
Abstract
Objective
Design
Longitudinal prospective cohort study.
Setting
Questionnaire data from the Cleft Collective.
Participants
Three-year-old (n = 928) and 5-year-old children (n = 795) born with cleft lip and/or palate.
Main Outcome Measure(s)
ICS – parent-reported measure using a 5-point Likert scale to indicate how intelligible their child is with seven different communication partners.
Results
Median scores for children born with cleft lip only were higher (4.14, 95% CI = 4.00–4.14 for 3-year-olds; 5.00, 95% CI = 4.29–5.00 for 5-year-olds) than those born with any form of cleft palate (3.71, 95% CI = 3.57–3.86 for 3-year-olds; 4.14, 95% CI = 4.14–4.29 for 5-year-olds). Scores for children born with cleft lip only aligned with studies comprising typically developing children and normative samples, whereas those born with any form of cleft palate did not. Children born with cleft palate and a diagnosed syndrome scored lower than those born with non-syndromic cleft palate. For children who had data at both ages, 75.4% showed improvement over time, 14.3% stayed the same and 10.3% scored lower at age 5.
Conclusion
Reference data are now available for children with the major cleft subtypes which can be used for comparison in clinical settings. These data show how children born with cleft compare with the non-cleft population and change over time.
Introduction
Measuring outcomes of cleft care is complicated by the nature of cleft lip and/or palate (CL/P) as a life-long condition and the number of domains in which outcomes need to be measured (speech/communication, eating and drinking, dental and oral health, breathing, hearing, appearance, psychosocial development, burden of care).1,2 Treatment is multifaceted and can involve surgeons, clinical nurse specialists, dentists, speech and language therapists, psychologists, dieticians, audiologists and numerous other professionals. 3 Treatment happens over time, so outcome measurement must be able to accommodate expected changes in children's growth and development as well as positive and negative results of treatment. Outcome measures often have a dual function of both reporting the impact of treatment to date whilst also identifying possible unmet needs which might require further intervention, either immediately or at some point in the future.
The multifaceted nature of outcome measurement in CL/P was recognised by Allori et al. (2017) in their working group which led to the development of a standard set of outcome measures for use in cleft care. 1 The standard set includes clinician and patient-reported measures. It covers six age points from the first encounter at less than 3 months old to end of treatment or age 22, whichever is soonest, and recommends use of 22 discrete tools covering eight domains of outcome. This standard set was developed for the International Consortium of Health Outcome Measures (ICHOM) and has become the basis for the “ICHOM Set of Patient-Centered Outcome Measures for Cleft Lip & Palate.”1,4
Intelligibility
Speech/communication is one of the eight domains covered by the standard set, with intelligibility being one of the five of the included outcomes. Intelligibility was defined by McLeod et al. (2012) as “the degree to which speech is understood by a listener”, 5 highlighting its listener-dependent nature. Studies examining intelligibility in children born with cleft palate with or without cleft lip (CP ± L) have reported that nearly 20% of 5-year-old children with non-syndromic unilateral cleft lip and palate are barely intelligible or unintelligible, 6 and 3-year-old children with CP ± L had lower intelligibility than children born with cleft lip only, with the lowest intelligibility scores being seen in children born with bilateral cleft lip and palate. 7
Intelligibility in Context Scale
The measure of intelligibility recommended for use in the ICHOM Set of Patient-Centered Outcome Measures for Cleft Lip & Palate (ICHOM Set) is the Intelligibility in Context Scale (ICS). The ICS is a parent report tool, designed to provide information relating to speech sound development to speech and language therapists.5,8 It is a seven-item questionnaire which asks parents to rate the degree to which their child's speech is understood by a range of communication partners (parents, immediate family, extended family, friends, acquaintances, teachers, and strangers) on a 5-point Likert scale. A mean score for intelligibility across all conversational partners is then derived from the total. The ICS is quick to administer and provides information on the parents’ perspective of their child's speech development and disorder. Its value is further enhanced by the fact that it is available in over 70 languages, meaning that it can be used with families who speak languages other than those spoken by the clinical team. This is particularly valuable in the domain of speech/communication where language-specific assessments are essential to the measurement of a language-based outcome. The ICS has been validated in 18 studies of over 4235 children from 14 countries and has been shown to correlate with other clinical measures of speech in children with velopharyngeal insufficiency. 9
Use of the ICS in the ICHOM Set is useful given the ease and versatility of the tool. However, to date, while there are data for typically developing children and normative samples within the general population emerging from across the globe (Appendix 1 in the Supplementary materials), there are limited reference data for children born with CL/P to facilitate comparison of scores. Analysis of data from 412 3-year-old children born with CL/P by Seifert et al. (2021) provided a mean of 3.75 across all cleft subtypes, with strong evidence for a difference in scores between children born with cleft lip only (n = 104; x̄ = 4.13, s = 0.62) and those born with CP ± L (n = 308; x̄ = 3.63, s = 0.76). 7 However, the ICHOM Set recommends assessment using the ICS at age 5. Ombashi et al. (2023) considered the speech assessment measures used in the ICHOM Set, using them with a sample of 2500 patients aged between 5 and 22. 10 The ICS was completed on a subsample of 397 children with CP ± L at ages 5 and 12, though it is unclear how many of these were each age. Mean scores for those at age 5 were determined for children with cleft palate only (x̄ = 4.08, s = 0.73) and those with cleft lip and palate (x̄ = 4.03, s = 0.5) but analyses did not distinguish between different subtypes of cleft lip and palate (unilateral versus bilateral) or children with and without identified syndromes. Further studies have reported ICS scores for children born with CL/P between the ages of 4 and 14 but do not specifically report ICS scores for 5-year-old children and all comprise small sample sizes.8,11–13 More reference data, specifically stratified by cleft type and syndromic status, are needed to assist clinicians in determining how well their individual patients perform on the ICS when compared to peers with the same cleft phenotype. This is important for reporting outcomes as well as to facilitate comparisons within the population to help determine the need for intervention and meaningfully observe changes over time.
Change Over Time in Typically Developing and Normative Samples
Many studies have reported use of the ICS with typically developing populations of varying ages. Data from typically developing and normative samples are available in multiple languages including: Cantonese, 14 English,15–17 Italian, 18 Jamaican Creole,17,19 Korean, 20 Portuguese, 21 Swedish, 22 and Vietnamese. 23 Across these studies 3-year-old children scored within a range of 3.68–4.26 and 5-year-old typically developing children scored within a range of 4.19–4.78 (see Appendix 1 in the Supplementary materials). An increase in score with increased age is clearly observed across the studies, but this does not represent change in individuals over time as the studies were all cross-sectional in design. While the intelligibility of all children would be expected to increase over time as a result of the expected maturation of the cognitive and motor development of speech production, children born with CL/P have additional impacts on their speech which, for some at least, would lead to a different pattern in the change in speech intelligibility than that observed in the typically developing and normative samples.24–27
Change Over Time in Children Born with CL/P
Speech production in children born with CL/P may be impacted by structural differences in the anatomy. Sometimes this can have a negative impact on intelligibility. For example, velopharyngeal insufficiency, which occurs when the soft palate is unable to make a complete closure with the pharynx, or presence of fistulae in the palate, will lead to hypernasal resonance and weak or absent pressure consonants (i.e., the consonants which involve plosion such as /p, b, t, d, k, ɡ/ or frication such as /f, v, s, z/) with significant impact on intelligibility. 28
Change can also lead to improvements in intelligibility and generally this will be due to one of three things: spontaneous maturation, speech-language pathology, and surgery. 29 Spontaneous maturation and intervention from a speech-language pathologist are likely to lead to a gradual increase in intelligibility.24,30 In contrast, surgery to address anatomical influences on speech, such as a pharyngoplasty to address velopharyngeal insufficiency or a repair to a palatal fistula, may lead to a step-change in the level to which a child can be understood. This is because the anatomical defect which made typical speech impossible to produce has been repaired. Scores for ICS over time in a longitudinal study are needed to determine the pattern of change in intelligibility in children born with CL/P which will be different to a typically developing or normative sample.
The Cleft Collective Cohort Study
Longitudinal research in CL/P is often hampered by the need to collect data on large samples over a long period of time. The Cleft Collective Cohort Study is a national longitudinal cohort study in the United Kingdom (UK). Established in 2012, the Cleft Collective has to date recruited over 12,000 participants from over 4000 families comprising children born with all types of CL/P, their parents and siblings. 31 Recruitment occurs across all 16 centralised cleft centres and provides a resource for clinicians and researchers looking to explore the cause, treatment, and psychological impact of CL/P on individuals and their families. Data are collected at baseline and at multiple timepoints throughout the child's development. Data comprises information on the child's social, emotional, behavioural, and cognitive development and the mother's (and if recruited, her partner's) economic, psychological health, and social status. In addition, biological samples are collected at or soon after recruitment. Data collection includes biological samples for DNA extraction and genotyping, clinical data, and parent- and self-report data. Further data collection comprises data from medical records, clinician reports of surgery, speech and language therapy and audiology, and audio recordings at 13 months are also collected. The aim of the Cleft Collective is to establish a resource which can be used by researchers across the globe to investigate the causes of cleft, the best treatments, and the outcomes from cleft care in the UK. Details on how to access the resource, including a data dictionary, can be found here: http://www.bristol.ac.uk/cleft-collective/professionals/access/.
Aim and Objectives
The Cleft Collective resource provides the wealth of data needed to address the challenges of presenting longitudinal reference data regarding intelligibility on the ICS for 3- and 5-year-old children with CL/P. Specifically, in line with the recommendations from the ICHOM Set, there is a need for reference data for the ICS for 3- and 5-year-old children for each of the major cleft subtypes, for those with and without identified syndromes and to determine the degree to which ICS scores show improvement over time compared to typically developing and normative samples. The Cleft Collective provides this unique opportunity to enable stratification of reference data for cleft subtypes and syndromic status whilst still maintaining large sample sizes for each subgroup. The objectives of the work described in this paper were therefore:
To provide reference data for the ICS for 3- and 5-year-old children born with CL/P, stratified by cleft type and syndromic status. To compare ICS scores for children with CL/P with data from typically developing and normative samples. To determine the change in ICS scores for children between the ages of 3 and 5 years old.
Method
The Cleft Collective comprises two cohorts: the Birth Cohort Study, where families are recruited in pregnancy or soon after the birth of their child; and the Five-Year-Old Cohort Study, where recruitment takes place between the child's fifth and sixth birthday. The research in this paper focuses on the data from the Cleft Collective Birth Cohort Study only. Recruitment to this study began in 2013 and is ongoing. 31
Participants
Participants included within these analyses were children recruited to the Cleft Collective Birth Cohort Study where a mother had responded to the 3-year-old or the 5-year-old follow-up questionnaire and completed the ICS questions. At the point of analyses, the Cleft Collective Cohort Study had recruited 11984 participants from 4264 families overall, of which 9133 participants from 3209 families had been recruited to the Birth Cohort Study. A total of 2626 and 2205 children within the birth cohort had reached the age of 3 and 5 years respectively; all parents and carers of these families were invited to complete the 3-year and where applicable the 5-year follow-up questionnaires containing the ICS, however, only maternal responses were used within these analyses. Questionnaires were returned and completed by 928 mothers (35.3% response rate) of 3-year-old children. Questionnaires were returned and completed by 795 mothers (36.1% response rate) of 5-year-old children. All questionnaires were provided to parents and carers in English, questionnaires were not available in alternative languages and therefore it is assumed all responders were English speaking.
Measure
The ICS is a seven-item questionnaire that invites parents to reflect on the past month and indicate how intelligible their child was to: themselves, immediate family, extended family, child's friends, acquaintances, child's teachers, and strangers. 5 Parents selected one of five options for each of the seven communicative partners: always (5), usually (4), sometimes (3), rarely (2), and never (1) and an average score is computed using the mean. The average ICS score was calculated using the mean values from six of the listed communicative partners for 3-year olds. Parental response to whether a teacher understand their child was excluded due to children not legally needing to start school until the year after their fourth birthday in the UK. Responses to all seven communicative partners were used to calculate the average ICS score for 5-year olds.
Data Collection
Both paper and online questionnaires were available for parents to complete and these included the seven ICS questions. The 3-year and 5-year follow-up questionnaires are sent to parents shortly after the child's third and fifth birthday, respectively. Where an email address was available for a parent, an email invite to complete the questionnaire with the online link was sent to them. Online questionnaires were designed using REDCap.32,33 Where an email address was not available for the parent, a paper questionnaire was sent to the parent's home address. Paper versions of the questionnaire are also sent to parents who received an email invitation and had not completed the questionnaire within two weeks. Parents received up to two reminders to complete their questionnaire if they had not responded.
Data Analysis
Descriptive statistics of child's biological sex and age at questionnaire response were calculated to detail the sample used within this analysis. Sample responses for each individual communicative partner explored within the ICS measure were described using frequencies and percentages for the whole sample at 3 and 5 years old. The distribution of the average ICS score for the whole sample was determined using a Shapiro-Wilk test for normality. The distributions of the average ICS score at both ages were deemed to be non-parametric, the median of the average ICS score with 95% confidence intervals and interquartile ranges were calculated. Although the data were non-parametric, to allow for direct comparisons to other cohorts, who have measured the ICS using parametric methods, mean values of the average ICS score with 95% confidence intervals and standard deviations were also calculated.
Data were stratified by cleft subtype, average ICS scores were described using both medians and means with 95% confidence intervals and interquartile ranges and standard deviations, respectively. Average ICS scores were compared between cleft subtypes using a Kruskal‒Wallis test followed by post-hoc analysis using a Dunn's test. Further stratification was implemented between syndromic and non-syndromic CP ± L. Average ICS scores were described using both medians and means with 95% confidence intervals and interquartile ranges and standard deviations, respectively. Average ICS scores were compared between syndromic status using a Mann-Whitney U test. Differences between cleft subtype and syndromic groups were graphically presented using box and whisker plots. Non-parametric reference data were generated for all cleft subtypes and for non-syndromic and syndromic cleft palate with or without lip using non-parametric empirical centiles (5th, 10th, 15th, 25th, 50th, 75th, 85th, 90th, 95th). Despite the non-parametric distribution of the data, parametric reference data using two standard deviations from the mean were calculated to enable comparison with similar cohorts where only parametric data were published.
Summary statistics of typically developing English-speaking cohorts were available for an American sample from the USA at ages 3 and 5 16 and for an Australian normative sample at the age of 5. 15 Due to these other cohorts only publishing parametric descriptive statistics of their samples we were limited to the statistical comparison that could be made. The difference in mean average ICS score between different cleft subtypes and typically developing/normative English-speaking cohorts from the USA and Australia were calculated using summary statistics presented within the papers. Further differences in mean average ICS score between non-syndromic CP ± L, syndromic CP ± L and typically developing/normative English-speaking cohorts from Australia and America were also calculated.
Longitudinal analyses were undertaken to allow comparison of the average ICS score between the ages of 3 and 5 years where data were available at both ages for Cleft Collective study children. Differences in average ICS score between both ages were calculated for each individual Cleft Collective study child. The proportion of children whose average ICS scores decreased, stayed the same or improved between the ages of 3 and 5 were further described. Shapiro-Wilks tests were performed to identify the distribution of the calculated differences. The distribution was initially explored with the full sample and further explored following exclusion of children who scored the highest possible average ICS score (five) at both ages. The Median of the change in average ICS scores with 95% confidence intervals were calculated for the sample overall, each cleft subtype and syndromic status. The variability of each sample was calculated using interquartile ranges. These descriptive statistics were calculated for everyone and then for a reduced sample excluding those who had scored the maximum possible average ICS score of five at both ages to account for ceiling effects. Paired Wilcoxon signed-rank tests were performed to identify whether there was a difference in average ICS score for children between the ages of 3 and 5 years for the whole sample and then stratified by cleft subtype and syndromic status. Visual comparison of average ICS scores at both ages were undertaken using box and whisker plots. Correlation analysis was further undertaken to identify the strength and direction of the linear relationship of change between average ICS score at ages 3 and 5 years for the whole sample, then stratified by cleft subtype and syndromic status. Scatter plots and the line of best fit were plotted for further visual comparison. To enable us to model the relationship between average ICS scores at ages 3 and 5 years whilst adjusting for confounders and considering the floor and ceiling effect of the average ICS score, Tobit regression models were performed. A total of three models were undertaken. Model 1 explored the unadjusted association between average ICS scores at ages 3 and 5 years. Model 2 was adjusted for cleft subtype and syndromic status (inclusive of cleft lip only). Model 3 was an extension of model 2 and further adjusted for the child's biological sex and socioeconomic status using the Index of Multiple Deprivation (IMD). 34 All analyses were performed using STATA (Release 18, StataCorp).
Governance
The Cleft Collective Cohort Study received ethical approval for recruitment and data collection by the South West Central Bristol Ethics (REC approval 13/SW/0064). Ethical approval for the analysis reported in this paper was obtained from the University of Bristol's Faculty of Health Sciences Research Ethics Committee (REC approval Ref: 18498). Consent for participation was obtained in writing from parents for their own participation and for the participation of their child or children. This study was conducted under project number CC060-YW for the Cleft Collective.
Results
Sample
At 3 years old, over half of the responses from the 928 questionnaires referred to male children (n = 556, 59.9%), and the median age of a child at response was 37.3 months (interquartile range = 36.8–38.5). At 5 years old, over half of the responses from the 795 questionnaires referred to male children (n = 483, 60.8%), and the median age of a child at response was 61.7 months (interquartile range = 61.1–63.3).
Intelligibility of Children with Cleft Lip and/or Palate
Frequencies and percentages of parent-reported intelligibility with each communicative partner are shown in Table 1. Mothers reported that they understood their child's speech most of the time, with 92.8% (3y) and 96.7% (5y) of mothers reporting that they usually (3y = 54.9%; 5y = 30.8%) or always (3y = 37.9%; 5y = 65.9%) understand their child. At both ages, mothers reported that strangers’ understanding of their child was the lowest of the communicative partners with 11.0% (3y) and 39.9% (5y) of strangers always understanding the child. Shapiro-Wilk tests for normality confirmed the distribution of the average ICS score at ages 3 and 5 were not normally distributed (Age 3 W = 0.98, p < 0.001; Age 5 W = 0.97, p < 0.001). At 3 years old, the median average ICS score across all cleft subtypes was 3.86 (95% CI = 3.86, 4.00; interquartile range = 3.29–4.29) and the mean average ICS score was 3.75 (95% CI = 3.70, 3.80; s = 0.79). By 5 years old, the median average ICS score across all cleft subtypes had increased to 4.29 (95% CI = 4.29, 4.43; interquartile range = 3.86–5.00) and the mean was 4.27 (95% CI = 4.22, 4.33; s = 0.76).
Maternal Response to the Intelligibility in Context Scale (ICS) for Children Born With a Cleft Lip and/or Palate at 3 and 5 Years Old.
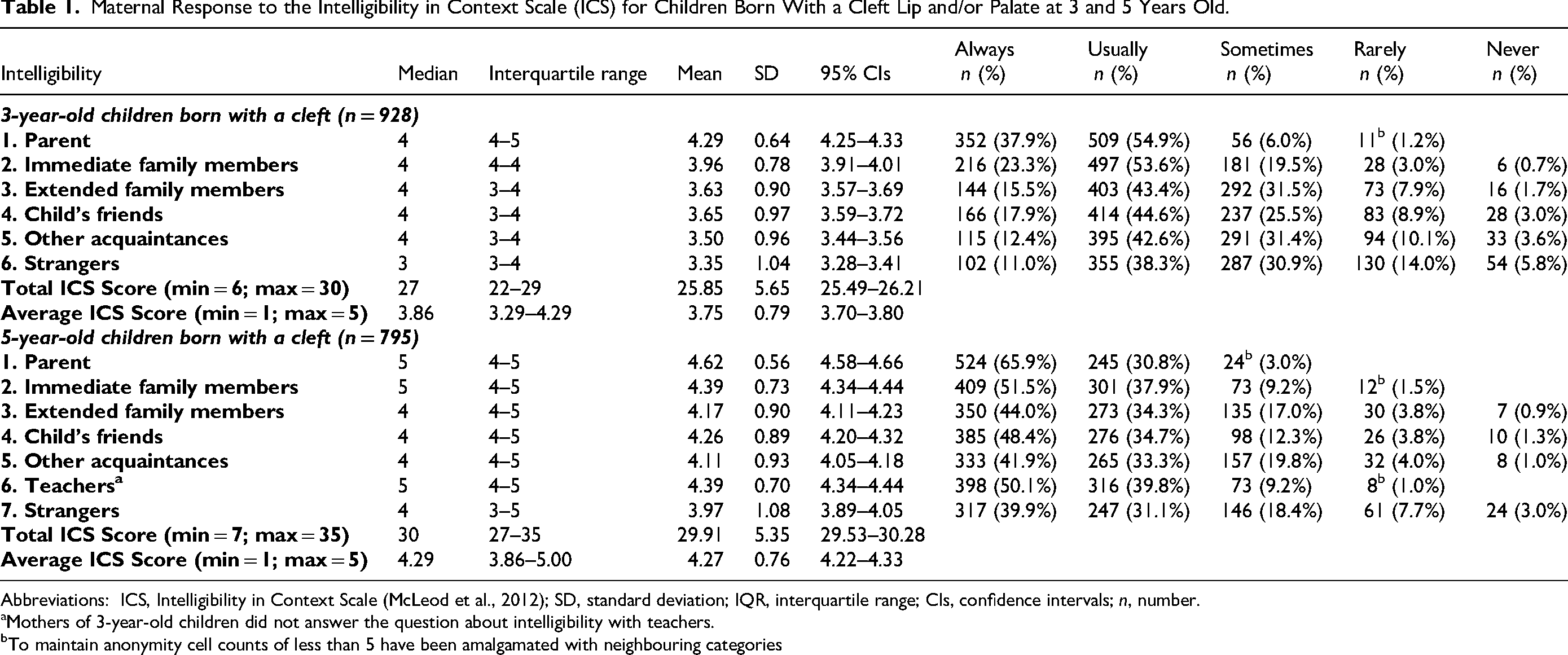
Abbreviations: ICS, Intelligibility in Context Scale (McLeod et al., 2012); SD, standard deviation; IQR, interquartile range; CIs, confidence intervals; n, number.
Mothers of 3-year-old children did not answer the question about intelligibility with teachers.
To maintain anonymity cell counts of less than 5 have been amalgamated with neighbouring categories
Intelligibility and Cleft Subtype
Across cleft subtype at age 3, the highest average ICS score was reported in children born with cleft lip only (CLO) with a median average ICS of 4.14 (95% CI = 4.00, 4.14; interquartile range = 3.86–4.57) and a mean average ICS score of 4.10 (95% CI = 4.01, 4.19; s = 0.73) (Table 2). The lowest average ICS score was reported in children born with a bilateral cleft lip and palate (BCLP), with a median average ICS score of 3.50 (95% CI = 3.29, 3.80; interquartile range = 3.00–4.00) and a mean average ICS score of 3.48 (95% CI = 3.31, 3.64; s = 0.81). Similarly at age 5, the highest average ICS score was reported in children born with CLO with a median average ICS score of 5.00 (95% CI = 5.00, 5.00; interquartile range = 4.29–5.00) and a mean average ICS score of 4.64 (95% CI = 4.56, 4.72; s = 0.59). The lowest average ICS score at age 5 was reported in children born with BCLP with a median average ICS score of 4.00 (95% CI = 3.95, 4.14; interquartile range = 3.57–4.64) and a mean average ICS score of 4.01 (95% CI = 3.86, 4.16; s = 0.77). A Kruskal‒Wallis test provided strong evidence to suggest the average ICS score was different in at least one cleft type at 3 years (χ2 = 77.55; p < .001) and at 5 years (χ2 = 78.26; p < .001). Post hoc analyses using a Dunn's Test provided strong evidence to suggest differences in average ICS scores being present between children born with CLO and children born with any form of cleft palate (all p values <.001) at 3 and 5 years old. No statistical evidence was found to suggest a difference in parent-reported intelligibility between children born with cleft palate only (CPO) compared to unilateral cleft lip and palate (UCLP) at 3 years old (p = .192) but there was some statistical evidence at 5 years old to suggest a difference in the average ICS score between these groups (p = .073). Evidence was also found to suggest a difference in parent-reported intelligibility between children born with CPO compared to BCLP at age 3 (p = .022) and 5 years old (p = .007). There was weak statistical evidence to suggest a difference in the parent-reported intelligibility between UCLP and BCLP at 3 years old (p = .088) or 5 years old (p = 0.106). Visual comparison of the average ICS score between cleft type, for the full sample at 3 years old (n = 928) and 5 years old (n = 795), is graphically displayed using a box and whisker plot in Figure 1.
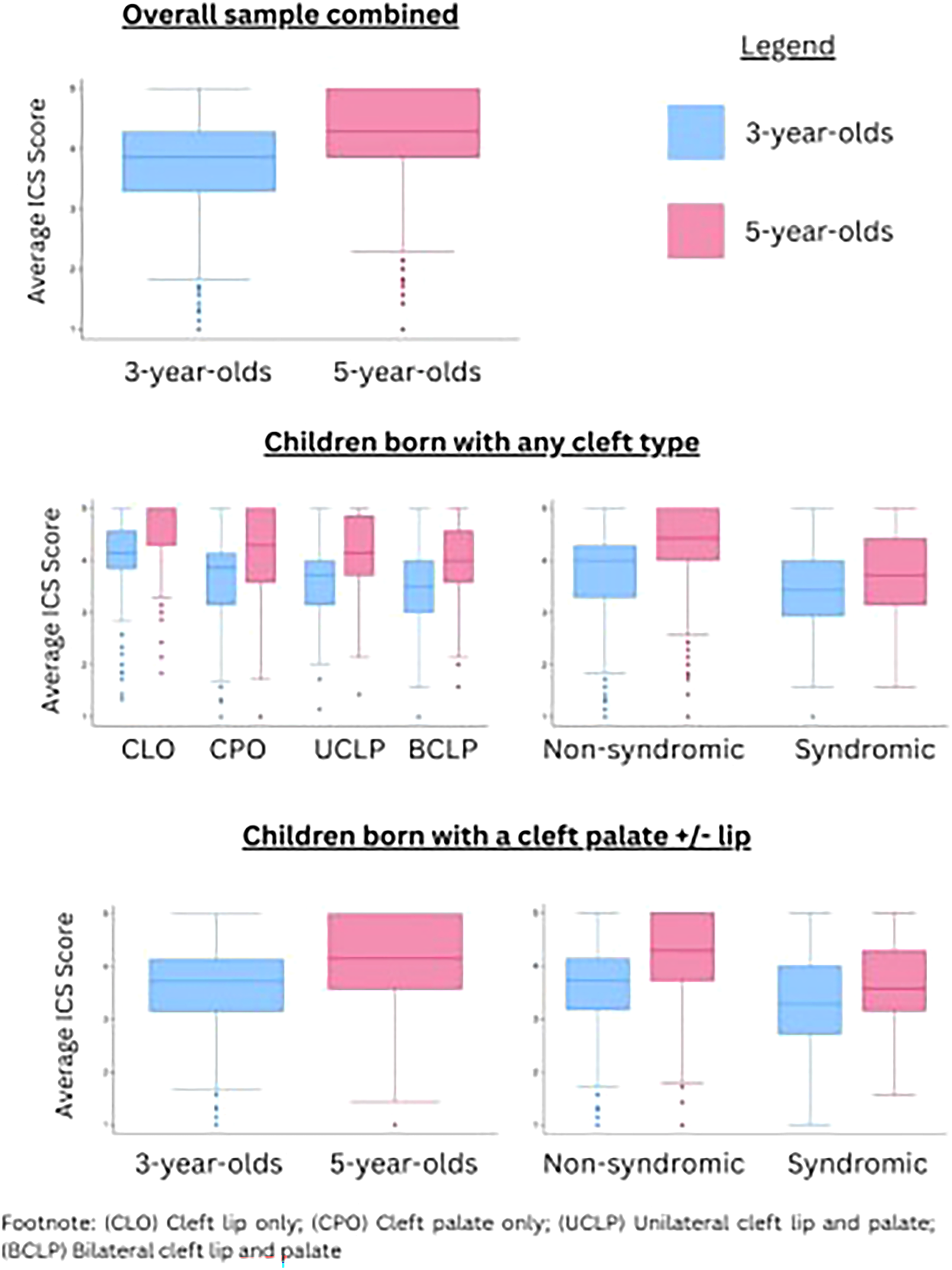
Box and Whisker plots of average intelligibility in context scale scores at 3 and 5 years old by subgroup.
Descriptive Statistics of Average Scores on the Intelligibility in Context Scale (ICS) by Cleft Type and Syndromic Status at 3 and 5 Years Old.
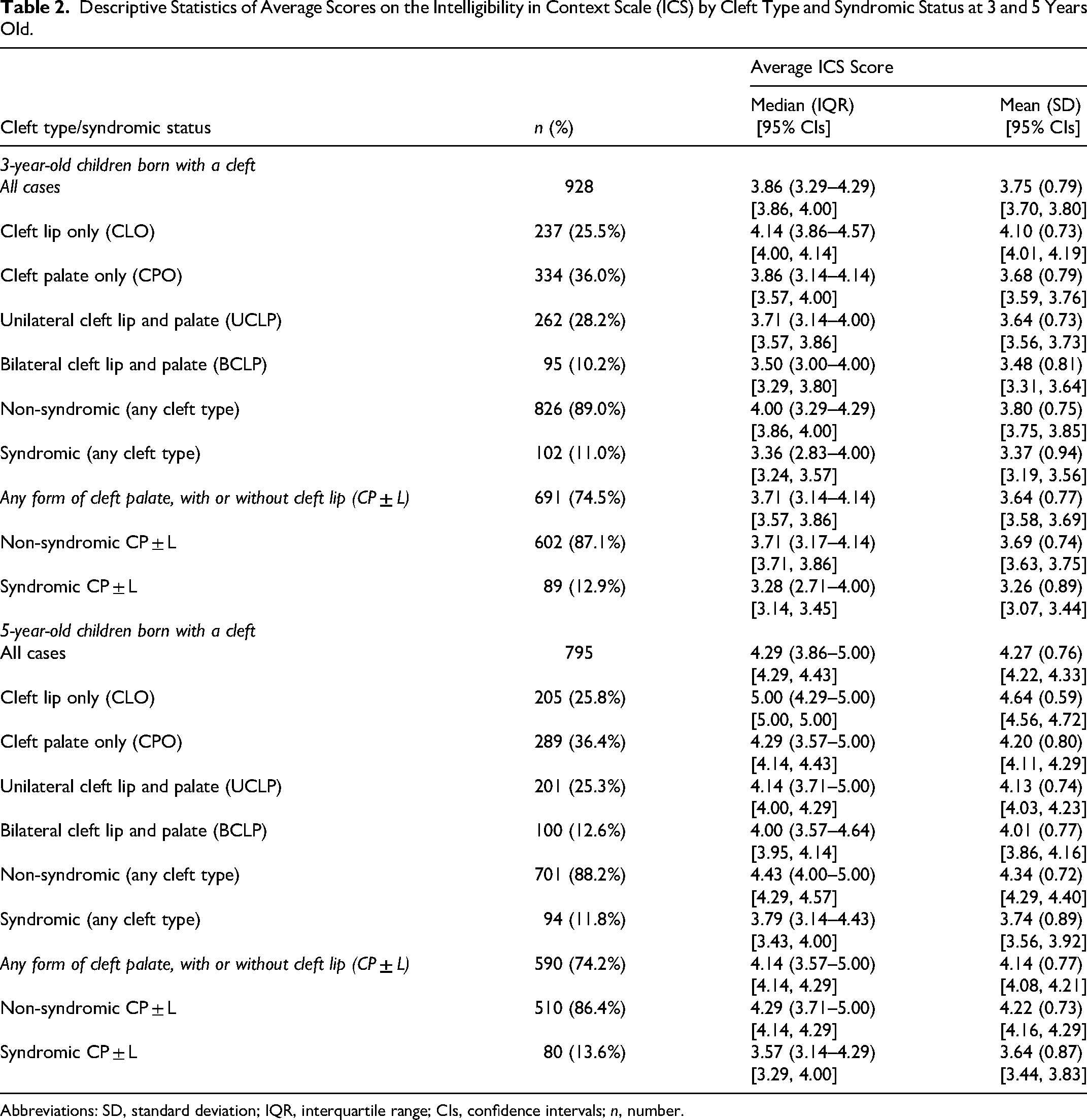
Abbreviations: SD, standard deviation; IQR, interquartile range; CIs, confidence intervals; n, number.
The Impact of Additional Syndromes
Children born with any form of cleft palate were combined into a CP ± L category and parent-reported intelligibility, using the average ICS score, was compared across children with non-syndromic and syndromic status. The sample for this analysis at 3 years old was n = 691 and at 5 years old was n = 590 (Table 2). When comparing the average ICS score, 3-year-old children born with non-syndromic CP ± L obtained higher scores than children born with syndromic CP ± L with a median average ICS score of 3.71 (95% CI = 3.71, 3.86; interquartile range = 3.17–4.14) and a mean of 3.69 (95% CI = 3.63, 3.75; s = 0.74). The median average ICS score for 3-year-old children born with syndromic CP ± L was 3.28 (95% CI = 3.14, 3.45; interquartile range = 2.71–4.00) and the mean was 3.26 (95% CI = 3.07, 3.44; s = 0.89). Similarly, 5-year-old children born with non-syndromic CP ± L obtained higher scores than children with syndromic CP ± L with a median average ICS score of 4.29 (95% CI = 4.14, 4.29; interquartile range = 3.71–5.00) and a mean average ICS score of 4.22 (95% CI = 4.16, 4.29; s = 0.73). The median average ICS score for children born with syndromic CP ± L was 3.57 (95% CI = 3.29, 4.00; interquartile range = 3.14–4.29) and the mean was 3.64 (95% CI = 3.44, 3.83; s = 0.87). Analysis using a Mann–Whitney U test showed strong evidence to suggest a difference in the average ICS score between children born with non-syndromic and syndromic CP ± L at both 3 years old (z = 4.08; p < .001) and 5 years old (z = 5.80; p < .001). Both non-parametric and parametric reference ranges were calculated and are displayed in Table 3 with graphical representation of the parametric reference ranges within Appendix 2 in the Supplementary materials. Reference ranges will enable clinicians to compare average ICS score for a child in their care against a sample of peers.
Intelligibility in Context Scale Reference Ranges (Both Non-Parametric and Parametric).
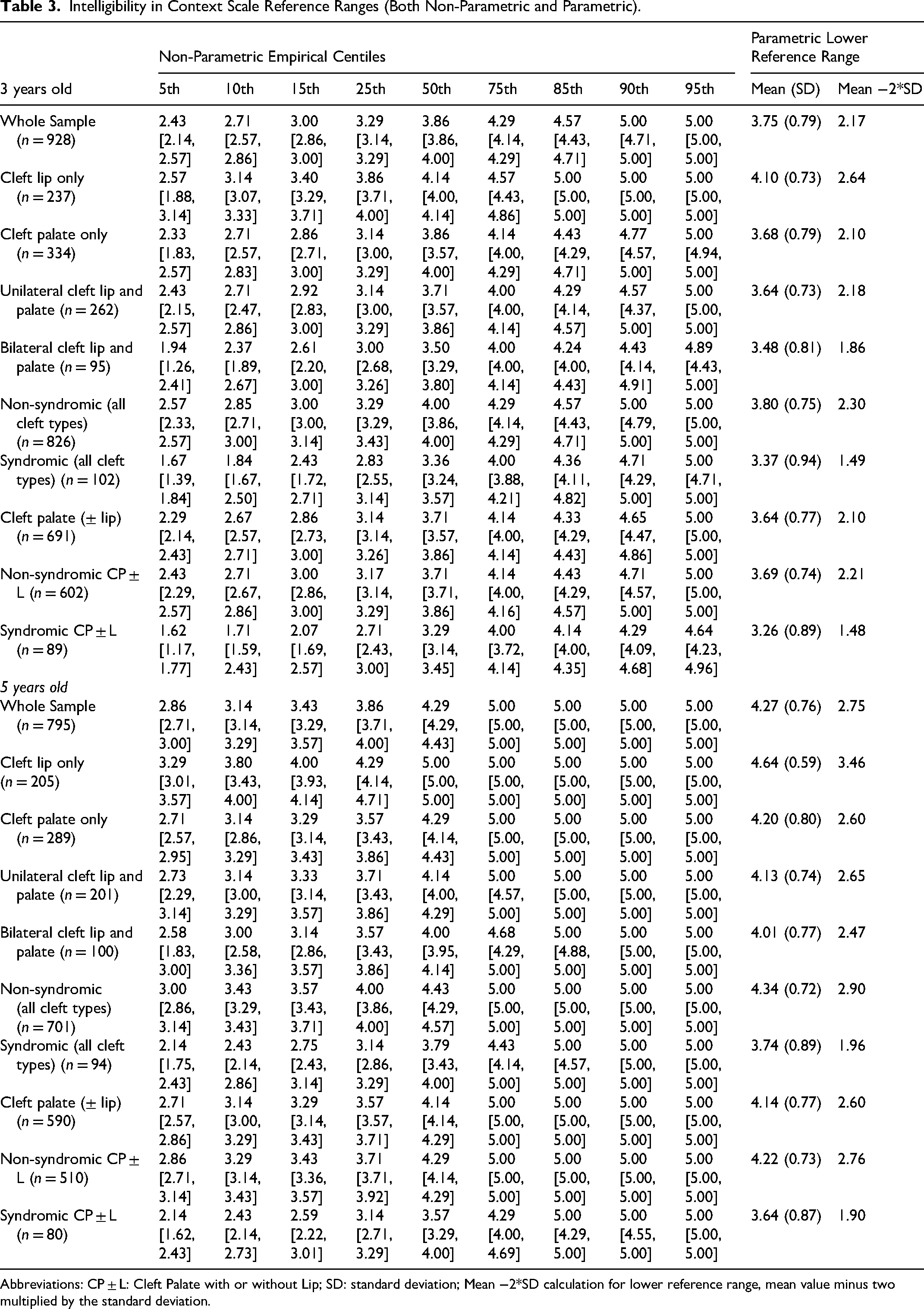
Abbreviations: CP ± L: Cleft Palate with or without Lip; SD: standard deviation; Mean −2*SD calculation for lower reference range, mean value minus two multiplied by the standard deviation.
Comparison with Typically Developing and Normative Samples
The mean average ICS score for the Soriano et al. (2023) English-speaking typically developing samples from the US was 4.06 between the ages of 3 years and 3 years 5 months and 4.48 between the ages of 5 years and 5 years 5 months. 16 For the McLeod et al. (2015) English-speaking normative sample from Australia the mean average ICS score was 4.3 between the ages of 5 years and 5 years 5 months (see Appendix 1 in the Supplementary materials). 15 Children born with CLO appeared to score similar average ICS scores to that of the typically developing and normative samples. At 3 years old the mean average ICS score for CLO was 0.04 points higher than the American typically developing sample. At age 5 the mean average ICS score for CLO was 0.16 points higher than the American typically developing sample and 0.34 points higher than the Australian normative sample. Children born with CP ± L scored lower than these samples. The mean average ICS score for children born with non-syndromic CP ± L was 0.37 points lower at 3 years old and 0.26 points lower at 5 years old when compared to the American typically developing sample. When compared to the Australian normative sample the average ICS score for children born with non-syndromic CP ± L was 0.08 points lower. The mean average ICS score for children born with syndromic CP ± L was 0.80 points lower at 3 years old and 0.84 points lower at 5 years old when compared to the American typically developing sample. When compared to the Australian normative sample, the average ICS score for children born with syndromic CP ± L was 0.66 points lower. Differences are further described in Table 4.
Difference in the Mean Average ICS Score Between Normative Samples and Children Born with a Cleft Lip and/or Palate.
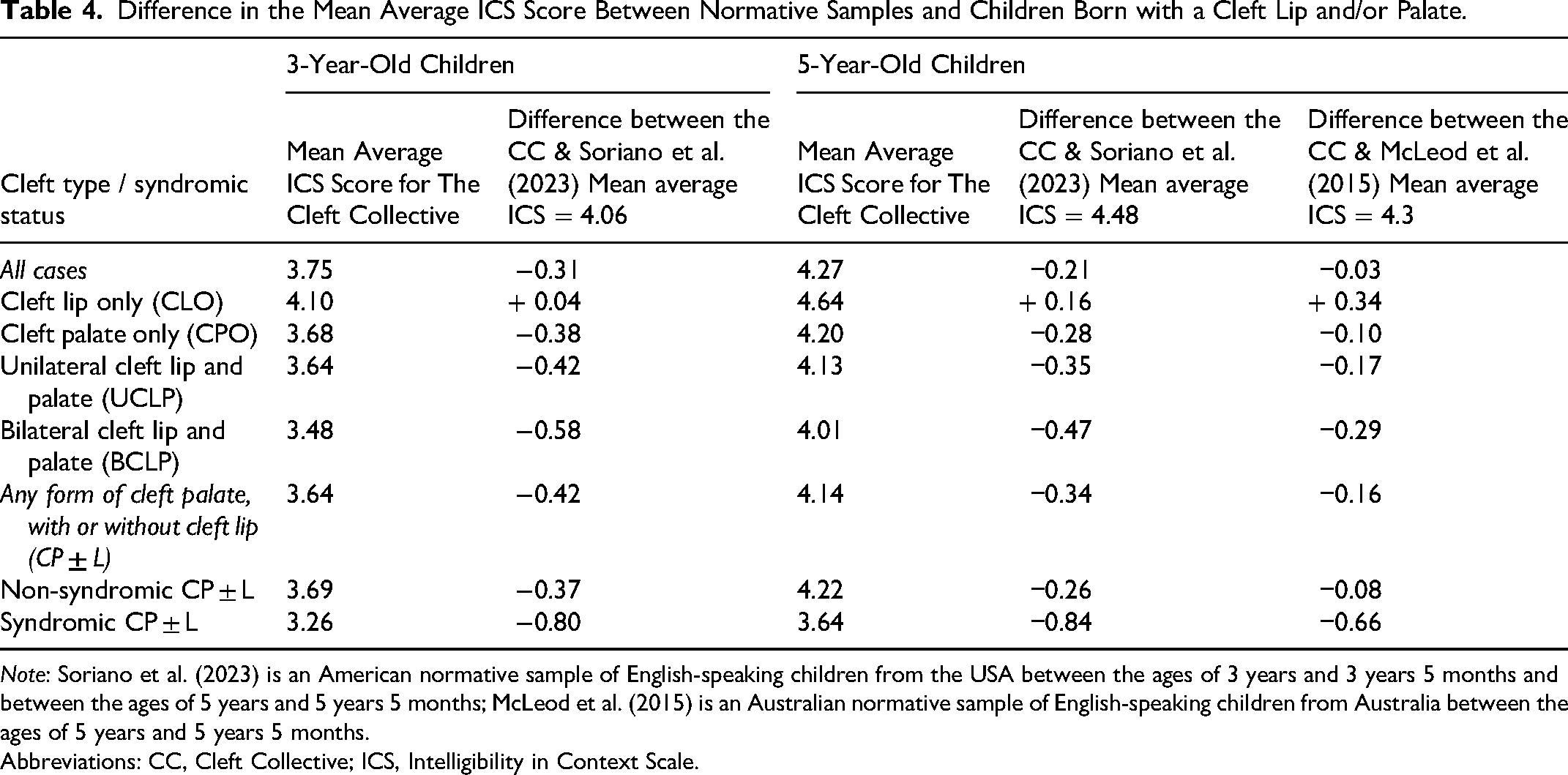
Note: Soriano et al. (2023) is an American normative sample of English-speaking children from the USA between the ages of 3 years and 3 years 5 months and between the ages of 5 years and 5 years 5 months; McLeod et al. (2015) is an Australian normative sample of English-speaking children from Australia between the ages of 5 years and 5 years 5 months.
Abbreviations: CC, Cleft Collective; ICS, Intelligibility in Context Scale.
Longitudinal Change in ICS Between 3- and 5-Year-Olds
Maternal ICS data reported for the same Cleft Collective study child at 3 and 5 years old were available for 574 children. Change in average ICS score between 3 and 5 years old was calculated for all children. An increase in average ICS score was seen in 75.4% (n = 433) of children between the ages of 3 and 5 years. The average ICS score (excluding those who scored five at both timepoints) remained the same at 3 and 5 years old for 5.9% (n = 34) and decreased for 10.3% (n = 59) of children. The remaining 8.4% (n = 48) of children in our sample scored the maximum possible average ICS score (five) at both timepoints. The distribution of the change in average ICS score between 3 and 5 years old was skewed when including all 574 children (Shapiro Wilk test: W = 0.99, p < .001) and when excluding cases with ceiling effects at both timepoints (Shapiro Wilk test: W = 0.96, p < .001). The median change in average ICS score was 0.57 (interquartile range = 0.10–0.98) when describing the full sample and 0.43 (interquartile range = 0.00–0.86) when excluding those who had a change score of zero due to the ceiling effect at both ages. Changes in average ICS score at 3 and 5 years old are described by cleft subtype and syndromic status in Table 5. Paired Wilcoxon signed-rank tests demonstrated strong evidence to suggest a difference in average ICS score at age 3 compared to age 5 for the whole sample (z = −16.84, p < .001), by each cleft subtype (CLO z = −9.89, p < .001; CPO z = −9.37, p < .001; UCLP z = −8.22, p < .001; BCLP z = −5.74, p < .001), for children born with a non-syndromic CP ± L (z = −15.78, p < .001) and for children born with a syndromic CP ± L (z = −5.86, p < .001). Correlation analysis suggested positive linear correlation between the average ICS score at 3- and 5 years old for the whole sample and each subgroup (r values ranged between 0.63 and 0.80), for the whole sample the r2 value was 0.50, suggesting 50% of the variation in average ICS at age 5 can be attributed to the average ICS score reported at age 3. Full correlation analysis results are presented in Appendix 3 in the Supplementary materials.
Longitudinal Analysis of Average Intelligibility in Context Scale Score Between the Ages of 3- and 5-Years-old; Median Change Over Time by Subgroup and Tobit Regression Analysis.
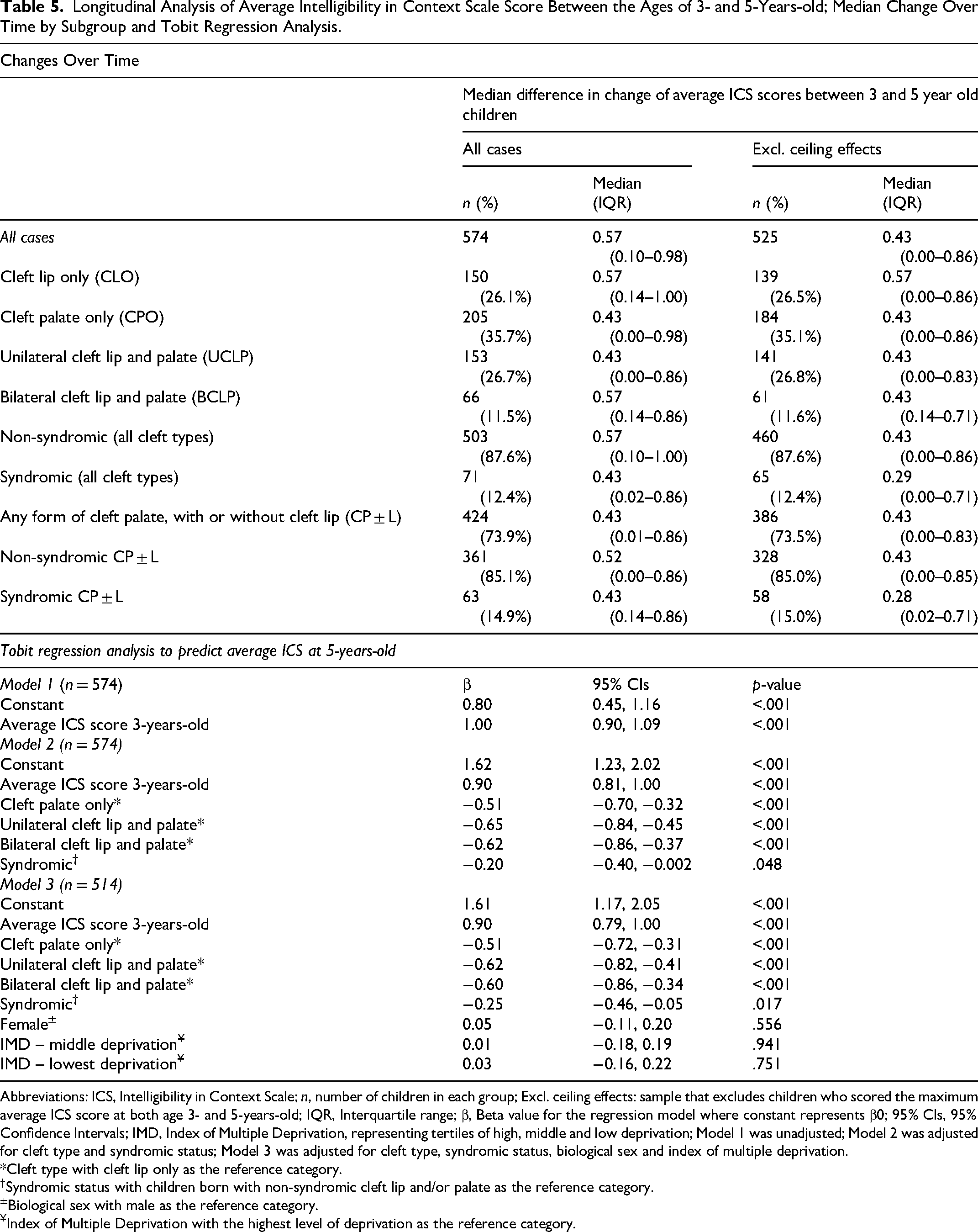
Abbreviations: ICS, Intelligibility in Context Scale; n, number of children in each group; Excl. ceiling effects: sample that excludes children who scored the maximum average ICS score at both age 3- and 5-years-old; IQR, Interquartile range; β, Beta value for the regression model where constant represents β0; 95% CIs, 95% Confidence Intervals; IMD, Index of Multiple Deprivation, representing tertiles of high, middle and low deprivation; Model 1 was unadjusted; Model 2 was adjusted for cleft type and syndromic status; Model 3 was adjusted for cleft type, syndromic status, biological sex and index of multiple deprivation.
*Cleft type with cleft lip only as the reference category.
†Syndromic status with children born with non-syndromic cleft lip and/or palate as the reference category.
±Biological sex with male as the reference category.
¥Index of Multiple Deprivation with the highest level of deprivation as the reference category.
Using an unadjusted Tobit regression model (model 1), strong evidence was found to suggest the average ICS score at 3 years old was a predictor of the average ICS score at 5 years old (β = 1.00, 95% CI = 0.90, 1.09, p < .001). Model 1 suggested that for each one-unit increase in the average ICS score at age 3, the expected ICS score at age 5 increased by 1.00 unit for children born with a cleft. Model 2 was adjusted for cleft type and syndromic status (β = 0.90, 95% CI = 0.81, 1.00, p < .001) and model 3 was further adjusted by biological sex and the IMD (β = 0.90, 95% CI = 0.79, 1.00, p < .001). Full Tobit regression results are presented in Table 5.
Discussion
Intelligibility is a core outcome for cleft care and the standard set of outcome measures for cleft suggest using the ICS to measure this. 1 Reference data on ICS performance for children born with CL/P are needed so that clinicians can determine how a child in their clinic compares with others in the population. Using data from the Cleft Collective Cohort Study, descriptive statistical analysis of ICS scores from 928 3-year-old and 795 5-year-old children was carried out to provide reference data on average ICS scores for children at each age for each cleft subtype and for syndromic and non-syndromic CP ± L.
Reference Data for Children Born with CL/P
Tables in this paper are available as reference sources for clinicians or families who want to determine how a particular ICS score for an individual child compares with others in the population of children with each of the major cleft subtypes and with or without an identified syndrome. These data showed that ICS scores increased as children matured and that mothers’ understanding of their speech was highest and strangers’ understanding was lowest. Children with CLO achieved the highest ICS scores and those with BCLP scored lowest. The amount of difference and level of importance of the difference in ICS scores varied between each of the cleft subtypes, though across both ages, there was strong evidence to suggest there are differences in ICS scores between children with CLO and those with any form of CP ± L. The higher scores in children with CLO compared to children with any degree of palate involvement reflects the greater impact of anatomical differences in the palate in the production of speech compared to differences in the lip so this finding was not surprising and indeed can be helpful in providing comparator data for children with and without palate involvement. Similarly, it was not unexpected that the most severe cleft subtype, BCLP, was associated with the lowest scores for ICS.
Children with any form of CP ± L who were non-syndromic achieved higher scores on the ICS compared to those who had been diagnosed with a syndrome and the analysis showed strong evidence to suggest a difference in these scores for both ages. As with cleft subtype, this was not unexpected and reflects the involvement of other systems involved in speech, in particular motor and cognitive skills, for children with some types of syndromes.
The median and mean average ICS score in this study for children with any form of cleft palate at 5 years old was 4.14, including those with and without diagnosed syndromes. These scores were very similar to those reported by Ombashi et al. (2023) for children aged between 5 and 7 years old, they reported a mean of 4.08 for children born with CPO and 4.03 for children born with cleft lip and palate. 10 The average scores also compared favourably with other smaller studies of children with CL/P which have reported use of the ICS. Chen et al. (2025) reported median scores of 4.57 for 11 children with cleft lip and palate and 4.29 for 11 children with cleft palate only. 11 Chee-Williams et al. (2025) reported a mean average score of 3.9 for their sample of 30 children aged between 4 and 7 years old with cleft palate. 12
The scores differed from other studies of children born with CL/P though these can be explained by differences in samples. Hashemi Hosseinabad et al. (2022) reported a lower mean ICS score of 3.53 in their sample of 20 children aged 4 to 12 years old. 8 However, all children within the study had velopharyngeal insufficiency, which would most likely have affected their intelligibility, whereas the sample reported in this study reflected a population of children born with CL/P at ages 3 and 5. Mirihagalla Kankanamalage et al. (2023) reported a higher score of 4.6 for their 38 participants born with CL/P, but the children were aged 12 to 15, and therefore it would be expected that scores would be close to ceiling. 13
Data on ICS scores at both ages were available for 574 children. Most children (75.4%) showed an increase in their ICS score over time while another 5.9% showed no change between ages 3 and 5. A further 8.4% showed no change but had scored the maximum possible score at both ages i.e., had no room for improvement. The remaining 10.3% showed a decrease in their ICS scores from age 3 to 5.
Comparison with Typically Developing and Normative Data
Studies reporting mean ICS scores across different languages report a range of 3.68 to 4.26 for 3-year-old children and 4.19–4.78 for 5-year-olds (see Appendix 1 in the Supplementary materials). Those in English for the specific ages are more limited but are reported by Soriano et al. (2023) with mean scores of 4.06 for 3-year-olds and 4.48 for 5-year-olds and McLeod et al. (2015) who reported a mean of 4.3 for 5-year-olds.15,16 The data from Soriano et al. was from typically developing children while the McLeod et al. (2015) used data from a normative sample.15,16
The reference data reported in this study shows that the mean for children born with CLO at both ages (4.10 for 3-year-olds; 4.64 for 5-year-olds) is comparable with the scores from the typically developing and normative samples. In contrast, those with any type of cleft palate had lower mean scores than the typically developing and normative samples (3.64 for 3-year-olds; 4.14 for 5-year-olds). The scores for the different cleft subtypes show variability however suggesting that some children with cleft palate, particularly those with CPO or UCLP, may achieve a mean ICS score within the range of the typically developing and normative studies. Although these data are not from UK children, they are other English-speaking children and show consistency in their scoring.
Change Over Time
The expectation of development is that skill improves over time and that is true for speech as for any other area of interest. The data showed that that was the case for 75.4% of children for whom data were available at both timepoints. What was surprising was the finding that 5.9% of children showed no change between the two time points and another 10.3% obtained lower mean scores at the older age. Moreover, it might be expected that the strongest predictor of the score at 5 years old would be the score at 3 years old but the data suggests that only 50% of the variation in average ICS score at the older age can be attributed to the score at age 3. Results from the Tobit regression suggest that cleft type and syndromic status are also strong predictors in the change of average ICS score from 3 to 5 years old.
Unlike unaffected children, those born with CP ± L may exhibit more variation in their journey towards intelligible speech as a consequence of changes in the anatomy and movement of the palate over time. Some children may be making the expected progress in their speech until a fistula starts to form in the palate or the growth in the pharynx combined with a short velum results in velopharyngeal insufficiency when the soft palate can no longer make an effective seal to close off the nasal cavity. One explanation for the deterioration in ICS scores is if these changes for the individual child occurred after the ICS at age 3 was completed and the required surgery did not take place until after the parent completed the ICS at age 5. Alternatively, it could reflect an increase in a child's language ability, which has extended the length of utterances used, leading to greater difficulty for conversational partners to understand them. Another possibility is that parents have become more aware of their child's intelligibility, possibly as a result of being asked to complete the questionnaire at the first timepoint, and that this has revealed greater problems than they were aware of originally. Of greatest concern is the possibility that these children have particularly severe speech disorders and progress was negligible during the period between the two data collection points. However, these are speculative suggestions and further research is needed to understand this phenomenon.
Other studies reporting ICS data with typically developing and normative samples have generally used cross-sectional designs to sample performance across ages and therefore are not able to measure change in individuals over time. Therefore, no data are available for comparison to determine if the pattern seen with children born with CL/P is replicated in other populations. However, Soriano et al. (2023) in their study of 545 typically developing children aged 2;6 to 9;11 found that increases in average ICS scores across the ages were usually small and incremental. 16 The most change however was seen between the ages of 3 and 5, suggesting a period of rapid change in intelligibility.
Limitations
The data used in this study came from a large-scale cohort study with over 11,000 participants from over 4000 families to date. However, as with many studies using questionnaire data, about one-third of participants responded to the specific questions which provided the data for the analysis. An incentive payment is made to participants which has led to an increase in response rates over time but nevertheless, with over 60% of participants not responding, there is the potential for bias in the sample. Furthermore, whilst the ICS has been selected as a core outcome measure for CL/P 4 it is important to remember that it is parent report rather than an objective measure of intelligibility.
This study investigated intelligibility as interpreted by parents. Children born with CL/P may be intelligible but may still have differences in their speech compared to their non-cleft peers. These differences could be described as affecting the level of ‘acceptability’ of a child's speech. This was not the focus of this paper but it is possible that differences in ‘acceptability’ may have affected how some parents completed the ICS. Objective measures of intelligibility were not included in this study so it is not known how scores on the ICS for this sample compare with any such objective measures.
Clinical Implications
The reference data provided in this paper can be used in clinical settings with 3- and 5-year-old children born with CL/P to determine how their intelligibility compares with other children of the same age and with the same cleft subtype. Moreover, there is the potential to compare against samples of children with cleft palate and with and without an identified syndrome. These data are useful in clinical decision making and identifying children to prioritise for intervention. They also provide a means to discuss with parents who may be concerned to know how their child is doing in comparison to others born with CL/P.
The data also show that children with any type of cleft palate have lower intelligibility in general than other unaffected children and this highlights the need for ongoing support and intervention where needed to reduce this gap. Moreover, the findings from Soriano et al. (2023) suggest there is no need to wait until they have reached 5 years old. 16 The biggest growth in intelligibility naturally occurs between 3 and 5 years old and we should seek to harness that natural spontaneous maturation with intervention whenever it is needed.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656261456526 - Supplemental material for Intelligibility in 3- and 5-Year-Old Children with Cleft Lip and/or Palate: Reference Data for Intelligibility in Context Scale Scores
Supplemental material, sj-docx-1-cpc-10.1177_10556656261456526 for Intelligibility in 3- and 5-Year-Old Children with Cleft Lip and/or Palate: Reference Data for Intelligibility in Context Scale Scores by Amy Davies, Sharynne McLeod and Yvonne Wren in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656261456526 - Supplemental material for Intelligibility in 3- and 5-Year-Old Children with Cleft Lip and/or Palate: Reference Data for Intelligibility in Context Scale Scores
Supplemental material, sj-docx-2-cpc-10.1177_10556656261456526 for Intelligibility in 3- and 5-Year-Old Children with Cleft Lip and/or Palate: Reference Data for Intelligibility in Context Scale Scores by Amy Davies, Sharynne McLeod and Yvonne Wren in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656261456526 - Supplemental material for Intelligibility in 3- and 5-Year-Old Children with Cleft Lip and/or Palate: Reference Data for Intelligibility in Context Scale Scores
Supplemental material, sj-docx-3-cpc-10.1177_10556656261456526 for Intelligibility in 3- and 5-Year-Old Children with Cleft Lip and/or Palate: Reference Data for Intelligibility in Context Scale Scores by Amy Davies, Sharynne McLeod and Yvonne Wren in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
We are grateful to the families who participated in the Cleft Collective study, the UK NHS cleft teams, and The Cleft Collective team, who helped facilitate the study. The views expressed in this publication are those of the author(s) and not necessarily those of The Scar Free Foundation, The Underwood Trust, the Vocational Training Charitable Trust or The Cleft Collective Cohort Studies team.
Authors’ Notes
The findings in this paper were presented at:
Speech and Language Clinical Excellence Network at the Craniofacial Society of Great Britain and Ireland April 2025, Newcastle, UK. International Clinical Phonetics and Linguistics Association June 2025 Patras, Greece.
And will be presented at:
The International Cleft Congress October 2025, Kyoto, Japan.
Ethical Approval and Informed Consent Statements
Ethical approval for the Cleft Collective was obtained from the South West National Research Ethics Service (REC 13/SW/0064). Informed consent to participate in the Cleft Collective was written.
Author Contributions
AD, SM & YW drafted the initial manuscript. AD performed the analyses. AD & YW were involved with data collection. All authors reviewed and edited the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication involves data derived from independent research, The Cleft Collective, funded by The Scar Free Foundation; additional funding was provided by The Underwood Trust and the Vocational Training Charitable Trust (VTCT) (REC approval 13/SW/0064). Further funding was obtained from the Benjamin Meaker Distinguished Visiting Professorship award provided by the University of Bristol.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Governance Statement Omitted from Anonymised Manuscript
The Cleft Collective Cohort Study received ethical approval for recruitment and data collection by the South West Central Bristol Ethics (REC approval 13/SW/0064). Ethical approval for the analysis reported in this paper was obtained from the University of Bristol's Faculty of Health Sciences Research Ethics Committee (REC approval Ref: 18498). Consent for participation was obtained in writing from parents for their own participation and for the participation of their child or children. This study was conducted under project number CC060-YW for the Cleft Collective.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.