
Abstract
Objective
Mercedes Benz craniosynostosis is a multisutural pattern characterized by posterior vault constriction due to fusion of sagittal and bilateral lambdoid sutures. Middle-posterior cranial vault remodeling (MPCVR) and posterior cranial vault distraction osteogenesis (PCVDO) are commonly used to address posterior vault deficiency, but comparative data in this population remain limited. This study evaluates perioperative, volumetric, and craniometric outcomes following MPCVR and PCVDO in Mercedes Benz craniosynostosis.
Design
A retrospective review of computed tomographic images before and 1 year after surgery.
Setting
Tertiary pediatric institution.
Patients, Participants
Eighteen patients with Mercedes Benz craniosynostosis.
Interventions
MPCVR or PCVDO.
Main Outcome Measure(s)
Demographics, operative characteristics, and craniometric measurements.
Results
Eighteen patients were included; 50% underwent MPCVR, 27.8% PCVDO, and 22.2% strip craniectomy. PCVDO demonstrated a significantly shorter operative time than MPCVR (P = .008) and trended toward lower blood loss. MPCVR produced a 50.8% increase in total intracranial volume, with the greatest expansion in the posterior vault (60.6%). PCVDO resulted in a 28.6% total volume increase, with posterior expansion (21.5%). Craniometric outcomes showed MPCVR achieved larger gains in width (20.4%), middle height (19.3%), and posterior height (14.7%), whereas PCVDO produced greater increases in circumference (11.22%), cranial length (15.28%), and vertex angle (18.99%). Both procedures improved skull base angles, with larger reductions observed in the PCVDO group.
Conclusions
MPCVR and PCVDO exhibit distinct expansion patterns in Mercedes Benz craniosynostosis. MPCVR offers broad volumetric remodeling, while PCVDO provides greater longitudinal expansion. These findings support individualized selection of posterior vault techniques for this rare craniosynostosis subtype.
Introduction
Mercedes Benz craniosynostosis is a rare and challenging form of multisutural synostosis characterized by premature fusion of the sagittal and bilateral lambdoid sutures, producing a distinctive tri-armed “Mercedes Benz” configuration of the posterior vault.1-3 The complex craniosynostosis pattern is associated with substantial posterior vault constriction, diminished intracranial volume, and secondary compensatory deformities affecting the cranial base and vault.3-7 Recently, genetic mutations in ERF have been shown to be associated with the tri-sutural pattern of Mercedes Benz craniosynostosis.8, 9 Owing to its rarity, the existing literature is limited to small case series and descriptive reports.
Two of the most commonly employed operative strategies include middle-posterior cranial vault remodeling (MPCVR), which provides immediate expansion through calvarial reshaping, and posterior cranial vault distraction osteogenesis (PCVDO), which gradually expands the vault through distraction forces.3-6 Although both techniques aim to increase intracranial volume and improve the posterior skull contour, they differ in invasiveness and in their approach to skull expansion. Comparative data on surgical techniques for Mercedes Benz craniosynostosis are sparse, and volumetric and craniometric outcomes have not been extensively described.3-6 The present study aims to provide a comparison of perioperative, volumetric, and craniometric outcomes following MPCVR or PCVDO in patients with Mercedes Benz craniosynostosis. By characterizing how each technique influences intracranial volume and cranial dimensions, this work aims to better define procedure-specific advantages to inform decision-making in the surgical care of this complex multisuture craniosynostosis pattern.
Methods
A retrospective review of 3-dimensionally rendered computed tomography (CT) images of patients diagnosed with Mercedes Benz craniosynostosis who underwent MPCVR or PCVDO was performed. Approval was obtained from the University of Texas Southwestern Medical Center Institutional Review Board. Fusion of only the sagittal and bilateral lambdoid sutures was confirmed on CT imaging. No patients with identified syndromic diagnosis, other involved sutures, or any other craniofacial conditions were included. Operative intervention was offered when there was concern for the development of increased intracranial pressure or evidence of progressive craniofacial deformity. The operative approach was selected solely based on the surgeon's preference for MPCVR or PCVDO. Patients presenting with early, significant elevations in intracranial pressure underwent strip craniectomy as an initial intervention to provide timely decompression during infancy and were not included in the analysis of the current study. This approach was undertaken with the understanding that a secondary posterior cranial vault expansion would likely be required at an older age to achieve sufficient intracranial volume augmentation.
Middle-Posterior Cranial Vault Remodeling Technique
A bicoronal incision was made, and a subgaleal dissection was carried posteriorly to just above the torcula, then transitioned to a subperiosteal plane to the inferior occipital constriction, with anterior dissection beyond the coronal sutures and inferior reflection of the temporalis muscles. Parietal and occipital bone flaps were removed, and split calvarial and particulate bone were harvested. An occipital bandeau was harvested and divided in the midline, with parietal flaps replaced orthotopically and occipital flaps rotated 180°. The bandeau was outfractured bilaterally and fixed to the cranial base, creating a gap that was grafted with split calvarial bone. The parietal and occipital flaps were repositioned to widen the biparietal and vertex dimensions and secured with sutures and resorbable plates. Particulate bone was placed into residual gaps. The temporalis muscles were resuspended, and the scalp was closed in layers.
PCVDO Technique
A bicoronal incision was made, and a subgaleal dissection was carried posteriorly to just above the torcula, then transitioned to a subperiosteal plane to the inferior occipital constriction, with anterior dissection to the coronal sutures. A biparietal craniotomy was marked, crossing the lambdoid sutures bilaterally and extending through the interparietal midline and horizontally across the occiput superior to the torcula. Two cranial distraction devices were contoured and placed in a posterior parallel vector, and secured with self-drilling screws, with Gelfoam interposed for dural protection. All distractors were placed in the same vector across patients. Additionally, the midline was opened along its entire length to divide the craniotomy into 2 symmetric halves, and a third cranial distraction device was placed for transverse distraction. 10 The scalp was closed in layers. The distraction protocol consisted of a latency period of 4 to 5 days, followed by 24 to 26 days of activation with 1 mm of daily distraction advancement, and then 4 to 6 weeks of consolidation.
CT imaging was obtained preoperatively and at 1 year postoperatively in a subgroup of patients (5 MPCVR, 5 PCVDO). Only patients with both pre- and postoperative CT imaging were included in the volumetric analysis. Three-dimensional CT images were rendered using Mimics 26 (Materialise NV, Belgium), and intracranial volume was evaluated using 3-Matic (Materialise NV, Belgium). The total intracranial volume was divided into the anterior, middle, and posterior fossa. Tracings from the border of the lesser wings of the sphenoid bone to the border of the cranial vault were used to separate the anterior fossa from the middle fossa. The middle fossa was separated from the posterior fossa by tracing the petrous ridges. Craniometric measurements included circumference, length (glabella—occipital protuberance), width (eurion—eurion), anterior height (nasion—calvarium), middle height (sella turcica—calvarium), posterior height (opisthion—calvarium), vertex angle (nasion—anterior sella turcica—vertex), petrous ridge angle (petrous ridge—sella turcica—petrous ridge), and lesser sphenoid angle (lesser sphenoid—sella turcica—lesser sphenoid) (Figure 1).
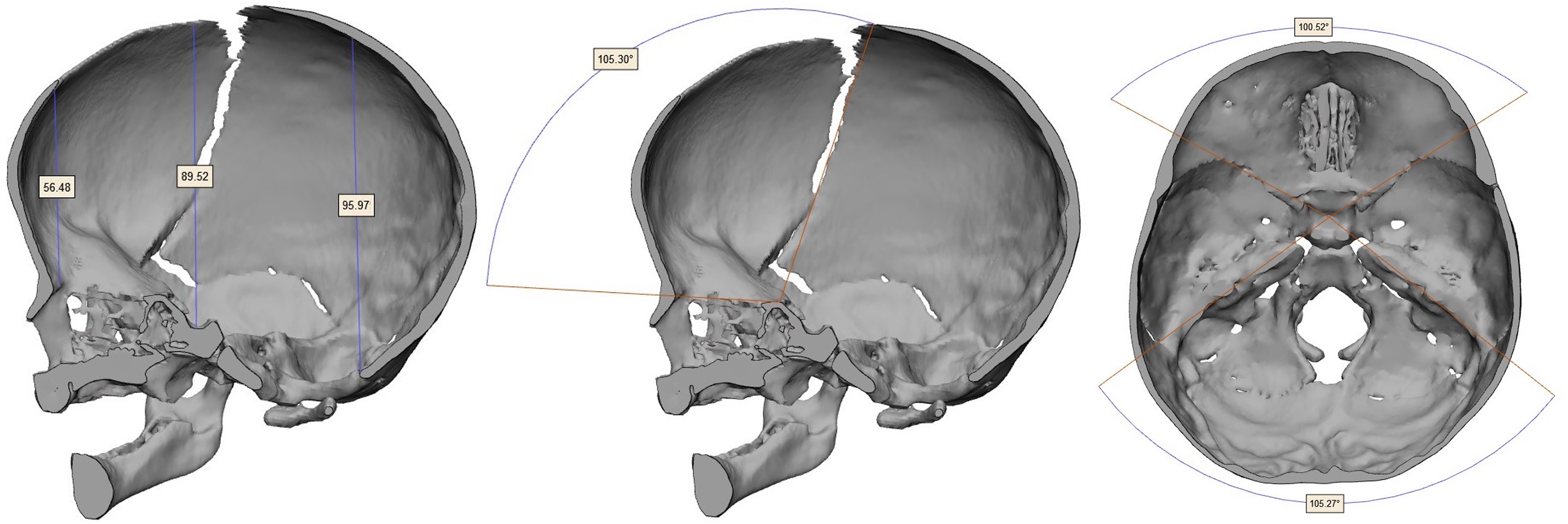
Craniometric measurements in patients with Mercedes Benz craniosynostosis: anterior, middle and posterior height (left), vertex angle (middle), petrous ridge angle and lesser sphenoid angle (right).
Results
Eighteen patients with Mercedes Benz craniosynostosis were included (Table 1). The cohort was 55.6% male and 44.4% female. All patients were White, and 83.3% identified as Hispanic. Nine patients (50.0%) underwent MPCVR, 5 (27.8%) underwent PCVDO, and 4 (22.2%) underwent strip craniectomy. All patients in both groups had identified Chiari malformations preoperatively. Hydrocephalus was noted in 22% of the MPCVR and 40% of the PCVDO groups. Postoperatively, all patients in both groups had stable Chiari malformations, and none had papilledema on ophthalmologic examination. Secondary procedures were common, with 22.2% of MPCVR and 75.0% of strip craniectomy patients requiring a secondary PCVDO procedure.
Demographics of Patients With Mercedes Benz Craniosynostosis.
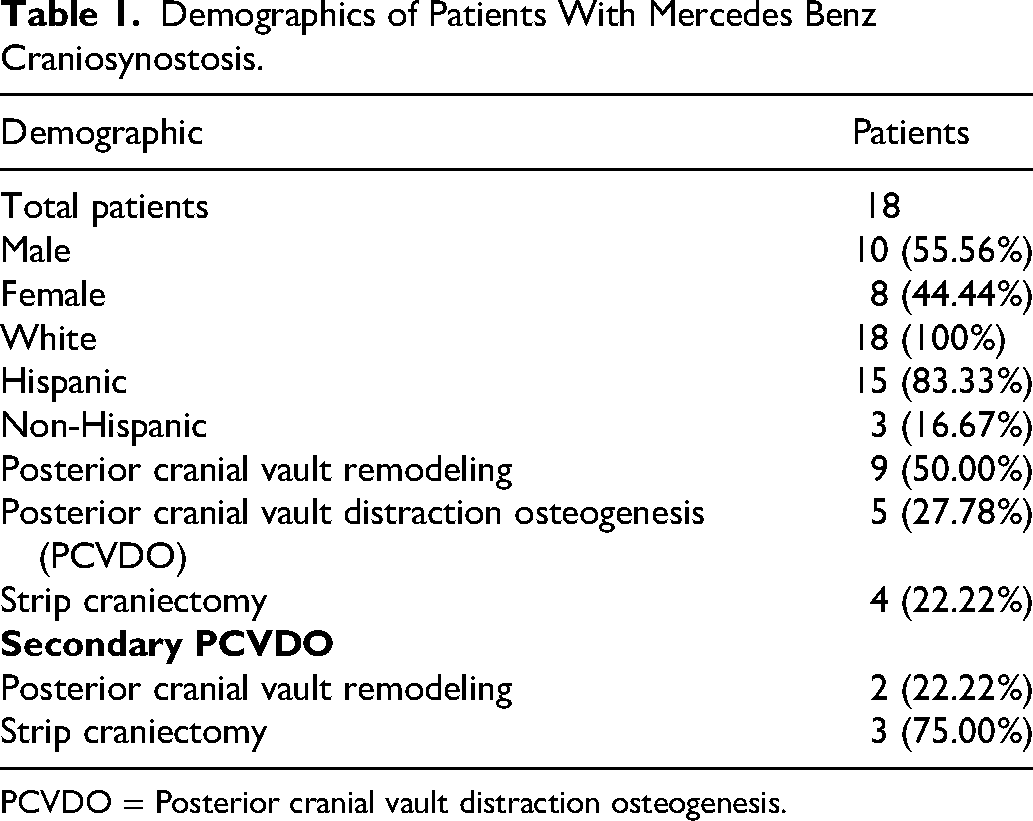
PCVDO = Posterior cranial vault distraction osteogenesis.
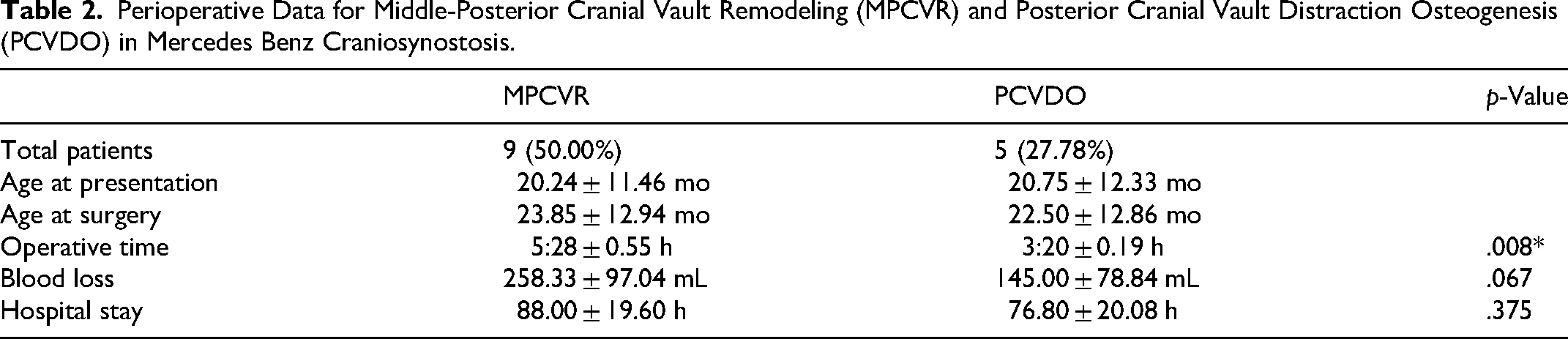
Perioperative characteristics of a subgroup of patients who underwent MPCVR and PCVDO are shown in Table 2. Age at presentation and age at surgery were similar between groups. PCVDO was associated with significantly shorter operative time compared with MPCVR (P = .008). Intraoperative blood loss was lower in the PCVDO cohort than in the MPCVR group, although the difference did not reach statistical significance (P = .067). Hospital length of stay was comparable between groups (P = .375).
Perioperative Data for Middle-Posterior Cranial Vault Remodeling (MPCVR) and Posterior Cranial Vault Distraction Osteogenesis (PCVDO) in Mercedes Benz Craniosynostosis.
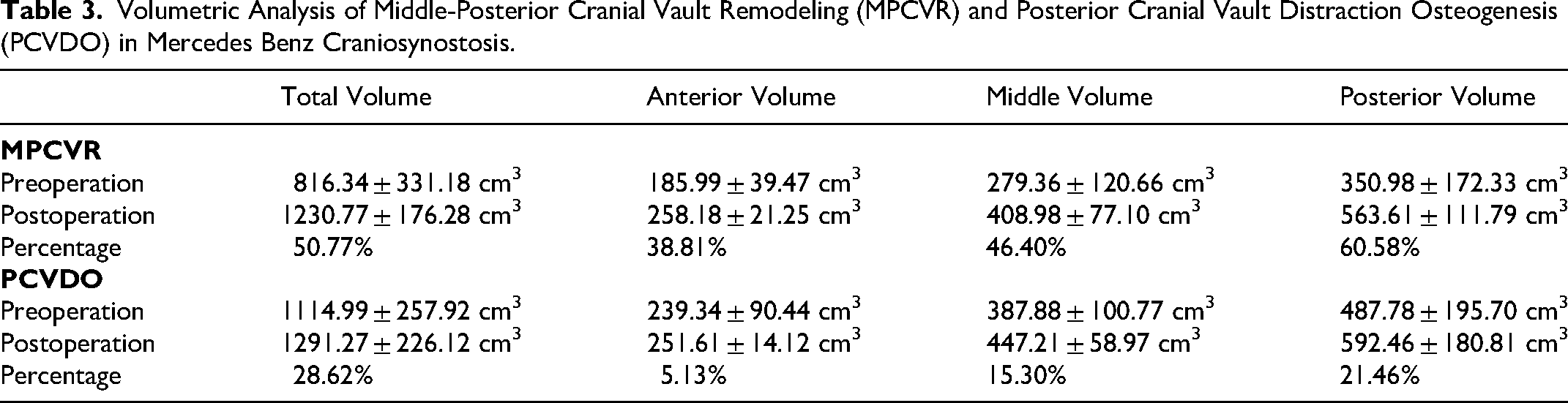
Volumetric analysis is summarized in Table 3. In the MPCVR cohort, total intracranial volume increased from 816.34 ± 331.18 cm3 preoperatively to 1230.77 ± 176.28 cm3 postoperatively, representing a 50.77% gain. The MPCVR group had a lower preoperative total volume than the PCVDO group, but the study was underpowered to detect a significant difference. MPCVR produced substantial increases across all subregions, including a 38.81% increase in anterior volume, 46.40% in middle volume, and 60.58% in posterior volume. In the PCVDO cohort, total volume increased from 1114.99 ± 257.92 cm3 preoperatively to 1291.27 ± 226.12 cm3 postoperatively, representing a 28.62% gain. Volume increases were concentrated primarily in the posterior vault (21.46%), with smaller gains in the middle (15.30%) and minimal change in the anterior vault (5.13%).
Volumetric Analysis of Middle-Posterior Cranial Vault Remodeling (MPCVR) and Posterior Cranial Vault Distraction Osteogenesis (PCVDO) in Mercedes Benz Craniosynostosis.
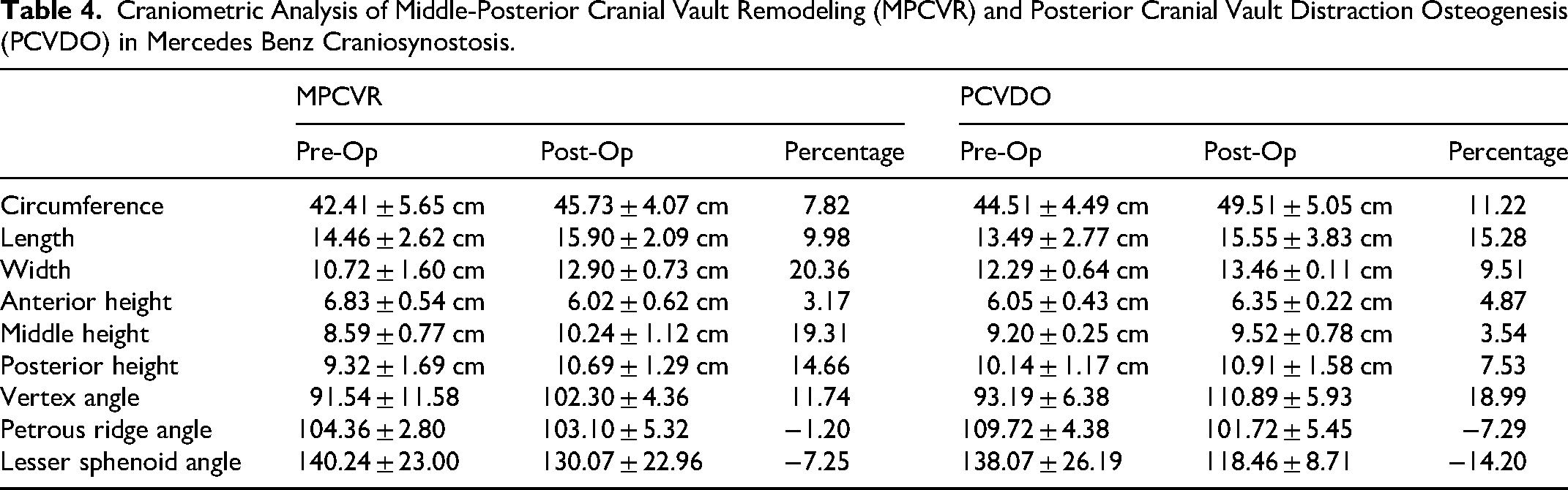
Craniometric outcomes for both groups are shown in Table 4. MPCVR resulted in significant postoperative increases in cranial width (20.36%), middle height (19.31%), posterior height (14.66%), and vertex angle (11.74%). PCVDO showed larger relative increases in circumference (11.22%) and cranial length (15.28%) than MPCVR. PCVDO resulted in greater improvement in the vertex angle (18.99%) and larger reductions in the lesser sphenoid angle (−14.20%) and the petrous ridge angle (−7.29%) compared with MPCVR.
Craniometric Analysis of Middle-Posterior Cranial Vault Remodeling (MPCVR) and Posterior Cranial Vault Distraction Osteogenesis (PCVDO) in Mercedes Benz Craniosynostosis.
Discussion
Mercedes Benz craniosynostosis represents a rare and complex form of multisutural cranial deformity, and operative strategies remain heterogeneous due to limited published data and variable cranial morphology. In this study, we present one of the most extensive series to date evaluating MPCVR and PCVDO in this population, with volumetric and craniometric comparisons. Our findings highlight meaningful differences in operative characteristics and postoperative cranial morphology that can help guide surgical decision-making. Secondary operations were relatively common in our study and the previous literature, underscoring the need for improved understanding of the differences in posterior vault techniques in Mercedes Benz craniosynostosis. 6
When comparing perioperative outcomes, PCVDO was associated with significantly shorter operative time than MPCVR and a trend toward lower blood loss. However, this did not reach statistical significance. These findings align with prior literature describing distraction as a less invasive technique that gradually distributes expansion to the postoperative period.11-13 Length of stay was comparable between groups, suggesting that the externalized distractors and activation phase of PCVDO do not impose additional inpatient burden.
Volumetric outcomes revealed important distinctions in how MPCVR and PCVDO reshape the cranial vault. MPCVR produced substantial increases across all cranial subregions, with the most significant relative gain observed in the posterior vault, consistent with the procedure's design to provide immediate, expansive remodeling. In contrast, PCVDO achieved more modest volumetric gains overall, with the most pronounced changes again concentrated in the posterior vault. The MPCVR group had a lower preoperative intracranial volume than the PCVDO group. Clinically volumetric analysis was not used directly for surgical decision-making, but it may have indirectly influenced decision-making through a more restricted cranial size. Our findings are similar to those by Marji et al., who demonstrated a 25.9% increase in total intracranial volume following PCVDO in 4 patients with Mercedes Benz craniosynostosis. 4
PCVDO is often preferred over anterior cranial vault remodeling techniques in patients with significant intracranial volume deficiency, as it offers superior expansion.14-17 However, volumetric comparison between PCVDO and MPCVR is limited. We found greater overall volumetric expansion in MPCVR than in PCVDO, including in the posterior fossa. The tri-sutural synostosis creates a severely constricted occipital coning that is not directly addressed by the osteotomies and posterior translation performed in PCVDO but is released and remodeled during MPCVR. Notably, anterior and middle volumes showed less expansion with PCVDO, suggesting that its expansion effect is more localized in the posterior vectors. In contrast, MPCVR may redistribute and enlarge the vault more globally, leading to increased volumetric expansion. Furthermore, the patients in our cohort had delayed presentation and older age at surgery, which is associated with diminished volume expansion and decreased ossification following PCVDO.18-20 Additional gains may also be achieved with an infratrocular osteotomy compared to the supratrocular osteotomy used at our center. 21 However, even with the greater expansion achieved in MPCVR, we found that 22% required a secondary posterior cranial vault expansion. This distinction between MPCVR and PCVDO is essential when selecting an operative approach based on individual patient morphology, which can vary based on whether the synostosis of the sagittal or the bilateral lambdoid sutures is the primary driver of cranial dysmorphology.5-7
Craniometric analysis further demonstrated the differences between techniques. MPCVR resulted in substantial increases in cranial width and middle/posterior height, consistent with immediate reshaping of the posterior contour. Rhodes et al reported a trend toward a more brachycephalic skull shape in 6 patients following MPCVR, but this difference was not significant. 3 PCVDO, while also increasing width and height, did so to a lesser degree, except for overall cranial length, which increased to a greater extent than MPCVR. Marji et al reported a greater increase in posterior height in 4 patients undergoing PCVDO, likely due to a posterior-superior vector rather than the posterior vector of the distractors used in our study. 4 Additionally, both procedures improved the vertex angle, with PCVDO demonstrating a larger relative increase, likely due to the greater length expansion associated with distraction. Changes in skull base angles showed decreases in both groups, though more prominently with PCVDO. The gradual distraction of the posterior cranium allows controlled expansion, transmitting tension to the cranial base, leading to greater remodeling.18, 22 The posterior cranial base changes to the foramen magnum and expansion additionally have potential benefits of resolving Chiari malformations which are commonly associated with Mercedes Benz craniosynostosis.3,23,24
Strip craniectomy was reserved for infants who presented at a young age with severe clinical or radiographic signs of elevated intracranial pressure, in whom immediate decompression was prioritized over definitive cranial vault reshaping. In these patients, limited strip craniectomies were performed to release the fused sutures and rapidly alleviate intracranial hypertension. This approach was undertaken with the understanding that strip craniectomy likely serves as a temporizing intervention rather than a definitive solution in the setting of Mercedes Benz craniosynostosis, given the extent of multisutural involvement and posterior vault constriction. As expected, the majority of these patients ultimately required secondary calvarial expansion at a later age to achieve adequate intracranial volume augmentation and durable morphologic correction. Secondary surgery was common following initial strip craniectomy, with 75% of patients subsequently undergoing PCVDO. In contrast to our experience, Hartman et al, reported that no patients treated with strip craniectomy required a secondary procedure in a series of 7 patients with Mercedez Benz craniosynostosis. 25
Patients in our cohort undergoing MPCVR were observed to undergo secondary surgery more often than those treated with PCVDO. Although cranial vault remodeling can achieve larger immediate increases in intracranial volume, over time relapse and diminished cranial growth required secondary intervention due to head shape in 2 patients. In contrast, distraction osteogenesis provides more gradual expansion with ongoing bone formation, which may reduce the likelihood of requiring additional surgical intervention. The majority of patients in our cohort presented at older ages, which may be due to the posterior sutures and, specifically, Mercedes Benz craniosynostosis, often having less noticeable deformities that may become more prominent with growth.5,26 If presenting early without the need for immediate decompression, our protocol would be to delay treatment until either MPCVR or PCVDO can be performed, with the choice of operation based on patient-specific needs for cranial deformity.
This study is limited by its small sample size due to the rarity of Mercedes Benz craniosynostosis. The cohort size limits the ability to perform statistical analysis comparing volumetric and craniometric variables. Additionally, the surgeon's bias in selecting the surgical intervention for each patient limits comparisons between techniques. However, the findings provide insight into the postoperative changes that occur following MPCVR and PCVDO in Mercedes Benz craniosynostosis. Larger multicenter studies and the incorporation of long-term volumetric and craniometric outcomes will further clarify statistical differences in postoperative morphology and changes over time due to growth and remodeling.
Conclusion
MPCVR and PCVDO in our study were found to differ in the treatment of patients with Mercedes-Benz craniosynostosis. MPCVR provided more widespread volumetric expansion, with improvements in posterior height and width, which may be advantageous for patients with posterior constriction or global cranial volume deficiency. PCVDO offers a shorter operative time and greater gains in length, potentially benefiting patients who need gradual, posterior directional growth and reduced operative morbidity. However, surgeon bias in technique selection for each patient should be kept in mind.
Footnotes
Ethical Statement
Institutional review board approval was granted for the current study.
Author Contribution Statements
LMH, RRH, AAK, and PSM contributed to project design. LMH and RRH performed data collection. LMH, RRH, AAK, and PSM performed data analysis and manuscript development.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.