
Abstract
There are more than 7,000 known rare diseases, yet around
Introduction
“Rare is not rare” is a well-known motto in the rare disease community, referring to the more than
There is no global consensus on a formal definition of rare diseases. In the United States, the Orphan Drug Act (ODA) defines a rare disease as a condition that affects fewer than
The objective of this paper is to encourage and stimulate new applications of Operations Management (OM) methodologies to advance the rare disease landscape.
1
Although there is extensive research on rare diseases in medical and life science journals, the concept of rare disease is relatively understudied in the OM literature. For example, as of October 2025, only two papers with the keyword “rare disease” have been published in the Production and Operations Management journal, while this number is only
The scope of the paper is structured around five main OM research directions: regulatory outlooks, incentive programs and subsidies, pricing and coverage schemes, (bio)pharmaceutical manufacturing, and developing economies. We begin with a brief overview of common challenges and opportunities from the perspectives of governments, industry, insurers, and patients in Section 2. We suggest several future research directions in Section 3, and provide concluding remarks in Section 4.
Overview of societal challenges
An important societal challenge is the high prices and limited treatment options for patients with rare diseases. The rare disease landscape is complex and many factors contribute to this societal challenge. Table 1 summarizes the key challenges from the perspectives of governments, industry, insurers, patients, and their families.
Overview of major challenges related to rare diseases.
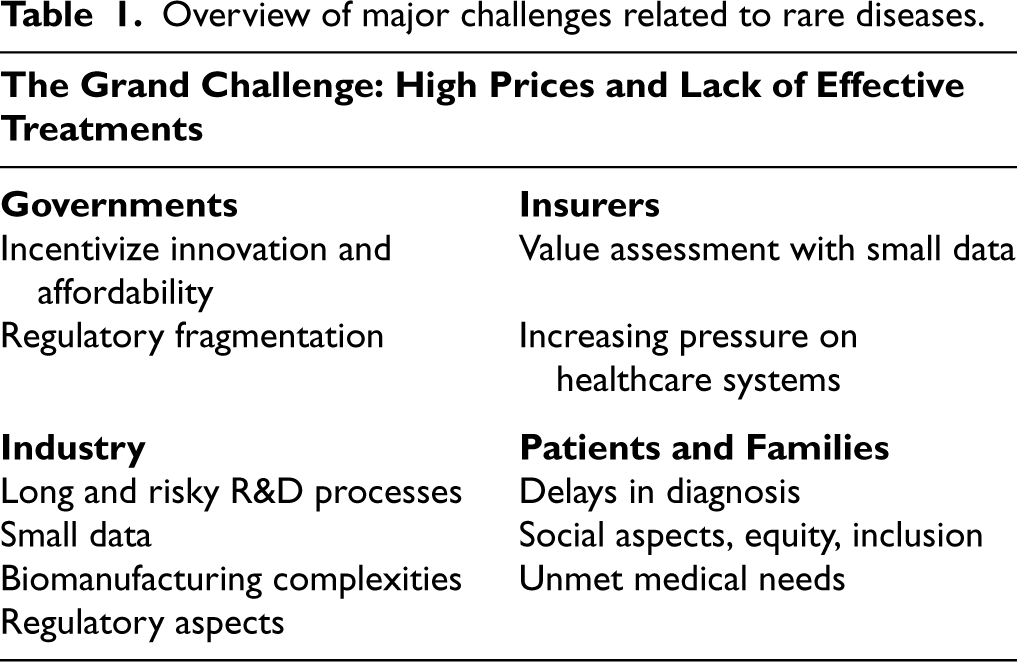
Overview of major challenges related to rare diseases.
Incentivizing the development of new drugs for rare diseases is a major challenge for governments. However, the ODA has played an important role in improving the rare disease landscape (FDA, 2025). The ODA provides several incentives to the industry, including tax rebates, subsidies, and extended market exclusivity periods. Since its inception in
Regulatory fragmentation is another global challenge for stakeholders. The U.S. Food and Drug Administration (FDA), European Medicines Agency, and other regulatory agencies serve as an overarching mechanism to ensure safety and quality. However, there are still many differences in pricing and reimbursement mechanisms in different countries around the world, creating fragmentation across regions. This fragmentation can lead to delays and additional efforts by the industry, and can also create gaps in the pricing and coverage of the same medicines between regions, with global implications for equity and accessibility. Therefore, there is a growing need to achieve global consistency and standardization (Umoh et al., 2024). Furthermore, as the industry moves toward small-scale production of personalized drugs and gene therapies, new regulatory perspectives are likely to be required to support the unique needs of these advanced treatments.
Low- and middle-income countries (LMICs) face several additional challenges in addressing the needs of patients with rare diseases. Recent studies highlight three critical issues for LMICs (Baynam et al., 2020; Rodrigues et al., 2024). The first challenge is limited access to expertise and specialized care. Some regions may have only a few or no specialists in rare diseases. Patients may have to travel long distances to receive a diagnosis and specialized care, which is often impractical. Moreover, Indigenous populations often live in dispersed, nonmetropolitan areas and may be more likely to experience health inequities (Baynam et al., 2020). A second challenge is limited access to advanced diagnostics and testing. Diagnosing a rare disease often requires specialized procedures, such as genetic testing, and the use of advanced technologies, such as spectroscopy. These diagnostic tests and equipment may not be readily available in LMICs. For example, studies show that the cost of diagnosing a rare disease is typically higher in Brazil than in the United States due to limitations in supplies and technology (Rodrigues et al., 2024). Third, it is important to increase funding and research collaborations in LMICs and to support local patient advocacy groups. A strong network of research collaborations and patient advocacy groups can help reduce healthcare disparities and provide better access to information (e.g., Baynam et al., 2020).
Challenges of the industry
Pharmaceutical research and development (R&D) involves high costs and risks. For example, the cost of developing a new drug can be around 1 to 2 billion dollars per drug over a period of
The small number of patients also presents challenges for clinical trials and postmarket studies to assess the effectiveness and safety of drugs. For example, it can be difficult to recruit a sufficient number of participants in clinical trials to obtain statistically meaningful results. Studies show that clinical trials for nonorphan drugs recruit three times more participants compared to orphan drugs (Pearson et al., 2022). In addition, patients with rare diseases may be geographically dispersed in different regions, which requires additional recruitment efforts. Another challenge is the identification of appropriate (surrogate) endpoints and the lack of an acceptable active comparator for unmet medical needs. All of these factors contribute to increased costs and delays in the R&D process. There are also ethical concerns. For example, placebo-controlled trials may be considered unethical when the medical condition is life-threatening with no other treatment options. However, there is growing awareness of the challenges associated with rare disease R&D programs, and new initiatives are being developed to address these challenges. One promising example is the FDA’s Rare Disease Endpoint Advancement Pilot Program launched in 2022, which aims to support the development of novel endpoints to evaluate the efficacy of orphan drugs.
Biopharmaceuticals account for a large portion of orphan drugs. In this setting, the industry faces additional challenges with biomanufacturing operations. For example, biomanufacturing processes have high variability and uncertainty in production yields, quality, lead times, and costs (Martagan et al., 2023). In addition, production processes are cost- and labor-intensive and carry a high risk of failure due to contamination, mutation, and other quality issues. In general, the industry benefits from economies of scale to reduce unit costs. However, the low volumes of orphan drugs, combined with the uncertain and complex nature of the biological processes, pose additional challenges to the cost-effectiveness of orphan drug production. An extreme example is the drug Glybera—the first gene therapy approved in Europe—which was discontinued due to high costs and low demand (Senior, 2017). However, the future of gene therapy is promising, with growing interest from both patients and industry. For the industry, this gradual transition toward small-scale personalized manufacturing is not an easy process and requires a fundamental rethinking of (bio)pharmaceutical manufacturing and supply chains.
Regulatory fragmentation adds another layer of challenge for the industry. (Bio)pharmaceutical processes are highly regulated to ensure safety and quality. However, global regulatory processes are fragmented, and specific procedures can vary from country to country. For example, the European Medicines Agency serves as an overarching mechanism in Europe, but countries within Europe may still have additional requirements and procedures to support product-specific dossiers, data collection, documentation, packaging, and, so on. In addition, emerging technologies (e.g., continuous biomanufacturing and real-time release testing) require evolving regulatory perspectives to support their adoption, safety, and efficiency (Martagan et al., 2024).
Challenges related to insurance and coverage mechanisms
In this section, we use the term “payer” to broadly refer to stakeholders involved in coverage and reimbursement decisions for orphan drugs (e.g., health technology assessment, public or private insurance companies). When making coverage and reimbursement decisions, payers typically evaluate the cost-effectiveness of the drug based on its added value (e.g., expected increase in the quality-adjusted life years, QALY) and associated costs. However, it is often difficult to robustly assess the cost-effectiveness of orphan drugs due to the relatively limited evidence generated from clinical trials and postmarket studies with small patient populations. In addition, payers typically use cost-effectiveness thresholds to guide coverage decisions, such that drugs exceeding a predetermined cost per QALY threshold are considered “low value.” For example, the framework used by the Institute for Clinical and Economic Review between 2017 and 2019 classified drugs costing more than $175,000 per QALY as low value (Chambers et al., 2020). However, the appropriate definition of these threshold values remains debated and coverage schemes vary substantially between countries.
There is increasing pressure on healthcare systems due to the growing number of expensive drugs, as discussed in Section 2.1. Research shows that orphan drugs provide greater health benefits but are less cost-effective than nonorphan drugs (Chambers et al., 2020). These observations, combined with budget constraints and the so-called orphan blockbuster effect, create a dilemma for equitable resource allocation. Consequently, there is a growing need for new mechanisms that can effectively lower prices and increase patient access while incentivizing the development of new orphan drugs.
Challenges of patients and families
Most rare diseases are genetic and disproportionately affect children. They often lead to developmental delays in motor skills, speech, and other essential functions required for independent living. Therefore, we recognize both patients and their families as critical stakeholders.
One critical concern is delayed access to correct diagnosis and treatment. Research shows that the average total diagnosis time for a rare disease is about
It is our social responsibility to acknowledge the daily challenges of rare disease patients and to help them achieve equal opportunities in social life, education, and employment. Raising awareness is especially important when an illness is “invisible” to the human eye. For example, Verger et al. (2020) highlight the challenges of schoolchildren when they have an “invisible” disease with chronic muscle pain, constant headaches, or difficulty breathing. Because their illnesses are not visible to the human eye (or cannot be easily diagnosed), many children struggle to receive adequate support to continue their education or integrate into social life. The “invisible” aspects can be even more profound for parents and caregivers. When a diagnosis or treatment option is not available, the rarity of the situation can leave families feeling lost with the “emptiness of no cure,” as one parent mentioned in our interactions. In this setting, patient organizations play a critical role in providing community support, raising awareness, influencing healthcare policy, and fostering research collaborations. Examples of prominent patient organizations are EURORDIS-Rare Diseases Europe, and the National Organization for Rare Disorders.
In summary, the combination of challenges faced by governments, industry, payers, and patients results in an important problem of unmet medical needs. For most rare diseases, there is either no treatment or existing treatments are not accessible to patients. High prices, combined with socioeconomic, geographic, educational, and cultural barriers, continue to play a critical role in limiting access. Even when patients have access to the right diagnosis and treatment, they may still struggle with social isolation and loneliness.
To recognize these challenges, the United Nations (UN) has published a resolution on “Addressing the challenges of persons living with a rare disease and their families” (United Nations, 2023). This resolution is an important step forward: It raises awareness of the challenges faced by patients with rare diseases and their families, and encourages new mechanisms for equity and inclusion. The resolution was adopted by all member states of the UN and is the first dedicated UN resolution to highlight the specific challenges of rare diseases.
OM research directions
In this section, we discuss several OM research directions to address the aforementioned challenges of the rare disease landscape. For each research direction, we begin with a brief review of the literature and then suggest future research opportunities. Table 2 provides an outline of Section 3 and highlights the main research themes, key challenges, and future OM research opportunities.
Roadmap for section 3: OM research directions for rare diseases.
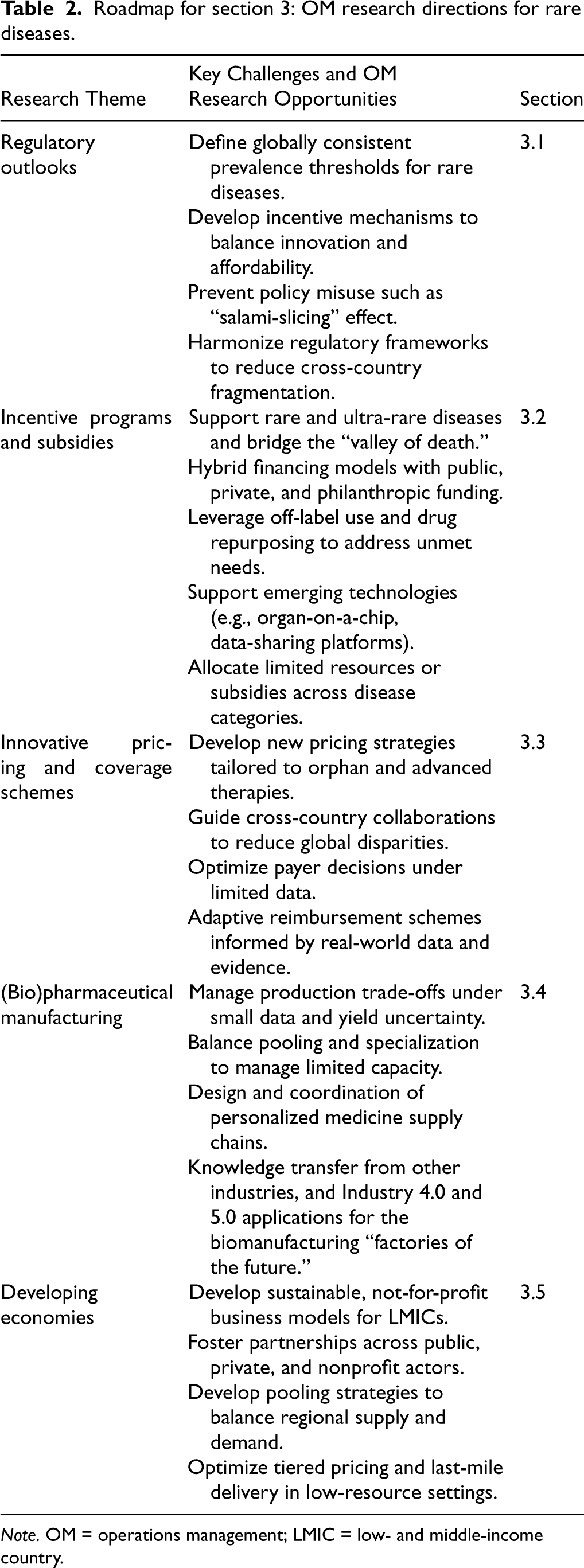
Roadmap for section 3: OM research directions for rare diseases.
Note. OM = operations management; LMIC = low- and middle-income country.
Several new regulatory approaches have been introduced to address unmet medical needs, including accelerated approval, priority review, and conditional marketing authorization. Although these programs differ in specific criteria and implementation, they share a common goal of accelerating patient access to lifesaving medicines and incentivizing new drug development.
A growing body of OM research explores innovative approaches to drug approval and regulation. For example, Bravo et al. (2022) studied flexible drug approval policies to inform regulators. They developed a stylized queueing model to generate insights for disease-specific approval guidelines based on disease severity and prevalence. Xu et al. (2021) examined a critical concern with the accelerated approval pathway, where manufacturers did not comply with the requirements of postmarketing studies. They developed a Stackelberg framework and explored potential solutions to address the problem of noncompliance. Similarly, multiple studies examined postmarketing drug safety and other regulatory issues, for example, Ahuja et al. (2021); Anderer et al. (2022) and Wang et al. (2023). Overall, these studies highlight the growing role of OM methodologies in drug development and regulatory decision-making.
In addition to approval pathways and regulatory compliance, a fundamental regulatory challenge concerns the definition of rare diseases themselves. Differences in prevalence thresholds between countries influence eligibility for orphan designation, incentive programs, and regulatory pathways. These definitional differences have important implications for innovation, patient access, and global consistency. Motivated by these challenges, we formalize several open research questions as follows.
(1) How can we establish a globally consistent prevalence threshold for rare diseases? If a new and globally consistent definition were established, how would it impact the industry and society?
What is the formal definition of a rare disease? Although this is a fundamental question, there is no universal definition. In the European Union, a disease is classified as rare if it affects fewer than
Although there is a growing need for global consistency, identifying an appropriate prevalence threshold is a complex issue with implications for industry and society. If the prevalence threshold is “too high,” more drugs will qualify for orphan designation and other incentives. In the long run, this may improve patient access and stimulate new drugs that would not otherwise be developed. However, if the overall system is not properly designed, it can also increase pressure on patients and society with an increasing number of expensive orphan drugs. If the threshold is “too low,” it may not be financially viable for the industry to develop new drugs, leaving patients at risk. In either case, the prevalence value will affect patient access and innovation, and its choice must carefully balance the complex dynamics between stakeholders. This definitional challenge has been widely recognized in the rare disease community, prompting recent efforts to develop new frameworks through multistakeholder collaboration (Wang et al., 2024b). Building on these initiatives, future OM research can help stakeholders navigate the resulting trade-offs by developing analytical and empirical models to evaluate how alternative definitions of prevalence thresholds may affect innovation, patient access, and overall social welfare.
(2) How can governments effectively balance innovation and affordability? When and how should existing incentive mechanisms (e.g., ODA and accelerated approval) be revised, and what are the most appropriate revisions and policy changes to support current industry and patient needs?
The market dynamics are changing rapidly with advances in biotechnology, oncology, and genomics, and the number of drugs with orphan designation is also increasing. This raises the question of when and how existing incentive mechanisms should be revised to reflect the fast pace of industry and the changing needs of society. To complement these discussions, future OM research can guide possible revisions of the prevalence threshold as discussed above.
Another important aspect is the “salami-slicing” effect (i.e., the practice of dividing a disease category into many smaller subgroups so that drugs can qualify for orphan designation). Advances in personalized medicine may further facilitate such practices in the future. In oncology, for example, there is growing interest in genetically defined subpopulations rather than broad indications, so that “almost any cancer drug can be maneuvered into an orphan disease category” (Pearson et al., 2022). While this may improve patient access to personalized and targeted therapies, there is no consensus on the long-term impact of the salami-slicing effect. However, some revisions to the ODA and related FDA policies were introduced to modernize the orphan drug designation process and address concerns about the potential misuse of orphan incentives (e.g., FDA, 2017). Another example is the “Build Back Better Act,” which proposed limitations on the ODA tax credit by restricting eligibility for multiple orphan indications of the same product. However, some stakeholders expressed concerns about the potentially adverse effects of such changes (Pearson et al., 2022). On the other hand, the Pediatric Rare Disease Priority Review Voucher Program, designed to support pediatric rare diseases, expired in December 2024. Patient organizations raised critical concerns about its expiration and encouraged efforts to reauthorize the program (Everylife Foundation for Rare Diseases, 2025). Identifying the right policy updates and assessing their impact is complex and challenging, and suboptimal decisions can adversely affect healthcare systems. Future research can develop empirical and analytical models to estimate the short- and long-term implications of potential policy reforms to guide decisions.
(3) How can we establish best practices to support cross-border collaboration, regulatory harmonization, and global consistency in (bio)pharmaceutical development and manufacturing? How can regulators and firms effectively navigate multicountry approval processes and balance speed, safety, and equity in new drug development?
Regulatory requirements for R&D and manufacturing often vary from country to country, but there is a growing need for global harmonization and consistency (Irowa-Omoregie et al., 2024). Governments acknowledge the need for a national and international strategy (e.g., Health Canada, 2021), and several initiatives are being conducted by The International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). These cross-country collaboration and harmonization efforts can help reduce duplicate efforts and simplify processes for industry, increase bargaining power to lower prices, reduce social disparities to improve patient access, and accelerate innovation.
Future OM research can have several contributions to global harmonization and collaboration efforts. In current practice, there are multiple prominent research directions with (1) the involvement of patients as research partners, collaboratively guiding decisions on the design and execution of clinical trials, (2) the use of real-world data (RWD) and real-world evidence (RWE) to complement clinical trials and accelerate drug development, and (3) innovative approaches to clinical trials for small populations, including sample size
OM models can guide public–private partnerships and cross-border collaborations not only for new drug development but also for the establishment of global data centers and networks. Empirical and analytical models can support multicountry risk-sharing strategies by informing decisions on resource allocation and policy design. In particular, cross-border collaboration and subsidy schemes can help pool risks and resources to promote orphan drug development and incentivize investments in data infrastructure. Network optimization models can guide the strategic placement of clinical trial sites and data centers to maximize global participation. Open innovation models can facilitate knowledge generation and collaboration between universities, patients, regulators, and industry.
Building on global efforts to harmonize regulation and data sharing, OM research can help regulators and firms navigate multicountry approval processes to balance speed, safety, and equity. For example, future research can design new mechanisms to coordinate regulatory resources, data, and expertise across countries to streamline approval processes. Such global pooling and collaboration mechanisms could align data requirements, coordinate scientific and regulatory reviews, and facilitate evidence sharing. By linking shared data systems with global coordination frameworks, these initiatives could help accelerate drug development, review, and approval timelines.
Incentive programs and subsidies
There is a large body of OM research on the use of incentive and subsidy schemes in the pharmaceutical industry. For example, incentive schemes have been analyzed to support new drug development and project management under uncertainty (Limon et al., 2023; Tang et al., 2015b), pharmaceutical supply chain coordination (Arifoğlu and Tang, 2022), and hospital workload management (Andritsos and Tang, 2018). Although most of the existing OM research focuses on a classical (nonorphan) pharmaceutical setting, these methods can be extended to orphan drug development and supply chains. Few OM studies have also specifically addressed the challenges of orphan drug development. For example, Olsder et al. (2023b) examined the problem of allocating limited government subsidies to patients and pharmaceutical manufacturers. They developed a Stackelberg game and analyzed the impact of government subsidies to encourage innovation and increase patient access to orphan drugs. In a follow-up study, Olsder et al. (2023a) examined the role of subsidies in incentivizing drug repurposing (i.e., converting a drug from off-label to on-label use) for unmet medical needs. They developed a game-theoretic model and analyzed optimal subsidy allocations to induce drug conversion. Subsidy programs have been analyzed for applications beyond the pharmaceutical industry, including implementations in developing economies (Tang et al., 2024; Yu et al., 2018, 2020). Building on the OM literature, we propose the following research questions.
(1) How can a structured approach be established to support drug development efforts for ultra-rare diseases? What are the best practices for ultra-rare diseases to support the advancement of promising preclinical studies into commercial production?
Although orphan drug development is already challenging, the landscape becomes even more complex for “ultra-rare” conditions (those that affect fewer than 1 in 50,000 people). Drug development efforts for ultra-rare diseases have largely been driven by nonprofit organizations, patients, and their families. Several promising drugs are currently in preclinical development through partnerships with universities, small biotechnology companies, and patient organizations. However, the extremely small size of the market makes it difficult to build an attractive business case to support the advancement of these drugs in later stages. As a result, many promising drugs for ultra-rare diseases are lost in the so-called “valley of death,” which refers to the failure to advance from preclinical studies to more advanced clinical trials due to limited funding and commercial interest.
To entice the development of new drugs for ultra-rare diseases, future OM research can explore new collaboration mechanisms between public and private partners. For example, hybrid financing models can be built to complement various funding sources such as venture capital, crowdfunding, and philanthropic investments. In addition, future research can develop frameworks to prioritize efforts for ultra-rare diseases and create synergies through alternative approaches such as basket trials. Off-label use can also provide a viable and rapid solution to unmet medical needs. In particular, new data- and model-driven approaches can be developed to fully exploit the potential use of existing treatments through off-label prescription. These models can help match the right patients with the best off-label treatment options. Strengthening global data-sharing initiatives can further accelerate access to the right diagnosis and treatment. Because rare and ultra-rare diseases involve small patient populations dispersed across regions, collaborative data networks could help aggregate clinical evidence and connect researchers, regulators, and patient groups. OM research can help design efficient and equitable data-sharing mechanisms that improve coordination, interoperability, and participation incentives.
(2) How can we incentivize the development of new technologies and initiatives to accelerate orphan drug development, such as organ-on-a-chip and global data-sharing platforms?
A well-known challenge in the development of new drugs is the long, expensive, and risky R&D processes. However, new technologies can provide innovative solutions to reduce risks and costs. An example is the organ-on-a-chip technology, a microdevice that can mimic a human organ and help understand how a drug works in the human body (Leung et al., 2022). Although organ-on-a-chip technology is still in its infancy, it has the potential to transform clinical trials and drug discovery. Other examples include the use of image processing and large language models to diagnose diseases and/or inform genomics. Data-driven approaches are relatively more mature and can help improve patient access to accurate diagnosis and treatment. However, the implementation of data-driven methods may require substantial infrastructure with data centers, patient registries, and even cross-regional data collection and analysis efforts. Several initiatives have been established to support these aspects, such as the NIH’s Bridge2AI program, which aims to generate a flagship dataset to support artificial intelligence (AI)-driven biomedical research. Another example is the ARPA-H program to support AI-driven approaches to drug repurposing for rare diseases.
The growing use of global databases and data-sharing platforms will help accelerate drug development and improve diagnostic accuracy. Building on these initiatives, future OM research can explore how to effectively design and manage global data-sharing ecosystems (i.e., ensuring data quality, privacy protection, interoperability, and equitable access). OM-driven frameworks can help optimize the coordination of these platforms among stakeholders, and promote efficient and transparent collaboration in the development of new drugs and diagnostics.
The OM community can play a critical role in streamlining the global guidelines on the use of AI in drug development and manufacturing. Governments and regulators are increasingly receptive to AI and OM applications in the pharmaceutical industry, and the recent ICH Q13 guidelines have generated enthusiasm (Martagan et al., 2024). To support these initiatives, AI/OM researchers could work with regulators to achieve global compliance and consistency. For example, game-theoretic models can guide the industry on the optimal timing and frequency of information exchange with regulators. AI/OM models can identify the minimum data or evidence requirements for effective interactions between regulators and industry. Future research can also inform globally accepted eligibility criteria and compliance-monitoring strategies for accelerated drug development programs.
(3) How to optimally allocate limited resources, such as subsidies and grants, to stimulate innovation and improve patient access? How to strike the right balance between incentivizing the development of new drugs with different risk–benefit profiles?
Limited resources such as subsidies and grants must be effectively allocated to maximize social impact. Future OM research can explore how to equitably allocate limited budgets across different drug categories, including treatments for rare diseases, ultra-rare diseases, and other high-risk or high-cost conditions. These decisions can be challenging in practice because different R&D projects involve different costs, risks, and social impacts. In the context of orphan drugs, these trade-offs are further complicated by different categories of treatments. For example, developing drugs for ultra-rare diseases may not be financially viable for manufacturers, highlighting the critical role of subsidies. Future empirical and analytical models can guide equitable prioritization and resource allocation strategies by estimating the impact of investments in treatments with different risk–benefit profiles, ultimately supporting innovation and patient access.
Future research can support the development of national frameworks to guide strategic decisions and maximize social impact. For example, the UK Rare Diseases Framework presents a national vision to achieve faster diagnosis and better coordination of care for patients with rare diseases. OM methodologies can inform such national strategies, guide resource allocation decisions, evaluate trade-offs, and translate policy goals into practical solutions. Despite ongoing global efforts, more than
When designing subsidy or resource allocation schemes, governments may face trade-offs between rare diseases and more common diseases. Allocating resources to rare diseases helps promote innovation and equity for underserved patients, whereas prioritizing common diseases may yield broader health benefits but risk neglecting vulnerable populations. Addressing this dilemma requires an ethical and transparent framework. Future OM research can develop multicriteria optimization frameworks and game-theoretic models to guide equitable allocation of limited public funds. Collectively, these new models and insights can help policymakers design balanced resource allocation strategies that support both innovation and equitable patient access.
Innovative pricing and coverage schemes
Orphan drugs can save lives, but many remain inaccessible to patients due to their high prices. In response to these challenges, OM research has explored alternative strategies for drug pricing and coverage. For example, several studies examined outcome-based payment models in which patients pay only if treatment proves beneficial to them. The analysis of outcome-based payments dates back to the early 2000s, when So and Tang (2000) examined the effect of outcome-based reimbursement on drug dosage. More recently, Adida (2021) and Xu et al. (2022) developed analytical models using game theory to analyze the impact of outcome-based payment on drug prices and social welfare. Studies showed that pay-for-performance schemes can ultimately lead to higher drug prices in certain settings. Other approaches such as fee-for-service and indication-based pricing have also been explored (Adida, 2024; Guo et al., 2019). However, only a limited number of OM studies have considered the specific setting of rare disease treatments. For example, in addition to subsidies, Olsder et al. (2023b) examined an exogenous pricing mechanism in which an independent multistakeholder consortium sets the price of orphan drugs. Inspired by the BeNeLuxA initiative, they developed a Stackelberg game to analyze the impact of exogenous pricing on drug development, social welfare, and patient access. Building on OM research, we propose the following research questions on orphan drug pricing and coverage.
(1) What pricing models are most appropriate for orphan drugs? How can we develop new pricing strategies to reflect the unique features of advanced treatments, such as gene therapy and personalized medicine?
The pricing and coverage mechanisms for orphan drugs vary widely between countries, leading to social inequalities (Irowa-Omoregie et al., 2024). Future OM research can help identify the best pricing models to promote global consistency and improve patient access. However, the pricing of orphan drugs presents unique challenges. Market dynamics are particularly complex due to small patient populations, and most settings are monopolistic with extended exclusivity periods. Even after exclusivity expires, competition in the biopharmaceutical market (large molecules) remains limited compared to the generic drug market (small molecules), because large-molecule drugs cannot be easily reproduced. Their production requires additional research and development due to the complexity of biomanufacturing processes. These factors collectively influence the bargaining power of governments, payers, and other stakeholders. However, there are several initiatives to support local and global price negotiations for certain expensive drugs. Promising examples include the BeNeLuxA initiative in Europe, where an independent international consortium negotiates prices, and the Inflation Reduction Act, where Medicare negotiates prices for certain medicines. Although there is growing interest in innovative price control mechanisms (e.g., cross-country negotiations and price caps), their implications for society and industry are not fully understood. Future OM research can help develop new approaches, including game-theoretic models, bargaining models, or risk-sharing agreements, to examine the short- and long-term implications of novel price control mechanisms and guide global policies.
There is a growing need to explore innovative pricing and reimbursement models that reflect the unique features of advanced therapies. Consider gene therapy, which repairs defective or missing genes in a patient’s body. These therapies are one-time, expensive treatments with long-term, transformative benefits. However, their unique characteristics challenge current approaches to pricing and coverage. A well-known example is GSK’s Strimvelis, a gene therapy for severe combined immunodeficiency, a rare pediatric disease (Senior, 2017). The treatment involves ex-vivo transduction of the patient’s stem cells with a gamma retrovirus containing the human adenosine deaminase gene. This one-time gene therapy costs around $665,000, but GSK uses outcome-based pricing with a money-back guarantee (Senior, 2017). This is a life-changing treatment, but it comes at a high price for patients. What is the best pricing and coverage mechanism for advanced treatments that offer lifetime benefits? How do we assess their long-term value to patients, payers, and society? Inspired by the salient features of these drugs, new approaches have been proposed, including the option of free retreatment when the drug’s effect wanes after a period of time. Other novel approaches include annuity-like payment models, subscription-based models, or indication-based pricing mechanisms (Adida, 2024; Fattahi et al., 2025; Rebitzer and Rebitzer, 2023; Senior, 2017). However, there is still limited understanding of which pricing and coverage strategies are most appropriate for these advanced therapies and how to enhance patient access.
(2) How can payers address the problem of decision-making with little data? Can we develop new approaches to inform coverage decisions with limited data?
Coverage and reimbursement decisions for orphan drugs vary widely among countries and may even be made on a case-by-case basis (Chambers et al., 2020; Health Canada, 2021). These decisions typically depend on an assessment of the potential costs and benefits of the drug. However, evaluating the cost-effectiveness is particularly challenging for orphan drugs due to limitations in available evidence (see Section 2.3 for details). Future OM research can help address these challenges by guiding payers to make better decisions with a small amount of data. For example, AI and OM models can leverage existing data in global networks and federated platforms to generate insights on rare disease prevalence, estimate disease progression, and predict patient response. AI and OM models can support innovative trial designs, such as master protocols and basket trials, which evaluate multiple diseases and/or drugs simultaneously by exploiting their common characteristics (Groft et al., 2021). In addition, analytical models can support the development of new policies based on RWD and RWE. Bayesian models and other data-driven approaches can enable dynamic (staggered) reimbursement mechanisms, where decisions are adjusted based on RWD/RWE collected over time (e.g., Coverage with Evidence Development program of the Centers for Medicare & Medicaid Services).
(Bio)pharmaceutical manufacturing
Manufacturing and supply chain decisions under random supply, demand, or yield have received considerable attention from the OM community. For example, studies have investigated vaccine supply chains under demand and supply uncertainty (Cho and Tang, 2013; Mak et al., 2022) and manufacturing systems under yield uncertainty (Tao et al., 2012). Empirical and analytical approaches have been developed to efficiently manage the quality and limited capacity of manufacturing systems (Andritsos and Tang, 2014; Bendoly and Tang, 2021), and support new products and technologies (Huang et al., 2018). Recent studies have also addressed the specific challenges of (bio)pharmaceutical manufacturing. For example, Wang et al. (2024a) developed a Bayesian decision framework to guide biomanufacturing harvesting decisions under limited production data. Similarly, Martagan et al. (2023) and Koca et al. (2023) developed stochastic optimization models to increase biomanufacturing yield under process uncertainty. These models have been implemented in practice, resulting in high cost savings. In collaboration with industry partners, Martagan et al. (2024) published a comprehensive dataset from a continuous tablet-manufacturing process to support the development of new OM research. Although OM research has helped transform many industries, its application in biomanufacturing remains limited and represents a significant opportunity for impact.
(1) What are the most effective strategies for (bio)pharmaceutical companies to address the unique challenges of small data? How can these processes be optimized to ensure cost reduction and supply chain robustness?
Orphan drug production faces additional economic challenges due to small production volumes and limited historical data to guide process optimization. Future OM research can help the industry by systematically applying predictive and prescriptive analytics to optimize biopharmaceutical-manufacturing processes with limited data. For example, learning-by-doing models using Bayesian approaches can guide operational decisions to reduce risks and costs based on additional process data collected over time (Wang et al., 2024a). Optimization models can inform scale-up decisions, bridging the gap between lab-scale development and commercial production of orphan drugs. Future OM research can guide the adoption of new technologies and process intensification strategies through a multidisciplinary approach based on OM, AI, and life sciences (Martagan et al., 2023). New predictive models that augment life science mechanistic models with advanced AI techniques can help identify quality issues in advance. Optimal control algorithms can help reduce process risks and costs, and digital twins can help support manufacturing and supply chain resilience. In summary, a systematic implementation of optimal learning models, capacity planning frameworks, and advanced analytics can help mitigate biomanufacturing challenges posed by small data and high process uncertainty.
The use of pooling, specialization, or a combination of both strategies presents another promising direction for managing scarce resources. Technically, the concept of pooling refers to redesigning parts of the supply chain by aggregating demand, resources, products, or capacity to reduce uncertainty or mitigate its effects (Betcheva et al., 2021). In the context of (bio)pharmaceutical manufacturing, pooling decisions could involve the use of shared resources (e.g., production capacity, materials, or expertise) within or across facilities to mitigate risks and reduce costs. For example, modular production units can be pooled to manufacture multiple therapies in a high-mix, low-volume drug-manufacturing environment or to support flexible capacity allocation across sites. However, specialization may be necessary when processes or technologies are highly specific to a drug or service. Therefore, future OM research can examine how to balance pooling and specialization decisions (e.g., when to share or dedicate resources) to achieve resilient and cost-effective biomanufacturing.
Despite their potential benefits, OM-driven approaches involve implementation challenges to realize their full potential in the (bio)pharmaceutical industry (Martagan and Dai, 2025). First, it is important to develop transparent and explainable models in order to maintain stakeholder trust and meet regulatory expectations. Second, the regulatory landscape surrounding AI and OM applications in biomanufacturing continues to evolve but still presents uncertainties. Third, there is still a talent gap to successfully lead and implement OM projects in the biomanufacturing industry. Bridging this talent gap requires experts with interdisciplinary skill sets, combining OM, life sciences, and data science. Addressing these challenges is important to realize the full potential of OM in practice. Future OM research should continue to examine these potential issues and develop frameworks that combine methodological rigor with practical and regulatory feasibility. We refer to Martagan and Dai (2025) for a roadmap outlining how OM and AI applications can be synergized to advance biomanufacturing.
(2) What innovative models and strategies can be developed to facilitate small-scale production and delivery of personalized biopharmaceuticals and gene therapies?
Advances in biotechnology and gene therapy have stimulated a growing interest in personalized drug manufacturing, with production scales as small as
Personalized medicine supply chains for gene therapies and biopharmaceuticals present several challenges. First, managing these supply chains requires close coordination among patients, hospitals, and manufacturers. In particular, biological materials such as blood have a limited shelf life, and therefore manufacturing and transportation activities must be conducted within strict time constraints to ensure quality and safety. Manufacturing and transportation activities must also be synchronized with clinical schedules. Furthermore, variability in biological processes poses operational challenges in delivering the right drug, with the right quality and quantity, at the right time. From an OM perspective, queueing, scheduling, and stochastic optimization models can help design agile production and supply chain systems under yield and quality uncertainty. Network coordination models can help synchronize the use of limited manufacturing and hospital capacity, balance information and material flow between manufacturing sites and hospitals, and optimize logistics between stakeholders. Looking ahead, future research can explore new perspectives such as magistral drug manufacturing in hospitals and pharmacies (Yu et al., 2026).
Addressing the aforementioned research questions requires the industry to adopt a systematic transformation toward an OM-driven mindset. Experience and lessons learned from other industries could offer valuable insights to support this transition. For example, industries such as retail, aerospace, automotive, and high-tech manufacturing have successfully implemented Industry 4.0 and 5.0 initiatives to strengthen supply chain resilience in high-mix, low-volume production environments. The biomanufacturing industry can benefit from adopting best practices from other industries. For example, future OM research can guide the adoption of automation, digital twins, and Internet of Things-enabled systems that connect physical and digital operations in biomanufacturing. Data-driven capacity planning and prediction models can help manage complex biological systems under yield uncertainty. OM research can inform operational decisions related to scheduling, inventory management, and risk pooling in small-batch production. Other industries have effectively used modular process design, risk-based maintenance, and traceability frameworks to ensure quality and compliance. Integrating these Industry 4.0 and 5.0 principles with OM models can help build more flexible and data-driven “factories of the future” in the biomanufacturing industry.
Developing economies
A growing body of OM literature supports the needs of consumers and supply chains in developing economies. OM research has focused on a variety of use cases in LMICs, including agriculture and retail. For example, prior studies examined aggregation mechanisms for smallholder farmers (An et al., 2015) and information-sharing mechanisms between farmers in developing economies (Chen and Tang, 2015; Liao et al., 2017; Tang et al., 2015a; Xiao et al., 2020). Several studies also examined supply chain operations to optimize replenishment decisions (Gui et al., 2018; Zhang et al., 2017) and subsidy allocation decisions in developing economies (Tang et al., 2024; Yu et al., 2020). Inspired by the challenges of developing economies, the concept of “supply chains with the poor as suppliers or distributors” offers significant opportunities for future research (Sodhi and Tang, 2014). In general, not-for-profit operations are gaining increasing attention from the OM community. For example, the Production and Operations Management journal has a not-for-profit OM department currently led by Professor Christopher Tang.
The application of OM methodologies to drug development, manufacturing, and distribution in LMICs remains relatively understudied and represents a major research opportunity. A key priority for patients with rare diseases in LMICs is improving access to accurate diagnosis and treatment. Achieving this goal requires considering multiple factors, including infrastructure, education, workforce development, financing, social awareness, regulations, and business models. The discussion below focuses on a few selected aspects to stimulate new OM research in this area.
(1) How can we develop new business models for not-for-profit pharmaceutical manufacturing to support rare disease patients living in LMICs?
Future research can help develop new not-for-profit business models for rare disease patients living in LMICs, and also optimize existing models to achieve greater impact. A promising example is Medicines Development for Global Health, a not-for-profit organization focused on improving access to medicines in LMICs (MDGH, 2025). Their operations are self-funded and independent of major philanthropic funders, governments, and pharmaceutical companies. In contrast, other approaches have explored the advantages of collaboration between nonprofit and for-profit stakeholders to provide affordable medicines in LMICs (e.g., Scudellari, 2011). Future research can help these organizations better understand which business models are most appropriate for their specific goals and needs, and how to design them for maximum impact. Moreover, future research can guide new initiatives by for-profit pharmaceutical companies to better address the needs of LMICs, including tiered pricing, multicountry pricing agreements, and partnerships with local stakeholders to improve production and distribution. Although the pharmaceutical industry has been adopting more inclusive business models, successful implementations in LMICs remain limited (Access to Medicines Foundation, 2024).
Future research can also examine strategies to support local pharmaceutical manufacturing in LMICs. Emerging technologies such as modular manufacturing and platform technologies may support smaller-scale, cost-effective, and resilient production systems tailored to local demand. OM models can guide technology adoption, capacity planning, and supply chain design decisions to support local production and improve patient access in underserved regions.
(2) How can we design resilient supply chains for resource-constrained settings? How could OM models inform risk-pooling mechanisms, tiered pricing agreements, or last-mile distribution in resource-constrained areas?
Developing economies face major challenges due to limited resources and infrastructure. However, OM research can help design new supply chain strategies to support patients in low-resource settings. In particular, the concept of pooling presents an opportunity to more effectively manage limited resources in LMICs. Pooling has a wide range of applications in healthcare (Betcheva et al., 2021; Jiang and Sodhi, 2019). For example, hospitals can share diagnostic and testing equipment or storage space between a network of hospitals. In addition, joint procurement strategies and purchasing alliances can help consolidate demand and improve purchasing power in developing economies. For example, the UNICEF’s Supply Division consolidates orders from LMICs and purchases medicines on their behalf to improve patient access (Betcheva et al., 2021). Financing mechanisms can also involve pooling, in which governments and patient organizations combine funds from different sources in low-resource settings.
Although pooling and specialization strategies have been successfully applied in various healthcare settings, their application to rare diseases and developing economies remains limited. In this context, future OM research could examine the pooling of scarce diagnostic and treatment resources between regions, regional or cross-country risk pooling agreements to balance supply and demand, and shared manufacturing and logistics networks to reduce fixed costs. However, previous research also shows that pooling can increase operational costs in certain settings with heterogeneous patient populations (Betcheva et al., 2021; Jiang and Sodhi, 2019). These insights are particularly relevant for rare diseases, where patients are few, diverse, and often require highly specialized resources. Furthermore, OM models can inform tiered pricing schemes and last-mile distribution strategies to ensure the timely delivery of medicines to remote areas. Together, these research directions can translate the principles of operational efficiency and resilience into actionable strategies that support equitable access in developing economies.
Conclusions and a call to action
The Sustainable Development Goals (SDGs) of the United Nations highlight the need for affordable and equitable access to healthcare (SDG 3: Good Health and Well-Being). There are significant opportunities for the OM community to help advance the SDGs by fostering synergies across different goals and disciplines (Sodhi and Tang, 2024). Consistent with the goals of SDG 3, this paper reflects on various challenges and opportunities in the rare disease landscape from the perspectives of governments, industry, payers, and patient organizations.
As an important step forward, the United Nations published a resolution recognizing the challenges faced by rare disease patients and their families (United Nations, 2023). This resolution highlights the societal relevance of rare diseases and the urgent need for change. It is our social responsibility to recognize these challenges and improve access to diagnosis, treatment, and care for patients in need. These initiatives also represent a timely opportunity for future OM research, consistent with the goal of socially responsible OM (Lee and Tang, 2018). A multidisciplinary approach that synthesizes insights from OM, data science, AI, and life sciences can help drive innovation and improve public health. Together, as the OM community, we can continue to push the boundaries of OM research (Kumar and Tang, 2022; Tang, 2022) and work toward a future where rare disease patients receive the care they deserve. Together, we can help make the world a better place.
Supplemental Material
sj-pdf-1-pao-10.1177_10591478261455121 - Supplemental material for Rare diseases are not rare: Challenges and opportunities for OM research
Supplemental material, sj-pdf-1-pao-10.1177_10591478261455121 for Rare diseases are not rare: Challenges and opportunities for OM research by Tugce Martagan in Production and Operations Management
Footnotes
Acknowledgments
This work was funded by the Dutch Research Council through the NWO-VIDI program. I thank the speakers and participants of the 10th Annual Rare Disease Day (Boston, February 2025) for their insightful discussions, which helped improve the content of this paper. I also thank Prof. Hau Lee and Prof. Mohan Sodhi for organizing this special issue. Finally, I would like to express my sincere gratitude to Prof. Chris Tang for his valuable mentorship.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the VIDI Talent Program of the Dutch Research Council (NWO, Dutch: Nederlandse Organisatie voor Wetenschappelijk Onderzoek).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Notes
How to cite this article
Martagan T (2026) Rare diseases are not rare: Challenges and opportunities for OM research. Production and Operations Management x(x): 1–15.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.