
Abstract
Background
People with Parkinson’s disease present with both motor and non-motor symptoms. Tele rehabilitation (TR) is effective to maintain and improve different functional activities in people with neurological disorders. Virtual reality (VR)-based rehabilitation involves training movement and activities in a virtual setting.
Objective
To systematically review the evidence and estimate the effect of virtual and tele-rehabilitation on motor and non-motor impairments in patients with PD.
Methods
The databases MEDLINE, PEDro, Scopus, and Web of Science were searched from inception to January 2024 for randomized controlled trials (RCTs) and quasi-experimental studies. The methodological quality of the included studies and risk of bias was assessed using the PEDro scale and Cochrane risk of bias tool respectively. Studies providing sufficient data on either of the pre-established outcome measure were included in the meta-analysis.
Results
Meta-analysis of the 18 studies showed that more improvement in balance function was seen with VR rehabilitation than with traditional exercise (TE) training. VR and TE were found to have similar effects on the (DGI) dynamic gait timed-up and go (TUG) test.
Conclusions
The available evidence suggests a positive effect of VR exercise on balance function. TR is feasible and provides similar clinical benefits to that of in-person care. VR and TR compared to TE in physiotherapy have similar effects on gait.
Introduction
Parkinson’s disease (PD) is an age-related complex, progressive, neurodegenerative disorder characterized by both motor and non-motor manifestations. 1 It is characterized by specific motor symptoms such as resting tremor, slowed movement, rigidity, and impaired posture. It can adversely affect gait and balance function, movement quality, and increased fall risk. 2 Non-motor features include impaired olfaction, cognitive impairment, mood disorders, sleep disorders, speech dysfunction, dysphagia, pain, and fatigue and can have an impact on patient’s functioning, independence, and health-related quality of life (QoL). 3 PD patients experience a deterioration of body function, daily activities, participation, 4 and decline in mobility. 5 These changes may eventually lead to inactivity and social isolation. 6
PD is the second most common neurodegenerative disease. 7 The prevalence of PD ranges from 0.13% to 1.6% in those under the age of 60, and it can reach 9% in those between the ages of 80 and 84, 8 with the disease prevailing in both genders between the ages of 70 and 79. Dopaminergic neuron loss in the substantia nigra pars compacta (SNpc), Lewy body pathology, and aggregation of abnormally folded proteins causing neurodegeneration are the pathogenic basis of PD 2 Neuro-inflammation-mediated, primarily, by activated astrocytes and microglia is another feature of PD pathology. 9
Virtual reality (VR) and telerehabilitation (TR) have been found effective and feasible in many neurological conditions like stroke 10 and multiple sclerosis. 11 TR is the delivery of rehabilitation services through electronic systems using information and remote medical communication tools. 12 TR is a good alternative for PD patients whose impairment is increasing and who find it difficult to schedule the hospital visits because of distance, additional cost of traveling, and uneven distribution of rehabilitation services. 13 TR aims to improve gait, balance, upper limb (UL) functions, speech and dysarthria, QoL, autonomy,14,15 and can be an effective means of rehabilitation, as it provides new opportunities for growing accessibility and generating a less restrictive environment. 16
In recent years, VR has emerged as a cutting-edge treatment tool in the neurorehabilitation of PD patients. VR offers an opportunity for high-intensity, task-oriented, and multi-sensory feedback training, to optimize motor learning in a safe environment. 17 VR technology provides greater potential for transfer to functional activities of daily living as it replicates real-life scenarios. Previous studies have confirmed that in patients with PD, VR technology plays an active role in improving gait, 18 balance function, daily life activities, 19 and QoL, and cognition in the elderly. 20
However, TR and VR are relatively novel technologies and not yet routinely used in clinical practice since there are only a handful of randomized controlled trials (RCTs) and even fewer meta-analyses performed in patients with PD. There has been no meta-analysis on any outcome of TR to date. A review investigated the role of VR for PD rehabilitation and reported a positive effect on gait parameters. 21 In addition, two recent meta-analyses have reported positive changes in various outcomes in people with PD.22,23 In order to integrate the new evidence updated in recent years given the potential advantages of VR and TR technology, the current research focuses on systematically reviewing the available literature on the role of VR and TR on gait, balance, upper limb function, speech, dysarthria, fall, global motor function, and neurocognitive and psychosocial aspects of living in people with PD.
Methods
Current review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 24 The pre-specified eligibility criteria and methods of analysis were reported in a protocol (CRD42022278486) registered on PROSPERO (International Prospective Register of Systematic Reviews).
Eligibility criteria
Studies which met the following criteria were included in the review.
Participants: adults older than 18 years with a clinical diagnosis of idiopathic PD were included and no restrictions were placed on the disease’s severity, duration of the disease, gender of the participants.
Intervention: trials administering either TR or VR were considered for the review. Comparator: no restrictions were placed on the comparator.
Outcome measures: to account for the measures of gait, balance and falls, upper limb function, speech and dysarthria, global motor function, neurocognition, and psychosocial aspects more comprehensively, following outcomes were considered for inclusion: Dynamic Gait Index (DGI), Functional Gait Assessment (FGA), Six- or Ten-Minute Walk Test (6MWT or 10MWT), Center of Pressure (CoP), Berg Balance Scale (BBS), Timed Up and Go Test (TUG), Mini Balance Evaluation System Test (Mini BESTest), the Trail Making Test (TMT-B), The Disabilities of Arm, Shoulder, and Hand (DASH), Unified Parkinson’s Disease Rating Scale (UPDRS) III, Box and Block Test (BBT), Nine-Hole Peg Test (9HPT), (PDQ-39), sound pressure levels (SPL), acoustic sound, loudness, Montreal Cognitive Assessment (MoCA), Mini-Mental State Examination (MMSE), Digit Span Forward (DSF) test, Geriatric Depression Scale (GDS), generic or disease-specific health-related QoL instruments (PDQ-39), the BI (Barthel Index), and Fall Efficacy Scale (FES).
Types of study: only RCTs and quasi-experimental design studies were included in the review. Studies on populations with neurological disorders other than PD, animal studies, and trials published in languages other than English were excluded. Trials lacking the approval of local ethics committee, case studies, pilot studies, conference proceedings, editorials, and narratives were excluded.
Information sources
Trials were identified through a systematic search in the following databases: MEDLINE (accessed by PubMed), PEDro, Scopus, and Web of Science (Web of Science Core Collection). The search was carried out from December 2023 to January 2024. The review included records available till December 7, 2023.
Search strategy
The search was done with a combination of MeSH (Medical Subject Headings) terms and keywords such as “Parkinson’s disease”, “Telerehabilitation”, “tele-exercise”, “e-health”, and “virtual reality”. Appropriate Boolean operators were used, including ‘AND' and ‘OR'. There were two steps in the entire search process – each intervention was searched separately, for example (“telerehabilitation” OR “tele-exercise” AND “Parkinson’s disease”), (“Virtual reality” AND “Parkinson’s disease”), and (“e-health” AND “Parkinson’s disease”) forming a subcategory of findings. Each subcategory was searched and analyzed independently. All results were imported in EndNoteTM online (reference management software) for screening
Selection and data collection process
Two reviewers (ZA and SP) conducted the literature search independently. When evaluating search results, the eligibility requirements were unanimously agreed upon. Elimination of duplicate references was done, followed by the screening of records by title and abstract. After screening, the full-text of the remaining records was assessed for eligibility. Any conflicts between the reviewers were resolved by consensus or in consultation with a third reviewer (MN).
Data extraction and analyses
The reviewers (ZA, SP, CS, and MN) extracted the data from the included studies related to participants (age, sex, sample size), intervention (VR, TR), and outcome measures. The standardized mean difference (SMD) and 95% confidence interval (CI) were determined under random-effects model. Cochrane Collaboration Review Manager (RevMan) 5.4.1 was used for the meta-analysis. For calculating the effect size (ES), Cohen’s d criteria were employed, where a value of <0.2 indicates small ES, a value between 0.2 and 0.5 indicates moderate ES, and a value of >0.5 indicates large ES. I2 statistics were used for determining the heterogeneity between the included trials (low heterogeneity: I2 < 25%; moderate heterogeneity: I2 < 25.75%; substantial heterogeneity: I2 > 50%). 25 Forest plots were used for summarizing the results. For the assessment of publication bias in the included studies, funnel plot was used.
Methodological quality and risk of bias assessment of the included studies
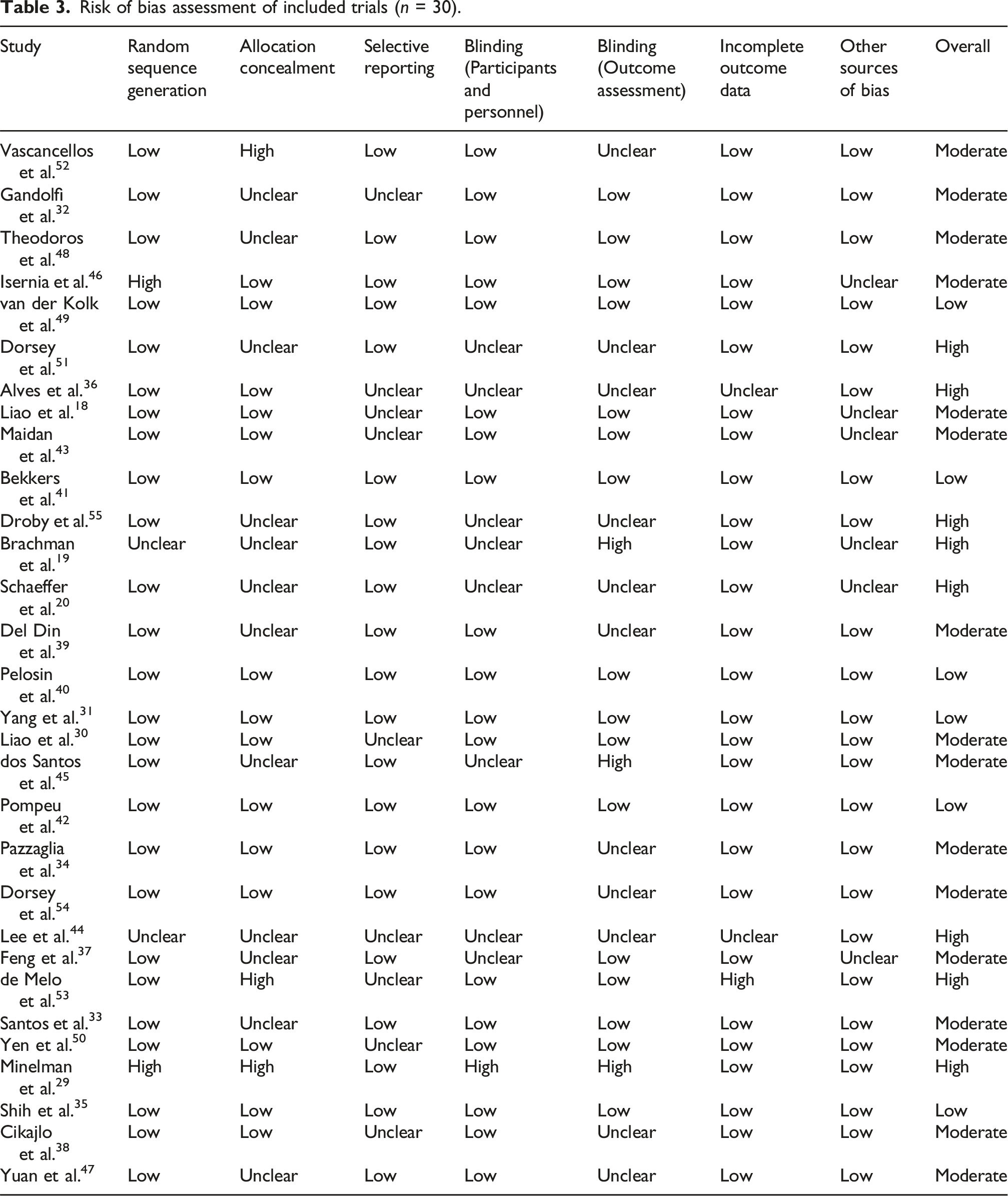
ZA and SP independently assessed the methodological quality and risk of bias of each included trial using the Physiotherapy Evidence Database (PEDro) scale 26 and the Cochrane risk of bias assessment tool 27 , respectively. PEDro is 11-point scale. Each item in the scale is scored as either present (1) or absent (0) and a total score is produced by summation. In accordance with the total score obtained, the trials can be classified as poor (<4), fair (4–5), good (6–8), and excellent quality (>8). 28 A third researcher mediated every disagreement (MN). The Cochrane risk of bias tool includes the following seven domains: random sequence generation, allocation concealment, selective reporting, other sources of bias, blinding (performance bias), blinding (detection bias), and incomplete outcome data. Each domain was categorized as low, unclear, or high with the risk of bias for each trial classified using the following criteria: (1) low risk of bias (all criteria graded as low), (2) moderate risk of bias (one criterion graded as high or two criteria graded as unclear), and (3) high risk of bias (more than one criterion graded as high or more than two graded as unclear). 27 Disagreements between reviewers were resolved through further discussion among themselves or with the third reviewer when required (MN).
Results
A systematic search of various databases revealed 687 records, out of which 220 duplicates were removed. This was followed by the title and abstract screening of the 467 records. A total of 47 studies went for eligibility screening. Of these, 17 were excluded and 30 met the inclusion criteria. Eighteen trials18,20,29–44 were considered for meta-analysis. The detailed selection process is described in Figure 1. PRISMA flow diagram depicting the study selection process.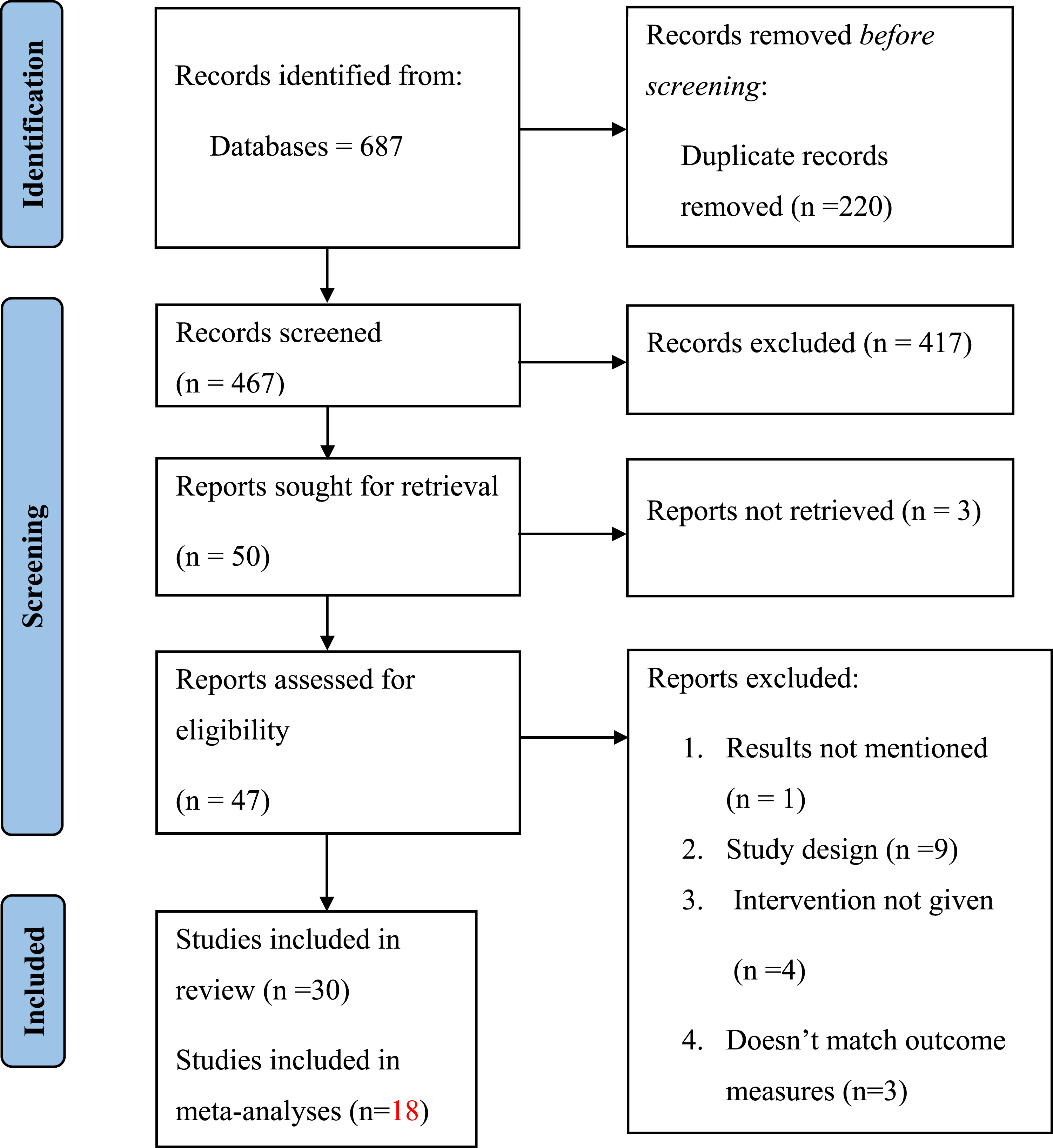
Characteristics of the included trials
Characteristics of the randomized controlled trials (n = 26).

M: male; F: female; TE: traditional exercise; UC: usual care; H&Y: Hoehn and Yahr scale; C: control group; I: intervention group; TT: treadmill training; LSVT: Lee Silverman Voice Treatment; VR: virtual reality; PD: Parkinson’s disease; PDQ-39: 39-Question Parkinson’s Disease Questionnaire; MMSE: Mini-Mental State Examination; DGI: Dynamic Gait Index; ABC: Activities-specific Balance Confidence Scale; 6MWT and 10MWT: 6 & 10 Minute Walk Test; MoCA: Montreal Cognitive Assessment; BBS: Berg Balance Scale; SIBT: Sensory Integration Balance Training; min: minute; wk: week; TUGT: Timed Up and Go Test; UPDRS: Unified Parkinson’s Disease Rating Scale; miniBEST: mini Balance Evaluation Systems Test. CBT: Conventional Balance Training; SOT: Sensory Organization Test; CoP: Center of Pressure; LOS: Limits of Stability; BBT: Box and Black Test; 9HPT: Nine-Hole Peg Test; MFES Modified Fall Efficacy Scale; MDRT Multi-Directional Reach Test; MSL Maximum Step Length; SF-36 36-Item Short Form Survey; IVGB: Interactive Video Game Based Exercise; SPPB: Short Physical Performance Battery; MBI: Modified Barthel Index; BAI: Beck Anxiety Index; BDI: Beck Depression Index; FGA: Functional Gait Assessment; DASH: Disabilities of Arm; Shoulder and Hand Questionnaire; FRA; Fall Risk Assessment; MCI: Mild Cognitive Impairment; OA: older adult; FOG: Freezing of Gait; FES: Fall Efficacy Scale; NW: Nintendo Wii; NWCE: Nintendo Wii Conventional Exercise.
Characteristics of the non-randomized controlled trials (n = 4).

M: male; F: female; TE: traditional exercise; UC: usual care; C: control group; I: intervention group; H&Y: Hoehn and Yahr scale; PD: Parkinson’s disease; FBT: Functional Balance Training; TUGT: Timed Up and Go Test; LOS: Limits of Stability; BBS: Berg Balance Scale; MMSE: Mini-Mental State Examination; FRT: Functional Reach Test; BAI: Beck Anxiety Index; WHOQOL-OLD: World Health Organization Quality of Life-Old; 10MWT: 10 Min Walk Test; DSF: Digit Span Forward; MoCA: Montreal Cognitive Assessment; BBT: Box and Black test; SF-12: Short Form Survey-12.
TR in people with PD
Six studies32,46,48,49,52,54 assessed the effect of TR (video conferencing, audio calls, and messages) or any remote communication technologies to rehabilitate PD patients at home. Out of the 6 studies, 5 were RCTs48,49,51,52,54 and one was a quasi-experimental study. 46 Participants (n = 425) included in the trials were adults (>18 years) with PD. Participants were a mixed ratio of both genders. The sample size ranged from 28 52 to 130. 49 The length of the intervention varied from 3 weeks 52 to 7 months. 54 The duration of a single session varied from 30 minutes 49 to 1 hour. 48
VR in people with PD
A total of 24 studies investigated the effect of VR in PD patients. Out of these 24 trials, only three studies19,36,45 were quasi-experimental, the while rest of the trials were RCTs. The sample size of the included trials ranged from 16 45 to 282. 29 All the participants (n = 1181) in the included studies were adults, older than 18 years, and having the mean age of 67.4 ± 8.2. The trials consist of both male and female participants. In the included studies, VR was either combined with treadmill/conventional/traditional training or administered alone. The length of the intervention in the included trials varied from 3 weeks 38 to 7 months. 37 A single session of intervention lasted from 30 minutes19,38,47 to 1 hour. 42 VR was delivered remotely in only two studies.20,31
Quality assessment of the included trials
The included trials scored from 3 47 to 9 49 on PEDro and the mean PEDro score was 6 (good) (provided as a supplemental material). High methodological quality was provided by most of the included trials. Among the included articles, three trials scored 4,38,40,43 five studies scored 5,19,39,45,54,55 six trials scored 6,20,36,41,44,46,51 four studies scored 8,18,29,30,42 and rest of the trials scored 7 on PEDro. Random allocation was reported in 26 studies (86.6%). Group similarity at the baseline was reported in most of the studies (90%). Blinding of the assessors (70%), follow-up of the participants (63.3%), carried out between-analysis (100%), employed both measures of variability and point measurement (93.3%) was reported in the majority of the trials.
Risk of bias assessment of the included trials
Risk of bias assessment of included trials (n = 30).

Risk of bias summary of the included trials for systematic review and meta-analysis.
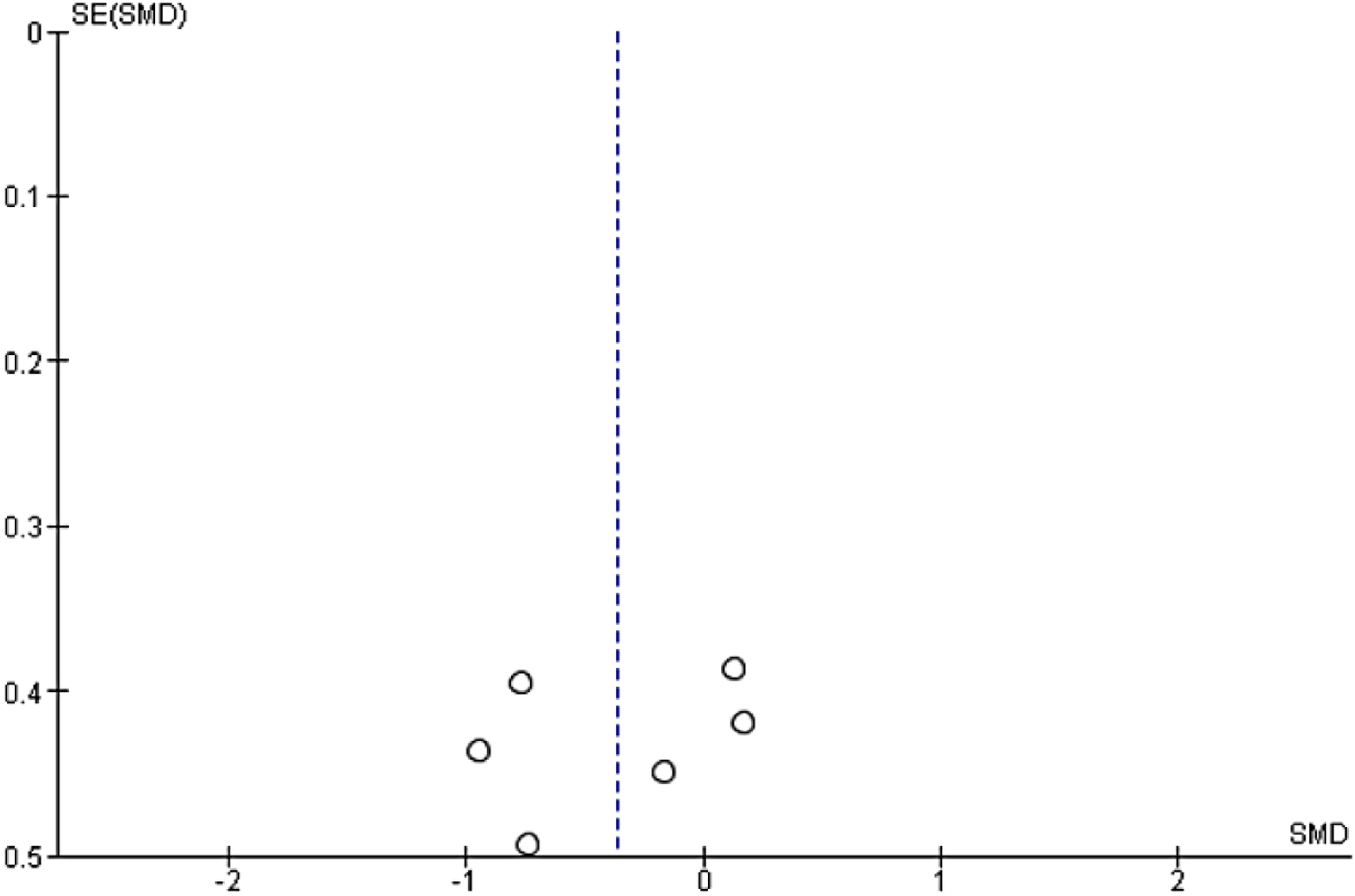
Funnel plot for the risk of publication bias (TUG test).

Funnel plot for the risk of publication bias (UPDRS III).

Funnel plot for the risk of publication bias (BBS).
Results of the meta-analysis
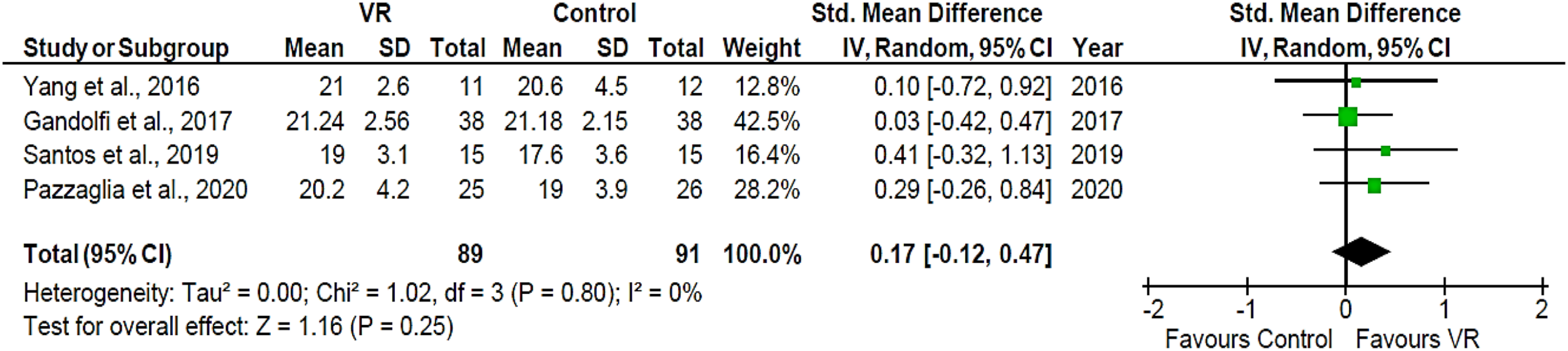
Gait: Three studies18,20,30 involving 101 PD patients reported the effects of experimental VR on stride length. High heterogeneity was observed (I2 = 87%, p = 0.0004). The pooled outcome showed no significant difference between the experimental VR and control group (SMD = 0.05; 95% CI = −0.41, 0.50; Z = 0.20; p = 0.84) (Figure 6). Four studies31–34 involving 180 participants with PD evaluated the effect of VR on DGI. Initial pooled outcome demonstrated no significant effect of VR on DGI (SMD = 0.17; 95%CI = −0.12, 0.47; Z = 1.16; p = 0.25) (Figure 7). Meta-analysis of included studies comparing stride length. Experimental: VR. Meta-analysis of included studies comparing Dynamic Gait Index.
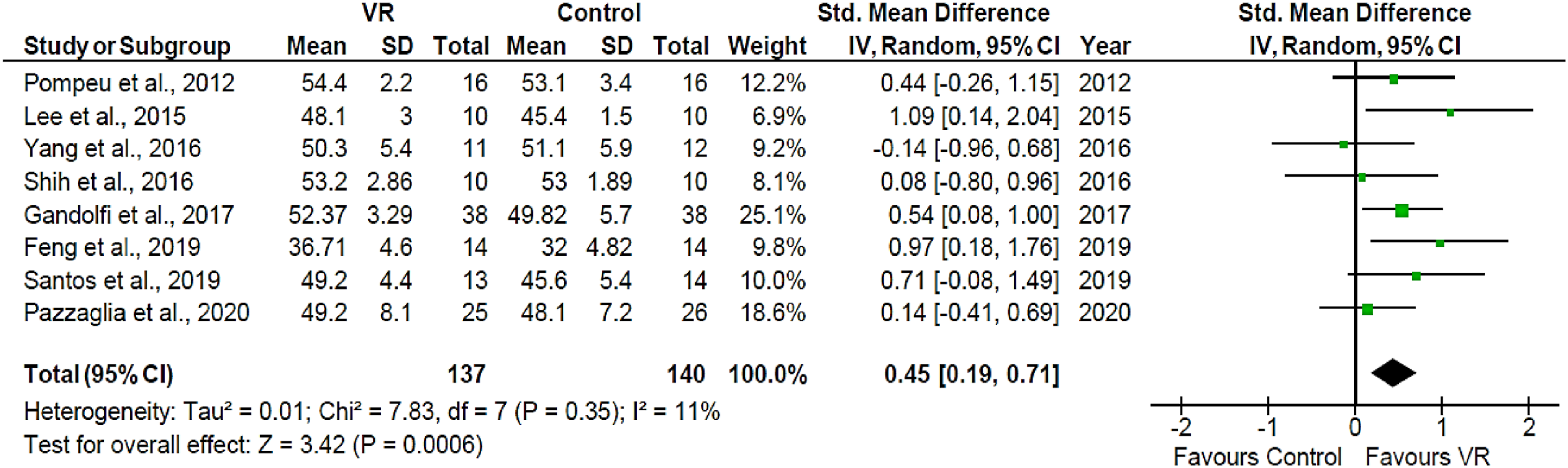
Balance: Six studies18,31,33,35–37 involving 140 PD patients observed the effect of VR on the TUG test. Low heterogeneity was reported (I2 = 27%, p = 0.23). The pooled analysis showed no significant effect of VR on the TUG score (SMD = −0.37; 95%CI = − 0.77, 0.03; Z = 1.81; p = 0.07) (Figure 8). Eight studies31–35,37,42,44 involving 177 PD patients investigated the effect of VR on BBS. Pooled analysis revealed positive improvement in the scores of BBS (SMD = 0.45; 95%CI = 0.19, 0.71; Z = 3.42; p = 0.0006) and low level of heterogeneity (I2 = 11%; p = 0.35) (Figure 9). Forest plot of changes in the score of timed-up and go test. Forest plot of changes in the score of Berg balance scale.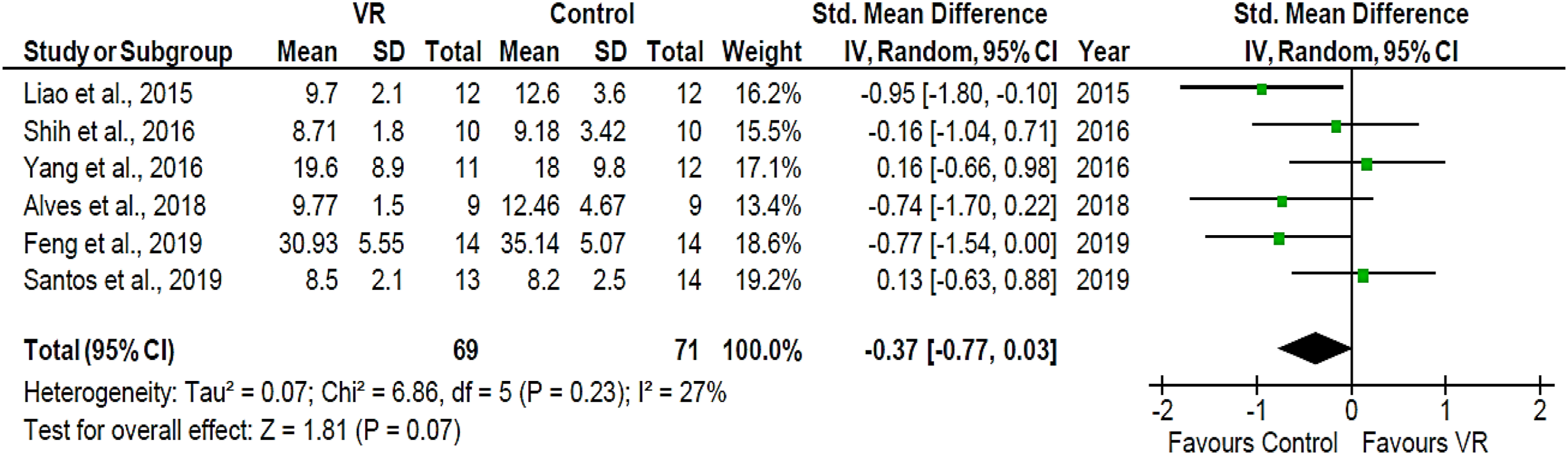
Neurocognitive and Psychosocial aspects: The effect of VR on PDQ-39 was observed in 3 trials.18,31,33 Pooled analysis failed to show any significant effect of VR PDQ-9 (SMD = 0.12; 95%CI = −0.33, 0.58; Z = 0.53; p = 0.59) and low heterogeneity was observed (I2 = 0%, p = 0.73) (Figure 10). Meta-analysis of included studies comparing PDQ-39.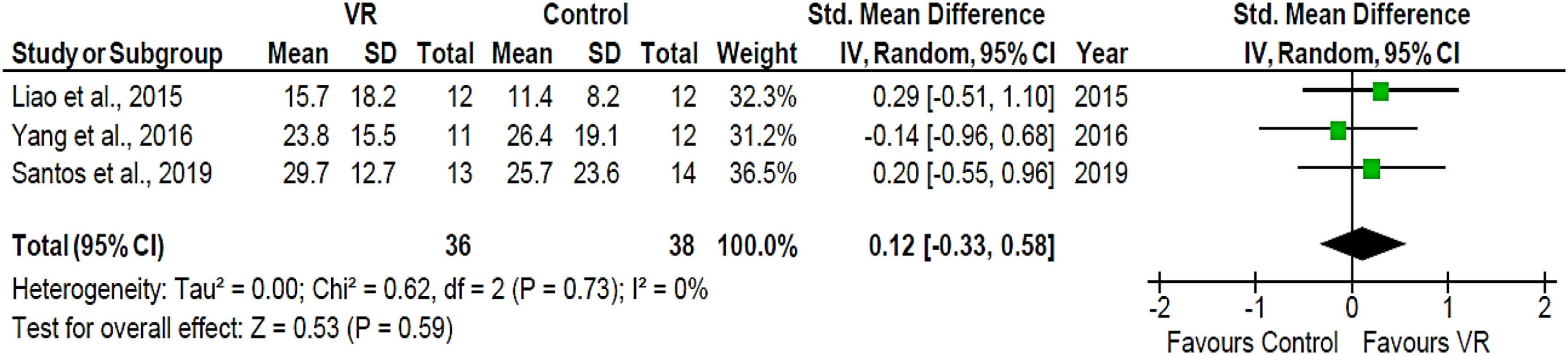
Falls: Three studies29,39,41 observed the effect of VR on falls. High statistical heterogeneity was reported (I2 = 86%, p = 0.0006). The pooled analysis indicates that VR does not have any significant effect in reducing the event of falls (SMD = −0.12; 95%CI = −0.68, 0.43; Z = 0.44; p = 0.66) (Figure 11). Forest plot for the changes in event of fall.
Global motor function: Six studies31,37,38,40,41,43 observed the effect of VR on UPDRS III. The pooled analysis indicates that VR doesn’t have any significant impact on UPDRS Ⅲ (SMD = 0.08; 95%CI = −0.25, 0.41; Z = 0.47; p = 0.64) and moderate heterogeneity was observed (I2 = 42%, p = 0.12) (Figure 12). Forest plot for changes in the scores of UPDRS III.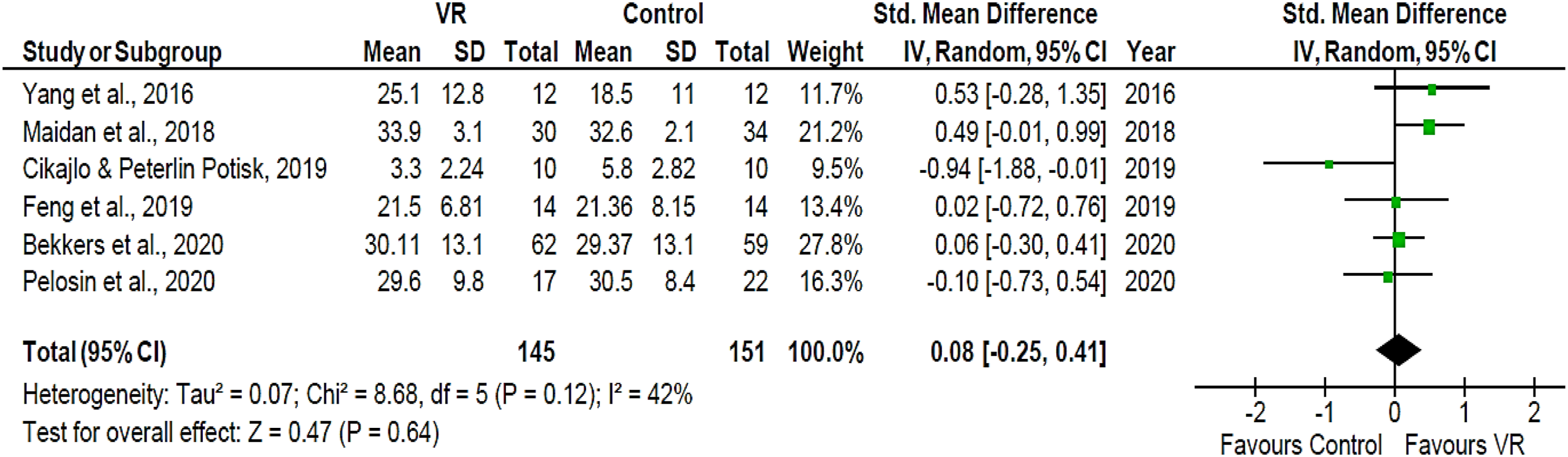
Discussion
The effect of VR on gait was examined in four studies, out of which three were RCTs. Two trials32,46 showed positive results with improvement in gait with TR on DGI, 10 MWT, and gait velocity. Two studies49,52 showed negative results with no improvement with TR in the gait of PD patients. However, no significant superiority of TR on gait compared to face-to-face or in-clinic rehabilitation was found, and the positive effects were not sustained beyond the intervention period. The brief intervention period and absence of face-to-face supervision may have resulted in poor patient engagement and performance.
Effect of VR in people with PD
Thirteen trials assessed the role of VR on the gait outcomes in the PD population, out of which 12 were RCTs and one study 36 was of quasi-experimental design. Eleven of the included studies18,20,29,30,33,34,36,37,40,43,47,53 reported a positive change in the gait after receiving VR in PD patients, which was tracked by improvements in gait speed, velocity, step/stride length, obstacle planning, and crossing performance. Alves and colleagues 36 reported an increase in the gait speed in the VR group, and the results were also sustained at a 1-month follow-up. One trial 33 reported that VR produced similar results to TE; however, when VR was given along with TE, it produced better results than every single intervention alone. Mirelman and colleagues 29 reported improved gait speed and gait variability immediately with a 6-week training in the VR + treadmill training (TT) group compared to the TT only group and also at 6-month follow-up. This result was supported by 2 other studies40,43 in which participants receiving VR + TT resulted in better gait and obstacle negotiation with 18 weeks of training compared to the TT only group; however, effects were either not reported or sustained at follow up in any of the studies. In a study by de Melo and colleagues 53 gait speed increased in the VR group compared to the TE group but was the same as the TT group with a training session of 12 weeks; however, the results were not sustained at 1-month follow-up. Two trials18,30 reported no significant difference in stride length and obstacle negotiation ability on a 1-month follow-up of VR Wii + TT compared to the TE + TT group; however, when compared to the control group receiving no exercise, VR Wii training was most successful in improving horizontal crossing distance and velocity rather than vertical toe clearance. The reason behind unaltered gait parameters after VR was speculated to be insufficient intensity and time effect or an interaction of the therapeutic effects of the interventions. Another trial by Yang and colleagues also showed that VR resulted in similar results to TE on gait using DGI and was not superior. 31 This could be attributed to the size of the population in the study; shorter follow-up periods were inadequate to show unequivocal changes in gait parameters. Of these 7 studies that reported sustained improvement at follow-up, effects vanished at 6 months of follow-up in the study by Pelosin and colleagues 40 while five of the studies did not report proper follow-up.
Fifteen trials studied the effectiveness of VR for balance outcomes. Of the included studies, eight trials18,19,29,34,36,37,44,47 showed a positive effect of VR on balance. Seven trials31,33,38,41,42,50,55 reported no significant difference between VR or TE. The possible reason behind these findings might be the use of similar design rationale used by most of the trials thus producing same treatment effects.
One study 36 compared the two forms of Nintendo Wii and Xbox Kinect along with a control group and found that Nintendo Wii resulted in a significant increase in the distance walked and step length training with Nintendo Wii in both simple and dual condition walking tasks. In a RCT done by Liao and colleagues 30 reported decreased postural sway in different manipulatory conditions in sensory organization test (SOT) to improve stance balance after 12 sessions (2 sessions/week) for 6-week training in the VR, however another RCT 50 with the same exercise duration and intensity reported no significant difference in sensory integration ability between the VR and TE group. Improvement in sensory integration due to VR could be due to the large amount of optical flow in the virtual environment with visual feedback.
Two trials41,55 compared TT with TT + VR group, where both reported that TT alone is showing similar results as TT + VR group in improving balance and sway during walking in PD patients. The possible mechanism for this could be the low exercise duration in both studies which might have been not sufficient to bring changes in the balance functions of patients and the lack of proper follow--up in both studies. Brachman and colleagues reported an improvement in limit of stability (LOS) after 12 sessions of training 19 which is supported by another study 47 with similar results after a training of 18 sessions. Therefore, the effect of VR balance training with respect to general exercise or no exercise remains unanswered.
Seven trials31,33,38,41,42,50,55 failed to produce any significant change in various balance parameters after receiving VR, where the total number of intervention sessions was less than or equal to 12. However, significant improvement was reported in seven studies18,29,39–41,43,47 in fall incidence in PD patients when they were administered with VR, where the number of sessions were more than or equal to 18. This reveals that the benefits of VR on balance may be more potent in those receiving higher intensity and longer duration of VR intervention.
Another trial 38 compared immersive with non-immersive VR technology and found similar improvements in UL hand functions in both groups after 6 weeks of training. Similar results were reported in the study by Pazzaglia and colleagues 34 on the DASH scale in which the VR group reportedly performed similarly to the TE group with 6 weeks of training. This could be attributed to low exercise frequency in both studies.
UPDRS III improved with VR even with different training durations: in one study 37 with 12 months of training, in another study 38 with 3 months of training, and in one study done by Schaeffer and colleagues 20 with 6 months of training. Three trials31,42,52 reported similar improvements on UPDRS III in both the experimental and control groups for VR. VR training in PD patients in the study by Schaeffer and colleagues 20 6 weeks also showed improvements in dual tasking on MoCA. In another trial 49 PD patients’ ability to recall improved on trial-making test with 6 months of training in both the VR intervention group at home and the VR control group at home.
Effect of TR in people with PD
Three trials reported positive effects of TR on balance training in patients with PD. Gandolfi and colleagues 32 reported that 7 weeks of training using in-home VR-based TR improved balance in PD patients. One study 46 found similar improvements in balance with a 12-week home VR training program compared to an in-clinic HEAD group with the effects being retained at 3 months follow-up. Vasconcellos and colleagues 52 reported the same effect with both trunk/global TR or TR focused on upper/lower limb on balance measures in a 3 weeks of training in PD population.
TR using UL exergames was found to be acceptable, feasible, and comparable with the TE but did not translate into functional improvement in the dexterity of the hand in the long term. One RCT 49 which compared TR-based intervention at home with TR-based control group at home, improvements in pegboard tests were reported after 72 sessions spread over 6 months. However, no follow-up was recorded.
UPDRS III also improved more with TR than TE in one study 49 with 6 months of training and another study 54 with 7 months of training. With TR, MoCA was found to improve in three studies.46,49 The feasibility and validity of TR compared to face-to-face rehabilitation were also assessed in the study by Isernia et al., 2020 and the group receiving HOME treatment resulted in better improvements that the TE after 3 months of training.
One study 48 compared face-to-face and online Lee Silverman Voice Treatment (LSVT LOUD) speech therapy for motor speech and voice disorders for 1 hour/day, 4 days/week, for 1 month in 30 patients with PD and reported the non-inferiority of the online LSVT as a tool for TR with gains in speech patterns and voice quality and loudness of speech, however as this was the only study and the population size was very small and no follow up was reported, so making any conclusions is not possible.
Strengths and imitations
One of the major limitations of this review is the small number of studies and participants and the short duration of intervention in most of the trials. In addition, different trials used different VR types (immersive, non-immersive, and custom-made) and all of them have different effects and thus could have impacted the result of our meta-analysis. Also, training time and dose, training intensity, and result evaluation indexes were all distinct in the included studies. Furthermore, none of the trials reported blinding of the participants and therapists. The intervention impact might have been influenced to some extent by the H&Y stage of people with PD which explains the variability observed in the results. The variations in the baseline values of the outcome measures of included trials might also have contributed to the observed heterogeneity. In the future, more rigorously designed research is required to assess the applicability of these novel approaches in patients with PD according to age, cognition, disease stage, and the presence of comorbidity to offer a more robust evidence-based foundation for validating the potential benefits of VR and TR.
Conclusion
The present review demonstrated that TR and VR are feasible remotely and can be used for rehabilitation in people with PD. However, the review only confirmed increased effects of VR and TR on balance, especially BBS but minimal effects of VR or TR on gait, upper limb function, speech and dysarthria, falls, neurocognitive and psychosocial aspects, incidence of falls, and global motor function. Even though the present research discovered weak evidence for TR or VR, they can still serve as adjuncts with traditional physiotherapy interventions.
Supplemental Material
Supplemental Material - Effects of remote rehabilitation with modern technologies on impairments in people with Parkinson’s disease: A systematic review and meta-analysis
Supplemental Material for Effects of remote rehabilitation with modern technologies on impairments in people with Parkinson’s disease: A systematic review and meta-analysis by Zikra Ain, Sarah Parveen, Chhavi Arora Sehgal, Md Dilshad Manzar and Majumi M Noohu in Technology and Disability
Statements and declarations
Footnotes
Authors’ contributions
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article, the study was supported by Jamia Millia Islamia, New Delhi, India.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.