
Abstract
Background
Spinal cord injury results in chronic neuropathic pain (CNP) which adds on detrimental effects on loss of function, social participation and quality of life. Various non-invasive treatments such as rTMS, TENS, tDCS and neurofeedback are available but effects of neurofeedback seem to be superior as it involves active modulation of cortical activity but its effects on pain are studied less when it is implemented using brain computer interface. Thus, this review aims to evaluate effects of neurofeedback training through EEG using Brain Computer Interface on CNP in SCI patients.
Methods
Scopus, PubMed and web of science were searched for finding the studies on the basis of inclusion criteria. Participants included were chronic CNP patients of age 18 to 75 years with at least 6 months’ history of SCI and CNP intensity >4.
Result
Total 6 studies met the inclusion criteria: 4 clinical trials, 1 usability study, and 1 pilot study. Overall risk of bias was moderate. Significant reductions in pain intensity were reported, with >30% clinical improvement in about 80% of patients, mainly linked to increased alpha band activity.
Conclusion
EEG-based neurofeedback using BCIs can reduce pain, particularly through alpha band upregulation, though further high-quality research is needed to confirm these findings.
Keywords
Introduction
Spinal cord injury (SCI) is a worldwide neurologic insult, which commonly result in severe disability with incidence ranging from 10.4 to 83 cases per million persons per year. 1 Spinal cord injury alters the regular sensory, motor, and autonomic function of the cord, either temporarily or permanently. Individuals with spinal cord injury may experience debilitating and long-lasting neurologic deficiencies. 2 SCI is often followed by complications, which add to the detrimental effect on loss of function, social participation and quality of life. 3 Patients may develop both acute and chronic complications; however its persistent effects have been found to further deteriorate patient’s functional independence and quality of life. 4
“Chronic neuropathic pain (CNP) is one of the frequent chronic complications for individuals with SCI. It is generally characterized as a burning, aching, tingling or stabbing sensation”. 4 The pooled point prevalence of neuropathic pain was reported to be 53% in SCI patients with 19% prevalence at the neurological level and 27% below the level and the rate was found to be higher in chronic patients than the acute SCI patients. 5 Neuronal hyper excitability in the spinal dorsal horn following spinal cord injury (SCI) leads to heightened pain transmission, which in turn causes an increase in neurotransmitter release, resulting in chronic neuropathic pain. 6 For individuals with SCI and their caregivers, chronic pain is a distressing comorbidity, many reporting that their symptoms have significantly decreased their quality of life. 7 For CNP, EEG bands act as both diagnostic markers, as well as cause of the complication. Increased EEG activity in the broad θ-low-α and potentially high-β bands is positively correlated with the degree of ongoing neuropathic pain. On the other hand, EEG activity in the wide high-α-low-θ range is likely to have a negative connection. 8 Pain associated changes occurring in θ band is supported by theory of thalamocortical dysrhythmia, which states that nociceptive stimulus causes a burst in the frequency of θ band at thalamus. 9 The shift in frequencies of θ-α band towards lower frequencies is considered to be the most important sign of thalamocortical dysrhythmia 10 as they are involved in various thalamocortical loops and pacemakers. 11 Also, EEG changes have been found preceding the onset of chronic pain in the sub-acute SCI indicating cause of neuropathic pain. 12
Among physiotherapy techniques, neuropathic pain has been found to have significant reduction in pain intensity through transcutaneous electrical nerve stimulation, but various other alternative therapies also appear to alleviate pain. 13 Although various non-invasive and invasive neurostimulation techniques have been used to treat neuropathic pain in SCI patients stimulating the desired cortical changes, the positive effects of invasive stimulation, such as deep brain and motor cortex stimulation using implanted electrodes in reducing neuropathic pain are limited. Non-invasive methods, such as central neuromodulation including repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS) are more appealing due to their lower risk of problems. 14 The emerging new concept of EEG bands has been found effective for treating the neuropathic pain by using it as a means of feedback in neurofeedback training. 15
EEG-based neurofeedback has the potential to alleviate central neuropathic pain (CNP) following a spinal cord injury by utilizing mental behaviours (MB) to provide intentional self-modulation of brain activity. 16 Neurofeedback training uses a single channel EEG recording in the central sensorimotor region (C4) to promote α(9–12 Hz) activities and suppress θ(4–8 Hz) and high-β(20–30 Hz) activity. 17 Though it produces extensive significant effects on several cortical structures involved in pain processing, it requires a medium such as brain computer interface to deliver a real time feedback. BCI is a newly developed method that allows the patient to receive visual and somatosensory information in real-time feedback involving cerebral activity. Through brain plasticity, BCI training may help patients with chronic neuropathic pain, enhance their quality of life, and enable them to engage in daily activities. 18 NFB has an advantage over other neurostimulation methods in that it allows patients to actively participate in treatment, shifting the focus of control from the external to the internal. As NFB training is an active process thus has high potential for treating the pain in SCI patients, however its effects after combining with brain computer interface has not yet been fully evident. 12 To the best of our knowledge, no prior systematic or scoping review has specifically evaluated EEG-based neurofeedback training using brain–computer interface (BCI) for pain management in individuals with spinal cord injury. The existing body of literature is limited to individual experimental and clinical studies, with no comprehensive synthesis addressing this focused intervention–population combination. Therefore, the present scoping review seeks to address this gap by systematically mapping and summarizing the available evidence in this emerging field
Thus, the aim of the present study is to find out the effects of EEG-based neurofeedback using brain computer interface on neuropathic pain in chronic SCI patients.
Review objectives
The objective of the present review was to examine the effects of neurofeedback training through the use of brain computer interface on modulation of pain in chronic SCI patients. The guiding research questions were: (1) Is NFB training effective in reducing pain in SCI patients? (2) How effective and efficient is BCI system for SCI patients?
Methods
The present scoping review followed the guidelines of scoping review methodology given by Arksey and O’Malley. 19 The study was done in accordance with the Preferred Reporting Items for Systematic Review and Meta – Analysis Extension for Scoping Reviews (PRISMA- ScR) checklist. 20
Eligibility criteria
In this review, the types of the studies included were clinical trials and pilot study.
Population
Patients with at least 6 months’ history of SCI and at least 3 months’ history of neuropathic pain, with age range from 18 to 75 years with no restrictions regarding the neurological level of injury were included for the study. The CNP intensity had to be equal to or greater than 4 on pain rating scale
Intervention
The studies involving neurofeedback (NFB) training using brain computer interface were included in the present review. The procedure involved the use of EEG for providing the feedback in the form of visual or auditory outputs. There was no restriction for the use of type of techniques to modulate the EEG frequencies. All the studies involving EEG modulation through predefined computer-generated techniques or patient specific modulation were included for the present study.
Comparator
The present review had no restriction regarding the comparator. All the studies were included regardless of having a control group/sham group or any other intervention.
Outcome measure
Studies having pain intensity as one of the outcome measurements were included for the review. There was no restriction on the method of assessment.
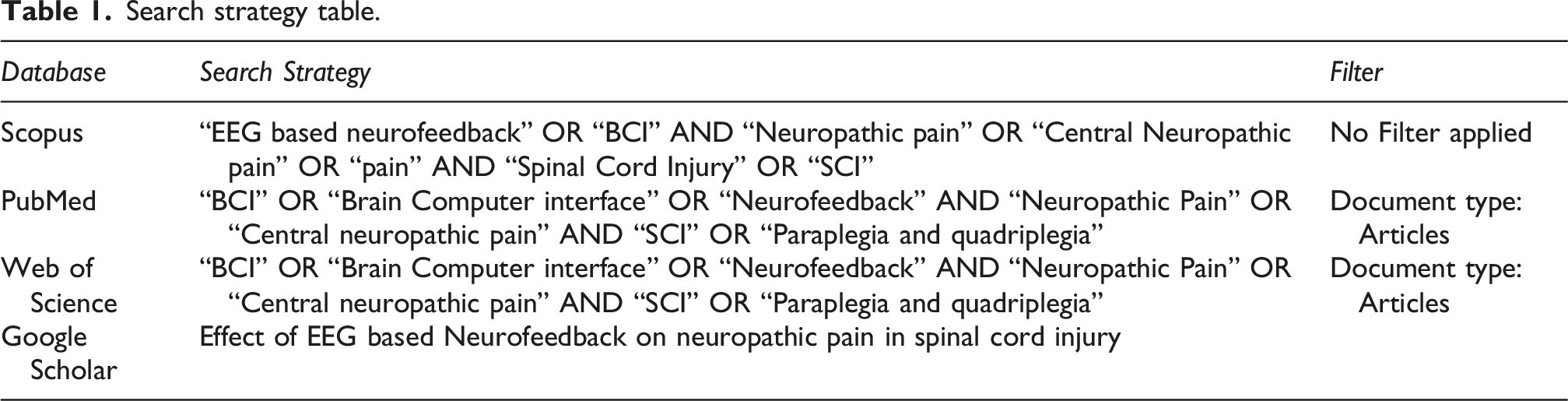
Search strategy
Search strategy table.
Study selection
End Note Classic reference management software was used to check the duplicates from the total records identified. The individual unique articles were then screened in three phases described as title screening phase, abstract screening phase and full text screening phase. 19
Title inclusion/exclusion criteria
Title must consist of neurofeedback training as an intervention with population as SCI patients. If title specifically mentioned other population such as stroke, Parkinson and other neurological conditions, those articles were excluded in the title screening phase.
Abstract or full text inclusion/exclusion criteria
In the abstract screening phase one of the outcome measurements has to be pain assessment along with the SCI population with intervention as neurofeedback using BCI. There were no restrictions on type of the paralysis and grade of spinal cord injury. Population included both paraplegic and quadriplegic patients. All grades of SCI according to ASIA grading system were included as, there were no such relationship found with degree of pain and grade of the SCI. 21
Risk of bias assessment
Evaluation for the Risk of bias will be done using Risk of bias assessment for non-randomized studies ROBINS – 1. It includes assessments of seven bias domains, which involves description of target trials and effect of interest and use of signalling questions to inform judgements of risk of bias. first two domains assess the bias due to confounding and selection of participants which together addresses the issues relating to baseline. The third domain assesses the biasness during the classification of intervention. The last four domains include issues occurring post intervention such as bias due to missing data, deviations from intended interventions, measurement of outcomes and deviations in selection of reported results. 22 For randomized studies ROB-2 will be used.
Results
Literature search
After all the screening process 6 studies were selected for present scoping review. Initially exploring all the databases yielded 749 results in which, 278 articles from web of science, 458 from PubMed and 13 studies were from Scopus. 124 studies were removed as duplicates. After duplicate removal 625 studies were screened. In title screening 588 studies were removed as they consist of populations other than the SCI such as stroke, Parkinson, and ADHD. After title screening 37 articles were assessed for the eligibility in which only 6 studies fulfilled the eligibility criteria which were included for the present review. PRISMA flow diagram is represented in Figure 1. PRISMA flow chart.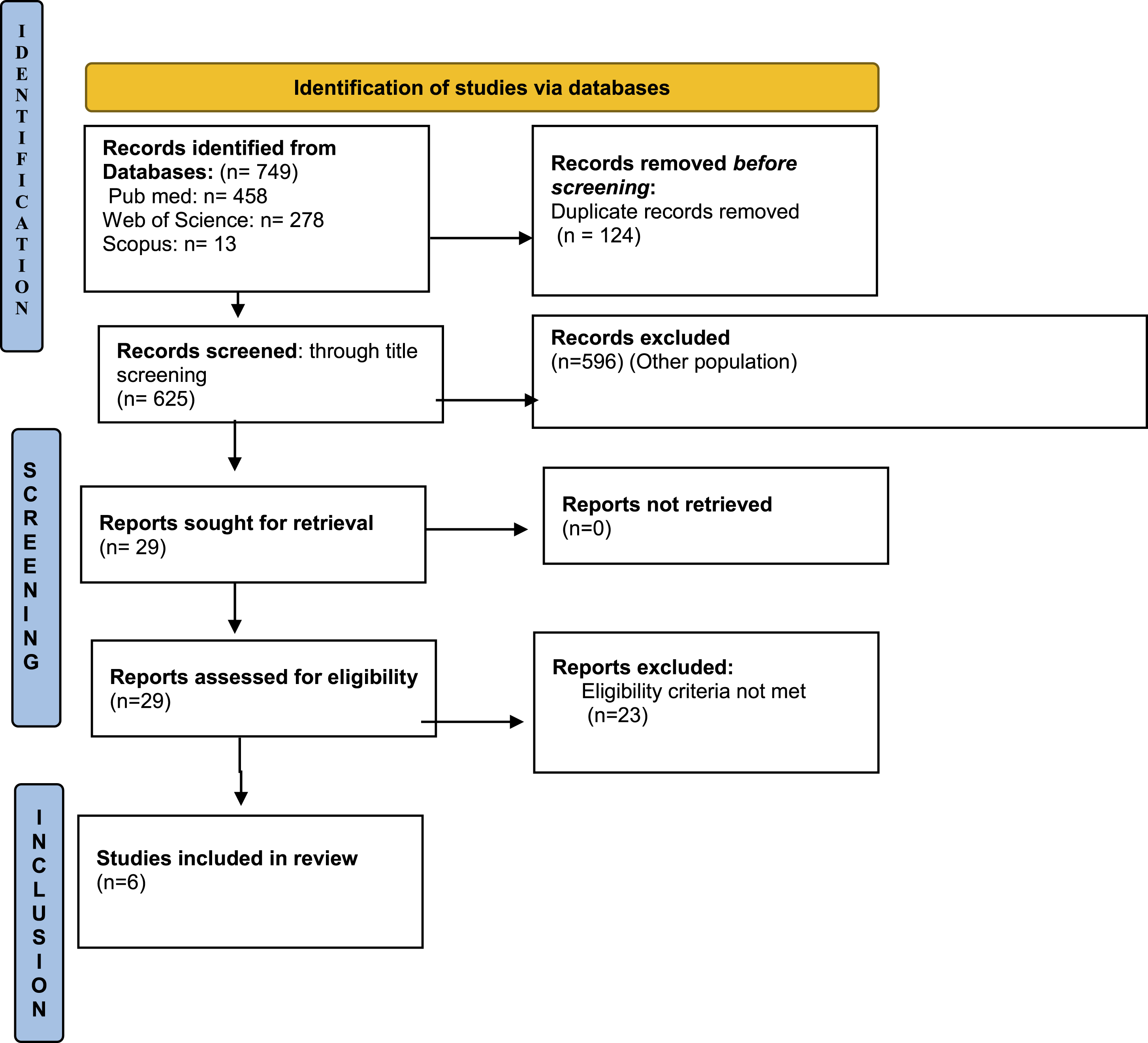
Characteristics of the studies
Characteristics table.
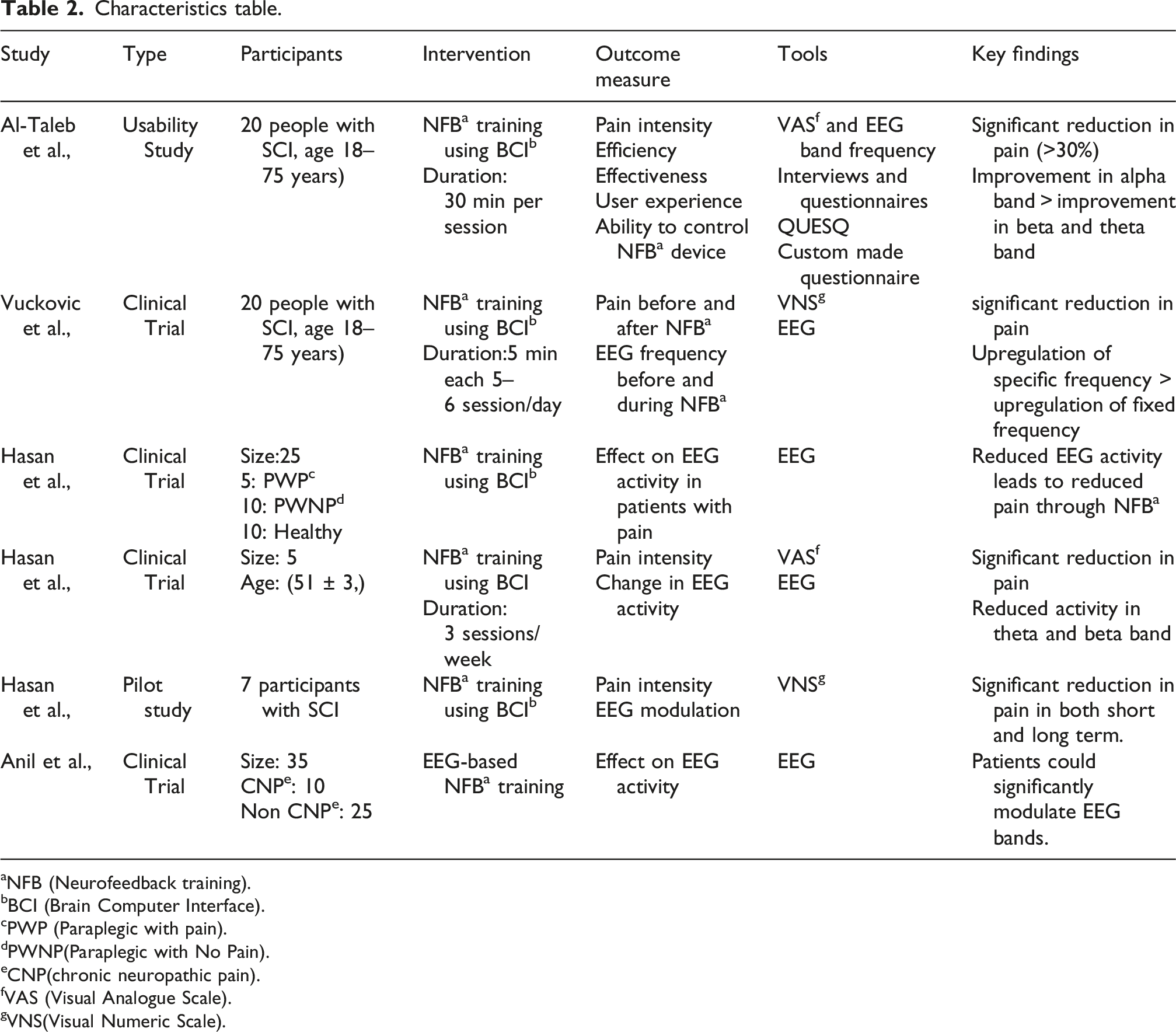
aNFB (Neurofeedback training).
bBCI (Brain Computer Interface).
cPWP (Paraplegic with pain).
dPWNP(Paraplegic with No Pain).
eCNP(chronic neuropathic pain).
fVAS (Visual Analogue Scale).
gVNS(Visual Numeric Scale).
Participants
This review included total 87 participants. All the participants in included studies were diagnosed with chronic SCI with duration of injury as at least 6 months. Two studies had participants in the age range of 18–75 years,12,23 three studies included participants with age range 40 years to 60 years10,17,24 and one study included participant with at least 18 years. 16 Based on the neurological level of injury 3 studies included paraplegic patients,10,17,24 whereas two studies included both paraplegic and quadriplegic patients with paraplegic > quadriplegic.12,23 All the studies had patients with ASIA grading as A, B, and D. None of the study had ASIA grade C, however one of the studies did not mention about the neurological level of injury and ASIA grading. 16
Intervention
In all studies included in the review, intervention given was EEG-based neurofeedback training using BCI where participants had to modulate the activity of EEG bands. In the included studies, the tasks were either closed that is neurofeedback tasks were set by the researcher or were opened that is outcome tasks was freely set by the patients. In two studies tasks were set to upregulate alpha bands to 9-12 Hz and downregulate beta and theta frequencies to 20-30 Hz and 4-8 Hz, respectively,16,17 whereas in other studies patients were freely allowed to regulate EEG frequencies.
Comparator
Four studies gave the intervention individually to the participants with no comparator group.10,12,17,23 Two studies compared the intervention group with SCI patients with the non-CNP group.16,24
Outcome measure
All the studies had “pain intensity” as an outcome measure. In 4 studies it was measured using visual analogue scale or visual numerical scale12,17,23,24 and in two studies pain was correlated with EEG analysis.16,24 Other outcome measurement includes efficacy, safety and effectiveness of the brain computer interface.
Assessment of risk of bias
Risk of bias assessment findings are given in Figure 2(a) and (b). The overall risk of bias was moderate except one study having high concerns.
12
In domain 1, which assess bias due to confounding, the risk was moderate in 3 studies10,16,17 and low in other three studies.12,23,24 In domain 2 and 7 which assess bias due to selection of participants and bias in selection of reported results respectively, the risk of bias was moderate in 80% of the study, whereas only one study reported low risk of bias.
17
In domain 3, which assess bias in classification of intervention, the risk was found to be moderate in 80% of studies with one study having high concerns.
12
Risk of bias was moderate in domain 4, which assess bias due to deviation from intended intervention. In domains 5 and 6, assessing bias due to missing data and bias in measurements of outcomes respectively, the results were found to be mixed with high concerns in one study in both the domains.
12
The risk was low in 3 studies10,16,23 in domain 5, whereas in domain 6, four studies had low risk.10,17,23,24 The risk was moderate in two studies in domain 5,17,24 whereas in domain 6 moderate risk was found in only one study.
16
(a) ROBINS plot graph; (b) ROBINS summary graph.
Effects of NFB on pain
The 6 studies recruited for this review, measured the pain directly through pain scales or by correlation with EEG band frequencies. Four studies evaluated pain using visual numerical scale10,12,17,23 and other two studies correlated pain with parameters of EEG.16,24
Two studies have reported significant reduction in pain intensity in 80% of participants with clinically significant results (>30%) in 8 participants.12,23 One study reported that pain reduction was statistically significant only during NFB training when compared to post training. It reported 2 patients with 30% improvement, 1 with 20% and 2 with 10% on visual Analogue Scale (VAS). 17 One study reported significant reduction in pain in 5 out of 7 patients and these patients received more than 20 sessions. 6 out of 7 patients had shown immediate reduction in pain intensity while all patients had long term reduction in pain but it was found to be very gradual. 10
One study compared the CNP with non-CNP participants and reported successful and unsuccessful participants for both groups individually. Successful CNP participants significantly upregulated the theta and alpha bands whereas successful non-CNP participants significantly upregulated only alpha band. Unsuccessful participants in both CNP and non-CNP groups did not have significant differences. 16 One of the studies has reported the cortical changes relating to pain in terms of Event related synchronization/desynchronization ratio (ERS/ERD). In all the patient’s reduction in alpha and beta ERD was reported after the neurofeedback training which relates to the reduction of pain 24.
EEG bands modulation
All of the included studies focused on upregulating the alpha band and downregulating the beta and theta bands. Though results were found to be variable, in most studies upregulation of alpha band was superior than the beta and theta bands.
In one of the studies, 10 patients upregulated the alpha band while only 5 participants were able to downregulate theta and beta bands.
12
Another study reported that patients were able to significantly upregulate alpha bands only when frequencies were participants specific. Twelve out of 15 participants upregulated alpha band, 10 people downregulated theta band and only 7 participants upregulated beta bands. When frequencies were fixed only 3 participants increased the alpha band frequency and 9 decreased the beta and theta band frequency.
23
Results of these two studies are presented in Figure 3. EEG frequency modulation graph.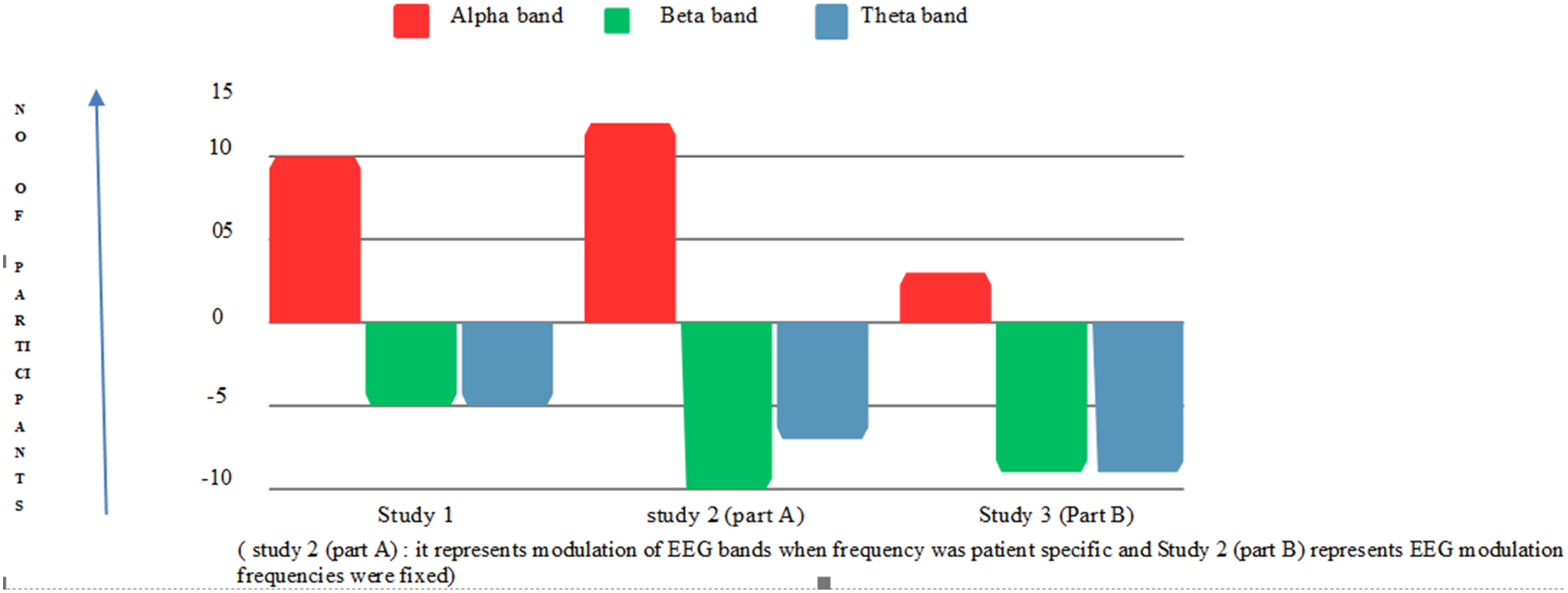
Discussion
This review aimed at examining the effects of neurofeedback training using brain computer interface on chronic pain in spinal cord injury patients. Total 6 studies were included which measured pain either directly through pain rating scales or indirectly correlating with change in EEG frequencies. This review found that NFB training using BCI can significantly reduce pain intensity with greater immediate effects rather than long term effects by upregulating the frequency of alpha band power and downregulating the theta and beta frequencies. NFB training has been found to reduce pain perception in SCI population.
In the present review direct effects on pain intensity were observed due to neurofeedback training with clinically significant improvements (>30%) in two studies.12,23 Similar positive effects have been seen earlier in various population. In a study by Birch and colleagues, in adults with chronic pain, home-based NFB training reduced VNS pain scores in 11 (69%) of the participants and 50% of them had a clinically significant drop in pain intensity of at least 30% that persisted until the 12-week follow-up. 25 Another study by Wu and colleagues on fibromyalgia also showed noticeably larger decrement in pain severity. 26 A study by Jensen and colleagues reported clinically significant reduction of pain intensity in complex regional pain syndrome, which occurred due to ability of NFB training to influence central regulation of pain by provoking cerebral networks to alter their relative timing relationship to promote renormalization of function. 27 The reduction in pain intensity has also been linked to decrease in the thalamocortical dysrhythmia (TCD), which is the underlying cause of several neurological conditions, including neuropathic pain.9,28 TCD is believed to result from excessive inhibition or disaffiliation of thalamic neurons, which causes hyperpolarization of these cells. Low-threshold calcium spike bursts caused by hyperpolarization of these cells result in extensive coherent slow-wave activity that propels thalamocortical modules during these rhythms. 29 Thus it has been found that in SCI population a slowing of the EEG towards the theta frequency range is linked to neuropathic pain in SCI, which is consistent with the possible occurrence of TCD in this population. 30 The reduction in pain intensity can be attributed to the active process of neurofeedback in modulating pain as it utilizes the real time feedback through EEG. 31
It has been seen that chronic pain perception is associated with various changes in frequency of EEG bands (alpha, beta and theta) 32 and NFB training with real time EEG has found to modulate these targeted maladaptive EEG frequency processes to reduce pain. 33 In present review most of the studies upregulated the alpha frequency band and downregulated the beta and theta frequency band for modulating the pain perception.12,23 A study by Barbosa-Torres & Cubo-Delgado, also reported the significant improvements in pain perception due to neurofeedback training and found that it can facilitate the inhibitory mechanisms of cerebral cortex, which could be connected to the increased perception of pain in fibromyalgia patients. 34 Inhibitory mechanism of the central system is influenced by various sensory inputs as similar brain structures are responsible for sensing and channelling of audio, visual, smell, taste and tactile stimuli, thus dampening the transmission of information of all sensory signals, especially pain, thus effective in reducing chronic pain symptoms
Pain was significantly reduced during the training only and had effects for shorter duration,10,17 this could be due to patient’s preference of taking the NFB sessions only when their pain was ongoing, and not continuing the treatment on the regular basis. 17 Long term effects were seen only when treatment duration was longer which results in decreased sensory – motor cortex activity 24 to the homeostatic points or closer to the activity of abled bodied of spinal cord injury without pain. 35 Decrease in sensory - motor cortex activity was represented by event related desynchronization (ERD) and has been found to be reduced mostly at frontal and parietal – occipital area. 24
In contrast to positive results of NFB on pain, one study by Jensen and colleagues, found no clinically significant and no immediate effects on pain reduction in SCI population, as minor variations in protocols, such as the choice of scalp sites for training, may not significantly influence immediate treatment outcomes. 15
The studies included in the present review highlighted the use of brain computer interface in home-based settings. The participants had minimal level of stress while using BCI at home with high level of efficiency and efficacy. In the home-based setting the recorded data was noisy only 10 to 15% which could enhance the adherence in the participants. 12
Though results were found to be significant but most of the studies had small sample size with approximately 30% dropouts, reducing the generalizability of the results. Another limitation is that none of the studies could be performed with randomized controlled design which decrease methodological rigour of the study. Only one study used patient selected frequency modulation and other studies used fixed ranges of frequency modulation which could have modulated the results. Thus, more studies are required to examine the effects of NFB using BCI on neuropathic pain and mechanism behind the reduction of pain. As minor variations in protocols, such as the choice of scalp sites for training, may not significantly influence immediate treatment outcomes, thus it holds a critical relevance for clinical decision-making in selecting NF training protocols for managing SCI-related pain and highlight the need for further research to refine and optimize these approaches.
Conclusion
In conclusion, the findings indicate that the, NFB substantially decreased pain, mostly via altering EEG frequencies and upregulating alpha band activity. However, as the overall certainty and reliability of the evidence remain limited due to moderate risk of bias among the included studies; further high-quality, rigorously designed studies with large sample sizes and standardized protocols are required to strengthen the current evidence. Future research should also focus on exploring long-term effects of BCI-based neurofeedback, optimizing intervention protocols and exploring the underlying mechanisms responsible for pain reduction. Additionally, comparative studies examining different neurofeedback paradigms and intervention intensities may help enhance the clinical applicability of these interventions.
Footnotes
Acknowledgements
We acknowledge Centre for Physiotherapy and Rehabilitation Sciences, Jamia Millia Islamia for their support in conducting this review.
CRediT author statement
Conceptualization, Methodology, writing original draft:
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.