
Abstract
Follow-up appointments are crucial for maintaining continuity of care, yet patients often encounter various barriers to accessing these services. In this study, we examine the potential of telemedicine applications for follow-up care (tele-follow-up), focusing on its impact on care access, service efficiency, and care quality. By collaborating with a large hospital that implemented tele-follow-up services across departments over time, we employ a staggered difference-in-differences design to identify the causal effects of tele-follow-up services. Our findings indicate that the adoption of tele-follow-up services increases total follow-up volume by 48.14%. Notably, we identify positive spillover effects on traditional onsite care, with onsite follow-up visits and initial visits increasing by 14.11% and 7.90%, respectively. We further investigate the mechanism underlying these results. On the demand side, patients with higher costs of accessing onsite follow-up care, such as those living in rural areas or with comorbidities, exhibit greater demand elasticity following the availability of the tele-follow-up channel. On the supply side, dedicating the telemedicine channel exclusively to follow-up care enhances physicians’ efficiency by enabling more focused practice across online and in-person work shifts. The increased access to follow-up services enabled by telemedicine further translates into better patient outcomes, as evidenced by a significant reduction in readmission rates. Our study demonstrates the value of tele-follow-up services and offers practical insights for healthcare decision-makers seeking to leverage digital health to enhance continuity of care.
Keywords
Introduction
In healthcare, follow-up refers to the act of providing continued care and monitoring to support patients after their initial medical evaluation or treatment. Follow-up care is an indispensable part of the care process and carries various benefits. According to the Agency for Healthcare Research and Quality, appropriate follow-up allows physicians to clarify misunderstandings, monitor patient conditions, identify complications, make further assessments, and adjust treatments (AHRQ, 2024). Timely check-ups and assessments by physicians have been shown to improve patient outcomes by reducing readmission (Brooke et al., 2014). Touching base with patients through follow-up appointments also helps improve patient-provider working relationships and medication adherence (Lindquist et al., 2012). Despite its importance, patients often lack access to timely follow-up care due to various barriers, such as transportation issues, lack of health insurance, and limited assistance from the front desk in scheduling follow-up appointments upon discharge (Misky et al., 2010). Failure to follow up not only poses risks to patient health but also triggers potential negligence claims against healthcare practitioners under medical liability (Callen et al., 2012). Hence, healthcare practitioners strive to encourage follow-up attendance, and the key is to ensure convenient access.
Telemedicine offers a potential solution to improve follow-up attendance, particularly by addressing transportation and logistical barriers. First, by enabling real-time interactive communication between patients and providers from remote locations, telemedicine offers a viable alternative for those facing transportation barriers. This includes individuals who face long travel distances, lack access to reliable transportation, are unable to drive, or have other mobility constraints. Such barriers are particularly pronounced in rural and underserved areas, where healthcare facilities may be sparsely located. Second, telemedicine significantly reduces travel and time costs, which can otherwise deter follow-up adherence. Instead of spending hours commuting, waiting, and navigating hospital systems, patients can receive virtual consultations from work or home. Such convenience especially appeals to patients with demanding schedules and caregiving responsibilities.
While telemedicine has shown great potential in several healthcare settings (Ekeland et al., 2010; Landro, 2021), evidence regarding its specific impact on follow-up care is limited thus far. Our paper thus aims to provide further analytics on the application of telemedicine applications for follow-up care (hereinafter, tele-follow-up). In particular, we will answer the following questions: Does the availability of the tele-follow-up channel improve patients’ access to follow-up care? Will the tele-follow-up channel affect patients’ demand for initial care? If yes to the above questions, what are the underlying mechanisms?
Toward these goals, we collaborate with a leading hospital in China, which serves approximately 11 million people in the region. The hospital first adopted the tele-follow-up service in the department of neurology on August 24, 2018, and subsequently extended the service to the department of primary care on March 11, 2019. Leveraging the difference-in-differences (DiD) design, we examine the impact of telemedicine on patient access to care, measured by the weekly patient volume to a department. In the analysis, we differentiate visits via online (i.e., telemedicine) and onsite (i.e., in-person) service channels and purposes of appointments (i.e., initial versus follow-up care).
We show that tele-follow-up adoption significantly increased total follow-up visits by 48.14%, highlighting telemedicine’s potential to facilitate access to follow-up care. More interestingly, the adoption of the tele-follow-up channel also generates positive spillover effects on the onsite demand, with onsite follow-up visits increasing by 14.11% and onsite initial visits increasing by 7.90%. These results thus suggest that the tele-follow-up channel not only improves access to follow-up care but also attracts more patients to the hospital for initial care. Our findings remain consistent through extensive robustness checks, including propensity score matching (PSM), instrumental variable (IV) analysis, falsification tests, and alternative models.
While the positive effect on follow-up care aligns with theoretical expectations and the hospital’s initiative, the spillover effects on the onsite channel are less intuitive. Through mechanism tests, we show that the effect of the tele-follow-up channel is strongest among patients with a consistent need for follow-up services yet face higher costs accessing in-person services. Additionally, the rise in initial visits was primarily driven by rural patients with comorbidities, who are most incentivized to seek both initial and follow-up care at the hospital. The findings corroborate the underlying mechanisms: patients with a higher cost of accessing onsite follow-up care are more likely to value telemedicine, and their demand elasticity is thus larger. Moreover, the adoption of the tele-follow-up channel enhances physicians’ service efficiency, evidenced by a significant reduction in service time for follow-up visits. The increased access to follow-up services enabled by telemedicine also improves patient outcomes, as evidenced by a significant reduction in readmission rates among adopting patients. These findings further reinforce the value of tele-follow-up applications for both providers and patients.
Literature review
The second stream examines the impact of telemedicine on patient visit behaviors. For example, Bavafa et al. (2018) demonstrate that e-visits via secure messaging can increase the volume of office visits. Çakıcı and Mills (2021) find that teletriage may improve cost outcomes for patients with high uncertainty regarding their health conditions, but the rate of arrivals to the emergency department may increase when the overtriage rate exceeds 5%. Huang et al. (2021) show that the integration of online-offline service increases online demand but decreases offline demand using evidence from an e-healthcare platform in China. By contrast, Fan et al. (2023) show that opening an online consultation service increases demand for doctors’ offline appointments, because doctors with online consultation services signal their willingness to communicate with patients. Tushe et al. (2025) find that adding an asynchronous telemedicine channel led to a sorting effect: more complex patients were directed to in-person visits, which improved efficiency in handling referrals and common medically necessary procedures. Zang et al. (2024) formulate patients’ strategic choices between telemedicine and in-person care as a queueing game and characterize the game-theoretic equilibrium and the socially optimal patients’ choices. Other studies have explored the unintended consequences of telemedicine adoption on patients. For example, Qin et al. (2025) find that telemedicine visits are associated with lower service completion rates when delays occur compared to in-person visits. Sunar and Staats (2022) highlight that telemedicine can exacerbate health disparities between low- and high-income patients, even when there are no technology access disparities between those groups.
The third stream focuses on healthcare providers, examining how telemedicine adoption influences their behavior, workload, and financial outcomes. Similarly, Wang et al. (2020) study physicians’ online–offline behavior dynamics, demonstrating that online activities can boost offline service volumes, whereas offline activities may limit online services due to resource constraints. Rajan et al. (2019) explore the speed-quality trade-off for physicians when managing chronic patients with telemedicine as part of their practice. Sun et al. (2020) show that telemedicine applications in emergency rooms can enable flexible allocation of physician resources, thus alleviating overcrowding and improving efficiency. Zhou et al. (2024) examine the effect of the state’s entry into the Interstate Medical Licensure Compact, showing that urban providers financially benefited more than rural providers from expanded telemedicine opportunities. Kim et al. (2023) investigate how telemedicine influences physician prescription decisions, finding lower antibiotic prescription errors via telemedicine.
First, this study contributes to the growing literature on telemedicine by investigating telemedicine as a solution to enhance follow-up care. We utilize granular data to differentiate between follow-up visits and initial visits, an important distinction that has received limited attention in the existing literature. Extending prior findings on telemedicine’s substitution effect for in-person visits (Ayabakan et al., 2024; Bavafa et al., 2018), our study uncovers a cross-type spillover effect: the adoption of the tele-follow-up service channel drives increased demand for initial care. These nuanced patient-flow dynamics provide valuable guidance for healthcare decision-makers, enabling more effective workforce planning and scheduling.
Second, our study complements prior research that primarily focuses on telehealth delivered through third-party, on-demand platforms (Fan et al., 2023; Huang et al., 2021; Wang et al., 2020). These platforms often rely on asynchronous text- or audio-based e-visits. In contrast, our research examines a hospital-integrated telemedicine system in which patients schedule telemedicine visits with the hospital in the same way as in-person appointments. Real-time video conferencing consultations closely resemble traditional in-office visits, effectively minimizing concerns about the quality of virtual care and physician self-selection.
Third, while previous studies have shown that telemedicine improves operational efficiency through flexible resource allocation (Sun et al., 2020), we use “focused practice” as a mechanism to explain how telemedicine further enhances service efficiency. By directing a substantial portion of follow-up appointments to the telemedicine channel, physicians experience a more homogeneous patient mix within online and offline care settings. This reduces the cognitive and logistical demands of alternating between initial and follow-up care during a work shift. Hence, our work contributes to the broader literature of physician task-switching, workflow efficiency, and focused operations (Celik et al., 2024; Clark and Huckman, 2012; Kc and Terwiesch, 2011; Narayanan et al., 2009), highlighting telemedicine as a tool for enhancing focus and operational efficiency.
Finally, aligning with the call for research on technological innovations and inclusive health (Sunar and Swaminathan, 2022), we demonstrate how tele-follow-up services help improve accessibility, particularly for disadvantaged patients who face transportation barriers or have chronic conditions. By enhancing access while ensuring efficiency, our findings offer actionable insights for healthcare providers seeking to balance equity and operational performance.
Hypothesis development
This section develops hypotheses on how telemedicine influences patients’ access to care, distinguishing by visit type (follow-up vs. initial) and modality (telemedicine vs. in-person).
When telemedicine becomes available for follow-up care, it has the potential to enhance access to follow-up services through two key mechanisms. First, telemedicine reduces the challenges associated with getting to an in-person appointment. Transportation barriers, often cited as a primary reason patients skip follow-up care (Misky et al., 2010), are minimized with telemedicine. Accordingly, patients who previously had difficulty reaching doctors’ offices can now attend follow-up appointments virtually, eliminating the need for travel and its associated costs. Second, telemedicine constitutes a simple, flexible, and convenient manner of delivering care compared to onsite visits. Unlike traditional onsite follow-up visits, where patients typically undergo a long and exhausting process from onsite registration, extended waiting for treatment and checking out, the visit process is much smoother in the virtual space. For instance, the “virtual waiting room” during a telemedicine visit shortens patients’ actual waiting time. According to the hospital in our study, when patients enter the virtual waiting room, they can monitor their position in the queue and receive real-time reminders through text messages and app notifications about their turn. Such features not only reduce the perceived waiting time but also allow patients to complete follow-up visits during breaks at work or from the comfort of home (Maister, 1984). Such flexibility particularly appeals to patients sensitive to the time costs of accessing onsite care.
While telemedicine seems to have great potential in increasing patients’ access to follow-up care, in practice, it may not function as intended due to several sources of friction. For instance, some patients may hesitate to utilize telemedicine if they worry that virtual communication is less effective than an in-person visit or are concerned about technological glitches that might disrupt the treatment session via telemedicine. Even if patients are willing to use telemedicine, the lack of IT literacy, mobile devices, or broadband access may hinder patients’ effective use of tele-follow-up services. These factors could limit the effectiveness of telemedicine in expanding patients’ access to follow-up care. Thus, while telemedicine holds promise, its impact on access to follow-up care remains an empirical question. To investigate this, we propose the following hypothesis:
Follow-up
The adoption of tele-follow-up channel increases patients’ demand for follow-up care
The introduction of the tele-follow-up service may further influence onsite care demand. Depending on the purpose of visits, patients’ preferences and choices may shape the onsite demand differently for follow-up and initial visits. Accordingly, we separately elaborate on the possible changes in the department-level patient volume for onsite follow-up (Hypothesis 2) and initial care (Hypothesis 3).
For patients, the tele-follow-up service could substitute or complement onsite follow-up care. In our research context, the telemedicine service enables real-time communication between patients and physicians via video conferencing, thereby replicating the in-person experience. Given the significant convenience and cost reductions in transportation, patients may consider tele-follow-up as a substitute for onsite follow-up and switch from onsite to online channel, thereby reducing onsite follow-up visits. On the other hand, tele-follow-up services could complement onsite follow-up care. First, according to the literature, the use of e-visits (i.e., secure messaging) will lead to more frequent in-person visits, as increased communication through e-visits makes physicians feel obligated to see patients in the office and encourages them to schedule additional onsite appointments for thorough evaluations (Bavafa et al., 2018). Second, telemedicine can serve as a gateway for identifying health issues that require further evaluation and physical examination. For example, a physician conducting a telemedicine follow-up for a diabetic patient may detect early complications, necessitating an onsite follow-up visit for additional lab tests. Similarly, patients with conditions like pediatric epilepsy may need periodic onsite evaluations for neurological assessments, vital signs monitoring, and physical exams for muscles, reflexes, and gait. Given the potential for both substitution and complementarity, the net effect of tele-follow-up adoption on onsite follow-up care demand remains uncertain. Hence, we propose the following hypothesis for empirical testing:
Onsite Follow-up
The adoption of tele-follow-up channel increases patients’ demand for onsite follow-up care
Tele-follow-up services may also generate positive spillover effects on demand for initial visits. According to our collaborating hospital, some patients hesitate to go to the hospital for initial diagnoses because of the inconvenience and high costs associated with follow-up care, particularly for whom the cost of an in-person follow-up visit is prohibitive (such as rural patients). As such, even though the care quality from our collaboration hospital is higher, patients may opt for a more accessible but lower-quality local clinic to avoid the potential burdens of follow-up appointments. Telemedicine may alleviate such concerns by lowering the cost and inconvenience of follow-up care, making the hospital a more attractive option for initial care. In sum, tele-follow-up services could increase the demand for onsite initial care by addressing patients’ concerns about the overall care process. To test this potential spillover effect, we propose the following hypothesis:
Initial Visit
The adoption of tele-follow-up channel increases patients’ demand for initial care
If tele-follow-up services influence patient behaviors in seeking onsite follow-up and initial care, as hypothesized above, the magnitude of the impact is likely contingent on patient characteristics. Specifically, patients who face higher costs of accessing onsite follow-up care are expected to show a stronger preference for telemedicine. Thus, their demand elasticity for tele-follow-up service will be greater. We focus on two key proxies for the cost of accessing onsite follow-up care: (i) transportation costs and (ii) the presence of chronic comorbidities. Patients with higher travel costs to onsite services, such as long travel distances to the hospital or a lack of automobiles, are more sensitive to the costs of in-person follow-up visits. Consequently, these patients will be more inclined to choose telemedicine services, especially when considering the overall costs of follow-up care in deciding where to seek initial treatment. Similarly, patients with chronic conditions often require routine follow-up care to monitor their health. For these patients, the cumulative costs of repeated follow-up visits are likely a crucial consideration in their choices of providers for initial care. The availability of tele-follow-up services reduces these recurring costs, thereby making the hospital a more attractive option for both initial and follow-up care. To sum up, this mechanism suggests that telemedicine could serve as a key lever to expand access to care, especially for patients with high sensitivity to in-person visits and a need for regular follow-up services. Accordingly, we propose the following hypothesis for empirical testing:
Heterogeneity
The effect of tele-follow-up channel is larger for patients with higher cost sensitivity to onsite follow-up care
Research background and data
We obtain data from a leading teaching hospital that provides primary and specialty care in China. The lack of follow-up attendance has been a longstanding issue in the hospital, even with providers informing patients about the necessity of follow-up appointments. Patients often ignore or skip such services for various reasons, such as transportation barriers to accessing onsite service and the lack of literacy regarding the importance of follow-up care. To improve patients’ access to follow-up care, the hospital adopted telemedicine, which is exclusively for follow-up services. The hospital confirmed that no other service changes occurred at either the department or hospital level during the study period. This ensures that telemedicine adoption was the sole intervention within the sample window, spanning February 2018 to December 2019.
The hospital initiated the tele-follow-up service in the department of neurology on August 24, 2018, and subsequently, extended this service to the department of primary care on March 11, 2019. According to the hospital, neurology and primary care departments were chosen for the rollout because they serve patients with chronic conditions requiring ongoing monitoring and management, such as pediatric epilepsy, neurodevelopmental delay, movement disorders, growth disorders, and mental health conditions. The hospital viewed telemedicine as suitable for non-urgent follow-up needs in these departments and believes that tele-follow-up services would not compromise care quality. Nonetheless, the hospital informed us that other departments may also be valid candidates for piloting telemedicine, such as endocrinology, dermatology, and ophthalmology, as their patients also require routine follow-up care and the liability risk of virtual care is minimal. It is worth noting that no financial incentives were provided to patients or providers for using telemedicine. The hospital established the necessary infrastructure and training for the practitioners involved, ensuring a seamless transition. Moreover, the cost to patients and the payment to physicians are identical per visit regardless of the modality (i.e., telemedicine or in-person visit). Therefore, the research setting is free from concerns related to physician self-selection.
Before the adoption of telemedicine, all follow-up care was conducted exclusively through in-person visits. With the introduction of telemedicine, patients gained the option to choose between telemedicine and in-person visits for follow-up care, and the scheduling process remained the same for both modalities. Patients accessed the hospital’s app portal to view available appointments and select their preferred care modality. Feedback from patients revealed minimal technological challenges with scheduling telemedicine visits, as the app portal was already well-established and widely utilized for appointment scheduling prior to our study. In our analysis, the treatment group includes the Department of Neurology and the Department of Primary Care. The control group comprises the remaining 22 hospital departments, excluding Emergency Care. Specifically, the control group encompasses a wide range of specialty care services, including Cardiology, Dermatology, Endocrinology, ENT (Otolaryngology), Gastroenterology, Ophthalmology, Pulmonology, Psychiatry, Urology, Hematology, Oncology, General Surgery, and Rehabilitation Medicine.
Figure 1 illustrates the process for scheduling and attending a tele-follow-up visit. Specifically, Figure 1(a) illustrates the app interface when scheduling a tele-follow-up appointment, and Figure 1(b) displays the appointment confirmation page. Around the scheduled appointment time, patients receive a text notification and can initiate the virtual visit by clicking the “Enter” button on the confirmation page. During the virtual visit, patients and physicians communicate in real-time via audio and video features (see Figure 1(c)), with physicians able to upload relevant files for patients to download and review. After completing the follow-up visit, physicians may prescribe medications and patients can arrange for the medication delivery to home (see Figure 1(d)). With its real-time, interactive video conferencing capability, the tele-follow-up service closely replicates the experience of an in-office visit. Patients share symptoms, medications, and other relevant information, while physicians adjust treatment plans, prescribe medications, and order lab tests as needed.
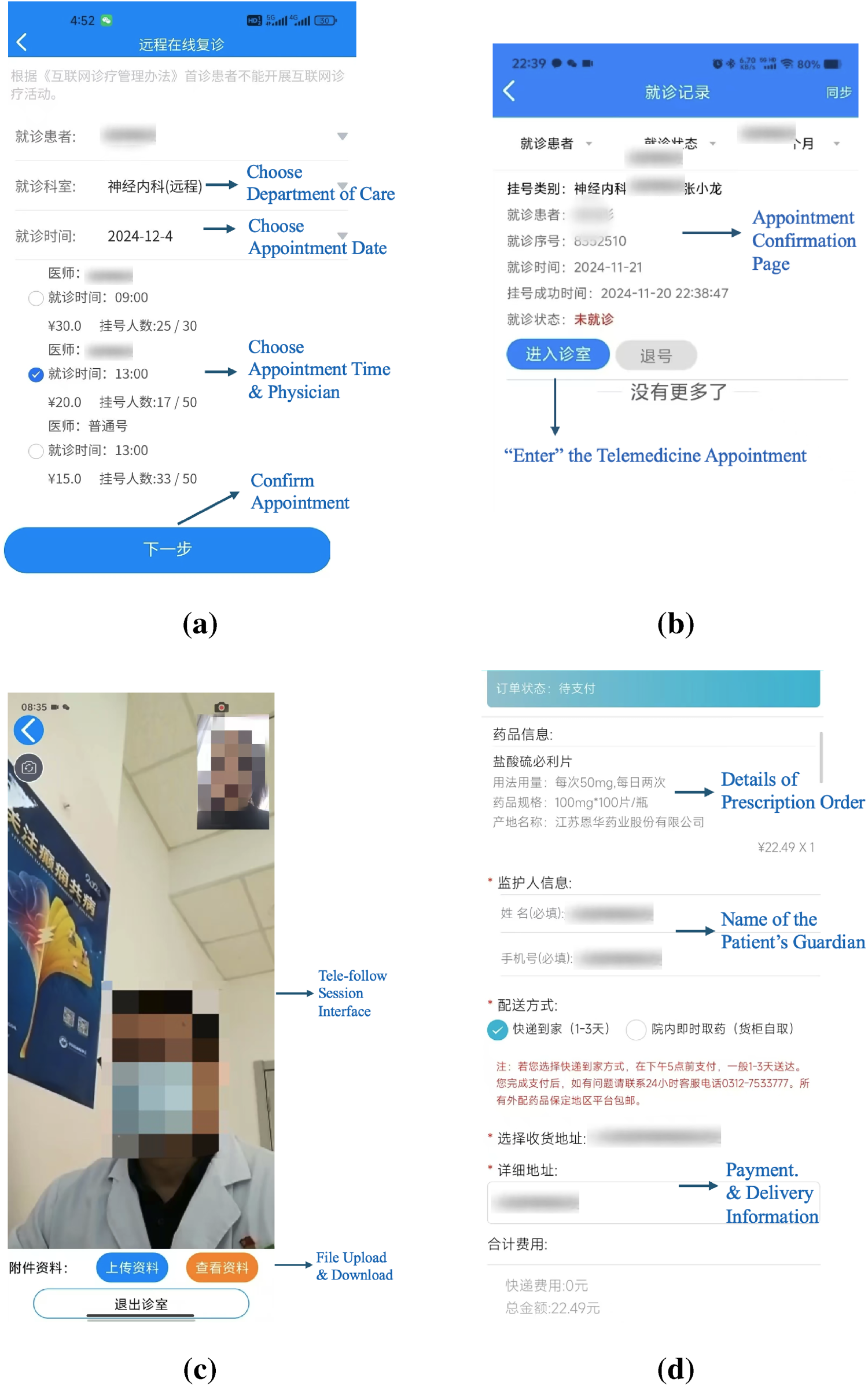
User interface of the tele-follow-up app. Notes. The figure illustrates the flow and user interface of a tele-follow-up visit. To protect patient privacy, we removed key identifying information of patients and physicians from the screenshots.
The primary outcome variable, patient volume, measures access to care, a key factor related to hospital efficiency (Athanassopoulos and Gounaris, 2001), healthcare costs (Freeman et al., 2021), and patient health outcomes (Begg et al., 1998; Gaynor et al., 2005; Halm et al., 2002). We calculate patient volume as the number of outpatient encounters by department and week, which captures the weekly patient demand by each department.
When scheduling an appointment, patients can choose either initial visit or follow-up visit. According to the hospital, an initial visit refers to a patient’s first consultation with a physician about a new or emerging health concern. Such visits are typically more comprehensive and take a long time, as the physician needs to gather detailed information about the patient’s medical history, current health issues, and any relevant diagnostic or laboratory results. A follow-up visit refers to check-ups following an initial visit, as part of the same care episode. Follow-up visits focus on evaluating treatment effectiveness, monitoring recovery progress, and making necessary adjustments to the treatment plan or medications. The hospital defines a care episode as a 3-month period, and visits that occur within 3 months following an initial visit are considered a follow-up appointment. If patients require medical attention beyond a care episode, they are generally advised to schedule a new initial visit unless otherwise directed by their physician.
For better illustration of initial and follow-up visits, we visualize an example visit trajectory in Figure 2, with
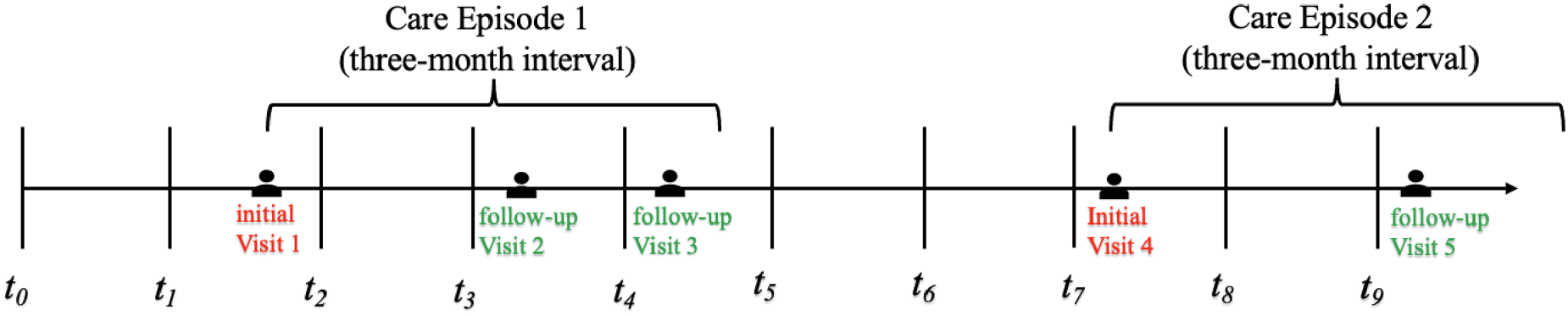
Visualization of a patient’s trajectory.
We further distinguish onsite from telemedicine visits. Before telemedicine adoption, there were two types of encounters: onsite initial and onsite follow-up visits. After telemedicine adoption, there are three types of encounters: onsite initial, onsite follow-up, and tele-follow-up visits. Correspondingly, we have three outcome measures for empirical tests—Total Follow-up Volume, Onsite Follow-up Volume, and Onsite Initial Volume—by department and week. Before telemedicine adoption, Total Follow-up Volume is equal to Onsite Follow-up Volume. After telemedicine adoption, Total Follow-up Volume comprises a mix of telemedicine and onsite follow-up visits for the treatment departments. Table 1 shows the summary statistics of the key variables by the treatment and control groups before and after telemedicine adoption. We control for patient characteristics including health status (measured by the Charlson Comorbidity Index,
Summary statistics.
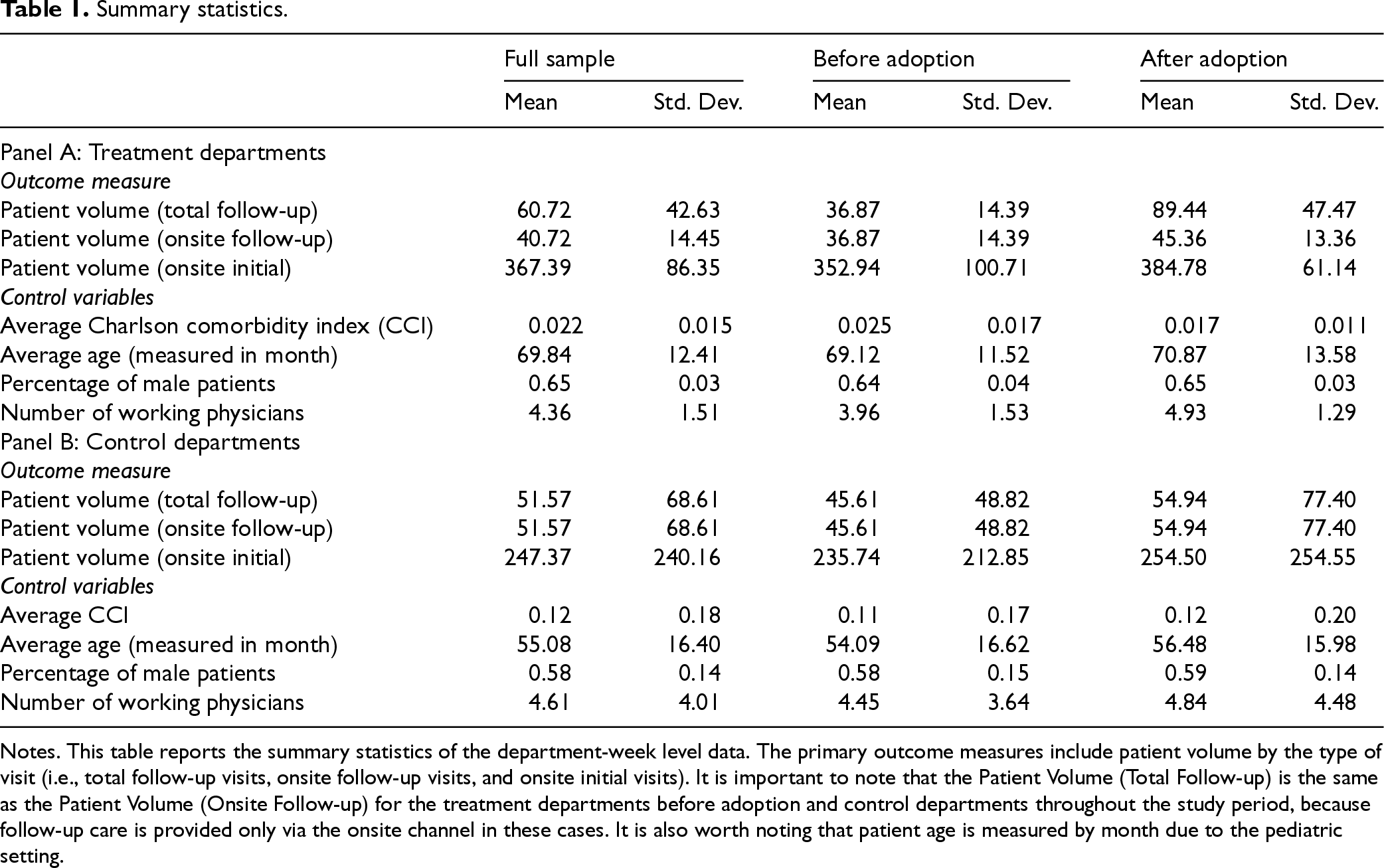
Notes. This table reports the summary statistics of the department-week level data. The primary outcome measures include patient volume by the type of visit (i.e., total follow-up visits, onsite follow-up visits, and onsite initial visits). It is important to note that the Patient Volume (Total Follow-up) is the same as the Patient Volume (Onsite Follow-up) for the treatment departments before adoption and control departments throughout the study period, because follow-up care is provided only via the onsite channel in these cases. It is also worth noting that patient age is measured by month due to the pediatric setting.
Given the staggered adoption of the tele-follow-up service channel across departments, we employ the DiD design as our identification strategy. The key identifying assumption in DiD is the parallel trends assumption, which means that in the absence of treatment, the difference in outcomes between the treatment and control groups would have remained constant over time. We begin with model-free evidence by plotting pre-treatment and post-treatment trends in patient volume. Consistent with our main analyses in the paper, we log-transform patient volume to account for its skewness. Figure 3(a) displays initial visit volume, and Figure 3(b) displays follow-up visit volume, separately for treatment and control groups over time. In both figures, pre-treatment trends appear parallel, while post-treatment differences widen, suggesting that telemedicine adoption took effect only after the post-treatment periods for adopting departments.
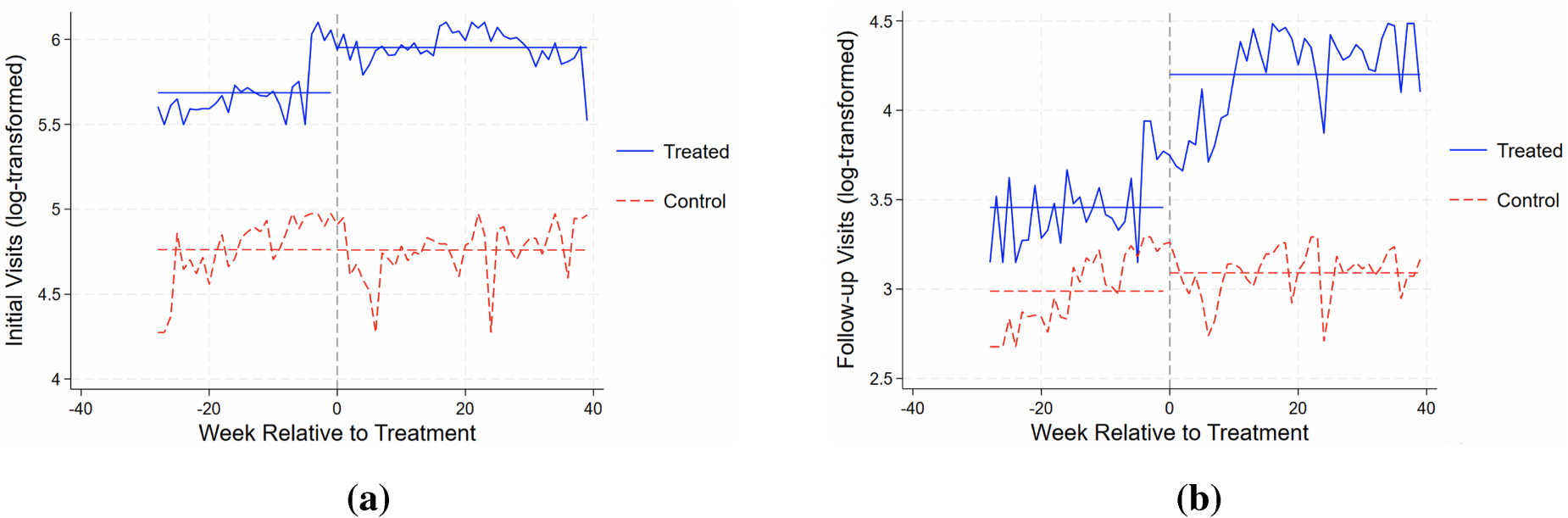
Weekly patient volume by treatment and control groups. Notes. The figure shows log-transformed patient volume over time for the treatment and control groups, and the horizontal line visualizes the average patient volumes in the pre- and post-treatment periods for both groups. The
We then examine whether telemedicine adoption was the sole treatment intervention driving the variations in patient volume during the sample period. Although the hospital reported no other concurrent events in health IT adoption, service provision, and labor force changes, unobserved seasonality could invalidate the identification. For example, the primary care department adopted telemedicine in March, a period with elevated flu activity, which could directly affect patient flow. If such seasonality affects the treatment and control departments to different extents, the observed change in patient demand could be driven by seasonality rather than the treatment of interest, which will bias the causal identification. Hence, we conduct a falsification test using the data one year before the main sample period (i.e., from February 2017 to December 2018) and assume the pseudo-treatment time to be one year before the actual adoption date (i.e., August 24, 2017, for the department of neurology and March 11, 2018, for the department of primary care). We then employ Equation (1) using this sample with pseudo-treatment status. More details about the specification of Equation (1) can be found in Section 5. As shown in E-companion Table EC.1, the estimated effects are small and statistically insignificant across all visit types, ruling out seasonality-driven spurious effects.
Finally, we evaluate whether unobserved hospital-wide initiatives other than telemedicine adoption could have driven changes in patient volume. Particularly, we restrict the sample to control departments and randomly assign treatment status to non-adopters. The intuition is that if telemedicine adoption happens to be part of a hospital-wide initiative that we have not observed, we may then see a similar impact on control departments. We repeat the random assignment 1,000 times and report the resulting coefficient estimates in E-companion Table EC.2. Across all visit types, the estimated effects remain small and statistically insignificant, indicating no evidence of concurrent hospital-wide changes coinciding with telemedicine adoption. This result further reinforces our identification strategy by supporting the assumption that telemedicine adoption was the sole treatment intervention during the sample period.
To test the impact of the tele-follow-up service on patient access, we conduct DiD regression with multiple groups and time periods following the literature (Angrist and Pischke, 2009). We adopt the following specification using aggregated data at the department-week level:

Table 2 reports the regression results. The significantly positive coefficient in Column (1) indicates that telemedicine adoption leads to a substantial increase in follow-up visit volume. In terms of magnitude, telemedicine increases follow-up volume by about 48.14% (i.e.,
Effect of telemedicine on patient volume.
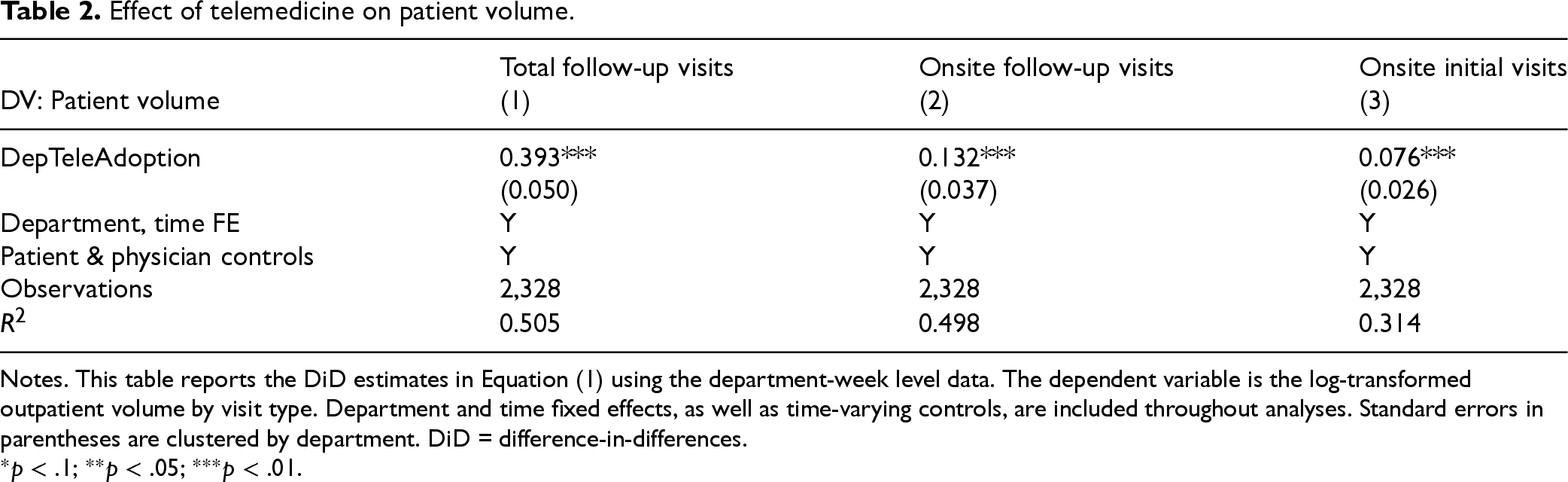
Notes. This table reports the DiD estimates in Equation (1) using the department-week level data. The dependent variable is the log-transformed outpatient volume by visit type. Department and time fixed effects, as well as time-varying controls, are included throughout analyses. Standard errors in parentheses are clustered by department. DiD = difference-in-differences.
Columns (2) and (3) show positive spillover effects on onsite demand. Specifically, following telemedicine adoption, onsite follow-up visits increased by 14.11% (i.e.,
In this section, we analyze both demand- and supply-side factors to understand the mechanisms driving the effect of tele-follow-up adoption.
Demand side analysis
Patient heterogeneity in onsite follow-up care costs
Our demand-side analysis aims to identify which types of patients contribute most to the observed spillover effects, shedding light on the changes in patient demand. In line with Hypothesis 4, our rationale is that telemedicine significantly lowers the costs associated with follow-up care, so patients who are most sensitive to these costs are more likely to take advantage of tele-follow-up services. To test this hypothesis, we conducted two empirical analyses, leveraging patient heterogeneity in their costs of traveling to the hospital for onsite service and their need for routine follow-up care.
In the first test, we segment patients into four groups based on their rural residence and the presence of comorbidities. These two factors are expected to influence patients’ response to the tele-follow-up service for two reasons: First, transportation has long been recognized as a significant barrier to accessing healthcare services (Syed et al., 2013). Rural patients, on average, have longer travel distances (31.5 miles) than urban patients (12.2 miles) to the hospital in our research. Moreover, rural patients often lack public transportation (RHIhub, 2022). Therefore, they are more likely to benefit from telemedicine as a lower-cost alternative to in-person visits. Second, chronic conditions often require regular monitoring and continuity of care (Hussey et al., 2014). Patients with comorbidities will likely need more frequent follow-ups, increasing the value of tele-follow-up service for ongoing care.
Accordingly, based on transportation costs and care needs, we categorize patients into the following groups: Group 1 consists of urban patients without any comorbidities. These patients face low costs for onsite care due to proximity and generally have low follow-up needs. Consequently, they are the least likely to adopt tele-follow-up services, and we expect minimal impact from tele-follow-up adoption in this group. Group 2 consists of urban patients with comorbidities, and Group 3 consists of rural patients without comorbidities. Patients in these two groups face mixed incentives for using tele-follow-up services. Rural patients without comorbidities encounter higher transportation costs but have limited need for follow-up care, while urban patients with comorbidities have higher follow-up needs but relatively lower transportation barriers to access onsite care. Due to these competing factors, the treatment effects for these two groups are unclear. Group 4 consists of rural patients with comorbidities. Patients in this group face both high transportation costs and high follow-up needs due to chronic conditions. Therefore, they are the most likely to benefit from tele-follow-up services, and we expect a more salient treatment effect in this group.
Table 3 reports the DiD estimates with the dependent variable being the visit volume from each patient group by department and week. There are several key findings. First, for urban patients without comorbidities (Column 1), the treatment effects are insignificant across all visit types, consistent with the expectation that these patients are unlikely to be affected by the introduction of the tele-follow-up service. Given their proximity to hospitals and limited follow-up needs, these patients face low costs of in-person care and are not significantly affected by the availability of tele-follow-up services. For urban patients with comorbidities (Column 2), we find significantly positive treatment effects, indicating that patients in this group respond to the telemedicine service, and their needs are mainly driven by the ongoing healthcare needs. For rural patients without comorbidities (Column 3), no significant treatment effects are observed, reflecting that while transportation costs are higher, the limited demand for follow-up care reduces the value of adopting tele-follow-up for this patient group. For rural patients with comorbidities (Column 4), we find the strongest treatment effects in both magnitude and significance. Facing both greater healthcare needs and higher transportation costs, these patients are the most likely to adopt tele-follow-up services, and their care utilization patterns shift most substantially.
Heterogeneous effects by patient groups.

Heterogeneous effects by patient groups.
Notes. This table reports the heterogeneous treatment effects by patient groups, where we distinguish patients based on transportation costs (i.e., rural vs. urban residence) and follow-up care needs (i.e., the presence of comorbidities). Department and time fixed effects, as well as time-varying controls, are included throughout analyses. Standard errors in parentheses are clustered by department. CCI = charlson comorbidity index.
In sum, these findings imply that the presence of comorbidities (
In the second test, we further refine the sample by focusing on rural patients with verified health conditions that require routine follow-up care. This subgroup is expected to be especially responsive to telemedicine due to the high transportation cost and the demand for ongoing medical attention. Based on feedback from physicians at our collaborating hospital, we identify several chronic conditions that typically necessitate regular follow-up: childhood epilepsy, tic disorders, neurodevelopmental delay, movement disorders, growth disorders, muscular dystrophy, intellectual disability, attention-deficit/hyperactivity disorder, and mental health conditions. We use International Classification of Diseases, Tenth Revision coding to identify visits associated with these conditions.
Table 4 reports the regression results, with the dependent variable being the visit volume for rural patients with the above conditions requiring routine follow-up care. Across all visit types, we observe a much larger effect size compared to the main result using the full sample (see Table 2), underscoring the heightened demand for tele-follow-up among patients facing higher costs to accessing long-term follow-up care. Together, these two mechanism tests provide consistent support for Hypothesis 4, indicating that the effects of tele-follow-up adoption are strongest among patients with higher sensitivity to onsite care costs and a consistent need for long-term follow-up services.
Effect on rural patients with routine follow-up need.

Notes. This table reports the treatment effect focusing on rural patients with routine follow-up needs. Department and time fixed effects, as well as time-varying controls, are included throughout analyses. Standard errors in parentheses are clustered by department.
To directly examine if the initial visits are actually driven by new patients, we construct the outcome variable Onsite Initial Visits (new patients), which captures the volume of initial visits from new patients only. 2 Column (1) of Table 5 reports a significant increase in the initial visit volume by new patients. This finding corroborates a key mechanism underlying the spillover effect of the tele-follow-up channel on initial visits. Some patients may initially hesitate to seek care at the hospital due to perceived inconveniences and costs associated with follow-up appointments. By reducing these barriers, telemedicine helps alleviate concerns about the overall cost of the care process, particularly the long-term costs of follow-up services. Consequently, the hospital becomes a more appealing choice for initial care.
Decomposition of initial and tele-follow-up visits by patient type.

Decomposition of initial and tele-follow-up visits by patient type.
Notes. This table reports the treatment effects on initial visits from new patients (column 1), new use of telemedicine visits (column 2), and repeated use of telemedicine visits (column 3), respectively. Department and time fixed effects, as well as time-varying controls, are included throughout analyses. Standard errors in parentheses are clustered by department.
Next, we aim to examine whether the telemedicine usage experience would affect patients’ future choice of follow-up modalities. As such, we construct two outcome variables by department
While the above analysis of tele-follow-up visits is informative, several points are worth noting. First, since the dependent variable (telemedicine visits) is inherently tied to the treatment itself, this analysis primarily reflects the implementation of the new service channel rather than fully capturing patients’ visit behavior. For this reason, we have included variables in the main analysis that are not directly linked to the treatment design, such as Total Follow-up Volume, Onsite Follow-up Volume, and Initial Volume, for validating the pre-trend assumption in DiD analysis. Second, related to the above point, since the telemedicine visits volume is zero before treatment for all departments and zero after treatment for control departments, the difference between treated and control groups mechanically shows a large increase due to the take-up of telemedicine service by patients in the treatment departments only.
We next introduce the supply-side factors (i.e., service efficiency and service quality) and examine how they change after the adoption of tele-follow-up service.
Service efficiency
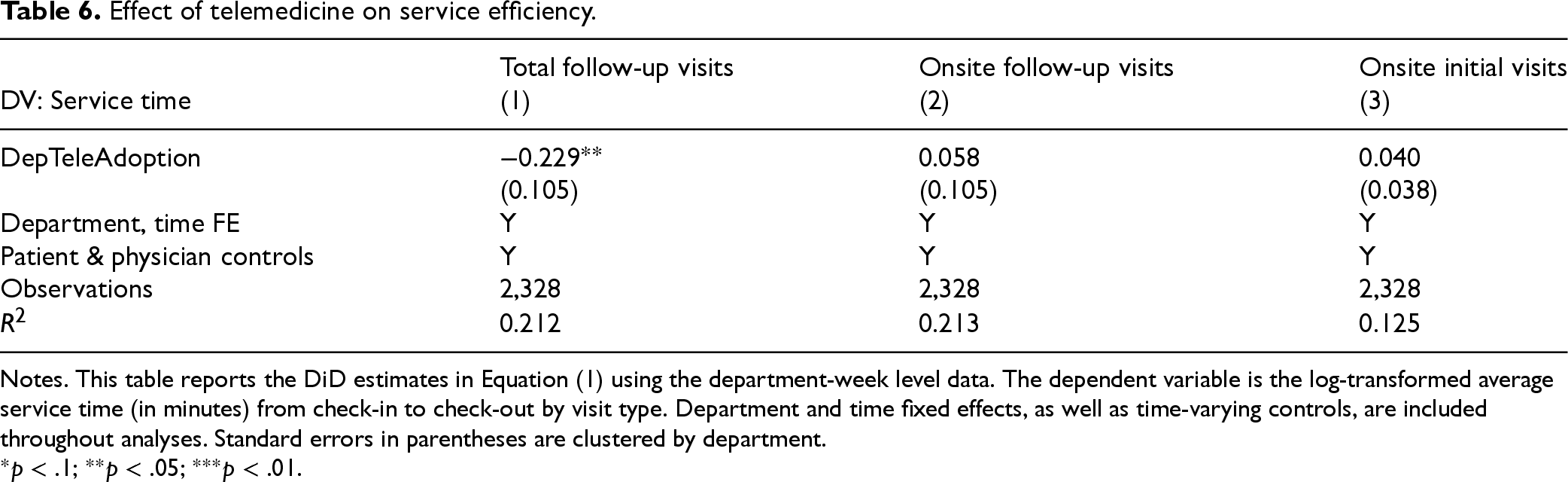
We measure service efficiency by the Service Time for each appointment. Using the data, we can track a physician’s check-in and check-out timestamps for each visit. Service time is then calculated as the time difference (in minutes) between the check-in and check-out time. We find that the average service time for follow-up visits decreased from 39.6 to 21.6 min. When breaking down follow-up visits by modality, we find that: (i) tele-follow-up appointments have an average service time of 12.4 min, and (ii) onsite follow-up appointments have an average of 30.5 min. The non-parametric evidence suggests that efficiency improvement is primarily driven by the significant reduction of service time via telemedicine. Nonetheless, changes in service efficiency may be due to other factors like patient mix and seasonality. As such, it is necessary to have formal empirical tests to identify the treatment effects on service efficiency. Hence, we replicate the DiD analysis with the dependent variable being the average service time (on the log scale) by department and week.
Table 6 reports the regression results. For follow-up visits, telemedicine adoption significantly reduces patients’ average service time by 20.5% (
Effect of telemedicine on service efficiency.
Effect of telemedicine on service efficiency.
Notes. This table reports the DiD estimates in Equation (1) using the department-week level data. The dependent variable is the log-transformed average service time (in minutes) from check-in to check-out by visit type. Department and time fixed effects, as well as time-varying controls, are included throughout analyses. Standard errors in parentheses are clustered by department.
According to interviews conducted in our collaborating hospital, physicians are able to speed up care provision via telemedicine in several ways. First, the telemedicine channel is dedicated to follow-up appointments only, thereby enabling physicians to achieve higher focus within a work shift by separating patients based on the type of appointment. Before telemedicine adoption, physicians encountered both initial and follow-up visits during a work shift. After the adoption, physicians encountered only follow-up patients during a “telemedicine work shift,” thus enabling more focused practice. Moreover, by rerouting a substantial portion of follow-up appointments from the offline to the telemedicine channel, the patient mix in both channels becomes more homogeneous. Specifically, the tele-follow-up channel now serves exclusively follow-up patients, while the offline channel primarily focuses on initial care. This separation allows physicians to concentrate more effectively on each type of care by eliminating the need to switch between different types of care in a work shift, thus leading to a more efficient and focused practice in both settings. The improved efficiency through higher focus is in the same spirit as what is suggested in the literature. For instance, Ibanez et al. (2018) show that radiologists take more time to read digital images (e.g., chest X-rays, head CT scans, and spine MRIs) when there is a greater variety of items in their queue. Second, patients are required to pre-fill their demographic and health information when scheduling a tele-follow-up appointment. Hence, tele-follow-up visits eliminate the paperwork compared to the office setting, thus facilitating the care process.
An increased workload and the acceleration of service delivery may pose risks to the quality of care. In practice, the rise in patient volume following telemedicine adoption could be attributed to faster but potentially lower-quality service. Specifically, patient volume might increase if physicians prioritize higher throughput by speeding up consultations, potentially compromising care quality by dedicating less time to each patient encounter. To check this, we examine the changes in readmission rate, a key care quality measure (Lu and Lu, 2018). We further collect all inpatient and ER records to track patients’ visits over time using their unique identifiers and generate binary readmission indicators corresponding to different time windows. A readmission is coded as one if a patient is readmitted to the hospital, either as an inpatient or through the ER, within 7, 14, or 30 days following discharge, and zero otherwise. This measure captures all-cause readmissions, encompassing those through emergency care, ambulatory care, or direct admissions to the inpatient department.
Table 7 reports a significant reduction in patients’ readmission rates for all time windows, suggesting that the use of tele-follow-up service improves rather than compromises patient health outcomes. The positive effect is feasible in our setting for two reasons. First, timely follow-up helps detect any early signals in patient health conditions, thus reducing the risk of hospital readmission (Brooke et al., 2014). Second, physicians can enhance the care quality due to improved focus during both the online and onsite work shifts. This finding aligns with the literature, which demonstrates a positive relationship between focused operations and care outcomes. For example, studies in cardiovascular care by Kc and Terwiesch (2011) and Clark and Huckman (2012) find that focused operations generally have a positive effect on quality outcomes, such as shorter lengths of stay and reduced mortality rates.
Effect of telemedicine on patient care quality.

Effect of telemedicine on patient care quality.
Notes. This table reports the DiD estimates using the individual-department-episode level data. The dependent variables are the average 7-day, 14-day, and 30-day readmission rates by individual, department, and episode of care. Department and time fixed effects, and time-varying controls, are included in all analyses. Standard errors in parentheses are clustered by department.
We conduct extensive robustness checks in this section to assess the sensitivity of our results to potential endogeneity issues.
Pre-trend analysis
A fundamental assumption of the DiD model is the parallel trend assumption, which states that the untreated units are appropriate counterfactuals of the trend that the treated units would have followed without treatments. In this section, we aim to test if there is any violation of the parallel trend assumption and examine how post-treatment effects evolve over time. Specifically, we create a series of binary indicators to represent the pre-treatment and post-treatment periods using the following specification (Angrist and Pischke, 2009):
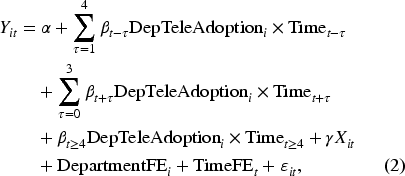
Table A1 provides no evidence of pre-treatment differences influencing our findings, as all coefficient estimates prior to telemedicine adoption are statistically insignificant. We observe an immediate impact on follow-up visits, beginning just 1 month after telemedicine adoption, indicating that patients quickly embraced tele-follow-up services once they were made available. However, the effect on initial visits takes longer to materialize, becoming significant after 2 months post-adoption. This delayed effect is reasonable, as the tele-follow-up option may have initially attracted existing patients for follow-up care, later increasing awareness and drawing new patients to the hospital for both initial and follow-up care over time.
Although we have controlled for time-varying changes in the patient mix throughout the analyses, concerns about unobserved heterogeneity between the treatment and control departments may still arise. For example, departments with higher demand for follow-up services might be more likely to adopt telemedicine, yet these departments could differ fundamentally from those with fewer patients requiring follow-up care. Alternatively, treatment departments might vary from control departments in terms of unobserved patient composition. Such unobserved heterogeneity could influence patient behavior and potentially bias the estimation of treatment effects.
To alleviate these concerns, we construct a matched sample based on the PSM so that the adoption of telemedicine more closely resembles a randomized assignment (Rosenbaum and Rubin, 1983). To proceed, we match treatment and control departments based on historical department-week-level characteristics. Specifically, we construct measures for patient volume by visit type and the average health condition of patients using data from one year prior to the hospital’s first adoption of telemedicine. This approach ensures that the matching variables are not influenced by the telemedicine adoption decision. E-companion Table EC.3 provides summary statistics of the covariates before and after matching, where the matched sample is balanced as the standardized differences are all below the threshold of 10% suggested in the literature (Austin, 2009). 3 The results using the PSM sample are reported in Table A2 (columns 1–3), corresponding to the main Result in Table 2. Across all three outcome variables, we find consistently robust treatment effects. We also replicate the analyses in Tables 3–7 using the matched sample and report these results in the E-companion Section EC.4. The matched-sample estimates remain consistent with those from the full sample, reinforcing the robustness of our findings.
Given that the sample size is substantially reduced after PSM, we further conduct analysis based on the propensity score weighting, which does not compromise sample size. In particular, we perform the propensity score weighting analysis for all three main outcome variables. First, we estimated the treatment propensity scores using logistic regression with pre-treatment cross-sectional department-level data and key pre-treatment covariates as predictors (i.e., follow-up visits, initial visits, average CCI, the percentage of male patients, and average patient age). Then, using the predicted propensity scores (ps) from the logistic regression in the first step, we calculate the inverse probability weights as follows:
In summary, both propensity score-based analyses yield consistently robust results across all visit types, reinforcing the validity of our findings. The effect sizes remain stable overall, though a slightly smaller effect was observed for total follow-up visit volume. This modest reduction may reflect underlying differences in patient needs, where patients in treatment departments may have a higher inherent demand for follow-up care, independent of the treatment itself.
Instrumental variable analysis
To further address endogeneity concerns related to department-level decisions on telehealth adoption—such as some departments being more suited for virtual care delivery, while others depend heavily on onsite care and physical examinations—we implement a two-step identification strategy similar to Ayabakan et al. (2024). Specifically, we use the lagged proportion of encounters requiring lab tests as an IV. This instrument is based on the observation that departments treating patients with chronic conditions often require more frequent lab tests for monitoring health status and treatment adjustments. As a result, the patient demand shift within these departments is more likely to be related to the tele-follow-up service, as it allows flexibility for both patients and physicians.
For the IV to be valid, it must satisfy two conditions: IV relevance (the IV is strongly correlated with the endogenous variable) and IV exclusion (the IV does not directly affect the outcome variable). To assess instrument strength, we first examine the correlation between the IV and the telemedicine adoption decision. In the first stage regression with DepTeleAdoption as the dependent variable and IV and other controls as the independent variable, we find a significant effect of the IV, with a coefficient of 0.705 and a standard error of 0.071 (
Since the endogenous treatment is a binary variable, we implement the maximum likelihood estimators via a latent variable model following the literature (Cameron and Trivedi, 2005):
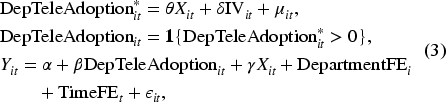
Table A3 shows consistently robust estimates. Moreover, the Wald tests of the null hypothesis
To assess whether our two-way fixed effects model produces biased estimates in staggered DiD settings with heterogeneous treatment effects, we employ doubly robust estimators (Baker et al., 2022; Callaway and Sant-Anna, 2021) as a further robustness check. These estimators account for potential biases associated with two-way fixed effects regressions or event study analyses in cases with multiple periods or variations in treatment timing. Table A4 reports the weighted average treatment effects with weights proportional to the group size. The results show qualitatively consistent treatment effects compared to the main analysis, reinforcing the robustness of our findings to alternative model specifications.
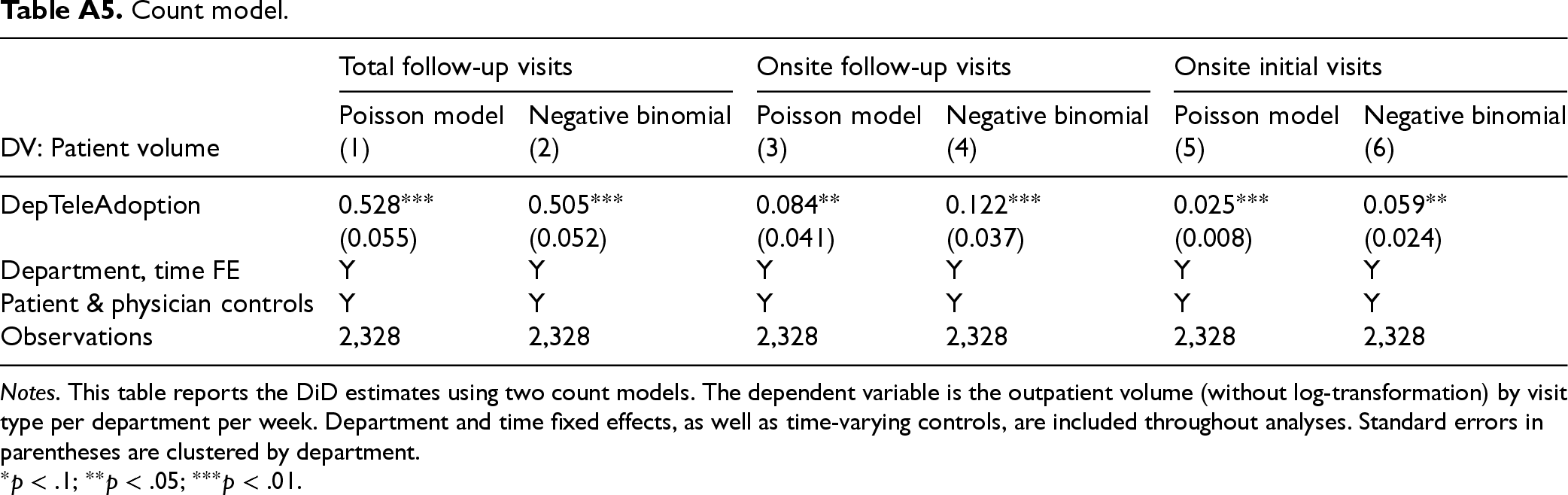
Another concern relates to the scale of the dependent variable. Since the main outcome variables are count data, one may wonder whether our findings are robust to the count model. To alleviate this concern, we implement two count models with the dependent variable measured in its original scale. As shown in Table A5, in both the Poisson model (Columns 1, 3, and 5) and negative binomial model (Columns 2, 4, and 6), all results remain qualitatively the same as the main analyses. These results further validate that our findings are not driven by the choice of the log-linear model.
Conclusion
Telemedicine is transforming the very nature of healthcare delivery, and increasing numbers of healthcare providers are making virtual visits available to their patients. According to the National Center for Health Statistics, between June 2020 and June 2021, over 30% of patients accessed telemedicine services (CDC, 2022). In this paper, we collect a unique dataset to evaluate the adoption of telemedicine in one important area of care delivery—follow-up care—and examine how this adoption affects initial care provision.
On the demand side, tele-follow-up services reduce barriers for patients, especially those facing higher costs of onsite follow-up appointments. Moreover, the tele-follow-up service alleviates concerns about the total costs of the care process and encourages more patients to seek initial care at the hospital. On the supply side, tele-follow-up services enhance physician efficiency through focused practice and better continuity of care. In summary, although telemedicine was dedicated to follow-up services, it significantly affected cross-channel services (i.e., demand for onsite follow-up care) and cross-type services (i.e., demand for initial care).
On the academic front, this study contributes to the growing telemedicine literature by examining its role in improving follow-up care. Leveraging granular data, we differentiate between follow-up and initial visits, an important yet understudied distinction in prior research. Despite the recognized potential of telemedicine, skepticism persists among practitioners regarding its applicability across broader healthcare contexts (Krall, 2021). Our findings show that tele-follow-up can play a critical role in enhancing post-discharge care, demonstrating its value as an integral component of the care process. More importantly, our paper points to telemedicine as a flexible solution to structure care channels based on visit type, thereby improving operational efficiency. By shifting a large proportion of follow-up appointments to telemedicine, physicians experience a more homogeneous patient mix during a work shift. This reduces the cognitive and logistical strain of alternating between initial and follow-up care. These findings thus extend the literature on focused operations (Clark and Huckman, 2012; Kc and Terwiesch, 2011), highlighting telemedicine as a tool for enhancing operational focus and efficiency.
Our findings offer actionable insights for healthcare decision-makers. First, our findings highlight the effectiveness of telemedicine in improving follow-up care. Since tele-follow-up services can foster greater adherence to follow-up schedules, support timely monitoring of health conditions, and improve overall patient outcomes, we recommend that practitioners incorporate tele-follow-up services as an integral component of the care process to enhance the accessibility and continuity of care. Second, we show that the tele-follow-up service is particularly useful for addressing the unmet needs of disadvantaged patients from rural areas and those with chronic conditions. The finding is important for healthcare decision-makers striving to reduce healthcare disparities. Third, enhanced follow-up care via telemedicine further enhances patient health by reducing readmission rates. Therefore, along with other benefits of telemedicine, such as monitoring patient health and improving medication adherence, wider adoption of the tele-follow-up service may ultimately improve population health. Fourth, to fully harness the power of telemedicine in outpatient care, hospitals should allocate dedicated work shifts specifically for tele-follow-up appointments, enhancing focused practice and operational efficiency. Furthermore, hospitals should proactively adjust physician schedules to meet the increased patient demand driven by telemedicine adoption.
Supplemental Material
sj-pdf-1-pao-10.1177_10591478261449973 - Supplemental material for Tele-follow-up and outpatient care
Supplemental material, sj-pdf-1-pao-10.1177_10591478261449973 for Tele-follow-up and outpatient care by Wei Gu, Meng Li and Shujing Sun in Production and Operations Management
Footnotes
Count model.
| Total follow-up visits | Onsite follow-up visits | Onsite initial visits | ||||
|---|---|---|---|---|---|---|
| Poisson model | Negative binomial | Poisson model | Negative binomial | Poisson model | Negative binomial | |
| DV: Patient volume | (1) | (2) | (3) | (4) | (5) | (6) |
| DepTeleAdoption | 0.528 | 0.505 | 0.084 | 0.122 | 0.025 | 0.059 |
| (0.055) | (0.052) | (0.041) | (0.037) | (0.008) | (0.024) | |
| Department, time FE | Y | Y | Y | Y | Y | Y |
| Patient & physician controls | Y | Y | Y | Y | Y | Y |
| Observations | 2,328 | 2,328 | 2,328 | 2,328 | 2,328 | 2,328 |
Notes. This table reports the DiD estimates using two count models. The dependent variable is the outpatient volume (without log-transformation) by visit type per department per week. Department and time fixed effects, as well as time-varying controls, are included throughout analyses. Standard errors in parentheses are clustered by department.
Acknowledgment
The authors are grateful to Professor Jayashankar Swaminathan, the anonymous senior editor, and anonymous referees for their invaluable and insightful feedback throughout the review process. Authors contributed equally to this work.
Funding
The authors received the following financial support for the research, authorship and/or publication of this article: Wei Gu received financial support from the National Natural Science Foundation of China (grant nos. 72072010, 72542010, and 72394372).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Notes
How to cite this article
Gu W, Li M and Sun S, (2026) Tele-follow-up and outpatient care. Production and Operations Management x(x): 1–21.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.