and Hanks (2010), persons who lost a close friend or relative overcame the tragedy by focusing on their personal strengths, new spiritual insights, and appreciating their relationships. In the same way, some participants in this study focused on the positive changes that cancer allowed as a way of dealing with the disease.
There are several views on use of forms of transformation as coping methods in relation to spirituality. Wong et al. (2006), for example, maintained that the Buddhist transformational approach advocates the development of the pathway of enlightenment and mental disciplines—to build up one’s inner resources such as wisdoms and compassion, so that one is able to face whatever life may throw at him or her with equanimity and compassion. Effective coping results in becoming free not only from the negative effects of stress, but also the source of suffering. (p. 7)
Body–Mind Relationship
Some cancer patients believe that an unhealthy and stressful lifestyle and negative mental state are the cause of cancer. They think that a negative mental state can bring about bodily dysfunction. Such a view can be interpreted as belief in a body–mind relationship. In this regard, we found that use of Complementary therapy, a coping pattern, is related to such a belief. Concerning this pattern, participants mentioned: I meditated while I went through chemotherapy. (…) After treatment I used to leave the hospital with a great sense of peace. (…) I did a lot of meditation. I did Past Life Regression Therapy. I tried everything [during treatments], because I think we only succeed if there are complementary treatments (…) My doctor always asked me what my secret was. So, I said that I did a lot Reconnection Healing. (Female, 40 years old) I got the strength [to deal with the disease] by using Reiki, Quantum touch, Reconnection healing. Especially the reconnection cure and quantum touch. After doing Reiki, I was fine. In quantum touch, I felt completely fragile, but after 2 or 3 days, I felt [better]. The quantum touch is what helped me feel free from this torment, this disease. (Female, 52 years old)
Currently, little is known about the use of complementary therapy in Portugal (Carvalho, Lopes, & Gouveia, 2012; Portela et al., 2017). However, one exploratory study with Portuguese participants found that 77% of them reported having used complementary therapies at least once (Carvalho et al., 2012). One possible reason for this percentage is that the Portuguese National Health System finds it difficult to meet the needs of patients, given the system’s long waiting lists. Since 2003, complementary therapies (such as acupuncture, osteopathy, naturopathy, among others) have been legally regulated in Portugal, and currently, some Portuguese public hospitals offer acupuncture and Reiki to their patients (Silva, 2015).
Working
In this study, some participants used paid work as a method of coping with cancer. Maintaining paid work promoted feelings of normality in participants’ daily life as well as positive feelings (e.g., calm, utility). I said, I’m going back to school. [She is a school teacher] and the doctor said, No, you’re not going back to school. You just started chemotherapy treatment and you’re going back to school now?. I told him, I will, because that’s where I’m nurtured emotionally. (…) I like what I do. I have a passion for what I do. I’m going back to school. (Female, 40 years old) I chose to work during treatment. (…) My physician asked me to stop working, but it [working] was the way I found to deal with the situation. (Female, 54 years old) I’m a person who needs to work with something. I must work to be calm. I must always have aims, always doing something. Always, always. I started working at 23 years old. … I must always have aims. I must work all the time. (Female, 58 years old)
Limitations and Conclusions
This study has some limitations that we will summarize. First, most of the participants were women. Choosing secular existential coping as a method may differ by gender owing to different gender role cultural expectations. Second, participants were recruited by convenience using a snowball method. Consequently, our participants may represent patients who experienced better psychological adaptation to cancer. Longitudinal studies could capture possible changes in patterns of meaning-making coping across the disease trajectory. Although this study has limitations, it also has several strengths. The sample was heterogeneous regarding the type of cancer and the age of participants at diagnosis. Thus, the sample captured diversity in the meaning-making coping used by different Portuguese cancer patients.
This study aimed to explore the secular existential coping strategies used by Portuguese cancer patients and to analyze how the choice of coping methods is embedded in the culture. We found six secular existential coping methods among Portuguese cancer patients: (a) discourse on self, (b) positive solitude, (c) nature, (d) positive transformational orientation, (e) body–mind relationship, and (f) working. These methods helped patients assign meaning to their cancer experiences and seemed to facilitate psychological adaptation to the disease (Lee et al., 2006a, 2006b; Vickberg et al., 2001). In general, the present findings are consistent with the literature. The cultural environment influences the meaning-making coping methods used by cancer patients (Banerjee et al., 2011). Therefore, in clinical practice, psychologists and other health professionals should consider cultural beliefs when they work with cancer patients as well as when they explore these patients’ coping strategies.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fundação para a ciência e a tecnologia (CPUP UID/PSI/00050/2013; FEDER/COMPETE2020 POCI-0 and SFRH/BD/129126/2017) and Högskolan i gävle.
Correction (February 2024):
Article updated online to correct the issue publication year from 2021 to 2022. See https://doi.org/10.1177/10541373241230139