
Abstract
Objectives
To assess the clinical and radiographic outcomes of segmental two-piece Le Fort I osteotomy in patients with cleft lip and palate (CLP) with residual alveolar clefts.
Design
This retrospective case series assessed the occlusal outcomes after Le Fort I osteotomy, and radiographic alveolar continuity using cone-beam computed tomography (CBCT).
Setting
Tertiary cleft and craniofacial center within an academic institution.
Patients/Participants
Patients aged ≥12 years with unilateral cleft lip and palate (UCLP) who presented with an anterior crossbite and residual alveolar defect and underwent orthodontic treatment and Le Fort I osteotomy between 2019 and 2025.
Interventions
Four patients with UCLP underwent pre-surgical orthodontic treatment to prepare for orthognathic surgery. Extractions were performed to correct crowding and/or dental impactions. Patients then underwent Le Fort I osteotomies to correct the anterior crossbite and close the cleft gap.
Main Outcome Measures
Correction of dental malocclusion and assessment of alveolar bone support of the residual alveolar cleft following segmental two-piece Le Fort I osteotomy.
Results
In all cases, anterior crossbite was corrected to positive overjet with normal overbite. Results were well accepted by all patients. Size of cleft defects was reduced with radiographic evidence of osseous continuity. The need for prosthodontic replacement teeth was eliminated in each case.
Conclusions
All four patients who underwent orthodontic treatment and segmental two-piece Le Fort I osteotomy resulted in corrected the anterior crossbite and closure of the cleft gap. Patients underwent several extractions to ensure that the remaining teeth were centered in alveolar bone, and their final occlusion was functional and stable.
Introduction
Cleft lip and palate (CLP) is the most common congenital craniofacial anomaly, with a prevalence of approximately one in 700 live births. 1 Restoration of alveolar continuity is a critical component of the cleft treatment pathway and is typically achieved through secondary alveolar bone grafting (ABG). The ideal age for secondary ABG remains a topic of debate, with many advocating for early grafting between ages 4 and 6, over the conventional ages 9 through 12, to allow for central and lateral incisor eruption through the grafted bone.2–4 Successful secondary ABG allows for proper eruption of the cleft-adjacent teeth through alveolar bone and stability of these teeth as occlusion is optimized. 5 However, reported success rates for secondary ABG range widely from approximately 30% to 96%.6–10 Furthermore, a substantial subset of patients requires revision ABG, with reported failure rates of around 20%, particularly in the setting of wide clefts, bilateral deformities, or the presence of erupted teeth in the cleft area. 11 Despite multiple grafting attempts, some patients progress into adulthood with a persistent alveolar cleft defect.
Residual alveolar clefts in adult patients are associated with a distinct set of dental and skeletal sequelae. In the setting of a hypoplastic maxilla and limited alveolar bone, cleft adjacent teeth demonstrate abnormal angulation, ectopic positioning, or impaction.12–14 These abnormalities often result in regions of alveolar bone that lack functional tooth support, predisposing the maxilla to progressive bone resorption over time. 15 Angulated teeth are biomechanically suboptimal for mastication and occlusal stability, while impacted teeth may require extraction, further exacerbating alveolar bone loss if the remaining dentition cannot adequately occupy the available space.16,17
Segmental two-piece Le Fort I osteotomy has been previously described as a surgical strategy to address complex maxillary deformities in patients with CLP. Posnick and colleagues first introduced this modification of the Le Fort I osteotomy for simultaneous correction of maxillary hypoplasia and alveolar cleft defect.18,19 Segmental two-piece Le Fort I osteotomy advances the maxilla and separates the right and left maxillary segments through the alveolar cleft. These segments are then approximated relative to one another to minimize the gap, and bone grafting is used to fill the residual defect. In contrast to traditional revision secondary or tertiary ABG, segmental two-piece Le Fort I osteotomy brings the alveolar segments together, reducing the cleft width and improving the predictability of bone grafting. It also eliminates the need for lateral incisor replacement, and thus also obviates the need to contend with the unpredictability of implant survival in the cleft gap.20,21
While segmental two-piece Le Fort I osteotomy has been reported in the context of maxillary hypoplasia and transverse deficiency, its specific role in managing residual alveolar clefts following failed bone grafting has not been well characterized. The purpose of this study was to evaluate occlusal and radiographic outcomes following segmental two-piece Le Fort I osteotomy in adolescent patients with CLP and a persistent alveolar cleft after prior secondary ABG. Specifically, we sought to assess postoperative alveolar continuity and characterize associated changes in dental occlusion.
Methods
This IRB-approved retrospective case series was conducted at a tertiary cleft and craniofacial center and included patients with unilateral CLP who underwent segmental two-piece Le Fort I osteotomy as part of their clinical care. Patients were identified through review of institutional surgical logs and clinical records between 2019 and 2025. Inclusion criteria were as follows: a confirmed diagnosis of unilateral CLP, a persistent alveolar cleft following prior secondary ABG, the presence of an anterior crossbite requiring surgical maxillary advancement, and availability of both preoperative and postoperative cone beam computer tomography (CBCT) imaging. Patients were excluded if they had syndromic clefts associated with atypical craniofacial or dental development, if imaging lacked adequate field of view or image quality to assess alveolar continuity and adjacent dentition, or if operative documentation was insufficient to confirm the indication for segmental maxillary osteotomy.
All CBCT scans were reviewed in Dolphin Imaging 12.0 by a craniofacial orthodontist experienced in cleft dental assessment. Demographic variables collected included age at surgery, age at secondary ABG, sex, and cleft laterality. Radiographic variables recorded included presence of a residual alveolar cleft on preoperative imaging and degree of alveolar cleft closure on postoperative imaging. For volumetric analysis, cleft width was defined as the linear distance between the medial and lateral margins of the cleft at its widest portion. Bone volume was measured using the volume sculpting tool in Dolphin software. The superior boundary was the nasal floor of the non-cleft side, inferior boundary was the marginal portion of the alveolar ridge, and lateral boundaries were the cleft-adjacent teeth (Figure 1). Alveolar continuity was defined radiographically as uninterrupted bone bridging across the prior cleft site on postoperative imaging. Dental alignment and occlusion were assessed based on tooth positioning, sequence, and inter-arch relationships.
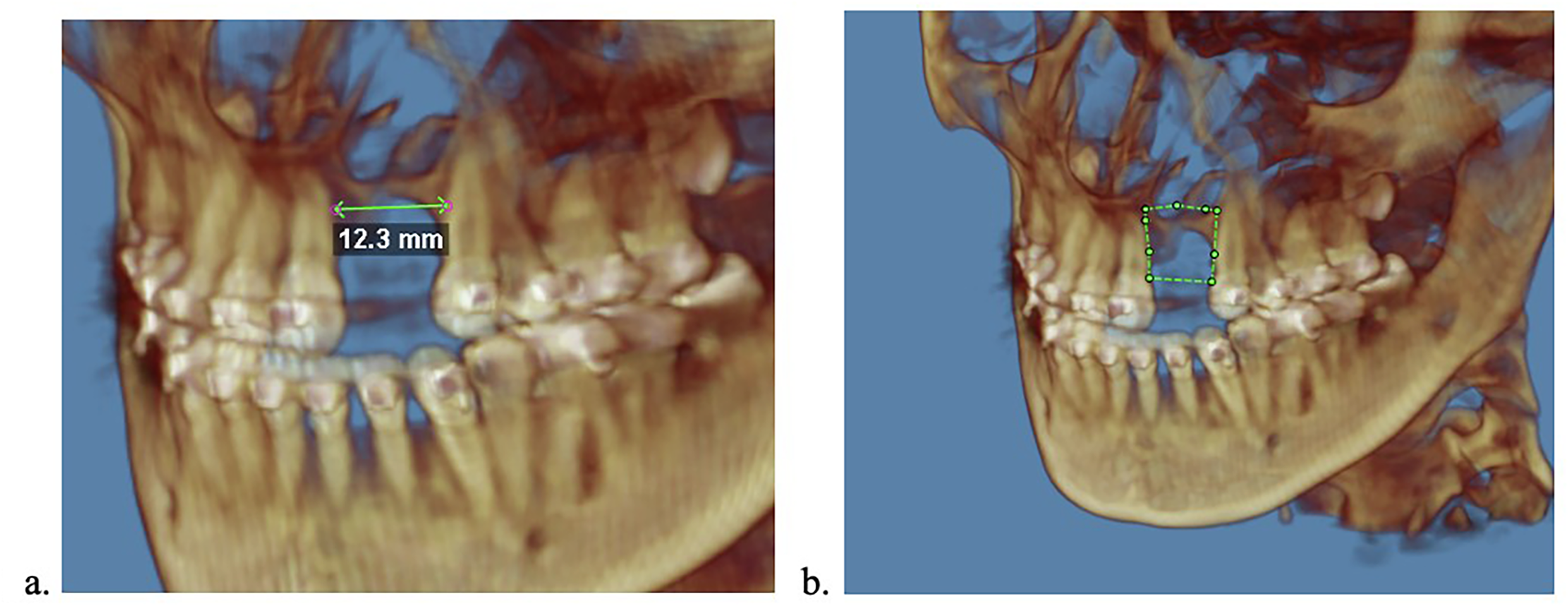
(a) Cleft width defined as the distance between the medial and lateral cleft margins. (b) Bone volume measured with the superior boundary as the nasal floor, inferior boundary as the marginal portion of the alveolar ridge, and lateral boundaries as the cleft-adjacent teeth.
The primary outcome measures included correction of the dental malocclusion and prevalence of radiographic closure of the residual alveolar cleft following segmental two-piece Le Fort I osteotomy.
Operative Technique
All segmental two-piece Le Fort I osteotomies were performed under general anesthesia with nasotracheal intubation. Intravenous prophylactic cefazolin and tranexamic acid (TXA) were administered at induction of anesthesia. Bilateral regional pterygopalatine blocks were performed using 0.25% bupivacaine with epinephrine.
Segmental two-piece Le Fort I osteotomies were performed for correction of maxillary hypoplasia and closure of residual alveolar cleft. Bovie electrocautery was used to make the maxillary buccal vestibular incision, and full thickness mucoperiosteal flaps were elevated over the entire maxilla. Dissection was carried posteriorly toward the pterygomaxillary region, allowing complete mobilization of the maxilla. A reciprocating saw was used to complete a standard Le Fort I osteotomy bilaterally. The nasal septum was separated, and pterygomaxillary disjunction was performed using osteotomes, followed by gentle down fracture of the maxilla. Palatal dissection was then performed between the greater and lesser maxillary segments, allowing mobilization of the maxilla into two segments.
Following segmentation, the palatal and nasal mucosa were carefully mobilized, and any associated palatal fistulae were repaired with layered closure as indicated. Either autogenous iliac bone grafting or cryopreserved allograft was placed into the alveolar cleft gap at the site of segmentation. The maxillary segments were repositioned into the planned occlusion using temporary occlusal splints, and temporary maxillomandibular fixation was applied to maintain alignment. Definitive internal fixation was achieved using titanium plates along the medial and lateral maxillary buttresses.
Results
A total of four patients met inclusion criteria, including three patients with left-sided UCLP (75%) and one patient with right-sided UCLP (25%). The mean age at the time of surgery was 16.3 years (range = 15–18) and 75% (n = 3) of the cohort was female. Prior secondary ABG was performed in all patients. All patients were satisfied and declined additional esthetic dental procedures such as bonding, veneers, or gingivectomy. There were no complications to report.
Case Reports
Case 1 (BT)
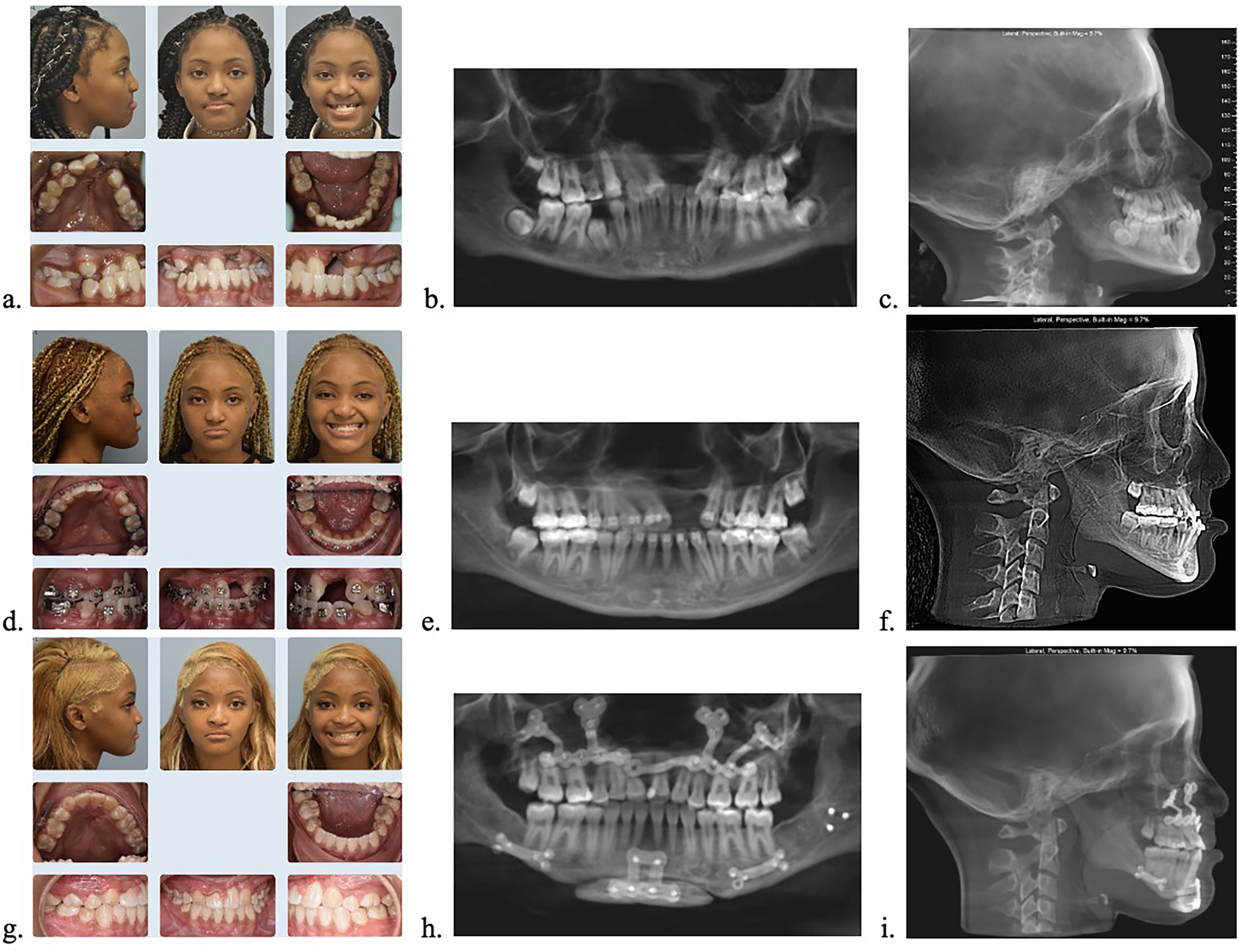
A 13-year-old female presented to an outside orthodontist with a history of right-sided complete UCLP and left-sided cleft lip (CL) with associated maxillary hypoplasia and anterior crossbite. Clinical and radiographic evaluation demonstrated missing permanent maxillary right and left lateral incisors, an ectopic and impacted permanent maxillary right canine adjacent to the alveolar cleft, severe dental crowding, and maxillary midline deviation to the right side. Additionally, there was marked paucity of alveolar bone at the cleft site with an absence of a bony bridge. The patient initiated orthodontic treatment, which included extraction of the mandibular right and left first premolars in an attempt to correct the anterior crossbite, as well as exposure of the maxillary right canine. The patient then transferred to our clinic. Due to crowding, the maxillary left first premolar was extracted. The ectopic canine was determined to have a poor prognosis due to inadequate bony support and limited potential for orthodontic alignment within the dental arch. Additionally, the patient still did not have adequate overjet and had an anterior open bite. Therefore, a segmental two-piece Le Fort I maxillary advancement was planned to close the cleft-associated dental gap and correct the anterior crossbite, open bite, and midline deviation. Presurgical orthodontics was performed, and then the patient underwent a segmental two-piece Le Fort I maxillary advancement with simultaneous extraction of the ectopic maxillary right canine. Autogenous iliac crest bone grafting was used to close the dental gap. The canine was not extracted prior to surgery in order to avoid additional bone loss. The patient then completed post-surgical orthodontic treatment and had mild cosmetic enameloplasty on the maxillary right premolar and left canine, which were in the lateral incisor positions. At the end of the patient's treatment, she had 10 maxillary teeth due to the missing maxillary lateral incisors and extracted maxillary right canine and left first premolar. Her final dental complement and sequence were unconventional, but her result was functional and esthetic. In fact, the patient was satisfied with her appearance and declined periodontal recontouring or prosthodontic veneers or crowns to reshape her teeth. Additionally, radiographic evaluation 10 months post-surgery indicated complete osseous continuity in the cleft. Furthermore, 2-year follow-up indicated that the occlusal results were stable (Figure 2). Pre- and postoperative bone volume were 46.21 and 600.88 mm3, respectively. Pre- and postoperative cleft width were 10.5 and 2.4 mm, respectively.
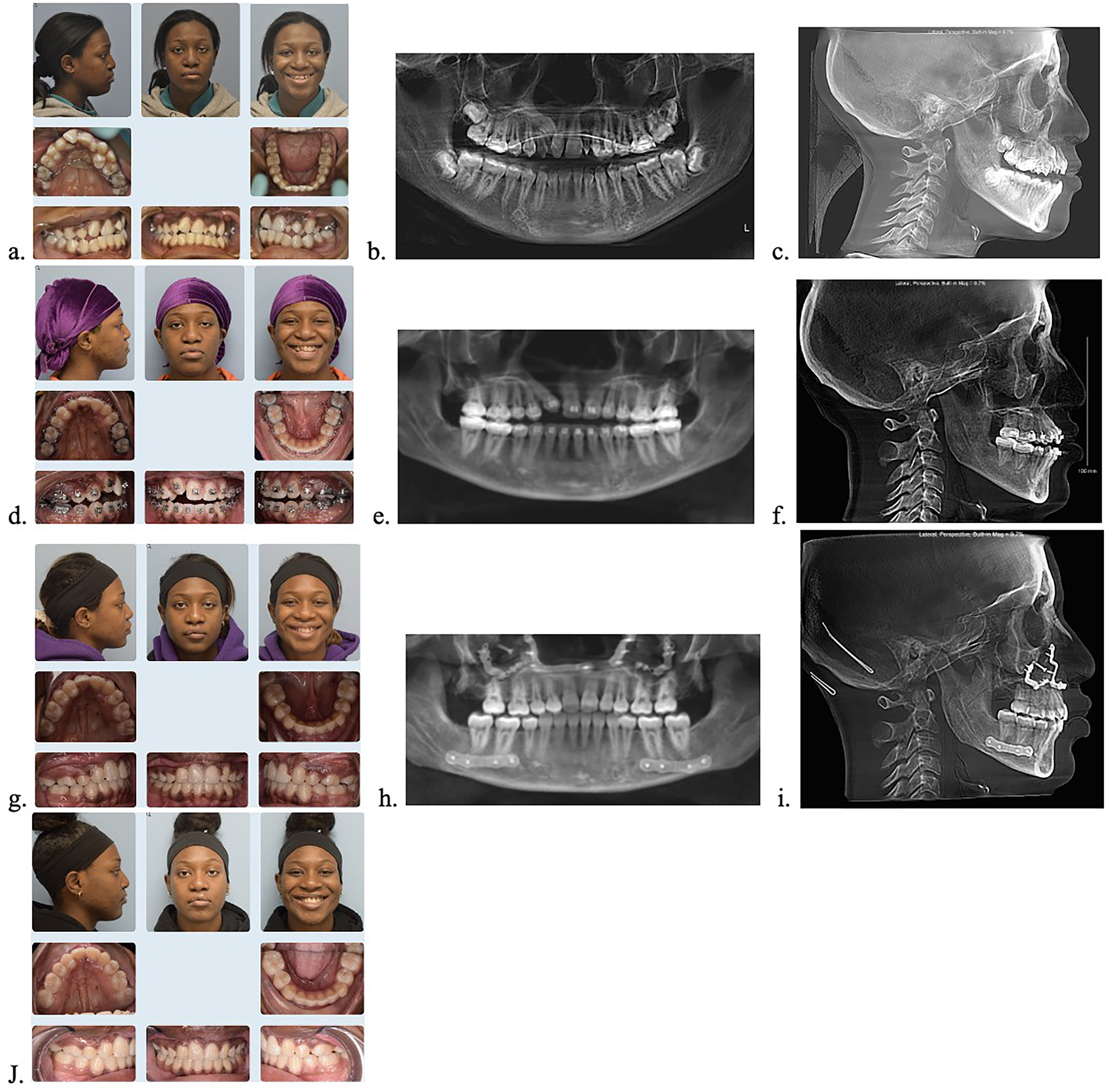
(a) Initial visit (T1) photo montage, note severe crowding and impacted maxillary right canine, (b) T1 CBCT, (c) T1 lateral cephalometric radiograph, (d) Progress report (T2) photo montage, note inadequate overjet, anterior open bite, and alveolar cleft gap with absence of bony bridge, (e) T2 CBCT, (f) T2 lateral cephalometric radiograph, (g) Ten-months post-op (T3) photo montage, note unconventional dental complement with adequate occlusion, positive overbite and overjet, and bony bridge present in cleft, (h) T3 CBCT, (i) T3 lateral cephalometric radiograph, (j) Two-years post-op (T4).
Case 2 (CB)
A 13-year-old male with a left-sided UCLP presented for phase II orthodontic treatment after undergoing phase I orthodontics and secondary ABG. Clinical examination and radiographic imaging revealed an anterior crossbite with associated maxillary hypoplasia, maxillary crowding in right and left quadrants, a compromised permanent maxillary right lateral incisor, impacted permanent maxillary left canine, and missing permanent maxillary left lateral incisor. Additionally, while previous ABG successfully corrected the oronasal fistula and provided adequate soft-tissue support, radiographic assessment demonstrated a residual alveolar defect without sufficient bone to support tooth movement. The maxillary crowding was corrected with extractions of the permanent maxillary right lateral incisor and left canine, followed by orthodontic braces to align the remaining dentition. Care was taken to avoid moving teeth into the residual cleft alveolar defect. A segmental two-piece Le Fort I osteotomy was then performed to facilitate closure of the residual dental gap and to correct the anterior crossbite. ViviGen bone graft was used to close the dental gap. After surgery and post-surgical orthodontic treatment were completed, the patient had optimal overbite and overjet despite missing three maxillary teeth. On the right side, he had canine substitution of the maxillary lateral incisor, and on the left side, he had premolars in the maxillary lateral incisor and canine positions. His occlusion was functional and stable at 1-year post-debond. There was slight paucity of bone in the cleft area, however, adequate bone was present to support the adjacent teeth (Figure 3). Pre- and postoperative bone volume were 148.54 and 387.61 mm3, respectively. Pre- and postoperative cleft width were 3.0 and 2.0 mm, respectively.
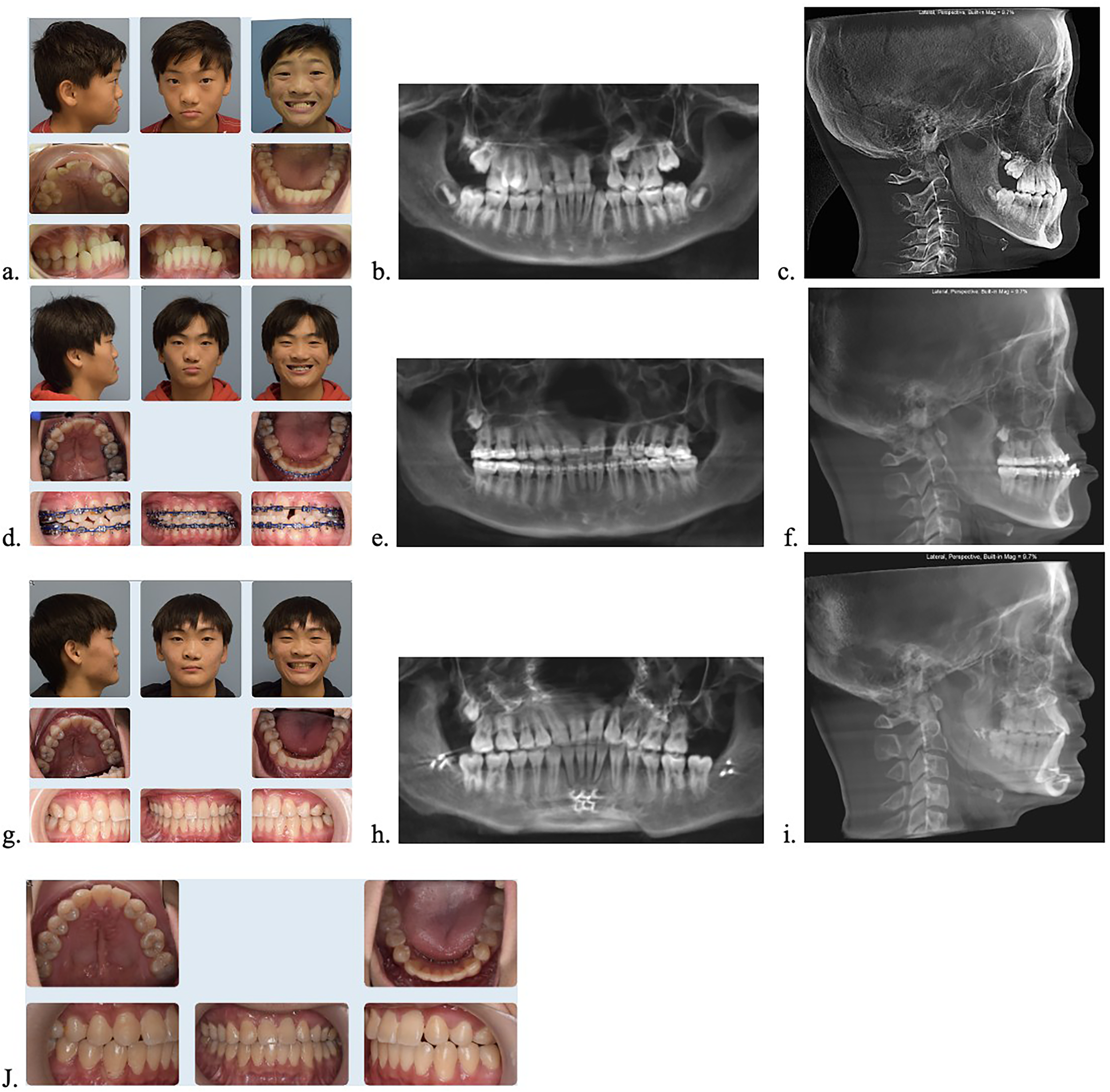
(a) Initial visit (T1) photo montage, note anterior crossbite, maxillary crowding in right and left quadrants, compromised permanent maxillary right lateral incisor, impacted permanent maxillary left canine, alveolar defect, (b) T1 CBCT, (c) T1 lateral cephalometric radiograph, (d) Progress report (T2) photo montage, note maxillary teeth were not moved into the alveolar defect, (e) T2 CBCT, (f) T2 lateral cephalometric radiograph, (g) Five-months post-op (T3) photo montage, note the maxillary left lateral incisor space was closed surgically, optimal overbite and overjet despite missing 3 maxillary teeth; slight paucity present in cleft area, however, adequate bone present to support adjacent teeth, (h) T3 CBCT, (i) T3 lateral cephalometric radiograph, (j) One and half years post-op (T4).
Case 3 (SS)
A 14-year-old female presented for phase-II orthodontic treatment with a history of left-sided UCLP with an anterior crossbite due to maxillary hypoplasia, missing maxillary right and left lateral incisors, transposed maxillary right canine and first premolar, missing maxillary right second premolar, and maxillary left crowding. Additionally, she had an edentulous space in the maxillary arch due to absence of a lateral incisor and a residual alveolar cleft defect. The maxillary left second premolar was extracted to alleviate crowding and to facilitate alignment of the remaining teeth in the maxillary left segment within alveolar bone. Orthodontic treatment with fixed orthodontic appliances was performed, and a segmental two-piece Le Fort I osteotomy was performed to close the cleft-associated dental gap and correct the anterior crossbite. ViviGen bone graft was used to close the dental gap. Post-surgical orthodontics was then completed, and final records demonstrate that the anterior crossbite was successfully corrected, the cleft gap was closed, and there is a solid bony bridge in cleft area. This patient finished treatment with an unconventional dental complement, due to missing teeth and the dental transposition. However, her overbite and overjet were optimal, her occlusion was functional, and she was satisfied with her appearance (Figure 4). Pre- and postoperative bone volume were 51.17 and 440.03 mm3, respectively. Pre- and postoperative cleft width were 6.6 and 4.2 mm, respectively.
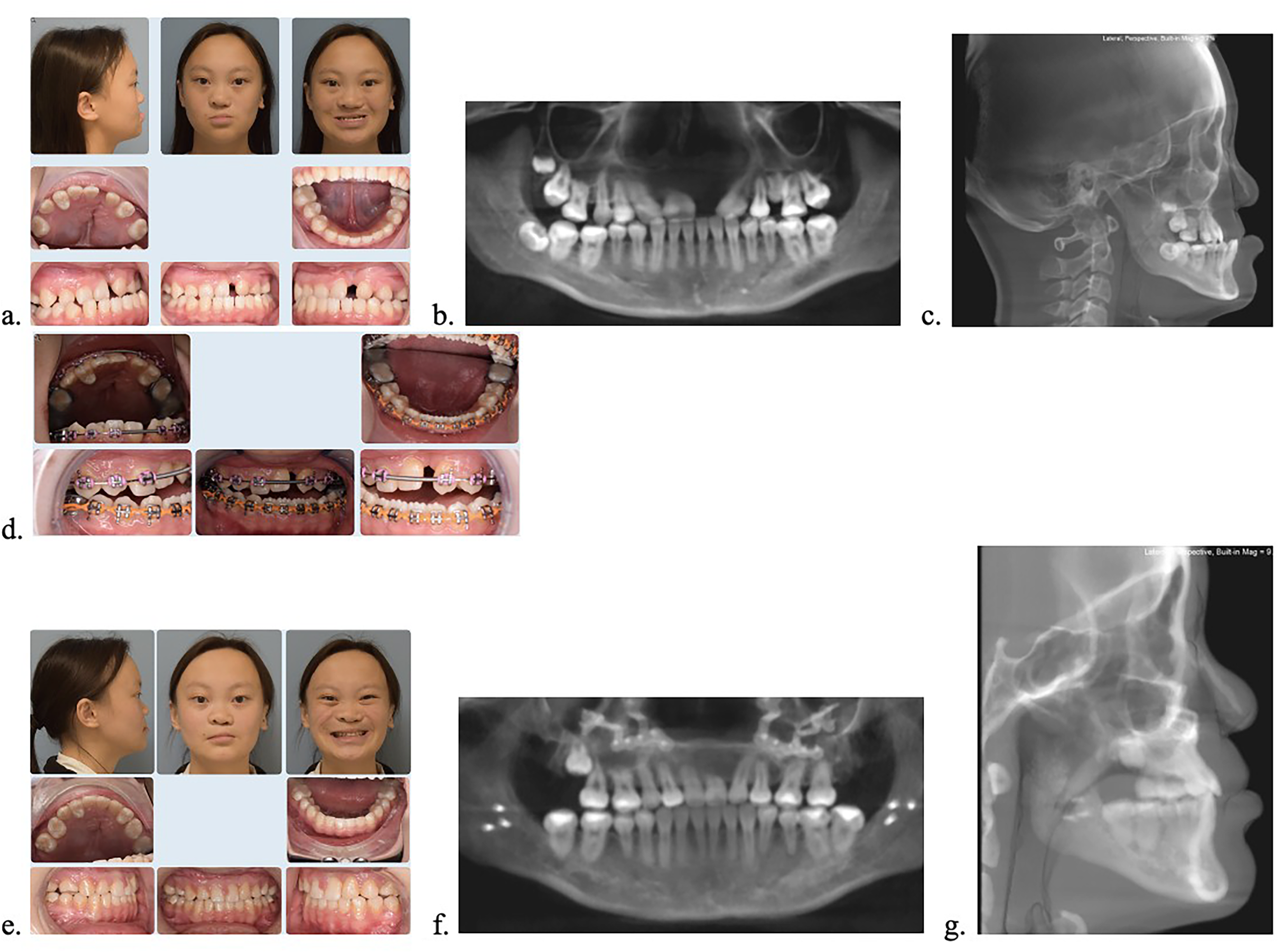
(a) Initial visit prior to treatment (T1) photo montage, note anterior crossbite due to maxillary hypoplasia, missing maxillary right and left lateral incisors, transposed maxillary right canine and first premolar, missing maxillary right second premolar, maxillary left crowding, residual alveolar cleft defect, (b) T1 CBCT, (c) T1 lateral cephalometric radiograph, (d) Presentation to cleft clinic (T2) photo montage, note root of the maxillary left central incisor was short, so a bracket was left off of the tooth as long as possible to avoid further root resorption, (e) One and half years post-op (T3) photo montage, note Cleft gap was closed surgically, and CBCT demonstrates bony bridge in cleft area, (f) T3 CBCT, and (g) T3 lateral cephalometric radiograph.
Case 4 (SB)
An 11-year-old female presented with a history of left-sided CLP. Clinical examination demonstrated maxillary hypoplasia with an anterior crossbite, missing maxillary right and left lateral incisors and second premolars, and a large edentulous area in maxillary lateral incisor space with paucity in the alveolar bone. Additionally, the maxillary dental midline was deviated to the non-cleft (right) side relative to the facial midline. After multidisciplinary assessment, presurgical orthodontic management involving a maxillary palatal expander and braces was initiated. Extractions of the primary maxillary right and left second molars and mandibular right and left first premolars were performed, and spaces were closed. Care was taken to avoid moving teeth into the cleft alveolar defect. Segmental two-piece Le Fort I osteotomy was then performed to advance the maxilla into positive overjet, close the cleft-associated dental gap and residual alveolar defect, and correct maxillary asymmetry. ViviGen bone graft was used to close the dental gap. After surgery, the patient overbite and overjet were improved, and there was closure of the cleft dental gap. Slight alveolar paucity was present in cleft area, however adequate bone was present to support adjacent teeth (Figure 5). Pre- and postoperative bone volume were 970.11 and 615.65 mm3, respectively. Pre- and postoperative cleft width were 12.3 and 1.5 mm, respectively. The decrease in bone volume postoperative can be explained by the fact that there was a bony bridge preoperatively, albeit incomplete, and the cleft was very wide initially. The cleft width decreased significantly after surgery, so even with more complete bony fill postoperatively, the measurement of bone volume decreased.
(a) Initial visit prior to treatment (T1) photo montage, note anterior crossbite, missing maxillary right and left lateral incisors and second premolars, large edentulous area in maxillary lateral incisor space with paucity in alveolar bone, (b) T1 CBCT, (c) T1 lateral cephalometric radiograph, (d) Progress report (T2) photo montage, note maxillary teeth were not moved into the alveolar defect, (e) T2 CBCT, (f) T2 lateral cephalometric radiograph, (g) Ten-months post-op (T3) photo montage, note improved overbite, overjet, and closure of cleft dental gap; slight paucity present in cleft area, however adequate bone present to support adjacent teeth, (h) T3 CBCT, (i) T3 lateral cephalometric radiograph.
Discussion
Correction of alveolar bone defects and persistent oronasal fistulas in patients with CLP has traditionally relied on secondary ABG. When successful, this approach restores alveolar continuity, supports tooth eruption, and closes fistulae.22,23 However, a subset of patients experiences graft failure due to resorption, inadequate local anatomy, or compromised vascularity. 24 In these patients, persistent alveolar clefts may be accompanied by malpositioned or impacted teeth, residual fistulas, and areas of unsupported alveolar bone. Segmental two-piece Le Fort I osteotomy offers an alternative surgical strategy to revision ABG in this setting by allowing direct closure of the alveolar bone gap and fistula through skeletal repositioning. In the setting of multiple failed ABG, it provides an alternative to repeated grafting with suboptimal outcomes. Moreover, in cases involving large defects requiring prosthetic lateral incisor replacement, this approach eliminates the need for prosthetic rehabilitation, thereby avoiding the associated maintenance and long-term replacement burden.
In this case series, we demonstrate the use of segmental two-piece Le Fort I osteotomy to achieve alveolar cleft closure, fistula repair, occlusal correction, and dental substitution in a single-stage procedure. In this approach, the maxilla is advanced to correct the anterior crossbite, and the lesser segment is mobilized to approximate the greater segment, closing the residual alveolar defect in a single approach compared to the historical two-stage approach previously described by Gillies and colleagues of secondary ABG and fistula closure followed by a second operative for Le Fort I osteotomy.25–27 Segmental repositioning allows for unification of the maxillary arch with tension-free closure of the cleft site. 19 Additionally, the need for prosthetic implants or a dental bridge is avoided, both of which require meticulous care to maintain long-term stability. In our experience, the segmental two-piece Le Fort I osteotomy provided a predictable means of addressing both skeletal and dental sequelae of failed secondary ABG while simultaneously correcting maxillary hypoplasia, malocclusion, and edentulous spans in the lateral incisor position.
Regarding management of the segmental site, simultaneous ABG may be performed at the time of segmental osteotomy. In our practice, secondary ABG is initially pursued during mixed dentition with the goal of achieving a single-piece maxilla. 28 In cases of graft failure, revision ABG is often performed. However, in patients who have a Class III malocclusion, a segmental two-piece Le Fort I osteotomy with concurrent grafting of the osteotomy site can be a viable treatment alternative to revision ABG, especially in patients who have already undergone multiple failed ABG. In select cases, grafting may be unnecessary if rigid skeletal approximation allows for direct bony contact between segments, although this has not been systematically evaluated. Furthermore, comparative outcomes between autograft and allograft at the segmental site remain poorly characterized in the literature. 29
Our findings build upon earlier work describing segmental cleft-orthognathic surgery. Posnick and colleagues first reported the use of modified and segmental two-piece Le Fort I osteotomies to address cleft-associated maxillary hypoplasia, transverse discrepancies, and residual alveolar defects, emphasizing the ability to achieve arch unification and fistula closure in skeletally mature patients.18,19 These earlier studies primarily focused on comparing a novel technique to previous methods of cleft-dental gap closure such as the use of prosthetics or osseointegrated implants. More recently, Parsaei et al. described segmental cleft-orthognathic surgery as a means of achieving facial balance, fistula closure, and arch unification, highlighting the versatility of this approach in complex cleft deformities. 21 However, this study was conducted in a single patient, and neither study provides objective pre- and postoperative measurements on changes in cleft-width and bone-volume. Our series adds to this literature by specifically focusing on patients with residual alveolar clefts following failed or incomplete secondary ABG and by demonstrating the feasibility of combining fistula closure, bone grafting, and dental substitution within a single operative setting. By providing objective measurements, our study offers a contemporary demonstration that segmental two-piece Le Fort I osteotomy is a well-suited and effective technique for closing cleft-related dental gaps in patients with failed ABG.
Several important considerations should be highlighted regarding these cases. First, in Case 1, the impacted maxillary right canine was extracted at the time of the segmental two-piece Le Fort I osteotomy. This illustrates that, in appropriately selected patients, impacted teeth can be removed concurrently with orthognathic surgery. Performing the extraction at the time of surgery avoids the need for a separate procedure and may help minimize potential bone loss associated with extraction at an earlier stage. Additionally, preservation of the tooth until the time of surgery allows for a convenient space to execute the osteotomy safely.
In Case 3, the permanent maxillary left second premolar was extracted to alleviate crowding in the left alveolar segment. Although space was present within the cleft defect, orthodontic movement of teeth into this area should be avoided. It is essential to ensure that teeth within each alveolar segment are supported by adequate bone, even if this necessitates extraction of a premolar in a quadrant already lacking a lateral incisor. Preservation of periodontal support and proper bony housing is prioritized over maintaining the full complement of teeth.
Lastly, in the fourth case presented, mandibular premolars were extracted in order to optimize the occlusion. However, in patients whose occlusion will finish with 10 maxillary teeth (i.e., missing four maxillary teeth), mandibular premolars do not necessarily need to be extracted. A decision regarding mandibular extractions should be made based on dentoalveolar factors (i.e., crowding, flaring, curve of Spee).30,31 A final occlusion with 10 maxillary teeth and 14 mandibular teeth is acceptable.
Future considerations regarding segmental cleft-orthognathic surgery include management of residual dental and periodontal asymmetries. Patients may present with asymmetric tooth number, transposed teeth, or uneven gingival margins that can affect aesthetic outcomes despite successful skeletal correction. In such cases, adjunctive periodontal procedures, including crown reshaping, gingivoplasty, or selective gingival contouring, may be required to optimize dental symmetry and smile aesthetics. Additionally, cosmetic dental procedures including crowns and veneers can optimize dental esthetics in the presence of dental asymmetries and substitutions. However, in our case series, the patients were each satisfied with their appearance and declined further dental or periodontal procedures.
Limitation
This study is limited by several factors including its retrospective design, small sample size, and single-institution experience, which preclude comparative analysis. First, the lack of a control or comparison group further limits the ability of this technique to assess relative effectiveness to traditional management protocols. Secondly, given the limited sample size of four patients, this study remains descriptive and should not be generalized to all patients; however, future prospective studies in larger cohorts will be necessary to better define the role of this technique. Thirdly, there is substantial patient heterogeneity in orthodontic management due to differences in dental anomalies, extractions, bone volume, and cleft-width which further preclude comparative analysis. Fourthly, as all subjects were clinical patients, blinding was not performed for CBCT evaluation.
Due to the missing teeth, patients did not necessarily finish in class I occlusion, and standardized occlusal indices were difficult to apply. However, patients finished their treatment with normal overbite and overjet, with proper occlusal interdigitation and centered midlines. Patients in this cohort underwent bone grafting with either autogenous iliac crest bone or ViviGen allograft, which may represent a potential confounder; however, a formal comparative analysis was not feasible due to the limited sample size. Additionally, follow-up duration was inconsistent and thus long-term stability was only noted in patients who had adequate follow-up time. Despite these limitations, this case series demonstrates that segmental two-piece Le Fort I osteotomy represents a viable surgical option for select patients with residual alveolar clefts, offering a comprehensive solution to skeletal, dental, and fistula-related deformities when conventional grafting strategies have failed or are no longer feasible.
Conclusion
Segmental two-piece Le Fort I osteotomy represents an effective surgical strategy for select patients with CLP who present with an anterior crossbite and residual alveolar cleft. In this case series, the technique reliably corrected the anterior crossbite and maxillary hypoplasia and achieved a functional and stable occlusion. Importantly, this approach allowed for simultaneous closure of the residual alveolar defect through skeletal approximation and limited bone grafting, restoring alveolar continuity in a single stage. By closing the cleft-associated dental gap, the need for prosthetic replacement of a lateral incisor within the cleft site can be avoided. Our findings further demonstrate that finishing orthodontic treatment with 10 maxillary teeth is both functionally acceptable and esthetically satisfactory when occlusion and arch form are appropriately optimized. Although limited by sample size and follow-up duration, these results support segmental two-piece Le Fort I osteotomy as a viable and comprehensive alternative for managing the dentoalveolar sequelae of failed secondary alveolar bone grafting.
Footnotes
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (No. IRB00546497) on February 2026.
Consent to Participate
Not Applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are not publicly available but may be shared upon reasonable request.